 Birgit Wagner
Birgit Wagner Nicole Rosenberg1
Nicole Rosenberg1 Laura Hofmann
Laura Hofmann Ulrike Maass
Ulrike Maass- 1Clinical Psychology and Psychotherapy, Medical School Berlin, Berlin, Germany
- 2Clinical Psychology and Psychotherapy, University of Potsdam, Potsdam, Germany
Background: Web-based interventions have been introduced as novel and effective treatments for mental disorders and, in recent years, specifically for the bereaved. However, a systematic summary of the effectiveness of online interventions for people experiencing bereavement is still missing.
Objective: A systematic literature search was conducted by four reviewers who reviewed and meta-analytically summarized the evidence for web-based interventions for bereaved people.
Methods: Systematic searches (PubMed, Web of Science, PsycInfo, PsycArticles, Medline, and CINAHL) resulted in seven randomized controlled trials (N = 1,257) that addressed adults having experienced bereavement using internet-based interventions. We used random effects models to summarize treatment effects for between-group comparisons (treatment vs. control at post) and stability over time (post vs. follow-up).
Results: All web-based interventions were based on cognitive behavioral therapy (CBT). In comparison with control groups, the interventions showed moderate (g = .54) to large effects (g = .86) for symptoms of grief and posttraumatic stress disorder (PTSD), respectively. The effect for depression was small (g = .44). All effects were stable over time. A higher number of treatment sessions achieved higher effects for grief symptoms and more individual feedback increased effects for depression. Other moderators (i.e. dropout rate, time since loss, exposure) did not significantly reduce moderate degrees of heterogeneity between the studies.
Limitations: The number of includable studies was low in this review resulting to lower power for moderator analyses in particular.
Conclusions: Overall, the results of web-based bereavement interventions are promising, and its low-threshold approach might reduce barriers to bereavement care. Nonetheless, future research should further examine potential moderators and specific treatment components (e.g. exposure, feedback) and compare interventions with active controls.
Introduction
Grief after the loss of a significant person is a natural process, and most people adapt their grief gradually to their life after the death of a loved one. However, some people experience difficulties adjusting their grief over time. These difficulties can include separation distress, avoidance behavior, yearning for the deceased or a lack of acceptance of the loss (1). The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders [DSM-5; (2)] included the diagnostic criteria of the Persistent Complex Bereavement Disorder (PCBD) as diagnosis requiring further research, and the 11th edition of the International Classification of Diseases [ICD-11; (3)] included the clinical diagnosis Prolonged Grief disorder (PGD). The main difference between these two criteria sets concerns the time criterion. The PCBD criteria require a functional impairment for at least 12 months after the loss of a significant person, while the PGD criteria require only 6 months of functional impairment. Boelen and Lenferink (4) analyzed in their study four additional existing criteria sets for pathological forms of grief and compared the six diagnostic criteria regarding symptom combination, prevalence, and dimensions. The results of their study indicate a variation in dimensions and symptom combinations and prevalence rates ranging from 10 to 20%. They conclude that the existing criteria sets do not identify the same diagnostic symptom cluster. Similar findings were found in a German treatment-seeking sample (5), showing larger prevalence rates for PGD (69%) compared to PCBD (48%). Studies have shown that pathological grief differs from other disorders such as depression and PTSD and described a distinct diagnosis (4). Nonetheless, there are important associations with depressive symptoms (e.g., feelings of meaninglessness and worthlessness) as well as posttraumatic stress symptoms [e.g., distressful remembrance of the traumatic death of a loved one; (6)].
Today the research on PGD implies not only that there is a strong need for sound and valid diagnostic criteria; there is also a great need for research for treatment strategies for the bereaved.
Previous meta-analyses and systematic reviews of the treatment effects of face-to-face grief interventions have shown inconsistent results (7–11). For example, whereas it was shown that preventive interventions (i.e. to prevent a worsening of normal grief processes) were largely ineffective [d = 0.03–0.16; (11, 12)], interventions that were specifically aimed at prolonged grief symptoms have yielded better treatment effects [d = 0.53; (11); see also (10, 12–14)]. The most recent meta-analysis analyzed 31 randomized controlled studies (8). The authors found small but significant effects for psychological interventions for grief symptoms at post-intervention (Hedge's g = 0.40). These effects could be maintained at follow-up. In addition to these reviews, treatment approaches that were based on cognitive–behavioral components yielded good treatment efficacy (15–18).
Irrespective of the clinical evidence, manualized interventions are still not routinely used in outpatient care, nor are they easily available to clients who suffer from PGD or belong to a high-risk group. Currently, therapists specializing in the treatment of PGD are still rare. The number of bereaved people seeking psychological treatment is relatively low, too. For example, Currow et al. (19) examined the nature of bereavement help-seeking following an expected death in a population-based survey (N = 6,034) in Australia, and only 1.5% reached out for help from a doctor or nurse; 2.2% contacted a grief counsellor, and 1.9% contacted a spiritual advisor. Another cross-sectional survey of young adults bereaved by suicide and other sudden deaths (N = 3,432) in the United Kingdom found that only 13% of the participants had received formal support from health professionals. The most common barriers to utilizing professional mental health support are the worry that it might be too painful to speak about the grief experience (20), the belief that it is too difficult to find help (21), or a fear of stigmatization, specifically for those bereaved by suicide (22).
In the past years, accumulating research has shown that internet-based interventions—particularly cognitive behavioral interventions—can be beneficial for most common mental health disorders, with treatment effects comparable to those of face-to-face treatments (23). Further, studies have shown that internet-based interventions for posttraumatic stress disorder (24, 25) yield medium to large treatment effects compared with a waitlist control group. The interventions are usually delivered in different forms, ranging from self-help treatments without a therapist's guidance to mainly text-based interventions with high therapist involvement (26–31). Web-based bereavement care has a number of advantages which can overcome typical obstacles to receiving support. For example, online interventions offer geographic independence and a widespread dissemination of treatments. In addition, they provide a user-friendly and flexible approach that is more responsive to the reality of most people living in today's digitalized societies. Finally, there is web-based support that can be relatively anonymous (e.g., self-help apps or text-based programs) and can help bereaved patients overcome their initial shame or perceived feelings of stigma and might encourage them to confront themselves with feelings of guilt or disclosure of painful feelings.
In sum, there is growing evidence that psychological interventions have a positive effect on pathological grief symptoms, and there is also research showing the efficacy of internet-based interventions for mental disorders such as anxiety and affective disorders for a variety of populations. Considering that only a minority of bereaved people actively seek traditional forms of support [e.g., (19, 32)], an additional digital dissemination of evidence-based bereavement care might reach even more mourners. With the growing interest of psychotherapy research for e-mental-health interventions, a review of web-based interventions for the bereaved is still missing.
The aim of this systematic review and meta-analysis is to investigate the effectiveness of web-based bereavement interventions compared with control groups in reducing symptoms of grief in adults. Further, we examine the effects of these interventions on PTSD or depression. Due to the fact that existing research has been based on different diagnostic criteria sets, this review does not limit its scope to ICD-11 defined PGD but also includes the other existing criteria sets of disturbed grief symptoms (4) that were, for example, defined as “complicated grief disorder” (33) or “prolonged grief disorder” (1).
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (Supplementary Table 1; 34) was used as a guide for the literature search and reporting of results.
In PICOS terms (35), the current review addressed adults (≥18 years) who have experienced all types of losses of a significant person (Population). The main focus was the use of a web-based psychological treatment (Intervention) which was compared to a control group of any kind (Comparator). We focused on the results of measurements assessing grief symptoms as defined by the original study authors (Outcomes). Here grief did not necessarily have to be determined as the primary outcome in the original study, but the intervention should be aimed at grief. In addition, we examined PTSD and depression as outcome measurements. We included only randomized-controlled trials (Study design).
Identification, Selection of Studies, and Data Extraction
We included all studies according to the following criteria: (a) publication in a peer-reviewed journal; (b) presence of a randomized controlled design; (c) use of an internet-based intervention; (d) participants lost someone through death (i.e. bereaved individuals); and (e) assessment of prolonged grief symptoms using (f) validated grief measurements. The following exclusion criteria were also applied: (a) presentation of secondary data only; and (b) investigation of a heterogeneous sample (e.g. individuals suffering from traumas other than loss) without presenting results for bereaved individuals separately.
The following databases were used for the literature search: PubMed, Web of Science, PsycInfo/PsycArticles, Medline, and CINAHL. The search included the terms [(“grief” OR “mourning” OR “bereaved” OR “bereavement” OR “death”) AND (“online” OR “internet” OR “computer” OR “web”) AND (“intervention” OR “therapy” OR “self-help” OR “treatment” OR “program” OR “expressive writing”) AND (“randomized” OR “randomized” OR “controlled”)]. We searched the titles and abstracts of relevant articles that were written in English and were published between 1990 and January 17, 2020. In addition, we screened the reference lists of previous reviews and meta-analyses dealing with the issue of internet-based interventions and bereavement/trauma for relevant articles.
Four authors (BW, UM, LH, NR) extracted the following variables: author(s), publication year, title, country, time points of assessment, conditions, outcomes measures, sample size, characteristics of participants and interventions, type of analysis, means and standard deviations of outcome measures (i.e. PGD, depression, PTSD), and characteristics of dropouts.
