
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry , 25 October 2019
Sec. Schizophrenia
Volume 10 - 2019 | https://doi.org/10.3389/fpsyt.2019.00751
 Eric Brunet-Gouet1,2,3*
Eric Brunet-Gouet1,2,3* Nils Myszkowski4,5
Nils Myszkowski4,5 Mickael Ehrminger3
Mickael Ehrminger3 Mathieu Urbach1,2,3
Mathieu Urbach1,2,3 Bruno Aouizerate1,6Lore Brunel1,7
Bruno Aouizerate1,6Lore Brunel1,7 Delphine Capdevielle1,8
Delphine Capdevielle1,8 Isabelle Chereau1,9Caroline Dubertret1,10
Isabelle Chereau1,9Caroline Dubertret1,10 Julien Dubreucq1,11
Julien Dubreucq1,11 Guillaume Fond1,12Christophe Lançon1,13Sylvain Leignier1,11Jasmina Mallet1,8David Misdrahi1,14Sylvie Pires1,9Priscille Schneider1,15Franck Schurhoff1,7Hanan Yazbek1,8Anna Zinetti-Bertschy1,15Nadine Bazin1,2,3
Guillaume Fond1,12Christophe Lançon1,13Sylvain Leignier1,11Jasmina Mallet1,8David Misdrahi1,14Sylvie Pires1,9Priscille Schneider1,15Franck Schurhoff1,7Hanan Yazbek1,8Anna Zinetti-Bertschy1,15Nadine Bazin1,2,3 Christine Passerieux1,2,3
Christine Passerieux1,2,3 Franck Zenasni5
Franck Zenasni5 Paul Roux3,2,1
Paul Roux3,2,1The Questionnaire of Cognitive and Affective Empathy (QCAE) is a tool for self-assessing the cognitive and emotional components of empathy. A study showed that a two-factor model fits the data of patients with schizophrenia, whereas other reports on healthy subjects have suggested a five-factor decomposition. We aimed to replicate the model of Horan et al. in a French population with schizophrenia spectrum disorders (i.e., schizophrenia and schizoaffective disorders) participating in the EVACO Study (NCT02901015). In total, 133 patients were assessed with the QCAE, the Positive and Negative Symptom Scale (PANSS), the Personal and Social Performance Scale (PSP), and the Self rating Quality of Life Scale (S-QoL). The two-factor model demonstrated an adequate fit with the data, comparable to that reported by Horan et al. Males scored higher on the Affective subscore than females. After correction for multiple tests, psychopathology (PANSS) and functioning (PSP) did not correlate significantly with the QCAE subscores. However, quality of life (S-QoL) correlated positively with the Emotional Contagion subscore. Thus, the variability of empathetic disposition in schizophrenia may be considered through the cognitive versus affective dichotomy and properly investigated with the QCAE. The results support further investigation of the relationship between QCAE scores and subjective outcome measurements, such as quality of life, and emphasize the importance of cross-cultural comparisons.
Schizophrenia is associated with profound impairments in social cognition that result in reduced functioning. Among the constructs of social cognition, empathy refers to the ability to represent, infer, and share the feelings and emotions of others. Both theoretical accounts and neuroscience findings acknowledge the composite nature of empathy, making it difficult to operationalize. Acknowledging it is not correlated with empathic accuracy measures (1), self-reported empathy (i.e., questionnaires) has been regularly used to better understand how individuals are disposed to empathize with others. A recent meta-analysis focused on the widely used Interpersonal Reactivity Index (IRI) (2), which allows subscore decomposition, and showed that patients with schizophrenia exhibit reduced empathic concern, perspective taking, and fantasy and increased personal distress (3). The Questionnaire of Cognitive and Affective Empathy (QCAE) gathers relevant items from other tools, including the IRI, and provides measures of both cognitive (i.e., perspective taking and online simulation) and affective (i.e., emotion contagion, proximal responsivity, and peripheral responsivity) components (4). Psychometric evaluations of the English (4), Portuguese (5), Chinese (6), Italian (7), and French (8) versions of the QCAE in healthy populations suggest a five-factor structure. However, confirmatory factor analysis in patients with schizophrenia failed to replicate this finding and showed that only a two-factor structure achieved a correct fit after a comprehensive reorganization of item parcels (9).
