 Giuseppe Riva1,2
Giuseppe Riva1,2 Luca Bernardelli3
Luca Bernardelli3 Matthew H. E. M. Browning4
Matthew H. E. M. Browning4 Gianluca Castelnuovo1,2
Gianluca Castelnuovo1,2 Silvia Cavedoni1
Silvia Cavedoni1 Alice Chirico2Pietro Cipresso1,2Dirce Maria Bengel de Paula5
Alice Chirico2Pietro Cipresso1,2Dirce Maria Bengel de Paula5 Daniele Di Lernia2*
Daniele Di Lernia2* Javier Fernández-Álvarez2Natàlia Figueras-Puigderrajols6
Javier Fernández-Álvarez2Natàlia Figueras-Puigderrajols6 Kei Fuji7
Kei Fuji7 Andrea Gaggioli1,2
Andrea Gaggioli1,2 Jose Gutiérrez-Maldonado6
Jose Gutiérrez-Maldonado6 Upyong Hong8
Upyong Hong8 Valentina Mancuso1
Valentina Mancuso1 Milena Mazzeo2
Milena Mazzeo2 Enrico Molinari1,2
Enrico Molinari1,2 Luciana F. Moretti5
Luciana F. Moretti5 Angelica B. Ortiz de Gortari9,10
Angelica B. Ortiz de Gortari9,10 Francesco Pagnini2
Francesco Pagnini2 Elisa Pedroli1,11
Elisa Pedroli1,11 Claudia Repetto2Francesca Sforza3
Claudia Repetto2Francesca Sforza3 Chiara Stramba-Badiale1Cosimo Tuena1,2
Chiara Stramba-Badiale1Cosimo Tuena1,2 Clelia Malighetti2
Clelia Malighetti2 Daniela Villani2
Daniela Villani2 Brenda K. Wiederhold12,13
Brenda K. Wiederhold12,13- 1IRCCS Istituto Auxologico Italiano, Milan, Italy
- 2Department of Psychology, Università Cattolica del Sacro Cuore, Milan, Italy
- 3Become-Hub, Milan, Italy
- 4Virtual Reality and Nature Lab, Clemson University, Clemson, SC, United States
- 5Sociedad Española de Realidad Virtual y Psicología, Las Rozas – Madrid, Spain
- 6Department of Clinical Psychology and Psychobiology, University of Barcelona, Barcelona, Spain
- 7Division of Psychology, University of Tsukuba, Tokyo, Japan
- 8Department of Media and Communication, Konkuk University, Seoul, South Korea
- 9The Centre for the Science of Learning & Technology (SLATE), University of Bergen, Bergen, Norway
- 10Psychology and Neuroscience of Cognition Research Unit, University of Liège, Liège, Belgium
- 11Faculty of Psychology, University of eCampus, Novedrate, Italy
- 12Virtual Reality Medical Center, La Jolla, CA, United States
- 13Virtual Reality Medical Institute, Brussels, Belgium
Background: Living in the time of the COVID-19 means experiencing not only a global health emergency but also extreme psychological stress with potential emotional side effects such as sadness, grief, irritability, and mood swings. Crucially, lockdown and confinement measures isolate people who become the first and the only ones in charge of their own mental health: people are left alone facing a novel and potentially lethal situation, and, at the same time, they need to develop adaptive strategies to face it, at home. In this view, easy-to-use, inexpensive, and scientifically validated self-help solutions aiming to reduce the psychological burden of coronavirus are extremely necessary.
Aims: This pragmatic trial aims to provide the evidence that a weekly self-help virtual reality (VR) protocol can help overcome the psychological burden of the Coronavirus by relieving anxiety, improving well-being, and reinforcing social connectedness. The protocol will be based on the “Secret Garden” 360 VR video online (www.covidfeelgood.com) which simulates a natural environment aiming to promote relaxation and self-reflection. Three hundred sixty–degree or spherical videos allow the user to control the viewing direction. In this way, the user can explore the content from any angle like a panorama and experience presence and immersion. The “Secret Garden” video is combined with daily exercises that are designed to be experienced with another person (not necessarily physically together), to facilitate a process of critical examination and eventual revision of core assumptions and beliefs related to personal identity, relationships, and goals.
Methods: This is a multicentric, pragmatic pilot randomized controlled trial involving individuals who experienced the COVID-19 pandemic and underwent a lockdown and quarantine procedures. The trial is approved by the Ethics Committee of the Istituto Auxologico Italiano. Each research group in all the countries joining the pragmatic trial, aims at enrolling at least 30 individuals in the experimental group experiencing the self-help protocol, and 30 in the control group, over a period of 3 months to verify the feasibility of the intervention.
Conclusion: The goal of this protocol is for VR to become the “surgical mask” of mental health treatment. Although surgical masks do not provide the wearer with a reliable level of protection against the coronavirus compared with FFP2 or FFP3 masks, surgical masks are very effective in protecting others from the wearer’s respiratory emissions. The goal of the VR protocol is the same: not necessarily to solve complex mental health problems but rather to improve well-being and preserve social connectedness through the beneficial social effects generated by positive emotions.
