 Jesús García-Jiménez1
Jesús García-Jiménez1 Luis Gutiérrez-Rojas2,3,4*
Luis Gutiérrez-Rojas2,3,4* Sara Jiménez-Fernández3,5
Sara Jiménez-Fernández3,5 Pablo José González-Domenech2,3María D. Carretero2Manuel Gurpegui2,3
Pablo José González-Domenech2,3María D. Carretero2Manuel Gurpegui2,3- 1Southern Mental Health Clinical Management Unit, Santa Ana Hospital, Motril, Spain
- 2Department of Psychiatry, University of Granada, Granada, Spain
- 3Psychiatry and Neurosciences Research Group (CTS-549), Institute of Neurosciences, University of Granada, Granada, Spain
- 4Granada Mental Health Clinical Management Unit, Hospital Clínico San Cecilio, Granada, Spain
- 5Child and Adolescent Mental Health Service, Jaén University Hospital Complex, Jaén, Spain
Objective: The aim of this study is to determine the prevalence of three possible diagnostic specifiers, namely predominant polarity (PP) throughout illness, polarity of the first episode and early age at onset, in a sample of bipolar disorder (BD) patients and their association with important socio-demographic, clinical and course-of-illness variables.
Methods: A retrospective and naturalistic study on 108 BD outpatients, who were classified according to the PP, polarity of the first episode and early age at onset (≤ 20 years) [vs. late (>20 years)] and were characterized by their demographics, clinical data, functionality and social support, among others features. After bivariate analyses, those variables showing certain association (P value < 0.25) with the three dependent variables were entered in logistic regression backward selection procedures to identify the variables independently associated with the PP, polarity of the first episode and early age at onset.
Results: The sample consisted of 75 women ad 33 men, 74% with type I BD and 26% with type II. Around 70% had depressive PP, onset with a depressive episode and onset after age 20. Depressive PP was independently associated with depressive onset, higher score on the CGI severity scale and work disability. Onset with depressive episode was associated with type II BD, longer diagnostic delay and higher score on family disability. Early age at onset (≤ 20 years) was associate with younger age, longer diagnostic delay, presence of ever psychotic symptoms, current use of antipsychotic drugs and higher social support score.
Conclusions: The results of this study show that BD patients with depressive PP, onset with depression and early age at onset may represent greater severity, because they are frequently associated with variables that worsen the prognosis. Our findings match up with the conclusions of two systematic reviews and we also include a disability factor (at family and work) that has not been previously reported. This work contributes to the use of polarity and age at onset in BD patients, as it can become a useful instrument in the prognostic and therapeutic applications.
Bipolar disorder (BD) is a chronic mood disorder with a global prevalence of 1–5% (1, 2), which is associated with high comorbidity rates, a large number of premature deaths due to suicide and a worse social and work performance (3–5). All of those characteristics entail a significant economic impact due to both direct and indirect costs (1) and require an effective diagnostic and therapeutic approach.
Diagnostic manuals [the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) (6) and the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (7)] compile the diagnostic criteria to correctly diagnose each of the episodes appearing in BD (mania, hypomania, and depression). The DSM-5 also proposes the use of specifiers for BD and related disorders, called Diagnostic Specifiers (DS) (7). The use of these DS adds relevant information on factors of poor prognosis of the acute relapse, allows focusing on the most conflicting points and, therefore, it leads to a more individualized approach to BD. Currently, the DSM-5 has accepted the use of nine DS for BD (7). For example, the DS “anxious distress” is associated with a higher risk of suicide, longer acute episodes and a worse response to treatment. Thus, a patient with an acute decompensation who also meets the criteria of “anxious distress” will present a risk of suicidal behavior significantly higher than another patient without this DS and, therefore, the treatment of this patient should especially consider this circumstance.
Several concepts related to BD have been proposed as DS in recent years, such as insight or response to lithium, but our study focuses on two of them, the age of onset (AO) and the polarity [polarity at onset (OP)and predominant polarity(PP)]. In the literature, many original articles conclude that AO, OP, and PP are associated with important prognostic factors (see below). However, two systematic reviews recently published indicate the existence of some contradictory associations, which could have influenced that they were not finally included in the DS list of the DSM-5 (8, 9). Regarding the AO, the meta-analysis of Joslyn et al. (9) indicates that patients under 20 years of age at BD onset show more frequently a greater diagnostic delay (10–12), longer delay in treatment initiation (9–14), they have more severe depressive symptoms (10–12, 15), high comorbidity with anxiety disorders (15–17) and higher risk of substance abuse (18, 19), all of which are associated with worse clinical course. The authors of this meta-analysis also report that the methodological variability and criteria when establishing a cut-off point for AO was very high among the selected studies and it could be a determining factor when no statistical association was found with variables that classically have also been related to a poor prognosis and early AO, such as psychotic symptoms (20) or suicidal risk (21).
The PP, defined as the tendency to present more frequently manic or depressive decompensations, and the OP or type of polarity of the index episode have been studied in another systematic review (8). The results of this study suggest that patients who are usually decompensated to the manic pole, i.e., manic PP (MPP), usually initiates with a manic episode (22–24), respond better to atypical antipsychotics and mood stabilizers (25) and they are frequently consumers of toxic substances prior to the onset of BD (24, 26, 27). Regarding depressive PP (DPP) patients, the most frequent initial episode found is of depressive characteristics (22, 28) and they present more suicidal risk (24, 26) and comorbidity with anxiety disorders (29). DPP also seems to be associated with a greater diagnostic delay (22, 28) and it has a characteristic pharmacological profile due to a greater use of quetiapine and lamotrigine (25). Again, the need to unify methodology and criteria in the study of the PP is pointed out, because contradictory results were also detected despite all these associations. These inconsistencies must be clarified before being able to recommend the systematic use of polarity when approaching the study of BD (8).