Noting the paucity of information on the properties of social cognition instruments in clinical populations across different languages and cultures, we provide psychometric validation data for patients with schizophrenia spectrum disorders using the French version of the QCAE (Supplementary Material 1). Previous studies showed certain discrepancies in the factorial models (i.e., five-factor vs. bifactorial model), making it necessary to replicate the findings. Additional insights into the correlations with clinical and objective/subjective outcomes are also required to better understand the potential role of the self-reported empathy in schizophrenia assessment.
We report data from adult volunteers with schizophrenia spectrum disorders (schizophrenia and schizoaffective disorder) referred to the Centers of Expertise for Schizophrenia (Foundation FondaMental) and included into the EVACO Study which is subordinated to the ongoing FACE-SZ Cohort (10). The local medical ethics committee (Comité de Protection des Personnes Ile-de-France XI, decision 2012-A00387-36) approved the study (EVACO, PHRC AOM11233).
The patients were diagnosed using a Structured Clinical Interview for assessing DSM-IV-R criteria. The study included only patients with clinically stable schizophrenia (no admission or treatment change in the past 4 weeks). Each participant received a complete description of the study in oral and written forms, gave written informed consent, and received monetary compensation.
Symptoms were assessed using the Positive and Negative Symptom Scale (11). Outcome measures, such as functioning and quality of life, were evaluated using the Personal and Social Performance Scale (PSP) (12) and the Self rating Quality of Life Scale (S-QoL) (13), respectively.
QCAE items were parcelled following the various procedures proposed by Reniers et al. (2011) and Horan et al. (2015). Confirmatory factor analyses (CFA) were then conducted using the R Lavaan package (14) to compute the robust fit indices of three models (Figure 1): 1) a five-factor first-order structure (perspective taking, online simulation, emotion contagion, proximal responsivity, and peripheral responsivity) (4), 2) a unique-factor first-order model with the revised item parcellation proposed by (9), and 3) a two-factor first-order structure with affective and cognitive factors from the same revised parcellation. The retained model was tested for correlations with demographic and clinical variables (Bonferroni correction for multiple tests was applied).
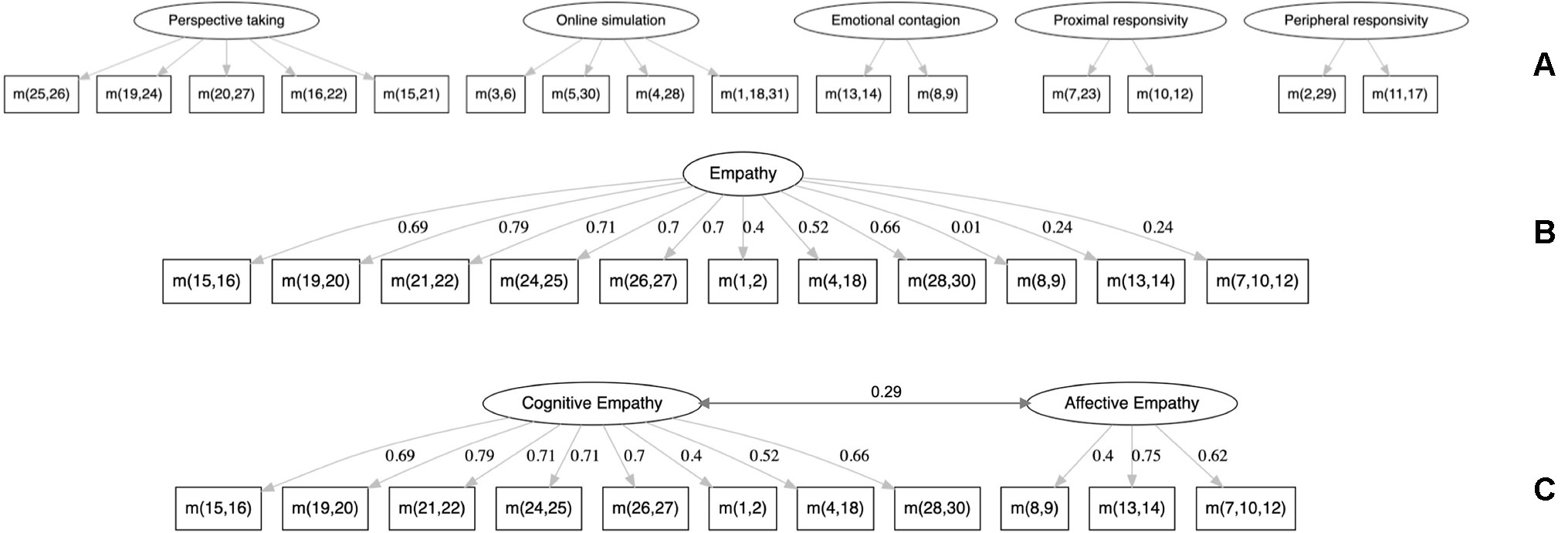
Figure 1 The three confirmatory factor analysis (CFA) models tested. (A) Five-factor first-order structure from (4). (B) Unique-factor first-order structure, without peripheral responsivity and parcellations, from (9). (C) Two-factor first-order structure from (9). m(x,y,z) signifies the mean of items x, y, and z.
