
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 06 June 2019
Sec. Schizophrenia
Volume 10 - 2019 | https://doi.org/10.3389/fpsyt.2019.00393
This article is part of the Research Topic Early Intervention in Psychotic Disorders View all 13 articles
 Maximus Berger1,2*
Maximus Berger1,2* Barnaby Nelson1,2
Barnaby Nelson1,2 Connie Markulev1,2Hok Pan Yuen1,2Miriam R. Schäfer1,2
Connie Markulev1,2Hok Pan Yuen1,2Miriam R. Schäfer1,2 Nilufar Mossaheb3,4
Nilufar Mossaheb3,4 Monika Schlögelhofer3Stefan Smesny5Ian B. Hickie6
Monika Schlögelhofer3Stefan Smesny5Ian B. Hickie6 Gregor E. Berger7Eric Y. H. Chen8
Gregor E. Berger7Eric Y. H. Chen8 Lieuwe de Haan9
Lieuwe de Haan9 Dorien H. Nieman9Merete Nordentoft10
Dorien H. Nieman9Merete Nordentoft10 Anita Riecher-Rössler11
Anita Riecher-Rössler11 Swapna Verma12Todd W. Mitchell13,14Barbara J. Meyer13,14
Swapna Verma12Todd W. Mitchell13,14Barbara J. Meyer13,14 Andrew Thompson1,2Alison Ruth Yung1,2,15Patrick D. McGorry1,2
Andrew Thompson1,2Alison Ruth Yung1,2,15Patrick D. McGorry1,2 G. Paul Amminger1,2
G. Paul Amminger1,2Background: Deficiencies in membrane polyunsaturated fatty acids (PUFA) such as omega-3 (n-3) fatty acids are thought to contribute to the pathophysiological processes underlying psychotic disorders. Emerging evidence suggests that the levels of PUFA are related to clinical symptoms but significant heterogeneity exists between studies. Here, we investigated associations of membrane PUFA with clinical symptoms and functioning in a large sample of individuals at ultra-high risk (UHR) for psychosis.
Methods: A total of 285 participants of the NEURAPRO clinical trial were investigated for erythrocyte PUFA levels, including the n-3 index, n-6/n-3 PUFA ratio, docosahexaenoic acid (DHA), and eicosapentaenoic acid (EPA). Severity of general psychopathology [Brief Psychiatric Rating Scale (BPRS)], psychotic symptoms (BPRS psychosis subscale), negative symptoms [Scale for the Assessment of Negative Symptoms (SANS)], manic symptoms [Young Mania Rating Scale (YMRS)], depressive symptoms [Montgomery Asberg Depression Rating Scale (MADRS)], and functioning [Social and Occupational Functioning Scale (SOFAS), Global Functioning Social (GF-S) and Role (GF-R) scales] were assessed concurrently. Partial correlation taking into account the effects of gender, age, and smoking was used to examine the relationship between PUFAs and symptoms severity.
Results: The n-3 index negatively correlated with the severity of general psychopathology, psychotic symptoms, depressive symptoms, and manic symptoms. The n-6/n-3 PUFA ratio positively correlated with severity of psychotic and depressive symptoms. The n-3 PUFA DHA negatively correlated with the severity of general psychopathology, positive, manic, and depressive symptoms. EPA negatively correlated with manic symptoms. Nervonic acid, an n-9 monounsaturated fatty acid, positively correlated with general psychopathology, positive and negative symptoms, depressive symptoms, and manic symptoms. The long-chain saturated fatty acid tetracosanoic acid positively correlated with general psychopathology, positive, manic, and depressive symptoms.
Conclusions: Partially consistent with a previous study, psychotic symptoms, depressive symptoms, and symptoms of mania were associated with several classes of FAs in the present study. These findings support the relevance of membrane fatty acids for the onset of psychotic symptoms and indicate that FAs should be further evaluated as biomarkers in the UHR for psychosis group.
Clinical Trial Registration: ANZCTR, identifier: 12608000475347
Young people at ultra-high risk (UHR) for psychosis have an elevated risk of developing psychosis of about 20% within 2 years and a significant risk for non-psychotic disorders (1, 2). The biological correlates underlying this risk state remain poorly understood but emerging evidence suggests the involvement of brain structural and functional alterations as well as peripheral pathology including immune activation, oxidative stress, endocrine abnormalities and deregulation of membrane lipid metabolism (3, 4). Given that it is currently unclear how to determine the biological risk for psychosis transition and other clinically relevant outcomes and how to develop treatments that target specific pathophysiological processes, it is important to elucidate the biological processes accompanying the UHR state. Moreover, declining transition rates in individuals who are clinically identified as being at UHR for psychosis (5) as well as uncertainty about the efficacy of specific interventions (6, 7) further add to the need to refine and improve risk prediction and consequently the identification of predictive biomarkers.
Deficits in long-chain omega-3 (n-3) polyunsaturated fatty acids (PUFAs) are one mechanism thought to contribute to psychosis risk (8, 9). In fact, n-3 PUFAs are integral components of the lipid bilayer forming the cell membrane and are found in high abundance in the human brain (10). There, they modulate the rigid formation of tightly packed saturated fatty acids through their structural characteristics, thereby also contributing to the biophysical properties of the neuronal membrane (11, 12). These in turn affect the function of ion channels and neurotransmitter receptors. Importantly, n-3 PUFA are essential fatty acids, meaning that their abundance in cell membranes is determined by intake from food and metabolic conversion. The lipid derivates of n-3 PUFA include anti-inflammatory eicosanoids such as resins and resolvins, which mediate the effects of n-3 PUFA on immune function (13, 14). Molecules derived from n-6 PUFA in contrast are known to have pro-inflammatory properties. First postulated by Horrobin et al. (15), the phospholipid structure of the cell membrane may be altered in schizophrenia and such alterations may contribute to various aspects of the pathophysiology observed in psychotic disorders, including neurotransmission, immune activation, and antioxidative defense. This is supported by studies showing n-3 PUFA deficiency in patients with schizophrenia compared to controls (16). Much less is known about the UHR for psychosis state, but evidence suggests lower levels of several n-3 and n-6 PUFA (17). Additionally, the balance between n-3 and n-6 PUFA, which is often seen as an indicator of immune activation, seems to be associated with depression in young people at UHR for psychosis (18).
