
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 06 December 2019
Sec. Addictive Disorders
Volume 10 - 2019 | https://doi.org/10.3389/fpsyt.2019.00886
This article is part of the Research Topic The Global Methamphetamine Problem: Approaches to Elucidate the Neurobiology, Epidemiology and Therapeutic Effectiveness View all 13 articles
 Henrike Schecke1*
Henrike Schecke1* Toby Lea2,3
Toby Lea2,3 Annette Bohn1
Annette Bohn1 Thorsten Köhler4Dirk Sander5
Thorsten Köhler4Dirk Sander5 Norbert Scherbaum1
Norbert Scherbaum1 Daniel Deimel4
Daniel Deimel4Introduction: Men who have sex with men (MSM) are a vulnerable subgroup for problems with substance use, including crystal methamphetamine. Drug use in sexual settings, commonly referred to as “chemsex,” has been an issue of growing concern in MSM communities. Recreational drugs commonly associated with chemsex include crystal methamphetamine, gamma-hydroxybutyrate/gamma-butyrolactone (GHB/GBL), mephedrone, and ketamine. Drug use in sexual settings is correlated with sexual practices associated with the acquisition and transmission of sexually transmitted infections, including HIV and hepatitis C. Adverse mental health outcomes are often reported at higher rates among MSM who use methamphetamine.
Methods: This paper refers to a subset of participants from the German Chemsex Survey, an MSM-community recruited, self-completed online survey with a self-selected convenience sample. Participants who used crystal methamphetamine for sex (n = 130) were compared to participants who did not use drugs for sex (n = 177). The survey comprised 420 different items considering recreational substance use, substance use in sexual settings, harm reduction strategies, mental health, sexual transmitted infections, and mental health care service utilization.
Results: A total of 1,583 men started the survey; 1,050 participants provided information on substance use. Twenty-seven percent of participants used crystal methamphetamine in the last 12 months, and of those, 89% used methamphetamine in a sexual setting and 50% reported injecting methamphetamine. Regarding mental health, participants who reported methamphetamine use in sexual settings were more likely to report symptoms of depression, somatization, anxiety, and posttraumatic stress disorder (PTSD) than the German male general population. Participants who reported methamphetamine use for sex were more likely to report symptoms of major depression, being HIV positive, and taking HIV pre-exposure prophylaxis (PrEP) than participants who did not report methamphetamine use. Most participants used harm reduction practices to reduce the risks associated with using methamphetamine in sexual settings.
Conclusion: Crystal methamphetamine is used in the context of sexual activities by German MSM. Poorer mental health status than in the male general population was observed. MSM who used methamphetamine in this study seemed to be aware of potential health risks associated with their substance use and utilized harm reduction strategies and biomedical HIV prevention strategies like PrEP.
Men who have sex with men (MSM) are a vulnerable subgroup for problems with substance use, including crystal methamphetamine (1, 2). Methamphetamine use in MSM populations is a growing issue of concern globally. Numerous studies from the United States (3), diverse countries in Asia (4), the United Kingdom (5–7), Ireland (8), Australia (9, 10), and the European Union (11) have consistently reported a heightened prevalence of methamphetamine use among MSM compared to heterosexual men.
Drug use in sexual settings, now commonly referred to as "chemsex," has been an issue of growing concern in MSM communities in recent years (5). Recreational drugs commonly associated with chemsex include crystal methamphetamine, gamma-hydroxybutyrate/gamma-butyrolactone (GHB/GBL), mephedrone, and ketamine, and are typically used with the intention to enhance, intensify, and prolong sexual experiences (2). Drug use in sexual settings can have benefits for MSM, such as fostering social and sexual connections with other men and the exploration of sexual desires (12). However, drug use in sexual settings is also associated with the acquisition and transmission of sexually transmitted infections (STIs), including HIV (13). It has been consistently shown that MSM who use drugs for sex are more likely to be HIV positive (14, 15) and have higher rates of STIs and hepatitis C (HCV) (16, 17) than those who do not engage in these practices. HIV-positive MSM are more likely to initiate methamphetamine use after seroconversion, for some men as a coping strategy (18). Current methamphetamine use also negatively affects adherence to the antiretroviral therapy (ART) in HIV-positive MSM (19).
Research indicates that injecting methamphetamine in sexual settings ("slamming") is also common in some networks of MSM (20, 5). Injecting drugs potentiates health risks such as blood-borne infections like HCV and HIV, injecting-related injuries and infections, overdose, and more severe substance dependence (21). Studies show that HCV infections are increasing among MSM, in particular among HIV-positive MSM who have never injected drugs (22–24). Drug use in sexual settings is also associated with engagement in group sex, having multiple sex partners (25, 26), transactional sex, sharing sex toys, sex practices with risks for injuries (27), and condomless anal intercourse (28) which also increases STI risks.
Adverse mental health outcomes are also reported at higher rates among MSM with longer-term methamphetamine use. In an US sample of ethnic minority MSM who use methamphetamine, a higher prevalence of major depressive disorder, social phobia, obsessive–compulsive disorder, antisocial personality disorder, and posttraumatic stress disorder (PTSD) and a higher risk for suicide attempts was reported, compared to the male US general population. In addition, mental health disorders were more commonly reported among men with more severe methamphetamine use disorders (29, 30). Lopez-Patton et al. found significantly higher rates for major depression and childhood trauma among methamphetamine-using MSM (31). In an online cohort study in Australia, while methamphetamine use overall was not negatively associated with mental health, men who were methamphetamine dependent were more likely to report depression and anxiety than men who used methamphetamine but were not dependent (32).
