
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry , 05 March 2019
Sec. Molecular Psychiatry
Volume 10 - 2019 | https://doi.org/10.3389/fpsyt.2019.00103
This article is part of the Research Topic The Role of Immune Components in Psychiatric Disorders View all 11 articles
 Sung-Wan Kim1
Sung-Wan Kim1 Hee-Ju Kang1Min Jhon1Ju-Wan Kim1
Hee-Ju Kang1Min Jhon1Ju-Wan Kim1 Ju-Yeon Lee1
Ju-Yeon Lee1 Adam J. Walker2Bruno Agustini2
Adam J. Walker2Bruno Agustini2 Jae-Min Kim1*
Jae-Min Kim1* Michael Berk2,3,4,5
Michael Berk2,3,4,5Statins, which are widely used to treat hypercholesterolemia, have anti-inflammatory and anti-oxidant effects. These are thought to be responsible for the potential effects of statins on various psychiatric disorders. In this study, we comprehensively review the literature to investigate the effects of statins on various psychiatric disorders including depression, schizophrenia, and dementia. In addition, we review adverse effects and drug interactions of statins to give clinically useful information guiding statin use in the psychiatric field. Statins seem useful in reducing depression, particularly in patients with physical disorders such as cardiovascular disease. In patients with schizophrenia, negative symptoms may be reduced by adjuvant statin therapy. Studies on cohorts at risk for dementia have generally shown protective effects of statins, while those on treatment for dementia show inconsistent results. In conclusion, statins used in combination with conventional psychotropic medications may be effective for various psychiatric disorders including depression, schizophrenia, and dementia. Further study is required to determine optimal doses and duration of statin use for the treatment of psychiatric disorders.
Statins (3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors) are widely used to prevent cardiac and cerebrovascular events by treating hypercholesterolemia. Statins also have anti-inflammatory effects, including reducing C-reactive protein (CRP) concentrations (1). The effects of lowering low-density lipoprotein (LDL) cholesterol with statins may lead to anti-inflammatory actions because LDL cholesterol itself strongly promotes inflammation (2). Furthermore, statins reduce tumor necrosis factor alpha (TNF-α) and interferon gamma (IFNγ) production in stimulated T-lymphocytes, and inhibit the T helper cell (Th-1) immune response (3). Addition of statins to human hepatocytes reduces the levels of C-reactive protein induced by circulating interleukin 6 (IL-6), suggesting that the anti-inflammatory effects of statins are hepatic in nature (4). These anti-inflammatory and anti-oxidant effects of statins are potential mechanisms for the effects of statins on various psychiatric disorders.
Many kinds of statins have been approved for treatment of hypercholesterolemia. Statins can be broadly classified as lipophilic or hydrophilic, which affect their ability to permeate the brain (5). Hydrophilic statins, such as pravastatin, rosuvastatin, and fluvastatin are not able to easily cross the blood brain barrier (BBB), and are also less efficient at permeating cell membranes. Conversely, lipophilic statins, such as simvastatin, lovastatin, pitavastatin, and atorvastatin (6) are more likely to cross the BBB. Moreover, lipophilic statins enter cells via passive diffusion and are thus widely distributed in various tissues, whereas hydrophilic statins are more liver-specific. Cellular uptake features a variety of carrier-mediated mechanisms (5, 7). These distinct characteristics of hydrophilic and lipophilic statins may lead to differential effects of statins in terms of efficacy, or could lead to neuropsychiatric adverse events. What remains unclear is if the beneficial effects of statins require brain penetrance, or are mediated by peripheral or hepatic suppression of circulating cytokines, as is best evidenced for rosuvastatin (8), or especially in the elderly are predicated by vascular improvements in domains such as plaque stability and vessel inflammation (9).
Most psychotropic medications currently used in depression and schizophrenia act on monoamine neurotransmitters. However, certain proportions of patients with depression and schizophrenia do not respond to the conventional medications currently available. Curiously, patients with higher levels of peripheral cytokines may be less likely to respond to antidepressants (10). Therefore, clinicians require other medications with different mechanisms. Growing evidence indicates that inflammation is a key mechanisms of pathogenesis in many psychiatric disorders including depression, schizophrenia, and neurocognitive disorders. In addition, medications that act on inflammation have shown potential as alternative treatment methods. Therefore, many researchers have measured the effects of statins on these psychiatric disorders. In this study, we comprehensively reviewed clinical trials and epidemiological studies to investigate the effects of statins on various psychiatric disorders including depression, psychosis, and dementia. In addition, this study aimed to give clinical information on the implications for statin for use in clinical psychiatry.
The “classic” mechanism of action of statins involves the reduction of endogenous cholesterol biosynthesis via the inhibition of HMG-CoA reductase, a rate limiting enzyme integral to the mevalonate pathway. The corresponding reduction in hepatic cholesterol synthesis instigates translocation of membrane-bound sterol regulatory element-binding proteins to the nucleus, subsequent upregulation of LDL receptors on the surface of hepatocytes, leading to elevated clearance of LDL cholesterol from the blood (11, 12). These effects make statins effective for treating hypercholesterolemia. However, brain cholesterol metabolism is largely independent of dietary lipid intake because of the BBB. Brain cholesterol is synthesized in the central nervous system (CNS), unlike peripheral cholesterol (13). Not all statins are equally effective in terms of lowering brain cholesterol levels (14).
Interestingly, statins also have a range of so-called “pleiotropic” effects (e.g., suppressing inflammation, reducing oxidative stress, reducing T-cell activation) that have implications for extrahepatic systems including the cardiovascular system, the CNS, and the immune system (15–17). Statins are thought to exert many of these pleiotropic effects by suppressing the downstream synthesis of molecules in the mevalonate pathway, mediated through the inhibition of small GTPase prenylation and thus, isoprenoid production. Importantly, such small GTPases play essential roles in regulating a number of signaling pathways and cellular processes which are dependent on isoprenylation (18, 19). For example Ras plays a key role in cellular growth and proliferation; Rac in reactive oxygen species generation; and Rho in the proinflammatory cytokines. This inhibition of isoprenoids leads to a host of anti-inflammatory, immunomodulatory, anti-oxidative, and anti-atherosclerotic effects, including but not limited to: downregulation of transcription factors (e.g., Nuclear Factor-κB, Activator Protein-1), reduced expression of SOCS3 and CD40, suppression of cytokine (IL-1β, TNFα, IL-6), chemokine (IL-8, Monocyte Chemotactic Protein-1) and CRP production, attenuated induction of adhesion molecules (P-selectin, Very Late Antigen-4, Intercellular Adhesion Molecule-1), suppression of IFN-γ dependent co-stimulation of MHC Class II expression, as well as downregulation of T cell and monocyte activation.
Statins also reduce negative regulation of nitric oxide, lower NADPH oxidase and superoxide formation, and increasing oxygen free radical scavenging, decrease inflammatory cell infiltration, macrophage accumulation, reduce metalloproteinase activity, and expression, and attenuate activation of the NLRP3 Inflammasome (18–23). Notably, evidence also suggests statins facilitate PI3K-Akt signaling (24, 25), and crosstalk with peroxisome proliferator-activated receptor (PPAR) signaling (26) Collectively, these resultant cardioprotective, immunoprotective, and neuroprotective benefits of the aforementioned pleiotripic effects make statins worthy of investigation for treating neuropsychiatric disorders with diffuse etiologies.
Several neuroimaging studies have explored the effects of brain statins. Serial volumetric magnetic resonance imaging of patients with multiple sclerosis, a chronic inflammatory/ neurodegenerative disorder, revealed significantly less whole-brain atrophy in a high-dose (80 mg daily) simvastatin group than in a placebo group (27). Studies using positron emission tomography or diffusion tensor imaging to evaluate dementia patients have yielded conflicting results in terms of the effects of statins on neurodegeneration and white matter integrity (28). Further research is required to explore whether statins control brain atrophy and functional connectivity.
Psychiatric disorders are often associated with several somatic consequences, including hypertension, heart disease, stroke, cancer, obesity, diabetes mellitus, and osteoporosis (29). It is known that individuals with psychiatric disorders tend to have unhealthier lifestyle habits, such as drinking excessive amounts of alcohol, are more likely to smoke, eat an unhealthy diet and be more physically inactive than their peers, be less compliant with medication regimens and have poorer self-care (30). All these factors significantly contribute to the development and maintenance of the above-mentioned comorbidities.
Also, shared immunometabolic pathways have been implicated in the link between psychiatric and physical disease. Psychiatric conditions are consistently linked to disruptions in the body's stress response system (mainly the Autonomic Nervous System (ANS) and the Hypothalamic-Pituitary-Adrenal (HPA) axis (31) and are often associated with a pro-inflammatory profile (32). The chronicity of these processes might lead to several somatic consequences, including elevated blood pressure, abdominal obesity, dyslipidaemia and increased blood glucose. These conditions constitute important risk factors for cardiovascular disease (CVD), diabetes (33), cognitive impairment and even cancer (34), among others.
A recent review suggests that abdominal obesity and lipid disturbances are one of the driving forces behind the relationship between psychiatric disorders, in this case depression, and inflammation (35). Abdominal obesity gives rise to multiple immunometabolic dysregulations. White adipose tissue, especially in the abdominal area, plays as an active endocrine organ producing inflammatory cytokines and hormones (especially leptin) that disrupt important immunometabolic pathways (36). Increased leptin is a risk pathway for depression (37). Increased inflammatory activity interferes with HPA axis regulation, altering cortisol secretion and feedback, leading to a progressive feedforward loop of inflammation-related conditions (38).
Statins, with their lipid lowering, immunomodulatory, anti-inflammatory, and antioxidant properties, may act to slow or indeed prevent some of these alterations, potentially leading to interruption of the neuroprogressive cascade in these disorders (39) and decreased morbidity and mortality for individuals with psychiatric conditions. Notably, the main cause of death in psychiatric disorders remains CVD (40), where statins have its most definitive proved role (41). The possible therapeutic benefits of statins in each psychiatric disorder are described individually in this paper.
The pathogenesis of depression is both complex and heterogeneous. Inflammation and immune dysfunction are major contributors to the development of depression (42, 43). Inflammatory markers have been associated both with the prognosis of depression (44) and the risks of associated cardiac events and cancer (45). Peripheral pro-inflammatory cytokine signals are transmitted to the CNS via both humoral and neural pathways and may trigger depression by increasing oxidative stress (46); interacting with the hypothalamic–pituitary–adrenal axis; causing impairments in neurotransmitter systems involving glutamate, serotonin, dopamine, and noradrenaline (47–49); disrupting mitochondrial biogenesis (50); decreasing neurogenesis (51); and causing persistent and detrimental changes in the brain.
The monoaminergic theory of depression has failed to deliver novel therapeutic agents. Drugs with anti-inflammatory properties are important potential alternatives for the treatment of depression (52). Antidepressant effects of anti-inflammatory agents were noted in earlier epidemiology studies and clinical trials, including celecoxib, pioglitazone, N-acetylcysteine and statins. Besides their lipid-lowering properties, statins possess direct anti-inflammatory effects as noted above (53), which led researchers to investigate the potential impact of statins on depression. The present study summarizes previous studies focusing on the prospective association between statins and depression in Table 1.
