 Emma M. Seppälä1,2*†Christina Bradley1†Julia Moeller3Leilah Harouni1,4Dhruv Nandamudi5Marc A. Brackett1
Emma M. Seppälä1,2*†Christina Bradley1†Julia Moeller3Leilah Harouni1,4Dhruv Nandamudi5Marc A. Brackett1- 1Yale Child Study Center & Yale Center for Emotional Intelligence, Yale University, New Haven, CT, United States
- 2Center for Compassion and Altruism Research and Education, Stanford University, Stanford, CA, United States
- 3Department of Education, Leipzig University, Leipzig, Germany
- 4Yale School of Management, Yale University, New Haven, CT, United States
- 5Medical Research Council Cognition and Brain Sciences Unit, University of Cambridge, Cambridge, United Kingdom
This study aimed to address the decline in mental health on U.S. university campuses by examining the effects of three interventions. University students suffer from high levels of anxiety, depression, and suicide. Counseling centers on university campuses are struggling to meet increased demand. The cost to students and universities could be buffered by offering preventative, psychoeducational, and skill-building training programs that promote mental health and psychological thriving. To date, the research literature has not yielded systematically evaluated and recommendable preventative mental health and well-being programs for university students. In a registered, randomized controlled trial, 131 university students were either placed in a non-intervention control group (N = 47) or received training in one of three 30-hour, eight-week semester-long well-being programs: SKY Campus Happiness (“SKY”; N = 29), Foundations of Emotional Intelligence (“EI”; N = 21) or Mindfulness-Based Stress Reduction (“MBSR”; N = 34). Compared to the control group and controlling for variance of baseline measurements and multiple comparisons, SKY Campus Happiness showed the greatest impact, benefiting six outcomes: depression, stress, mental health, mindfulness, positive affect and social connectedness. EI benefited one outcome: mindfulness. The MBSR group showed no change. Delivering SKY or EI to university students may be a cost-effective and efficient way to proactively and preventatively address mental health for university students and reduce the financial strain on universities.
Introduction
The World Health Organization defines health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” (1). Similarly, we can think of mental health as not merely the absence of mental illness (e.g., anxiety and depression), but also the presence of psychological thriving (e.g., gratitude, social connectedness, mindfulness).
Mental health in college and university students in the United States has declined over the last decade (2). College-aged adults (18–25 years of age) are at greatest risk for mental illness (3) and have the highest prevalence of any type of mental illness [25.8%; (4)]. The most common self-reported concerns by university students visiting counseling centers in the United States between 2017 and 2018 were anxiety (58.9%), depression (48.0%) and stress (46.9%) (5, 6). A 2018 American College Health Association survey of 88,178 college students across 140 campuses reported that 60% of students self-reported experiencing overwhelming anxiety and 40% self-reported feeling so depressed they had difficulty functioning (7).
Mental illness interferes with student learning and is significantly associated with lower GPA (7, 8). Mental illness is also associated with substance abuse in university students in the United States (9), which further negatively impacts academic performance (10) and exacerbates mental illness.
Mental illness and substance abuse are associated with more than 90% of all cases of suicide in the United States (11, 12). While suicide is the tenth leading cause of death in the United States (13), it is the second leading cause of death for college-aged students, after traffic accidents (14). Recent years have seen a record increase in suicides by young adults aged 15–24 years old (13). The highest number of suicides ever reported for this age group was in 2017 (2, 13, 15). From 2000 to 2016, over 10% of students reported having seriously considered suicide in the past year (2, 5–7, 11, 13, 16).
Whereas social connection, a measure of psychological thriving, is predictive of emotional health, mental illness is often associated with loneliness and isolation which in turn can further deteriorate mental health and increase suicidal ideation (17–24).
Campus counseling centers are inadequately prepared to meet increased demand for services. From 2009 to 2014, campus counseling centers experienced an average increase of 30% of students seeking treatment for an average 6% institutional enrollment increase (25). Ninety-four percent of counseling center directors report an increasing number of students with severe diagnosed mental health problems presenting on their campuses (26), and 57% of directors indicate that their resources are insufficient to meet students’ needs (5).
The traditional approach to addressing mental illness is to address symptoms after they have presented themselves. Students are typically diagnosed and then prescribed medication, counseling or a combination thereof (27, 28). A steady increase in demand for counseling, however, makes this recourse financially unsustainable (29). Moreover, medications often present with aversive side effects (4) that can disrupt cognitive functions [e.g., attention and memory, essential for succeeding in college (30)]. Finally, these types of interventions are not only applied post-hoc but also focus exclusively on treating mental illness symptoms without setting up the conditions for psychological resilience and thriving.
A preventative and proactive approach to mental health that provides students with empirically validated tools for psychological resilience and thriving prior to developing symptoms may be a viable additional support to the efforts made by campus counseling centers. Several studies indicate that skill-building interventions are effective in improving the lives of adolescents and college students (31–33). A recent meta-analysis of universal mental health prevention programs on university campuses showed that the most successful programs included skill-building with supervised practice (34). These programs, as compared with skill-building programs without supervised practice or those with only psychoeducational curricula, were significantly more successful in reducing anxiety, stress, depression, and distress and improving social and emotional skills (34).
However, most mental health prevention programs offered by campuses tend to fail due to a primary focus on psychoeducation (34). Without the components of skill-building (including practice time, reflection, questions and discussion) and supervised practice, integration of the material is challenging (34). Overall, the research literature has not yielded systematically evaluated and recommendable skill-building protocols for psychological resilience that university administrators can implement (35). Our study aimed to address this gap in the literature: we examined the impacts of three different skill-building prevention interventions with supervised practice that past research suggests could improve student mental health.
We selected SKY Campus Happiness (SKY) because it has been shown to increase psychological resilience (36, 37), decrease stress (38) and reduce impulsive behavior (39) in students. In general populations, SKY has also been shown to improve emotion regulation (40), decrease stress (41–43), anxiety and depression (44–50), and reduce PTSD (51, 52).
The second program we selected was Foundations in Emotional Intelligence (EI), a program that was adapted from both a university course and a pre-existing evidence-based approach to social and emotional learning, RULER (53). RULER has shown promising results for school-aged children in quasi-experimental and randomized controlled studies. In particular, RULER, has been shown to increase social and emotional competence (54), improve academic grades (54), emotion skills (54), cooperation (55), social problem-solving skills (56), and student-teacher relationships (57).
The third program we selected was Koru Mindfulness. Mindfulness-based interventions have been shown to reduce psychological distress (58, 59), stress (60), and anxiety (61) in university students. In general populations it has also been shown to reduce depression (62), anxiety (62), and stress symptoms (63), and to increase self-compassion (64), self-esteem (65), sleep quality (65), and physical health (66).
Since mental health may be considered on a spectrum from mental illness to psychological thriving, we aimed to measure the impact of the interventions with measures spanning that spectrum (from anxiety and depression to gratitude and social connectedness). We hypothesized that the manner in which each workshop would impact mental health would differ depending on the focus of the intervention curricula. Based on past research, we hypothesized that all three groups would benefit measures of mental health such as anxiety, stress and depression. We also hypothesized that the interventions would improve measures of psychological thriving. Given past research, we further hypothesized that SKY would also improve psychological resilience measures. We hypothesized that EI, given its emphasis on emotion regulation, would also improve positive affect. With its focus on mindfulness and self-compassion, we hypothesized that Koru Mindfulness would also benefit mindfulness and self-compassion.
An initial pilot study compared three well-being/skill-building interventions—SKY Campus Happiness (SKY), Foundations of Emotional Intelligence (EI), and Koru Mindfulness—to an inactive control group. The majority of the 203 pilot undergraduate participants recommended the well-being interventions. However, largely no effects were observed in self-reported well-being. The lack of intervention effects despite high likability was potentially due to low exposure and practice of the techniques and strategies taught during intervention delivery (10 h over 5 weeks) and lack of at-home practice (mode days of reported at-home practice was zero).
Building on the pilot, our pre-registered main study (Clinicaltrials.gov, Registration number: NCT03229577) had the same randomized controlled design with more intervention exposure (30 h over 8 weeks) in addition to at-home practice requirements. SKY and EI expanded the curriculum to include 8 weeks of content. We used the Mindfulness-Based Stress Reduction program instead of Koru Mindfulness since its curriculum is designed for an 8-week period. The same self-reported well-being measures were used here as in the pilot.
Materials and Methods
Recruitment
Undergraduate students from a large, four-year private university learned about the study through departmental email lists. Applicants who had participated in programs similar to the study interventions or had significant mindfulness expertise were excluded. One hundred ninety-three students committed to joining the semester-long study.
A total of 1,305 students declared an initial interest in the study. See Figure 1 for the process by which the final participant sample was formed. Participants were excluded from this study if they had previously partaken in any of the study’s interventions or similar programs. Students considered “experts” in mindfulness (who practiced any type of mindful practice five or more times a week) were also excluded. Likewise, students who participated in the previous year’s pilot study were excluded from participation. Based on these criteria, 515 students were excluded from the study.