Crystal methamphetamine use is uncommon in most parts of Germany, with exceptions to regions near the Czech border (33). In a representative survey of the general population in Germany, the 12-month prevalence of methamphetamine use was only 0.2% among men (34). To date, there has been limited research about methamphetamine use among MSM in Germany. A recent study on motivations for psychostimulant use among German adults found that MSM most commonly reported using methamphetamine in sexual settings (35). However, little is known about German MSM who use crystal methamphetamine in sexual settings, nor their mental health (e.g., depression, anxiety, and posttraumatic stress), HIV prevention strategies such as pre-exposure prophylaxis (PrEP), or drug-related harm reduction practices. This paper aims to address these research gaps using findings from a recent national online survey. In addition, the paper examines the utilization of mental health, alcohol, and drug treatment and related support services among German MSM.
The analysis refers to a subset of participants from the German Chemsex Survey, an MSM-community recruited, self-completed online survey with a self-selected convenience sample. Eligible participants were at least 18 years of age, identified as male, and as gay, bisexual, or MSM. The present study is focused on two groups: men who reported crystal methamphetamine use in sexual settings in the previous 12 months, and men who reported no illicit drug use in sexual settings in the previous 12 months.
The survey was promoted via Lesbian, Gay, Bisexual, Transexual, Intersexual and Queer (LGBTIQ)-community websites, social media postings, HIV non-profit organizations, free-of-charge advertisements on "planetromeo" (MSM-dating website/smartphone application), and HIV/sexual health care service providers. The survey was online for 12 weeks between September and December 2018 and used the open-source survey software "LimeSurvey." All data collected were anonymous. Participants could skip questions they did not want to answer and could withdraw from the survey at any time during completion. At the end of the survey, links to nationwide accessible psychosocial support services were presented to offer support for participants who felt uncomfortable as a consequence of being confronted with questions on substance use and mental health issues. Ethical approval for the study was received from the Ethics Committee of the Medical Department of the University of Duisburg-Essen (UDE-18-8209-BO).
The survey consisted of 420 items including demographic characteristics, recreational substance use, substance use in sexual settings, mental health, sexual behavior, STIs, psychosocial/health outcomes of methamphetamine use, harm reduction practices, and use of mental health care and drug treatment services. Mental health was assessed using the German version of the Patient Health Questionnaire (PHQ-D) with subscales for depressive symptoms (PHQ-9), generalized anxiety symptoms (GAD-7), and somatization symptoms (PHQ-15) (36). The PHQ-9 scale assesses severity of depressive symptoms with a maximum score of 27. The PHQ-15 score gives information about symptoms of somatization with a maximum value of 30. GAD-7 measures symptoms of anxiety with a maximum of 21. A score of 10 or above on each of the three scales signifies an at least moderate major depressive episode, moderate levels of somatization, and moderate levels of clinical anxiety. For trauma and PTSD, the life events checklist for DSM-5 (37) as well as the four-item PTSD primary care screener (38) were conducted.
Given that participants were able to stop and save their data at any point of the survey and the survey software was not programmed in a "forced choice" format, sample size varies for different items. Data analysis was conducted using IBM SPSS Statistics 25.0. For group comparisons of participants who reported methamphetamine in sexual settings (methamphetamine group) with participants who did not report drug use in sexual settings (no drug use for sex = NDUS group), Chi² tests were used for binary and categorical dependent variables and Mann–Whitney U tests for continuous dependent variables which were not normally distributed. Where statistical tests were performed, p-values of <0.05 were taken to be statistically significant.
A total of 1,583 men started the survey, and 1,050 participants provided information on substance use (66.3%). Of the 1,050 participants who provided data on substance use, 231 (22%) reported any methamphetamine use: 36.8% ever, 26.8% in the last 12 months, 17.3% in the last 30 days, and 19% in the last 7 days. Fifty percent of the methamphetamine group had injected methamphetamines in the last 12 months. Methamphetamine use in a sexual setting in the last 12 months was reported by 130 participants (12.4%). Ninety-three percent also used amyl nitrite ("poppers"), 90% alcohol, 76.2% medication for erectile dysfunction, and 70.8% GHB/GBL in sexual settings in the last 12 months. All other substances are listed in Table 1.

Table 1 Sample characteristics and substance use.
The present analysis includes men who reported methamphetamine use in sexual settings in the last 12 months (n = 130; 8.2% of the sample) and men who reported no illicit drug use in sexual settings in the last 12 months (n = 170; 10.7% of the sample). For demographics of both groups, see Table 1.
The median PHQ-9 score was significantly higher in the methamphetamine group compared to the NDUS group. Eleven percent of participants in the methamphetamine group and 12.1% in the NDUS group had PHQ-9 scores above the cutoff for moderate depressive symptoms (see Table 2). There was no significant difference between the methamphetamine group and the NDUS group regarding GAD-7 scores. Five percent of participants in the methamphetamine group and 8.7% of participants in the NDUS group had a GAD-7 score of 10 or above, which indicates at least moderate levels of anxiety. There was no significant difference between the methamphetamine group and NDUS group regarding PHQ-15 scores. Thirteen percent of participants in the methamphetamine group and 10.6% in the NDUS group had a score of 10 or above, indicating at least moderate levels of clinically relevant somatization. In both groups together, 76.4% of participants had experienced at least one potentially traumatizing event according to the DSM-5 life events scale, with a mean number of 1.86 potentially traumatizing events. There was no significant difference between the two groups in the number of traumatic events reported. In the methamphetamine group, 6.4% had a score of 3 or more on the PTSD primary care screener, indicating a possible diagnosis of PTSD. In the NDUS group, 12.9% were above the cutoff for PTSD, although the difference between the groups was not statistically significant (see Table 2).