More recently, clinical trials have tested the efficacy of n-3 PUFA for the prevention of psychosis transition in UHR individuals (19–21). While the first single-center trial showed significant benefits of n-3 PUFA over placebo in terms of the transition to psychosis risk (19), a multicenter replication study failed to show significant effects of n-3 PUFA supplementation on the transition rate (21). Possible reasons for the failure to replicate a reduction of transitions include true inefficacy of n-3 PUFA in this particular outcome measure, the background intervention of high-quality psychosocial care in both groups that may have created a ceiling effect, the use of antidepressants, or the high rate of non-adherence (57%) (22). Importantly, investigating the relationship between pre-treatment PUFA levels and symptom measures can provide further insight into potential mechanisms underlying lipid biology in regard to psychosis risk. A secondary analysis of the original single-center trial revealed associations of several classes of fatty acids with clinical symptoms and psychosocial functioning (23). In light of these observations, it seems important to replicate the findings of the original trial in the larger sample of the NEURAPRO clinical trial.
The aim of the present analysis was to examine associations of the cell membrane levels of fatty acids with clinical symptoms and functioning at baseline (i.e., prior to the intervention) in the NEURAPRO RCT. Specifically, we hypothesized that the n-3 index would be associated with less severe symptoms and better functioning. Given the limited evidence for fatty acid variations in the UHR stage, we did not formulate specific hypotheses for other fatty acid classes.
The study cohort consisted of 285 of 304 (94%) participants in the NEURAPRO study who provided consent for additional biomarker analysis. NEURAPRO was a double-blind placebo-controlled randomized clinical trial of fish oil (1.4 g fish oil/day) in people at UHR for psychosis (21) (ANZCTR identifier: 12608000475347) with 10 study sites (Amsterdam, Basel, Copenhagen, Jena, Hong Kong, Melbourne, Singapore, Sydney, Vienna, and Zurich). The intervention was administered in addition to cognitive behavioral case management (CBCM) for 6 months followed by a 6-month follow-up period. Help-seeking individuals attending UHR services in the trial centers were eligible if they were aged 13–40 years and met UHR criteria (24, 25). Exclusion criteria were a previous psychotic episode, acute intoxication, organic brain disease, serious developmental disorder, abnormal coagulation profile or thyroid function, physical illness with a psychotropic effect, current treatment with mood stabilizers, past neuroleptic exposure to a total lifetime haloperidol equivalent dose of more than 50 mg, IQ of less than 70, dangerous behavior, aggression or suicidality, pregnancy, or current supplementation with n-3 PUFA (25). All participants provided written informed consent (parent/guardian consent for participants aged <17 years). The NEURAPRO study was approved by the local human research ethics committees of the study centers.
Psychiatric symptoms at baseline were assessed with the Brief Psychiatric Rating Scale (BPRS), the Scale for the Assessment of Negative Symptoms (SANS), the Montgomery Asberg Depression Rating Scale (MADRS) for depressive symptoms, the Young Mania Rating Scale (YMRS) for manic symptoms, the Social and Occupational Functioning Scale (SOFAS), and the Global Functioning Social (GF-S) and Role (GF-R) scales.
Total fatty acid levels were quantified from erythrocyte samples collected at baseline. Erythrocytes were separated from plasma and extracted using an automated extraction method described previously by (26). Fatty acid levels were measured using mass spectrometry utilizing a hybrid triple quadrupole linear ion trap mass spectrometer (QTRAP 5500 AB Sciex, MA, USA) with an automated chip-based nanoelectrospray source (Triversa NanoMate, Advion Biosciences, New York, USA). Ionized lipids identified with a minimum signal-to-noise ratio of 10 were included in the analysis. Identification and quantification was accomplished using LipidView (v1.2, Sciex, MA, USA). Quantification was performed using LipidView software by comparing the spectral peak area of individual lipids to their class specific internal standards following isotope correction. Mass spectrometry is unable to identify fatty acid double bond isomers which limited our ability to distinguish between 18:1n-7/9, 20:3n-3/6/9 and 22:5n-3/6, respectively.
The n-3 index was calculated as the proportion of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) expressed as percent of total fatty acids. The n-6/n-3 PUFA ratio was calculated as arachidonic acid (AA) divided by the sum of EPA and DHA. To examine the relationship between PUFA and psychopathology, partial correlation coefficients (adj. R) were calculated adjusting for age, gender, and smoking, as these covariates have been found to influence both fatty acid levels and psychopathology. Given the explorative nature of the study and the fact that variations in PUFA concentrations in the UHR stage is still in a hypothesis-generating phase, we did not to correct for multiple testing. The significance for all tests was set at α < 0.05. Stata 13.1 (StataCorp, College Station, TX, USA) for Mac OS was used for all analyses.
Relevant demographic and psychological variables are presented Table 1. The sample comprised 285 participants (mean age 19.0 years ± 4.5; 45.26% male).
