 Michał Lis1Bartłomiej Stańczykiewicz2
Michał Lis1Bartłomiej Stańczykiewicz2 Lilla Pawlik-Sobecka2Agnieszka Samochowiec3
Lilla Pawlik-Sobecka2Agnieszka Samochowiec3 Artur Reginia4
Artur Reginia4 Błażej Misiak5*
Błażej Misiak5*- 1Clinical Department of Internal Diseases, Endocrinology and Diabetology, The Central Clinical Hospital of the Ministry of the Interior in Warsaw, Warsaw, Poland
- 2Department of Nervous System Diseases, Wroclaw Medical University, Wrocław, Poland
- 3Department of Clinical Psychology, Institute of Psychology, University of Szczecin, Szczecin, Poland
- 4Department of Psychiatry, Pomeranian Medical University, Szczecin, Poland
- 5Department of Genetics, Wroclaw Medical University, Wrocław, Poland
It has been found that antipsychotic-naïve patients with first-episode psychosis (FEP) present with impaired hormonal regulation of appetite in terms of low leptin and high insulin levels (the adipoinsular axis). These findings imply that certain intrinsic mechanisms might play a role in the development of metabolic dysregulation in early psychosis. However, clinical correlates of this phenomenon remain unknown. Moreover, these alterations have not been tested in individuals at familial high risk of psychosis (FHR-P). In this study we aimed to assess the levels of adiponectin, insulin, leptin, glucose, total cholesterol, lipoproteins and triglycerides in FEP patients, unaffected offspring of schizophrenia patients (FHR-P individuals) and healthy controls (HCs) with respect to cognitive performance and psychopathological manifestation. Participants were 35 FEP patients, 33 FHR-P individuals, and 32 HCs. Cognitive performance was assessed using the Repeatable Battery for Assessment of Neuropsychological Status (RBANS). The levels of leptin and high-density lipoproteins (HDL) were significantly lower (leptin: 10.7 ± 15.7 vs. 12.6 ± 10.1, p = 0.046, and HDL: 48.0 ± 16.9 vs. 59.8 ± 17.5 mg/dl, p = 0.007), while the levels of triglycerides and insulin were significantly higher (triglycerides: 137.4 ± 58.8 vs. 77.5 ± 33.2 mg/dl, p < 0.001, and insulin: 15.2 ± 13.1 vs. 9.6 ± 5.0 µIU/ml, p = 0.023) in FEP patients compared to HCs. These differences were significant after controlling for the effects of potential confounding factors. No significant differences in the levels of serum markers between FHR-P individuals and HCs were found. There was a significant negative correlation between the level of leptin and the RBANS language score after covarying for potential confounding factors in FEP patients (B = –0.226, p = 0.006) but not in other subgroups of participants. Our findings confirm impairment of adipoinsular axis in early psychosis. However, results of our study do not support the hypothesis that familial liability to psychosis might be associated with metabolic dysregulation. Leptin levels might be associated with cognitive deficits in FEP patients. Longitudinal studies of individuals at risk of psychosis are needed to provide insights into causal mechanisms underlying our results.
Introduction
Cardiovascular comorbidities largely contribute to reduced life expectancy in patients with schizophrenia-spectrum disorders (1). Although environmental factors that underlie this phenomenon have been widely recognized, accumulating evidence indicates that certain intrinsic mechanisms might also be relevant. Indeed, antipsychotic-naïve or minimally-medicated patients with first-episode psychosis (FEP) present with a number of cardio-metabolic, immune and the hypothalamic-pituitary-adrenal (HPA) axis dysregulations (2). One of hypotheses beyond these observations states that psychotic disorders and cardiovascular risk factors share overlapping genetic backgrounds (3). However, the role of environmental factors (e.g., unhealthy life style or early-life stress) that act in the premorbid phase of illness cannot be excluded.
Our group performed a systematic review and meta-analysis of studies investigating the levels of appetite-regulating hormones in (FEP) patients (4). We found that patients with FEP present with increased levels of insulin and reduced levels of leptin. Subgroup analysis of antipsychotic-naïve patients confirmed these findings. No significant differences in the levels of other hormones (adiponectin, ghrelin, orexin, resistin, and visfatin) between FEP and healthy controls (HCs) were observed in this meta-analysis. Notably, studies of multiple-episode schizophrenia patients revealed increased levels of leptin and insulin (5). Although our meta-analysis did not demonstrate altered levels of adiponectin in FEP, low adiponectin levels were reported in multiple-episode schizophrenia patients (6). The authors of a recent meta-analysis of studies in this field found that low adiponectin levels in this group of patients might occur as a consequence of antipsychotic treatment (6). Notably, adiponectin is another hormone that regulates secretion of insulin. It has been found that adiponectin not only increases insulin sensitivity but it can also exert antiangiogenic, antiatherogenic and neuroprotective effects (7). Although it has been observed that adiponectin levels might be associated with cognitive performance in the general population, these observations have not been confirmed in patients with schizophrenia (8).