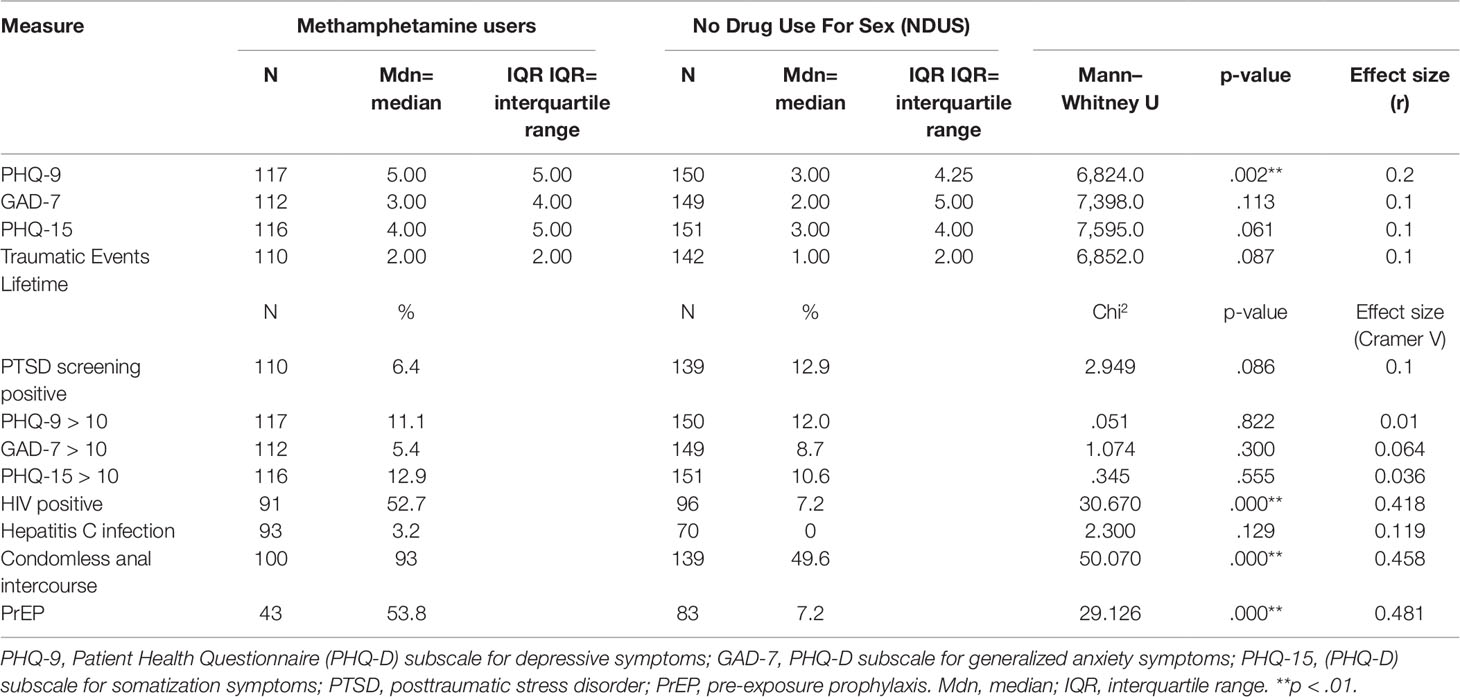
Table 2 Mental health, infectious diseases, and biomedical HIV prevention.
Regarding HCV, 3.2% of the methamphetamine group reported that they were HCV positive. None of the NDUS group was positive for HCV. Fifty-three percent of the methamphetamine group reported being HIV positive, 42.9% were HIV negative, and 4.4% did not know their current HIV status. Compared to the NDUS group, participants in the methamphetamine group were significantly more likely to report being HIV positive (7.3% vs. 52.7%). All HIV-positive participants were taking HIV ART and reported having an undetectable viral load. Among HIV-negative men, a higher proportion of men in the methamphetamine group (53.8%) were currently taking PrEP than in the NDUS group (7.2%). Any condomless anal intercourse in the last 12 months was reported by a significantly higher proportion of men in the methamphetamine group (93.0%) than in the NDUS group (49.6%).
Participants who reported methamphetamine use for sex reported a range of drug- and sex-related harm reduction practices. The practices that men most commonly reported always doing were: drinking enough non-alcoholic beverages, making sure to get enough sleep after consumption, and having enough lube available at all times Table 3).
