
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry , 21 December 2018
Sec. Psychological Therapy and Psychosomatics
Volume 9 - 2018 | https://doi.org/10.3389/fpsyt.2018.00690
This article is part of the Research Topic Reducing the Mortality Gap in People with Severe Mental Disorders: The Role of Lifestyle Psychosocial Interventions View all 19 articles
 Andrea Schmitt1,2*
Andrea Schmitt1,2* Isabel Maurus1Moritz J. Rossner1
Isabel Maurus1Moritz J. Rossner1 Astrid Röh1Moritz Lembeck1Martina von Wilmsdorff3Shun Takahashi1,4Boris Rauchmann5
Astrid Röh1Moritz Lembeck1Martina von Wilmsdorff3Shun Takahashi1,4Boris Rauchmann5 Daniel Keeser5
Daniel Keeser5 Alkomiet Hasan1
Alkomiet Hasan1 Berend Malchow6
Berend Malchow6 Peter Falkai1
Peter Falkai1Schizophrenia is a severe psychiatric disorder with a lifetime prevalence of about 1%. People with schizophrenia have a 4-fold higher prevalence of metabolic syndrome than the general population, mainly because of antipsychotic treatment but perhaps also because of decreased physical activity. Metabolic syndrome is a risk factor for cardiovascular diseases, and the risk of these diseases is 2- to 3-fold higher in schizophrenia patients than in the general population. The suicide risk is also higher in schizophrenia, partly as a result of depression, positive, and cognitive symptoms of the disease. The higher suicide rate and higher rate of cardiac mortality, a consequence of the increased prevalance of cardiovascular diseases, contribute to the reduced life expectancy, which is up to 20 years lower than in the general population. Regular physical activity, especially in combination with psychosocial and dietary interventions, can improve parameters of the metabolic syndrome and cardiorespiratory fitness. Furthermore, aerobic exercise has been shown to improve cognitive deficits; total symptom severity, including positive and negative symptoms; depression; quality of life; and global functioning. High-intensity interval endurance training is a feasible and effective way to improve cardiorespiratory fitness and metabolic parameters and has been established as such in somatic disorders. It may have more beneficial effects on the metabolic state than more moderate and continuous endurance training methods, but to date it has not been investigated in schizophrenia patients in controlled, randomized trials. This review discusses physical training methods to improve cardiorespiratory fitness and reduce metabolic syndrome risk factors and symptoms in schizophrenia patients. The results of studies and future high-quality clinical trials are expected to lead to the development of an evidence-based physical training program for patients that includes practical recommendations, such as the optimal length and type of aerobic exercise programs and the ideal combination of exercise, psychoeducation, and individual weight management sessions.
Schizophrenia is a severe neuropsychiatric disease that affects ~1% of the population (1, 2). It strikes young adults between 20 and 30 years of age (3), and symptoms persist throughout adult life in 30–50% of affected patients (4, 5). The disease leads to impaired social functioning; for example, only 20% of patients are able to have a job on the primary market, and only about 30% have a stable relationship (5). Because of the high hospitalization rates and high levels of both disease-related incapacity to work and early retirement, schizophrenia-related costs exceed even those of widespread diseases such as cardiovascular diseases (CVD) (6). According to the WHO report on the global burden of disease, schizophrenia is one of the most common conditions associated with a high rate of years lived with disability (YLD), one of the leading causes of disease burden (7), and among the 10 most costly illnesses worldwide (8).