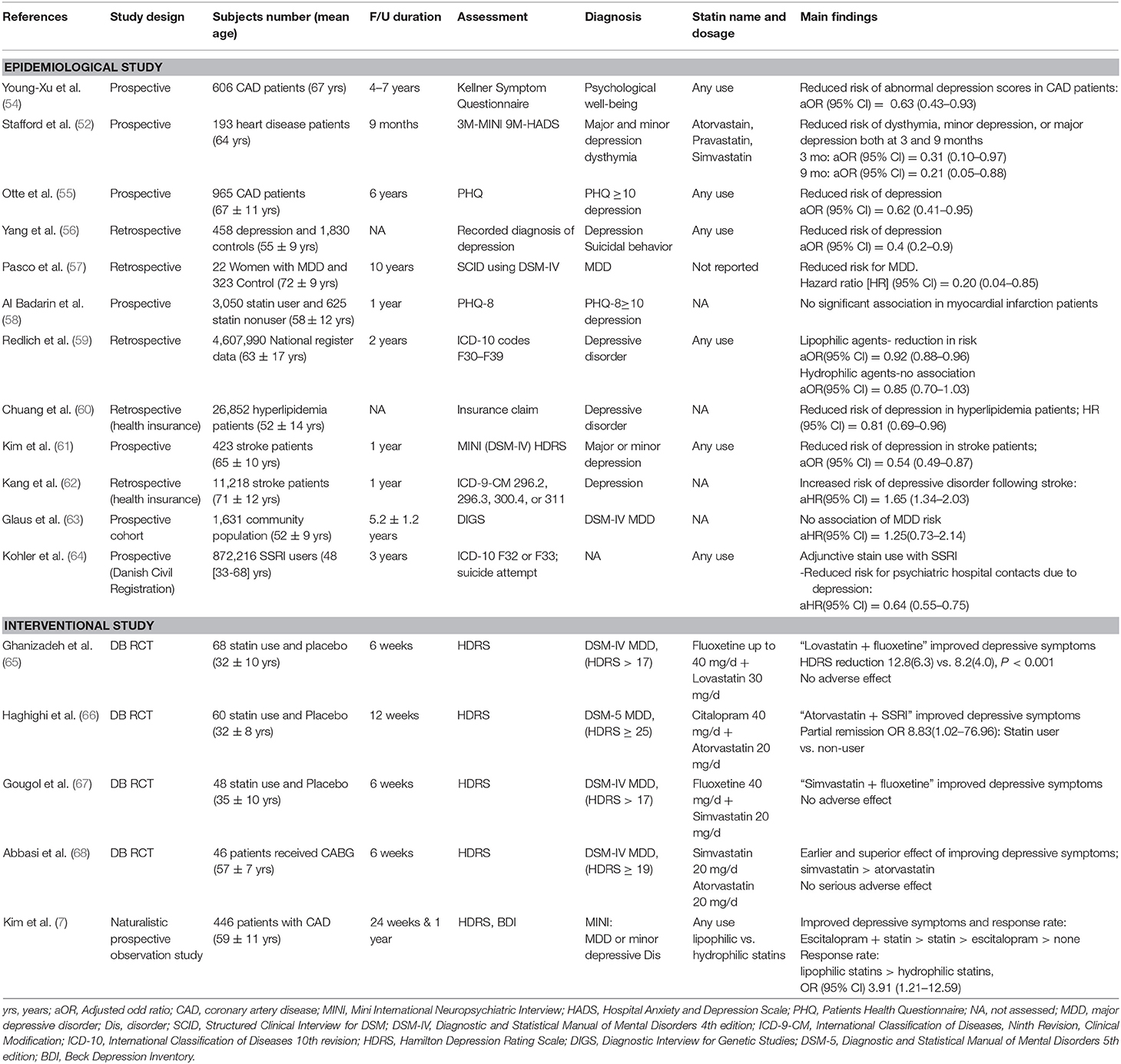
Table 1. Studies investigating the associations between statin use and depression.
To date, there has been one meta-analysis including seven observational studies (four cohort, two nested case-control, and one cross-sectional study), which found that statin users were less likely to develop depression than non-users (69). In addition to this meta-analysis, four prospective studies including large populations (n = 26,852–4,607,990) using national register data reported that statin use was associated with a reduced risk of depression (59–61, 64). Meanwhile, two prospective studies found that statin use was not associated with worsening of depression in acute myocardial infarction (AMI) patients (58) or with depression risk in a community population (n = 1,631) (63). Another study reported that statin use in stroke patients was associated with heightened depression risk (62). However, this study on stroke patients (62) did not adjust for significant covariates, limiting our ability to interpret the results (70). The study of AMI patients assessed changes in depression scale scores, which were at non-significant levels at baseline (58). Moreover, the community studies that reported potential beneficial effects of statins on depression (59, 60, 64) included larger numbers of participants and younger populations compared to the study that reported a detrimental effect of statins on depression (63). We hypothesize that the direction of associations may depend on the characteristics of the participants. In healthy populations without inflammatory loading, statins may not have beneficial anti-inflammatory effects. This finding is concordant with the findings of Miller and Raison, who found that levels of inflammation predicted response to infliximab; those with high levels benefitted, and those that had low levels worsened. The cholesterol-lowering effects of statins may make fragile people (e.g., the elderly) who are likely to already have low cholesterol levels vulnerable to depression via lowered serotonin levels. Therefore, the risks and benefits of statin use may depend on patient characteristics.
Statin use could be helpful in reducing the risk of depression in populations who are experiencing excess inflammation due to physical diseases such as CVD–highly comorbid across major psychiatric disorders. Additionally, statin use could be beneficial for depression prevention in populations with balanced nutrition who, therefore, have a plentiful reserve cholesterol, in whom lowering cholesterol does not impact the onset of depression. Although further research is needed to confirm the type of statins that would be most beneficial for depression prevention, lipophilic statins (including simvastatin) that have better brain penetrance may have greater protective effects against depression than hydrophilic statins (including rosuvastatin and pravastatin) (59). Equally statins that most robustly suppress peripheral inflammation, such as rosuvastatin, evidenced in the JUPITER study, may have advantages (8).
Because epidemiological studies showed that statins have beneficial effects on mood, randomized controlled trials (RCTs) have been conducted to examine the efficacy of statins in treating depression (65–67). A meta-analysis including three double-blind RCTs in subjects with depression found that adjunctive therapy with statins in addition to antidepressants could be useful for the treatment of depression without any serious adverse effects, although this finding is limited by the small number of studies and short-term follow-up periods (6–12 weeks) (71). In addition to this meta-analysis, a 6-weeks double-blind RCT of simvastatin and atorvastatin without antidepressants was conducted in depressive patients after a coronary artery bypass graft (68). Although response rates by treatment were not significantly different, simvastatin tended to improve depressive symptoms earlier and more effectively than did atorvastatin, probably because the former drug can penetrate the BBB.
A non-randomized, 1-year prospective study of depressive patients after acute coronary syndrome (ACS) demonstrated that statins were effective for the treatment of depression independently of medical status and escitalopram use. In this study, the combination of statins and escitalopram had larger effects than either drug alone. In addition, lipophilic statins showed greater potential to improve depression than hydrophilic statins (7). Further analysis of this study population (72) found that levels of pro-inflammatory cytokines, including IL-6 and IL-18, predicted subsequent depression in patients with ACS. However, the trigger effects of IL-6 and IL-18 on depression were attenuated in patients receiving statins, suggesting that the antidepressant effects of such drugs are attributable to reductions in the actions of pro-inflammatory cytokines. These recent publications suggest that statins have independent effects with regard to improving depression (7, 68), but further research is needed with larger sample sizes and well-designed randomized trials in to clarify the potential benefits of statins alone in depression treatment.
In summary, both epidemiological and interventional studies show that statins are useful in reducing depression risk in patients with physical disorders such as CVD. However, caution is warranted before prescribing statins in the general population without higher inflammation loads or in populations with poor nutritional states and low cholesterol stores, because the cholesterol-lowering effects of statins could theoretically at least increase the risk of depression in these populations. Furthermore, in depressive patients, statins have been shown to be beneficial for improving depressive symptoms when used as an adjunctive therapy to antidepressants, but the independent effects of statins are yet to be confirmed.
Schizophrenia is a severe chronic mental disorder characterized by delusions, hallucinations, cognitive impairment, avolition, reduced emotional expression, social withdrawal, and marked functional decline (73). Immune dysfunction and inflammation have been implicated in the pathogenesis of schizophrenia by numerous epidemiological and clinical studies (74, 75). Specifically, people with schizophrenia show increased levels of pro-inflammatory cytokines, and the vulnerability-stress-inflammation model also supports the role of inflammation in schizophrenia (76). Patients with schizophrenia have elevated blood levels of IL-1β, IL-6, and transforming growth factor-β (77), and they have elevated microglia activation in the brain compared to normal controls (78). As the associations between inflammation and schizophrenia have been found repeatedly, anti-inflammatory agents including non-steroidal anti-inflammatory drugs and acetylcysteine have been used as adjunctive therapies for improving symptoms of schizophrenia (79–81).
An important consideration for understanding schizophrenia is that 50–75% of deaths among patients with schizophrenia are due to CVD, while about 33% of deaths in the general population are due to CVD (82). Metabolic syndrome and dyslipidemia are associated with second generation antipsychotics and have very high prevalence rates in patients with schizophrenia. Statins effectively manage dyslipidaemia in patients with schizophrenia (83). As statins also exert anti-inflammatory actions, they are useful in preventing cardiovascular conditions in such patients and are employed to augment schizophrenia treatment.
To date, there have been six RCTs investigating the efficacy of statins as an adjuvant treatment for schizophrenia (Table 2). Five of these RCTs had small sample sizes of 12–36 patients in each treatment arm, and short treatment durations of 6–12 weeks. Only one study (86) had a larger sample size of 65 patients in each treatment arm, and investigated Positive and Negative Syndrome Scale (PANSS) negative symptom score over 6 months. Most of the studies followed patients who were outpatients in a stable state (e.g., stable on medication for several weeks prior to baseline assessment), whereas one study included inpatients in the active phase of the disease (89). Three studies used simvastatin 40 mg, while other studies used lovastatin 20 mg, atorvastatin 20 mg, or pravastatin 40 mg.
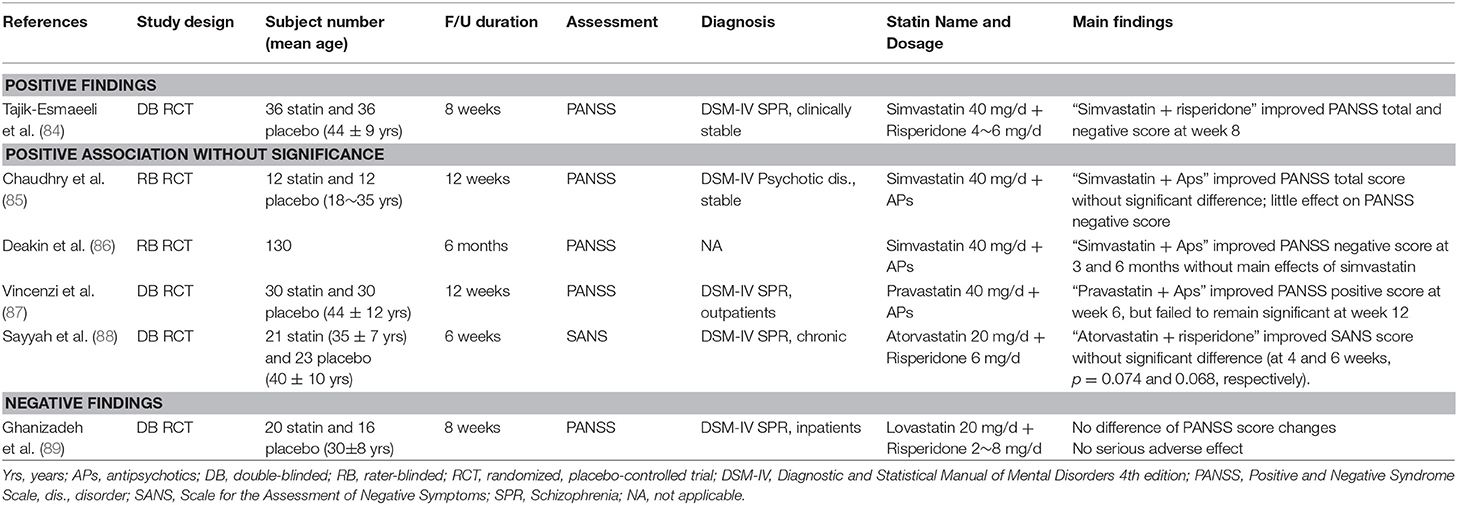
Table 2. Clinical trials investigating the efficacy of statins in patients with schizophrenia.