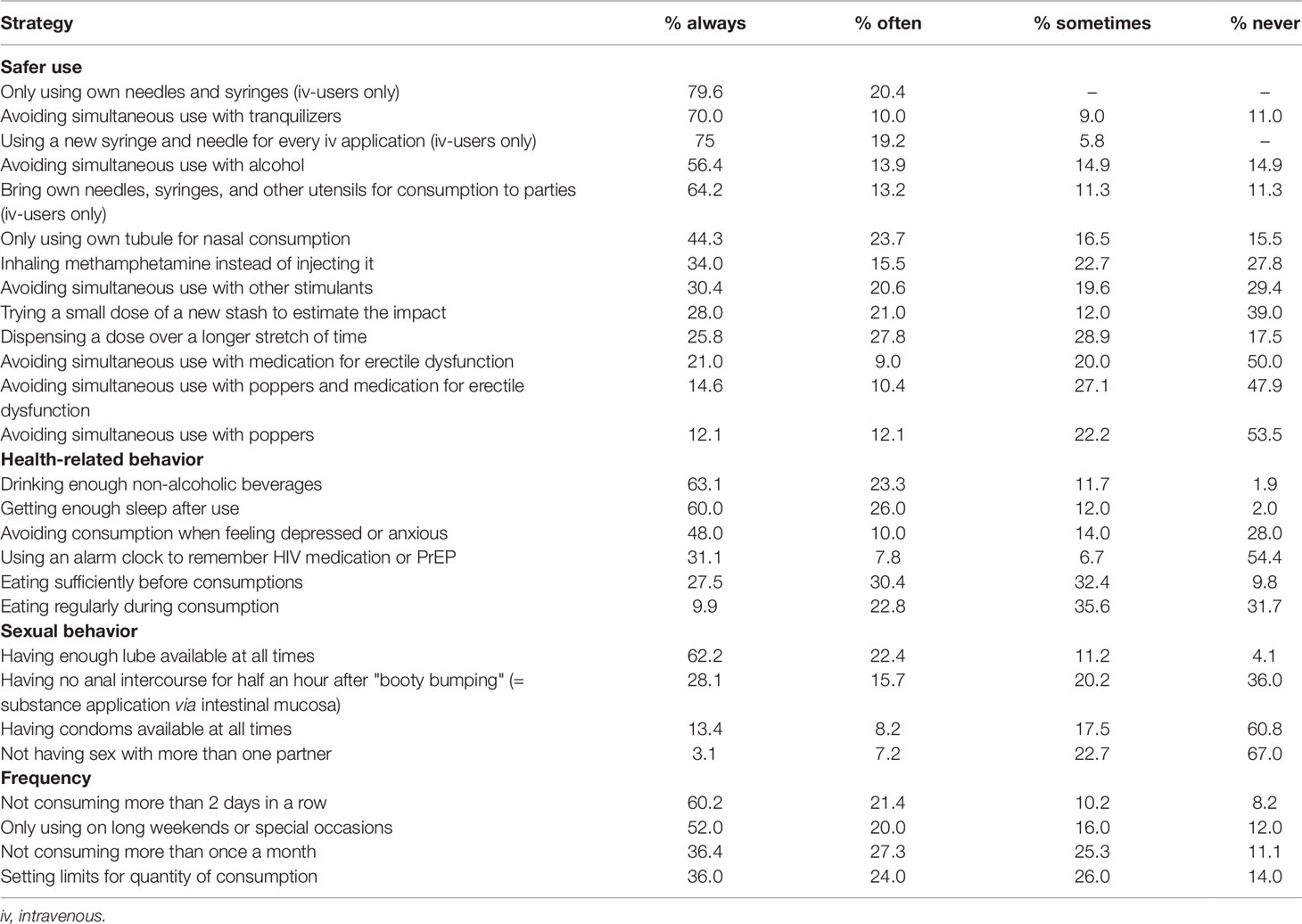
Table 3 Utilization of harm reduction strategies of methamphetamine-using participants.
Thirteen percent of men in the methamphetamine group and 4.1% in the NDUS group were seeing a psychotherapist at the time of the survey, while 6.9% in the methamphetamine group and 1.8% in the NDUS group were seeing a psychiatrist. Two percent (2.3%) of men in the methamphetamine group and 1.8% in the NDUS group were attending an outpatient alcohol and other drug counseling service at the time of the survey. In the methamphetamine group, the most common forms of engagement with the health care system were with a general practitioner (52.8%) or an infectious diseases specialist (35.2%). Participants also had contact with other psychosocial support services, including counseling for people living with HIV (17.4% methamphetamine group and 2.9% NDUS group) and LGBTIQ-specific counseling services (9.2% of participants in methamphetamine group and 0.6% in the NDUS group).
In this study, German MSM who used crystal methamphetamine commonly did so in the context of sexual activities. Poorer mental health status was observed among MSM who used methamphetamine than in the general male population. Men who used crystal methamphetamine for sex seemed to be aware of potential health risks associated with their substance use and utilized harm reduction strategies and biomedical HIV prevention strategies like PrEP and HIV treatment as prevention (TasP).
These results support previous research in a German sample of people who use psychostimulant that methamphetamine use for sex is an important motive of MSM (35). Polydrug use was commonly reported in this subset of methamphetamine-using German MSM. Nearly all participants used amyl nitrite in the previous 12 months, and more than two-thirds used erectile dysfunction medications. Amyl nitrite is commonly used as a muscle relaxant to facilitate receptive anal intercourse, and erectile dysfunction medications are often reported by MSM who used methamphetamine for sex as psychostimulant use is often associated with difficulties gaining and maintaining an erection (39). About half of the sample reported consumption of other substances that are commonly associated with chemsex (e.g., GHB/GBL, mephedrone, ketamine) (2).
Eleven percent in the methamphetamine group had a score on the PHQ-9 scale indicating at least moderate depressive symptoms. This is comparable to a sample of MSM in the UK (40), but considerably lower than in an Australian study among MSM. Here, nearly one-third of gay and bisexual men reported moderate depressive symptoms on the PHQ-9 scale (32). Regarding most mental health measures, there were no significant differences between men who used methamphetamine for sex and men who reported no drug use for sex. However, both groups of MSM reported consistently higher levels of depression, somatization (41), generalized anxiety (42), number of traumatic life events (43), and PTSD (44) compared to representative data among the general population of men in Germany. Crystal methamphetamine use does not seem to be the most contributing factor, given that both groups of MSM showed lower mental well-being.
In summary, the results underline that both groups of MSM, irrespective of substance use, were more likely to experience poor mental health than the male general population. According to the minority stress model (45), a minority status, like a non-heterosexual sexual orientation, has an impact on psychological well-being and can increase likelihood of experiencing problems with mental health and substance use.