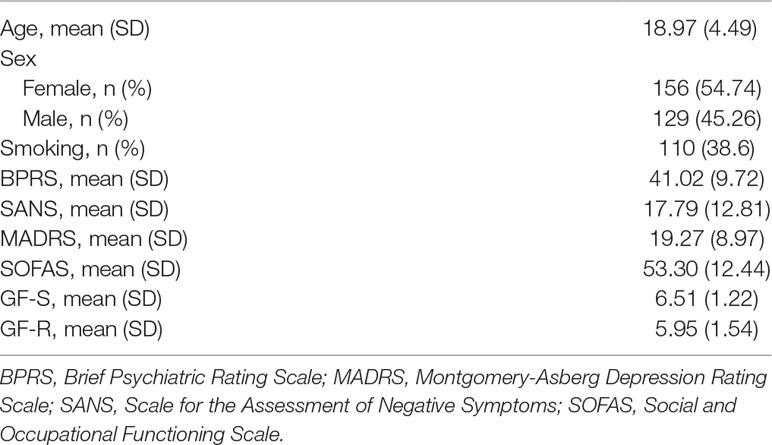
Table 1 Demographic and clinical characteristics and inflammatory markers of 285 NEURAPRO study participants.
Partial correlations between fatty acids and related indices and psychological variables, adjusted for age, gender and smoking, are reported in Table 2. BPRS scores were positively correlated with 24:0 (p < 0.001), 24:1n-9 (p < 0.001) and the n-6/3 PUFA ratio (p=0.01), and negatively correlated with the n-3 index (p=0.003), 20:3 (p=0.010), 22:6n-3 (p < 0.001), 20:4n-6 (p=0.037) and 18:2n-6 (p < 0.001). The BPRS psychotic symptoms sub-scale was positively correlated with 24:1n-9 (p=0.009) and with the n-6/3 PUFA ratio (p=0.01), and negatively correlated with 18:2n-6 (p=0.04) and the n-3 index (p=0.008). Negative symptoms (SANS) were positively correlated with 24:0 (p < 0.001) and 24:1n-9 (p < 0.001) and negatively correlated with 16:0 (p < 0.001), 20:3 (p < 0.001), 18:2n-6 (p < 0.001) and 18:1 (p=0.004).
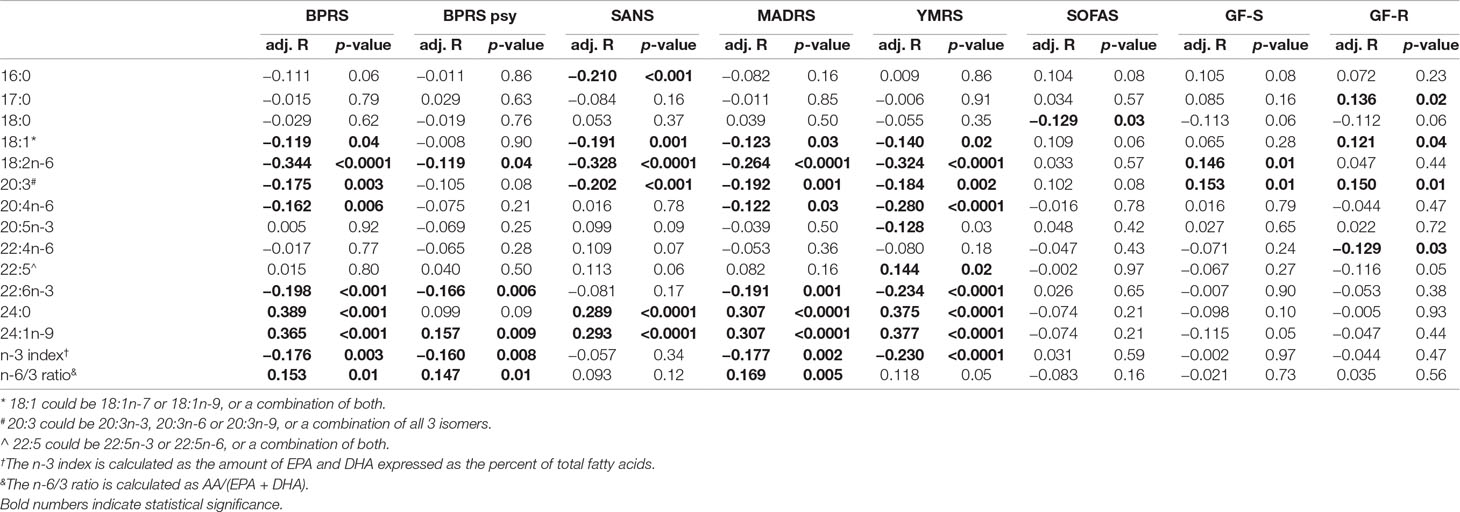
Table 2 Partial correlations of fatty acids with symptom and functioning scores in 285 participants of the Neurapro-E study.
YMRS scores were positively correlated with 24:0 (p < 0.0001) and 24:1n-9 (p < 0.0001) and negatively correlated with 20:3 (p=0.002),20:5n-3 (p=0.03), 22:6n-3 (p < 0.0001), 18:2n-6 (p < 0.0011), 20:4n-6 (p < 0.0001) and the n-3-index (p < 0.0001). MADRS scores were positively correlated with 24:0 (p < 0.0001), 24:1n-9 (p < 0.0001) and the n-6/3 PUFA ratio (p=0.005), and negatively correlated with the n-3-index (p=0.002), 20:3 (p=0.001), 22:6n-3 (p=0.001), 18:2n-6 (p < 0.0001), 20:4n-6 (p=0.03) and 18:1 (p=0.03). SOFAS scores were negatively correlated with 18:0 (p=0.031). GF-S scores were positively correlated with 18:2n-6 (p < 0.01) and 20:3 (p=0.01). Finally, GF-R scores were positively correlated with 17:0 (p=0.02), 18:1 (p=0.04), 22:4n-6 (p=0.03) and 20:3 (p=0.01).