One study (84) showed that statin add-on therapy for schizophrenia patients was superior to placebo in terms of improving negative symptoms as measured by the PANSS subscale evaluating blunted affect, emotional withdrawal, apathetic social withdrawal, and poverty of speech. Although negative symptoms constitute the major barrier to functional recovery in patients with schizophrenia, the current antipsychotics exert only modest effects on negative symptoms (90, 91). Therefore, studies showing effects of statins on negative symptoms in patients with schizophrenia could have important clinical implications. Another study (89) did not show any effect of statins. The four remaining studies (85, 87, 88) reported non-significant benefits of statins. Most studies noted no significant differences in the adverse event rates between the statin user and non-user groups.
The participants of the study that reported a significant reduction in PANSS negative scores had the lowest baseline PANSS score among the six RCTs (84). This implies that the effect of statins may be more pronounced in stabilized patients than acutely ill patients. Another consideration is the type of antipsychotic medication used. There may be interactions of statins and antipsychotics, because some antipsychotics also have anti-inflammatory actions (92). Appropriate statin use may also affect the results since lipophilic statins, which can cross the BBB more readily, are more likely to interact with central brain regions (7). Simvastatin, which is the most lipophilic statin, was the most commonly used statin type in RCTs. Whether lipophilic statins improve inflammatory markers in patients with schizophrenia should be studied further.
Although there has been no study of the optimal dose and duration of statin therapy in schizophrenia, a few studies suggested the advantages of high dosage and long duration of statin therapy for CVD (93, 94). An animal study showed that hyper-locomotive activity and reduced anxiety-like behavior via NMDA receptor upregulation were initiated after high-dose simvastatin, which was higher than clinical dosages (95). Previous studies on N-acetylcysteine, which inhibits oxidative and inflammatory pathways, reported clear evidence of efficacy only after 6 months (96, 97), and a replication study noted benefits only after 9 and 12 months (98). Therefore, long-term treatment with high-dose statins may better alleviate psychotic and negative symptoms in patients with schizophrenia.
The lipid-lowering effects of statins may alleviate symptoms of schizophrenia, because studies have suggested associations between hyperlipidemia and the pathophysiology of schizophrenia (99, 100). One study found that pravastatin significantly decreased the PANSS positive subscale scores, commencing at week 6, in schizophrenia patients, but the decrease failed to remain significant to 12 weeks (87). Interestingly, the similar pattern of decrease at 6 weeks and increase at 12 weeks was found with levels of triglycerides, LDL-cholesterol, and total cholesterol. This suggests a link between lipid levels and the psychopathology of schizophrenia. However, we should consider that reduced efficacy for both psychotic symptoms and cholesterol levels could be due to poor adherence to statin medications. Additionally, a study on patients taking clozapine revealed that increases in the serum total cholesterol and triglyceride levels significantly predicted reductions in the PANSS total and/or negative subscale scores (101, 102). Furthermore, a positive longitudinal association was evident between changes in cholesterol levels and improved global cognition, particularly in verbal memory (103). Thus, further study is required to understand how changes in the serum levels of lipids and inflammatory reactions relate to changes in the symptoms of schizophrenia during statin use, and how these relationships vary with different antipsychotic drugs.
In summary, the anti-inflammatory actions of statins are expected to alleviate symptoms of schizophrenia as an augmentation to other drugs, and they have the added benefits of treating metabolic abnormalities such as hyperlipidemia to prevent CVD. We recommend the use of a sufficient dose of statins for at least 12 weeks in stable patients with schizophrenia for functional recovery as well as liberal use of statins in those with high levels of cardiovascular risk. Further studies are required in various populations and stages of illness.
Dementia has complex and heterogenous etiologies, including cerebrovascular disease, amyloid plaques, and tauopathy (104). Alzheimer disease (AD) is the most common cause of dementia and represents one of the largest burdens of disease in elderly persons (105). Evidence suggests that the deposition of ß-amyloid plaques and inflammatory processes in the CNS play important roles in the development and progression of AD (106, 107). Excessive amyloid beta (Aβ) accumulation is a hallmark feature of the AD neurodegenerative cascade (108). The dysregulation of the Aβ clearance process is characterized by elevated levels of pro-inflammatory cytokines, and this induces Aβ accumulation and continuous immune activation (109).
Defects in brain cholesterol homeostasis have been implicated in neurodegenerative diseases including AD and cognitive deficits typical of old age (13). Most brain cholesterol is synthesized in astrocytes; ApoE shuttles cholesterol (in a lipoprotein complex) from these cells to neurons. Therefore, ApoE may play an important role in cholesterol homeostasis in aging and diseased brains (110). Furthermore, cholesterol homeostasis may significantly affect the synthesis, deposition, and clearance of β-amyloid plaques (111, 112). The major brain cholesterol metabolite 24S-hydroxycholesterol (24S-OHC) may affect the NMDA receptor, in turn triggering cell death associated with AD (113). Statins exert anti-inflammatory and cholesterol-lowering effects in the brain, and also reduce the levels of oxysterols such as 24S-OHC (114). Statins may thus be useful in preventing/managing AD. Previous research on the association between statin use and AD, derived from cardiovascular studies, suggested that elective statin use has a beneficial effect on AD (115).
Table 3 summarizes previous studies investigating the associations between statin use and AD. Epidemiological cross-sectional and case-control studies have generally found that statins usefully prevent AD (119, 120, 125). Several prospective studies on the incidence of statin use and AD have also shown a protective association, although these studies have limitations. The Adult Changes in Thought (ACT) study was a prospective study that found that statin use may be associated with reduced risk of AD, particularly in those younger than 80 (118). The 2-year follow-up of the Alzheimer's Disease Anti-inflammatory Prevention Trial (ADAPT) found reduced risk of AD in people taking statins, but it is important to note that participants regularly using NSAIDs were excluded, but non-statin lipid lowering agent use was permitted (117). Conversely, the Cache County Study found no association between statin use and the risk of AD over 72 weeks (116). There was no randomized clinical trial assessing statin use and risk of developing AD. A large primary prevention study of statins in the elderly, STAREE will explore this outcome (126).
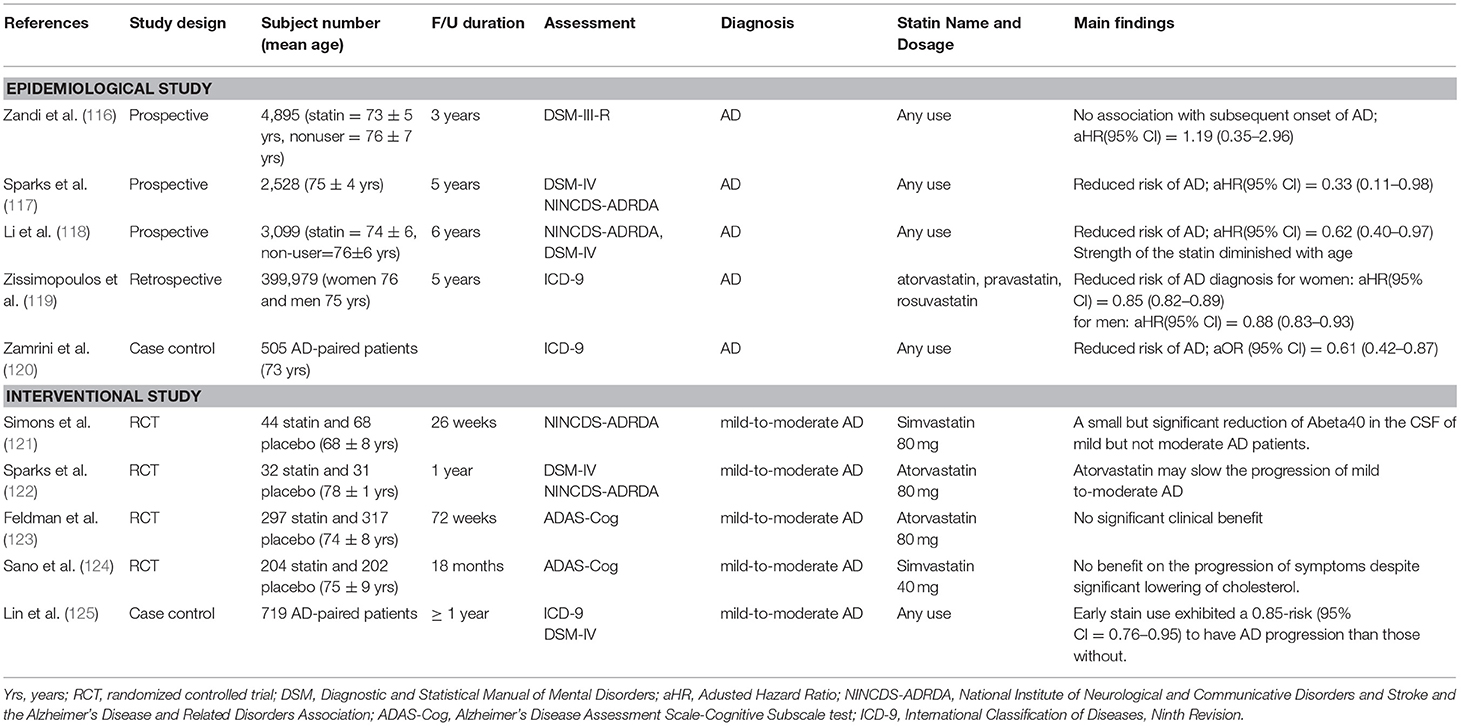
Table 3. Studies investigating the associations between statin use and Alzheimer disease (AD).
There have been four published RCTs of statins as an intervention in patients with mild to moderate AD. The Lipitor's Effect in Alzheimer's Dementia (LEADe) study was the largest with 640 patients, and found that a regimen of atorvastatin (80 mg/day) plus donepezil was not associated with significant benefits for treatment over 72 weeks (123). Similarly, a medium-sized, placebo-controlled, double-blind, randomized study found that simvastatin (20~40 mg) had no benefit for the progression of symptoms in individuals with mild to moderate AD (124). In contrast, a RCT showed that AD progressed more slowly (as measured by the Mini-Mental State Examination) in patients treated with simvastatin (80 mg/day) than placebo, over 26 weeks (121). Furthermore, this study showed that statins also decreased levels of beta-amyloid in the cerebrospinal fluid of patients with mild AD. In the 1-year follow-up of the Alzheimer's Disease Cholesterol-Lowering Treatment (ADCLT) trial study, there were also positive effects for treatment outcomes between 32 patients receiving 1 year of atorvastatin (80 mg/day) and 31 receiving placebo (122). Atorvastatin significantly improved memory performance as measured by the ADAS-Cog instrument after 6 months of treatment in patients with mild to moderate AD. These inconsistent results may be attributed by differences in sample size, statin dosage, characteristics of the statin used (lipophilic vs. hydrophilic), baseline lipid level, and assessment tools used for cognitive function.