We conducted a study on a sample of outpatients diagnosed with BD. The main objective was to describe the prevalence of OP, PP, and AO. The second objective was to analyze the sociodemographic, clinical and therapeutic characteristics that are significantly associated with the three main variables of the study. Thus, we aim to analyze the usefulness of OP, PP, and AO as DS contributing to individualize and, therefore, optimize the clinical approach of BD.
Methods
Participants
The methodology used has been previously described by Gutiérrez-Rojas et al. (30). In summary, a psychiatrist (LGR) collected data from BD patients receiving treatment at an outpatient mental health clinic in the city of Jaén (Spain). A total of 210 patients were identified as suffering from BD. Out of these 210 patients, four had died (three by suicide), and 35 could not be located; of the remaining 171 patients, 16 (9%) refused to participate, nine fulfilled the exclusion criteria (see below), and 38 did not fulfill the diagnostic criteria. The remaining 108 patients were interviewed as they were attending the outpatient clinics or by specific appointment, after providing their informed consent to participate in the study. The patients were specifically interviewed for this research purpose in a personal appointment. They usually went to the clinic with their principal caregiver. The protocol was approved by the Ethics Committee of the Jaén Hospital Complex. Patients under 18 years of age and patients affected by a severe cognitive deficit, as dementia or intellectual disability, were excluded.
Assessment Instruments and Procedure
Axis I psychopathology was measured in each interview using the Structured Clinical Interview for DSM-IV (SCID) (31). The referring psychiatrist was asked to confirm the diagnosis (according to the same criteria) and the therapeutic regimen.
The study has a retrospective design. Several data (for example the presence of affective symptoms, level of disability or social support) was measured in the initial interview meanwhile prognosis variables (as number and kind of episodes, PP, OP, AO and family history of mental disorders) were analyzed using the information from the medical records and from the interview with the patients and their principal caregivers. The following information was collected in the initial interview: sociodemographic data (sex, age, marital status, number of siblings and children, educational level and work status), clinical variables (AO of symptoms, age at diagnosis of BD, years of illness, OP [depressive, (hypo) manic or mixed], number of episodes of each polarity, number of hospital admissions and suicide attempts). Diagnosis delay was defined as the time (in years) between the first appearance of affective symptoms and the correct diagnoses of BD. The OP refers to first mood episode that the patient suffers and not to the index episode of consultation. The AO of symptoms was defined as the age at which the first manic episode or major depressive episode occurred and was classified as early (≤ 20 years) or late (>20 years). The PP was defined by the higher number of episodes of one subtype (manic) or the other (depressive), as previous studies have used (28). The principal reasons to adopt this definition are the relatively small sample size, the cross-sectional nature of the assessments, and the retrospective design. If we had chosen to divide the sample in three groups (with the option of indeterminate PP) we would not get enough statistical power.
The affective symptomatology was evaluated using the Young's scale for manic symptoms –YMRS- (32) and the Hamilton's scale for depression –HDRS- (33). Due to the naturalistic design of the study, we included euthymic and non-euthymic patients. Moreover, we administered the Clinical Global Impression (CGI) severity scale (34).
Social support was measured by Social Adaptation Self-evaluation Scale (SASS) (35) which is made up of 21 items that explore the functioning of the patient in five areas: work, family, leisure, social relationships, and motivational skills. The score ranges between 0 and 60 (a higher score means better social support).
To evaluate the substance abuse of legal (tobacco and alcohol) and illegal substances we used the Fagerström Test for Nicotine Dependence (FTND) (36) and the CAGE questionnaire (37). To measure the three principal dimensions of the disability (work, social and family) we used the Sheehan Disability Scale (SDS) (38). This scale is a brief self-rated assessment of impairment caused by a disease in three dimensions: work or studies, social life (and leisure) and family life (home responsibility) during the last week. Each item has 11 possible responses ranging from 0 through 10 (0, not at all; 1–3, mildly; 4–6, moderately; 7–9, markedly; and 10, extremely). The psychometric properties of SDS have been previously evaluated in BD (39) and have been validated in Spanish (40). Significant functional impairment for work as well as for social life and family life has been defined as a score of 7 or higher in patients with a positive screen for BD (41).
Statistical Analysis
Collected data were summarized using descriptive measures (mean, median, standard deviation, frequency, and percentage). Continuous variables were analyzed using the Student's t-test or analysis of variance (ANOVA) and categorical variables were determined using the Pearson's chi-square test or the Fisher's exact test. For the bivariate analysis, as cautious approach to multiple testing, rather than using Bonferroni correction, we have set two-tail statistical significance was set at P < 0.01. The analyses were performed using the Statistical Package for the Social Sciences (SPSS) program (version 24).
Differences between groups were analyzed using standard bivariate parametric or nonparametric tests as appropriate, comparing sociodemographic variables, the subtype of BD, the presence of psychotic symptoms at some point throughout the disease, current or past substance abuse, delay in diagnosis delay, types of psychopharmacological treatments, illness duration, social support and disability extent. These variables were entered in the logistic regression backward selection procedures examining their association with dependent outcomes of interest (PP, OP and early AO of BD) when their bivariate association reached a P value < 0.25, in order to adjust for potential confounding variables. All logistic regression models fit well according to the Hosmer-Lemeshow goodness of fit test (42).
Results
The sample included 108 participants (33 men and 75 women) with a median age of 48 ± 14 years. A total of 80 (out of 108, 74.1%) participants met the type I BD criteria and 28 (25.9%) participants were diagnosed with type II BD. Regarding the PP, 29.6% of the sample showed MPP compared to the 70.4% that showed DPP. Table 1 summarizes the main sociodemographic, clinical and course-of-illness variables related with the PP. The depressive PP group (in comparison with the manic PP) showed significantly higher proportion of patients with type I BD (vs. type II), more diagnostic delay, higher score on the CGI severity scale, higher number of depressive episodes, more frequently onset with depressive episode and lower proportion of patients with ever psychiatric hospitalization.