The quality of the included studies was evaluated according to the list of Van Tulder et al. (36), which was based on recommendations by the Cochrane Collaboration Back Review Group (rating scale: yes, no, or unclear) and which the authors applied for their review on internet-based interventions. We eliminated one item because it was not suitable for this review and would have biased the results. The methodological quality of a study was rated good if it achieved a total yes-score ≥ 8 (i.e. met at least two thirds of the criteria). The rating was implemented independently by two of the authors (NR, BW) and was discussed in the case of dissent.
Effect Size Calculation
The meta-analytical summary of the effect sizes was done using RStudio 1.1.456 (37) and the metafor package (38) for two comparisons: (1) a between-group (treatment versus control group) at the post assessment, and (2) a within-group design to estimate the stability of the effects of the treatment from post to follow-up assessments. When studies reported several follow-up assessments, we took the one that was closer to the mean time interval. The mean differences between the means of the symptom levels were determined using the results of the studies' intention to treat (ITT) or per protocol (PP) data if ITT were not available. Hedge's g was used as the standardized effect size (ES) to correct for sample size differences (39) and was classified as small (g < 0.50), moderate (0.50 ≤ g ≤ 0.80), or large (g > 0.80) (40). Multiple assessments of the same outcome were combined to control for dependencies within the data. Heterogeneity (i.e. variation in ESs between the studies) using the Q-statistic and the I2 index, which indicates low (25%), moderate (50%), or high (75%) levels (41). In cases of at least moderate heterogeneity, we conducted separate meta-regressions to identify potential sources of this heterogeneity (42). The following moderators were considered relevant to explain potential differences in intervention characteristics: (a) dropout rate in the treatment and control group, (b) time since loss in months and number of treatment sessions, (c) the extent of personal therapeutic feedback during treatment (no feedback = 0, informative feedback = 1, personal therapeutic feedback = 2), and (d) the use of exposure, cognitive reappraisal, or behavioral activation within the treatment (each: not applied = 0, applied = 1). All analyses used random-effects models that allowed the amount of residual heterogeneity to be different in each study. A power analysis for random effects models (42) revealed that 6 studies are needed to achieve a power of.84 expecting a moderate mean ES of Hedge's g = 0.50 for grief in studies with at least 20 participants per group and moderate heterogeneity (11, 24).
Results
Figure 1 shows the selection process. Seven studies were included in this review.
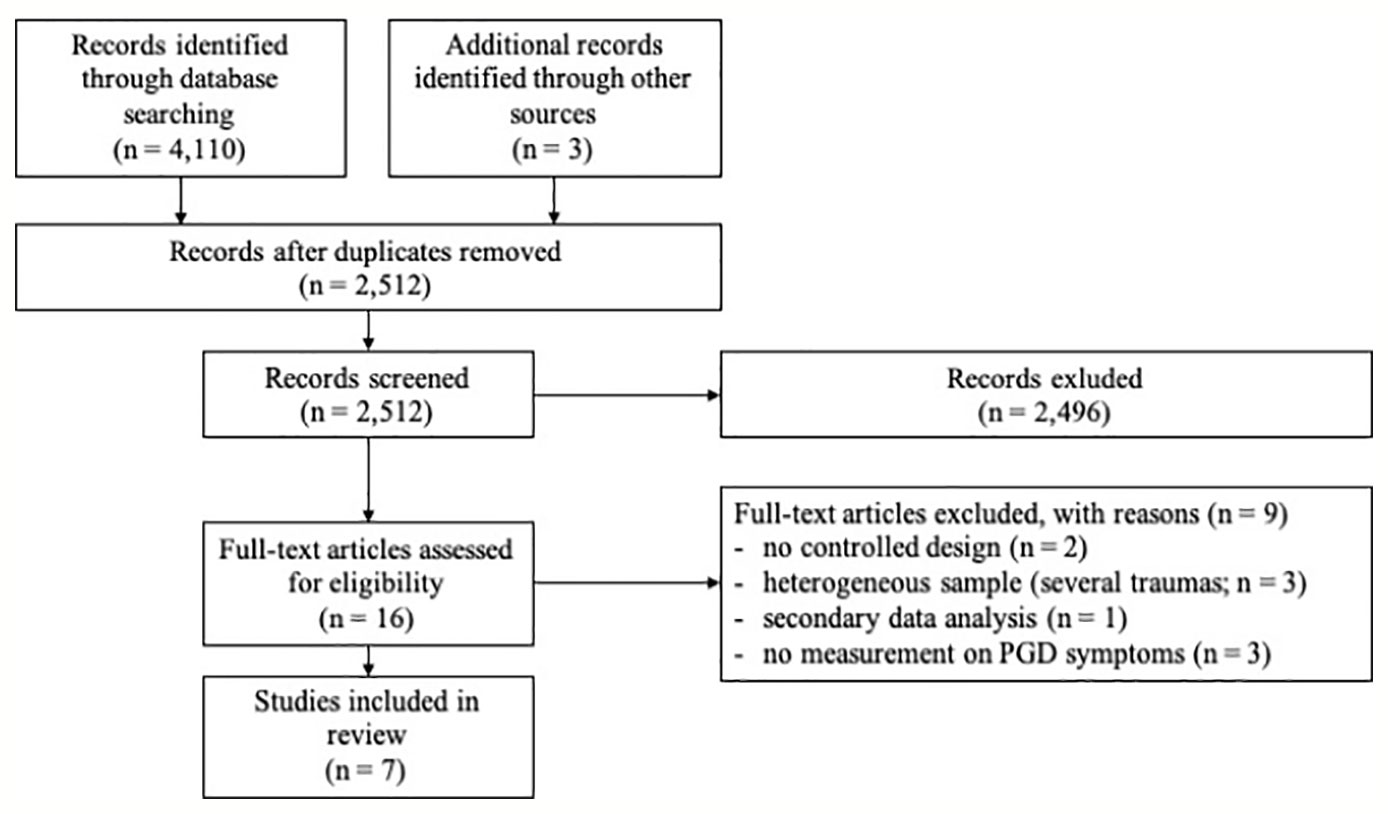
Figure 1 Study flow diagram, showing the results of the literature search for this current review.
Study Characteristics and Methodological Quality
The study characteristics are presented in Table 1. One study (43) provided two between-group comparisons because the authors compared two conditions with each other (exposure vs. behavioral activation) and against a control group. The studies of Wagner (18) and Wagner and Maercker (44) were based on the same trial but focused on different time points: posttreatment symptoms versus follow-up. Consequently, there were seven studies based on six trials yielding seven comparisons at post and follow-up for grief.
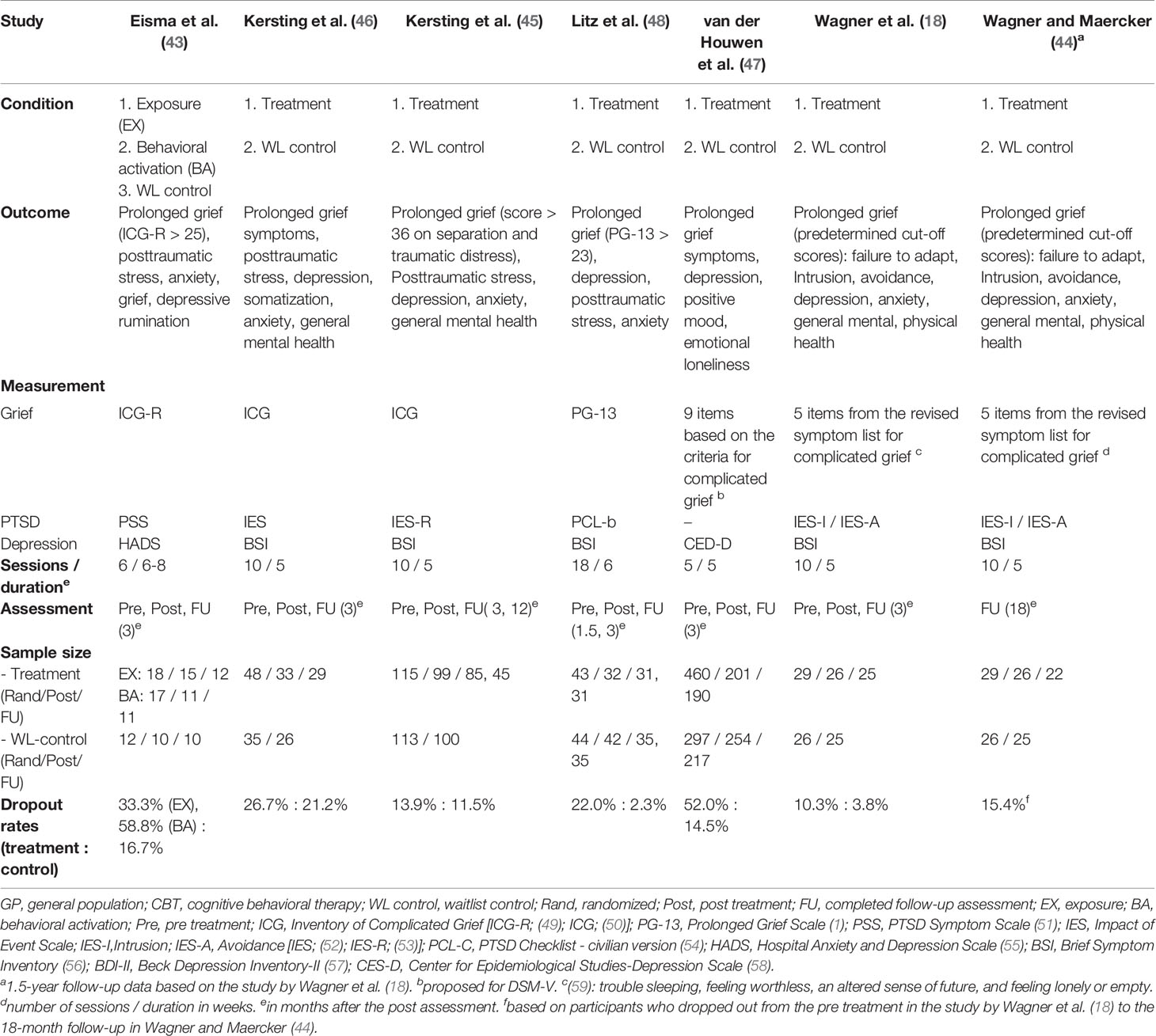
Table 1 Study characteristics.