Leptin is a hormone released by white adipose tissue and is able to pass through the blood-brain barrier. It reduces appetite via interactions with receptors located in the arcuate nucleus of the hypothalamus. Moreover, leptin plays an important role in the brain development and may be responsible for learning and memory processes (9). Apart from the hypothalamus, leptin receptors are expressed by neurons of the cerebral cortex, hippocampus, basal ganglia and cerebellum (10, 11). Leptin-deficient mice not only develop extreme obesity and other components of the metabolic syndrome but also show decreased brain weight and cortical volumes (9, 12, 13). There is evidence that leptin suppresses secretion of insulin by central actions and direct effects on pancreatic cells. This peripheral regulation of insulin secretion has been named as the adipoinsular axis (14).
Insulin receptors are expressed by various cells of the central nervous system. The highest concentration of insulin receptors has been found in the olfactory bulb, cerebral cortex, hippocampus, cerebellum, and hypothalamus (15). Notably, insulin resistance has been associated with cognitive impairment in FEP patients (16). There are various mechanisms underlying the effects of central insulin signaling on cognitive performance. Indeed, central insulin plays an important role in maintaining neuronal plasticity (17). More specifically, it has been demonstrated that central insulin is involved in spatial learning and memory processes through its interactions with receptors located in the hippocampus (18). In addition, patients with type 2 diabetes are at risk of cognitive impairment across various domains, including, i.e., attention, learning, memory and executive function (19).
It should be noted that insulin resistance is not the only cardiovascular risk factor associated with cognitive impairment in schizophrenia. A recent meta-analysis revealed that a diagnosis of metabolic syndrome and its single components (hypertension, abdominal obesity, insulin resistance and dyslipidemia) are also related to cognitive deficits (20). However, this meta-analysis included only two studies that investigated the effects of dyslipidemia on cognition in schizophrenia (21, 22). These studies revealed that dyslipidemia is related to impairments of executive function, verbal memory and attention. Dyslipidemia may impact cognitive performance through various mechanisms associated with the injury of the blood-brain barrier and blood vessels as well as increased amyloid deposition (23).
Although there is evidence that subclinical indices of metabolic dysregulation, such as lipid profile disturbances, decreased leptin levels and decreased insulin sensitivity, occur in patients with FEP, it remains unknown whether these alterations are present in unaffected individuals at familial high risk of psychosis (FHR-P). Moreover, clinical correlates of metabolic dysregulation in early psychosis are yet to be established. Therefore, we aimed to compare the levels of glucose, insulin, adiponectin and leptin as well as lipid profile in FEP patients, FHR-P individuals and HCs. In addition, we investigated whether these metabolic parameters are related to psychopathological manifestation and cognitive performance.
Material and Methods
Participants
We enrolled 35 FEP inpatients, 33 FHR-P individuals, and 32 HCs. The group of FHR-P individuals represented unaffected offspring of patients with schizophrenia, who were diagnosed according to the ICD-10 criteria. A diagnosis of FEP was established based on the DSM-IV criteria using the Operational Criteria for Psychotic Illness (OPCRIT) checklist (24). All patients were recruited during their first inpatient treatment and they had a negative history of antipsychotic treatment before admission to the inpatient unit. The following diagnoses were established in FEP patients: schizophrenia, schizoaffective disorder, schizophreniform disorder, brief psychotic disorder, and delusional disorder. In turn, HCs were recruited through advertisements and had a negative family history of psychotic and mood disorders in first- and second-degree relatives. Participants were matched for age, sex, and parental education level (the proxy measure of socioeconomic status). The exclusion criteria were as follows: (1) comorbid neurological disorders; (2) intellectual disability; (3) physical health impairment that might affect biochemical markers measured in the study (diabetes, hypertension, coronary artery disease, autoimmune disorders, inflammatory diseases, endocrine disorders); (4) drug and/or alcohol dependence (except for nicotine) and (5) duration of antipsychotic treatment longer than 30 days. Participants were recruited in two big Polish cities (Wroclaw and Szczecin) in the time period between October, 2016 and December, 2019. The study protocol was approved by the Ethics Committee of Wroclaw Medical University (Poland) and all participants gave a written informed consent.
We used the following measures of psychopathology: the Positive and Negative Syndrome Scale (PANSS) (25), the Hamilton Depression Rating Scale (HDRS) (26), the Young Mania Rating Scale (YMRS) (27), the Global Assessment of Functioning (GAF) (28) and the Social and Occupational Assessment of Functioning (SOFAS) (28). Cognitive performance was recorded using the Repeatable Battery for Assessment of Neuropsychological Status (RBANS) (29). The RBANS includes several tests that are grouped into the following domains: immediate memory (list learning and story memory), visuospatial/constructional functions (figure copy and line orientation), language (picture naming and semantic fluency), attention (digit span and coding), and delayed memory (list recall, list recognition, story memory, and figure recall).
Anthropometric Measures and Biochemical Parameters
All participants underwent physical examination to record the waist-to-hip ratio (WHR) and the body mass index (BMI). Blood samples were collected between 7 a.m. and 9 a.m. after overnight fasting. Subsequently, they were centrifuged to obtain serum samples. Colorimetric methods were used to determine the levels of glucose, total cholesterol, triglycerides and high-density lipoproteins (HDL) in the Konelab 60 analyzer (Argenta). The level of low-density lipoproteins (LDL) was calculated using the Friedewald formula. Electrochemiluminescence analysis was applied to measure the levels of insulin (the Cobas e411 analyzer, Roche). The levels of adiponectin and leptin were determined using the Enzyme-Linked Immunosorbent Assay (ELISA) kits.