Introduction
Background
Living in the time of the COVID-19 means experiencing not only a global health emergency but also extreme psychological stress that puts a strain on our identity and our relationships. Coronavirus and the associated isolation and quarantine require people to manage three different psychological dilemmas simultaneously (1).
i. the stress due to the disease,
ii. the inaccessibility to physical places,
iii. and the sense of community crisis.
The core stress of the disease comes from the worry and concerns about personal health and the health of friends and family members. This stress can be exacerbated both among general public and medical staff via the vicarious traumatization effect (2) when empathizing with those suffering, resulting in fatigue, physical decline, sleep disorder, irritability, inattention, fear, and despair (3).
The traumatic effects are further aggravated by living in quarantine and its restrictions on movement and social interaction. In fact, evidence has shown that quarantine causes significant psychological effects including post-traumatic stress symptoms, confusion, and anger (4).
The inaccessibility to physical places is one of the first clear negative effects of quarantine. A conflict arises that is provoked by losing access to physical places where people can meet and that we feel belongs to us. A “place” can be understood as any space delimited by borders and that gives identity to individuals and represents a space to be. Related to place is the concept of place attachment (5) which is the bonding of people to places. This bond includes cognitive and emotional components and is a common phenomenon observed across cultures with significant psychological benefits (6). However, quarantine disrupts place attachment, and therefore, has negative implications. As noted by Scannel and Gilford (6), separation from one’s significant place can be devastating: “broken or stretched place bonds are associated with physical health problems, lower grades, sadness, longing alienation, and disorientation” (pp. 256–257). Women tend to report stronger place attachment than men (6) and, therefore, the disruption of place attachment provoked by the quarantine may have stronger psychological effects in women.
Å crisis of the sense of community is caused by disconnect from the places where communities are born (7), and provide significant negative effect on subjective well-being (8, 9). The disruption of places produced by the quarantine also affects the communities that use these places to meet and interact. Without everyday places to meet at—such as the workplace and the classroom—friends and acquaintances are more difficult to reach and to interact with. This weakens social bonds and declines the social significance of the local community in terms of social capital and interpersonal support.
These negative psychological effects may be aggravated by other stressors such as having inadequate basic supplies (e.g., food, etc.), insufficient clear guidelines about actions to take and the prolonged duration of quarantine, the interruption of professional activities and the subsequent financial loss (4).
In this view, any strategy that aims to reduce the psychological burden of coronavirus is extremely necessary (10). As recently underlined by Holmes and colleagues (10): “There is an urgent need for the discovery, evaluation, and refinement of mechanistically driven interventions to address the psychological, social, and neuroscientific aspects of this pandemic. This includes bespoke psychological interventions to boost wellbeing and minimize mental health risks across society.” (p. 10). Crucially, given the mandatory loneliness resulting from lockdown measures, easy-to-use, inexpensive, and scientifically validated self-help solutions could be the key (11–16).
Aims
This pragmatic trial seeks to provide the evidence that a weekly self-help protocol based on a virtual reality experience—“The Secret Garden”, available in the www.covidfeelgood.com website—can help to overcome the psychological burden of the Coronavirus.
It is important to underline that the goal of the self-help protocol is not to provide a full structured psychological intervention, but to build the “surgical mask” of mental health support. Surgical Masks do not provide the wearer with a reliable level of protection against coronavirus (20%) versus the 95/99% of FFP2 and FFP3 masks. However, they are very effective in protecting others from the wearer’s respiratory emissions, and their use is significantly better than wearing a scarf.
The self-help VR protocol assessed in the trial aims to do the same. The goal is not to solve complex mental health problems, but rather to reduce the burden of the coronavirus: Specifically, the protocol aims at relieving anxiety and stress and improving well-being and social connectedness through these two assets:
i. The potential of (also) simulated nature for improving people’ wellbeing, health and ameliorating anxiety and depressive feelings (17–19) with or without a direct interaction with it (20). Crucially, simulated nature can ameliorate negative moods in the short-term, and besides individual preferences towards nature (20);
ii. The potential of all types of VR formats, including 360° videos, to resemble even distant, complex, even paradoxical scenarios in a realistic, immersive and engaging way, thus providing the illusion of being really “there”, in the simulated place (21–23).
This last asset provided by VR is the pathway to the transformation of people’s experiences in a several and profound ways (24–26). For instance, immersive experiences can enhance individuals’ personal efficacy and self-reflectiveness through the manipulation of the sense of presence, flow, and emotional engagement (27, 28). Moreover, VR’s unique ability to evoke complex emotions, which are drivers of people’ health, wellbeing and sense of social connection (29, 30), would allow designing unique experiences leading to long-terms benefits.
The protocol will be based on the same 10-min 360° VR video (“The Secret Garden”) used by Chirico and colleagues (29, 30).
“The Secret Garden” VR video has been developed through an integrated process involving psychologists, 3D artists, musicians, storytellers and designers (Figure 1). This immersive experience storyboard has been:

Figure 1 A screenshot of the “Secret Garden” VR experience.
● written by well-being psychologists to mimic the structure and the experience of walking in a Japanese garden (31) providing the visual (i.e., the flow of water) and auditory (i.e., the sound of running water) natural elements available outdoors.
● converted in a VR experience by 3D specialists using the Unreal Engine 4 technology.