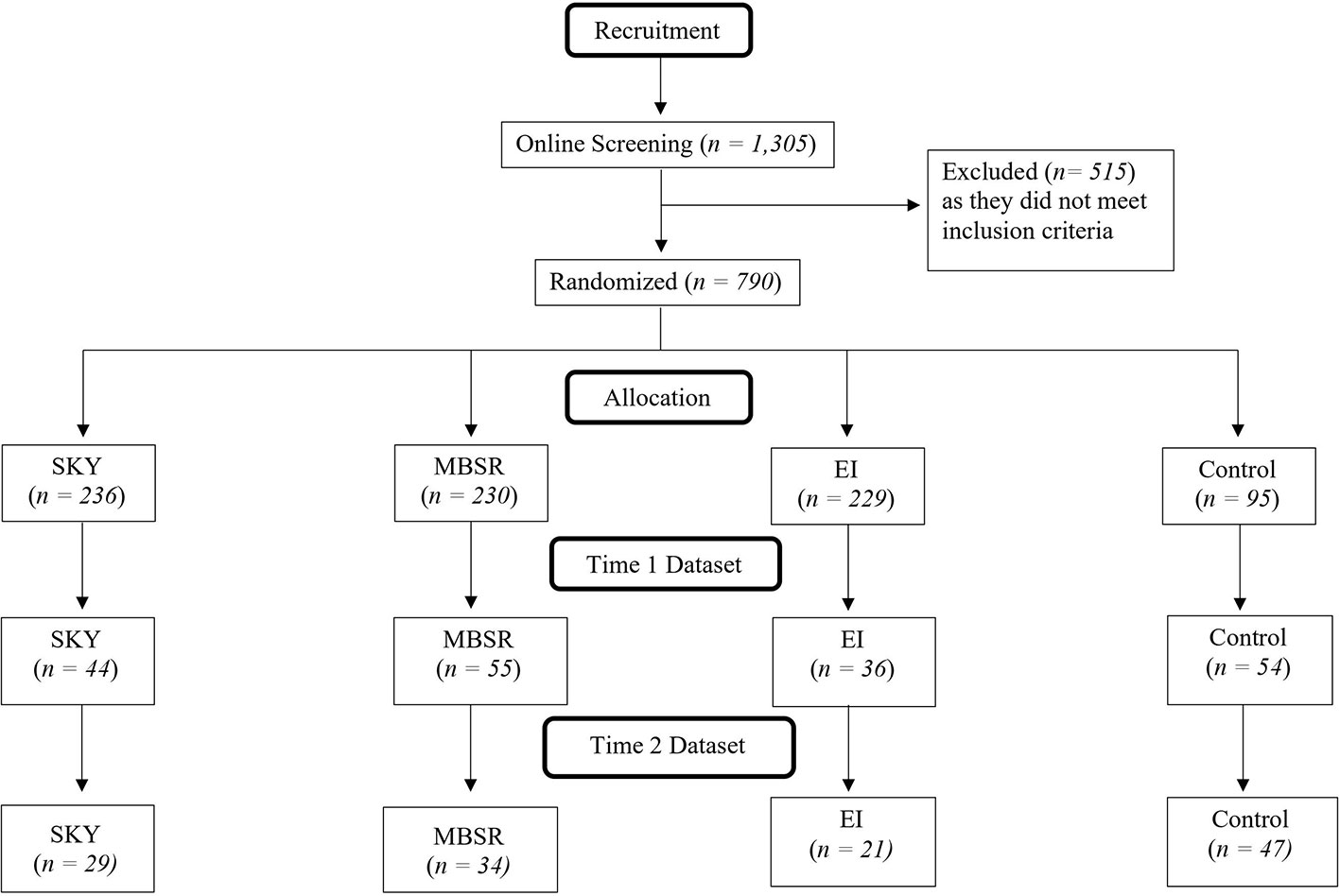
Figure 1 Diagram summarizing participant flow for recruitment, allocation, and analysis.
The remaining sample of 790 prospective students were randomly distributed into the study’s four groups: SKY, MBSR, EI, and control. After randomization, each student interested in participating in the study was provided with the schedule and requirements. Prospective participants at this time were invited to enroll, committing to pre- and post-testing, attendance and dedication requirements. Of the 790 prospective participants, 193 students accepted the invitation to join the study.
During the course of the study, fifty-eight students dropped out due to schedule conflicts (N = 11), inability to meet the time commitment (N = 9), dismissal for excessive absences (N = 4), discontinued correspondence with the researchers (N =11), physical health reasons (N = 1), mental health reasons (N = 1) or unknown reasons (N = 21). One hundred and thirty-five students completed the study. Another three participants were removed for having extreme outlier data on ten or more outcome variables. A fourth participant was removed for reporting lying on all of their practice logs.
The final sample included 131 participants with an average age of 19.67 years (SD = 1.02). 56.5% of participants were White, 30.5% Asian, 16.0% Hispanic or Latino, 13.0% Black or African American, 6.1% two or more races, 3.8% American Indian or Alaskan Native, 1.5% other, and 0.8% declined to provide information. Thirty-five and one-half percent of participants were male, 59.5% female, 3.1% genderqueer/gender non-conforming, and 0.8% reported “different identity”.
There were no significant differences between groups in gender, mental health diagnoses, current psychological treatment, or personality [measured by the Big Five Inventory, (67)].
Descriptive statistics for all measures at T1 and T2 can be found in Table A (overall descriptives) and Table B (group-specific descriptives) in Supplementary Materials.
Procedure
Exactly one week prior to the interventions, all participants completed Time 1 (T1) questionnaires in person after providing written informed consent for the protocol approved by the Yale University Institutional Review Board. Exactly three days after the last intervention session, all participants completed the Time 2 (T2) questionnaires in person. Students practiced techniques learned in class at least three times per week and filled out practice logs. Active group participants were compensated $300. Control group participants were compensated $80.
Interventions
The three interventions (SKY, EI and MBSR) offered equal dosage of instruction: classes were taught twice per week for a total of 30 h over eight weeks during the course of a university semester (with a two-week break in the middle for spring break). The 30 h of intervention included one or more short retreats in addition to class time. Attendance was mandatory (2 absences were allowed). Interventions were delivered by certified facilitators with seven or more years of teaching experience. Facilitators were blind to research hypotheses, data collection, and analyses.
SKY Campus Happiness (SKY)
SKY is a university leadership and well-being program (campushappiness.org) that includes stress-management and tools for psychological resilience: yoga postures, breathing exercises, a breath-based meditation technique [Sudarshan Kriya Yoga; (68)]. SKY also includes positive psychology skills (e.g., gratitude, social connection, acts of kindness, meaning and purpose). In addition, the curriculum includes discussion and application of leadership skills and service learning.
Foundations of Emotional Intelligence (EI)
EI is an emotional intelligence program focused on teaching knowledge of emotions and emotion regulation (54). EI was adapted from a university course on emotional intelligence and an evidence-based approach to social and emotional learning for school-aged children, RULER (www.rulerapproach.org). RULER is an acronym that stands for the five skills of emotional intelligence: recognizing, understanding, labeling, expressing and regulating emotions.
Mindfulness-Based Stress Reduction (MBSR)
MBSR is a mindfulness meditation program [https://www.umassmed.edu/cfm/mindfulness-based-programs/, (69)] designed for “progressive acquisition of mindful awareness, of mindfulness” (66). It involves instruction in three formal techniques: mindfulness meditation, body scanning (systematic awareness of different parts of the body from toes to the head) and simple yoga postures. In addition, the class includes discussions about meditation and its practical application to daily life.
Measures
Outcome variables were divided along three categories: mental health, psychological thriving and health outcomes (physical health and sleep). We used a wide range of self-reported outcome measures to ensure reliable capture of change. Self-report measures assessed the effects of the programs at T1 and T2 along these categories. Participants completed two additional measures not included here: an emotion perception task and the Human Well-Being Scale. Both are in the development phase and unvalidated. In addition, participants completed a measure of creativity not related to well-being, not included here.
Mental Health
Burnout
The Single-Item Measure of Burnout (70, 71) contains the item: “Overall, based on your definition of burnout, how would you rate your level of burnout?”. Participants choose one answer ranging from 1 = I enjoy my work. I have no symptoms of burnout to 5 = I feel completely burned out and often wonder if I can go on. I am at the point where I may need some changes or may need to seek some sort of help.
Stress
The Perceived Stress Scale 10-Item Inventory [PSS-10; (72); Cronbach’s Alpha=0.85] asks how frequently participants felt stress or had difficulties coping with life stresses on a scale ranging from 1 = never to 4 = very often. Example items include, “In the last month, how often have you felt that you were unable to control the important things in your life?” and “In the last month, how often have you felt that things were going your way?”.
Distress, Anxiety and Depression.
The Mood and Anxiety Symptom Questionnaire [MASQ-D30; (73)] consists of three subscales that measure: general distress symptoms (Cronbach’s Alpha=0.87), anhedonic depressive symptoms (Cronbach’s Alpha=0.80), and anxious arousal symptoms (Cronbach’s Alpha=0.90). Items were rated on a scale of 1 = very slightly or not at all to 5 = extremely. Examples of items include, “In the last two weeks I felt irritable” or “felt optimistic.”
Mental Health
Participants answered the question: “In general, would you say your health is…?” Items were rated on a scale 1 = poor to 5 = excellent. This self-assessment item was modeled from the Center for Disease Control’s (CDC) National Health Survey (12), and The RAND Corporation’s 36-Item Short Form Health Survey [SF-36; (74)].