Statistics
Bivariate comparisons were performed using the χ2 test (categorical variables) and the Mann-Whitney U test or t-tests (continuous variables). Normality of data distribution was assessed using the Kolmogorov-Smirnov test. The Spearman rank correlation coefficients were used to test bivariate correlations. The analysis of covariance (ANCOVA) was performed to test for between-group differences in metabolic parameters after adjustment for age, sex, BMI, and cigarette smoking status. Similarly, linear regression analysis was performed in case of significant bivariate correlations between the measures of psychopathology or cognitive performance and metabolic parameters. Age, sex, BMI, cigarette smoking status, and chlorpromazine equivalent dosage (CPZeq) were included as covariates. Results were considered statistically significant if the p-value was less than 0.05. All analyses were conducted using the Statistical Package for Social Sciences, version 20 (SPSS Inc., Chicago, Illinois, USA).
Results
General characteristics of the participants were shown in Table 1. There were no significant between-group differences in age, sex, parental education level, BMI, and WHR. As expected, cigarette smoking rates were significantly higher, while the number of education years was significantly lower, in FEP patients. Similarly, patients with FEP scored significantly lower on all domains of cognitive performance compared to HCs or FHR-P individuals (except for visuospatial/constructional abilities). In turn, FHR-P individuals had significantly lower scores of visuospatial/constructional abilities, attention and delayed memory in comparison with HCs.
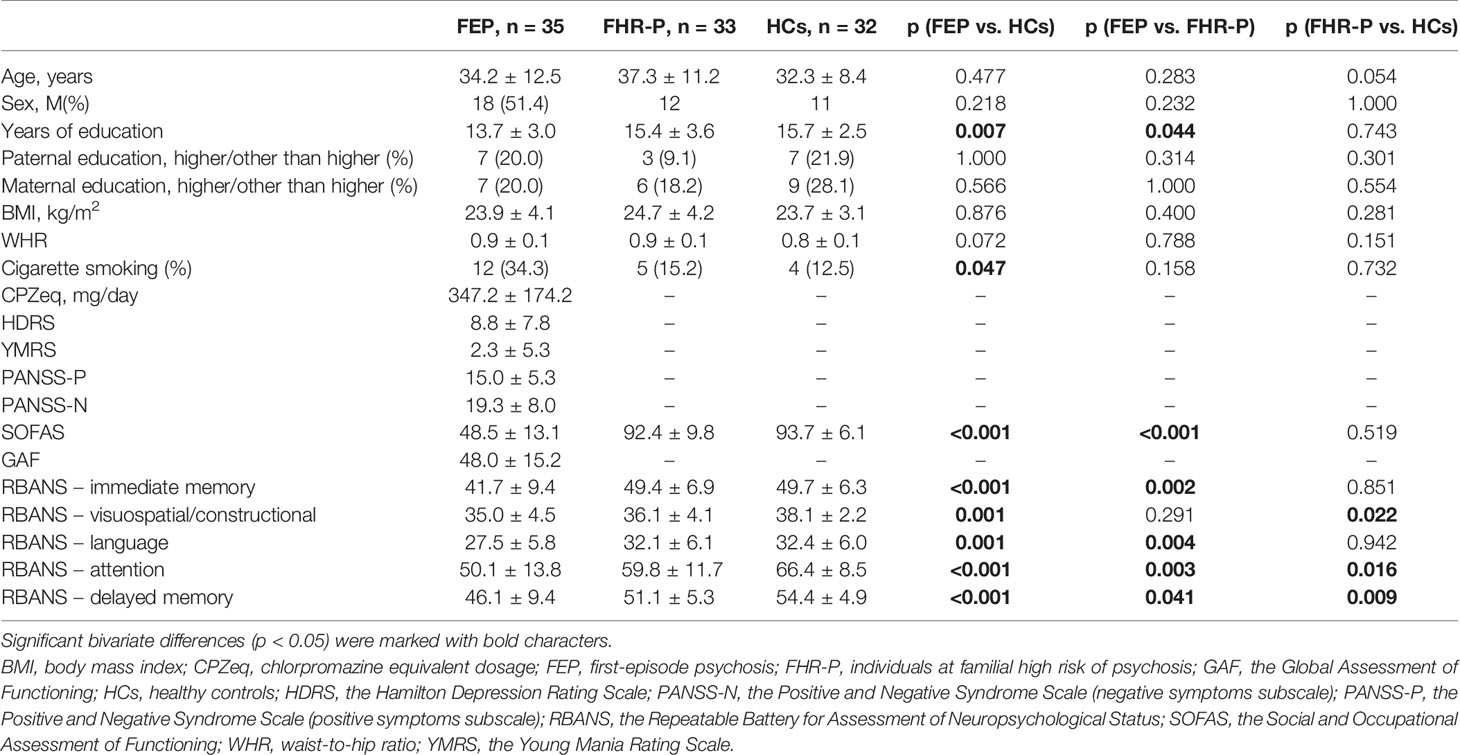
Table 1 General characteristics of participants.