In total, 105 males and 28 females were recruited. Ninety-seven were diagnosed with schizophrenia and 36 with schizoaffective disorders. Their mean age was 31.6 ± 7.8 years. Their mean scores by the PANSS were 19.3 ± 7.6 for negative symptoms, 14.3 ± 5.5 for positive symptoms, and 33.4 ± 9.6 for general psychopathology.
The subscores are reported in Table 1. The five-factor first-order model converged (RMSEA = 0.067, p of close fit = 0.088, 90% CI [0.046–0.087], CFI = 0.90, SRMR = 0.062). However, peripheral responsivity did not provide reliable estimates of regression coefficients with its two parcels. Metrological problems were previously reported with this subscore (9). Thus, we followed the recommendation of the authors to remove it and revised the parcel computation.
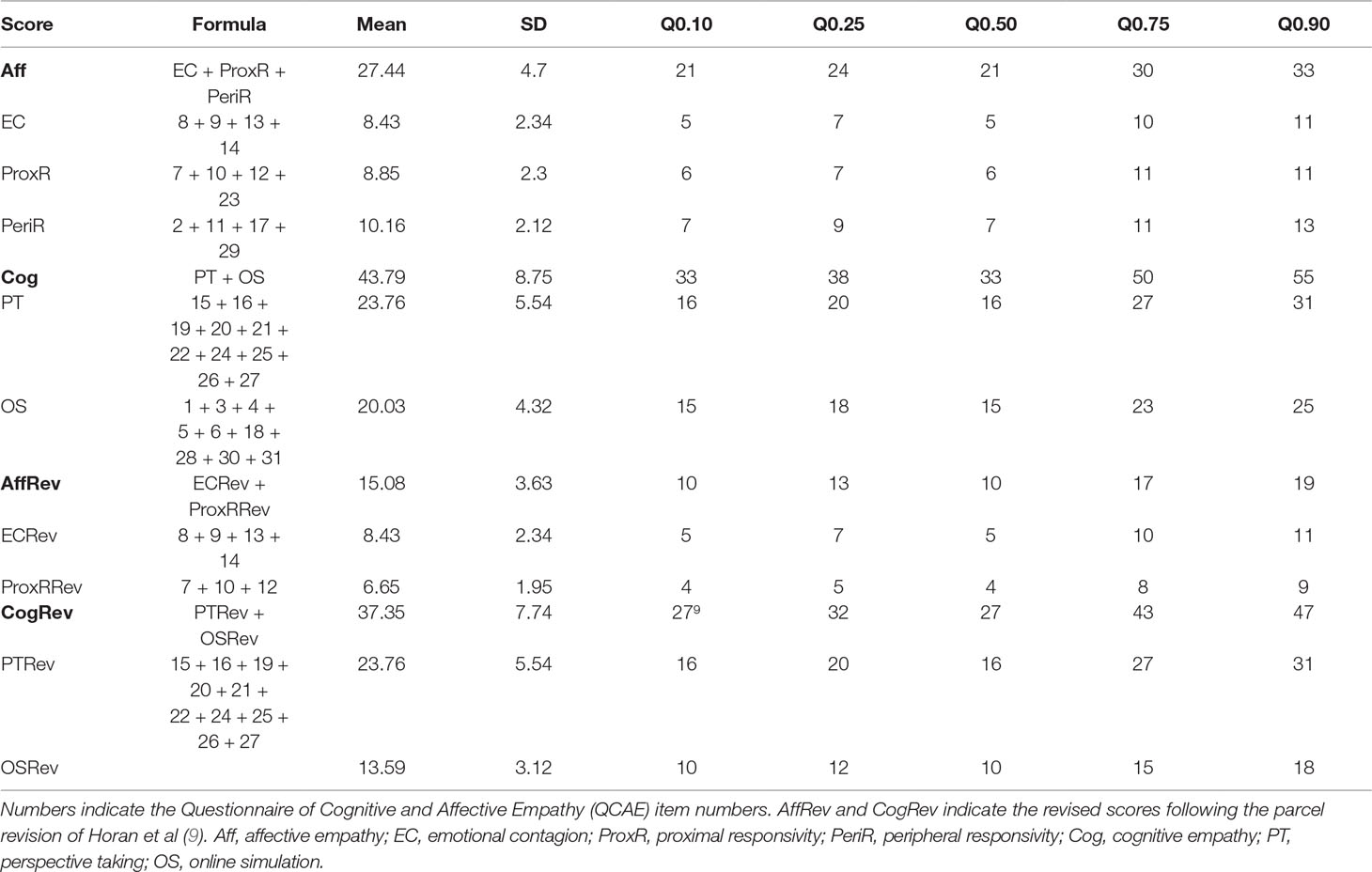
Table 1 Mean, standard deviations, and quantiles of the different scores with their formulae.
We thus tested the unique-factor model, which exhibited poor fit indices (RMSEA = 0.11, p of close fit = 0.000, 90% CI [0.091–0.137], CFI = 0.801, SRMR = 0.093).
The two-factor model adequately fits the data (RMSEA = 0.084, p of close fit = 0.019, 90% CI [0.058–0.109], CFI = 0.896, SRMR = 0.074), with the indices comparable to those reported by Horan et al. (9): RMSEA = 0.089, 90% CI [0.064–0.11], CFI = 0.91, SRMR = 0.069. All standardized factor loadings were above 0.3 and significant (p < 0.01). The correlation between the cognitive and affective factors was estimated to be 0.29 (p < 0.05). Note that this model gives similar results when applied to the subgroup of patients with schizophrenia (Supplementary Table 1).