Psychological Thriving
Psychological Well-Being
The Ryff Scale of Psychological Well-being is an 18-item scale [RYFF; (75)]. Items are phrased as statements about the self, to which participants rate their agreement on a scale of 1 = strongly disagree to 7 = strongly agree. Examples of items include, “I like most parts of my personality” and “The demands of everyday life often get me down.” This scale includes six subscales, each measured using three items.: Autonomy (Cronbach’s Alpha=0.70), Environmental Mastery (Cronbach’s Alpha=0.61), Personal Growth (Cronbach’s Alpha=0.48), Positive Relations (Cronbach’s Alpha=0.67), Purpose in Life (Cronbach’s Alpha=0.35), Self-acceptance (Cronbach’s Alpha=0.72).
Life Satisfaction
The Satisfaction with Life Scale [SWLS; (76); Cronbach’s Alpha=0.82] is a five-item scale. Items are rated on a scale from 1 = strongly disagree to 7 = strongly agree. Examples of items include, “The conditions of my life are excellent” and “If I could live my life over, I would change almost nothing.”
Positive Affect
The Positive and Negative Affect Schedule [PANAS; (77); Cronbach’s Alpha=0.89] is a 20-item scale containing two subscales each containing ten items: pleasant emotions and unpleasant emotions. Participants rate the extent to which they feel specific emotions over the past week on a scale from 1 = very slightly or not at all to 5 = extremely. Examples of emotions include “Excited”, “Nervous”, “Ashamed”, and “Determined”.
Negative Affect
The Positive and Negative Affect Schedule, see Positive Affect, above (Cronbach’s Alpha=0.87).
Gratitude
The Gratitude Questionnaire-Six Item Form [GQ-6; (78); Cronbach’s Alpha=0.86] is a 6-item measure. Items are rated on a scale from 1 = strongly disagree to 7 = strongly agree. Examples of items include, “I have so much in my life to be thankful for” and “Long amounts of time can go by before I feel grateful to something or someone.”
Self-Compassion
The Self-Compassion-Short Form [SCS-SF; (79); Cronbach’s Alpha=0.89] is a 12-item scale measuring the three components of self-compassion: self-kindness, common humanity, and mindfulness. Participants rate how often they act in the presented manner using a five-point scale from 1 = almost never to 5 = almost always. Examples of items include “I try to be understanding and patient toward aspects of my personality I don’t like” and “I’m disapproving and judgmental about my own flaws and inadequacies.”
Mindfulness
Five Facet Mindfulness Questionnaire [FFMQ-15; (80); Cronbach’s Alpha=0.81] is a fifteen-item scale that participants rate on a scale from 1 = never or very rarely true to 5 = very often or always true depending on how their level of agreement with the statements. Examples of items include, “I’m good at finding words to describe my feelings” and “I do jobs or tasks automatically without being aware of what I’m doing.”
Adaptive Coping
The Brief COPE scale has 28 items that assess tendencies for using adaptive and maladaptive coping strategies [(81); Cronbach’s Alpha=0.81] Items are rated on a scale from 1 = I haven’t been doing this at all to 4 = I’ve been doing this a lot. Examples of items include, “I’ve been giving up trying to deal with it” and “I’ve been trying to come up with a strategy about what I should do.”
Maladaptive Coping
See Adaptive Coping, above (Cronbach’s Alpha=0.75).
Optimism
The Life Orientation Test- Revised [LOT-R; (82); Cronbach’s Alpha=0.852] measures optimism. This test includes 10 items rated on a 5-point scale from 1 = I disagree a lot to 5 = I agree a lot. Examples of items include, “ If something can go wrong for me, it will” and “In uncertain times, I usually expect the best.”
Self-Esteem
The Single Item Self-Esteem Scale [SISE; (83)] is a single item measure of the construct of self-esteem that has been validated against the well-known Rosenberg Self-Esteem Scale. Scores range from 1 - 5 with low self-esteem indicated by a score of 1.
Social Connectedness
The Social Connectedness Scale Revised [SCS-R; (84); Cronbach’s Alpha=0.94] was used to measure social connectedness. Items were rated on a scale ranging from 1 = strongly disagree to 6 = strongly agree. Sample items include, “I am able to connect with other people”, “I see myself as a loner”, and “I feel like an outsider.”
Physical Health and Sleep
Participants answered two questions: “In general, would you say your health is…?” Items were rated on a scale 1 = poor to 5 = excellent. And “Over the last 2 weeks, how many days have you had trouble falling asleep, staying asleep, or sleeping too much?” Items were rated on a scale from 1 (day) to 14 (days). These assessments were also modeled on the CDC and RAND questionnaires mentioned under “Mental Health.”
Acceptability Assessments
At T2 (post-test), students answered 2 questions to which they could answer “yes,” “no,” or “maybe”: 1) Would you recommend that your university provide students with this workshop?, 2) Would you recommend this workshop to a friend?
Analyses
The correlations between variables can be found in Table 1. Cronbach’s alphas for each of the measures at each of time points can be found in Table A in Supplementary Materials. Treatment effects were tested with autoregressive models. Dummy variables were used to compare each of the three treatment groups to the control group, which was used as the reference group in the dummy variables (see Figure 2). The outcomes at T1 (pre-test) and T2 (post-test) were regressed on the dummy variables representing the effects of the three treatment groups, compared to the control group. The outcome at T2 was regressed on the outcome at T1 to control for T1 levels. All regressions were conducted in Mplus [Version 8.1; (85)], using a robust estimator (Maximum Likelihood Robust, MLR) due to non-normal distributions and outliers and Full Information Maximum Likelihood (FIML) estimation for missing data. This regression-based approach was selected over repeated measures MANOVAs to address the non-normality of the outcome variables, particularly outliers, and the problem of missing data from dropouts.
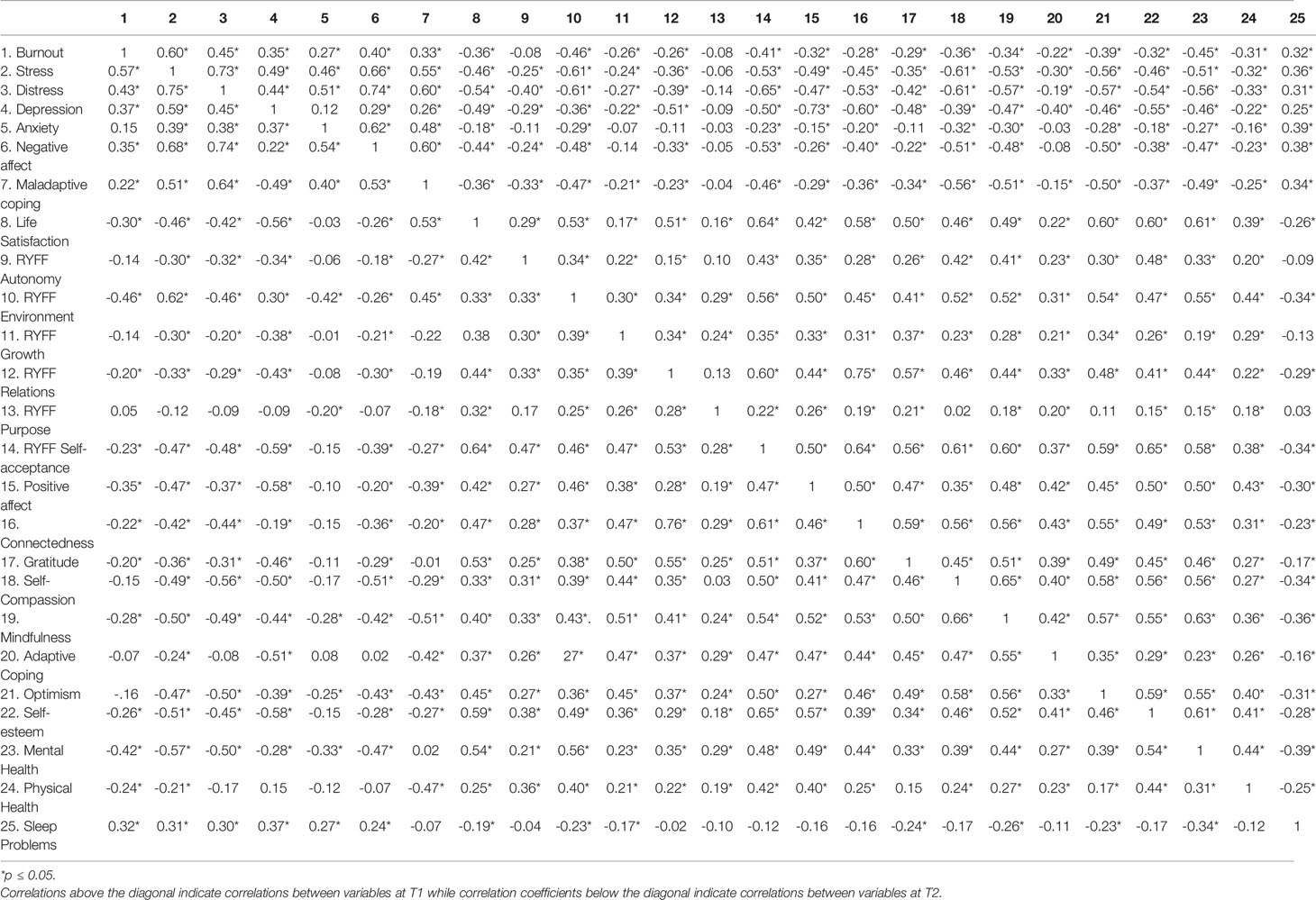
Table 1 Inter-correlations of outcome measures.