● dubbed by a professional dubber in the different languages used in the trial using the back-translation method. In all languages a a slow, calm, clear voice provides a relaxation induction structured following the principles of Compassion Focused Therapy (32, 33). Specifically, the induction aims at deactivating the human threat protection system and activating the soothing system (with a mindset attended to giving and receiving care, affecting, and nurturance).
We decided to use a computer-graphic 360° video (artificial) instead of a video-recorded format (natural) for the following reasons. First, we selected a video whose efficacy in positive emotional induction was already validated in a previous study. Second, using computer-graphic it is easier to manipulate specific features of the natural environment aimed at improving positive affect (i.e., the extreme blossoming of the peach trees presented in the VR experience) that are more difficult to achieve using a real natural environment. Third, during lockdown was impossible access to real natural places.
Three hundred sixty–degree videos have the power to virtually transport users, immersing them in the video recording, allowing them to actively explore its content and experience the video from any angle. With this regard, as shown by Robertson and colleagues the neural representations of the part of the 360° video presented in VR (the scene within the current field of view) prime the associated representations of the full panoramic environment (34). In other words, 360° videos generate a dynamic interplay between memory and perception that can be used to improve the features of these cognitive processes and to update their content.
To anchor the generated update to the autobiographical memory of the user, at end of the VR exposure the subjects will be asked to perform together different tasks related to personal identity and interpersonal relationships (35). These tasks, are an adaptation of the different “emotional prescriptions” designed by the psychologist Guy Winch (35) to react to personal experiences that generate emotional pain: loneliness, rejection, or rumination. The tasks want to achieve the following goals: a) to pay attention and recognize emotional pain; b) work to treat it before it feels all-encompassing; c) monitor and protect self-esteem; d) find meaning even in difficult times. The full description of the tasks is provided in Table 1.
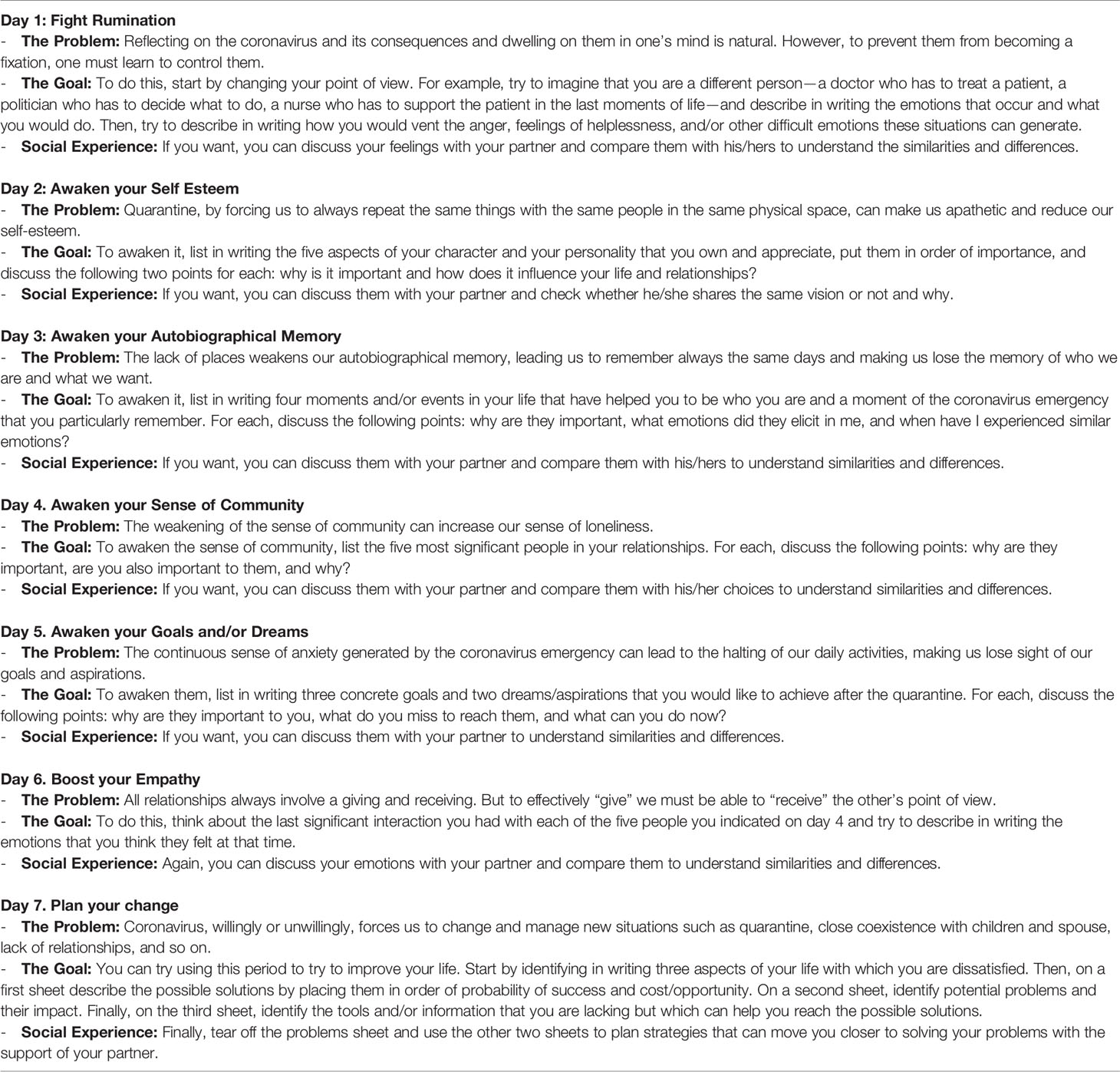
Table 1 Descriptions of the daily exercises.