All studies assessed PGD, depression, and PTSD symptoms in response to the loss (see Table 1 for the according measurements).
The methodological quality of the included studies varied, with no study meeting all 12 criteria (see Table 2). Four studies (50%; 43, 45–47) were rated as having good methodological quality.
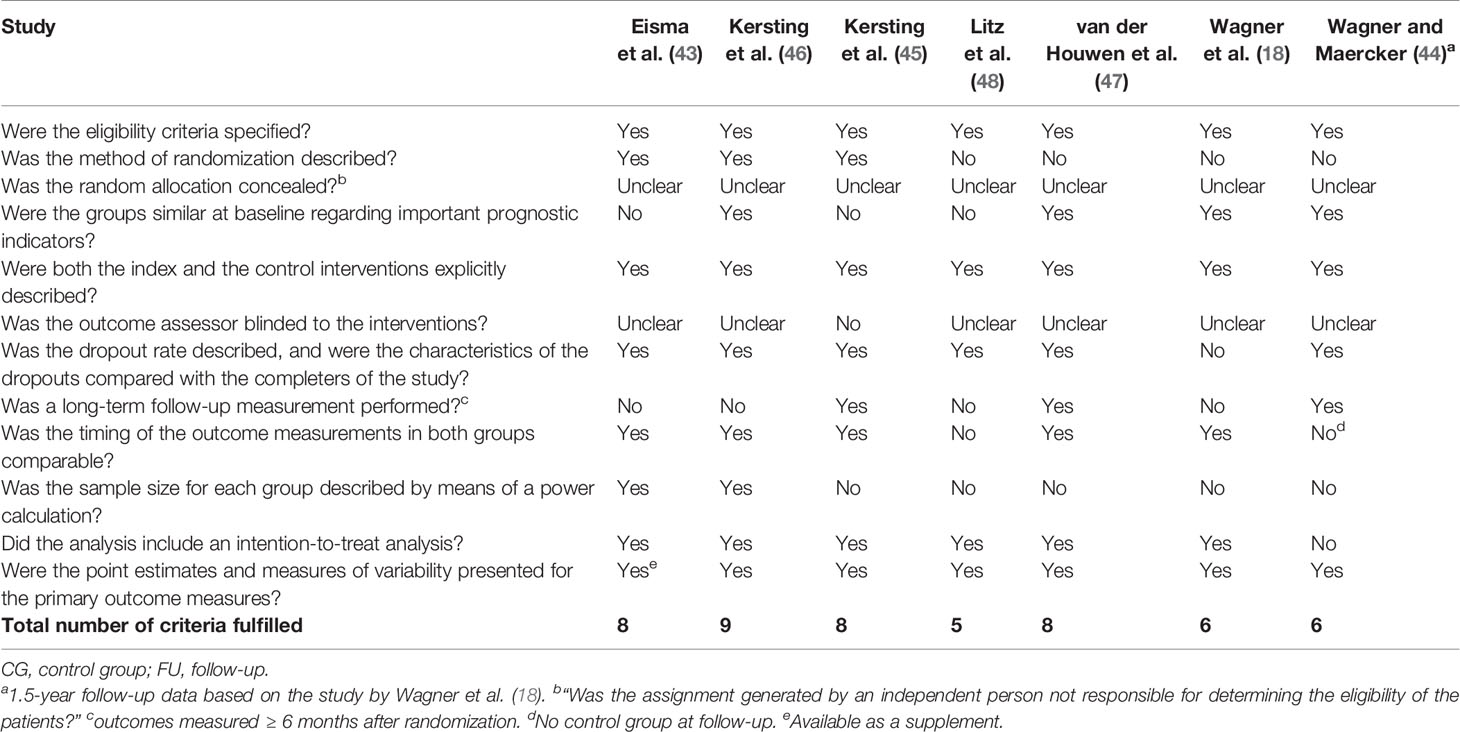
Table 2 Methodological quality of included studies.
Six studies (18, 43, 45–48) reported results from ITT analyses. One study (48) applied linear mixed models using REML, two studies applied multilevel analyses (43, 47), and three studies used the last observation carried forward approach to handle missing data (18, 45, 46). To calculate the ES for our review, we referred to the corresponding sample sizes per protocol (PP) except for Kersting et al. (45), who reported means from ITT data, and Wagner et al. (18), who reported means for completers only.
Samples
The studies included a total of N = 1,257 randomized participants from the general population. Table 3 presents the sample's characteristics. Women comprised between 68 and 100% of the samples. The average age of the total sample was 41.7 years. Overall, participants tended to be well-educated (i.e., college and university degrees), with five studies indicating that the education level of most of their participants was high.
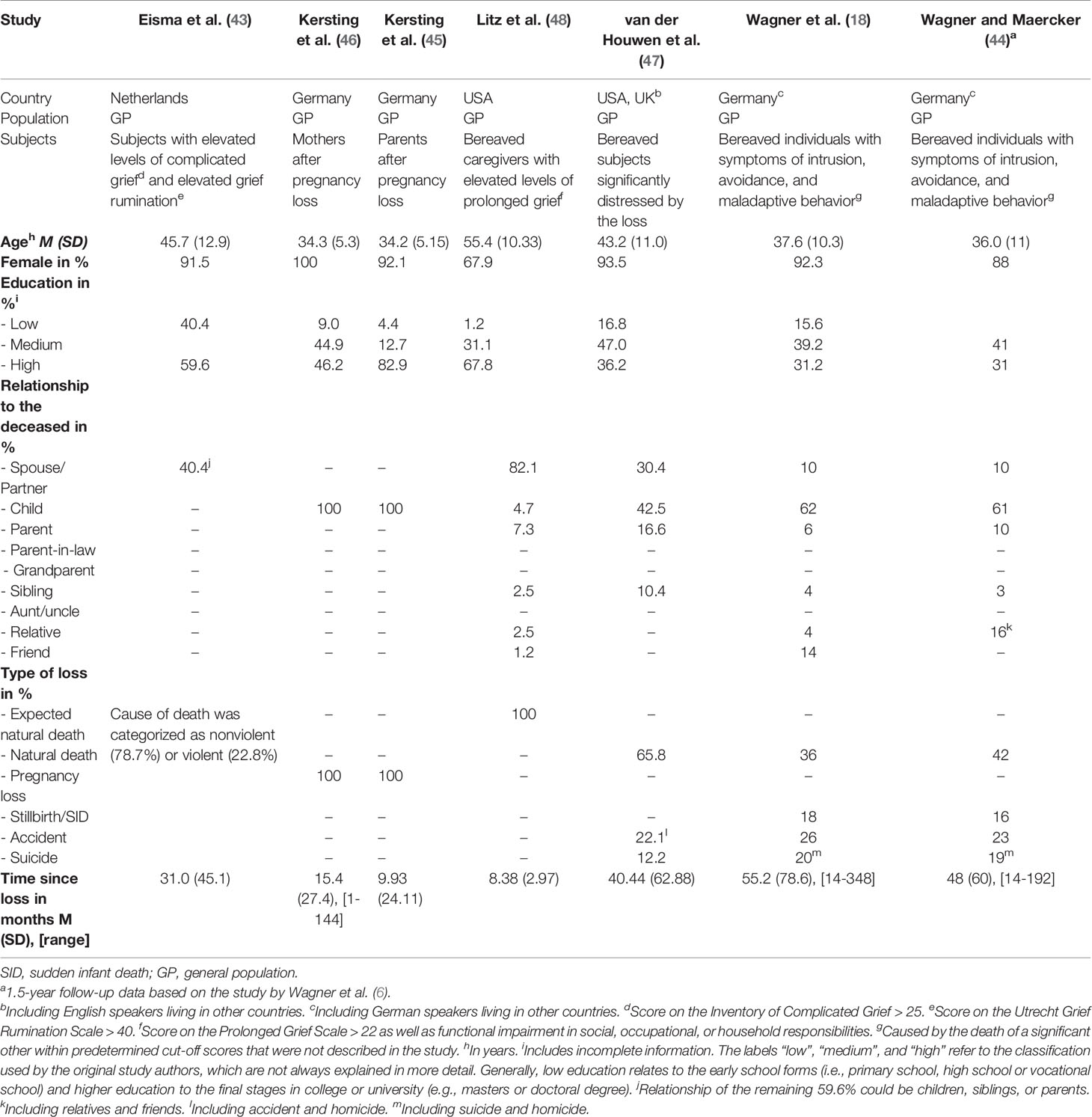
Table 3 Sample characteristics.