Cognitive impairment is a frequent core feature of schizophrenia (9), in addition to positive and negative symptoms, and is related to the reported volume loss of the hippocampus, a region central to memory, learning, and cognitive integration (10). Cognitive deficits and negative symptoms are the most important predictors for poor social and functional outcome and are major contributors to disability (11). Cognitive deficits are present in domains such as executive function, episodic memory, attention, and social cognition (11–13), functions that are particularly dependent on the hippocampus and prefrontal cortex (14). In schizophrenia, neurodevelopmental disturbances in vulnerable periods of brain development are thought to lead to hippocampal-prefrontal pathway deficits, resulting in the onset of disease symptoms in young adulthood (15). Meta-analyses of structural magnetic resonance imaging (sMRI) studies revealed gray matter volume reduction of 5–10% in the prefrontal cortex and hippocampus in schizophrenia patients (16). In the polymorph layer of the dentate gyrus (CA4) of the hippocampus, decreased numbers of oligodendrocytes (17, 18)—an indicator of disturbed myelination—have been detected in schizophrenia. A meta-analysis of diffusion-tensor imaging (DTI) studies in schizophrenia revealed decreased fractional anisotropy in white matter tracts interconnecting the prefrontal cortex and hippocampus (19); such white matter disruption is known to play a crucial role in cognition and psychopathology (20). Of interest in this context is that schizophrenia patients with overweight and obesity showed disturbed white matter integrity, with lower fractional anisotropy than normal-weight schizophrenia patients (21).
Several environmental factors, such as psychosocial stress associated e.g., with an urban lifestyle or childhood trauma, interact with genetic factors to increase the risk of a chronic disease course (22). The prefrontal cortex and hippocampus are central to cognitive processing and are also involved in the regulation of the neuroendocrine control of stress hormone secretion, including glucocorticoids (23). Whereas, acute stress can increase fear-associated memory, chronic stress with cortisol-based stress reactivity levels has a negative impact on spatial-reference memory and cognitive flexibility, induces hippocampal volume loss, adversely alters dendritic morphology and reduces adult neurogenesis and synaptic plasticity (23). Chronic stress during the pubertal period up to young adulthood, when synaptic pruning and oligodendrocyte-related myelination take place, has been shown to induce symptoms of schizophrenia (24).
Schizophrenia affects daily life and subjective well-being. Low physical activity, impaired physical health, and reduced activities of daily living (25, 26) are just some aspects of the disease. Compared with the general population, individuals with schizophrenia have a 12-fold higher mortality from all external causes (27), which can largely be explained by the high incidence of somatic comorbidities; unhealthy lifestyles, such as high rates of cigarette smoking and low physical activity; and increased rate of suicides (26, 28, 29). Estimates indicate that together these health-related risk factors and suicides reduce life expectancy by nearly 10–20 years compared with the general population (30, 31). A meta-analysis of data from 29 countries on six continents found that mortality was significantly higher among people with mental disorders and that, in 65 studies, the highest mortality rate (relative risk 2.54, 95% CI 2.35–2.75) was among patients with psychosis (31). The relative risk for natural causes, such as CVD, was 1.80 (95% CI 1.71–1.88), but that for unnatural causes, such as suicides, was even higher (7.22, 95% CI 6.43–8.12). Cardiovascular risk was higher in schizophrenia patients than in patients with depressive disorder or multiple psychiatric diagnoses (32). People with severe mental illness, including schizophrenia, had a higher risk of developing coronary heart disease than controls (adjusted hazard ratio 1.54; 95% CI 1.30–1.82) and a higher rate of autonomic nervous system dysfunction, including diminished heart rate variability, hypertension, alterations of the QT interval, and lipid pattern abnormalities (33). During the year after the first diagnosis of psychosis, a study found that the relative risk for all-cause mortality was 54.6 (95% CI 41.3–68.0) per 10,000, whereby the highest relative risk of death was found for self-inflicted injury or poisoning; during this period, the relative risk of death due to heart disease or diabetes did not differ between the group of people with a psychotic disorder and the general outpatient group (34).