Concerning direct comparisons, males scored higher than females at a trend level for the affective and proximal responsivity subscores (Welch tests: 15.4 vs. 14.0, t = 1.8, df = 45.4, p = 0.07 and 6.8 vs. 6.0, t = 1.9, df = 42.3, p = 0.06, respectively). Neither the age, the PANSS subscores nor the PSP exhibited significant corrected correlations with the QCAE subscores (Supplementary Table 2). The S-QoL total score correlated positively with the emotional contagion subscore (r = 0.29, p < 0.05 corrected) and showed a trend with the affective subscore (r = 0.26, p = 0.11 corrected). These findings are similar to those using the original subscores (4).
Questionnaires such as the QCAE provide simple means to assess subjective aspects of empathy through self-evaluation. The translation of this scale into French required the gathering of psychometric data for patients with schizophrenia spectrum disorders and further exploration of the main properties of this instrument. Our results confirm those of the study of Horan et al., showing that unless a better solution is proposed, the fit of the affective and cognitive bifactorial model, excluding the peripheral responsivity parcels, is acceptable and may be used for research. As our population was defined with broader criteria (adding schizoaffective disorders to the group) to be representative of the population with psychotic disorders, it is worth noting that the proposal of Horan et al. can still be used.
The retained model differed from that of studies in the healthy population, which favored a five-factor first-order structure (4–8). One interpretation is that healthy subjects may exert and assess their own social disposition in a more diverse way than patients with schizophrenia spectrum disorders who may poorly discriminate between them. A consequence for research is that caution should be used when comparing patients to healthy controls with this instrument as core structural properties depend on the group. Another consequence is that the peripheral responsivity subscore should be considered cautiously or ignored for patients with schizophrenia spectrum disorders as its items do not appear to cover a reliable construct.