Metabolic parameters in distinct groups of participants were presented in Table 2. Patients with FEP had significantly lower levels of leptin and HDL than HCs. The difference in HDL levels between FEP patients and FHR-P individuals was also significant. In turn, the levels of triglycerides and insulin were significantly higher in FEP patients compared to HCs. Moreover, patients with FEP had significantly higher levels of triglycerides than HCs. These between-group differences remained significant after covarying for age, sex, BMI, and cigarette smoking status (Table 2).
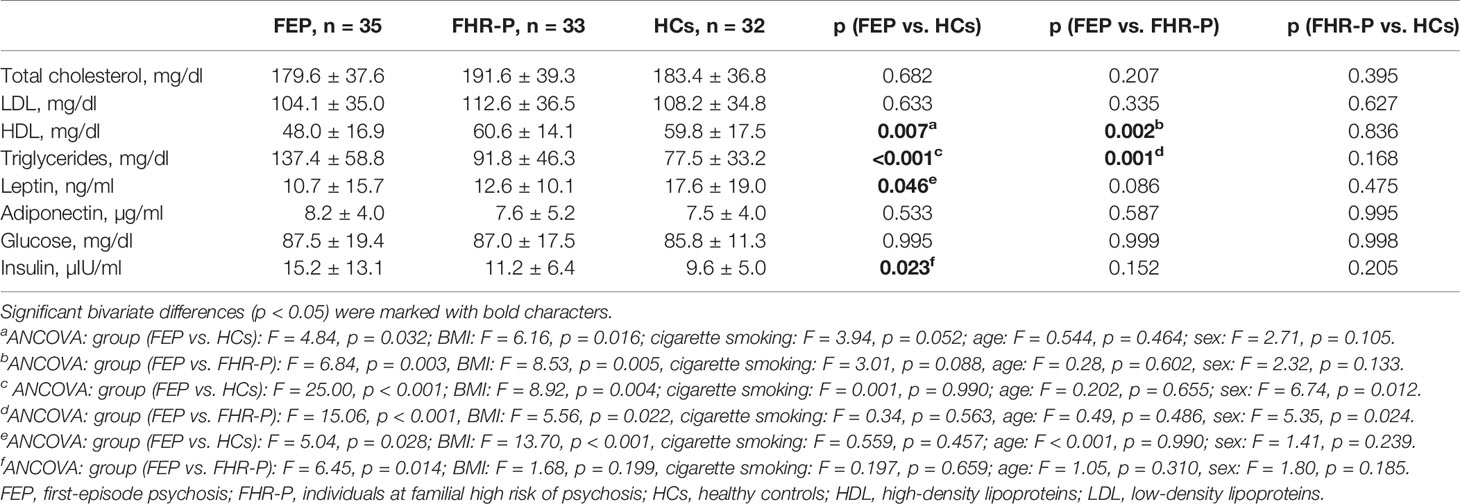
Table 2 Metabolic parameters in FEP patients, FHR-P individuals and HCs.
There were several significant bivariate correlations between metabolic parameters, psychopathological manifestation and cognitive performance, especially in FEP patients (Table 3). However, only a negative correlation between leptin levels and the RBANS language score remained significant (B = −0.226, p = 0.006) in FEP patients after controlling for the effects of age (B = 0.023, p = 0.795), sex (B = 2.221, p = 0.314), BMI (B = −0.071, p = 0.817), cigarette smoking status (B = −3.771, p = 0.047) and CPZeq (B = −0.004, p = 0.358) in linear regression analysis. Other bivariate correlations between metabolic parameters, psychopathological manifestation and cognitive performance were not significant in linear regression analysis (data not shown).