In summary, statins may reduce the incidence of AD (126). However, RCTs assessing cognition in AD patients have yielded inconsistent results (127). A key point emerging from this research is the importance of the timing of statin treatment for achieving benefits in AD. Because AD progresses over long periods of time, future studies should include long-term follow-up periods to enable detection of any effects of statin treatment and might usefully focus early in the illness course, such as mild cognitive impairment.
There have been several clinical trials of statins for delirium prevention or treatment in critically ill patients. Based on the neuroinflammatory hypothesis of delirium, which is characterized by acute release of inflammatory mediators during critical illness, the pleiotropic effects of statins may prevent or attenuate delirium due to their effects on neutrophil migration, BBB injury, and inflammation (94, 128). However, a review of the literature regarding the use of statins for delirium prevention or treatment reveals no clear overall conclusions. Differential effects of statins on neuroinflammation during delirium may be due to treatment with lipophilic vs. hydrophilic statins. The current study demonstrated that the use of a hydrophilic statin (pravastatin) was associated with reduced delirium incidence compared with a lipophilic statin (atorvastatin), but the reverse has also been found (129). A recent comprehensive meta-analysis found that statins did not reduce the incidence of delirium in physically ill patients (130). There are many confounding factors that might account for these inconsistent results, including heterogeneity of study designs, variability of patient populations, the multifactorial nature of delirium, inconsistent delirium assessments, limited study power and lack of information on co-administration of other neuropsychiatric medications. Therefore, well-designed studies on delirium are still needed.
When considering bipolar disorder as a multisystemic inflammatory disease (131), it is important to examine the effect of statins on the manic phase as well as the depressive phase. An RCT evaluating lovastatin as an adjuvant to lithium in patients in the manic phase of bipolar disorder found that lovastatin neither exacerbated nor improved manic symptoms (132). That study suggested that the combination of statins with lithium is well-tolerated in patients with bipolar disorder, without evidence of exacerbation of mania by the antidepressant effects of statins.
The usual doses of statins are generally safe, being rarely associated with clinically significant adverse events (133). However, clinicians should know the general adverse events when prescribing statins. Statin-associated muscle symptoms (SAMs) are clinically important side effects of statins. SAMs are the most common side effects, reported by 10–25% of patients undergoing statin therapy, and are also the most common cause of statin discontinuation (134–136). SAMs range in severity from muscle cramps and weakness to creatine kinase (CK) elevation and rhabdomyolysis. Severe muscle damage is relatively rare among SAMs, but rhabdomyolysis should be distinguished from neuroleptic malignant syndrome (NMS), which is a rare but life-threatening disease that can occur with antipsychotic medication (137). Recent studies have found that patients who experienced non-severe SAMs can tolerate statins upon blinded re-challenge (138–140). Many reported adverse events can be predicated on expectancy and nocebo phenomena (141, 142). Therefore, it is necessary to consider a comprehensive approach and management such as patient assessment, treatment according to severity, re-assessment and considering other treatment options for SAMs (143). Neuropathy is most likely to develop after long-term treatment, and it generally resolves after the discontinuation of statins (144).
Statin use increased diabetes risk by 9–13% in a meta-analysis of randomized trials (145). Additionally, high-dose statins increased the risk of diabetes compared to that associated with standard-dose statins (146). Predictors of new-onset diabetes in patients treated with atorvastatin were baseline fasting blood glucose level, body mass index, hypertension, and fasting triglyceride level (147). However, a study on diabetes risks associated with statin therapy showed that patients lacking baseline risk factors (metabolic syndrome, impaired fasting glucose level, body mass index >30 kg/m2, or HbA1c >6%) did not develop diabetes (148). In addition, several studies have suggested that statin-mediated prevention of cardiovascular disease should receive more emphasis than the risk of diabetes (149–151). Risk factors for diabetes should be routinely evaluated before prescribing statins. L-carnitine (500–1,000 mg twice daily) may prevent any increase in blood sugar levels (152).
Although the serum levels of hepatic transaminases may increase in patients taking statins, routine measurement of liver enzyme levels is not required (153). Other possible physical side effects of statins are hemorrhagic stroke, decreased renal function, tendon rupture, interstitial lung disease, and low testosterone levels (154).
Risk for potential neuropsychiatric adverse events may also be increased in the use of long-term high doses of statins. Mood disturbance, sleep changes, cognitive impairment, and suicide have been reported in patients taking statins, although casual links are uncertain (69, 155–157). Clinicians should assess neuropsychiatric adverse events associated with statin use.
The US Food and Drug Administration recently issued a warning stating that statins could cause mild cognitive impairment (158). Some case reports and several studies have reported small cognitive decreases in patients on statin therapy (159–161); other studies have found that statins reduced cognitive decline in older adults (117, 162, 163). A recent systematic review and meta-analysis found no significant association between statin use and cognitive impairment (164, 165). Neurocognitive impairment following the initiation of statins appears to depend on statin type; lipophilic statins are associated with more cognitive impairments (159, 166), while clinical trials using hydrophilic statins, which are less likely to cross the blood brain barrier, did not show any significant cognitive impairment.
It seems biologically plausible that lowering cholesterol levels with statins could cause several changes in the serotonergic system, which might lead to increased irritability and violent ideation (167–169). Despite some case reports of mood disturbance with statin use (170, 171), evidence of any relationship between statins and mood is conflicting. It has been suggested that statins might be associated with a higher rate of sleep disturbance, especially for lipophilic statins (172, 173). Multi-methodological approaches using different databases suggest that statin use was associated with an increased risk of sleep disturbances (including sleep initiation and maintenance) and parasomnias (173). However, there is no conclusive evidence that any particular statin is more likely to cause sleep disturbances than other statins, and a recent meta-analysis found that statins exerted no significant adverse effects on sleep duration or efficiency (155).
The literature regarding statin-associated suicide risk remains limited, and there is no proven association between statin use and increase in suicide (56). A Danish population-based study (n = 642,058) showed that the SSRI-statin (citalopram 57.2%, simvastatin 92%) group was associated with fewer psychiatric hospital contacts and no increase in suicidal behavior compared to populations who used SSRI alone (174). Overall, even if the cholesterol-lowering effects of statins could be associated with potential adverse events, there has been little conclusive evidence of statins causing serious side effects that would outweigh the advantages of this medication. Furthermore, the advantageous anti-inflammatory actions of statins may alleviate any potential negative effects of lower cholesterol.
Metabolism of statins is complex, and begins with absorption, followed by hepatic uptake, metabolism, and elimination (175). Individual characteristics and multiple transporters acting on each phase interact with concomitant medications, leading to changes in serum concentrations of statins, may change. Among multiple pathways, the role of the cytochrome P-450 (CYP) system has been most commonly described (133). Most statins are metabolized by CYP 3A4. Exceptions include fluvastatin and rosuvastatin, which are largely metabolized by CYP 2C9 (176), and pravastatin, which is mainly metabolized by renal clearance (177). Antidepressants, antipsychotics, anxiolytics, and cognitive enhancers that are metabolized by CYP isoenzymes can increase serum statin concentrations by competing for catabolism and vice versa (176). Also, inhibition and enhancement of the CYP isoenzymes by psychotropic medications can increase or decrease serum concentrations of statins. One case report described a 79-year-old female prescribed nefazodone 300 mg daily for 8 years, who then took simvastatin 40 mg daily, and subsequently developed rhabdomyolysis, perhaps attributable to potent inhibition of CYP 3A4 by nefazodone (178). CYP status must be evaluated when combining antidepressants and statins (178).
Drug interactions between statins and antipsychotics may influence the efficacy of antipsychotics through P-glycoprotein 1 (P-gp), which is a transporter in the BBB and regulates brain tissue for access of centrally acting drugs. Both statins and some antipsychotic drugs are substrates of P-gp (179). Thus, statins and antipsychotic agents may act synergistically in terms of CNS access (180). The increased CNS levels may improve psychotic symptoms in schizophrenia patients (180).
The degree of lipophilicity required to cross the BBB may be associated with direct effects of statins on the brain, as might their capacity to suppress peripheral cytokines. Neuropsychiatric side effects of statins including neuropathy and cognitive impairment may be more closely associated with the lipophilic statins, probably because they are more likely to cross the BBB. However, lipophilic statins such as simvastatin have demonstrated effectiveness for improving depression as well as the negative symptoms of schizophrenia. Clinicians should be aware of these contradictory findings that lipophilic statins are associated with a higher potential for neuropsychiatric adverse events as well as increased efficacy for psychiatric symptoms when selecting the type of statin to prescribe.
The half-life of cholesterol in the adult brain ranges from 6 months to 5 years; in contrast, the half-life of plasma cholesterol is only a few days. Thus, any brain lipid-lowering effect of statins may be very slow (13, 181). Statins exert anti-inflammatory and anti-oxidant effects, which may explain their benefits in patients with various psychiatric disorders. Therefore, for psychiatric patients, high-dose long-term statin therapy may be required. Future long-term studies should explore the effects of statins in various psychiatric disorders.
In conclusion, statin therapy appears to be safe in the majority of patients, and the benefits of statin use far outweigh the potential risks. Statins used with conventional psychotropic medications may be effective in various psychiatric disorders including depression, schizophrenia, and the risk for dementia. Statins seem useful in reducing depression, particularly in patients with physical disorders. In patients with schizophrenia, negative symptoms may be reduced by adjuvant statin therapy. Studies on cohorts at risk for dementia have generally shown protective effects of statins, while those on treatment for dementia show inconsistent results. Further study is required to investigate optimal statin dose and duration of use. In addition, population studies using statins are ideal candidates for further investigations of the efficacy of statins in mitigating the risk and prevention of psychiatric conditions and their cardiovascular comorbidities.
SWK, JMK, and MB designed the strategy for the present review. SWK, HJK, MJ, JWK, JYL, AW, and BA wrote the first outlined of the review. SWK, JMK, and MB critically revised the draft. All authors read and approved the submitted version.