Besides this, poorer mental health status among men who used methamphetamine in our study may be traced back to the fact that half of the sample was HIV positive. Since ART, HIV is a chronic condition similar to other chronic conditions [e.g., diabetes (46)], and living with HIV and other chronic conditions is associated with an increased likelihood of experiencing depression (47). Experiences of HIV-related stigma may also be a contributing factor to the higher rates of depression reported, which can negatively impact mental health and well-being (48).
The heightened proportion of men who live with HIV in the methamphetamine group is consistent with previous research (14, 15). All HIV-positive men in the sample were taking ART and self-reported an undetectable viral load. Successful treatment of HIV is an important contribution to prevent HIV transmission (TasP). Large-scale, prospective studies have shown no HIV transmission in serodiscordant couples when the viral load of the HIV-positive partner was suppressed sufficiently by ART (49). The latest addition to biomedical HIV prevention strategies is PrEP. PrEP refers to the use of HIV-antiretrovirals in HIV-negative people at high risk for HIV to prevent infection (50). In Germany, PrEP is only available on prescription and has been available at an affordable price since 2017. As a result of an initiative of a pharmacist in Cologne and negotiations with a pharmaceutical company to distribute a generic version of PrEP, it was available nationally for 50 Euros (about 55 USD) per month. Since September 2019, PrEP has been covered by health insurance free of charge for people at high risk of becoming infected with HIV. HIV-negative men who use methamphetamine seem to reflect that they may be at risk for HIV infection due to their substance use in sexual settings and therefore decide for PrEP. Under the influence of methamphetamines, other prevention strategies, like condom use, may be compromised (51). Nonetheless, PrEP and TasP do not prevent the acquisition of other STIs.
Half of the methamphetamine user sample injected drugs in sexual settings, which carries a risk for the transmission of blood-borne viruses like HCV, as well as HIV. Although the prevalence of HCV was 10 times higher than in the German general population (52), it was significantly lower than in other groups of people who inject drugs in Germany, which has been estimated at between 42% and 75% (53). The routine utilization of harm reduction strategies can help prevent HCV among people who inject drugs (54). In the German Chemsex Survey sample, men who use methamphetamine seem to be aware and well informed about various harm reduction strategies. Most participants used at least some harm reduction practices to prevent negative health outcomes related to methamphetamine use. Injecting substances carries the highest risk for negative health consequences. Among those who injected methamphetamine in sexual settings, harm reduction practices appeared to be well established. More than two-thirds of men who injected methamphetamine stated that they always used their own needle and syringe and used a new needle and syringe every time they injected. There has been very little research published on the harm reduction practices of MSM. In a Canadian study, harm reduction strategies with focus on safety when injecting drugs were most common (55). Other strategies refer to restrictions of frequency or maintaining a healthy lifestyle, such as eating regularly, getting enough sleep, and staying hydrated (55). Avoidance of polydrug use is another important harm reduction practice, given the increased risk of overdose and other negative consequence of combining drugs in the same session. Half of the sample stated that they never refrain from simultaneous use of methamphetamine and amyl nitrite or erectile dysfunction medications. One-third reported never avoiding using other stimulants at the same time as methamphetamine. Combined use of erectile dysfunction medications and alcohol, other recreational drugs, and especially amyl nitrite, increases risks for potentially fatal cardiovascular events and other serious drug interactions (56). Given that polydrug use was common in this sample and in other studies of MSM (57), there is some potential for improvement of applying this harm reduction strategy.
About one in five men of the sample currently consults a psychotherapist or psychiatrist. This is a good fit to the proportion of men who report mental health problems in the sample, so mental health care service utilization seems to be high. Only few men seek support from alcohol or drug treatment facilities. Perhaps, they do not need such treatment since they do not have any substance-related problems or disorders. Other reasons could be that there are only very few target group–specific services for MSM who use drugs for sex or that they fear rejection or stigmatization by service staff because of their sexual orientation. Future work could have a further look at what type of counseling or treatment services MSM who use drugs for sex need and where those services should be located. An integration of sexual health, LGBTIQ counseling, and drug treatment services would be helpful to exchange expertise and improve care for support-seeking MSM who use drugs for sex.
About one in five participants reported lifetime methamphetamine use, which is a considerably higher prevalence than in the German male general population. The German Chemsex Survey was not designed to determine prevalence rates for methamphetamine use among MSM, but to recruit a sample of MSM who report substance use, and was advertised accordingly. The results should thus be interpreted with this in mind, and may not be generalizable to all MSM in Germany. The inclusion of a self-selected convenience sample may contribute to bias, with overestimation of substance use in sexual settings and mental health problems. In addition, the sample had a high socioeconomic and educational status, clearly above the average in the German male general population. Moreover, the sample was not diverse as very few trans men or men born outside of Germany participated. The survey was only available in German, so men with insufficient German language skills would have been discouraged from participating. The high number of HIV-positive participants may be due to the recruitment sources as the survey was promoted via community-based organizations that provide services for people living with HIV. Another obvious limitation is the high rate of attrition, most likely due to the large number of items. Despite these limitations, the study provides some relevant findings on MSM who use substances in sexual settings, regarding mental health, biomedical HIV prevention, and harm reduction strategies.
The datasets generated for this study are available on request to the corresponding author.
The studies involving human participants were reviewed and approved by the Ethics Committee of the Medical Department of the University of Duisburg-Essen. The patients/participants provided their written informed consent to participate in this study.
HS: study conceptualization, data analysis, article writing. TL: article writing, language editing. AB: data analysis and literature search. DS: study conceptualization, editing article. TK: consulting data analysis. NS: editing article. DD: study conceptualization, editing article.