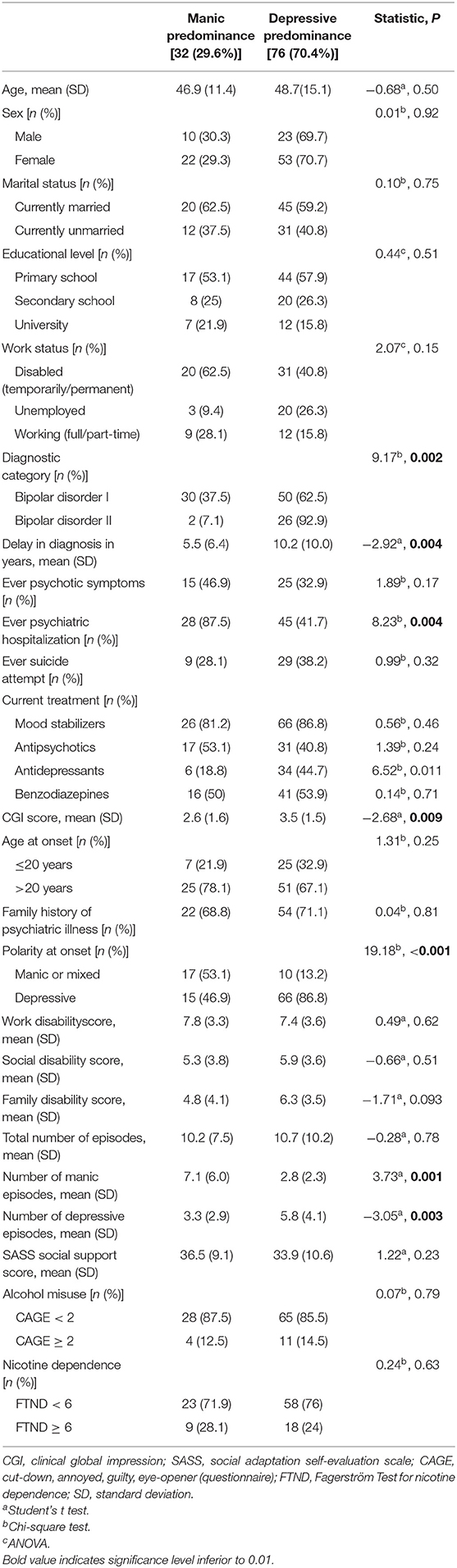
Table 1. Predominant polarity and their associated variables.
Regarding the onset polarity, a depressive beginning of the illness appeared in 75% of patients (25% started with a manic episode). The age at onset in the sample had a mean of 30.4 (SD, 13.7) years. Early onset (≤ 20 years) was present in 30% of the patients [late onset (>20 years) in 70%]. Onset with manic polarity showed the same proportion (25%) among those with early onset than among those with late onset. Table 2 shows the results of the bivariate analysis of variables according to early or late age at onset. The factors associated with an early age at onset were: younger age, higher proportion of unmarried marital status, ever use of antipsychotic drugs and larger diagnosis delay.
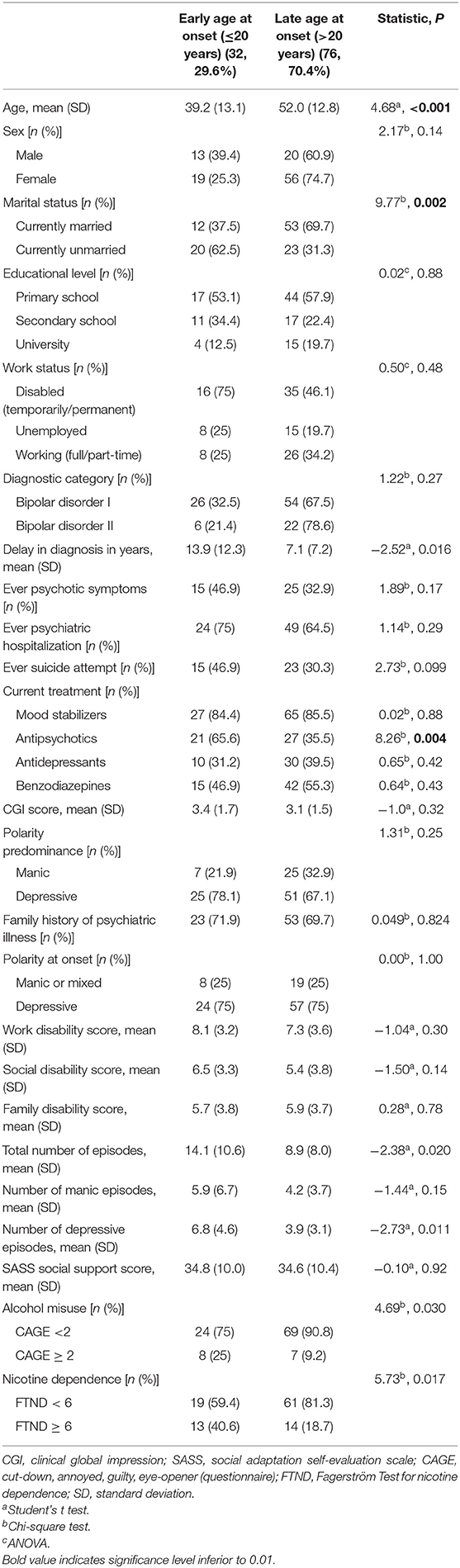
Table 2. Association of variables with early or late onset in bipolar disorder.