Although this was only found at a trend level, self-reported proximal responsivity (i.e., emotional responsiveness to the moods of relatives) was found to be lower in females than males, and other subscores showed comparisons in the same direction. This was quite unexpected as the opposite effect was reported in healthy subjects by Reniers et al. (4). Contrary to Michaels et al., we did not find a significant correlation of empathy measures with functioning (9, 15). Similarly, psychopathology did not reveal significant relationships with empathy dispositions. Taken together with the small effect-sized findings of other studies (9, 15), these negative results emphasize the importance of investigating larger populations to determine the importance of the putative clinical expression of dispositional empathy.
In the absence of a relationship with functioning, the results with quality of life are of interest. Affective empathy/emotional contagion was positively associated with quality of life ratings, whereas cognitive empathy/perspective taking were negatively associated at a trend level. The items pertaining to the former dimension of empathy have in common that they describe the emotional disposition of the subjects toward others. The items of emotional empathy reflect a sense of closeness to others, which may explain the positive association with quality of life. In contrast, the negative correlation between perspective taking and quality of life is intriguing and should be investigated further because this did not reach the corrected significance threshold. However, the identification of factors that negatively influence quality of life is of clinical importance as they may favor depression and suicidality (16).
In conclusion, this study demonstrates the possibility of using self-administered empathy questionnaires in patients with schizophrenia spectrum disorders and suggests, through confirmatory factor analysis, that the structure of the QCAE tool is robust to language change in a clinical population. Intercultural studies should give priority to establishing the instrument’s properties in terms of measurement invariance in order to open up the possibility of making large-scale comparisons of international populations.
The datasets generated for this study will not be made publicly available. These data belong to the FondaMental network of Center of Expertise.
The studies involving human participants were reviewed and approved by Comité de Protection des Personnes Ile-de-France XI, decision 2012-A00387-36. The patients/participants provided their written informed consent to participate in this study.
Conceptualization: EB-G, PR, and CP. Methodology: EB-G and PR. Formal analysis: EB-G, PR, and ME. Investigation: MU, BA, LB, DC, IC, CD, JD, GF, CL, SL, JM, DM, SP, PS, FS, HY, and AZ-B. Writing—preparation of the original draft: EB-G, PR, and ME. Writing—review and editing: all authors. Supervision and project administration: EB-G. Funding acquisition: EB-G and CP.
The study was supported by the Centre Hospitalier de Versailles, Le Chesnay, France and the Fondation FondaMental, Créteil, France; and funded by the Programme Hospitalier de Recherche Clinique (AOM11233); the Investissements d’Avenir program managed by the Agence Nationale de la Recherche (ANR-11-IDEX-0004-02 and ANR-10-COHO-10-01); and the Institut National de la Santé et de la Recherche Médicale.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank K. Souyris from the Fondation Fondamental for data management and A. Cattenoy and L. Morisset from the Maison de la Recherche at Versailles Hospital for administrative support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00751/full#supplementary-material
1. van Donkersgoed RJM, de Jong S, aan het Rot M, Wunderink L, Lysaker PH, Hasson-Ohayon I, et al. Measuring empathy in schizophrenia: the empathic accuracy task and its correlation with other empathy measures. Schizophr Res (2019) 208:153–9. doi: 10.1016/j.schres.2019.03.024
2. Davis MH. Measuring individual differences in empathy: evidence for a multidimensional approach. J Pers Soc Psychol (1983) 44(1):113–26. doi: 10.1037//0022-3514.44.1.113