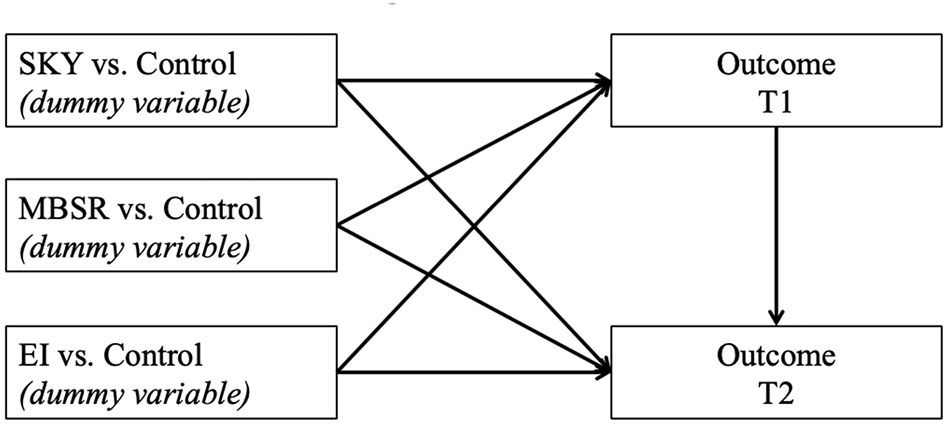
Figure 2 Regressions predicting outcomes at T2.
Since we had directed hypotheses for the comparisons of each intervention group to the control group, we report one-tailed p-values. Due to the multiple comparisons, the p-values were Bonferroni-corrected for 72 hypotheses; 24 outcomes multiplied with 3 intervention dummy variables. The adjusted p-value needed to be <= 0.000641026 (or 0.001, since Mplus only reports three decimal points).
Results
Treatment Effects at T2
To estimate treatment effects, we conducted autoregressive regression models. In these models, treatment groups were represented by dummy variables, comparing each treatment group to the reference control group. The outcomes at T1 and T2 were regressed on the three treatment group dummy variables, and the outcome at T1 was regressed on the T1-level of itself, to control for baseline levels. Due to the relatively small sample size, we conducted a separate regression for each outcome. Figure 1 shows examples of the regression models conducted (for treatment effects at T2). The detailed results for all regressions that examined treatment effects, including p-values, are reported in Tables 2–4. All effects below are in comparison to the control group and controlling for T1:
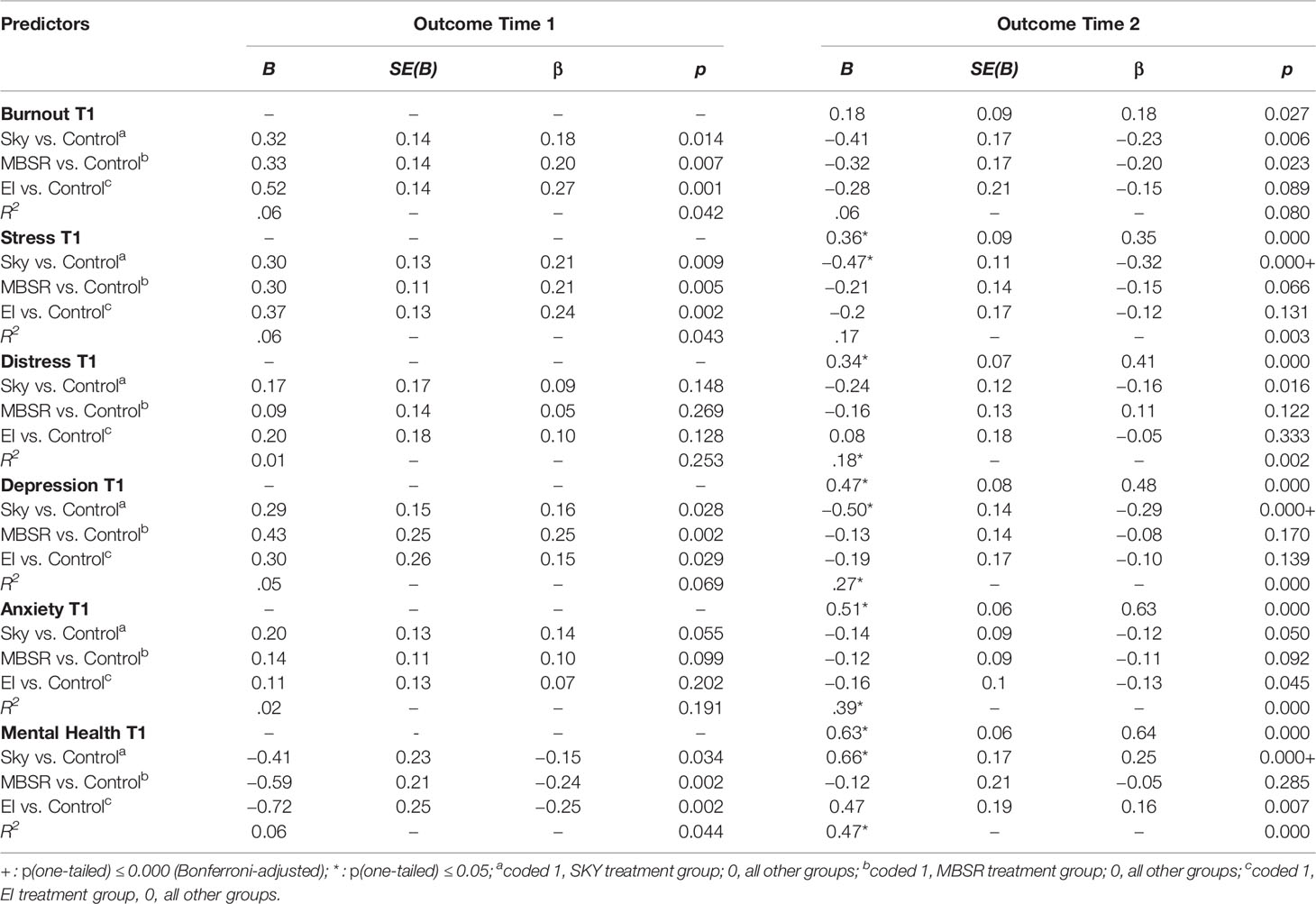
Table 2 From T1 to T2: Regressions for mental health outcomes regressed on groups.
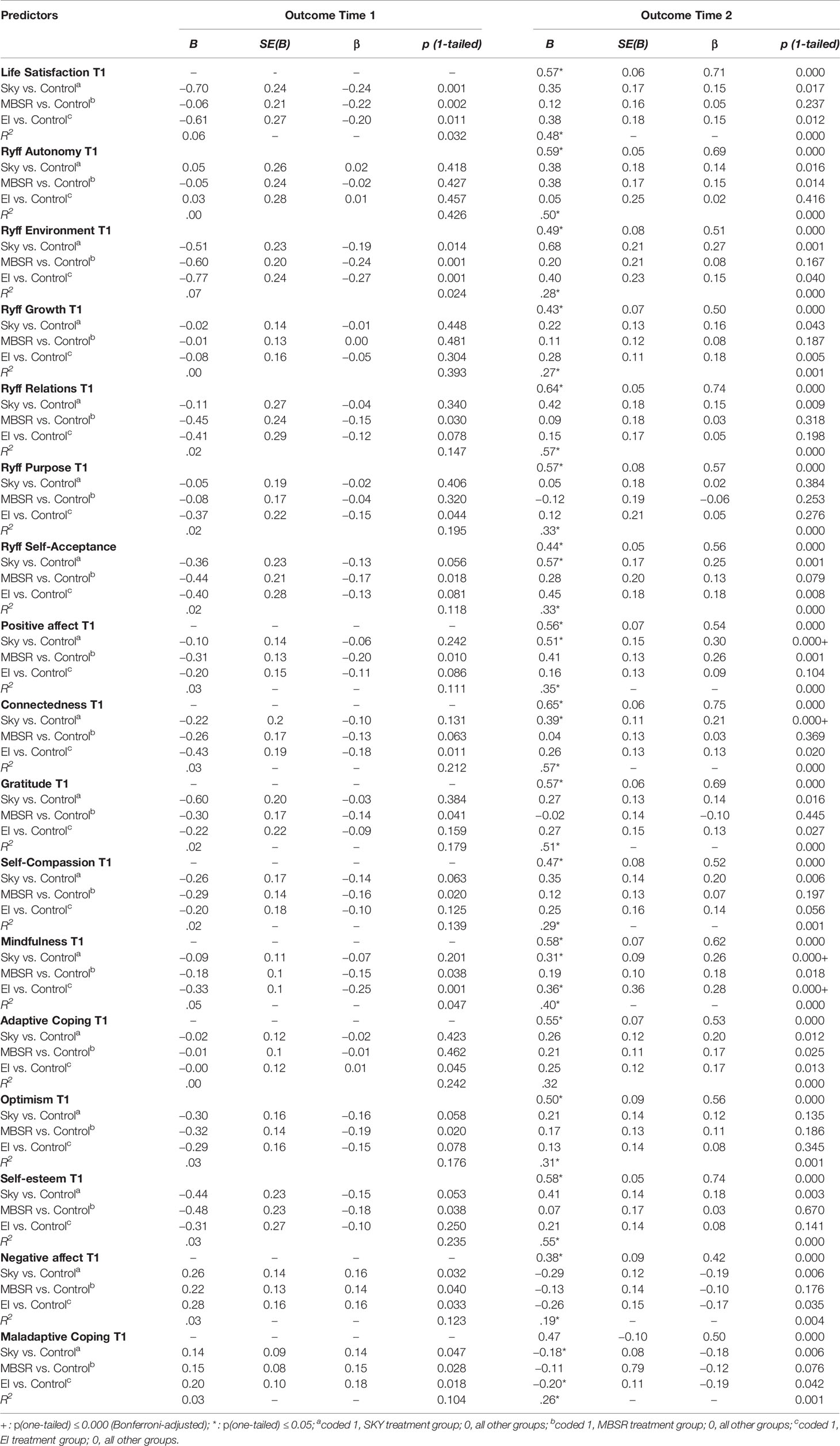
Table 3 From T1 to T2: Regressions for well-being outcomes regressed on groups.