Multivariate logistic regression analyses were performed to identify the variables significantly associated with depressive PP, depressive polarity of the first episode and early age at onset (Tables 3–5, respectively). The factors associated with depressive PP (Table 3) were the following: being work disabled due to the BD, having had depressive onset and higher score on the CGI severity scale (the use of antidepressant medication was significant in the bivariate but not in the multivariate analysis). Variables associated with an onset depressive polarity (Table 4) were type II BD, higher family disability (rated on the SDS score) and a longer diagnostic delay. Finally, early age at onset was significantly associated with younger age, longer diagnostic delay, higher social support score, presence of ever psychotic symptoms and current use of antipsychotic drugs (Table 5).
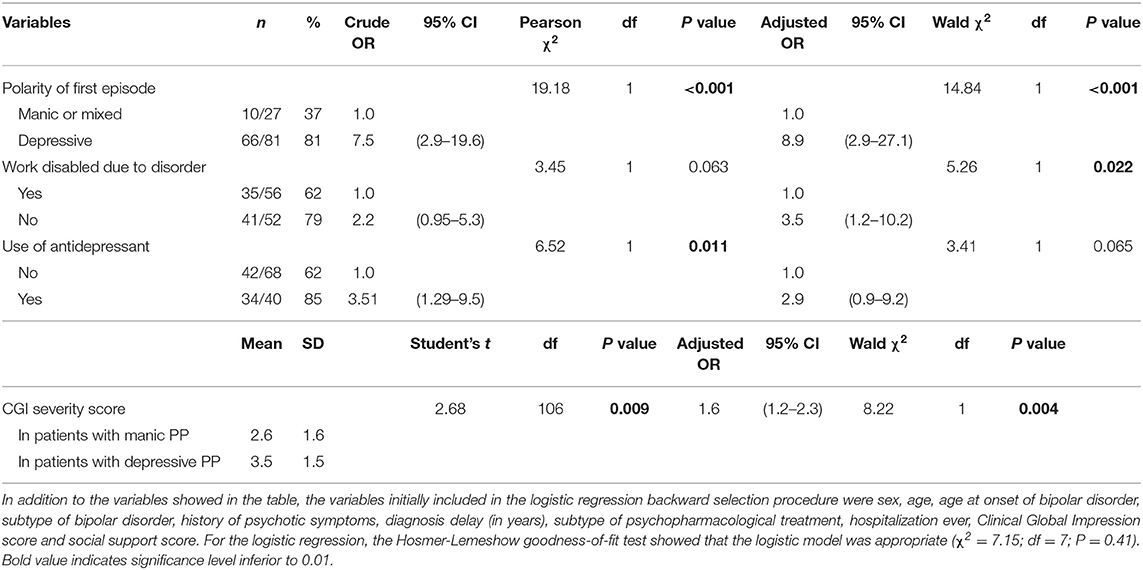
Table 3. Logistic regression of factors associated with a depressive predominant polarity in a bipolar disorder sample (n = 108).
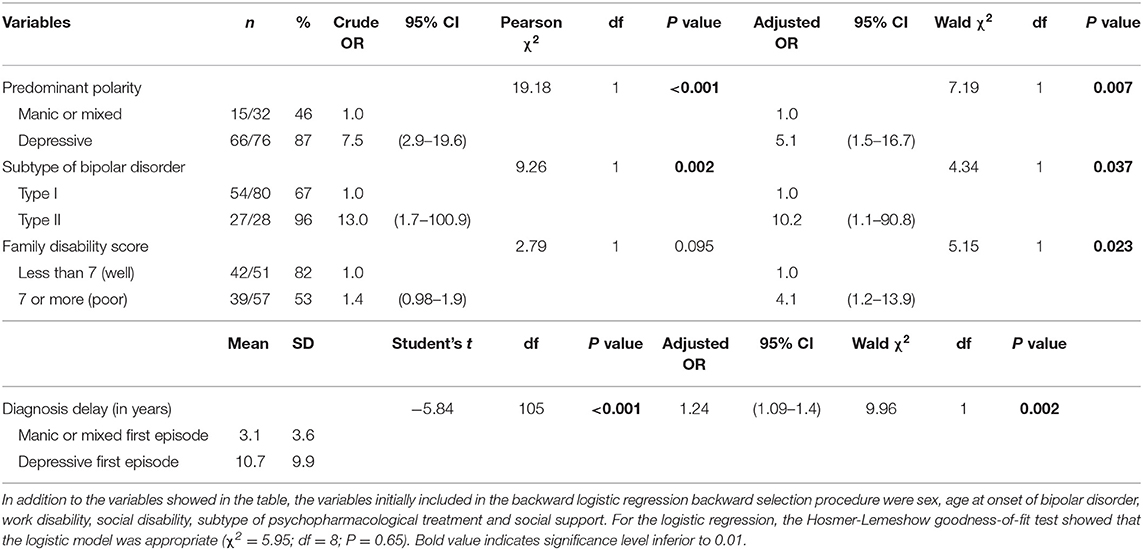
Table 4. Logistic regression of factors associated with depressive polarity of the first episode in a bipolar disorder sample (n = 108).