The aim of this study was to investigate associations of cell membrane fatty acids with clinical characteristics in a large multi-centre RCT of fish oil supplementation in individuals at UHR for psychosis. After taking into account the effects of age, gender and smoking, we found several PUFAs related to psychopathology, including general psychopathology (BPRS), psychotic symptoms (BPRS), negative symptoms (SANS), manic symptoms (YMRS) and depressive symptoms (MADRS). The n-3 index, DHA, AA, 20:3, and 18:2n6 were negatively correlated with BPRS, MADRS and YMRS scores, while the n-6/3 PUFA ratio was positively correlated with general psychopathology (BPRS), psychotic symptoms (BPRS) and depressive symptoms (MADRS). 24:0 and 24:1n-9 in turn were significantly positively correlated with BPRS, SANS, MADRS and YMRS scores. Collectively, these findings support the notion that several classes of fatty acids are associated with symptom severity in this group.
Our analysis contributes important insights into the relationship between PUFA and psychopathology by replicating findings of our previous smaller study in UHR (23) in a large (n=285) and well-characterised sample. Overall, our results confirm that higher levels of n-3 PUFA (n-3 index) correspond to fewer symptoms in this population. The n-3 index, calculated as the sum of EPA and DHA as percent of total fatty acids, was significantly associated with lower general psychopathology (BPRS) scores, which is broadly consistent with a previous study (27), as well as with lower manic (YMRS) and depressive (MADRS) symptoms. The n-6/n-3 PUFA ratio, reflective of the balance between n-3 and n-6 PUFA, was positively correlated with psychotic symptoms (BPRS) and MADRS scores, suggesting that a higher relative proportion of n-6 PUFA compared to n-3 PUFA correlates with more severe symptoms. Consistent with the present findings, Kim et al. (23) found that the n-6/n-3 PUFA ratio was associated with psychotic symptoms, and the sum of n-3 PUFA negatively with negative symptoms. This suggests that the n-3 index is relevant to a range of symptoms in the UHR state. Consistent with this, DHA was also associated with lower BPRS scores in our study. DHA is the most abundant n-3 PUFA in the human brain and integral to the neuronal membrane. Importantly, erythrocyte DHA correlates with grey matter DHA (28) and may be particularly relevant during adolescence, where increases in the level of DHA may be critical for the development of the prefrontal cortex and cortical maturation more generally (29–31). Given that the UHR state and the onset of psychotic disorders fall within this developmental period in many cases, n-3 PUFA including DHA may play a particularly important role in this phase.
Our results also support an association of the n-3 index and the n-6/n-3 PUFA ratio with depressive symptoms in this UHR cohort. Considering that young people at UHR for psychosis have a high risk for depression of up to 42% (1), these findings are highly relevant to the UHR group. There is ample evidence to support n-3 PUFA deficiency in patients with major depressive disorders (32) and for the efficacy of n-3 PUFA as a potential treatment of depressive symptoms [see meta-analyses in Refs. (33–35)]. Moreover, we recently reported that in individuals at UHR for psychosis, a high n-6/n-3 PUFA ratio is predictive of depression within a 7-year follow-up (18). Our present findings support an association of the n-3 index as well as of DHA levels with depressive symptoms, thereby confirming previous results. However, EPA, the n-3 PUFA found to be most effective for the treatment of depression (34), was not related to depressive symptoms in this study.
In addition to n-3 PUFA, linoleic acid (18:2), an n-6 PUFA and precursor to arachidonic acid, EPA and DHA, was inversely associated with symptoms severity and positively associated with functioning. Previous studies examining the relationship between linoleic acid and psychopathology have yielded mixed results. For example, in a recent study of 154 patients with major depressive disorder, linoleic acid was found to be reduced compared to controls and inversely correlated with depressive symptoms severity (36). Similarly, in a population-based study of otherwise healthy adults, low levels of linoleic acid were associated with depressive symptoms (37). However, other studies found no association of linoleic acid with depression (38, 39). While our results suggest that linoleic acid is associated with fewer symptoms and better functioning, these observations warrant further confirmation.
An interesting observation in our study was that tetracosanoic acid (lignoceric acid; 24:0), a very long chain saturated fatty acid mainly found in peanut and canola oil (40), was strongly positively correlated with all symptom scores. Few studies to date have investigated saturated fatty acids in the UHR group. Of note, Hamazaki et al. (41) found elevated levels of these fatty acids in post-mortem brain tissue of patients with schizophrenia compared to controls.
The mechanisms linking deficits in n-3 PUFA with psychopathology in the UHR group are only partially understood but likely include effects on serotonergic and dopaminergic neurotransmission through the modulation of membrane fluidity and ion channel function (42), PUFA effects on HPA axis regulation and the regulation of antioxidative defense (43), as well as the production of pro- and anti-inflammatory derivatives of PUFA (14, 44, 45). EPA rapidly beta-oxidized once in the brain (46, 47), and oxidation products are not specific for EPA. Therefore, EPA effects in depression cannot be explained by effects in the brain; rather, peripheral anti-inflammatory effects may be relevant. EPA’s oxidation products are anti-inflammatory eicosanoids, and oxidative stress as seen in psychiatric disorders would only increase these. This is supported by Rapaport et al. (48), who showed that high inflammation is a predictor of response to n-3 PUFA supplementation.
Other fatty acids related to psychopathology in our study include NA. NA, an n-9 monounsaturated fatty acid, is abundant in the white matter of the central nervous system and important for the biosynthesis and maintenance of the myelin sheath. For example, the levels of NA (but also AA and DHA) were found to be related to decreased white matter integrity in the corpus callosum, parietal, occipital, temporal, and frontal lobes (49). Impaired myelin pathways and impairments in white matter integrity in the medial frontal lobe and other brain areas relevant to psychosis have been observed in individuals who later transitioned to psychosis (50). Decreased levels of NA have previously been observed in association with more severe psychotic symptoms and with higher transition risk (23, 51). The present findings seem difficult to reconcile as they suggest the opposite relationship. However, differences in the methodology between the present study and previous studies may explain these discrepancies (52). While Amminger et al. (51) measured NA from the phosphatidylethanolamine fraction of erythrocytes using gas chromatographic analysis, NA was quantified in this study from whole erythrocyte membranes using mass spectrometry. In patients with major depressive disorder, where white matter dysfunction is similarly hypothesized, both increases and decreases in NA have been observed (52, 53).