Two of the included studies addressed only mothers (46) and parents (45), respectively, who had lost a child during pregnancy, whereas one study (48) included only people who had experienced the expected natural death of someone. The causes of death in the remaining studies were (unexpected) natural death, stillbirth, sudden infant death, or death by accident, suicide, or homicide. Time since loss ranged from 8.38 to 55.2 months, with a mean of 26.7 months, indicating great variability for this variable.
All studies used measurements that explicitly addressed symptoms that were labeled as “complicated” or “prolonged” grief or grief disorder [see (4) for a comparison of different criteria sets for PGD]. As Table 1 displays, only two studies did not apply a cut-off score to indicate higher levels of PGD (46, 47).
Characteristics of the Interventions
Table 4 provides an overview of the characteristics of the different intervention programs. Three studies included minimal therapeutic support, such as explanations regarding homework and minor logistical help (43, 47, 48). Four studies involved individualized feedback after most treatment modules (18, 44–46). Further, five studies used structured writing assignments (18, 44–47) based on the Pennebaker paradigm (62). All of the included studies used an approach based on cognitive behavioral therapy (CBT).
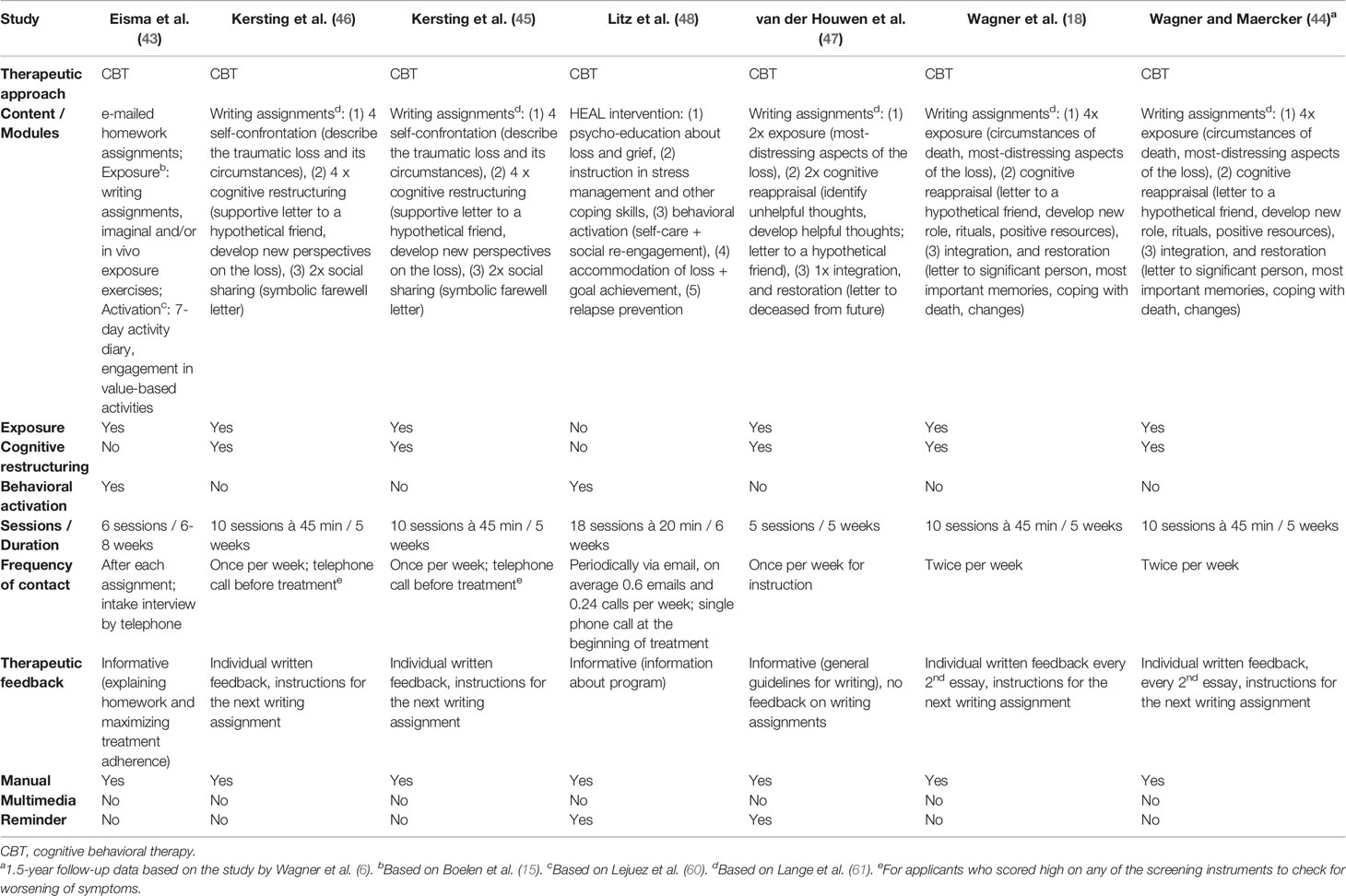
Table 4 Characteristics of the intervention programs
Regarding the content of the programs, six studies used a manual and included an exposure module (18, 43–47), five studies involved cognitive reappraisal (including integration and restoration, also called social sharing) (18, 44–47), and two studies used behavioral activation modules (43, 48). Five studies were based on an adjusted protocol for the treatment of posttraumatic stress disorder through the internet by Lange et al. (63).
Dropouts
We defined dropouts as all participants who completed pre-assessments but did not complete the treatment (or waitlist period). The rates of dropouts (Table 1) ranged from 10.3 (18) to 58.8% (43).
All included studies provided some information about the characteristics of dropouts, except for Wagner et al. (18). Eisma et al. (43) reported no significant differences between completers and dropouts on any of the assessed variables (demographic, loss-related, symptom, and rumination). In the study by Kersting et al. (46), time since loss was significantly longer for dropouts. By contrast, time since loss was shorter for Kersting et al.'s (45) dropouts, who were also younger and lost their child significantly earlier in pregnancy (the study investigated pregnancy loss). Litz et al. (48) reported that their dropouts received more average weekly emails from the therapist during the program and that they were more often employed full-time than completers. Dropouts differed on several variables in the study by van der Houwen et al. (47): They were younger, had lower levels of education, experienced more grief and were more likely to be in the treatment condition.
Effect Sizes
The results for the between-group comparisons are displayed in Figure 2. The overall effect on grief symptoms was moderate and significant with moderate to high heterogeneity between the studies. The ESs for PTSD1 and depression were almost moderate (depression) to large (PTSD) and statistically significant with low (PTSD) and high (depression) heterogeneity.
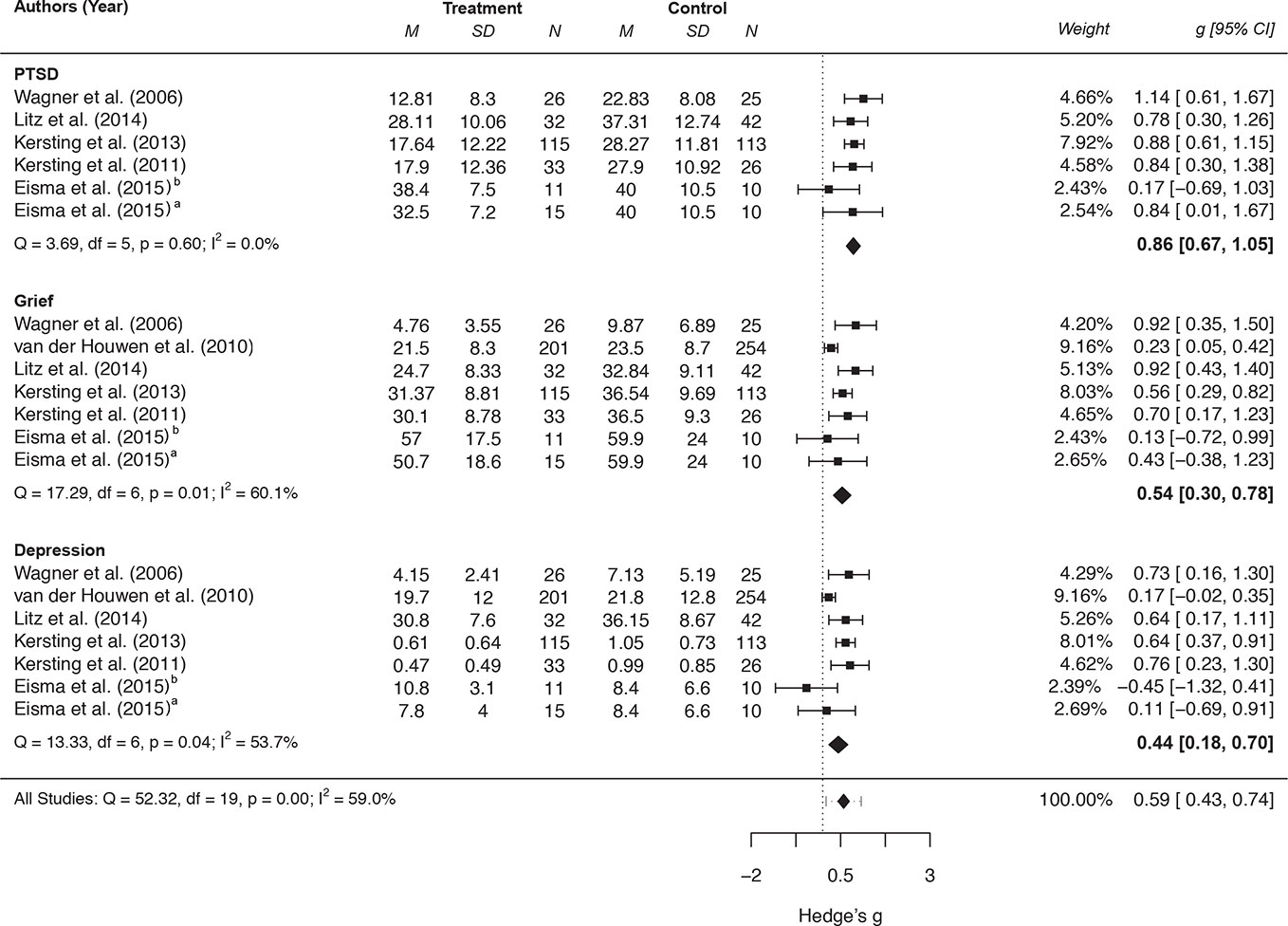
Figure 2 Forest plot of between-group effect sizes of internet-based interventions for PGD, depression and PTSD symptoms. aComparison between Exposure-based treatment and waitlist control group. bComparison between Behavioral activation and waitlist control group.