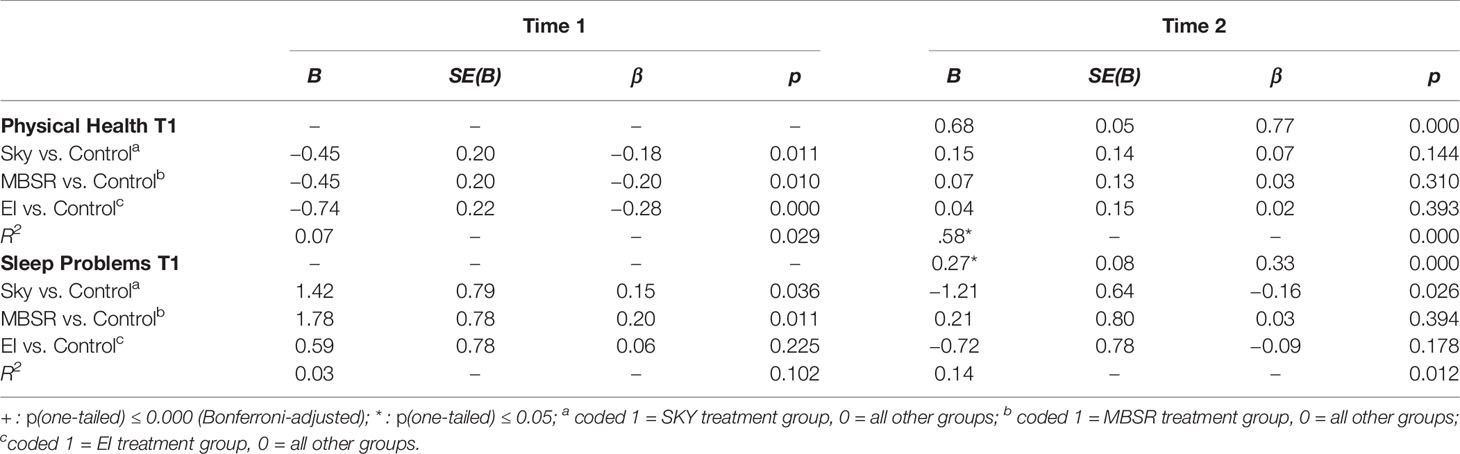
Table 4 From T1 to T2: Regressions for health well-being outcomes regressed on groups.
Effects of SKY
The SKY group scored significantly higher than the control group on three mental health outcomes at T2, while controlling for the T1 levels in these three outcomes: depression (MASQ; β = −0.29), mental health (β = 0.25), and stress (PSS-10; β = −0.32). Moreover, the SKY group scored significantly higher than the control group on three outcomes of psychological thriving: mindfulness (FFMQ-15; β = 0.26), positive affect (PANAS; β = 0.30), and social connectedness (SCS-R; β = 0.21).
Effects of EI
The EI group scored significantly higher than the control group on one aspect of psychological thriving: mindfulness (FFMQ-15; β = 0.28).
Effects of MBSR
The MBSR group did not differ in any outcome from the control group at T2. (However, see below for findings warranting replications with larger samples).
Uncorrected Treatment Effects at T2
The strict Bonferroni correction, used to correct for the multiple comparisons, led us to decrease the acceptable p-value from the conventional 0.050 to 0.000. However, given our small sample size, the likelihood of detecting effects with such a strict threshold for significance is small. There were several findings of effects that were significant at the p ≤ 0.05 level that became insignificant after the alpha adjustment. We suggest that these effects be examined in future studies with larger samples as these effects do warrant further investigation. These were the differences between intervention groups and the control group at T2 that were significant at the p ≤ 0.05-level but not at the adjusted p ≤ 0.000-level were:
Effects of SKY
Twelve outcomes warranting replication with larger samples: environment-related well-being (Ryff; β = 0.27); self-acceptance (Ryff; β =0.25); burnout (β = −0.23), self-compassion (SCS-SF; β = 0.20), adaptive coping (COPE; β = 0.20), negative affect (PANAS; β = −0.19), self-esteem (β = 0.18), maladaptive coping (COPE; β = −0.18), distress (MASQ; β = −0.16), sleep problems (β = −0.16), life satisfaction (SWLS; β = 0.15), relationship-related well-being (Ryff; β = 0.15); autonomy (Ryff; β = 0.14), gratitude (GQ-6; β = 0.14), anxiety (MASQ; β = −0.12).
Effects of EI
Nine outcomes warranting replication with larger samples: maladaptive coping (COPE; β = −0.19), self-acceptance (RYFF; β =0.18), growth-related well-being (RYFF; β =0.18), adaptive coping (COPE; β = 0.17), negative affect (PANAS; β = −0.17), mental health (β = 0.16), life satisfaction (SWLS; β = 0.15), social connectedness (SCS-R; β = 0.13), anxiety (MASQ; β = −0.13), and gratitude (GQ-6; β = 0.13).
Effects of MBSR
Five outcomes warranting replication with larger samples: positive affect (PANAS; β = 0.26), burnout (β = −0.20), autonomy (Ryff; β =0.15), mindfulness (FFMQ-15; β = 0.18), and adaptive coping (COPE; β = 0.17).
We also compared the intervention groups with each other on all the outcomes for which multiple interventions showed significant differences (p ≤ 0.05) to the control group (see Tables F-N in Supplementary Materials). There was no significant difference between the intervention groups on any of these outcomes after multiple comparison correction using the strict Bonferroni correction.
Robustness Check
We used nonparametric Mann-Whitney-U-tests for pairwise comparisons between each treatment group and the control group in the change score T2 minus T1 on the outcome variables. The Mann-Whitney-U test indicated largely the same results as the aforementioned regressions. Please see the Tables in the Supplementary Materials detailing results of the Mann-Whitney-U tests for the comparisons of the change scores from T1 to T2 (Table C). Since the regression analyses did not directly assess change from T1 to T2, we additionally examined whether the change was significant by comparing T1 and T2 for each outcome variable with paired-samples t-test (Table D, Supplementary Materials). Attrition analyses can also be found in the Supplementary Material (Table E).
Acceptance of the Intervention
Similarly to the pilot study, the majority of students in all three groups said they would recommend the interventions to their university and friends, suggesting good acceptance of the programs among the students. See Figure 1, Supplementary Materials.
Discussion
In sum, compared to the control group and controlling for baseline levels in the outcomes and for multiple comparisons, the SKY group benefited six outcomes (depression, stress, mental health, positive affect, mindfulness, and social connectedness), the EI group benefited one outcome (mindfulness), and the MBSR benefited none.
SKY’s wide range of results may be explained by its multi-component and comprehensive curriculum including a number of different factors that prior research suggests can improve mental health and psychological thriving: positive psychology (86), yoga/breathing/meditation (87–89), and community service (90). Modulation of respiration, in particular, has been linked to improvements in neuro-cognitive function (91, 92). Since cognitive deficits are often observed in mental health conditions (93), breathing exercises may impact mental health and psychological thriving via improved cognitive function, such as enhanced attention (94). Breathing techniques have also been found to enhance autonomic, cerebral and psychological flexibility related to emotional control and psychological well-being in healthy participants (95).
The EI program impacted mindfulness, perhaps because of the program’s focus on self-awareness and emotional awareness in particular (54).
MBSR’s lack of significant findings were surprising given a substantial body of research suggesting its potential benefits for a wide range of populations [e.g., (62, 80)]. Meta-analyses on MBSR, however, are mixed and suggest a range of effect sizes from small to large depending on the measured construct [e.g., (96)]. MBSR’s comparatively modest impact in the current study’s population may be explained by the fact that MBSR is designed for a general community audience whereas SKY and EI programs are specifically tailored for university students. Further studies are required to determine the impact of potential adaptations of the MBSR curriculum for university students.
While the MBSR intervention showed no significant difference from the control group at T2 in any outcome with the Bonferroni-adjusted p-value of 0.000, there were several outcomes for which the difference between the MBSR and the control group would have been significant at the conventional level of p ≤ .05. The same is true for the SKY group and the MBSR group. Because the current study is underpowered to detect effects at the stricter level of significance, this study warrants replication with larger sample sizes. Based on these indications, it is worth investigating whether all of the interventions might show additional benefits.