Hypotheses
The study has the following hypotheses:
1. The use of the weekly VR self-help protocol will reduce the level of depression, anxiety, perceived stress, and hopelessness;
2. The use of the weekly VR self-help protocol will promote the relaxation and social connectedness of the participants.
Methods and Analysis
Study Design
This will be a multicentric pragmatic pilot randomized controlled trial involving individuals who have experienced the isolation and quarantine associated to the Coronavirus pandemic. In contrast to explanatory trials that often include highly selected, “ideal” patients, pragmatic trials adopt broader eligibility criteria that reflect the diversity of patients who are treated in routine situations (36). In accordance with the real-life approach of our study, we expect a heterogeneous patient population, which is the goal of pragmatic trials. The trial overall will show results that pertain to the heterogeneous population, including subgroups representative of the target population. Potential participants will be contacted through web, e-mail, or social media postings. Individuals who will express interest in participating to the trials will be contacted to verify if they meet the inclusion criteria (below). Each eligible participant will provide written informed consent for study participation.
After signing the informed consent, participants will be randomly assigned to the experimental (VR) or control (Waiting-list) conditions (Two-Group Random Assignment Pretest–Posttest Design). Baseline measures of anxiety, depression, perceived stress, general wellbeing, and relaxation will be collected at the baseline (Day 7), before the starting of the protocol (Day 0), at the end of the protocol (Day 7) and after a 2-week follow-up (Day 21). State measures of anxiety, perceived stress, and relaxation will be collected each day of the protocol after the experimental condition, from Day 1 to Day 7.
Randomization
Randomization will be done by a computer algorithm written in SAS (37). Participants will be randomly allocated in a 1:1 ratio, and using randomly chosen block sizes (37).
Sample
Each research group in all the countries joining the trial (at the moment Italy, Spain, and USA) will recruit two samples of at least 30 subjects. The experimental group will experience the VR protocol described below.
Inclusion criteria will be:
a. adult patients (≥18 years);
b. of mother tongue of the country where they will be enrolled;
c. have experienced at least two months of quarantine or isolation related to the coronavirus pandemic;
d. give full, written, informed consent;
e. have the availability of a smartphone and a cardboard VR headset;
f. availability and agreement of a partner for conducting the self-help component of the treatment.
To reflect routine, everyday practice, subjects will not excluded if they have other medical conditions, or are taking medication (38).
Exclusion criteria, assessed through an interview with the participants will be:
a. Visual of ear impairments that can limit the participation to the protocol.
b. Participants reporting vestibular and/or balance disorders.
Psychological Measures
Participants will complete two series of questionnaires.
The baseline, post intervention, and follow-up measures are a series of semi-trait questionnaires that will assess how the participants felt in the previous week. These instruments will assess perceived stress, depression and anxiety, hopelessness, social connectedness, fear of coronavirus, and social contacts interactions. The compilation will require approximately 20 min.
The state measures are a series of questionnaires and scales that assess how participants feel after the experimental procedure. They will be collected daily (from Day 1 to Day 7) immediately after the protocol and will assess state anxiety, self-reported stress, and relaxation. The compilation will require approximately 5–10 min.
Baseline, Post Intervention, and Follow Up Measures Collected at Day 0 and at Day 7
● Perceived Stress Scale (PSS): The PSS (39) is a widely used instrument for measuring individuals’ perceived stress. It assesses how much our daily situations are perceived as stressful, unpredictable, and ultimately overloading. Moreover, the PSS also assess the current level of perceived stress directly, providing a reliable and robust instrument for stress assessment. Items in the PSS assess feelings and thoughts the last month, however the scale will be adapted to assess perceived stress in the last week. The instrument is composed by 10 items on a 5-point Likert A composite score of the 10 items provide a general measure of perceived stress.
● Depression Anxiety Stress Scale (DASS-21): The DASS-21 (40) is a short version of the original instrument developed by Lovibond and it is composed of 21 items divided into 3 subscales that measure anxiety, depression, and perceived stress. The scale assesses how the participants felt in the previous 7 days on a 4-point Likert. Scores are computed individually for each subscale. A composite score of general distress is obtained by computing all the three subscale scores together.
● Beck Hopelessness Scale (BHS): The BHS (41) is a self-report instrument that measures pessimistic tendencies or negative attitude towards the future within three major aspects of hopelessness: feelings about the future, loss of motivation, and expectations. The scale is composed of 20 items with a True/False response.
● Social Connectedness Scale (SCS): The SCS (42) is composed of 8-items and aims at measuring how much the individual feels connected to other persons or to the social context. The scale asks to evaluate agreement or disagreement to several contextual statements on a 6-point Likert scale. Higher scores represent a higher sense of social connectedness.