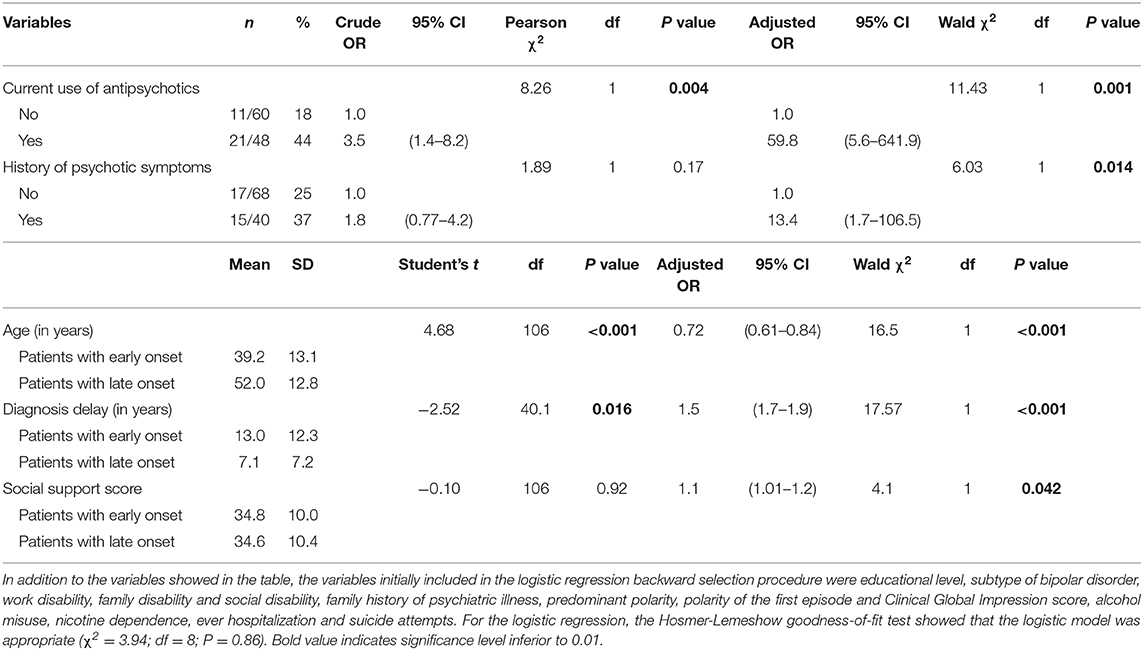
Table 5. Logistic regression of factors associated with an early age of onset (≤ 20 years) in a bipolar disorder sample (n = 108).
Discussion
In the present study, we measured the prevalence and the associated variables of PP, of polarity of the onset episode and of early (vs. late) age at onset.
For the PP, we selected a less restrictive definition according to other studies (27, 43), allowing us to determine the polarity in the whole sample, obtaining a distribution of 29.6% for manic PP (32 out of 108) compared to 70.4% for depressive PP (76 out of 108). However, other authors have used a more restrictive definition of the PP (26). No consensus on what is the best option has been reached to date. A consensus is needed because the percentage of patients in which the PP can be determined based on each definition ranges between 42.4 and 71.8%, reaching even 100% for the less restrictive definition (8). Similarly, the distribution of manic PP and depressive PP in the literature ranges from 12 to 55% and from 17 to 34%, respectively (8). We selected a less restrictive definition because our sample size was small, which might explain the high percentage of patients with depressive PP, and such an open definition was needed to increase the statistical power. Therefore, close definitions with criteria that are more difficult to meet are recommended for larger samples; probably these criteria would reflect better the practical reality, where some cases show no clear predominance of one or the other polarity (indeterminate PP), which can represent up to 30% of the total of BD patients (44).
Regarding the association of PP with clinical variables, we find that patients with depressive PP show higher frequency of work disability, a worse clinical condition according to the CGI severity score and more frequent onset by a depressive episode. Consistency between PP and polarity at the onset episode is one of the most replicated findings in the literature (22–24, 28) and our results confirmed the association between depressive PP and depressive polarity at the first episode (the association between manic PP and manic first episode did not reach statistical significance in our study). According to our findings, the polarity of the first episode can become a key factor in the early stages of BD because it may predict later PP in a high percentage of cases, contributing to establish a suitable clinical path from the beginning. Our data on more frequent work disability and worse scores on the CGI severity scale are also consistent with the literature reporting a higher severity in depressive PP due to its more frequent association with variables of poor prognosis, such as comorbidity with anxiety disorders (29) or more frequent and more serious relapses (27). However, in contrast with previous studies, we found no association between depressive PP and other relevant variables, such as high indexes of suicidal behavior (22, 24, 26, 45) or more delay until the right diagnosis of BD (22, 28). These inconsistencies could be explained by differences in methodology and designs of the studies; for example, different criterion to define PP or prospective rather than retrospective design.
The second diagnostic specifier that we analyzed was polarity of the first episode. We found that depressive onset was notably the quite high in our sample (76 out of 108 patients, 70.4%), in line with other studies reporting onset with a depressive episode in two thirds of BD patients (27, 46, 47), although this proportion can be different if mixed episodes are considered (48). In consistency with previous studies (47, 48), we found that depressive onset was associated with type II BD, being one of the factors contributing to a worse perceived quality of life in these patients compared to patients diagnosed with type I BD (49).
One of the most novel findings in our study (not previously reported) is the relation found between depressive onset and both diagnosis delay and family disability, two variables indicating poor prognosis. These two variables affect negatively the clinical course and would strengthen the idea that the long-term clinical course of patients with depressive PP would be worse compared to patients with manic PP (50). Again, some authors found other associations between depressive onset and variables of poor prognosis that we could not replicate, such as higher rates of suicidal behavior (51) or more frequent and lasting relapses (27, 51).