This study was supported by a grant (BCRI 18018) from Chonnam National University Hospital Biomedical Research Institute to JMK and a grant from the Basic Science Research Program through the National Research Foundation of Korea (NRF-2017R1A2B4010830) to SWK. MB is supported by a NHMRC Senior Principal Research Fellowship (1059660 and 1156072). The funders had no role in study design; in the writing of the report; or in the decision to submit the paper for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Montecucco F, Burger F, Pelli G, Poku NK, Berlier C, Steffens S, et al. Statins inhibit C-reactive protein-induced chemokine secretion, ICAM-1 upregulation and chemotaxis in adherent human monocytes. Rheumatology. (2009) 48:233–42. doi: 10.1093/rheumatology/ken466
2. Quist-Paulsen P. Statins and inflammation: an update. Curr Opin Cardiol. (2010) 25:399–405. doi: 10.1097/HCO.0b013e3283398e53
3. Link A, Ayadhi T, Bohm M, Nickenig G. Rapid immunomodulation by rosuvastatin in patients with acute coronary syndrome. Eur Heart J. (2006) 27:2945–55. doi: 10.1093/eurheartj/ehl277
4. Mayer C, Gruber HJ, Landl EM, Pailer S, Scharnagl H, Truschnig-Wilders M, et al. Rosuvastatin reduces interleukin-6-induced expression of C-reactive protein in human hepatocytes in a STAT3- and C/EBP-dependent fashion. Int J Clin Pharmacol Ther. (2007) 45:319–27. doi: 10.5414/CPP45319
5. Schachter M. Chemical, pharmacokinetic and pharmacodynamic properties of statins: an update. Fundam Clin Pharmacol. (2005) 19:117–25. doi: 10.1111/j.1472-8206.2004.00299.x
6. Rojas-Fernandez CH, Cameron JC. Is statin-associated cognitive impairment clinically relevant? A narrative review and clinical recommendations. Ann Pharmacother. (2012) 46:549–57. doi: 10.1345/aph.1Q620
7. Kim SW, Bae KY, Kim JM, Shin IS, Hong YJ, Ahn Y, et al. The use of statins for the treatment of depression in patients with acute coronary syndrome. Transl Psychiatry. (2015) 5:e620. doi: 10.1038/tp.2015.116
8. Mora S, Ridker PM. Justification for the use of statins in primary prevention: an intervention trial evaluating rosuvastatin (JUPITER)–can C-reactive protein be used to target statin therapy in primary prevention? Am J Cardiol. (2006) 97:33a−41a. doi: 10.1016/j.amjcard.2005.11.014
9. Koh KK. Effects of statins on vascular wall: vasomotor function, inflammation, and plaque stability. Cardiovasc Res. (2000) 47:648–57. doi: 10.1016/S0008-6363(00)00146-2
10. Haroon E, Daguanno AW, Woolwine BJ, Goldsmith DR, Baer WM, Wommack EC, et al. Antidepressant treatment resistance is associated with increased inflammatory markers in patients with major depressive disorder. Psychoneuroendocrinology. (2018) 95:43–9. doi: 10.1016/j.psyneuen.2018.05.026
11. Bedi O, Dhawan V, Sharma PL, Kumar P. Pleiotropic effects of statins: new therapeutic targets in drug design. Naunyn Schmiedebergs Arch Pharmacol. (2016) 389:695–712. doi: 10.1007/s00210-016-1252-4
12. Horton JD, Goldstein JL, Brown MS. SREBPs: activators of the complete program of cholesterol and fatty acid synthesis in the liver. J Clin Invest. (2002) 109:1125–31. doi: 10.1172/jci15593
13. Zhang J, Liu Q. Cholesterol metabolism and homeostasis in the brain. Protein Cell. (2015) 6:254–64. doi: 10.1007/s13238-014-0131-3
14. Gibson Wood W, Eckert GP, Igbavboa U, Muller WE. Amyloid beta-protein interactions with membranes and cholesterol: causes or casualties of Alzheimer's disease. Biochim Biophys Acta. (2003) 1610:281–90. doi: 10.1016/S0005-2736(03)00025-7
15. Babelova A, Sedding DG, Brandes RP. Anti-atherosclerotic mechanisms of statin therapy. Curr Opin Pharmacol. (2013) 13:260–4. doi: 10.1016/j.coph.2013.01.004
16. Koskinas KC, Windecker S, Raber L. Regression of coronary atherosclerosis: current evidence and future perspectives. Trends Cardiovasc Med. (2016) 26:150–61. doi: 10.1016/j.tcm.2015.05.004
17. Sirtori CR. The pharmacology of statins. Pharmacol Res. (2014) 88:3–11. doi: 10.1016/j.phrs.2014.03.002
18. Greenwood J, Mason JC. Statins and the vascular endothelial inflammatory response. Trends Immunol. (2007) 28:88–98. doi: 10.1016/j.it.2006.12.003
19. Liao JK. Isoprenoids as mediators of the biological effects of statins. J Clin Invest. (2002) 110:285–8. doi: 10.1172/jci16421
20. Diamantis E, Kyriakos G, Quiles-Sanchez LV, Farmaki P, Troupis T. The Anti-inflammatory effects of statins on coronary artery disease: an updated review of the literature. Curr Cardiol Rev. (2017) 13:209–16. doi: 10.2174/1573403x13666170426104611
21. Greenwood J, Steinman L, Zamvil SS. Statin therapy and autoimmune disease: from protein prenylation to immunomodulation. Nat Rev Immunol. (2006) 6:358–70. doi: 10.1038/nri1839
22. Morris G, Fernandes BS, Puri BK, Walker AJ, Carvalho AF, Berk M. Leaky brain in neurological and psychiatric disorders: Drivers and consequences. Aust N Z J Psychiatry. (2018) 52:924–48. doi: 10.1177/0004867418796955
23. Wang S, Xie X, Lei T, Zhang K, Lai B, Zhang Z, et al. Statins attenuate activation of the NLRP3 inflammasome by oxidized LDL or TNFalpha in vascular endothelial cells through a PXR-dependent mechanism. Mol Pharmacol. (2017) 92:256–64. doi: 10.1124/mol.116.108100
24. Ampuero J, Romero-Gomez M. Prevention of hepatocellular carcinoma by correction of metabolic abnormalities: role of statins and metformin. World J Hepatol. (2015) 7:1105–11. doi: 10.4254/wjh.v7.i8.1105
25. Ma Y, Chen Z, Zou Y, Ge J. Atorvastatin represses the angiotensin 2-induced oxidative stress and inflammatory response in dendritic cells via the PI3K/Akt/Nrf 2 pathway. Oxid Med Cell Longev. (2014) 2014:148798. doi: 10.1155/2014/148798
26. Balakumar P, Mahadevan N. Interplay between statins and PPARs in improving cardiovascular outcomes: a double-edged sword? Br J Pharmacol. (2012) 165:373–9. doi: 10.1111/j.1476-5381.2011.01597.x
27. Chataway J, Schuerer N, Alsanousi A, Chan D, MacManus D, Hunter K, et al. Effect of high-dose simvastatin on brain atrophy and disability in secondary progressive multiple sclerosis (MS-STAT): a randomised, placebo-controlled, phase 2 trial. Lancet. (2014) 383:2213–21. doi: 10.1016/s0140-6736(13)62242-4
28. Ramanan VK, Przybelski SA, Graff-Radford J, Castillo AM, Lowe VJ, Mielke MM, et al. Statins and brain health: Alzheimer's disease and cerebrovascular disease biomarkers in older adults. J Alzheimers Dis. (2018) 65:1345–52. doi: 10.3233/jad-180446
29. Penninx BW, Milaneschi Y, Lamers F, Vogelzangs N. Understanding the somatic consequences of depression: biological mechanisms and the role of depression symptom profile. BMC Med. (2013) 11:129. doi: 10.1186/1741-7015-11-129
30. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. (2000) 160:2101–7. doi: 10.1001/archinte.160.14.2101
31. Lupien SJ, McEwen BS, Gunnar MR, Heim C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat Rev Neurosci. (2009) 10:434–45. doi: 10.1038/nrn2639
32. Reus GZ, Fries GR, Stertz L, Badawy M, Passos IC, Barichello T, et al. The role of inflammation and microglial activation in the pathophysiology of psychiatric disorders. Neuroscience. (2015) 300:141–54. doi: 10.1016/j.neuroscience.2015.05.018
33. Sattar NA, Ginsberg H, Ray K, Chapman MJ, Arca M, Averna M, et al. The use of statins in people at risk of developing diabetes mellitus: evidence and guidance for clinical practice. Atheroscler Suppl. (2014) 15:1–15. doi: 10.1016/j.atherosclerosissup.2014.04.001
34. Pan A, Keum N, Okereke OI, Sun Q, Kivimaki M, Rubin RR, et al. Bidirectional association between depression and metabolic syndrome: a systematic review and meta-analysis of epidemiological studies. Diabetes Care. (2012) 35:1171–80. doi: 10.2337/dc11-2055
35. Delgado I, Huet L, Dexpert S, Beau C, Forestier D, Ledaguenel P, et al. Depressive symptoms in obesity: Relative contribution of low-grade inflammation and metabolic health. Psychoneuroendocrinology. (2018) 91:55–61. doi: 10.1016/j.psyneuen.2018.02.030
36. Horowitz MA, Zunszain PA. Neuroimmune and neuroendocrine abnormalities in depression: two sides of the same coin. Ann N Y Acad Sci. (2015) 1351:68–79. doi: 10.1111/nyas.12781
37. Pasco JA, Jacka FN, Williams LJ, Henry MJ, Nicholson GC, Kotowicz MA, et al. Leptin in depressed women: cross-sectional and longitudinal data from an epidemiologic study. J Affect Disord. (2008) 107:221–5. doi: 10.1016/j.jad.2007.07.024
38. Nikkheslat N, Zunszain PA, Horowitz MA, Barbosa IG, Parker JA, Myint AM, et al. Insufficient glucocorticoid signaling and elevated inflammation in coronary heart disease patients with comorbid depression. Brain Behav Immun. (2015) 48:8–18. doi: 10.1016/j.bbi.2015.02.002
39. Anderson G, Berk M, Dodd S, Bechter K, Altamura AC, Dell'osso B, et al. Immuno-inflammatory, oxidative and nitrosative stress, and neuroprogressive pathways in the etiology, course and treatment of schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. (2013) 42:1–4. doi: 10.1016/j.pnpbp.2012.10.008
40. Grigoletti L, Perini G, Rossi A, Biggeri A, Barbui C, Tansella M, et al. Mortality and cause of death among psychiatric patients: a 20-year case-register study in an area with a community-based system of care. Psychol Med. (2009) 39:1875–84. doi: 10.1017/s0033291709005790
41. Heart Protection Study Collaborative G. Effects on 11-year mortality and morbidity of lowering LDL cholesterol with simvastatin for about 5 years in 20,536 high-risk individuals: a randomised controlled trial. Lancet. (2011) 378:2013–20. doi: 10.1016/s0140-6736(11)61125-2
42. Anderson G, Berk M, Dean O, Moylan S, Maes M. Role of immune-inflammatory and oxidative and nitrosative stress pathways in the etiology of depression: therapeutic implications. CNS Drugs. (2014) 28:1–10. doi: 10.1007/s40263-013-0119-1
43. Moylan S, Maes M, Wray NR, Berk M. The neuroprogressive nature of major depressive disorder: pathways to disease evolution and resistance, and therapeutic implications. Mol Psychiatry. (2013) 18:595–606. doi: 10.1038/mp.2012.33
44. Vogelzangs N, Beekman AT, van Reedt Dortland AK, Schoevers RA, Giltay EJ, de Jonge P, et al. Inflammatory and metabolic dysregulation and the 2-year course of depressive disorders in antidepressant users. Neuropsychopharmacology. (2014) 39:1624–34. doi: 10.1038/npp.2014.9
45. Howren MB, Lamkin DM, Suls J. Associations of depression with C-reactive protein, IL-1, and IL-6: a meta-analysis. Psychosom Med. (2009) 71:171–86. doi: 10.1097/PSY.0b013e3181907c1b