All effects remained stable from post-assessment to follow-up (3 months) with low (depression) to moderate (grief, PTSD) heterogeneity between the studies: (a) grief: k = 7, Hedge's g = 0.17, 95% CI [−0.03, 0.36], p = .094, I2 = 34.1%, Q(6) = 7.69, p = .261, (b) PTSD: k = 6, Hedge's g = 0.17, 95% CI [−0.06, 0.40], p = .154, I2 = 27.1%, Q(5) = 5.85, p = .321, and (c) depression: k = 7, Hedge's g = 0.07, 95% CI [−0.07, 0.20], p = .324, I2 <.01%, Q(6) = 1.54, p = .957.
There were only two moderators with a significant impact on the ESs (ps < 0.05, Table 5) and significantly reduced heterogeneity at post-assessment: A higher number of therapeutic sessions were associated with a higher ES for grief, and more individual feedback increased the ES for depression.
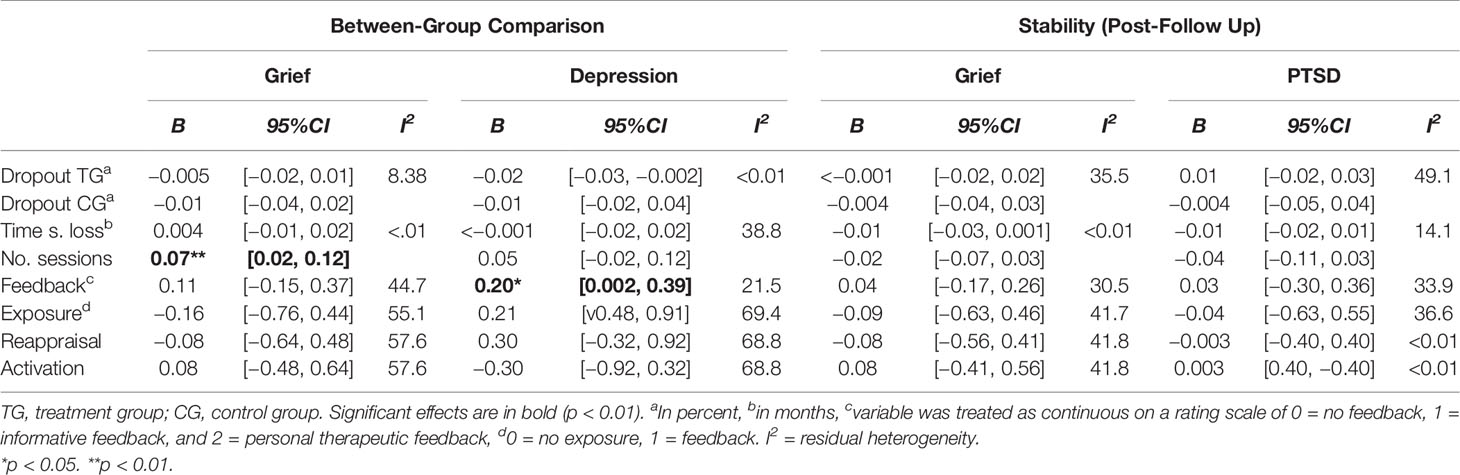
Table 5 Meta-regressions to test for the influence of moderators in models with moderate to high heterogeneities.
Potential outliers for all outcomes were detected using influential case diagnostics (see Supplementary Table 2) Viechtbauer and Cheung (64), which marked two studies: van der Houwen et al., (47) at post-assessment (grief and depression) and Kersting et al. (45) at follow-up (grief and PTSD). While the results did not substantially change after recalculating the meta-analyses without Kersting et al.'s study, the ESs increased to a moderate degree and the heterogeneities decreased to zero after recalculating the analyses without van der Houwen et al.'s study (see Supplementary Table 3) (65). Publication bias was not inspected because the analysis included fewer than 10 studies and heterogeneity was often greater than 10 (66).
Discussion
The present review systematically evaluated the efficacy of web-based bereavement care interventions for bereaved people with higher levels of disturbed grief, based on seven RCTs using active or waitlist control groups. The effects of the web-based interventions on grief reduction were promising with moderate ESs (Hedge's gbetween = 0.54), which was also stable from post to 3-months follow-up assessment. Overall, the results are in line with an earlier review of face-to-face interventions for grief (11) which yielded an effect size of 0.53. However, the most recent review (8) found only small effects for bereavement interventions, particularly when considering publication bias (g = 0.31). One explanation for the diverging results might be that the present review explicitly focused on online interventions while the Johannsen et al. (8) combined face-to-face and online treatments. Another reason might lie in the slightly different definitions of grief and the assessment of its pathological levels. For example, Johannsen et al. (8) included only studies that assessed grief using one of the versions of the ICG-R or PG-13. Facing similar decisions regarding definition and assessment, this review relied on the definitions of prolonged grief that was presented by the original authors of the included studies. With the new ICD-11 criteria and the use of consistent measurements, it should be possible to reduce variance between studies resulting from variance in outcome assessments in the future. Finally, the differences might also be due to different methodological approaches. For example, Johannsen calculated their effect sizes considering pre-post differences while this review based its estimation on postscores. Nonetheless, it is noteworthy that despite these different methodological approaches, the main conclusions from the existing reviews still seem to be comparable: Psychological treatment for pathological grief in general, and based on this review delivered via online-based formats in particular, is effective, but it is not yet as effective as it is in treating online, for example, panic or social anxiety disorders, given the absolute numbers of ESs (67).
The largest and most robust effect, however, was found for grief-related PTSD symptoms (Hedge's gbetween = 0.86) which also remained stable over time. These results are generally in line with research demonstrating the effectiveness of e-mental health approaches in the reduction of PTSD (24, 68). The result that interventions had stronger effects on posttraumatic symptoms than on prolonged grief had already been noted previously (8) but still needs clarification. One reason could be that the disturbed grief and PTSD have “less clear boundaries” (6, p. 2446). In fact, the majority of the current treatment protocols (i.e., 86% of the included studies) are largely tailored to treat distressing memories that are associated with the loss and reduce avoidance using exposure-elements. Distressing remembrance is a cluster that shows the largest overlap between PCBD and PTSD (6). Thus, the current treatment protocols might address mutual grief and posttraumatic stress symptoms more than they address the specific symptoms of prolonged grief [i.e., role confusion, meaninglessness, and loneliness; (6)].
The weakest effect was found for depression (Hedge's gbetween = 0.44), which is still comparable to the effects of general internet-based treatments for depression [(69–71); but see e.g., (72) for larger effects] and the effects of general PGD interventions for secondary depression outcomes (8). There might be two reasons for the smaller effects on depression. First, there was high heterogeneity in our results that might partly be explained by the variability in the extent of therapeutic feedback. As our moderator analyses showed, studies with more personal feedback were more likely to report higher ESs for depression. Previous studies also reported that individualized internet interventions achieve higher outcomes compared to pure self-help or no guided tools (73). However, because our meta-regressions were somewhat underpowered, we interpret the results for depression cautiously with the outlook that more studies are needed to disentangle the associations between interventions, depression, and feedback. Second, given that major depression and PCBD are more distinct categories than PTSD and PBCD (6), the comparably smaller ESs might reflect the narrow focus of current treatment protocols to grief and not depression. However, because there is still overlap between both diagnoses with respect to, for example, worthlessness and guilt, the applied treatment concepts might still address some parts of depressive symptoms. Again, Johannsen et al. (8) also found no significant effect of bereavement treatments on depression and hypothesized that there might be no “spill-over effect of grief interventions on other psychological morbidities” (p. 78). This raises the question what kind of treatment ingredients are currently missing in treatment protocols that would address depressive symptoms more directly. Eisma et al. (43) examined a pure behavioral activation module but did not yield sufficient ES for depression. However, it would be interesting to combine writing assignments using exposure and cognitive reappraisal [e.g., based on the approach by (50)] with behavioral activation.