● Fear of Coronavirus (FCOR): FCOR is a series of statements presented in (43) to measure the level of fear toward the COVID-19 pandemic. FCOR is composed of 8 items that explore different components of fear such as the personal experience of concern regarding the current situation, avoidance behaviors and attention bias. Each statement is evaluated on a 5-point Likert.
● Online and offline contact (COO): COO is a series of questions (44) to measure the number and quality of online and offline contacts during the COVID-19 pandemic. Individuals are asked to report the number of online contacts in the past week evaluating on a 5-point likert scale how close they felt to those contacts. The same two questions are repeated for offline contacts.
State Measures Collected From Day 1 to Day 7
● Smith Relaxation State Inventory 3 (SRSI3): The SRSI3 (45) is the revised form of the original Smith Relaxation State inventory and it measures both relaxation and perceived stresses. Individuals rate their agreement to several statements on a 6-point Likert scale. The scale is composed of 38 items; however, it is divided into several subscales that can be selected independently. For this protocol, the following subscales have been selected, for a total of 20 items: rest/refresh, energized, physical relaxation, at ease/peace, joy, mental quiet, aware, somatic stress, emotional stress, and cognitive stress.
● Subjective Units of Distress Scale (SUDS): The SUDS (46) is simple numeric rating scale from 0 to 100 that measures the level of distress perceived by the individual. It is a reliable measure of state distress, commonly used in cognitive behavioral therapy.
Post Intervention Measure Collected at Day 7
● Negative Effects Questionnaire (NEQ): The self-report measure consists of three parts for a total of 32 items (47). First, respondents endorse specific items in case they have occurred or not during treatment, yes/no (dummy coded as a variable: 1/0). Second, the respondents rate how negatively the negative effect was on four-point Likert-scale, ranging from “Not at all” to “Extremely”, 0–4 (“0” being minimum and “4” being maximum). Third, the respondents attribute the negative effect to “The treatment I received” (1) or “Other circumstances” (0) (dummy coded as a variable: 1/0).
● Simulation Sickness Questionnaire (SSQ): The self-report measure is composed by 16 items used to users’ level of sickness symptoms after a VR experience (48).
● Final Interview: This final interview aims at collecting any additional information related to practical challenges of using the VR app and coordinating the self-help social task.
Study Period
The enrolment is planned to start from June 2020 and will last until the planned number of enrolled patients has been met.
Outcomes
Considering the presented hypotheses, the primary outcomes expected for the group that will perform the experimental VR procedure compared to the control group are:
● A reduction in anxiety, depression, perceived stress, and hopelessness, as measured by DASS-21, PSS, and BHS.
● A reduction in state anxiety and subjective distress, as measured by SUDS.
● And an increase in relaxation, as measured by SRSI3.
Secondary outcomes of the protocol are
● a decrease in fear of the coronavirus, as measured by FCOR;
● an increase in social connectedness, as measured by SCS;
● an increase in feelings of closeness to online and offline contacts, as measured by COO.
Description of the Intervention
The 10-min “Secret Garden” 360° VR experience available on the www.covidfeelgood.com website will be used for one week, once per day. To experience the “Secret Garden” the sample will need:
- any Android of iOS smartphone with installed the YouTube App;
- any VR headset compatible with the Cardboard format. These headsets are easily available in online stores for a price ranging between 10 and 50 US$.
Each individual will involve a partner in the process who will share the VR exposure, to discuss the emotions and reflections induced by it. Specifically, at the end of the VR exposure the subjects will be asked to perform together different tasks related to personal identity and interpersonal relationships (35). The full description of the tasks is provided in Table 1.
Statistical Analysis
Categorical variables will be compared using Fisher or chi-square tests and continuous variables using t test or Mann-Whitney tests, as appropriate. Groups will be compared for variables such as sex, age, education, geographic area, stage of disease, type of proposed treatment, and other available data. To assess the effectiveness of the intervention, groups will be compared with a 2 × 2 repeated measure mixed ANOVA for the pre and post measures (factor Group X factor Time: pre and post). Analysis will be performed for all the relevant variables: perceive stress, anxiety, depression, hopelessness, fear of the coronavirus, and social contacts. A repeated measures ANOVA (factor Group × factor Time: day of the week) will compare treatment effects within the seven-day intervention, for all the relevant measures: relaxation, perceived stress, and state anxiety. Tests of statistical significance and confidence intervals will be two-sided; a p < 0.05 will be considered to be statistically significant. Statistical computations and data analysis will be performed using R, a multi-platform (Windows, UNIX, Mac OS), free software environment for statistical computing and graphics.
Power Size Calculation
Power size calculation was performed with GPower 3.1. Considering an anticipated effect size (f) of.25, an alpha set at.05, 2 groups, and a.95 statistical power, the total sample size required is N = 54.