In schizophrenia patients, suicidal thoughts and suicide planning and attempts were significantly associated with completed suicide in the following year (35). In first-episode patients, more symptoms of depression, longer duration of untreated psychosis, and positive symptoms, such as hallucinations and delusions, were found to increase the odds of experiencing suicidal ideation (36). Another study found that the severity of negative symptoms was lower in schizophrenia patients who attempted suicide (37). With respect to cognitive performance, decreased global cognitive functioning and visual memory predicted suicidal behavior in non-affective psychosis (38). In a meta-analysis and meta-regression analysis in over 80,000 patients with schizophrenia, depressive symptoms, the Positive and Negative Symptom Scale (PANSS) general score, and the number of hospitalizations were higher in patients with suicidal ideation (39). A history of alcohol use, family history of psychiatric illness, physical comorbidity, history of depression, and depressive symptoms were associated with suicide attempts, whereas poor adherence to treatment, hopelessness, higher intelligence quotient, history of attempted suicide, and being male were most consistently associated with completed suicide (39).
This qualitative review will provide a current overview of clinical studies aimed at reducing the socioeconomic burden of schizophrenia and mortality by addressing metabolic risk factors and symptom severity in schizophrenia patients.
The International Diabetes Federation defines the metabolic syndrome as a combination of increased waist circumference (a mandatory feature) and two of the following criteria: elevated triglycerides, high blood pressure, elevated fasting glucose, and low high-density lipoprotein (HDL) cholesterol (Table 1) (40). Metabolic syndrome is defined slightly differently by the Adult Treatment Panel III (ATP III) of the National Cholesterol Education Program (41) and the adapted Adult Treatment Panel III (ATP III-A) of the American Heart Association (42), both of which require 3 of 5 criteria to be fulfilled (Table 2). In the general population, the metabolic syndrome is associated with a 4-fold increased relative risk to develop type 2 diabetes mellitus (43) and a 2-fold increased relative risk to develop CVD, such as stroke and coronary heart disease (44). Schizophrenia patients have a higher prevalence of metabolic syndrome than the general population and a 2- to 3-fold increased risk for CVD, resulting in increased cardiac mortality (30, 45). Metabolic syndrome was present in 37.3% of schizophrenia patients treated with second-generation antipsychotics and associated with an increased 10-year risk of coronary heart disease (risk ratio 2.18, 95% CI 1.88–2.48) in both male and female patients (risk ratio 1.94, 95% CI 1.65–2.23). Among the criteria for metabolic syndrome, triglyceride levels and waist circumference were significantly associated with the 10-year risk of coronary heart disease events (46). A meta-analysis found that the overall rate of metabolic syndrome in schizophrenia patients was 32.5% (95% CI 30.1–35.0%) and showed only minor differences between treatment settings (inpatient vs. outpatient), country of origin, and gender. Duration of illness and older age had the strongest influence. Among the criteria for metabolic syndrome, waist circumference was the strongest predictor (47). Additionally, the prevalence of metabolic syndrome was higher in patients with negative symptoms, which are associated with a sedentary lifestyle and lack of physical activity (48). Furthermore, in schizophrenia patients metabolic syndrome was significantly associated with cognitive impairment and was found to contribute to cognitive deficits throughout the course of the disease (49).
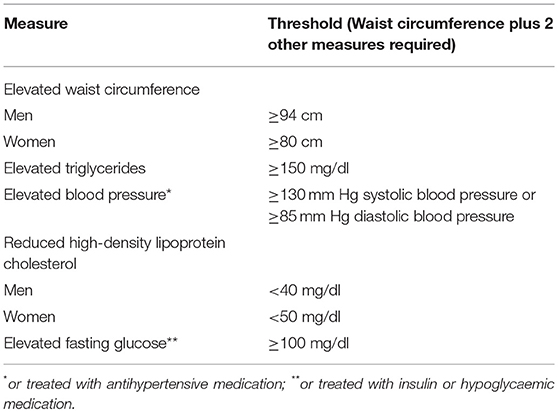
Table 1. International Diabetes Federation criteria for metabolic syndrome.