An important question not answered by our study is whether young individuals at UHR for psychosis show deficits in those n-3 PUFAs associated with more severe symptoms compared to healthy (non-UHR) individuals. To date, only one study of our group addressed this question and reported deficits in two n-3 PUFAs and several n-6 PUFAs (17). We are currently investigating this question in the NEURAPRO trial and a matched control group. Studies in patients with chronic schizophrenia provided heterogeneous findings and showed decreases in AA, DPA, and DHA (54). However, several studies in schizophrenia patients including a more recent study showed increases in these fatty acids in patients compared to controls as well as in unaffected siblings compared to controls (55–57). Findings in youth at UHR for bipolar disorder showed deficits in the n-3-index compared to healthy controls (58, 59). It therefore seems important to clarify if low n-3 PUFA levels precede the onset of psychosis.
A strength of our study is the sample size, making this the largest examination of membrane PUFA in UHR to date. A second strength is the well-characterized sample and the availability of a variety of clinical measures. Limitations include the cross-sectional nature of this analysis, which precludes causal inferences. The effects sizes of several correlations reported here—while statistically significant—are small (adj. R < 0.2). Also, the selection of fatty acids measured is not fully consistent with a previous study (23) due to the choice of methods used for the analysis. The present study used mass spectrometry, a novel method recently published (26), while previous studies used mostly gas chromatography. While dietary habits were not considered here, we argue that membrane PUFA status is a valid biological measure of lipid biology irrespective of source. Finally, we did not correct for multiple comparisons in the present study due to its exploratory nature.
Future studies should further confirm if the UHR for psychosis group has deficits in PUFA compared to healthy individuals as well as other high-risk groups; clarify causality by testing whether the relationship with clinical symptoms persists at follow-up and is predictive of treatment response and long-term remission; if supplementation with fish oil can reverse potential deficits and associations with psychopathology; and whether the relationship between lipid biology and symptoms is attributable to inflammation or other biological mechanisms that may serve as potential treatment targets.
In conclusion, our study confirms that membrane PUFAs are associated with the severity of clinical symptoms in individuals at UHR for psychosis. In particular, we found that the n-3 index was negatively correlated with multiple measures, including total BPRS scores, MADRS, and YMRS scores. These results suggest that n-3 PUFA are important in the pathophysiology of the UHR state and may indicate risk for poor mental health outcomes. Given that recent RCTs of n-3 PUFA in the UHR were unable to demonstrate superiority of n-3 PUFA over placebo for transition to psychosis, biomarker studies are warranted to clarify if low n-3 PUFA levels predispose for adverse outcomes and are indicative of treatment response with n-3 PUFA.
This study was approved by the local human ethics review board of each site (Melbourne, Australia: Melbourne Health Research Ethics Committee; Sydney, Australia: Sydney South West Area Health Service Ethics Review Committee; Basel, Switzerland: Ethics Commission for Basel; Zurich, Switzerland: Cantonal Ethics Commission Zurich; Jena, Germany: University Clinic Jena Ethics Commission; Copenhagen, Denmark: Capital Region Research Ethics Committee; Hong Kong: Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster; Vienna, Austria: Medical University of Vienna Ethics Commission; Singapore: National Healthcare Group Domain Specific Review Board; and Amsterdam, the Netherlands: Academic Medical Centre Medical Ethics Committee). This study was carried out in accordance with the Declaration of Helsinki and The National Health and Medical Research Council of Australia National Statement on Human Research with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki.
MB and GA designed the study. MB analyzed the data and wrote the manuscript. BN, CM, HY, MRS, NM, MS, SS, IH, GB, EC, LH, DN, MN, AR-R, SV, AY, PM, and GA contributed to the primary study that provided data for this analysis, including acquisition of funding, recruitment of participants, and/or collection of data. TM and BM analyzed erythrocyte fatty acids. All authors contributed to the interpretation of results and to the manuscript.
The NEURAPRO clinical trial was supported by grant 07TGF-1102 from the Stanley Medical Research Institute, grant 566529 from the NHMRC Australia, and a grant from the Colonial Foundation. The analysis of fatty acids was supported by grant 1128631 from the NHMRC Australia. MB is supported by a MACH Translational Research Fellowship. GB is supported by the Swiss National Science Foundation (SNF 33IC30_166826).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank the participants and their families.