The American Council for Education emphasizes the cost-benefit analyses of offering mental health programming to reduce costs related to dropout and earnings (29). Counseling expenses for an average public 4-year college or university serving 15,000-20,000 students, with an average staff of 10 full-time staff, are around $1,560,000 (including salary, benefits, operational costs and professional development) (5). Programs like SKY, EI or MBSR can be taught in a large group format by trainers hired as lecturers. The cost of hiring lecturers per year is low [average salary during the academic year 2016–17 was $58,749; (97)]. Given that these programs offer empirically validated education that leads to observable improvements in well-being and mental health, and given the affordability of their delivery, universities could stand to benefit financially from including them in their curricula.
Limitations and Future Directions
Although effect sizes were consistent and in expected directions across many outcome variables, group sizes were small. Due to randomization and dropout, group sizes were also uneven. There was also low internal consistency of the dimensions that make up the Ryff Scale of Psychological Well-Being.
Replications with larger samples and group sizes are recommended. Moreover, future research should include clinical and biological measures in addition to self-report.
Whereas the 10-hour pilot study showed no effects, the 30-hour program with required at-home practice did. The previous null findings may indicate that the amount of training hours used in this study should not be reduced in future studies and in trainings implemented in colleges and universities. Further research could also examine the replicability of these findings for online delivery of these programs.
With the modest effects of psychoeducation-only programs for students (as discussed in the introduction), the integrative format of the workshops studied here, which include both skill-building and group dynamics, may be critical for the effectiveness of the programs (34). In addition, future research should investigate mechanisms responsible for the effects of SKY and EI and interactive effects of different curricula components.
It is unclear whether the results would differ if the program structure and incentivization process were altered. Future research may also consider the role of personality traits or a natural propensity toward well-being on outcomes.
Participants were restricted to undergraduate students from a particularly competitive university in the United States. Replicating the study across a variety of campuses and cultural contexts and including additional student populations, such as graduate students, would provide a more comprehensive assessment of the interventions. Moreover, the findings should be considered in relation to the large number of outcome measures, which necessitated correction for multiple comparisons.
Inactive control groups make it difficult to determine whether the effect of a given intervention is due to content alone (35). Future studies should include an active control group.
In sum, this study is one of the first to offer an evaluation of several recommendable and effective protocols for university administrators. Given the growing mental health crisis among college-aged students and increasing demand for university campus mental health services, there is an urgent need for cost-effective and preventative ways to address the problem. Providing preventative skills-building psychoeducational programs such as SKY and EI, as a supplement to standard care, may help buffer students’ mental health and well-being while providing relief from the financial and counseling burden on universities.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Yale Human Research Protection Program. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
ES, CB, and MB designed the pilot study and main study, participated in recruitment and data collection, consulted on data analysis, and wrote up the manuscript. JM conducted most of the data analyses and contributed to the manuscript. LH participated in recruitment, data collection and manuscript write-up. DN collected the pilot study data, consulted on the main study, and contributed to the manuscript.
Funding
This research was funded by an anonymous donor to the Yale Center for Emotional Intelligence. This project was in part also supported by a Jacobs Foundation Early Career Research Fellowship to JM.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank Julie McGarry, Amanda Votto and Annelies Richmond for their help in teaching the EI, MBSR and SKY programs respectively; Julie McGarry and Jessica Hoffman for developing the EI program; Dara Ghahremani for advising on statistical analyses and providing comments on the manuscript; and Carol Finke, Saijel Verma, Aryan Arora, Travers Brooks, and Antonia Pizzimenti for their help collecting and coding data. Thank you to Marissa King for helping us secure key locations for study procedures.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2020.00590/full#supplementary-material
References
1. World Health Organization (WHO). Constitution. (2020). https://www.who.int/about/who-we-are/constitution.
2. Lipson SK, Lattie EG, Eisenberg D. Increased rates of mental health service utilization by US college students: 10-year population-level trends (2007–2017). Psychiatr Serv (2018) 70(1):60–3. doi: 10.1176/appi.ps.201800332
3. Substance Abuse and Mental Health Services Administration (SAMHSA). 2017 National Survey on Drug Use and Health. (2017). Retrieved from https://www.nami.org/Learn-More/Mental-Health-By-the-Numbers.
4. National Institutes of Mental Health (NIMH). Mental Health Mediations. (2016). Retrieved October 7, 2019, Retrieved from https://www.nimh.nih.gov/health/topics/mental-health-medications/index.shtml.
5. Association for University and College Counseling Center Directors (AUCCCD). The Association for University and College Counseling Center Directors Annual Survey – Public Version 2018. (2018). Retrieved from https://www.aucccd.org/assets/documents/Survey/2018%20AUCCCD%20Survey-Public-June%2012-FINAL.pdf.
6. Pérez-Rojas AE, Lockard AJ, Bartholomew TT, Janis RA, Carney DM, Xiao H, et al. Presenting concerns in counseling centers: The view from clinicians on the ground. psychol Serv (2017) 14(4):416–27. doi: 10.1037/ser0000122
7. American College Health Association – National College Health Assessment (ACHA). Fall 2018 Reference Group Executive Summary. (2018). Retrieved from https://www.acha.org/documents/ncha/NCHA-II_Fall_2018_Reference_Group_Executive_Summary.pdf.
8. Eisenberg D, Golberstein E, Hunt JB. Mental health and academic success in college. BE J Econ Anal Policy (2009) 9(1). doi: 10.2202/1935-1682.2191
9. Walters KS, Bulmer SM, Troiano PF, Obiaka U, Bonhomme R. Substance use, anxiety, and depressive symptoms among college students. J Child Adolesc Subst Abuse (2018) 27(2):103–11. doi: 10.1080/1067828X.2017.1420507
10. Meshesha LZ, Utzelmann B, Dennhardt AA, Murphy JG. A behavioral economic analysis of marijuana and other drug use among heavy drinking young adults. Trans Issues psychol Sci (2018) 4(1):65–75. doi: 10.1037/tps0000144
11. Liu CH, Stevens C, Wong SH, Yasui M, Chen JA. The prevalence and predictors of mental health diagnoses and suicide among US college students: Implications for addressing disparities in service use. Depression Anxiety (2019) 36(1):8–17. doi: 10.1002/da.22830
12. World Health Organization (WHO). Prevention of Suicidal Behaviors: A Task for All. (2019). Retrieved from: https://www.who.int/mental_health/prevention/suicide/background/en/.
13. Centers for Disease Control and Prevention (CDC). (2017). Data & Statistics Fatal Injury Report for 2017. Retrieved from https://afsp.org/about-suicide/suicide-statistics/.
14. World Health Organization (WHO). World health statistics: Monitoring health for the sustainable development goals. Geneva, Switzerland: World Health Organization (2016).
15. Miron O, Yu KH, Wilf-Miron R, Kohane IS. Suicide rates among adolescents and young adults in the United States, 2000-2017. Jama (2019) 321(23):2362–4. doi: 10.1001/jama.2019.5054
16. National Institutes of Mental Health (NIMH). Suicide. (2018). Retrieved December 6, 2018, Retrieved from https://www.nimh.nih.gov/health/statistics/suicide.shtml.
17. Baumeister RF, Leary MR. The need to belong: desire for interpersonal attachments as a fundamental human motivation. psychol Bull (1995) 117(3):497. doi: 10.1037/0033-2909.117.3.497
18. Beutel ME, Klein EM, Brähler E, Reiner I, Jünger C, Michal M, et al. Loneliness in the general population: prevalence, determinants and relations to mental health. BMC Psychiatry (2017) 17(19). doi: 10.1186/s12888-017-1262-x
19. Burke TJ, Ruppel EK, Dinsmore DR. Moving away and reaching out: Young adults’ relational maintenance and psychosocial well-being during the transition to college. J Family Commun (2016) 16(2):180–7. doi: 10.1080/15267431.2016.1146724
20. Cacioppo JT, Cacioppo S. Social Relationships and Health: The Toxic Effects of Perceived Social Isolation. Soc Pers Psychol Compass (2014) 8(2):58–72. doi: 10.1111/spc3.12087
21. Drake EC, Sladek MR, Doane LD. Daily cortisol activity, loneliness, and coping efficacy in late adolescence: A longitudinal study of the transition to college. Int J Behav Dev (2016) 40(4):334–45. doi: 10.1177/0165025415581914
22. Erzen E, Çikrikci Ö. The effect of loneliness on depression: A meta-analysis. Int J Soc Psychiatry (2018) 64(5):427–35. doi: 10.1177/0020764018776349
23. Matthews T, Danese A, Caspi A, Fisher HL. Lonely young adults in modern Britain: findings from an epidemiological cohort study. psychol Med (2019) 49(2):268–77. doi: 10.1017/S0033291718000788
24. Stoliker BE, Lafreniere KD. The influence of perceived stress, loneliness, and learning burnout on university students’ educational experience. Coll Stud J (2015) 49(1):146–60.
25. Xiao H, Carney DM, Youn SJ, Janis RA, Castonguay LG, Hayes JA, et al. Are we in crisis? National mental health and treatment trends in college counseling centers. psychol Serv (2017) 14(4):407–15. doi: 10.1037/ser0000130
26. Gallagher RP. National Survey of College Counseling Centers 2014. Project Report. Int Assoc Couns Serv (IACS) (2015).