46. Fernandez-Sanchez A, Madrigal-Santillan E, Bautista M, Esquivel-Soto J, Morales-Gonzalez A, Esquivel-Chirino C, et al. Inflammation, oxidative stress, and obesity. Int J Mol Sci. (2011) 12:3117–32. doi: 10.3390/ijms12053117
47. Anisman H. Stress, immunity, cytokines and depression. Acta Neuropsychiatr. (2002) 14:251–61. doi: 10.1034/j.1601-5215.2002.140601.x
48. Prossin AR, Koch AE, Campbell PL, Barichello T, Zalcman SS, Zubieta JK. Acute experimental changes in mood state regulate immune function in relation to central opioid neurotransmission: a model of human CNS-peripheral inflammatory interaction. Mol Psychiatry. (2016) 21:243–51. doi: 10.1038/mp.2015.110
49. Turnbull AV, Rivier CL. Regulation of the hypothalamic-pituitary-adrenal axis by cytokines: actions and mechanisms of action. Physiol Rev. (1999) 79:1–71. doi: 10.1152/physrev.1999.79.1.1
50. Hunter RL, Dragicevic N, Seifert K, Choi DY, Liu M, Kim HC, et al. Inflammation induces mitochondrial dysfunction and dopaminergic neurodegeneration in the nigrostriatal system. J Neurochem. (2007) 100:1375–86. doi: 10.1111/j.1471-4159.2006.04327.x
51. Ekdahl CT, Claasen JH, Bonde S, Kokaia Z, Lindvall O. Inflammation is detrimental for neurogenesis in adult brain. Proc Natl Acad Sci USA. (2003) 100:13632–7. doi: 10.1073/pnas.2234031100
52. Stafford L, Berk M. The use of statins after a cardiac intervention is associated with reduced risk of subsequent depression: proof of concept for the inflammatory and oxidative hypotheses of depression? J Clin Psychiatry. (2011) 72:1229–35. doi: 10.4088/JCP.09m05825blu
53. Weitz-Schmidt G. Statins as anti-inflammatory agents. Trends Pharmacol Sci. (2002) 23:482–6. doi: 10.1016/S0165-6147(02)02077-1
54. Young-Xu Y, Chan A, Liao JK, Ravid S, Blatt CM. Long-term statin use and psychological well-being in the elderly. J Am Coll Cardiol. (2003) 42:690–7. doi: 10.1016/S0735-1097(03)00785-X
55. Otte C, Zhao S, Whooley MA. Statin use and risk of depression in patients with coronary heart disease: longitudinal data from the Heart and Soul Study. J Clin Psychiatry. (2012) 73:610–5. doi: 10.4088/JCP.11m07038
56. Yang CC, Jick SS, Jick H. Lipid-lowering drugs and the risk of depression and suicidal behavior. Arch Intern Med. (2003) 163:1926–32. doi: 10.1001/archinte.163.16.1926
57. Pasco JA, Jacka FN, Williams LJ, Henry MJ, Nicholson GC, Kotowicz MA, et al. Clinical implications of the cytokine hypothesis of depression: the association between use of statins and aspirin and the risk of major depression. Psychother Psychosom. (2010) 79:323–5. doi: 10.1159/000319530
58. Al Badarin FJ, Spertus JA, Gosch KL, Buchanan DM, Chan PS. Initiation of statin therapy after acute myocardial infarction is not associated with worsening depressive symptoms: insights from the prospective registry evaluating outcomes after myocardial infarctions: events and recovery (PREMIER) and translational research investigating underlying disparities in acute myocardial infarction patients' health status (TRIUMPH) registries. Am Heart J. (2013) 166:879–86. doi: 10.1016/j.ahj.2013.09.001
59. Redlich C, Berk M, Williams LJ, Sundquist J, Sundquist K, Li X. Statin use and risk of depression: a Swedish national cohort study. BMC Psychiatry. (2014) 14:348. doi: 10.1186/s12888-014-0348-y
60. Chuang CS, Yang TY, Muo CH, Su HL, Sung FC, Kao CH. Hyperlipidemia, statin use and the risk of developing depression: a nationwide retrospective cohort study. Gen Hosp Psychiatry. (2014) 36:497–501. doi: 10.1016/j.genhosppsych.2014.05.008
61. Kim JM, Stewart R, Kang HJ, Bae KY, Kim SW, Shin IS, et al. A prospective study of statin use and poststroke depression. J Clin Psychopharmacol. (2014) 34:72–9. doi: 10.1097/jcp.0000000000000051
62. Kang JH, Kao LT, Lin HC, Tsai MC, Chung SD. Statin use increases the risk of depressive disorder in stroke patients: a population-based study. J Neurol Sci. (2015) 348:89–93. doi: 10.1016/j.jns.2014.11.013
63. Glaus J, Vandeleur CL, Lasserre AM, Strippoli MP, Castelao E, Gholam-Rezaee M, et al. Aspirin and statin use and the subsequent development of depression in men and women: Results from a longitudinal population-based study. J Affect Disord. (2015) 182:126–31. doi: 10.1016/j.jad.2015.03.044
64. Kohler O, Gasse C, Petersen L, Ingstrup KG, Nierenberg AA, Mors O, et al. The effect of concomitant treatment with SSRIs and statins: a population-based study. Am J Psychiatry. (2016) 173:807–15. doi: 10.1176/appi.ajp.2016.15040463
65. Ghanizadeh A, Hedayati A. Augmentation of fluoxetine with lovastatin for treating major depressive disorder, a randomized double-blind placebo controlled-clinical trial. Depress Anxiety. (2013) 30:1084–8. doi: 10.1002/da.22195
66. Haghighi M, Khodakarami S, Jahangard L, Ahmadpanah M, Bajoghli H, Holsboer-Trachsler E, et al. In a randomized, double-blind clinical trial, adjuvant atorvastatin improved symptoms of depression and blood lipid values in patients suffering from severe major depressive disorder. J Psychiatr Res. (2014) 58:109–14. doi: 10.1016/j.jpsychires.2014.07.018
67. Gougol A, Zareh-Mohammadi N, Raheb S, Farokhnia M, Salimi S, Iranpour N, et al. Simvastatin as an adjuvant therapy to fluoxetine in patients with moderate to severe major depression: a double-blind placebo-controlled trial. J Psychopharmacol. (2015) 29:575–81. doi: 10.1177/0269881115578160
68. Abbasi SH, Mohammadinejad P, Shahmansouri N, Salehiomran A, Beglar AA, Zeinoddini A, et al. Simvastatin versus atorvastatin for improving mild to moderate depression in post-coronary artery bypass graft patients: a double-blind, placebo-controlled, randomized trial. J Affect Disord. (2015) 183:149–55. doi: 10.1016/j.jad.2015.04.049
69. Parsaik AK, Singh B, Murad MH, Singh K, Mascarenhas SS, Williams MD, et al. Statins use and risk of depression: a systematic review and meta-analysis. J Affect Disord. (2014) 160:62–7. doi: 10.1016/j.jad.2013.11.026
70. Huang J. Letter by Huang regarding the article, “Statin use increases the risk of depressive disorder in stroke patients: A population-based study”. J Neurol Sci. (2015) 358:471. doi: 10.1016/j.jns.2015.08.023
71. Salagre E, Fernandes BS, Dodd S, Brownstein DJ, Berk M. Statins for the treatment of depression: A meta-analysis of randomized, double-blind, placebo-controlled trials. J Affect Disord. (2016) 200:235–42. doi: 10.1016/j.jad.2016.04.047
72. Kim SW, Kang HJ, Bae KY, Shin IS, Hong YJ, Ahn YK, et al. Interactions between pro-inflammatory cytokines and statins on depression in patients with acute coronary syndrome. Prog Neuropsychopharmacol Biol Psychiatry. (2018) 80:250–4. doi: 10.1016/j.pnpbp.2017.07.003
73. Owen MJ, Sawa A, Mortensen PB. Schizophrenia. Lancet. (2016) 388:86–97. doi: 10.1016/S0140-6736(15)01121-6
74. Miller BJ, Culpepper N, Rapaport MH. C-reactive protein levels in schizophrenia: a review and meta-analysis. Clin Schizophr Relat Psychoses. (2014) 7:223–30. doi: 10.3371/csrp.micu.020813
75. Najjar S, Pearlman DM. Neuroinflammation and white matter pathology in schizophrenia: systematic review. Schizophr Res. (2015) 161:102–12. doi: 10.1016/j.schres.2014.04.041
76. Muller N, Weidinger E, Leitner B, Schwarz MJ. The role of inflammation in schizophrenia. Front Neurosci. (2015) 9:372. doi: 10.3389/fnins.2015.00372
77. Miller BJ, Buckley P, Seabolt W, Mellor A, Kirkpatrick B. Meta-analysis of cytokine alterations in schizophrenia: clinical status and antipsychotic effects. Biol Psychiatry. (2011) 70:663–71. doi: 10.1016/j.biopsych.2011.04.013
78. van Berckel BN, Bossong MG, Boellaard R, Kloet R, Schuitemaker A, Caspers E, et al. Microglia activation in recent-onset schizophrenia: a quantitative (R)-[11C]PK11195 positron emission tomography study. Biol Psychiatry. (2008) 64:820–2. doi: 10.1016/j.biopsych.2008.04.025
79. Keller WR, Kum LM, Wehring HJ, Koola MM, Buchanan RW, Kelly DL. A review of anti-inflammatory agents for symptoms of schizophrenia. J Psychopharmacol. (2013) 27:337–42. doi: 10.1177/0269881112467089
80. Nitta M, Kishimoto T, Muller N, Weiser M, Davidson M, Kane JM, et al. Adjunctive use of nonsteroidal anti-inflammatory drugs for schizophrenia: a meta-analytic investigation of randomized controlled trials. Schizophr Bull. (2013) 39:1230–41. doi: 10.1093/schbul/sbt070
81. Sommer IE, van Westrhenen R, Begemann MJ, de Witte LD, Leucht S, Kahn RS. Efficacy of anti-inflammatory agents to improve symptoms in patients with schizophrenia: an update. Schizophr Bull. (2014) 40:181–91. doi: 10.1093/schbul/sbt139
82. Hennekens CH, Hennekens AR, Hollar D, Casey DE. Schizophrenia and increased risks of cardiovascular disease. Am Heart J. (2005) 150:1115–21. doi: 10.1016/j.ahj.2005.02.007
83. Hanssens L, De Hert M, Kalnicka D, van Winkel R, Wampers M, Van Eyck D, et al. Pharmacological treatment of severe dyslipidaemia in patients with schizophrenia. Int Clin Psychopharmacol. (2007) 22:43–9. doi: 10.1097/YIC.0b013e3280113d3b
84. Tajik-Esmaeeli S, Moazen-Zadeh E, Abbasi N, Shariat SV, Rezaei F, Salehi B, et al. Simvastatin adjunct therapy for negative symptoms of schizophrenia: a randomized double-blind placebo-controlled trial. Int Clin Psychopharmacol. (2017) 32:87–94. doi: 10.1097/yic.0000000000000159
85. Chaudhry IB, Husain N, Drake R, Dunn G, Husain MO, Kazmi A, et al. Add-on clinical effects of simvastatin and ondansetron in patients with schizophrenia stabilized on antipsychotic treatment: pilot study. Ther Adv Psychopharmacol. (2014) 4:110–6. doi: 10.1177/2045125313511487
86. Deakin JHN, Parkier JJ, Husain MO, Kazmi A, Rahman R. Efficacy of ondansetron and simvastatin on cognition and negative symptoms in established schizophrenia. Neuropsychopharmacology. (2014) 39:S355–6.
87. Vincenzi B, Stock S, Borba CP, Cleary SM, Oppenheim CE, Petruzzi LJ, et al. A randomized placebo-controlled pilot study of pravastatin as an adjunctive therapy in schizophrenia patients: effect on inflammation, psychopathology, cognition and lipid metabolism. Schizophr Res. (2014) 159:395–403. doi: 10.1016/j.schres.2014.08.021
88. Sayyah M, Boostani H, Ashrafpoori M, Pakseresht S. Effects of atorvastatin on negative sign in chronic schizophrenia: a double blind clinical trial. Iran J Pharm Res. (2015) 14:1269–74.