1. Lin A, Wood SJ, Nelson B, Beavan A, Mcgorry P, Yung AR. Outcomes of nontransitioned cases in a sample at ultra-high risk for psychosis. Am J Psychiatry (2015) 172:249–58. doi: 10.1176/appi.ajp.2014.13030418
2. Fusar-Poli P, Cappucciati M, Borgwardt S, Woods SW, Addington J, Nelson B, et al. Heterogeneity of psychosis risk within individuals at clinical high risk: a meta-analytical stratification. JAMA Psychiatry (2016) 73:113–20. doi: 10.1001/jamapsychiatry.2015.2324
3. Davis J, Moylan S, Harvey BH, Maes M, Berk M. Neuroprogression in schizophrenia: pathways underpinning clinical staging and therapeutic corollaries. Aust N Z J Psychiatry (2014) 48:512–29. doi: 10.1177/0004867414533012
4. McGorry P, Keshavan M, Goldstone S, Amminger P, Allott K, Berk M, et al. Biomarkers and clinical staging in psychiatry. World Psychiatry (2014) 13:211–23. doi: 10.1002/wps.20144
5. Fusar-Poli P, Bonoldi I, Yung AR, Borgwardt S, Kempton MJ, Valmaggia L, et al. Predicting psychosis: meta-analysis of transition outcomes in individuals at high clinical risk. Arch Gen Psychiatry (2012) 69:220–9. doi: 10.1001/archgenpsychiatry.2011.1472
6. Davies C, Cipriani A, Ioannidis JPA, Radua J, Stahl D, Provenzani U, et al. Lack of evidence to favor specific preventive interventions in psychosis: a network meta-analysis. World Psychiatry (2018a) 17:196–209. doi: 10.1002/wps.20526
7. Davies C, Radua J, Cipriani A, Stahl D, Provenzani U, Mcguire P, et al. Efficacy and acceptability of interventions for attenuated positive psychotic symptoms in individuals at clinical high risk of psychosis: a network meta-analysis. Front Psychiatry (2018b) 9:187. doi: 10.3389/fpsyt.2018.00187
8. Amminger GP, Mcgorry PD. Update on omega-3 polyunsaturated fatty acids in early-stage psychotic disorders. Neuropsychopharmacology (2012) 37:309–10. doi: 10.1038/npp.2011.187
9. Amminger GP, Berger M, Rice SM, Davey CG, Schafer MR, Mcgorry PD. Novel biotherapies are needed in youth mental health. Australas Psychiatry (2017) 25:117–20. doi: 10.1177/1039856217698237
10. Dyall SC. Long-chain omega-3 fatty acids and the brain: a review of the independent and shared effects of EPA, DPA and DHA. Front Aging Neurosci (2015) 7:52. doi: 10.3389/fnagi.2015.00052
11. Van Meer G, Voelker DR, Feigenson GW. Membrane lipids: where they are and how they behave. Nat Rev Mol Cell Biol (2008) 9:112–24. doi: 10.1038/nrm2330
12. Gorjão R, Azevedo-Martins AK, Rodrigues HG, Abdulkader F, Arcisio-Miranda M, Procopio J, et al. Comparative effects of DHA and EPA on cell function. Pharmacol Ther (2009) 122:56–64. doi: 10.1016/j.pharmthera.2009.01.004
13. Weylandt KH, Chiu CY, Gomolka B, Waechter SF, Wiedenmann B. Omega-3 fatty acids and their lipid mediators: towards an understanding of resolvin and protectin formation. Prostaglandins Other Lipid Mediat (2012) 97:73–82. doi: 10.1016/j.prostaglandins.2012.01.005
14. Calder PC. Marine omega-3 fatty acids and inflammatory processes: effects, mechanisms and clinical relevance. Biochim Biophys Acta (2015) 1851:469–84. doi: 10.1016/j.bbalip.2014.08.010
15. Horrobin DF, Glen AI, Vaddadi K. The membrane hypothesis of schizophrenia. Schizophr Res (1994) 13:195–207. doi: 10.1016/0920-9964(94)90043-4
16. Van Der Kemp WJ, Klomp DW, Kahn RS, Luijten PR, Hulshoff Pol HE. A meta-analysis of the polyunsaturated fatty acid composition of erythrocyte membranes in schizophrenia. Schizophr Res (2012) 141:153–61. doi: 10.1016/j.schres.2012.08.014
17. Rice SM, Schafer MR, Klier C, Mossaheb N, Vijayakumar N, Amminger GP. Erythrocyte polyunsaturated fatty acid levels in young people at ultra-high risk for psychotic disorder and healthy adolescent controls. Psychiatry Res (2015) 228:174–6. doi: 10.1016/j.psychres.2015.04.036
18. Berger ME, Smesny S, Kim SW, Davey CG, Rice S, Sarnyai Z, et al. Omega-6 to omega-3 polyunsaturated fatty acid ratio and subsequent mood disorders in young people with at-risk mental states: a 7-year longitudinal study. Transl Psychiatry (2017) 7:e1220. doi: 10.1038/tp.2017.190
19. Amminger GP, Schafer MR, Papageorgiou K, Klier CM, Cotton SM, Harrigan SM, et al. Long-chain omega-3 fatty acids for indicated prevention of psychotic disorders: a randomized, placebo-controlled trial. Arch Gen Psychiatry (2010) 67:146–54. doi: 10.1001/archgenpsychiatry.2009.192
20. Cadenhead K, Addington J, Cannon T, Cornblatt B, Mathalon D, Mcglashan T, et al. 23. omega-3 fatty acid versus placebo in a clinical high-risk sample from the North American Prodrome Longitudinal Studies (NAPLS) Consortium. Schizophr Bull (2017) 43:S16–S16. doi: 10.1093/schbul/sbx021.042
21. McGorry PD, Nelson B, Markulev C, Yuen HP, Schafer MR, Mossaheb N, et al. Effect of omega-3 polyunsaturated fatty acids in young people at ultrahigh risk for psychotic disorders: the neurapro randomized clinical trial. JAMA Psychiatry (2017) 74(1):19–27. doi: 10.1001/jamapsychiatry.2016.2902