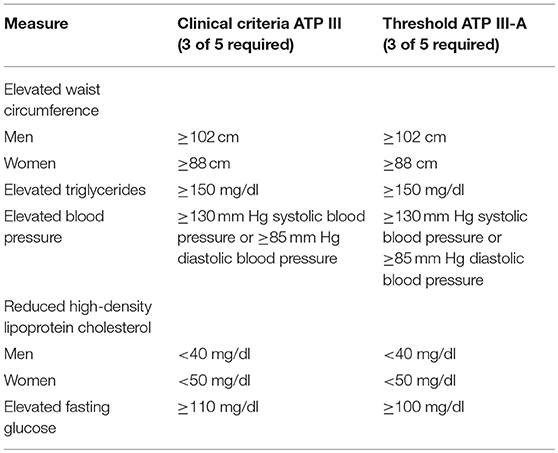
Table 2. Adult Treatment Panel III and III-A criteria for metabolic syndrome.
One study found that the risk of metabolic syndrome was elevated in all patients with severe mental illness (32.6%, 95% CI 30.8–34.3%) and did not differ between patients with schizophrenia and those with bipolar disorder or between patients with bipolar disorder and those with major depression (45). In a meta-analysis of first-episode schizophrenia patients, the rate of metabolic syndrome was only 9.9%; the rate of overweight was 22%; hypertriglyceridemia, 19.6%; low HDL, 21.9%; hyperglycaemia, 6.4%; high blood pressure 24.3%; and smoking, 46.8% (50). This indicates that the cardiovascular risk is lower in first-episode than in multi-episode schizophrenia patients. Longer duration of illness is also predictive for longer treatment with antipsychotics, and treatment with second-generation antipsychotics in particular is a risk factor for developing metabolic syndrome (see below).
Despite reducing positive symptoms, first- and second-generation antipsychotics have demonstrated only poor or no efficacy in improving cognitive deficits and negative symptoms in schizophrenia (51, 52). Depending on the dose, users of typical and atypical antipsychotics had higher rates of sudden cardiac death than non-users (adjusted incidence rate 1.99, 95% CI 1.68–2.34) (53). Furthermore, atypical antipsychotics are known to prolong the QTc interval and increase resting heart rate, thereby affecting autonomic neurocardiac function (54). However, a decrease in heart rate variability has also been shown in unmedicated schizophrenia patients and is a cardiac risk factor, together with low physical fitness (55). A meta-analysis showed that second-generation antipsychotics have fewer extrapyramidal side effects than first-generation drugs, such as haloperidol (52). Many of the most effective second-generation antipsychotics, including olanzapine, clozapine, and risperidone (52, 56), however, are associated with substantial weight gain and sedation (52), leading to increased rates of the metabolic syndrome. In unmedicated and first-episode schizophrenia patients, the overall rate of the metabolic syndrome was only about 10%, the rate of diabetes was only 1–2%, and the rate of overweight was 22–26%. Therefore, the cardiovascular risk can be assumed to be higher in multi-episode patients with a long treatment history (50). A meta-analysis found that patients with severe mental illness who were treated with any antipsychotic had a significantly higher risk of metabolic syndrome than antipsychotic-naïve individuals. The risk was higher with olanzapine and clozapine than with other antipsychotics, especially aripirazole, and higher in patients on polypharmacotherapy than in those on monotherapy (45). Another meta-analysis also found the highest rates of metabolic syndrome in patients treated with clozapine (51.9%) and the lowest rates in unmedicated patients (20.2%) (47). One study found a positive association between a serotonin receptor gene (HTR2C) polymorphism and metabolic syndrome in patients treated with olanzapine, clozapine, and risperidone and that genetic factors may influence the prevalence of the metabolic syndrome in schizophrenia (57).
In summary, lifestyle changes can be assumed to be warranted, especially in multi-episode patients on long-term antipsychotic treatment. To reduce the risk for metabolic syndrome, subsequent CVD, and mortality, add-on therapeutic interventions aimed at improving symptoms of the disease, such as depression or negative symptoms; reducing the smoking rate; and increasing physical activity are needed (58).