89. Ghanizadeh A, Rezaee Z, Dehbozorgi S, Berk M, Akhondzadeh S. Lovastatin for the adjunctive treatment of schizophrenia: a preliminary randomized double-blind placebo-controlled trial. Psychiatry Res. (2014) 219:431–5. doi: 10.1016/j.psychres.2014.06.039
90. Kim SW, Stewart R, Park WY, Jhon M, Lee JY, Kim SY, et al. Latent iron deficiency as a marker of negative symptoms in patients with first-episode schizophrenia spectrum disorder. Nutrients. (2018) 10:E1707. doi: 10.3390/nu10111707
91. Leucht S, Arbter D, Engel RR, Kissling W, Davis JM. How effective are second-generation antipsychotic drugs? A meta-analysis of placebo-controlled trials. Mol Psychiatry. (2009) 14:429–47. doi: 10.1038/sj.mp.4002136
92. Kato TA, Monji A, Mizoguchi Y, Hashioka S, Horikawa H, Seki Y, et al. Anti-Inflammatory properties of antipsychotics via microglia modulations: are antipsychotics a ‘fire extinguisher’ in the brain of schizophrenia? Mini Rev Med Chem. (2011) 11:565–74. doi: 10.2174/138955711795906941
93. Athyros VG, Katsiki N, Karagiannis A, Mikhailidis DP. High-intensity statin therapy and regression of coronary atherosclerosis in patients with diabetes mellitus. J Diabetes Compl. (2015) 29:142–5. doi: 10.1016/j.jdiacomp.2014.10.004
94. Khemasuwan D, Chae YK, Gupta S, Carpio A, Yun JH, Neagu S, et al. Dose-related effect of statins in venous thrombosis risk reduction. Am J Med. (2011) 124:852–9. doi: 10.1016/j.amjmed.2011.04.019
95. Wang Q, Zengin A, Deng C, Li Y, Newell KA, Yang GY, et al. High dose of simvastatin induces hyperlocomotive and anxiolytic-like activities: The association with the up-regulation of NMDA receptor binding in the rat brain. Exp Neurol. (2009) 216:132–8. doi: 10.1016/j.expneurol.2008.11.016
96. Berk M, Copolov D, Dean O, Lu K, Jeavons S, Schapkaitz I, et al. N-acetyl cysteine as a glutathione precursor for schizophrenia–a double-blind, randomized, placebo-controlled trial. Biol Psychiatry. (2008) 64:361–8. doi: 10.1016/j.biopsych.2008.03.004
97. Berk M, Copolov DL, Dean O, Lu K, Jeavons S, Schapkaitz I, et al. N-acetyl cysteine for depressive symptoms in bipolar disorder–a double-blind randomized placebo-controlled trial. Biol Psychiatry. (2008) 64:468–75. doi: 10.1016/j.biopsych.2008.04.022
98. Breier A, Liffick E, Hummer TA, Vohs JL, Yang Z, Mehdiyoun NF, et al. Effects of 12-month, double-blind N-acetyl cysteine on symptoms, cognition and brain morphology in early phase schizophrenia spectrum disorders. Schizophr Res. (2018) 199:395–402. doi: 10.1016/j.schres.2018.03.012
99. Correll CU, Kane JM. Schizophrenia: mechanism of action of current and novel treatments. J Clin Psychiatry. (2014) 75:347–8. doi: 10.4088/JCP.13078co8c
100. Wysokinski A, Strzelecki D, Kloszewska I. Levels of triglycerides, cholesterol, LDL, HDL and glucose in patients with schizophrenia, unipolar depression and bipolar disorder. Diabetes Metab Syndr. (2015) 9:168–76. doi: 10.1016/j.dsx.2015.04.004
101. Lally J, Gallagher A, Bainbridge E, Avalos G, Ahmed M, McDonald C. Increases in triglyceride levels are associated with clinical response to clozapine treatment. J Psychopharmacol. (2013) 27:401–3. doi: 10.1177/0269881112472568
102. Procyshyn RM, Honer WG, Barr AM. Do serum lipids predict response to clozapine treatment? J Psychiatry Neurosci. (2009) 34:168
103. Krakowski M, Czobor P. Cholesterol and cognition in schizophrenia: a double-blind study of patients randomized to clozapine, olanzapine and haloperidol. Schizophr Res. (2011) 130:27–33. doi: 10.1016/j.schres.2011.04.005
104. Carlson MC, Helms MJ, Steffens DC, Burke JR, Potter GG, Plassman BL. Midlife activity predicts risk of dementia in older male twin pairs. Alzheimers Dement. (2008) 4:324–31. doi: 10.1016/j.jalz.2008.07.002
105. Brookmeyer R, Corrada MM, Curriero FC, Kawas C. Survival following a diagnosis of Alzheimer disease. Arch Neurol. (2002) 59:1764–7. doi: 10.1001/archneur.59.11.1764
106. Akiyama H, Barger S, Barnum S, Bradt B, Bauer J, Cole GM, et al. Inflammation and Alzheimer's disease. Neurobiol Aging. (2000) 21:383–421.
107. De Strooper B, Annaert W. Proteolytic processing and cell biological functions of the amyloid precursor protein. J Cell Sci. (2000) 113 (Pt 11):1857–70.
108. Kumar A, Singh A, Ekavali. A review on Alzheimer's disease pathophysiology and its management: an update. Pharmacol Rep. (2015) 67:195–203. doi: 10.1016/j.pharep.2014.09.004
109. Zheng C, Zhou XW, Wang JZ. The dual roles of cytokines in Alzheimer's disease: update on interleukins, TNF-alpha, TGF-beta and IFN-gamma. Transl Neurodegener. (2016) 5:7. doi: 10.1186/s40035-016-0054-4
110. de Chaves EP, Narayanaswami V. Apolipoprotein E and cholesterol in aging and disease in the brain. Future Lipidol. (2008) 3:505–30. doi: 10.2217/17460875.3.5.505
111. Gamba P, Testa G, Sottero B, Gargiulo S, Poli G, Leonarduzzi G. The link between altered cholesterol metabolism and Alzheimer's disease. Ann N Y Acad Sci. (2012) 1259:54–64. doi: 10.1111/j.1749-6632.2012.06513.x
112. Reed B, Villeneuve S, Mack W, DeCarli C, Chui HC, Jagust W. Associations between serum cholesterol levels and cerebral amyloidosis. JAMA Neurol. (2014) 71:195–200. doi: 10.1001/jamaneurol.2013.5390
113. Sun MY, Linsenbardt AJ, Emnett CM, Eisenman LN, Izumi Y, Zorumski CF, Mennerick S. 24(S)-hydroxycholesterol as a modulator of neuronal signaling and survival. Neuroscientist. (2016) 22:132–44. doi: 10.1177/1073858414568122
114. Dias IHK, Milic I, Lip GYH, Devitt A, Polidori MC, Griffiths HR. Simvastatin reduces circulating oxysterol levels in men with hypercholesterolaemia. Redox Biol. (2018) 16:139–45. doi: 10.1016/j.redox.2018.02.014
115. Haag MD, Hofman A, Koudstaal PJ, Stricker BH, Breteler MM. Statins are associated with a reduced risk of Alzheimer disease regardless of lipophilicity. the rotterdam study. J Neurol Neurosurg Psychiatry. (2009) 80:13–7. doi: 10.1136/jnnp.2008.150433
116. Zandi PP, Sparks DL, Khachaturian AS, Tschanz J, Norton M, Steinberg M, et al. Do statins reduce risk of incident dementia and Alzheimer disease? The cache county study. Arch Gen Psychiatry. (2005) 62:217–24. doi: 10.1001/archpsyc.62.2.217
117. Sparks DL, Kryscio RJ, Sabbagh MN, Connor DJ, Sparks LM, Liebsack C. Reduced risk of incident AD with elective statin use in a clinical trial cohort. Curr Alzheimer Res. (2008) 5:416–21. doi: 10.2174/156720508785132316
118. Li G, Shofer JB, Rhew IC, Kukull WA, Peskind ER, McCormick W, et al. Age-varying association between statin use and incident Alzheimer's disease. J Am Geriatr Soc. (2010) 58:1311–7. doi: 10.1111/j.1532-5415.2010.02906.x
119. Zissimopoulos JM, Barthold D, Brinton RD, Joyce G. Sex and race differences in the association between statin use and the incidence of Alzheimer disease. JAMA Neurol. (2017) 74:225–32. doi: 10.1001/jamaneurol.2016.3783
120. Zamrini E, McGwin G, Roseman JM. Association between statin use and Alzheimer's disease. Neuroepidemiology. (2004) 23:94–8. doi: 10.1159/000073981
121. Simons M, Schwarzler F, Lutjohann D, von Bergmann K, Beyreuther K, Dichgans J, et al. Treatment with simvastatin in normocholesterolemic patients with Alzheimer's disease: a 26-week randomized, placebo-controlled, double-blind trial. Ann Neurol. (2002) 52:346–50. doi: 10.1002/ana.10292
122. Sparks DL, Connor DJ, Sabbagh MN, Petersen RB, Lopez J, Browne P. Circulating cholesterol levels, apolipoprotein E genotype and dementia severity influence the benefit of atorvastatin treatment in Alzheimer's disease: results of the Alzheimer's Disease Cholesterol-Lowering Treatment (ADCLT) trial. Acta Neurol Scand Suppl. (2006) 185:3–7. doi: 10.1111/j.1600-0404.2006.00690.x
123. Feldman HH, Doody RS, Kivipelto M, Sparks DL, Waters DD, Jones RW, et al. Randomized controlled trial of atorvastatin in mild to moderate Alzheimer disease: LEADe. Neurology. (2010) 74:956–64. doi: 10.1212/WNL.0b013e3181d6476a
124. Sano M, Bell KL, Galasko D, Galvin JE, Thomas RG, van Dyck CH, Aisen PS. A randomized, double-blind, placebo-controlled trial of simvastatin to treat Alzheimer disease. Neurology. (2011) 77:556–63. doi: 10.1212/WNL.0b013e318228bf11
125. Lin FC, Chuang YS, Hsieh HM, Lee TC, Chiu KF, Liu CK, et al. Early statin use and the progression of Alzheimer disease: a total population-based case-control study. Medicine. (2015) 94:e2143. doi: 10.1097/md.0000000000002143
126. Chu CS, Tseng PT, Stubbs B, Chen TY, Tang CH, Li DJ, et al. Use of statins and the risk of dementia and mild cognitive impairment: a systematic review and meta-analysis. Sci Rep. (2018) 8:5804. doi: 10.1038/s41598-018-24248-8
127. Power MC, Weuve J, Sharrett AR, Blacker D, Gottesman RF. Statins, cognition, and dementia—systematic review and methodological commentary. Nat Rev Neurol. (2015) 11:220–9. doi: 10.1038/nrneurol.2015.35
128. Blum A, Shamburek R. The pleiotropic effects of statins on endothelial function, vascular inflammation, immunomodulation and thrombogenesis. Atherosclerosis. (2009) 203:325–30. doi: 10.1016/j.atherosclerosis.2008.08.022
129. Taburyanskaya M, Hassig T. Statins and delirium: is there a role? Curr Atheroscler Rep. (2015) 17:470. doi: 10.1007/s11883-014-0470-9
130. Vallabhajosyula S, Kanmanthareddy A, Erwin PJ, Esterbrooks DJ, Morrow LE. Role of statins in delirium prevention in critical ill and cardiac surgery patients: A systematic review and meta-analysis. J Crit Care. (2017) 37:189–96. doi: 10.1016/j.jcrc.2016.09.025
131. Leboyer M, Soreca I, Scott J, Frye M, Henry C, Tamouza R, et al. Can bipolar disorder be viewed as a multi-system inflammatory disease? J Affect Disord. (2012) 141:1–10. doi: 10.1016/j.jad.2011.12.049
132. Ghanizadeh A, OmraniSigaroodi M, Javadpour A, Dabbaghmanesh MH, Shafiee S. Lovastatin as an adjuvant to lithium for treating manic phase of bipolar disorder: a 4-week, randomized, double-blind, placebo-controlled clinical trial. Depress Res Treat. (2014) 2014:730505. doi: 10.1155/2014/730505
133. Bellosta S, Paoletti R, Corsini A. Safety of statins: focus on clinical pharmacokinetics and drug interactions. Circulation. (2004) 109:Iii50–7. doi: 10.1161/01.CIR.0000131519.15067.1f
134. Cohen JD, Brinton EA, Ito MK, Jacobson TA. Understanding statin use in America and Gaps in patient education (USAGE): an internet-based survey of 10,138 current and former statin users. J Clin Lipidol. (2012) 6:208–15. doi: 10.1016/j.jacl.2012.03.003
135. Cornier MA, Eckel RH. Non-traditional dosing of statins in statin-intolerant patients-is it worth a try? Curr Atheroscler Rep. (2015) 17:475. doi: 10.1007/s11883-014-0475-4
136. Bruckert E, Hayem G, Dejager S, Yau C, Begaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients–the PRIMO study. Cardiovasc Drugs Ther. (2005) 19:403–14. doi: 10.1007/s10557-005-5686-z
137. Cooper JM, Jones AL. Neuroleptic malignant syndrome or a statin drug reaction? A case report. Clin Neuropharmacol. (2009) 32:348–9. doi: 10.1097/WNF.0b013e3181acc92d
138. Moriarty PM, Thompson PD, Cannon CP, Guyton JR, Bergeron J, Zieve FJ, et al. Efficacy and safety of alirocumab vs ezetimibe in statin-intolerant patients, with a statin rechallenge arm: the odyssey alternative randomized trial. J Clin Lipidol. (2015) 9:758–69. doi: 10.1016/j.jacl.2015.08.006
139. Nissen SE, Stroes E, Dent-Acosta RE, Rosenson RS, Lehman SJ, Sattar N, et al. Efficacy and tolerability of evolocumab vs ezetimibe in patients with muscle-related statin intolerance: the GAUSS-3 randomized clinical trial. JAMA. (2016) 315:1580–90. doi: 10.1001/jama.2016.3608
140. Taylor BA, Lorson L, White CM, Thompson PD. A randomized trial of coenzyme Q10 in patients with confirmed statin myopathy. Atherosclerosis. (2015) 238:329–35. doi: 10.1016/j.atherosclerosis.2014.12.016
141. Data-Franco J, Berk M. The nocebo effect: a clinicians guide. Aust N Z J Psychiatry. (2013) 47:617–23. doi: 10.1177/0004867412464717
142. Dodd S, Dean OM, Vian J, Berk M. A review of the theoretical and biological understanding of the nocebo and placebo phenomena. Clin Ther. (2017) 39:469–76. doi: 10.1016/j.clinthera.2017.01.010
143. Saxon DR, Eckel RH. Statin intolerance: a literature review and management strategies. Prog Cardiovasc Dis. (2016) 59:153–64. doi: 10.1016/j.pcad.2016.07.009
144. Otruba P, Kanovsky P, Hlustik P. Treatment with statins and peripheral neuropathy: results of 36-months a prospective clinical and neurophysiological follow-up. Neuro Endocrinol Lett. (2011) 32:688–90.