22. Kane JM, Correll CU. Ω-3 polyunsaturated fatty acids to prevent psychosis: the importance of replication studies. JAMA Psychiatry (2017) 74:11–2. doi: 10.1001/jamapsychiatry.2016.2945
23. Kim SW, Jhon M, Kim JM, Smesny S, Rice S, Berk M, et al. Relationship between erythrocyte fatty acid composition and psychopathology in the vienna omega-3 study. PLoS One (2016) 11:e0151417. doi: 10.1371/journal.pone.0151417
24. Yung AR, Phillips LJ, Mcgorry PD, Mcfarlane CA, Francey S, Harrigan S, et al. Prediction of psychosis. Br J Psychiatry Suppl (1998) 172:14–20. doi: 10.1192/S0007125000297602
25. Markulev C, Mcgorry PD, Nelson B, Yuen HP, Schaefer M, Yung AR, et al. NEURAPRO-E study protocol: a multicentre randomized controlled trial of omega-3 fatty acids and cognitive-behavioural case management for patients at ultra high risk of schizophrenia and other psychotic disorders. Early Interv Psychiatry (2015) 11(5):418–28. doi: 10.1111/eip.12260
26. Alqarni A, Mcintyre KJ, Brown SHJ, Meyer BJ, Mitchell TW. A high-throughput method for the analysis of erythrocyte fatty acids and the omega-3 index. Lipids (2018) 53:1005–15. doi: 10.1002/lipd.12108
27. Cadenhead KS, Minichino A, Kelsven S, Addington J, Bearden C, Cannon TD, et al. Metabolic abnormalities and low dietary Omega 3 are associated with symptom severity and worse functioning prior to the onset of psychosis: findings from the North American Prodrome Longitudinal Studies Consortium. Schizophr Res (2018) 209:96–103. doi: 10.1016/j.schres.2018.09.022
28. Carver JD, Benford VJ, Han B, Cantor AB. The relationship between age and the fatty acid composition of cerebral cortex and erythrocytes in human subjects. Brain Res Bull (2001) 56:79–85. doi: 10.1016/S0361-9230(01)00551-2
29. Conklin SM, Gianaros PJ, Brown SM, Yao JK, Hariri AR, Manuck SB, et al. Long-chain omega-3 fatty acid intake is associated positively with corticolimbic gray matter volume in healthy adults. Neurosci Lett (2007) 421:209–12. doi: 10.1016/j.neulet.2007.04.086
30. Mcnamara RK, Able J, Jandacek R, Rider T, Tso P, Eliassen JC, et al. Docosahexaenoic acid supplementation increases prefrontal cortex activation during sustained attention in healthy boys: a placebo-controlled, dose-ranging, functional magnetic resonance imaging study. Am J Clin Nutr (2010a) 91:1060–7. doi: 10.3945/ajcn.2009.28549
31. Mcnamara RK, Vannest JJ, Valentine CJ. Role of perinatal long-chain omega-3 fatty acids in cortical circuit maturation: mechanisms and implications for psychopathology. World J Psychiatry (2015) 5:15–34. doi: 10.5498/wjp.v5.i1.15
32. Lin PY, Huang SY, Su KP. A meta-analytic review of polyunsaturated fatty acid compositions in patients with depression. Biol Psychiatry (2010) 68:140–7. doi: 10.1016/j.biopsych.2010.03.018
33. Bloch MH, Hannestad J. Omega-3 fatty acids for the treatment of depression: systematic review and meta-analysis. Mol Psychiatry (2012) 17:1272–82. doi: 10.1038/mp.2011.100
34. Martins JG, Bentsen H, Puri BK. Eicosapentaenoic acid appears to be the key omega-3 fatty acid component associated with efficacy in major depressive disorder: a critique of Bloch and Hannestad and updated meta-analysis. Mol Psychiatry (2012) 17:1144–9. doi: 10.1038/mp.2012.25
35. Mocking RJ, Harmsen I, Assies J, Koeter MW, Ruhe HG, Schene AH. Meta-analysis and meta-regression of omega-3 polyunsaturated fatty acid supplementation for major depressive disorder. Transl Psychiatry (2016) 6:e756. doi: 10.1038/tp.2016.29
36. Cribb L, Murphy J, Froud A, Oliver G, Bousman CA, Ng CH, et al. Erythrocyte polyunsaturated fatty acid composition is associated with depression and FADS genotype in Caucasians. Nutr Neurosci (2018) 21:589–601. doi: 10.1080/1028415X.2017.1327685
37. Kurotani K, Sato M, Ejima Y, Kashima K, Nanri A, Pham NM, et al. Serum alpha-linolenic and linoleic acids are inversely associated with depressive symptoms in adults. e-SPEN Journal (2014) 9:e7–e12. doi: 10.1016/j.clnme.2013.12.003
38. Arnold LE, Young AS, Belury MA, Cole RM, Gracious B, Seidenfeld AM, et al. Omega-3 fatty acid plasma levels before and after supplementation: correlations with mood and clinical outcomes in the omega-3 and therapy studies. J Child Adolesc Psychopharmacol (2017) 27:223–33. doi: 10.1089/cap.2016.0123
39. Pinto TJ, Vilela AA, Farias DR, Lepsch J, Cunha GM, Vaz JS, et al. Serum n-3 polyunsaturated fatty acids are inversely associated with longitudinal changes in depressive symptoms during pregnancy. Epidemiol Psychiatr Sci (2017) 26:157–68. doi: 10.1017/S204579601500116X
40. US Department of Agriculture, A.R.S., Nutrient Data Laboratory. (2018). USDA National Nutrient Database for Standard Reference, Legacy. [Online]. Available: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/nutrient-data-laboratory/docs/usda-national-nutrient-database-for-standard-reference/ [Accessed April 2018].