A worldwide analysis of adverse health conditions in the general population estimated that physical inactivity causes 6% of the burden of disease from coronary heart disease; 7%, from type 2 diabetes; and 10%, from breast cancer and colon cancer. Overall, inactivity causes 9% of premature mortality (59). The health benefits of physical activity in adults include reduced rates of metabolic syndrome, coronary heart disease, high blood pressure, type 2 diabetes, stroke, depression, and cancer. Additionally, there is strong evidence for increased cardiorespiratory fitness, healthier body mass and composition, and improved cognitive functioning (59). The high prevalence of the metabolic syndrome in schizophrenia may be a result of the disease itself and treatment with antipsychotics (see above) or of sedentary behavior and low physical activity and aerobic fitness, which play an important role in this patient group (60, 61), or a combination of these factors. Studies have repeatedly shown that schizophrenia patients show reduced cardiovascular fitness and physical activity (62). In a meta-analysis of 13 studies, sedentary behavior measured in hours per day was significantly higher in schizophrenia patients (hedges g = 1.13, 95% CI 1.47–4.1) than in healthy controls (63). According to a meta-analysis, schizophrenia patients engage in less moderate (hedges g = −0.45, 95% CI −0.79 to −0.1) and vigorous physical activity (g = −0.4, 95% CI −0.60 to −0.18) than healthy controls, and depressive symptoms and older age are associated with less vigorous physical activity (64). A meta-analysis of 212 schizophrenia patients and 132 healthy individuals confirmed that physical activity was lower in the patient group and showed that decreased physical activity was correlated with impaired quality of life and social functioning, increased social withdrawal, and lower motivation and employment rates (65). Furthermore, low physical fitness was associated with illness duration, smoking, the presence of the metabolic syndrome, and more severe negative, depressive, and cognitive symptoms (26). In schizophrenia patients, the duration of physical activity was negatively correlated with waist circumference and body mass index, while food intake variables correlated with HDL cholesterol and triglyceride levels (66). A systematic review found that lifestyle interventions with psychoeducation, diet, and recommendations on physical activity were associated with significant weight reduction, reduced body mass index, decreased waist circumference, and lower blood glucose levels (67).
Compared with the healthy population, patients with schizophrenia have specific characteristics that decrease their motivation to perform physical activity; these characteristics include sedation related to antipsychotic treatment; schizophrenia symptoms, including anxiety and depression; a lower level of education; little experience with exercise; social withdrawal; and negative symptoms (68, 69). Therefore, it is essential that aerobic exercise interventions aimed at improving cardiovascular fitness are supervised by a sports scientist to increase patients' motivation to participate (70). Schizophrenia patients and healthy controls showed comparable adaptations to endurance training, as assessed by physical working capacity and maximal achieved power, but differences were found in changes of performance at a given lactate concentration (70). Under supervision by a sports scientist, endurance training was feasible and effective in both groups (70). The first studies to investigate aerobic exercise in schizophrenia patients had many methodological limitations (71). Major concerns included missing healthy or patient control groups or both, inadequate sample sizes, and non-randomized or non-controlled designs (72–74). In later endurance training studies, a minimum of 30 min per training session and at least three sessions per week were recommended in schizophrenia patients (75). According to the criteria of the American College of Sports Medicine, in healthy individuals 150 min of moderate training per week are necessary to improve cardiorespiratory fitness (76). A recent cross-sectional study examined the exercise behavior and mental health of 1,237,194 people aged 18 years or older in the USA and found that individuals who exercised had 43.2% fewer days of poor mental health in the past month and a lower mental health burden than the non-exercising groups. Interestingly, the largest effects were seen for popular team sports, cycling, and aerobic and gym activities and for durations of 45 min and frequencies of three to five times per week (77).