Considering the attrition rates of the reviewed treatments, our results showed that, generally, the average attrition rate of 27% is comparable with other internet-based treatment studies (74). However, one interesting finding was the wide range of dropout rates between the treatment groups (i.e., 10 to 58%). One factor that might contribute to this range could be the degree of guidance and personal feedback, because the highest dropout rates were found in treatments that offered only informative feedback (43, 47). These studies also mentioned that some participants dropped out because the intervention was “too impersonal”, or that the “treatment did not help”, “was too difficult”, or that they had “no confidence” in it [(43), p. 5; 47, p. 362]. The behavioral activation group in Eisma et al.'s study, for example, had the highest dropout rate, which might further point to difficulties that are associated with implementing behavioral changes by oneself. In addition, the average dropout rate for studies providing informative feedback was 41% (SD = 17) and only 17% (SD = 15) for studies providing personal feedback. Previous research suggested the importance of guidance in internet-based interventions for their efficacy and its superiority on adherence over completely unguided interventions (75, 76). This does not necessarily mean that the treatment concepts are ineffective but that additional factors (i.e., guidance) are needed to facilitate change. The results of the outlier analysis similarly point to this direction, because, after excluding van der Houwen et al.'s study, heterogeneity between the studies was reduced and the ESs for grief and depression rose to a moderate level. This study applied writing assignments including exposure and reappraisal elements. Both seemed to be effective in the other included studies, but the intervention was very short (i.e., five sessions) and dispensed with personal feedback. Thus, the dropout rate was high.
Similar to the range of dropouts, there was a large range between the number of sessions across studies (i.e., five to 18). The moderator analyses showed that a higher number of treatment sessions were associated with higher effect sizes for grief. It is noticeable that the interventions with the highest dropout rates (43, 47) also had the lowest number of sessions (i.e., six and five) and the lowest personal support. Again, this finding might also add to the hypothesis that participants suffering from PGD need more personal support over a longer period of time.
In sum, the interpretation of the present results on web-based bereavement care are mostly in line with previous research on face-to-face treatments: While online treatment is largely effective in treating PTSD symptoms, its effect on grief symptoms themselves is comparably lower, although moderate and stable over time. The effects on depression, however, are less clear and tend to be small.
Limitations
A number of limitations of this review need to be addressed. First, only a small number of studies could be included in this review. E-mental health for the bereaved is still in its infancy, and further randomized controlled trials are needed. Although we reached the required number of at least seven studies to achieve adequate power, the number of included studies varied depending on the specific comparison and outcome (i.e. for meta-regressions). Also, not all studies included 20 participants per study group (43). It remains unclear whether the nonsignificant results for study characteristics (e.g. influence of exposure vs. no exposure) are true effects or whether our analyses were underpowered (42, 77).
Second, because all interventions were based on CBTs and almost all used exposure modules, we cannot make specific conclusions about their effectiveness compared to other treatment approaches. Nonetheless, they seem promising, since memories of the death and its circumstances are often experienced as very distressful and are therefore avoided. In line with this assumption is the rationale and effectiveness of face-to-face exposure-based treatments for PTSD (78) and PGD symptoms (15, 79). Interestingly, Eisma et al.'s (43) behavioral activity intervention did not reveal significant effects on grief-related PTSD, but the exposure group did. However, because of the very small sample sizes in each group (11 vs. 10 participants at the post assessment) and because of the significant baseline differences, the results were not considered in the effect size calculations for this review.
Third, the fact that in most studies, different types of losses were addressed (e.g. parental loss, bereaved parents, suicide bereavement) complicates the process of reaching a reliable conclusion.
Finally, this group of bereaved people included in this meta-analysis might not reflect the naturalistic setting in the treatment of clients with disturbed grief symptoms who are traditionally looking for help in self-help groups and who might additionally suffer from comorbid disorders, increased suicidality, and alcohol and substance abuse. Consequently, effectiveness studies should be conducted to provide better knowledge about the generalization of previous results from randomized controlled trials.
Future Directions and Practical Implications
Since this review included all studies that measured PGD symptoms on a continuous scale, future studies might address PGD diagnosed according to one validated sound diagnostic criterion. Further, the identification of relevant moderators, such as symptom severity, type of loss, length of treatment, and amount of therapist support is needed to improve treatment outcomes from web-based interventions. Further, randomized controlled trials should involve active control groups, such as face-to-face groups or self-help interventions and compare writing assignments directly to other online-approaches.
Generally, there is a great need to understand the help-seeking patterns of bereaved people depending on gender, type of loss (e.g. suicide, illness), age group (e.g. adolescents, the elderly), and relationship to the deceased (e.g. child, parent, sibling). Further, dismantling studies should be conducted as well as blended care interventions, which could include internet-based interventions in existing psychosocial support (e.g. self-help groups). A challenging task might be the inclusion and treatment of less-educated participants in internet-based interventions because, so far, they are reaching a better-educated group of people (80).
In addition, future research studies should examine the underlying mechanisms of effective treatments. For example, it is worth mentioning that all interventions [except the behavioral activation group in (43)] included extensive structured writing assignments, which might be one promising treatment approach that is applicable to both, online and face-to-face interventions. A number of previous studies showed that expressive writing assignments on specific bereavement-related themes can be effective in reducing the symptoms of PGD (81) because it enhances deep reflection on the loss, leads to new perspectives, or supports the process of sense-making (82). Only recently, Sloan and colleagues (83) compared a five session written exposure intervention with cognitive processing therapy (CPT), a first line treatment approach for PTSD. The results indicate that the written exposure intervention was equally effective as CPT in trauma-related symptom reductions. Expressive writing might enhance a deep reflection on the loss or the traumatic experience and might help to develop a narrative of it. The emotional processing during writing might finally lead to new perspectives that are perceived as less threatening. Further, writing might support the process of sense-making and relieve the distressed mourner (82). Taken together, the positive treatment effect of the analyzed internet-based interventions could be largely due to the written tasks. Hence, written assignments that foster self-disclosure and reduce avoidance seem worth considering in future online-interventions as well.
This review offers some practical implications. First, internet-based interventions are a promising alternative to treat PGD when face-to-face encounters are not possible or wanted. Because all reviewed interventions were based on CBT and mostly used writing assignments based on the Pennebaker paradigm (49), there seems to be evidence that clinicians can implement these structured writing approaches in their clinical practice. The main elements hereby are the examination of distressing remembrance using exposure elements, and cognitive restructuring of grief-related dysfunctional thoughts, as well as the integration and restoration (i.e., development of new goals for the future). Although more research is still necessary to improve internet-based treatments for PGD, clinicians might pay special attention to very specific grief- and depression-related symptoms in addition to posttraumatic stress symptoms. Further, it seems advisable to offer online programs that are not too short (i.e., >6 sessions) and to provide personal feedback and guidance to avoid frustration and early dropout.
In conclusion, the results suggest that internet-based treatments, based on CBT, can help to reduce the symptoms related to the loss of a significant person in a relatively short time. Yet, more qualitative RCTs with adequate power on that topic are needed.
Data Availability Statement
The data that support the findings of this study are openly available in Open Science Framework at https://osf.io/7re5m/?view_only=66a8043dfe644b4699d619e03ee10c76.
Author Contributions
BW: substantial contribution to the conception, drafting the work, and revising it critically for important intellectual content; final approval of the version to be published. UM: substantial contribution to every aspect of the manuscript, critical revision, interpretation of the data, and final approval and agrees to be accountable. LH: substantial contribution to interpretation of data, critical revision, and final approval and agrees to be accountable. NR: Initial substantial contribution to the conception and design of the work.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2020.00525/full#supplementary-material
Footnotes
- ^ Wagner et al. (18) report ESs for two IES subscales (i.e. Intrusion and Avoidance), which were combined into one ES for PTSD symptoms on the basis of a correlation of r = .59 (42, 53).
References
1. Prigerson HG, Horowitz MJ, Jacobs SC, Parkes CM, Aslan M, Goodkin K, et al. Prolonged grief disorder: Psychometric validation of criteria proposed for DSM-V and ICD-11. PloS Med (2009) 6(8):e1000121. doi: 10.1371/journal.pmed.1000121
2. Association AP. Diagnostic and statistical manual of mental disorders (DSM-5®) Washington D.C.: American Psychiatric Pub. (2013).