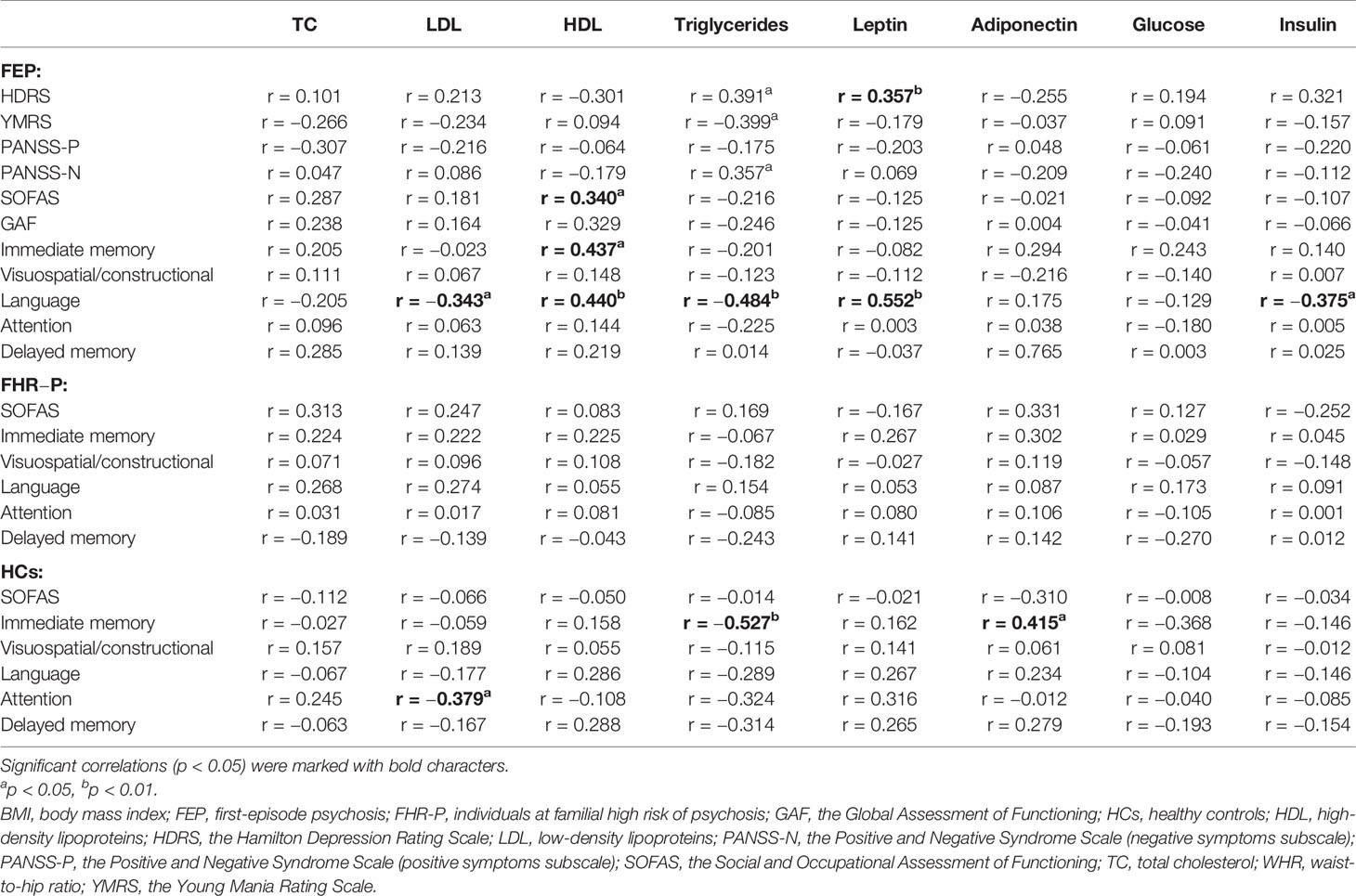
Table 3 Correlations between metabolic parameters, psychopathological manifestation, and cognitive performance.
Discussion
Our results provide further evidence that impaired adipoinsular axis is an early sign of metabolic dysregulation in psychosis. These findings are consistent with results of our meta-analysis showing increased levels of insulin and decreased levels of leptin in FEP patients compared to HCs (4). Leptin is an anorexigenic hormone released by adipose tissue and suppresses the release of insulin by direct interactions with its receptors expressed by β-cells (14). Therefore, leptin deficiency can contribute to excessive release of insulin that is an adipogenic hormone. Increased storage of adipose tissue leads to overproduction of leptin and subsequent leptin resistance. Indeed, there is evidence that multiple-episode schizophrenia patients present with increased leptin levels (5). Impaired leptin signaling might also be related to the pathophysiology of psychosis. It has been found that leptin reduces dopamine neuronal firing in the mesolimbic system (30).
The observation that higher leptin levels are associated with lower RBANS scores of language performance also support the involvement of leptin in the pathophysiology of psychosis. Notably, the RBANS language score is composed of two cognitive tasks—picture naming and semantic fluency. Patients with schizophrenia show robust deficits of verbal fluency, with semantic fluency being more impaired than phonemic fluency (31). These impairments can be attributed to attenuated frontal activation (32). There is evidence that neonatal leptin deficiency reduces the frontal cortex volumes (33). Desensitization of leptin receptors in the prefronal cortex has been associated with upregulation of dopaminergic genes in this brain region (34). Another potential explanation is related to the effects of leptin on immune-inflammatory processes. Elevated levels of leptin in obesity might contribute to the release of pro-inflammatory cytokines (35). In turn, elevated levels of proinflammatory cytokines have been associated with cognitive impairment in patients with schizophrenia (36). Surprisingly, our study demonstrated a negative correlation between leptin levels and performance of the language domain. However, a cross-sectional study design does not allow to conclude regarding direction of causality. One of potential scenarios is that higher secretion of leptin is a response to neurostructural alterations of the frontal cortex and related cognitive impairment in FEP. A lack of significant correlations between the RBANS scores and leptin levels in FHR-P individuals as well as HCs further support this interpretation.