New add-on treatment options, such as aerobic exercise, are needed to reduce the risk of cardiometabolic diseases in schizophrenia. However, results of intervention studies examining the effects endurance training on parameters of the metabolic syndrome in schizophrenia patients were mainly negative. In a combined Weight Watchers intervention, exercise had no effects on weight loss (78). A randomized controlled trial in schizophrenia patients consisting of 2 h of aerobic exercise per week over a period of 6 months had no effects on body mass index, body fat percentage, or factors of the metabolic syndrome (79). A meta-analysis of aerobic exercise interventions in patients with bipolar or schizophrenia spectrum disorders found no effects of aerobic exercise on body weight or body mass index (80), and another meta-analysis also reported no effects of aerobic exercise on body mass index in schizophrenia patients (81). In contrast, in a small sample of schizophrenia patients aerobic exercise improved physical activity, blood pressure, and body composition (82). In a randomized study of an intervention comprising aerobic group exercise and individual weight management sessions in obese or overweight patients with schizophrenia, schizoaffective disorder, bipolar disorder, and major depression, weight loss in the intervention group increased progressively over the 18-month study period and differed from the control group (83). In summary, findings to date indicate that isolated exercise interventions are unlikely to induce weight loss in patients with schizophrenia (84). However, adding psychosocial interventions or diet to aerobic exercise programs seem to be a promising approach to reduce body weight. Increased physical activity (pedometer walking) plus motivational interviewing reduced body weight in obese schizophrenia patients after 12 weeks (85). In obese schizophrenia patients, a 3-month lifestyle intervention comprising psychosocial treatment, behavior therapy, and aerobic exercise reduced waist circumference, body weight, and body mass index but did not affect blood lipids or glucose levels (86). In a small study in multi-episode schizophrenia patients, an aerobic exercise program consisting of three 30-min sessions per week over a period of 24 weeks significantly reduced weight and body mass index (73). In a personalized diet and exercise program (3 exercise sessions per week) in 106 schizophrenia patients treated with antipsychotics, the months of participation correlated with weight loss (87) (Table 3).