27. American Psychological Association (APA). Clinical Practice Guideline for the Treatment of Depression Across Three Age Cohorts American Psychological Association Guideline Development Panel for the Treatment of Depressive Disorders. (2019). Retrieved from https://www.apa.org/depression-guideline/guideline.pdf.
28. Davidson JR. Major depressive disorder treatment guidelines in America and Europe. J Clin Psychiatry (2010) 71 Suppl E1:e04. doi: 10.4088/JCP.9058se1c.04gry
29. Lipson SK, Abelson S, Ceglarek P, Philips M, Eisenberg D. Investing in Student Mental Health: Opportunities & Benefits for College Leadership. Am Counc Educ (2019).
30. Popovic D, Vieta E, Fornaro M, Perugi G. Cognitive tolerability following successful long-term treatment of major depression and anxiety disorders with SSRI antidepressants. J Affect Disord (2015) 173:211–5. doi: 10.1016/j.jad.2014.11.008
31. Durlak JA. Successful prevention programs for children and adolescents. New York: Plenum Press (1997). doi: 10.1007/978-1-4899-0065-4
32. Botvin GJ, Griffin KW. School-based programmes to prevent alcohol, tobacco and other drug use. Int Rev Psychiatry (2007) 19:607–15. doi: 10.1080/09540260701797753
33. Stice E, Shaw H, Marti CN. A meta-analytic review of eating disorder prevention programs: Encouraging findings. Annu Rev Clin Psychol (2007) 3:207–31. doi: 10.1146/annurev.clinpsy.3.022806.091447
34. Conley CS, Durlak JA, Kirsch AC. A meta-analysis of universal mental health prevention programs for higher education students. Prev Sci (2015) 16(4):487–507. doi: 10.1007/s11121-015-0543-1
35. Yusufov M, Nicoloro-SantaBarbara J, Grey NE, Moyer A, Lobel M. Meta-analytic evaluation of stress reduction interventions for undergraduate and graduate students. Int J Stress Manage (2019) 26(2):132–45. doi: 10.1037/str0000099
36. Goldstein MR, Lewis GF, Newman R, Brown JM, Bobashev G, Kilpatrick L. Improvements in well-being and vagal tone following a yogic breathing- based life skills workshop in young adults: Two open-trial pilot studies. Int J Yoga (2016) 9(1):20. doi: 10.4103/0973-6131.171718
37. Kjellgren A, Bood S, Axelsson K, Norlander T, Saatcioglu F. Wellness through a comprehensive Yogic breathing program–A controlled pilot trial. BMC Complement Altern Med (2007) 7(1):43. doi: 10.1186/1472-6882-7-43
38. Subramanian S, Elango T, Malligarjunan H, Kochupillai V, Dayalan H. Role of sudarshan kriya and pranayam on lipid profile and blood cell parameters during exam stress: A randomized controlled trial. Int J Yoga (2012) 5(1):21. doi: 10.4103/0973-6131.91702
39. Ghahremani DG, Oh EY, Dean AC, Mouzakis K, Wilson KD, London ED. Effects of the Youth Empowerment Seminar on impulsive behavior in adolescents. J Adolesc Health (2013) 53(1):139–41. doi: 10.1016/j.jadohealth.2013.02.010
40. Gootjes L, Franken IH, Van Strien JW. Cognitive emotion regulation in yogic meditative practitioners. J Psychophysiol (2011) 25(2):87–94. doi: 10.1027/0269-8803/a000043
41. Agte VV, Chiplonkar SA. Sudarshan kriya yoga for improving antioxidant status and reducing anxiety in adults. Altern Complement Ther (2008) 14(2):96–100. doi: 10.1089/act.2008.14204
42. Chandra S, Jaiswal AK, Singh R, Jha D, Mittal AP. Mental stress: Neurophysiology and its regulation by Sudarshan Kriya Yoga. Int J Yoga (2017) 10(2):67. doi: 10.4103/0973-6131.205508
43. Kumar N, Bhatnagar S, Velpandian T, Patnaik S, Menon G, Mehta M, et al. Randomized controlled trial in advance stage breast cancer patients for the effectiveness on stress marker and pain through Sudarshan Kriya and Pranayama. Indian J Palliat Care (2013) 19(3):180. doi: 10.4103/0973-1075.121537
44. Doria S, De Vuono A, Sanlorenzo R, Irtelli F, Mencacci C. Anti-anxiety efficacy of Sudarshan Kriya Yoga in general anxiety disorder: a multicomponent, yoga based, breath intervention program for patients suffering from generalized anxiety disorder with or without comorbidities. J Affect Disord (2015) 184:310–7. doi: 10.1016/j.jad.2015.06.011
45. Hamilton-West K, Pellatt-Higgins T, Sharief F. Evaluation of a Sudarshan Kriya Yoga (SKY) based breath intervention for patients with mild-to-moderate depression and anxiety disorders. Prim Health Care Res Dev (2019) 20(e73):1–8. doi: 10.1017/S1463423619000045
46. Janakiramaiah N, Gangadhar BN, Murthy PNV, Harish MG, Subbakrishna DK, Vedamurthachar A. Antidepressant efficacy of Sudarshan Kriya Yoga (SKY) in melancholia: a randomized comparison with electroconvulsive therapy (ECT) and imipramine. J Affect Disord (2000) 57(1-3):255–9. doi: 10.1016/S0165-0327(99)00079-8
47. Katzman MA, Vermani M, Gerbarg PL, Brown RP, Iorio C, Davis M, et al. A multicomponent yoga-based, breath intervention program as an adjunctive treatment in patients suffering from generalized anxiety disorder with or without comorbidities. Int J Yoga (2012) 5(1):57–65. doi: 10.4103/0973-6131.91716
48. Sharma A, Barrett MS, Cucchiara AJ, Gooneratne NS. Thase ME. A breathing-based meditation intervention for patients with major depressive disorder following inadequate response to antidepressants: a randomized pilot study. J Clin Psychiatry (2017) 78(1):e59. doi: 10.4088/JCP.16m10819
49. Toschi-Dias E, Tobaldini E, Solbiati M, Costantino G, Sanlorenzo R, Doria S, et al. Sudarshan Kriya Yoga improves cardiac autonomic control in patients with anxiety-depression disorders. J Affect Disord (2017) 214:74–80. doi: 10.1016/j.jad.2017.03.017
50. Vedamurthachar A, Janakiramaiah N, Hegde JM, Shetty TK, Subbakrishna DK, Sureshbabu SV, et al. Antidepressant efficacy and hormonal effects of Sudarshan Kriya Yoga (SKY) in alcohol dependent individuals. J Affect Disord (2006) 94(1-3):249–53. doi: 10.1016/j.jad.2006.04.025
51. Descilo T, Vedamurtachar A, Gerbarg PL, Nagaraja D, Gangadhar BN, Damodaran B, et al. Effects of a yoga breath intervention alone and in combination with an exposure therapy for post-traumatic stress disorder and depression in survivors of the 2004 South-East Asia tsunami. Acta Psychiatr Scand (2010) 121(4):289–300. doi: 10.1111/j.1600-0447.2009.01466.x
52. Seppälä EM, Nitschke JB, Tudorascu DL, Hayes A, Goldstein MR, Nguyen DT, et al. Breathing-based meditation decreases posttraumatic stress disorder symptoms in US Military veterans: A randomized controlled longitudinal study. J Trauma Stress (2014) 27(4):397–405. doi: 10.1002/jts.21936
53. Brackett MA, Bailey CS, Hoffmann JD, Simmons DN. RULER: A Theory-Driven, Systemic Approach to Social, Emotional, and Academic Learning. Educ Psychol (2019) 19:1–18. doi: 10.1080/00461520.2019.1614447
54. Brackett MA, Rivers SE, Reyes MR, Salovey P. Enhancing academic performance and social and emotional competence with the RULER feeling words curriculum. Learn Individ Dif (2012) 22(2):218–24. doi: 10.1016/j.lindif.2010.10.002
55. Rivers SE, Brackett MA, Reyes MR, Elbertson NA, Salovey P. Improving the social and emotional climate of classrooms: A clustered randomized controlled trial testing the RULER approach. Prev Sci (2013) 14(1):77–87. doi: 10.1007/s11121-012-0305-2
56. Reyes MR, Brackett MA, Rivers SE, Elbertson NA, Salovey P. The interaction effects of program training, dosage, and implementation quality on targeted student outcomes for the RULER approach to social and emotional learning. Sch Psychol Rev (2012) 41(1):82–99. doi: 10.1037/t36292-000
57. Castillo R, Fernández-Berrocal P, Brackett MA. Enhancing teacher effectiveness in Spain: A pilot study of the RULER approach to social and emotional learning. J Educ Training Stud (2013) 1(2):263–72. doi: 10.11114/jets.v1i2.203
58. Canby NK, Cameron IM, Calhoun AT, Buchanan GM. A brief mindfulness intervention for healthy college students and its effects on psychological distress, self-control, meta-mood, and subjective vitality. Mindfulness (2015) 6(5):1071–81. doi: 10.1007/s12671-014-0356-5
59. Felver JC, Morton ML, Clawson AJ. Mindfulness-Based Stress Reduction Reduces Psychological Distress in College Students. Coll Stud J (2018) 52(3):291–8.