Furthermore, we demonstrated significantly lower levels of HDL as well as significantly higher levels of triglycerides in FEP patients than in HCs. These findings are also in line with those provided by recent meta-analyses of lipid profile alterations in FEP patients (37, 38). Notably, we did not confirm the hypothesis that familial liability to psychosis is related to metabolic alterations and impaired appetite regulation. However, it should be noted that our operationalization of familial liability might be insufficient to detect a significant association as we did not assess prodromal symptoms. Moreover, due to low sample size, we were not able to test our hypotheses in a subgroup of individuals meeting the criteria of at-risk mental state (genetic risk and deterioration syndrome) (39). Indeed, there is evidence that individuals at clinical high risk of psychosis show a high percentage of metabolic syndrome components prior to exposure to antipsychotic treatment (40). Moreover, it has been shown that measuring the levels of fatty acids in subjects at ultra-high risk of psychosis may improve prediction of transition to overt psychotic episode (41). Another study demonstrated that FEP patients have significantly higher levels of prolactin, fasting glucose, glycosylated hemoglobin and insulin resistance compared to individuals at clinical high risk of psychosis (42). It cannot also be excluded that results of our study simply reflect the effects of environmental factors or unhealthy lifestyle characteristics that are highly prevalent in early psychosis and include nutritional deficiencies as well as low exercise activity (43–45).
There are some important limitations of this study that need to be acknowledged. Firstly, our sample size was not large. Therefore, it cannot be excluded that our sample had insufficient power to detect the association between familial liability to psychosis and metabolic alterations. Moreover, we did not perform a detailed clinical assessment of FHR-P individuals, especially with respect to prodromal symptoms of psychosis. In light of these two limitations, we were unable to test the hypothesis whether metabolic dysregulation assessed in this study appears in individuals at clinical high risk of psychosis. Another limitation is that we cannot exclude medication effects. However, exposure to antipsychotic treatment was low in our study and linear regression analyses did not confirm a significant effect of CPZeq. It is also important to note that we did not record initial sample of individuals approached for participation and reasons for nonparticipation. Therefore, it is difficult to evaluate representativeness of our sample. Finally, a lack of longitudinal study design does not allow to establish conclusions regarding causality and temporal patterns of changes in metabolic parameters.
In summary, this study provides additional evidence of impaired adipoinsular axis, in terms of low leptin and high insulin levels, in early psychosis. Leptin levels might be related to cognitive impairment in FEP patients; however, causal mechanisms of this association need to be confirmed. Our findings provide novel insights into potential mechanisms of early metabolic disturbances and cognitive impairment in psychotic disorders. Moreover, we confirmed that FEP is associated with specific lipid profile disturbances. Longitudinal studies investigating our findings in subjects at clinical high risk of psychosis, especially in those with genetic risk and deterioration syndrome, are needed to confirm direction of causality and address limitations of our study.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by The Ethics Committee at Wroclaw Medical University, Poland. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
ML and BM designed the study. ML, BM, BS, AS and AR were involved in recruitment of participants. LP-S measured the levels of leptin and adiponectin. BM performed data analysis. ML and BM wrote the first draft of the manuscript. All authors contributed to reviewing and editing the first draft of the manuscript.
Funding
This study was funded from science budget resources granted for the years 2016–2019 (the Iuventus Plus grant awarded by the Ministry of Science and Higher Education, grant number: IP2015 052474).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Piotrowski P, Gondek TM, Królicka-Deręgowska A, Misiak B, Adamowski T, Kiejna A. Causes of mortality in schizophrenia: An updated review of European studies. Psychiatr Danub (2017) 29:108–20. doi: 10.24869/psyd.2017.108
2. Pillinger T, D’Ambrosio E, McCutcheon R, D Howes O. Is psychosis a multisystem disorder? A meta-review of central nervous system, immune, cardiometabolic, and endocrine alterations in first-episode psychosis and perspective on potential models. Mol Psychiatry (2018) 24:776–94. doi: 10.1038/s41380-018-0058-9