NS received honoraria for several activities (advisory boards, lectures, manuscripts) by AbbVie, Hexal, Janssen-Cilag, MSD, Medice, Mundipharma, Reckitt-Benckiser/Indivior, and Sanofi-Aventis. During the last 3 years, he participated in clinical trials financed by the pharmaceutical industry.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Bourne A, Weatherburn P. Substance use among men who have sex with men: patterns, motivations, impacts and intervention development need. Sex Transm Infect (2017) 93:342–6. doi: 10.1136/sextrans-2016-052674
2. Tomkins A, George R, Kliner M. Sexualised drug taking among men who have sex with men: a systematic review. Perspect In Public Health (2018) 139(1):23–33. doi: 10.1177/1757913918778872
3. Shoptaw S. Methamphetamine use in urban gay and bisexual populations. Top HIV Med (2006) 14(2):84–7.
4. Lim SH, Akbar M, Wickersham JA, Kamarulzaman A, Altice FL. The management of methamphetamine use in sexual settings among men who have sex with men in Malaysia. Int J Drug Policy (2018) 55:256–62. doi: 10.1016/j.drugpo.2018.02.019
5. Bourne A, Reid D, Hickson F, Torres-Rueda S, Steinberg P, Weatherburn P. "Chemsex" and harm reduction need among gay men in South London. Int J Drug Policy (2015) 26:1171–6. doi: 10.1016/j.drugpo.2015.07.013
6. Bourne A, Reid D, Hickson F, Torres-Rueda S, Weatherburn P. Illicit drug use in sexual settings (’chemsex’) and HIV/STI transmission risk behaviour among gay men in South London: findings from a qualitative study. Sex Transm Infect (2015) 91:564–8. doi: 10.1136/sextrans-2015-052052
7. Hickson F, Bonell C, Weatherburn P, Reid D. Illicit drug use among men who have sex with men in England and Wales. Addict Res Theory (2010) 18(1):14–22. doi: 10.1016/j.drugpo.2015.07.013
8. Barrett P, O’Donnell K, Fitzgerald M, Schmidt AJ, Hickson F, Quinlan M, et al. Drug use among men who have sex with men in Ireland: Prevalence and associated factors from a national online survey. Int J Drug Policy (2019) 64:5–12. doi: 10.1016/j.drugpo.2018.11.011
9. Lea T, Mao L, Hopwood M, Prestage G, Zablotska I, de Wit J, et al. Methamphetamine use among gay and bisexual men in Australia: Trends in recent and regular use from the Gay Community Periodic Surveys. Int J Drug Policy (2016) 29:66–72. doi: 10.1016/j.drugpo.2016.01.003
10. Roxburgh A, Lea T, de Wit J, Degenhardt L. Sexual identity and prevalence of alcohol and other drug use among Australians in the general population. Int J Drug Policy (2016) 28:76–82. doi: 10.1016/j.drugpo.2015.11.005
11. Schmidt AJ, Bourne A, Weatherburn P, Reid D, Marcus U, Hickson F. Illicit drug use among gay and bisexual men in 44 cities: Findings from the European MSM Internet Survey (EMIS). Int J Drug Policy (2016) 38:4–12. doi: 10.1016/j.drugpo.2016.09.007
12. Race K, Lea T, Murphy D, Pienaar K. The future of drugs: recreational drug use and sexual health among gay and other men who have sex with men. Sex Health (2017) 14(1):42–50. doi: 10.1071/sh16080
13. Vosburgh HW, Mansergh G, Sullivan PS, Purcell DW. A review of the literature on event-level substance use and sexual risk behavior among men who have sex with men. AIDS Behav (2012) 16:1394–410. doi: 10.1007/s10461-011-0131-8
14. Frankis J, Flowers P, McDaid L, Bourne A. Low levels of chemsex among men who have sex with men, but high levels of risk among men who engage in chemsex: analysis of a cross-sectional online survey across four countries. Sex Health (2018) 15(2):144–50. doi: 10.1071/sh17159
15. Pakianathan M, Whittaker W, Lee MJ, Avery J, Green S, Nathan B, et al. Chemsex and new HIV diagnosis in gay, bisexual and other men who have sex with men attending sexual health clinics. HIV Med (2018) 19(7):485–90. doi: 10.1111/hiv.12629
16. Pufall EL, Kall M, Shahmanesh M, Nardone A, Gilson R, Delpech V, et al. Sexualized drug use (’chemsex’) and high-risk sexual behaviours in HIV-positive men who have sex with men. HIV Med (2018) 55:231–41. doi: 10.1111/hiv.12574
17. Rosińska M, Gios L, Nöstlinger C, Vanden Berghe W, Marcus U, Schink S, et al. Prevalence of drug use during sex amongst MSM in Europe: Results from a multi-site bio-behavioural survey. Int J Drug Policy (2018) 55:231–41. doi: 10.1016/j.drugpo.2018.01.002
18. Halkitis PN, Levy MD, Solomon TM. Temporal relations between methamphetamine use and HIV seroconversion in gay, bisexual, and other men who have sex with men. J Health Psychol (2016) 21(1):93–9. doi: 10.1177/1359105314522675