60. Shapiro SL, Oman D, Thoresen CE, Plante TG, Flinders T. Cultivating mindfulness: effects on well-being. J Clin Psychol (2008). 64(7):840–62. doi: 10.1002/jclp.20491
61. Song Y, Lindquist R. Effects of mindfulness-based stress reduction on depression, anxiety, stress and mindfulness in Korean nursing students. Nurse Educ Today (2015) 35(1):86–90. doi: 10.1016/j.nedt.2014.06.010
62. Cramer H, Lauche R, Paul A, Dobos G. Mindfulness-based stress reduction for breast cancer—a systematic review and meta-analysis. Curr Oncol (2012) 19(5):e343–52. doi: 10.3747/co.19.1016
63. Speca M, Carlson LE, Goodey E, Angen M. A randomized, wait-list controlled clinical trial: the effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. Psychosom Med (2000) 62(5):613–22. doi: 10.1097/00006842-200009000-00004
64. Robins CJ, Keng SL, Ekblad AG, Brantley JG. Effects of mindfulness-based stress reduction on emotional experience and expression: A randomized controlled trial. J Clin Psychol (2012) 68(1):117–31. doi: 10.1002/jclp.20857
65. Biegel GM, Brown KW, Shapiro SL, Schubert CM. Mindfulness-based stress reduction for the treatment of adolescent psychiatric outpatients: A randomized clinical trial. J Consult Clin Psychol (2009) 77(5):855–66. doi: 10.1037/a0016241
66. Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J Psychosom Res (2004) 57(1):35–43. doi: 10.1016/S0022-3999(03)00573-7
67. John OP, Srivastava S, Pervin LA, John OP. Handbook of personality: Theory and research Vol. 2. New York: Guilford Press (1999). p. 102–38.
68. Zope SA, Zope RA. Sudarshan kriya yoga: Breathing for health. Int J Yoga (2013) 6(1):4–10. doi: 10.4103/0973-6131.105935
69. Kabat-Zinn J. Mindfulness-based interventions in context: past, present, and future. Clin Psychol: Sci Pract (2003) 10(2):144–56. doi: 10.1093/clipsy.bpg016
70. Schmoldt R, Freeborn D, Klevit H. Physician burnout: Recommendations for HMO managers. HMO Practice/HMO Group (1994) 8:58–63.
71. Rohland BM, Kruse GR, Rohrer JE. Validation of a single-item measure of burnout against the Maslach Burnout Inventory among physicians. Stress Health: J Int Soc Invest Stress (2004) 20(2):75–9. doi: 10.1002/smi.1002
72. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav (1983) 24(4):385–96. doi: 10.2307/2136404
73. Lin A, Yung AR, Wigman JT, Killackey E, Baksheev G, Wardenaar KJ. Validation of a short adaptation of the Mood and Anxiety Symptoms Questionnaire (MASQ) in adolescents and young adults. Psychiatry Res (2014) 215(3):778–83. doi: 10.1016/j.psychres.2013.12.018
74. Hays DR, Sherborne CD, Mazel RM. Mazel RM, Sherbourne CD, Mazel RM, editors. Hayes, Cathy Donald Sherbourne. Santa Monica, CA: Rand Corp (1995).
75. Ryff CD, Keyes CLM. The structure of psychological well-being revisited. J Pers Soc Psychol (1995) 69(4):719–27. doi: 10.1037/0022-3514.69.4.719
76. Diener ED, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess (1985) 49(1):71–5. doi: 10.1207/s15327752jpa4901_13
77. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol (1988) 54(6):1063–70. doi: 10.1037/0022-3514.54.6.1063
78. McCullough ME, Emmons RA, Tsang JA. The grateful disposition: A conceptual and empirical topography. J Pers Soc Psychol (2002) 82(1):112–27. doi: 10.1037//0022-3514.82.1.112
79. Raes F, Pommier E, Neff KD, Van Gucht D. Construction and factorial validation of a short form of the self-compassion scale. Clin Psychol Psychother (2011) 18(3):250–5. doi: 10.1002/cpp.702
80. Baer RA, Carmody J, Hunsinger M. Weekly change in mindfulness and perceived stress in a mindfulness-based stress reduction program. J Clin Psychol (2012) 68(7):755–65. doi: 10.1002/jclp.21865
81. Carver CS. You want to measure coping but your protocol’ too long: Consider the brief cope. Int J Behav Med (1997) 4(1):92. doi: 10.1207/s15327558ijbm0401_6
82. Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A re-evaluation of the Life Orientation Test. J Pers Soc Psychol (1994) 67:1063–78. doi: 10.1037/0022-3514.67.6.1063
83. Robins RW, Hendin HM, Trzesniewski KH. Measuring Global Self-Esteem: Construct Validation of a Single-Item Measure and the Rosenberg Self-Esteem Scale. Pers Soc Psychol Bull (2001) 27:151–61. doi: 10.1177/0146167201272002
84. Lee RM, Draper M, Lee S. Social connectedness, dysfunctional interpersonal behaviors, and psychological distress: Testing a mediator model. J Couns Psychol (2001) 48(3):310–8. doi: 10.1037/0022-0167.48.3.310
86. Chakhssi F, Kraiss JT, Sommers-Spijkerman M. Bohlmeijer ET. The effect of positive psychology interventions on well-being and distress in clinical samples with psychiatric or somatic disorders: a systematic review and meta-analysis. BMC Psychiatry (2018) 18:211. doi: 10.1186/s12888-018-1739-2
87. Breedvelt JJF, Amanvermez Y, Harrer M, Karyotaki E, Gilbody S, Bockting CLH, et al. The Effects of Meditation, Yoga, and Mindfulness on Depression, Anxiety, and Stress in Tertiary Education Students: A Meta-Analysis. Front Psychiatry (2019) 10:193. doi: 10.3389/fpsyt.2019.00193
88. Hendriks T, de Jong J, Cramer H. The effects of yoga on positive mental health among healthy adults: a systematic review and meta-analysis. J Altern Complement Med (2017) 23(7):505–17. doi: 10.1089/acm.2016.0334
89. Zoogman S, Goldberg SB, Vousoura E, Diamond MC, Miller L. Effect of yoga-based interventions for anxiety symptoms: A meta-analysis of randomized controlled trials. Spiritual Clin Pract (2019) 6(4):256–78. doi: 10.1037/scp0000202
90. Yeung J, Zhang Z, Kim TY. Volunteering and health benefits in general adults: cumulative effects and forms. BMC Public Health (2017) 18(1):8. doi: 10.1186/s12889-017-4561-8
91. Maric V, Ramanathan D, Mishra J. Respiratory Regulation & Interactions with Neuro-Cognitive Circuitry. Neurosci Biobehav Rev (2020) 112:95–106. doi: 10.1016/j.neubiorev.2020.02.001
92. Nakamura NH, Fukunaga M, Oku Y. Respiratory modulation of cognitive performance during the retrieval process. PloS One (2018) 13(9):e0204021. doi: 10.1371/journal.pone.0204021
93. Ahern E, Semkovska M. Cognitive functioning in the first-episode of major depressive disorder: A systematic review and meta-analysis. Neuropsychology (2017) 31(1):52–72. doi: 10.1037/neu0000319
94. Melnychuk MC, Dockree PM, O’Connell RG, Murphy PR, Balsters JH, Robertson IH. Coupling of respiration and attention via the locus coeruleus: Effects of meditation and pranayama. Psychophysiology (2018) 55(9):e13091. doi: 10.1111/psyp.13091
95. Zaccaro A, Piarulli A, Laurino M, Garbella E, Menicucci D, Neri B, et al. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Front Hum Neurosci (2018) 12:353. doi: 10.3389/fnhum.2018.00353
96. Khoury B, Sharma M, Rush SE, Fournier C. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J Psychosom Res (2015) 78(6):519–28. doi: 10.1016/j.jpsychores.2015.03.009
97. National Center for Education Statistics (NCES). Average salary of full-time instructional faculty on 9-month contracts in degree-granting postsecondary institutions, by academic rank, control and level of institution, and sex: Selected years, 1970-71 through 2016-17. (2017). Retrieved October 7, 2019, Retrieved from https://nces.ed.gov/programs/digest/d17/tables/dt17_316.10.asp.
Keywords: emotional intelligence, mindfulness-based stress reduction, Sudarshan Kriya, college mental health, well-being, sky campus happiness, depression, anxiety
Citation: Seppälä EM, Bradley C, Moeller J, Harouni L, Nandamudi D and Brackett MA (2020) Promoting Mental Health and Psychological Thriving in University Students: A Randomized Controlled Trial of Three Well-Being Interventions. Front. Psychiatry 11:590. doi: 10.3389/fpsyt.2020.00590
Received: 19 February 2020; Accepted: 08 June 2020;
Published: 15 July 2020.
Edited by:
Liam Mason, University College London, United KingdomReviewed by:
Carlos Freire, University of A Coruña, SpainAlyson Dodd, Northumbria University, United Kingdom
Copyright © 2020 Seppälä, Bradley, Moeller, Harouni, Nandamudi and Brackett. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emma M. Seppälä, ZW1tYXNlcEBnbWFpbC5jb20=
†These authors have contributed equally to this work