Discussion
Living in the time of the coronavirus means experiencing not only a global health emergency but also extreme psychological stress that puts a strain on our identity and our relationships. The fears about personal health and the health of friends and family members, and the effects of the quarantine generate significant psychological effects including post-traumatic stress symptoms, depression confusion, and anger. These negative psychological effects may be enhanced by other stressors such as having inadequate basic supplies (i.e., food, masks, etc.), insufficient clear guidelines about actions to take and the duration of quarantine, the interruption of professional activities and the related financial loss (4). In this view, any strategy that aims to reduce the psychological burden of the coronavirus is extremely necessary (10). In particular, the outbreak of coronavirus is rapidly changing stakeholders’ attitudes towards e-mental health, and this should be harnessed given the fact that many technological solutions are not only cost-effective but nowadays the only possible intervention that confined individuals can receive (49). Despite the undoubted negative consequences of this context, it can be also conceived as an opportunity to achieve an implementable revolution in digital mental health (50).
This pragmatic pilot trial seeks to understand if and how a weekly self-help protocol—The Secret Garden—can help overcome the psychological burden of the coronavirus. To reach this goal, the protocol will use virtual reality (24) to provide a transformative experience (27, 51, 52) by offering a natural digital place in which subjects can relax and reflect. This effect will be enhanced by different daily social tasks aiming at facilitating a process of critical examination and eventually revision of core assumptions and beliefs. It is important to underline that the goal of the self-help protocol is not to provide a full structured psychological intervention, but to build the “surgical mask” of mental health support. Its goal is not to solve complex mental health problems, but rather to reduce the coronavirus of the by relieving anxiety and stress and improving interpersonal relationships: when a user is positive and healthy, he/she generates a positive social effect that contributes to the well-being of the community. If the present pragmatic pilot trial will support the feasibility of the approach, further actions to promote the dissemination and the use of the self-help protocol will be encouraged.
Ethics Statement
The trial is approved by the Ethics Committee of the Istituto Auxologico Italiano.
Author Contributions
GR conceived the original idea, designed the study and the original protocol. GR, AC, AO, DL, BW and MB wrote the paper. LB and FS developed the “Secret Garden” VR environment used in the study. BW supervised the clinical framework of the study. BW, JG-M, AO, LM, NF-P, MM, KF, DP, and UH contributed to the translations of the protocol in different languages. All authors contributed to the article and approved the submitted version.
Funding
This paper was supported by the Marie Skłodowska-Curie Innovative Training Networks AffecTech (project ID:722022 - https://www.affectech.org/) and Entwine (project ID: 814072 - https://entwine-itn.eu/) funded by the European Commission H2020.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer SV declared a past co-authorship with one of the authors GR to the handling Editor.
References
1. Riva G, Wiederhold BK. How Cyberpsychology and Virtual Reality Can Help Us to Overcome the Psychological Burden of Coronavirus. Cyberpsychol Behav Soc Network (2020) 5:227–9. doi: 10.1089/cyber.2020.29183.gri
2. Blair DT, Ramones VA. Understanding vicarious traumatization. J Psychosoc Nurs Ment Health Serv (1996) 34:24–30. doi: 10.3928/0279-3695-19961101-15
3. Cavalera C, Pepe A, Zurloni V, Diana B, Realdon O, Jiang R. A short version of the state shame and guilt scale (SSGS-8). TPM - Testing, Psychometrics, Methodology in Applied Psychology. (2017) 24(1):99–106. doi: 10.4473/TPM24.1.6
4. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
5. Low SM, Altman I. Place Attachment. In: Altman I, Low SM, editors. Place Attachment. Boston, MA: Springer US (1992). p. 1–12.
6. Scannell L, Gifford R. The experienced psychological benefits of place attachment. J Environ Psychol (2017) 51:256–69. doi: 10.1016/j.jenvp.2017.04.001
7. Silk J. The Dynamics of Community, Place, and Identity. Environ Plann A: Econ Space (1999) 31:5–17. doi: 10.1068/a310005
8. Farrell SJ, Aubry T, Coulombe D. Neighborhoods and neighbors: Do they contribute to personal well-being? J Community Psychol (2004) 32:9–25. doi: 10.1002/jcop.10082
9. Hooghe M, Vanhoutte B. Subjective Well-Being and Social Capital in Belgian Communities. The Impact of Community Characteristics on Subjective Well-Being Indicators in Belgium. Soc Indic Res (2011) 100:17–36. doi: 10.1007/s11205-010-9600-0
10. Holmes EA, O’Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L. et al: Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry (2020) 7(6): 547–60. doi: 10.1016/S2215-0366(20)30168-1