19. Moore DJ, Blackstone K, Woods SP, Ellis RJ, Atkinson JH, Heaton RK, et al. Methamphetamine use and neuropsychiatric factors are associated with antiretroviral non-adherence. AIDS Care (2012) 24(12):1504–13. doi: 10.1080/09540121.2012.672718
20. Bui H, Zablotska-Manos I, Hammoud M, Jin F, Lea T, Bourne A, et al. Prevalence and correlates of recent injecting drug use among gay and bisexual men in Australia: Results from the FLUX study. Int J Drug Policy (2018) 55:222–30. doi: 10.1016/j.drugpo.2018.01.018
21. Strang J, Bearn J, Farrell M, Finch E, Gossop M, Griffiths P, et al. Route of drug use and its implications for drug effect, risk of dependence and health consequences. Drug Alcohol Rev (1998) 17(2):197–211. doi: 10.1080/09595239800187001
22. Chan DP, Sun HY, Wong HT, Lee SS, Hung CC. Sexually acquired hepatitis C virus infection: a review. Int J Infect Dis (2016) 49:47–58. doi: 10.1016/j.ijid.2016.05.030
23. Van De Laar TJW, Matthews GV, Prins M, Danta M. Acute hepatitis C in HIV-infected men who have sex with men: An emerging sexually transmitted infection. Aids (2010) 24(12):1799–812. doi: 10.1097/QAD.0b013e32833c11a5
24. Van De Laar TJW, Van Der Bij AK, Prins M, Bruisten SM, Brinkman K, Ruys TA, et al. Increase in HCV incidence among men who have sex with men in Amsterdam most likely caused by sexual transmission. J Infect Dis (2007) 196(2):230–8. doi: 10.1086/518796
25. Glynn RW, Byrne N, O’Dea S, Shanley A, Codd M, Keenan E, et al. Chemsex, risk behaviours and sexually transmitted infections among men who have sex with men in Dublin, Ireland. Int J Drug Policy (2017) 52:9–15. doi: 10.1016/j.drugpo.2017.10.008
26. Sewell J, Miltz A, Lampe FC, Cambiano V, Speakman A, Phillips AN, et al. Poly drug use, chemsex drug use, and associations with sexual risk behaviour in HIV-negative men who have sex with men attending sexual health clinics. Int J Drug Policy (2017) 43:33–43. doi: 10.1016/j.drugpo.2017.01.001
27. Hegazi A, Lee MJ, Whittaker W, Green S, Simms R, Cutts R, et al. Chemsex and the city: sexualised substance use in gay bisexual and other men who have sex with men attending sexual health clinics. Int J STD AIDS (2016) 28:362–6. doi: 10.1177/0956462416651229
28. Daskalopoulou M, Rodger AJ, Phillips AN, Sherr L, Elford J, McDonnell J, et al. Condomless sex in HIV-diagnosed men who have sex with men in the UK: prevalence, correlates, and implications for HIV transmission. Sex Transm Infect (2017) 93:590–8. doi: 10.1136/sextrans-2016-053029
29. Fletcher JB, Swendeman D, Reback CJ. Associations between major depressive episode, methamphetamine use disorder severity, and engagement in sexual risk-taking among methamphetamine-using men who have sex with men. AIDS Behav (2018a) 22(5):1461–6. doi: 10.1007/s10461-017-1974-4
30. Fletcher JB, Swendeman D, Reback CJ. Mental health and substance use disorder comorbidity among methamphetamine-using men who have sex with men. J Psychoactive Drugs (2018b) 50(3):206–13. doi: 10.1080/02791072.2018.1447173
31. Lopez-Patton M, Kumar M, Jones D, Fonseca M, Kumar AM, Nemeroff CB. Childhood trauma and METH abuse among men who have sex with men: Implications for intervention. J Psychiatr Res (2016) 72:1–5. doi: 10.1016/j.jpsychires.2015.09.009
32. Prestage G, Hammoud M, Jin F, Degenhardt L, Bourne A, Maher L. Mental health, drug use and sexual risk behavior among gay and bisexual men. Int J Drug Policy (2018) 55:169–79. doi: 10.1016/j.drugpo.2018.01.020
33. Pfeiffer-Gerschel T, Schneider F, Dammer E, Braun B, Kraus L. (2019). Methamphetaminkonsum in deutschland: verbreitung und problemlage. sucht.
34. Matos EGD, Atzendorf J, Kraus L, Piontek D. Substanzkonsum in der allgemeinbevölkerung in deutschland: ergebnisse des epidemiologischen suchtsurveys 2015. Sucht (2016) 62(5):271–81. doi: 10.1024/0939-5911/a000445
35. Milin S, Kleinau C, Lüdorf T, Lotzin A, Degkwitz P, Verthein U, et al. Konsummotive bei stimulanzienkonsum. Suchttherapie (2016) 17(01):17–21.
36. Gräfe K, Zipfel S, Herzog W, Löwe B. Screening psychischer Störungen mit dem "Gesundheitsfragebogen für Patienten (PHQ-D)". Diagnostica (2004) 50(4):171–81. doi: 10.1026/0012-1924.50.4.171
37. Kruger-Gottschalk A, Knaevelsrud C, Rau H, Dyer A, Schafer I, Schellong J, et al. The German version of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): psychometric properties and diagnostic utility. BMC Psychiatry (2017) 17(1):379. doi: 10.1186/s12888-017-1541-6
38. Schäfer I, Schulze C. Deutsche Version des" Primary CarePosttraumatic Stress Disorder screening questionnaire". Hamburg. (2010).