Besides, we aimed to analyze the role of age at onset, since several studies suggest its role as a prognosis variable for BD (9, 52, 53). We decided to split age at onset into early (≤ 20 years) and late (>20 years), based on the criterion used by other authors (53), obtaining among 29.6% (32 out of 108) of the participants an early age at onset, slightly superior to the 22% described by Belteczki et al. (53). Indeed, we found a more frequent association with variables of poor prognosis in these patients; in particular, higher frequency of ever psychotic symptoms and use of antipsychotic drugs, worse social support and higher diagnostic delay, in consistency with the findings described by other authors (52, 53). These results are in line with the most recent meta-analysis on age at onset (9), according to which the risk of poor prognosis increases when the onset of symptoms has been early. However, it remains to be clarified whether the variables found have a direct effect per se or if these variables are related with higher suicidal behavior (21) or more mixed symptoms (17) found in these patients. Reaching a consensus among researchers must be a fundamental issue when studying age at onset and its role as a DS in BD (9).
Finally, we should mention the findings of a recently published 5-year prospective study (54), which develops the idea of time ill, according to which not only the number of episodes is important but also the total time that each patient remains in each one of the phases of the disease would determine the prognosis. The mentioned study showed that patients with manic PP spend more time in the manic phase than depressive PP and undetermined PP patients, but it is worth noting that manic PP patients also remained euthymic for longer periods and, therefore, compensated. These are additional data supporting the better evolution of manic PP compared to depressive PP patients.
Among the strengths of our study, we would like want to point out that since it is an observational study, the characteristics of the sample closely resemble that of patients in the usual clinical practice and that we find associations that had not previously been described, such as the association of depressive onset with diagnostic delay and high family disability. All the participants were evaluated by the same clinical researcher and accurately fulfilled the diagnostic criteria of BD. Among the limitations, we should mention the cross-sectional design itself, the relatively small sample size and the selection of an open definition for the PP, which can be less stable over time and, therefore, it can influence the long-term stability of the findings.
In conclusion, PP, polarity of the first episode and age at onset can be good complementary to the current diagnostic criteria for BD because of both their usefulness for the classification and their prognostic impact. All these three characteristics may be differential in each patient and may contribute to focus the psychoeducation and the clinical path on the most important aspects of each patient from the beginning of the disorder, allowing a much more specific approach (8). Certainly, the use of PP, polarity of the first episode and age at onset have some limitations, such as the lack of consensus in their definitions or which features show the patients of undetermined PP. However, the results of the present and previous studies are important and continue representing a promising line of research in which follow-up studies sharing a common methodology are needed.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the protocol was approved by the Ethics Committee of the Jaén Hospital Complex. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
LG-R has participated in the design of the study, collected the data, participated in the statistical analysis, the interpretation of the data and the drafting of the article. JG-J, PG-D, SJ-F, and MC have participated in the interpretation of the data and the drafting of the article. MG has participated in the design of the study, the statistical analysis, the interpretation of the data and the drafting of the article. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Fagiolini A, Forgione R, Maccari M, Cuomo A, Morana B, Dell'Osso MC, et al. Prevalence, chronicity, burden and borders of bipolar disorder. J Affect Disord. (2013) 148:161–9. doi: 10.1016/j.jad.2013.02.001
2. Ketter T. Diagnostic features, prevalence, and impact of bipolar disorder. J Clin Psychiatry. (2010) 71:e14. doi: 10.4088/JCP.8125tx11c
3. Costa Lda S, Alencar ÁP, Nascimento Neto PJ, dos Santos Mdo S, da Silva CG, Pinheiro Sde F, et al. Risk factors for suicide in bipolar disorder: a systematic review. J Affect Disord. (2015) 170:237–54. doi: 10.1016/j.jad.2014.09.003
4. Hayes J, Miles J, Walters K, King M, Osborn D. A systematic review and meta- analysis of premature mortality in bipolar affective disorder. Acta Psychiatry Scand. (2015) 131:417–25. doi: 10.1111/acps.12408
5. Coryell W, Scheftner W, Keller M, Endicott J, Maser J, Klerman GL. The enduring psychosocial consequences of mania and depression. Am J Psychiatry. (1993) 150:720–7. doi: 10.1176/ajp.150.5.720
6. World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10). Geneva: WHO (1992).
7. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association (2013).
8. García-Jiménez J, Álvarez-Fernández M, Aguado-Bailón L, Gutiérrez-Rojas L. Epidemiological and clinical variables related with the predominant polarity on bipolar disorder: a systematic review. Rev Psiquiatr Salud Ment. (2019) 12:52–62. doi: 10.1016/j.rpsm.2017.06.008