11. Villani D, Grassi A, Cognetta C, Toniolo D, Cipresso P, Riva G. Self-help stress management training through mobile phones: an experience with oncology nurses. Psychol Serv (2013) 10:315–22. doi: 10.1037/a0026459
12. Carissoli C, Villani D, Riva G. Does a meditation protocol supported by a mobile application help people reduce stress? Suggestions from a controlled pragmatic trial. Cyberpsychol Behav Soc Netw (2015) 18:46–53. doi: 10.1089/cyber.2014.0062
13. Freeman D, Haselton P, Freeman J, Spanlang B, Kishore S, Albery E, et al. Automated psychological therapy using immersive virtual reality for treatment of fear of heights: a single-blind, parallel-group, randomised controlled trial. Lancet Psychiatry (2018) 5:625–32. doi: 10.1016/S2215-0366(18)30226-8
14. Donker T, Cornelisz I, van Klaveren C, van Straten A, Carlbring P, Cuijpers P, et al. Effectiveness of Self-guided App-Based Virtual Reality Cognitive Behavior Therapy for Acrophobia: A Randomized Clinical Trial. JAMA Psychiatry (2019) 76:682–90. doi: 10.1001/jamapsychiatry.2019.0219
15. Lindner P, Hamilton W, Miloff A, Carlbring P. How to Treat Depression With Low-Intensity Virtual Reality Interventions: Perspectives on Translating Cognitive Behavioral Techniques Into the Virtual Reality Modality and How to Make Anti-Depressive Use of Virtual Reality–Unique Experiences. Front Psychiatry (2019) 10:792. doi: 10.3389/fpsyt.2019.00792
16. Di Lernia D, Cipresso P, Pedroli E, Riva G. Toward an Embodied Medicine: A Portable Device with Programmable Interoceptive Stimulation for Heart Rate Variability Enhancement. Sensors (Basel) (2018) 18:2–13. doi: 10.3390/s18082469
17. Berman MG, Kross E, Krpan KM, Askren MK, Burson A, Deldin PJ, et al. Interacting with nature improves cognition and affect for individuals with depression. J Affect Disord (2012) 140:300–5. doi: 10.1016/j.jad.2012.03.012
18. Roberts H, Van Lissa C, Hagedoorn P, Kellar I, Helbich M. The effect of short-term exposure to the natural environment on depressive mood: A systematic review and meta-analysis. Environ Res (2019) 2019:108606. doi: 10.1016/j.envres.2019.108606
19. Harshfield A, Manville C, Elmore NL, Smith P, Rincon DR, Hood C, et al. A scoping study on the link between exposure to or interaction with the natural environment and mental health outcomes. RAND (2019).
20. Browning MH, Mimnaugh KJ, van Riper CJ, Laurent HK, LaValle SM. Can Simulated Nature Support Mental Health? Comparing Short, Single-Doses of 360-Degree Nature Videos in Virtual Reality With the Outdoors. Front Psychol (2019) 10: 2–14. doi: 10.3389/fpsyg.2019.02667
21. Riva G, Waterworth JA. Presence and the Self: A cognitive neuroscience approach. Presence Connect (2003) 3:2–3. doi: 10.1007/978-3-319-10190-3_3
22. Riva G, Waterworth JA, Waterworth EL. The layers of presence: a bio-cultural approach to understanding presence in natural and mediated environments. Cyber Psychol Behav (2004) 7:402–16. doi: 10.1089/cpb.2004.7.402
23. Waterworth JA, Waterworth EL, Riva G, Mantovani F. Presence: Form, content and consciousness. In: Lombard M, , Freeman BF, , IJsselsteijn J, Schaevitz W, editors. Immersed in Media: Telepresence Theory, Measurement & Technology. Berlin: Springer (2015). p. 35–58.
24. Riva G, Wiederhold BK, Mantovani F. Neuroscience of Virtual Reality: From Virtual Exposure to Embodied Medicine. Cyberpsychol Behav Soc Netw (2019) 22:82–96. doi: 10.1089/cyber.2017.29099.gri
25. Gaggioli A. Transformative Experience Design. In: Gaggioli A, Ferscha A, Riva G, Dunne S, Viaud-, Delmon I, editors. Human Computer Confluence Transforming Human Experience Through Symbiotic Technologies. Berlin: De Gruyter Open (2016). p. 96–121.
26. Riva E, Rainisio N, Boffi M. Positive change in clinical settings: flow experience in psychodynamic therapies. In: Inghilleri P, Riva G, Riva E, editors. Enabling positive change: flow and complexity in daily experience. Berlin: De Gruyter Open (2014). p. 74–90.
27. Riva G, Baños RM, Botella C, Mantovani F, Gaggioli A. Transforming Experience: The Potential of Augmented Reality and Virtual Reality for Enhancing Personal and Clinical Change. Front Psychiatry (2016) 7:164. doi: 10.3389/fpsyt.2016.00164.
28. Riva E, Freire T, Bassi M. The Flow Experience in Clinical Settings: Applications in Psychotherapy and Mental Health Rehabilitation. In: Harmat L, Ørsted Andersen F, Ullén F, Wright J, Sadlo G, editors. Flow Experience. Cham: Springer (2016). p. 309–26.
29. Chirico A. Awe. In: The Palgrave Encyclopedia of the Possible. Cham: Springer International Publishing (2020). p. 1–9.
30. Chirico A, Robert R C, David B,Y, Gaggioli A. Nature versus Art as Elicitors of the Sublime: A Virtual Reality study. PloS One (2020).
31. Van Tonder GJ, Lyons MJ, Ejima Y. Visual structure of a Japanese Zen garden. Nature (2002) 419:359–60. doi: 10.1038/419359a
32. Gilbert P. Developing a compassion-focused approach in cognitive behavioural therapy. In: Cognitive behaviour therapy: A guide for the practising clinician, Vol 2. New York, NY, US: Routledge/Taylor & Francis Group (2009). p. 205–20.