39. Dolatshahi B, Farhoudian A, Falahatdoost M, Tavakoli M, Rezaie Dogahe E. A qualitative study of the relationship between methamphetamine abuse and sexual dysfunction in male substance abusers. Int J High Risk Behav Addict (2016) 5(3):e29640. doi: 10.5812/ijhrba.29640
40. Miltz AR, Rodger AJ, Sewell J, Speakman A, Phillips AN, Sherr L, et al. Clinically significant depressive symptoms and sexual behaviour among men who have sex with men. BJPsych Open (2017) 3(3):127–37. doi: 10.1192/bjpo.bp.116.003574
41. Kocalevent RD, Hinz A, Brahler E. Standardization of a screening instrument (PHQ-15) for somatization syndromes in the general population. BMC Psychiatry (2013) 13:91. doi: 10.1186/1471-244x-13-91
42. Hinz A, Klein AM, Brahler E, Glaesmer H, Luck T, Riedel-Heller SG, et al. Psychometric evaluation of the generalized anxiety disorder screener GAD-7, based on a large German general population sample. J Affect Disord (2017) 210:338–44. doi: 10.1016/j.jad.2016.12.012
43. Hauffa R, Rief W, Brahler E, Martin A, Mewes R, Glaesmer H. Lifetime traumatic experiences and posttraumatic stress disorder in the German population: results of a representative population survey. J Nerv Ment Dis (2011) 199(12):934–9. doi: 10.1097/NMD.0b013e3182392c0d
44. Jacobi F, Hofler M, Siegert J, Mack S, Gerschler A, Scholl L, et al. Twelve-month prevalence, comorbidity and correlates of mental disorders in Germany: the mental health module of the german health interview and examination survey for adults (DEGS1-MH). Int J Methods Psychiatr Res (2014) 23(3):304–19. doi: 10.1002/mpr.1439
45. Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull (2003) 129(5):674–97. doi: 10.1037/0033-2909.129.5.674
46. Roy T, Lloyd CE. Epidemiology of depression and diabetes: a systematic review. J Affect Disord (2012) 142 Suppl:S8–21. doi: 10.1016/s0165-0327(12)70004-6
47. Nanni MG, Caruso R, Mitchell AJ, Meggiolaro E, Grassi L. Depression in HIV infected patients: a review. Curr Psychiatry Rep (2015) 17(1):530. doi: 10.1007/s11920-014-0530-4
48. Felker-Kantor EA, Wallace ME, Madkour AS, Duncan DT, Andrinopoulos K, Theall K. HIV Stigma, mental health, and alcohol use disorders among people living with HIV/AIDS in New Orleans. J Urban Health (2019) 1–11. doi: 10.1007/s11524-019-00390-0
49. Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, van Lunzen J, et al. Sexual activity without condoms and risk of hiv transmission in serodifferent couples when the hiv-positive partner is using suppressive antiretroviral therapy. Jama (2016) 316(2):171–81. doi: 10.1001/jama.2016.5148
50. Molina JM, Charreau I, Spire B, Cotte L, Chas J, Capitant C, et al. Efficacy, safety, and effect on sexual behaviour of on-demand pre-exposure prophylaxis for HIV in men who have sex with men: an observational cohort study. Lancet HIV (2017) 4(9):e402–10. doi: 10.1016/s2352-3018(17)30089-9
51. Hoenigl M, Chaillon A, Moore DJ, Morris SR, Smith DM, Little SJ. Clear links between starting methamphetamine and increasing sexual risk behavior: A cohort study among men who have sex with men. J Acquired Immune Defic Syndr (2016) 71(5):551–7. doi: 10.1097/QAI.0000000000000888
52. Poethko-Muller C, Zimmermann R, Hamouda O, Faber M, Stark K, Ross RS, et al. [Epidemiology of hepatitis A, B, and C among adults in Germany: results of the German Health Interview and Examination Survey for Adults (DEGS1)]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz (2013) 56(5-6):707–15. doi: 10.1007/s00103-013-1673-x
53. Wenz B, Nielsen S, Gassowski M, Santos-Hovener C, Cai W, Ross RS, et al. High variability of HIV and HCV seroprevalence and risk behaviours among people who inject drugs: results from a cross-sectional study using respondent-driven sampling in eight German cities (2011–14). BMC Public Health (2016) 16:927.
54. Murdock RM, Brizzi MB, Perez O, Badowski ME. Public health considerations among people who inject drugs with HIV/HCV co-infection: a review. Infect Dis Ther (2019) 8(1):23–32. doi: 10.1007/s40121-018-0228-8
55. Wilkerson JM, Noor SW, Rhoton JM, Li D, Rosser BRS. Differentially classified methamphetamine-using men who have sex with men: a latent class analysis. Drug Alcohol Depend (2018) 192:129–36. doi: 10.1016/j.drugalcdep.2018.07.003
56. Smith KM, Romanelli F. Recreational use and misuse of phosphodiesterase 5 inhibitors. J Am Pharm Assoc (2005) 45(1):63–72. quiz 73-65. doi: 10.1016/j.drugalcdep.2018.07.003
57. Daskalopoulou M, Rodger A, Phillips AN, Sherr L, Speakman A, Collins S, et al. Recreational drug use, polydrug use, and sexual behaviour in HIV-diagnosed men who have sex with men in the UK: results from the cross-sectional ASTRA study. Lancet HIV (2015) 1:e22–31. doi: 10.1016/s2352-3018(14)70001-3
Keywords: methamphetamine, men who have sex with men, mental health, harm reduction, HIV, chemsex
Citation: Schecke H, Lea T, Bohn A, Köhler T, Sander D, Scherbaum N and Deimel D (2019) Crystal Methamphetamine Use in Sexual Settings Among German Men Who Have Sex With Men. Front. Psychiatry 10:886. doi: 10.3389/fpsyt.2019.00886
Received: 19 September 2019; Accepted: 11 November 2019;
Published: 06 December 2019.
Edited by:
Milky Kohno, Oregon Health and Science University, United StatesReviewed by:
Robert W. Moeller, Middlebury College, United StatesCopyright © 2019 Schecke, Lea, Bohn, Köhler, Sander, Scherbaum and Deimel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Henrike Schecke, SGVucmlrZS5TY2hlY2tlQHVuaS1kdWUuZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.