41. Hamazaki K, Maekawa M, Toyota T, Iwayama Y, Dean B, Hamazaki T, et al. Fatty acid composition and fatty acid binding protein expression in the postmortem frontal cortex of patients with schizophrenia: a case-control study. Schizophr Res (2016) 171:225–32. doi: 10.1016/j.schres.2016.01.014
42. Mocking RJT, Assies J, Ruhe HG, Schene AH. Focus on fatty acids in the neurometabolic pathophysiology of psychiatric disorders. J Inherit Metab Dis (2018) 41:597–611. doi: 10.1007/s10545-018-0158-3
43. Kiecolt-Glaser JK, Epel ES, Belury MA, Andridge R, Lin J, Glaser R, et al. Omega-3 fatty acids, oxidative stress, and leukocyte telomere length: a randomized controlled trial. Brain Behav Immun (2013) 28:16–24. doi: 10.1016/j.bbi.2012.09.004
44. Kiecolt-Glaser JK, Belury MA, Porter K, Beversdorf DQ, Lemeshow S, Glaser R. Depressive symptoms, omega-6:omega-3 fatty acids, and inflammation in older adults. Psychosom Med (2007) 69:217–24. doi: 10.1097/PSY.0b013e3180313a45
45. Svahn SL, Varemo L, Gabrielsson BG, Peris E, Nookaew I, Grahnemo L, et al. Six tissue transcriptomics reveals specific immune suppression in spleen by dietary polyunsaturated fatty acids. PLoS One (2016) 11:e0155099. doi: 10.1371/journal.pone.0155099
46. Bazinet RP, Laye S. Polyunsaturated fatty acids and their metabolites in brain function and disease. Nat Rev Neurosci (2014) 15:771–85. doi: 10.1038/nrn3820
47. Chen CT, Bazinet RP. Beta-oxidation and rapid metabolism, but not uptake regulate brain eicosapentaenoic acid levels. Prostaglandins Leukot Essent Fatty Acids (2015) 92:33–40. doi: 10.1016/j.plefa.2014.05.007
48. Rapaport MH, Nierenberg AA, Schettler PJ, Kinkead B, Cardoos A, Walker R, et al. Inflammation as a predictive biomarker for response to omega-3 fatty acids in major depressive disorder: a proof-of-concept study. Mol Psychiatry (2016) 21:71–9. doi: 10.1038/mp.2015.22
49. Peters BD, Machielsen MW, Hoen WP, Caan MW, Malhotra AK, Szeszko PR, et al. Polyunsaturated fatty acid concentration predicts myelin integrity in early-phase psychosis. Schizophr Bull (2013) 39:830–8. doi: 10.1093/schbul/sbs089
50. Bloemen OJ, De Koning MB, Schmitz N, Nieman DH, Becker HE, De Haan L, et al. White-matter markers for psychosis in a prospective ultra-high-risk cohort. Psychol Med (2010) 40:1297–304. doi: 10.1017/S0033291709991711
51. Amminger GP, Schafer MR, Klier CM, Slavik JM, Holzer I, Holub M, et al. Decreased nervonic acid levels in erythrocyte membranes predict psychosis in help-seeking ultra-high-risk individuals. Mol Psychiatry (2012) 17:1150–2. doi: 10.1038/mp.2011.167
52. Kageyama Y, Kasahara T, Nakamura T, Hattori K, Deguchi Y, Tani M, et al. Plasma nervonic acid is a potential biomarker for major depressive disorder: a pilot study. Int J Neuropsychopharmacol (2018) 21:207–15. doi: 10.1093/ijnp/pyx089
53. Assies J, Pouwer F, Lok A, Mocking RJ, Bockting CL, Visser I, et al. Plasma and erythrocyte fatty acid patterns in patients with recurrent depression: a matched case-control study. PLoS One (2010) 5:e10635. doi: 10.1371/journal.pone.0010635
54. Hoen WP, Lijmer JG, Duran M, Wanders RJ, Van Beveren NJ, De Haan L. Red blood cell polyunsaturated fatty acids measured in red blood cells and schizophrenia: a meta-analysis. Psychiatry Res (2013) 207:1–12. doi: 10.1016/j.psychres.2012.09.041
55. Arvindakshan M, Ghate M, Ranjekar PK, Evans DR, Mahadik SP. Supplementation with a combination of omega-3 fatty acids and antioxidants (vitamins E and C) improves the outcome of schizophrenia. Schizophr Res (2003) 62:195–204. doi: 10.1016/S0920-9964(02)00284-0
56. Peet M. Nutrition and schizophrenia: beyond omega-3 fatty acids. Prostaglandins Leukot Essent Fatty Acids (2004) 70:417–22. doi: 10.1016/j.plefa.2003.12.019
57. Medema S, Mocking RJ, Koeter MW, Vaz FM, Meijer C, De Haan L, et al. Levels of red blood cell fatty acids in patients with psychosis, their unaffected siblings, and healthy controls. Schizophr Bull (2016) 42:358–68. doi: 10.1093/schbul/sbv133
58. McNamara RK, Jandacek R, Rider T, Tso P, Dwivedi Y, Pandey GN. Selective deficits in erythrocyte docosahexaenoic acid composition in adult patients with bipolar disorder and major depressive disorder. J Affect Disord (2010b) 126:303–11. doi: 10.1016/j.jad.2010.03.015
59. McNamara RK, Jandacek R, Tso P, Blom TJ, Welge JA, Strawn JR, et al. Adolescents with or at ultra-high risk for bipolar disorder exhibit erythrocyte docosahexaenoic acid and eicosapentaenoic acid deficits: a candidate prodromal risk biomarker. Early Interv Psychiatry (2016) 10:203–11. doi: 10.1111/eip.12282
Keywords: ultra-high risk, omega-3 fatty acids, psychosis, psychopathology, outcomes
Citation: Berger M, Nelson B, Markulev C, Yuen HP, Schäfer MR, Mossaheb N, Schlögelhofer M, Smesny S, Hickie IB, Berger GE, Chen EYH, de Haan L, Nieman DH, Nordentoft M, Riecher-Rössler A, Verma S, Mitchell TW, Meyer BJ, Thompson A, Yung AR, McGorry PD and Amminger GP (2019) Relationship Between Polyunsaturated Fatty Acids and Psychopathology in the NEURAPRO Clinical Trial. Front. Psychiatry 10:393. doi: 10.3389/fpsyt.2019.00393
Received: 14 January 2019; Accepted: 17 May 2019;
Published: 06 June 2019.
Edited by:
Claes Wahlestedt, Leonard M. Miller School of Medicine, United StatesReviewed by:
Kristin Suzanne Cadenhead, University of California, San Diego, United StatesCopyright © 2019 Berger, Nelson, Markulev, Yuen, Schäfer, Mossaheb, Schlögelhofer, Smesny, Hickie, Berger, Chen, de Haan, Nieman, Nordentoft, Riecher-Rössler, Verma, Mitchell, Meyer, Thompson, Yung, McGorry and Amminger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maximus Berger, bWF4aW11cy5iZXJnZXJAb3J5Z2VuLm9yZy5hdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.