33. Gilbert P. An introduction to compassion focused therapy in cognitive behavior therapy. Int J Cogn Ther (2010) 3:97–112. doi: 10.1521/ijct.2010.3.2.97
34. Robertson CE, Hermann KL, Mynick A, Kravitz Dwight J, Kanwisher N. Neural Representations Integrate the Current Field of View with the Remembered 360° Panorama in Scene-Selective Cortex. Curr Biol (2016) 26:2463–8. doi: 10.1016/j.cub.2016.07.002
35. Winch G. Emotional First Aid: Practical Strategies for Treating Failure, Rejection, Guilt, and Other Everyday Psychological Injuries. Hudson Street Press: New York (2013).
36. Oude Rengerink K, Kalkman S, Collier S, Ciaglia A, Worsley SD, Lightbourne A, et al. Series: Pragmatic trials and real world evidence: Paper 3. Patient selection challenges and consequences. J Clin Epidemiol (2017) 89:173–80. doi: 10.1016/j.jclinepi.2016.12.021
37. Efird J. Blocked randomization with randomly selected block sizes. Int J Environ Res Public Health (2011) 8:15–20. doi: 10.3390/ijerph8010015
38. MacPherson H. Pragmatic clinical trials. Complement Ther Med (2004) 12:136–40. doi: 10.1016/j.ctim.2004.07.043
39. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav (1983) 1983:385–96. doi: 10.2307/2136404
40. Henry JD, Crawford J. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br J Clin Psychol (2005) 44:227–39. doi: 10.1348/014466505X29657
41. Beck AT, Steer RA, Pompili M. BHS, Beck hopelessness scale: manual. Psychological corporation: San Antonio, TX (1988).
42. Lee RM, Robbins S. Measuring belongingness: The social connectedness and the social assurance scales. J Couns Psychol (1995) 42:232. doi: 10.1037/0022-0167.42.2.232
43. Mertens G, Gerritsen L, Salemink E, Engelhard I. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. (2020).
44. Pancani L, Marinucci M, Aureli N, Riva P. Forced social isolation and mental health: A study on 1006 Italians under COVID-19 lockdown. PsyArXiv (2020). doi: 10.31234/osf.io/uacf
46. McCabe RE. Subjective Units of Distress Scale. J Phobias: Psychol Irrational Fear (2015) 18:361.
47. Rozental A, Kottorp A, Forsström D, Månsson K, Boettcher J, Andersson G, et al. The Negative Effects Questionnaire: psychometric properties of an instrument for assessing negative effects in psychological treatments. Behav Cogn Psychother (2019) 47:559–72. doi: 10.1017/S1352465819000018
48. Sevinc V, Berkman MI. Psychometric evaluation of Simulator Sickness Questionnaire and its variants as a measure of cybersickness in consumer virtual environments. Appl Ergonom (2020) 82:102958. doi: 10.1016/j.apergo.2019.102958
49. Wind TR, Rijkeboer M, Andersson G, Riper H. The COVID-19 pandemic: The ‘black swan’ for mental health care and a turning point for e-health. Internet Interventions (2020) 20:100317–7. doi: 10.1016/j.invent.2020.100317
50. Mohr DC, Riper H, Schueller SM. A Solution-Focused Research Approach to Achieve an Implementable Revolution in Digital Mental Health. JAMA Psychiatry (2018) 75:113–4. doi: 10.1001/jamapsychiatry.2017.3838
51. Gaggioli A, Chirico A, Triberti S, Riva G. Transformative Interactions: Designing Positive Technologies to Foster Self-Transcendence and Meaning. Annu Rev Cyberther Telemed (2016) 14:169–73.
Keywords: COVID, virtual reality, self-help, stress, emotion regulation, mental health
Citation: Riva G, Bernardelli L, Browning MHEM, Castelnuovo G, Cavedoni S, Chirico A, Cipresso P, de Paula DMB, Di Lernia D, Fernández-Álvarez J, Figueras-Puigderrajols N, Fuji K, Gaggioli A, Gutiérrez-Maldonado J, Hong U, Mancuso V, Mazzeo M, Molinari E, Moretti LF, Ortiz de Gortari AB, Pagnini F, Pedroli E, Repetto C, Sforza F, Stramba-Badiale C, Tuena C, Malighetti C, Villani D and Wiederhold BK (2020) COVID Feel Good—An Easy Self-Help Virtual Reality Protocol to Overcome the Psychological Burden of Coronavirus. Front. Psychiatry 11:563319. doi: 10.3389/fpsyt.2020.563319
Received: 20 May 2020; Accepted: 31 August 2020;
Published: 23 September 2020.
Edited by:
Ursula Werneke, Umeå University, SwedenReviewed by:
Sara Ventura, University of Valencia, SpainAlexander Miloff, Stockholm University, Sweden
Copyright © 2020 Riva, Bernardelli, Browning, Castelnuovo, Cavedoni, Chirico, Cipresso, de Paula, Di Lernia, Fernández-Álvarez, Figueras-Puigderrajols, Fuji, Gaggioli, Gutiérrez-Maldonado, Hong, Mancuso, Mazzeo, Molinari, Moretti, Ortiz de Gortari, Pagnini, Pedroli, Repetto, Sforza, Stramba-Badiale, Tuena, Malighetti, Villani and Wiederhold. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniele Di Lernia, ZGFuaWVsZS5kaWxlcm5pYUB1bmljYXR0Lml0