3. Andreassen OA, Djurovic S, Thompson WK, Schork AJ, Kendler KS, O’Donovan MC, et al. Improved detection of common variants associated with schizophrenia by leveraging pleiotropy with cardiovascular-disease risk factors. Am J Hum Genet (2013) 92:197–209. doi: 10.1016/j.ajhg.2013.01.001
4. Misiak B, Bartoli F, Stramecki F, Samochowiec J, Lis M, Kasznia J, et al. Appetite regulating hormones in first-episode psychosis: A systematic review and meta-analysis. Neurosci Biobehav Rev (2019) 102:362–70. doi: 10.1016/j.neubiorev.2019.05.018
5. Stubbs B, Wang AK, Vancampfort D, Miller BJ. Are leptin levels increased among people with schizophrenia versus controls? A systematic review and comparative meta-analysis. Psychoneuroendocrinology (2016) 63:144–54. doi: 10.1016/j.psyneuen.2015.09.026
6. Bartoli F, Lax A, Crocamo C, Clerici M, Carrà G. Plasma adiponectin levels in schizophrenia and role of second-generation antipsychotics: A meta-analysis. Psychoneuroendocrinology (2015) 56:179–89. doi: 10.1016/j.psyneuen.2015.03.012
7. Lihn AS, Pedersen SB, Richelsen B. Adiponectin: Action, regulation and association to insulin sensitivity. Obes Rev (2005) 6:13–21. doi: 10.1111/j.1467-789X.2005.00159.x
8. Lee EE, Sears DD, Liu J, Jin H, Tu XM, Eyler LT, et al. A novel biomarker of cardiometabolic pathology in schizophrenia? J Psychiatr Res (2019) 117:31–7. doi: 10.1016/j.jpsychires.2019.06.011
9. Farr OM, Tsoukas MA, Mantzoros CS. Leptin and the brain: Influences on brain development, cognitive functioning and psychiatric disorders. Metabolism (2015) 64:114–30. doi: 10.1016/j.metabol.2014.07.004
10. Tang BL. Leptin as a neuroprotective agent. Biochem Biophys Res Commun (2008) 368:181–5. doi: 10.1016/j.bbrc.2008.01.063
11. Venkatasubramanian G, Chittiprol S, Neelakantachar N, Shetty TK, Gangadhar BN. A longitudinal study on the impact of antipsychotic treatment on serum leptin in schizophrenia. Clin Neuropharmacol (2010) 33:288–92. doi: 10.1097/WNF.0b013e3181fa2a6f
12. Bereiter DA, Jeanrenaud B. Altered neuroanatomical organization in the central nervous system of the genetically obese (ob/ob) mouse. Brain Res (1979) 165:249–60. doi: 10.1016/0006-8993(79)90557-2
13. Vannucci SJ, Gibbs EM, Simpson IA. Glucose utilization and glucose transporter proteins GLUT-1 and GLUT-3 in brains of diabetic (db/db) mice. Am J Physiol - Endocrinol Metab (1997) 272:E267–74. doi: 10.1152/ajpendo.1997.272.2.e267
14. Kieffer TJ, Habener JF. The adipoinsular axis: Effects of leptin on pancreatic β-cells. Am J Physiol - Endocrinol Metab (2000) 278:E1–E14. doi: 10.1152/ajpendo.2000.278.1.e1
15. Park CR. Cognitive effects of insulin in the central nervous system. Neurosci Biobehav Rev (2001) 25:311–23. doi: 10.1016/S0149-7634(01)00016-1
16. Zhang X, Yang M, Du X, Liao W, Chen D, Fan F, et al. Glucose disturbances, cognitive deficits and white matter abnormalities in first-episode drug-naive schizophrenia. Mol Psychiatry (2019). doi: 10.1038/s41380-019-0478-1
17. Ferrario CR, Reagan LP. Insulin-mediated synaptic plasticity in the CNS: Anatomical, functional and temporal contexts. Neuropharmacology (2018) 136:182–91. doi: 10.1016/j.neuropharm.2017.12.001
18. Agarwal SM, Caravaggio F, Costa-Dookhan KA, Castellani L, Kowalchuk C, Asgariroozbehani R, et al. Brain insulin action in schizophrenia: Something borrowed and something new. Neuropharmacology (2020) 163:107633. doi: 10.1016/j.neuropharm.2019.05.010
19. Zhang X, Jiang X, Han S, Liu Q, Zhou J. Type 2 Diabetes Mellitus Is Associated With the Risk of Cognitive Impairment: A Meta-Analysis. J Mol Neurosci (2019) 68:251–60. doi: 10.1007/s12031-019-01290-3
20. Bora E, Akdede BB, Alptekin K. The relationship between cognitive impairment in schizophrenia and metabolic syndrome: A systematic review and meta-analysis. Psychol Med (2017) 47:1030–40. doi: 10.1017/S0033291716003366
21. Wysokiński A, Dzienniak M, Kłoszewska I. Effect of metabolic abnormalities on cognitive performance and clinical symptoms in schizophrenia. Arch Psychiatry Psychother (2013) 4:13–25. doi: 10.12740/APP/19967
22. Botis AC, Miclutia I, Vlasin N. Cognitive function in female patients with schizophrenia and metabolic syndrome. Eur Psychiatry (2016) 33:S97. doi: 10.1016/j.eurpsy.2016.01.070
23. Li R, Wang TJ, Lyu PY, Liu Y, Chen WH, Fan MY, et al. Effects of Plasma Lipids and Statins on Cognitive Function. Chin Med J (Engl) (2018) 131:471–6. doi: 10.4103/0366-6999.225062
24. McGuffin P. A Polydiagnostic Application of Operational Criteria in Studies of Psychotic Illness. Arch Gen Psychiatry (1991) 48:764. doi: 10.1001/archpsyc.1991.01810320088015
25. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull (1987) 13:261–76. doi: 10.1093/SCHBUL/13.2.261
26. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56
27. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