3. Bonfils KA, Lysaker PH, Minor KS, Salyers MP. Empathy in schizophrenia: a meta-analysis of the interpersonal reactivity index. Psychiatry Res (2017) 249:293–303. doi: 10.1016/j.psychres.2016.12.033
4. Reniers RL, Corcoran R, Drake R, Shryane NM, Vollm BA. The QCAE: a questionnaire of cognitive and affective empathy. J Pers Assess (2011) 93(1):84–95. doi: 10.1080/00223891.2010.528484
5. Queirós A, Fernandes E, Reniers R, Sampaio A, Coutinho J, Seara-Cardoso A. Psychometric properties of the questionnaire of cognitive and affective empathy in a Portuguese sample. Tran US, editor. PLOS ONE (2018) 13(6):e0197755. doi: 10.1371/journal.pone.0197755
6. Liang Y, Yang H, Ma Y, Lui SSY, Cheung EFC, Wang Y, et al. Validation and extension of the questionnaire of cognitive and affective empathy in the Chinese setting. PsyCh J (2019). doi: 10.1002/pchj.281
7. Di Girolamo M, Giromini L, Winters CL, Serie CMB, de Ruiter C. The questionnaire of cognitive and affective empathy: a comparison between paper-and-pencil versus online formats in Italian samples. J Pers Assess (2019) 101(2):159–70. doi: 10.1080/00223891.2017.1389745
8. Myszkowski N, Brunet-Gouet E, Roux P, Robieux L, Malezieux A, Boujut E, et al. Is the questionnaire of cognitive and affective empathy measuring two or five dimensions? Evidence in a French sample. Psychiatry Res (2017) 255:292–6. doi: 10.1016/j.psychres.2017.05.047
9. Horan WP, Reise SP, Kern RS, Lee J, Penn DL, Green MF. Structure and correlates of self-reported empathy in schizophrenia. J Psychatry Res (2015) 66–67:60–6. doi: 10.1016/j.jpsychires.2015.04.016
10. Schürhoff F, Fond G, Berna F, Bulzacka E, Vilain J, Capdevielle D, et al. A national network of schizophrenia expert centres: an innovative tool to bridge the research–practice gap. Eur Psychiatry (2015) 30(6):728–35. doi: 10.1016/j.eurpsy.2015.05.004
11. Kay SR, Fisz-Bein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS). Schizophr Bull (1987) 13:261–74. doi: 10.1093/schbul/13.2.261
12. Nasrallah H, Morosini P, Gagnon DD. Reliability, validity and ability to detect change of the personal and social performance scale in patients with stable schizophrenia. Psychiatry Res (2008) 161(2):213–24. doi: 10.1016/j.psychres.2007.11.012
13. Auquier P, Simeoni MC, Sapin C, Reine G, Aghababian V, Cramer J, et al. Development and validation of a patient-based health-related quality of life questionnaire in schizophrenia: the S-QoL. Schizophr Res (2003) 63(1–2):137–49. doi: 10.1016/S0920-9964(02)00355-9
14. Rosseel Y. lavaan: an R package for structural equation modeling. J Stat Softw (2012) . [cited 2019 May 21];48(2):1–36. Available from: http://www.jstatsoft.org/v48/i02/ doi: 10.18637/jss.v048.i02
15. Michaels TM, Horan WP, Ginger EJ, Martinovich Z, Pinkham AE, Smith MJ. Cognitive empathy contributes to poor social functioning in schizophrenia: evidence from a new self-report measure of cognitive and affective empathy. Psychiatry Res (2014) 220(3):803–10. doi: 10.1016/j.psychres.2014.08.054
Keywords: schizophrenia spectrum, empathy, assessment method, quality of life, functioning
Citation: Brunet-Gouet E, Myszkowski N, Ehrminger M, Urbach M, Aouizerate B, Brunel L, Capdevielle D, Chereau I, Dubertret C, Dubreucq J, Fond G, Lançon C, Leignier S, Mallet J, Misdrahi D, Pires S, Schneider P, Schurhoff F, Yazbek H, Zinetti-Bertschy A, Bazin N, Passerieux C, Zenasni F and Roux P (2019) Confirmation of a Two-Factor Solution to the Questionnaire of Cognitive and Affective Empathy in a French Population of Patients With Schizophrenia Spectrum Disorders. Front. Psychiatry 10:751. doi: 10.3389/fpsyt.2019.00751
Received: 18 July 2019; Accepted: 18 September 2019;
Published: 25 October 2019.
Edited by:
Francesco Papaleo, Italian Institute of Technology, ItalyReviewed by:
Vaibhav A. Diwadkar, Wayne State University, United StatesCopyright © 2019 Brunet-Gouet, Myszkowski, Ehrminger, Urbach, Aouizerate, Brunel, Capdevielle, Chereau, Dubertret, Dubreucq, Fond, Lançon, Leignier, Mallet, Misdrahi, Pires, Schneider, Schurhoff, Yazbek, Zinetti-Bertschy, Bazin, Passerieux, Zenasni and Roux. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eric Brunet-Gouet, ZWJydW5ldEBjaC12ZXJzYWlsbGVzLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.