9. Joslyn C, Hawes DJ, Hunt C, Mitchell PB. Is age of onset associated with severity, prognosis, and clinical features in bipolar disorder? A meta-analytic review. Bipolar Disord. (2016) 18:389–403. doi: 10.1111/bdi.12419
10. Azorin JM, Kaladjian A, Adida M, Fakra E, Hantouche E, Lancrenon S. Correlates of first-episode polarity in a French cohort of 1089 bipolar I disorder patients: role of temperaments and triggering events. J Affect Disord. (2011) 129:39–46. doi: 10.1016/j.jad.2010.08.020
11. Drancourt N, Etain B, Lajnef M, Henry C, Raust A, Cochet B, et al. Duration of untreated bipolar disorder: missed opportunities on the long road to optimal treatment. Acta Psychiatr Scand. (2013) 127:136–44. doi: 10.1111/j.1600-0447.2012.01917.x
12. Suominen K, Mantere O, Valtonen H, Arvilommi P, Leppämäki S, Paunio T, et al. Early age at onset of bipolar disorder is associated with more severe clinical features but delayed treatment seeking. Bipolar Disord. (2007) 9:698–705. doi: 10.1111/j.1399-5618.2007.00388.x
13. Post RM, Leverich GS, Kupka RW, Keck PE Jr, McElroy SL, Altshuler LL, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. (2010) 71:864–72. doi: 10.4088/JCP.08m04994yel
14. Dagani J, Signorini G, Nielssen O, Bani M, Pastore A, Girolamo G, et al. Meta-analysis of the interval between the onset and management of bipolar disorder. Can J Psychiatry. (2017) 62:247–58. doi: 10.1177/0706743716656607
15. Azorin JM, Bellivier F, Kaladjian A, Adida M, Belzeaux R, Fakra E, et al. Characteristics and profiles of bipolar I patients according to age- at- onset: findings from an admixture analysis. J Affect Disord. (2013) 150:993–1000. doi: 10.1016/j.jad.2013.05.026
16. Biffin F, Tahtalian S, Filia K, Fitzgerald PB, de Castella AR, Filia S, et al. The impact of age at onset of bipolar I disorder on functioning and clinical presentation. Acta Neuropsychiatrica. (2009) 21:191–6. doi: 10.1111/j.1601-5215.2009.00399.x
17. Mick E, Biederman J, Faraone SV, Murray K, Wozniak J. Defining a developmental subtype of bipolar disorder in a sample of nonreferred adults by age at onset. J Child Adolesc Psychopharmacol. (2003) 13:453–62. doi: 10.1089/104454603322724841
18. Perlis RH, Miyahara S, Marangell LB, Wisniewski SR, Ostacher M, DelBello MP, et al. Long- term implications of early onset in bipolar disorder: data from the first 1000 participants in the systematic treatment enhancement program for bipolar disorder (STEP- BD). Biol Psychiatry. (2004) 55:875–81. doi: 10.1016/j.biopsych.2004.01.022
19. Cate-Carter TD, Mundo E, Parikh SV, Kennedy JL. Early age at onset as a risk factor for poor outcome of bipolar disorder. J Psychiatr Res. (2003) 37:297–303. doi: 10.1016/S0022-3956(03)00052-9
20. Coryell W, Fiedorowicz J, Leon AC, Endicott J, Keller MB. Age of onset and the prospectively observed course of illness in bipolar disorder. J Affect Disord. (2013) 146:34–8. doi: 10.1016/j.jad.2012.08.031
21. Chengappa KN, Kupfer DJ, Frank E, Houck PR, Grochocinski VJ, Cluss PA, et al. Relationship of birth cohort and early age at onset of illness in a bipolar disorder case registry. Am J Psychiatry. (2003) 160:1636–42. doi: 10.1176/appi.ajp.160.9.1636
22. Baldessarini RJ, Tondo L, Vazquez GH, Undurraga J, Bolzani L, Yildiz A, et al. Age at onset versus family history and clinical outcomes in 1665 international bipolar- I disorder patients. World Psychiatry. (2012) 11:40–6. doi: 10.1016/j.wpsyc.2012.01.006
23. Baldessarini RJ, Undurraga J, Vázquez GH, Tondo L, Salvatore P, Ha K, et al. Predominant recurrence polarity among 928 adult international bipolar I disorder patients. Acta Psychiatr Scand. (2012) 125:293–302. doi: 10.1111/j.1600-0447.2011.01818.x
24. Forty L, Jones L, Jones I, Smith DJ, Caesar S, Fraser C, et al. Polarity at illness onset in bipolar I disorder and clinical course of illness. Bipolar Disord. (2009) 11:82–8. doi: 10.1111/j.1399-5618.2008.00654.x
25. Popovic D, Torrent C, Goikolea JM, Cruz N, Sánchez-Moreno J, González-Pinto A, et al. Clinical implications of predominant polarity and the polarity index in bipolar disorder: a naturalistic study. Acta Psychiatr Scand. (2013) 129:366–74. doi: 10.1111/acps.12179
26. Nivoli AM, Colom F, Pacchiarotti I, Murru A, Scott J, Valentí M, et al. Treatment strategies according to clinical features in a naturalistic cohort study of bipolar patients: a principal component analysis of lifetime pharmacological and biophysic treatment options. Eur Neuropsychopharmacol. (2013) 23:263–75. doi: 10.1016/j.euroneuro.2012.07.015
27. Colom F, Vieta E, Daban C, Pacchiarotti I, Sánchez-Moreno J. Clinical and therapeutic implications of predominant polarity in bipolar disorder. J Affect Disord. (2006) 93:13–7. doi: 10.1016/j.jad.2006.01.032
28. Daban C, Colom F, Sanchez-Moreno J, Garcia-Amador M, Vieta E. Clinical correlates of first-episode polarity in bipolar disorder. Compr Psychiatry. (2006) 47:433–7. doi: 10.1016/j.comppsych.2006.03.009
29. Rosa AR, Andreazza AC, Kunz M, Gomes F, Santin A, Sanchez-Moreno J, et al. Predominant polarity in bipolar disorder: diagnostic implications. J Affect Disord. (2008) 107:45–51. doi: 10.1016/j.jad.2007.07.021
30. Gutiérrez-Rojas L, Jurado D, Gurpegui M. Factors associated with work, social life and family life disability in bipolar disorder patients. Psychiatry Res. (2011) 186:256–60. doi: 10.1016/j.psychres.2010.06.020
31. First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clinical Interview for DSM-IV Axis I Disorders—Clinician Version (SCID-I-CV). New York, NY: New York State Psychiatric Institute, Biometrics Research Department (1996).
32. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
33. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56
34. Guy W. Early Clinical Drug Evaluation (ECDEU) Assessment Manual. Rockville: National Institute Mental Health (1976).
35. Bosc M, Dubini A, Polin V. Development and validation of a social functioning scale, the social adaptation self-evaluation scale. Eur Neuropsychopharm. (1997) 7:57–70. doi: 10.1016/S0924-977X(97)00420-3
36. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström test for nicotine dependence: a revision of the Fagerström tolerance questionnaire. Br J Addict. (1991) 86:1119–27. doi: 10.1111/j.1360-0443.1991.tb01879.x
37. Ewing JA. Detecting alcoholism: the CAGE questionnaire. JAMA. (1984) 252:1905–7. doi: 10.1001/jama.1984.03350140051025
38. Sheehan DV, Harnett-Sheehan K, Raj BA. The measurement of disability. Int Clin Psychopharmachol. (1996) 11:89–95. doi: 10.1097/00004850-199606003-00015
39. Arbuckle R, Frye MA, Brecher M, Paulsson B, Rajagopalan K, Palmer S, et al. The psychometric validation of the Sheehan Disability Scale (SDS) in patients with bipolar disorder. Psychiatry Res. (2009) 165:163–74. doi: 10.1016/j.psychres.2007.11.018
40. Bobes J, Baldía X, Luque A, García M, González MP, Dal-Ré R. Validation of the Spanish versions of the Liebowitz social anxiety scale, social anxiety and distress scale and Sheehan disability inventory for the evaluation of social phobia. Med Clin. (1999) 112:530–8.
41. Das AK, Olfson M, Gameroff MJ, Pilowsky DJ, Blanco C, Feder A, et al. Screening for bipolar disorder in primary care practice. JAMA. (2005) 293:956–63. doi: 10.1001/jama.293.8.956
42. Hosmer DW, Lemeshow S. Applied Logistic Regression. 2nd ed. New York, NY: John Wiley & Sons Inc (2000).
43. Henry C, Lacoste J, Bellivier F, Verdoux H, Bourgeois ML, Leboyer M. Temperament in bipolar illness: impact on prognosis. J Affect Disord. (1999) 56:103–8. doi: 10.1016/S0165-0327(98)00219-5
44. Vidal-Rubio SL, Balanzá-Martínez V, Cuenca M, Vila-Francés J, Vieta E, Romeu JE. Duration of euthymia and predominant polarity in bipolar disorder. J Affect Disord. (2018) 241:356–9. doi: 10.1016/j.jad.2018.08.001
45. González-Pinto A, Alberich S, Barbeito S, Alonso M, Vieta E, Martínez-Arán A, et al. Different profile of substance abuse in relation to predominant polarity in bipolar disorder. J Affect Disord. (2010) 124:250–5. doi: 10.1016/j.jad.2009.11.005
46. Etain B, Lajnef M, Bellivier F, Mathieu F, Raust A, Cochet B, et al. Clinical expression of bipolar disorder type I as a function of age and polarity at onset: convergent findings in samples from France and the United States. J Clin Psychiatry. (2012) 73:e561–6. doi: 10.4088/JCP.10m06504
47. Baldessarini RJ, Tondo L, Visioli C. First-episode types in bipolar disorder: predictive associations with later illness. Acta Psychiatr Scand. (2013) 129:383–92. doi: 10.1111/acps.12204
48. Tundo A, Musetti L, Benedetti A, Berti B, Massimetti G, Dell'Osso L. Onset polarity and illness course in bipolar I and II disorders: the predictive role of broadly defined mixed states. Compr Psychiatry. (2015) 63:15–21. doi: 10.1016/j.comppsych.2015.07.018
49. Judd LL, Schettler PJ, Akiskal HS, Maser J, Coryell W, Solomon D, et al. Long-term symptomatic status of bipolar I vs. bipolar II disorders. Int J Neuropsychopharmacol. (2003) 6:127–37. doi: 10.1017/S1461145703003341
50. Cremaschi L, Dell'Osso B, Vismara M, Dobrea C, Buoli M, Ketter TA, et al. Onset polarity in bipolar disorder: a strong association between first depressive episode and suicide attempts. J Affect Disord. (2017) 209:182–7. doi: 10.1016/j.jad.2016.11.043
51. Perugi G, Micheli C, Akiskal HS, Madaro D, Socci C, Quilici C, et al. Polarity of the first episode, clinical characteristics, and course of manic depressive illness: a systematic retrospective investigation of 320 bipolar I patients. Compr Psychiatry. (2000) 41:13–8. doi: 10.1016/S0010-440X(00)90125-1
52. Altamura AC, Buoli M, Cesana BM, Fagiolini A, de Bartolomeis A, Maina G, et al. Psychotic versus non-psychotic bipolar disorder: socio-demographic and clinical profiles in an Italian nationwide study. Aust N Z J Psychiatry. (2019) 53:772–81. doi: 10.1177/0004867418823268
53. Belteczki Z, Rihmer Z, Ujvari J, Lamis DA, Dome P. Differences in clinical characteristics between bipolar patients with current psychotic symptoms and those who have never been psychotic. Psychiatr Danub. (2018) 30:183–8. doi: 10.24869/spsih.2018.183
Keywords: bipolar disorder, age at onset, disability, polarity predominance, diagnosis delay
Citation: García-Jiménez J, Gutiérrez-Rojas L, Jiménez-Fernández S, González-Domenech PJ, Carretero MD and Gurpegui M (2020) Features Associated With Depressive Predominant Polarity and Early Illness Onset in Patients With Bipolar Disorder. Front. Psychiatry 11:584501. doi: 10.3389/fpsyt.2020.584501
Received: 17 July 2020; Accepted: 15 October 2020;
Published: 16 November 2020.
Edited by:
Zhaoyu Gan, Third Affiliated Hospital of Sun Yat-sen University, ChinaReviewed by:
Janardhan Y. C. Reddy, National Institute of Mental Health and Neurosciences (NIMHANS), IndiaKyooseob Ha, Seoul National University, South Korea
Copyright © 2020 García-Jiménez, Gutiérrez-Rojas, Jiménez-Fernández, González-Domenech, Carretero and Gurpegui. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis Gutiérrez-Rojas, Z3V0aWVycmV6cm9qYXNAdWdyLmVz