3. World Health Organization. (2019). International Statistical Classification of Diseases and Related Health Problems, 11 ed. Retrieved from https://icd.who.int/browse11/l-m/en
4. Boelen PA, Lenferink LIM. Comparison of six proposed diagnostic criteria sets for disturbed grief. Psychiatry Res (2020) 285:112786. doi: 10.1016/j.psychres.2020.112786
5. Comtesse H, Vogel A, Kersting A, Rief W, Steil R, Rosner R. When does grief become pathological? Evaluation of the ICD-11 diagnostic proposal for prolonged grief in a treatment-seeking sample. Eur J Psychotraumatol (2020) 11(1):1694348. doi: 10.1080/20008198.2019.1694348
6. Malgaroli M, Maccallum F, Bonanno GA. Symptoms of persistent complex bereavement disorder, depression, and PTSD in a conjugally bereaved sample: a network analysis. psychol Med (2018) 48(14):2439–48. doi: 10.1017/S0033291718001769
7. Allumbaugh DL, Hoyt WT. Effectiveness of grief therapy: A meta-analysis. J Couns Psychol (1999) 46(3):370. doi: 10.1037/0022-0167.46.3.370
8. Johannsen M, Damholdt MF, Zachariae R, Lundorff M, Farver-Vestergaard I, O'Connor M. Psychological interventions for grief in adults: A systematic review and meta-analysis of randomized controlled trials. J Affect Disord (2019) 253:69–86. doi: 10.1016/j.jad.2019.04.065
9. Kato PM, Mann T. A synthesis of psychological interventions for the bereaved. Clin Psychol Rev (1999) 19(3):275–96. doi: 10.1016/S0272-7358(98)00064-6
10. Neimeyer RA. Searching for the meaning of meaning: grief therapy and the process of reconstruction. Death Stud (2000) 24(6):541–58. doi: 10.1080/07481180050121480
11. Wittouck C, Van Autreve S, De Jaegere E, Portzky G, van Heeringen K. The prevention and treatment of complicated grief: a meta-analysis. Clin Psychol Rev (2011) 31(1):69–78. doi: 10.1016/j.cpr.2010.09.005
12. Currier JM, Neimeyer RA, Berman JS. The effectiveness of psychotherapeutic interventions for bereaved persons: a comprehensive quantitative review. Psycholical Bull (2008) 134(5):648–61. doi: 10.1037/0033-2909.134.5.648
13. Andriessen K, Krysinska K, Hill NTM, Reifels L, Robinson J, Reavley N, et al. Effectiveness of interventions for people bereaved through suicide: a systematic review of controlled studies of grief, psychosocial and suicide-related outcomes. BMC Psychiatry (2019) 19(1):49. doi: 10.1186/s12888-019-2020-z
14. Schut H, Stroebe MS, van den Bout J, Terheggen M. The efficacy of bereavement interventions: Determining who benefits. In: . Handbook of bereavement research: Consequences, coping, and care. Washington, DC, US: American Psychological Association (2001). p. 705–37.
15. Boelen PA, de Keijser J, van den Hout MA, van den Bout J. Treatment of complicated grief: a comparison between cognitive-behavioral therapy and supportive counseling. J Consult. Clin Psychol (2007) 75(2):277. doi: 10.1037/0022-006X.75.2.277
16. Rosner R, Lumbeck G, Geissner E. Effectiveness of an inpatient group therapy for comorbid complicated grief disorder. Psychother Res (2011) 21(2):210–8. doi: 10.1080/10503307.2010.545839
17. Shear MK, Frank E, Houck PR, Reynolds CF. Treatment of complicated grief: a randomized controlled trial. JAMA (2005) 293(21):2601–8. doi: 10.1001/jama.293.21.2601
18. Wagner B, Knaevelsrud C, Maercker A. Internet-based cognitive-behavioral therapy for complicated grief: a randomized controlled trial. Death Stud (2006) 30(5):429–53. doi: 10.1080/07481180600614385
19. Currow DC, Allen K, Plummer J, Aoun S, Hegarty M, Abernethy AP. Bereavement help-seeking following an ‘expected' death: a cross-sectional randomised face-to-face population survey. BMC Palliat. Care (2008) 7, 19. doi: 10.1186/1472-684X-7-19
20. Andriessen K, Lobb E, Mowll J, Dudley M, Draper B, Mitchell PB. (2018). Help-seeking experiences of bereaved adolescents: A qualitative study. Death studies. pp. 1–8. doi: 10.1080/07481187.2018.1426657
21. Lichtenthal WG, Corner GW, Sweeney CR, Wiener L, Roberts KE, Baser RE, et al. Mental Health Services for Parents Who Lost a Child to Cancer: If We Build Them, Will They Come? J Clin Oncol (2015) 33(20):2246–53. doi: 10.1200/JCO.2014.59.0406
22. Pitman AL, Osborn D, Rantell K, King M. The stigma perceived by people bereaved by suicide and other sudden deaths: A cross-sectional UK study of 3432 bereaved adults. J Psychosom. Res (2016) 87:22–9. doi: 10.1016/j.jpsychores.2016.05.009
23. Andersson G, Cuijpers P, Carlbring P, Riper H, Hedman E. Guided Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: a systematic review and meta-analysis. World Psychiatry (2014) 13(3):288–95. doi: 10.1002/wps.20151
24. Kuester A, Niemeyer H, Knaevelsrud C. Internet-based interventions for posttraumatic stress: A meta-analysis of randomized controlled trials. Clin Psychol Rev (2016) 43:1–16. doi: 10.1016/j.cpr.2015.11.004
25. Sijbrandij M, Kunovski I, Cuijpers P. Effectiveness of Internet-Delivered Cognitive Behavioral Therapy for Posttraumatic Stress Disorder: A Systematic Review and Meta-Analysis. Depress Anxiety (2016) 33(9):783–91. doi: 10.1002/da.22533
26. Andersson G. Internet-based cognitive-behavioral self-help for depression. Expert Rev Neurother (2006) 6(11):1637–42. doi: 10.1586/14737175.6.11.1637
27. Andersson G, Topooco N, Havik O, Nordgreen T. Internet-supported versus face-to-face cognitive behavior therapy for depression. Expert Rev Neurother (2016) 16(1):55–60. doi: 10.1586/14737175.2015.1125783
28. Johansson R, Andersson G. Internet-based psychological treatments for depression. Expert Rev Neurother (2012) 12(7):861–869; quiz 870. doi: 10.1586/ern.12.63
29. Ruwaard J, Schrieken B, Schrijver M, Broeksteeg J, Dekker J, Vermeulen H, et al. Standardized web-based cognitive behavioural therapy of mild to moderate depression: a randomized controlled trial with a long-term follow-up. Cognit Behav Ther (2009) 38(4):206–21. doi: 10.1080/16506070802408086
30. Spek V, Cuijpers PIM, Nyklicek I, Riper H, Keyzer J, Pop V. Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: a meta-analysis. psychol Med (2006) 37(03):319–28. doi: 10.1017/S0033291706008944
31. Wagner B, Horn AB, Maercker A. Internet-based versus face-to-face cognitive-behavioral intervention for depression: a randomized controlled non-inferiority trial. J Affect Disord (2014) 152-154:113–21. doi: 10.1016/j.jad.2013.06.032
32. Pitman AL, Rantell K, Moran P, Sireling L, Marston L, King M, et al. Support received after bereavement by suicide and other sudden deaths: a cross-sectional UK study of 3432 young bereaved adults. BMJ Open (2017) 7(5):e014487. doi: 10.1136/bmjopen-2016-014487
33. Shear MK, Simon N, Wall M, Zisook S, Neimeyer R, Duan N, et al. Complicated grief and related bereavement issues for DSM-5. Depression Anxiety (2011) 28(2):103–17. doi: 10.1002/da.20780
34. Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PloS Med (2009) 6(7):e1000097. doi: 10.1371/journal.pmed.1000097
36. Van Tulder M, Furlan A, Bombardier C, Bouter L, Editorial Board of the Cochrane Collaboration Back Review group. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine (2003) 28(12):1290–9. doi: 10.1097/01.BRS.0000065484.95996.AF
37. RStudio Team. (2016). RStudio: Integrated Development for R: RStudio, Inc., Boston, MA URLhttp://www.rstudio.com/.
38. Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. (2010) 36(3):1–48. doi: 10.18637/jss.v036.i03
41. Crombie IK, Davies HT. What is meta-analysis. What is (2009), Hayward Medical Communications, s division of Hayward Group Ltd. 1–8. Retrieved from http://www.bandolier.org.uk/painres/download/whatis/Meta-An.pdf
42. Borenstein M, Hedges LV, Higgins JP, Rothstein HR. Introduction to meta-analysis. Chichester: John Wiley & Sons. (2011).
43. Eisma MC, Boelen PA, van den Bout J, Stroebe W, Schut H, Lancee J, et al. Internet-Based Exposure and Behavioral Activation for Complicated Grief and Rumination: A Randomized Controlled Trial. Behav Ther (2015) 46(6):729–48. doi: 10.1016/j.beth.2015.05.007
44. Wagner B, Maercker A. A 1.5-year follow-up of an Internet-based intervention for complicated grief. J Trauma Stress (2007) 20(4):625–9. doi: 10.1002/jts.20230
45. Kersting A, Dolemeyer R, Steinig J, Walter F, Kroker K, Baust K, et al. Brief Internet-based intervention reduces posttraumatic stress and prolonged grief in parents after the loss of a child during pregnancy: a randomized controlled trial. Psychother Psychosom. (2013) 82(6):372–81. doi: 10.1159/000348713
46. Kersting A, Kroker K, Schlicht S, Baust K, Wagner B. Efficacy of cognitive behavioral internet-based therapy in parents after the loss of a child during pregnancy: pilot data from a randomized controlled trial. Arch Women's Ment Health (2011) 14(6):465–77. doi: 10.1007/s00737-011-0240-4
47. van der Houwen K, Schut H, van den Bout J, Stroebe MS, Stroebe W. The efficacy of a brief internet-based self-help intervention for the bereaved. Behav Res Ther (2010) 48(5):359–67. doi: 10.1016/j.brat.2009.12.009
48. Litz BT, Schorr Y, Delaney E, Au T, Papa A, Fox AB, et al. A randomized controlled trial of an internet-based therapist-assisted indicated preventive intervention for prolonged grief disorder. Behav Res Ther (2014) 61:23–34. doi: 10.1016/j.brat.2014.07.005
49. Prigerson HG, Jacobs SC. Traumatic grief as a distinct disorder: A rationale, consensus criteria, and a preliminary empirical test. In: Stroebe MS, Hansson RO, Stroebe W, Schut H, editors. Handbook of bereavement research: Consequences, coping, and care. Washington DC, US: American Psychological Association (2001). p. 613–45.