145. Sattar N, Preiss D, Murray HM, Welsh P, Buckley BM, de Craen AJ, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet. (2010) 375:735–42. doi: 10.1016/s0140-6736(09)61965-6
146. Preiss D, Seshasai SR, Welsh P, Murphy SA, Ho JE, Waters DD, et al. Risk of incident diabetes with intensive-dose compared with moderate-dose statin therapy: a meta-analysis. JAMA. (2011) 305:2556–64. doi: 10.1001/jama.2011.860
147. Waters DD, Ho JE, DeMicco DA, Breazna A, Arsenault BJ, Wun CC, et al. Predictors of new-onset diabetes in patients treated with atorvastatin: results from 3 large randomized clinical trials. J Am Coll Cardiol. (2011) 57:1535–45. doi: 10.1016/j.jacc.2010.10.047
148. Ridker PM, Pradhan A, MacFadyen JG, Libby P, Glynn RJ. Cardiovascular benefits and diabetes risks of statin therapy in primary prevention: an analysis from the JUPITER trial. Lancet. (2012) 380:565–71. doi: 10.1016/s0140-6736(12)61190-8
149. Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J. (2016) 37:2999–3058. doi: 10.1093/eurheartj/ehw272
150. Kim SH. Drug treatment of dyslipidemia. J Korean Med Assoc. (2016) 59:366–73. doi: 10.5124/jkma.2016.59.5.366
151. Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. (2014) 63:2889–934. doi: 10.1016/j.jacc.2013.11.002
152. Spence JD, Dresser GK. Overcoming challenges with statin therapy. J Am Heart Assoc. (2016) 5:e002497. doi: 10.1161/jaha.115.002497
153. Adhyaru BB, Jacobson TA. Safety and efficacy of statin therapy. Nat Rev Cardiol. (2018) 15:757–69. doi: 10.1038/s41569-018-0098-5
154. Thompson PD, Panza G, Zaleski A, Taylor B. Statin-associated side effects. J Am Coll Cardiol. (2016) 67:2395–410. doi: 10.1016/j.jacc.2016.02.071
155. Broncel M, Gorzelak-Pabis P, Sahebkar A, Serejko K, Ursoniu S, Rysz J, et al. Sleep changes following statin therapy: a systematic review and meta-analysis of randomized placebo-controlled polysomnographic trials. Arch Med Sci. (2015) 11:915–26. doi: 10.5114/aoms.2015.54841
156. Davison KM, Kaplan BJ. Lipophilic statin use and suicidal ideation in a sample of adults with mood disorders. Crisis. (2014) 35:278–82. doi: 10.1027/0227-5910/a000260
157. While A, Keen L. The effects of statins on mood: a review of the literature. Eur J Cardiovasc Nurs. (2012) 11:85–96. doi: 10.1016/j.ejcnurse.2010.08.008
158. Marcum ZA, Vande Griend JP, Linnebur SA. FDA drug safety communications: a narrative review and clinical considerations for older adults. Am J Geriatr Pharmacother. (2012) 10:264–71. doi: 10.1016/j.amjopharm.2012.05.002
159. Muldoon MF, Barger SD, Ryan CM, Flory JD, Lehoczky JP, Matthews KA, et al. Effects of lovastatin on cognitive function and psychological well-being. Am J Med. (2000) 108:538–46. doi: 10.1016/S0002-9343(00)00353-3
160. Muldoon MF, Ryan CM, Sereika SM, Flory JD, Manuck SB. Randomized trial of the effects of simvastatin on cognitive functioning in hypercholesterolemic adults. Am J Med. (2004) 117:823–9. doi: 10.1016/j.amjmed.2004.07.041
161. Wagstaff LR, Mitton MW, Arvik BM, Doraiswamy PM. Statin-associated memory loss: analysis of 60 case reports and review of the literature. Pharmacotherapy. (2003) 23:871–80. doi: 10.1592/phco.23.7.871.32720
162. Bernick C, Katz R, Smith NL, Rapp S, Bhadelia R, Carlson M, et al. Statins and cognitive function in the elderly: the cardiovascular health study. Neurology. (2005) 65:1388–94. doi: 10.1212/01.wnl.0000182897.18229.ec
163. Etminan M, Gill S, Samii A. The role of lipid-lowering drugs in cognitive function: a meta-analysis of observational studies. Pharmacotherapy. (2003) 23:726–30. doi: 10.1592/phco.23.6.726.32184
164. Ott BR, Daiello LA, Dahabreh IJ, Springate BA, Bixby K, Murali M, et al. Do statins impair cognition? A systematic review and meta-analysis of randomized controlled trials. J Gen Intern Med. (2015) 30:348–58. doi: 10.1007/s11606-014-3115-3
165. Swiger KJ, Manalac RJ, Blumenthal RS, Blaha MJ, Martin SS. Statins and cognition: a systematic review and meta-analysis of short- and long-term cognitive effects. Mayo Clin Proc. (2013) 88:1213–21. doi: 10.1016/j.mayocp.2013.07.013
166. Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. (1981) 30:239–45. doi: 10.1038/clpt.1981.154
167. Asellus P, Nordstrom P, Jokinen J. Cholesterol and CSF 5-HIAA in attempted suicide. J Affect Disord. (2010) 125:388–92. doi: 10.1016/j.jad.2010.02.111
168. De Berardis D, Conti CM, Serroni N, Moschetta FS, Carano A, Salerno RM, et al. The role of cholesterol levels in mood disorders and suicide. J Biol Regul Homeost Agents. (2009) 23:133–40.
169. Shrivastava S, Pucadyil TJ, Paila YD, Ganguly S, Chattopadhyay A. Chronic cholesterol depletion using statin impairs the function and dynamics of human serotonin(1A) receptors. Biochemistry. (2010) 49:5426–35. doi: 10.1021/bi100276b
170. Cham S, Koslik HJ, Golomb BA. Mood, personality, and behavior changes during treatment with statins: a case series. Drug Saf Case Rep. (2016) 3:1. doi: 10.1007/s40800-015-0024-2
171. Golomb BA, Kane T, Dimsdale JE. Severe irritability associated with statin cholesterol-lowering drugs. QJM. (2004) 97:229–35. doi: 10.1093/qjmed/hch035
172. Roth T, Richardson GR, Sullivan JP, Lee RM, Merlotti L, Roehrs T. Comparative effects of pravastatin and lovastatin on nighttime sleep and daytime performance. Clin Cardiol. (1992) 15:426–32. doi: 10.1002/clc.4960150607
173. Takada M, Fujimoto M, Yamazaki K, Takamoto M, Hosomi K. Association of statin use with sleep disturbances: data mining of a spontaneous reporting database and a prescription database. Drug Saf. (2014) 37:421–31. doi: 10.1007/s40264-014-0163-x
174. Andrade C. Relative to SSRI users, SSRI-statin users have fewer psychiatric hospital contacts and no increase in suicidal behaviour or all-cause mortality. Evid Based Ment Health. (2017) 20:60. doi: 10.1136/eb-2016-102566
175. Niemi M, Pasanen MK, Neuvonen PJ. Organic anion transporting polypeptide 1B1: a genetically polymorphic transporter of major importance for hepatic drug uptake. Pharmacol Rev. (2011) 63:157–81. doi: 10.1124/pr.110.002857
176. Bellosta S, Corsini A. Statin drug interactions and related adverse reactions. Expert Opin Drug Saf. (2012) 11:933–46. doi: 10.1517/14740338.2012.712959
177. Paoletti R, Corsini A, Bellosta S. Pharmacological interactions of statins. Atheroscler Suppl. (2002) 3:35–40. doi: 10.1016/S1567-5688(02)00002-8
178. Karnik NS, Maldonado JR. Antidepressant and statin interactions: a review and case report of simvastatin and nefazodone-induced rhabdomyolysis and transaminitis. Psychosomatics. (2005) 46:565–8. doi: 10.1176/appi.psy.46.6.565
179. Wang E, Casciano CN, Clement RP, Johnson WW. HMG-CoA reductase inhibitors (statins) characterized as direct inhibitors of P-glycoprotein. Pharm Res. (2001) 18:800–6. doi: 10.1023/A:1011036428972
180. Shen H, Li R, Yan R, Zhou X, Feng X, Zhao M, Xiao H. Adjunctive therapy with statins in schizophrenia patients: a meta-analysis and implications. Psychiatry Res. (2018) 262:84–93. doi: 10.1016/j.psychres.2018.02.018
Keywords: statin, depression, schizophrenia, dementia, inflammation
Citation: Kim SW, Kang HJ, Jhon M, Kim JW, Lee JY, Walker AJ, Agustini B, Kim JM and Berk M (2019) Statins and Inflammation: New Therapeutic Opportunities in Psychiatry. Front. Psychiatry 10:103. doi: 10.3389/fpsyt.2019.00103
Received: 21 November 2018; Accepted: 12 February 2019;
Published: 05 March 2019.
Edited by:
Naguib Mechawar, McGill University, CanadaReviewed by:
Adonis Sfera, Loma Linda University, United StatesCopyright © 2019 Kim, Kang, Jhon, Kim, Lee, Walker, Agustini, Kim and Berk. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jae-Min Kim, am1raW1AY2hvbm5hbS5hYy5rcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.