28. Goldman HH, Skodol AE, Lave TR. Revising axis V for DSM-IV: A review of measures of social functioning. Am J Psychiatry (1992) 149:1148–56. doi: 10.1176/ajp.149.9.1148
29. Randolph C, Tierney MC, Mohr E, Chase TN. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary Clinical Validity. J Clin Exp Neuropsychol (Neuropsychology Dev Cognit Sect A) (1998) 20:310–9. doi: 10.1076/jcen.20.3.310.823
30. Hommel JD, Trinko R, Sears RM, Georgescu D, Liu ZW, Gao XB, et al. Leptin Receptor Signaling in Midbrain Dopamine Neurons Regulates Feeding. Neuron (2006) 51:801–10. doi: 10.1016/j.neuron.2006.08.023
31. Henry JD, Crawford JR. A meta-analytic review of verbal fluency deficits in schizophrenia relative to other neurocognitive deficits. Cognit Neuropsychiatry (2005) 10:1–33. doi: 10.1080/13546800344000309
32. Curtis VA, Bullmore ET, Brammer MJ, Wright IC, Williams SCR, Morris RG, et al. Attenuated frontal activation during a verbal fluency task in patients with schizophrenia. Am J Psychiatry (1998) 155:1056–63. doi: 10.1176/ajp.155.8.1056
33. Dexter BC, Rahmouni K, Cushman T, Hermann GM, Ni C, Nopoulos PC, et al. Neonatal leptin deficiency reduces frontal cortex volumes and programs adult hyperactivity in mice. Behav Brain Res (2014) 263:115–21. doi: 10.1016/j.bbr.2014.01.021
34. Del Rio D, Del Olmo N, Ruiz-Gayo M. Desensitization of leptin receptors is coincident with the upregulation of dopamine-related genes in the prefrontal cortex of adolescent mice. Neuroreport (2016) 27:516–21. doi: 10.1097/WNR.0000000000000574
35. Iikuni N, Kwan Lam Q, Lu L, Matarese G, Cava A. Leptin and Inflammation. Curr Immunol Rev (2008) 4:70–9. doi: 10.2174/157339508784325046
36. Misiak B, Beszłej JA, Kotowicz K, Szewczuk-Bogusławska M, Samochowiec J, Kucharska-Mazur J, et al. Cytokine alterations and cognitive impairment in major depressive disorder: From putative mechanisms to novel treatment targets. Prog Neuropsychopharmacol Biol Psychiatry (2017) 80:177–88. doi: 10.1016/j.pnpbp.2017.04.021
37. Misiak B, Stańczykiewicz B, Łaczmański Ł, Frydecka D. Lipid profile disturbances in antipsychotic-naive patients with first-episode non-affective psychosis: A systematic review and meta-analysis. Schizophr Res (2017) 190:18–27. doi: 10.1016/j.schres.2017.03.031
38. Pillinger T, Beck K, Stubbs B, Howes OD. Cholesterol and triglyceride levels in first-episode psychosis: systematic review and meta-analysis. Br J Psychiatry (2017) 211:339–49. doi: 10.1192/bjp.bp.117.200907
39. Fusar-Poli P, Cappucciati M, Borgwardt S, Woods SW, Addington J, Nelson B, et al. Heterogeneity of psychosis risk within individuals at clinical high risk: A meta-analytical stratification. JAMA Psychiatry (2016) 73:113–20. doi: 10.1001/jamapsychiatry.2015.2324
40. Cadenhead KS, Minichino A, Kelsven S, Addington J, Bearden C, Cannon TD, et al. Metabolic abnormalities and low dietary Omega 3 are associated with symptom severity and worse functioning prior to the onset of psychosis: Findings from the North American Prodrome Longitudinal Studies Consortium. Schizophr Res (2019) 204:96–103. doi: 10.1016/j.schres.2018.09.022
41. Clark SR, Baune BT, Schubert KO, Lavoie S, Smesny S, Rice SM, et al. Prediction of transition from ultra-high risk to first-episode psychosis using a probabilistic model combining history, clinical assessment and fatty-acid biomarkers. Transl Psychiatry (2016) 6:e897. doi: 10.1038/tp.2016.170
42. Petruzzelli MG, Margari M, Peschechera A, de Giambattista C, De Giacomo A, Matera E, et al. Hyperprolactinemia and insulin resistance in drug naive patients with early onset first episode psychosis. BMC Psychiatry (2018) 18:246. doi: 10.1186/s12888-018-1827-3
43. Borgan F, O’Daly O, Hoang K, Veronese M, Withers D, Batterham R, et al. Neural Responsivity to Food Cues in Patients With Unmedicated First-Episode Psychosis. JAMA Netw Open (2019) 2:e186893. doi: 10.1001/jamanetworkopen.2018.6893
44. Firth J, Carney R, Stubbs B, Teasdale SB, Vancampfort D, Ward PB, et al. Nutritional Deficiencies and Clinical Correlates in First-Episode Psychosis: A Systematic Review and Meta-analysis. Schizophr Bull (2017) 44:1275–92. doi: 10.1093/schbul/sbx162
Keywords: adipose tissue, lipid, hormone, schizophrenia, obesity
Citation: Lis M, Stańczykiewicz B, Pawlik-Sobecka L, Samochowiec A, Reginia A and Misiak B (2020) Assessment of Appetite-Regulating Hormones Provides Further Evidence of Altered Adipoinsular Axis in Early Psychosis. Front. Psychiatry 11:480. doi: 10.3389/fpsyt.2020.00480
Received: 26 February 2020; Accepted: 11 May 2020;
Published: 29 May 2020.
Edited by:
Grazia Rutigliano, University of Pisa, ItalyReviewed by:
Milica Milovan Borovcanin, University of Kragujevac, SerbiaMaria Giuseppina Petruzzelli, University of Bari Aldo Moro, Italy
Copyright © 2020 Lis, Stańczykiewicz, Pawlik-Sobecka, Samochowiec, Reginia and Misiak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Błażej Misiak, bWJsYXplakBpbnRlcmlhLmV1