50. Prigerson HG, Maciejewski PK, Reynolds CF 3rd, AJ B, JT N, Fasiczka A, et al. Inventory of Complicated Grief: A scale to measure maladaptive symptoms of loss. Psychiatry Res (1995) 59(1–2):65–79.
51. Foa EB, Cashman L, Jaycox L, Perry K. The validation of a self-report measure of posttraumatic stress disorder: The Posttraumatic Diagnostic Scale. Psychol Assess (1997) 9(4):445. doi: 10.1037/1040-3590.9.4.445
52. Horowitz M, Wilner N, Alvarez W. Impact of Event Scale: A measure of subjective stress. Psychosom Med (1979) 41(3):209–18. doi: 10.1097/00006842-197905000-00004
53. Maercker A, Schützwohl M. Erfassung von psychischen Belastungsfolgen: Die Impact of Event Skala-revidierte Version (IES-R). Diagnostica (1998). 44: 130–41. doi: 10.1037/t55092-000
54. Weathers FW, Litz BT, Herman D, Huska J, Keane T. The PTSD checklist-civilian version (PCL-C). Boston, MA: National Center for PTSD (1994).
55. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand (1983) 67(6):361–70.
56. Derogatis LR. Brief Symptom Inventory (BSI): Administration, scoring, and procedures manual. Minneapolis: National Computer Systems (NCS) (1993).
57. Beck AT, Steer RA, Brown GK. Manual for the BDI-II. San Antonio, TX: Psychological Corporation (1996).
58. Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas (1977) 1(3):385–401. doi: 10.1177/014662167700100306
59. Langner R, Maercker A. Complicated grief as a stress response disorder: Evaluating diagnostic criteria in a German sample. J Psychosom Res (2005) 58(3):235–42. doi: 10.1016/j.jpsychores.2004.09.012
60. Lejuez CW, Hopko DR, Acierno R, Daughters SB, Pagoto SL. Ten Year Revision of the Brief Behavioral Activation Treatment for Depression: Revised Treatment Manual. Behav Modification (2011) 35(2):111–61. doi: 10.1177/0145445510390929
61. Lange A, Rietdijk D, Hudcovicova M, van de Ven J-P, Schrieken B, Emmelkamp PMG. Interapy: A controlled randomized trial of the standardized treatment of posttraumatic stress through the internet. J Consult Clin Psychol (2003) 71(5):901–09. doi: 10.1037/0022-006X.71.5.901
62. Pennebaker JW. Writing about emotional experiences as a therapeutic process. psychol Sci (1997) 8(3):162–6. doi: 10.1111/j.1467-9280.1997.tb00403.x
63. Lange A, Schoutrop M, Schrieken B, van de Ven J-P. Interapy: a model for therapeutic writing through the Internet. In: Lepore SJ, Smyth JM, editors. The writing cure: How expressive writing promotes health and emotional well-being. Washington, DC, US: American Psychological Association (2002). p. 215–38.
64. Viechtbauer W, Cheung MW. Outlier and influence diagnostics for meta-analysis. Res Synth. Methods (2010) 1(2):112–25. doi: 10.1002/jrsm.11
65. Niemeyer H, Musch J, Pietrowsky R. Publication bias in meta-analyses of the efficacy of psychotherapeutic interventions for depression. J Consult Clin Psychol (2013) 81(1):58–74. doi: 10.1037/a0031152
66. Higgins JPT, Green S eds. Cochrane Handbook for Systematic Reviews of Interventions Version 5. 1. 0. [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org
67. Andrews G, Basu A, Cuijpers P, Craske MG, McEvoy P, English CL, et al. Computer therapy for the anxiety and depression disorders is effective, acceptable and practical health care: an updated meta-analysis. J Anxiety Disord (2018) 55:70–8. doi: 10.1016/j.janxdis.2018.01.001
68. Sloan DM, Gallagher MW, Feinstein BA, Lee DJ, Pruneau GM. Efficacy of telehealth treatments for posttraumatic stress-related symptoms: a meta-analysis. Cognit Behav Ther (2011) 40(2):111–25. doi: 10.1080/16506073.2010.550058
69. Cowpertwait L, Clarke D. Effectiveness of web-based psychological interventions for depression: a meta-analysis. Int J Ment Health Addict (2013) 11(2):247–68. doi: 10.1007/s11469-012-9416-z
70. Richards D, Richardson T. Computer-based psychological treatments for depression: a systematic review and meta-analysis. Clin Psychol Rev (2012) 32(4):329–42. doi: 10.1016/j.cpr.2012.02.004
71. So M, Yamaguchi S, Hashimoto S, Sado M, Furukawa TA, McCrone P. Is computerised CBT really helpful for adult depression?-A meta-analytic re-evaluation of CCBT for adult depression in terms of clinical implementation and methodological validity. BMC Psychiatry (2013) 13(1):113. doi: 10.1186/1471-244X-13-113
72. Sztein DM, Koransky CE, Fegan L, Himelhoch S. Efficacy of cognitive behavioural therapy delivered over the Internet for depressive symptoms: A systematic review and meta-analysis. J Telemed. Telecare (2018) 24(8):527–39. doi: 10.1177/1357633X17717402
73. Andersson G, Cuijpers P. Internet-based and other computerized psychological treatments for adult depression: a meta-analysis. Cogn Behav Ther (2009) 38(4):196–205. doi: 10.1080/16506070903318960
74. Melville KM, Casey LM, Kavanagh DJ. Dropout from Internet-based treatment for psychological disorders. Br J Clin Psychol (2010) 49(4):455–71. doi: 10.1348/014466509X472138
75. Baumeister H, Reichler L, Munzinger M, Lin J. The impact of guidance on Internet-based mental health interventions—A systematic review. Internet Interventions (2014) 1(4):205–15. doi: 10.1016/j.invent.2014.08.003
76. Domhardt M, Geßlein H, von Rezori RE, Baumeister H. Internet- and mobile-based interventions for anxiety disorders: A meta-analytic review of intervention components. Depression Anxiety (2019) 36(3):213–24. doi: 10.1002/da.22860
77. Hempel S, Miles JN, Booth MJ, Wang Z, Morton SC, Shekelle PG. Risk of bias: a simulation study of power to detect study-level moderator effects in meta-analysis. Syst. Rev (2013) 2(1):107. doi: 10.1186/2046-4053-2-107
78. Bradley R, Greene J, Russ E, Dutra L, Westen D. A multidimensional meta-analysis of psychotherapy for PTSD. Am J Psychiatry (2005) 162(2):214–27. doi: 10.1176/appi.ajp.162.2.214
79. Bryant RA, Kenny L, Joscelyne A, Rawson N, Maccallum F, Cahill C, et al. Treating prolonged grief disorder: a randomized clinical trial. JAMA Psychiatry (2014) 71(12):1332–9. doi: 10.1001/jamapsychiatry.2014.1600
80. Lampe LA. Internet-based therapy: too good to be true? Aust New Z J Psychiatry (2011) 45(4):342–3. doi: 10.3109/00048674.2011.560138
81. Kalantari M, Yule W, Dyregrov A, Neshatdoost H, Ahmadi S. Efficacy of writing for recovery on traumatic grief symptoms of Afghani refugee bereaved adolescents: A randomized control trial. OMEGA-J. Death Dying (2012) 65(2):139–50. doi: 10.2190/OM.65.2.d
82. Lichtenthal WG, Cruess DG. Effects of directed written disclosure on grief and distress symptoms among bereaved individuals. Death Stud (2010) 34(6):475–99. doi: 10.1080/07481187.2010.483332
Keywords: grief, bereavement, depression, post-traumatic stress disorder, Internet, e-health, intervention, psychotherapy
Citation: Wagner B, Rosenberg N, Hofmann L and Maass U (2020) Web-Based Bereavement Care: A Systematic Review and Meta-Analysis. Front. Psychiatry 11:525. doi: 10.3389/fpsyt.2020.00525
Received: 24 February 2020; Accepted: 22 May 2020;
Published: 24 June 2020.
Edited by:
Roumen Milev, Queen's University, CanadaReviewed by:
Rolf J. Kleber, Utrecht University, NetherlandsNazanin Alavi, Queen's University, Canada
Copyright © 2020 Wagner, Rosenberg, Hofmann and Maass. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Birgit Wagner, YmlyZ2l0LndhZ25lckBtZWRpY2Fsc2Nob29sLWJlcmxpbi5kZQ==