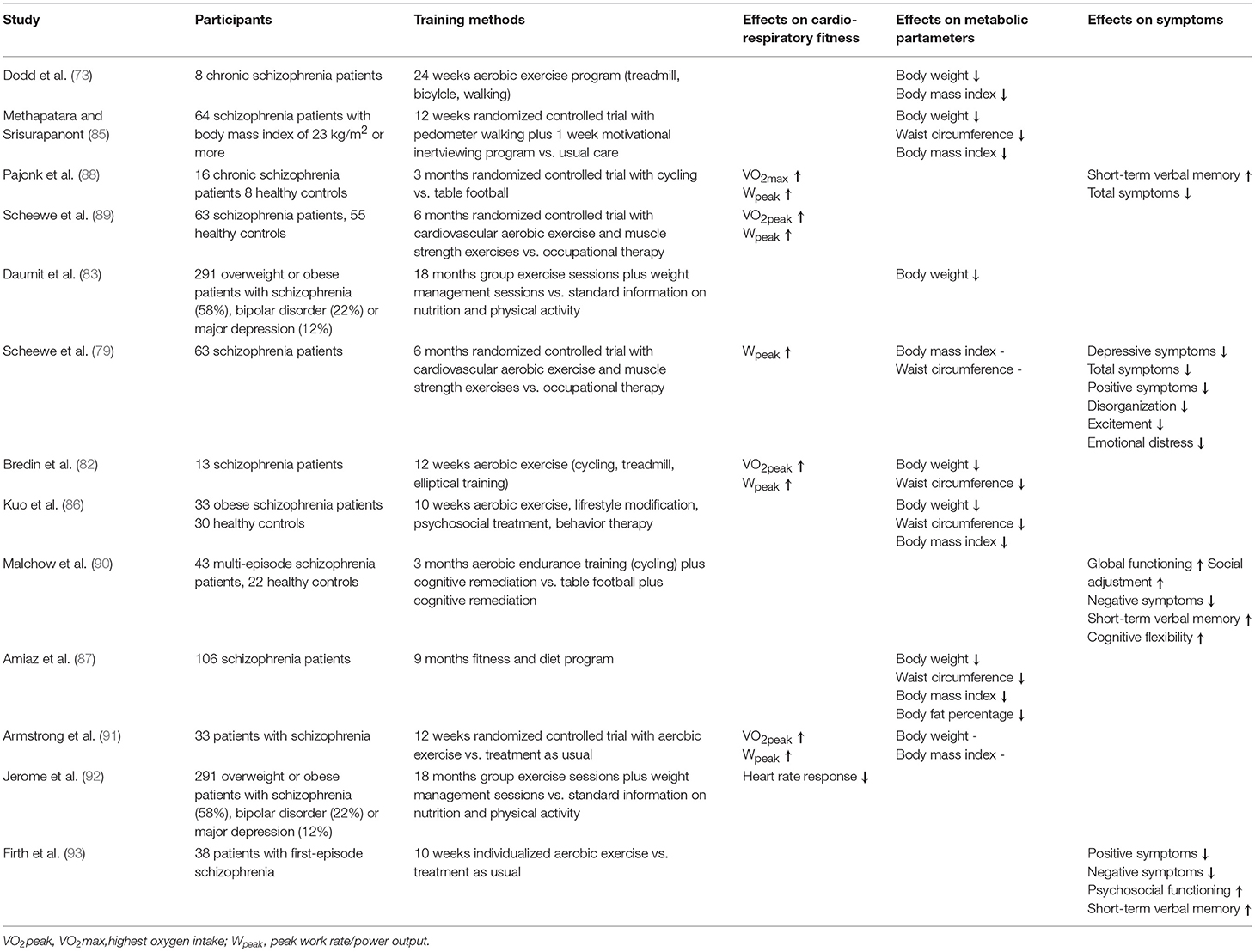
Table 3. Effects of continuous endurance training on metabolic risk factor and symptoms of the disease in patients with schizophrenia.
Because of the need to improve the efficacy of aerobic exercise, higher intensity training, such as high-intensity interval training (HIIT), has been used in obese individuals. HIIT is a promising new method of intensified endurance training. A 12-week HIIT significantly improved metabolic parameters, such as waist circumference, body mass, fasting glucose, HDL cholesterol, and blood pressure, in mentally healthy patients with cardiometabolic risk factors and obesity (94–98). HIT has the highest potential to reduce visceral adipose tissue in obese individuals (99). Compared with continuous training, HIIT significantly reduced insulin resistance, HbA1c, and body weight in healthy adults and reduced fasting glucose in participants at risk of type 2 diabetes (100). However, a recent meta-analysis found no difference between HIIT and moderate-intensity continuous training for body fat reduction (101). This finding was supported by a meta-analysis of 12-month interventions in obese adults, which showed weight loss but found no difference between HIIT and moderate-intensity exercise (102). Another meta-analysis showed that HIIT performed as cycling or running significantly reduced abdominal and visceral fat mass but that running was more effective than cycling (103). In a group of obese men, HIIT significantly improved insulin sensitivity and muscle mitochondrial content (increased muscle mitochondrial content is assumed to be a basic mechanism of effect of HIIT) compared with continuous aerobic training (104). To date, only two studies have applied HIIT interventions in patients with schizophrenia. One evaluated a 14-week program of 40 min HIIT twice a week in first-episode patients and showed a significant decrease in waist circumference and heart rate (105). The other studied an 8-week HIIT program comprising 25-min sessions three times a week in multi-episode patients and showed reduced body weight, body mass index, and resting heart rate (106) (Table 4). Overall, HIIT has the potential to improve parameters of the metabolic syndrome in patients with schizophrenia.
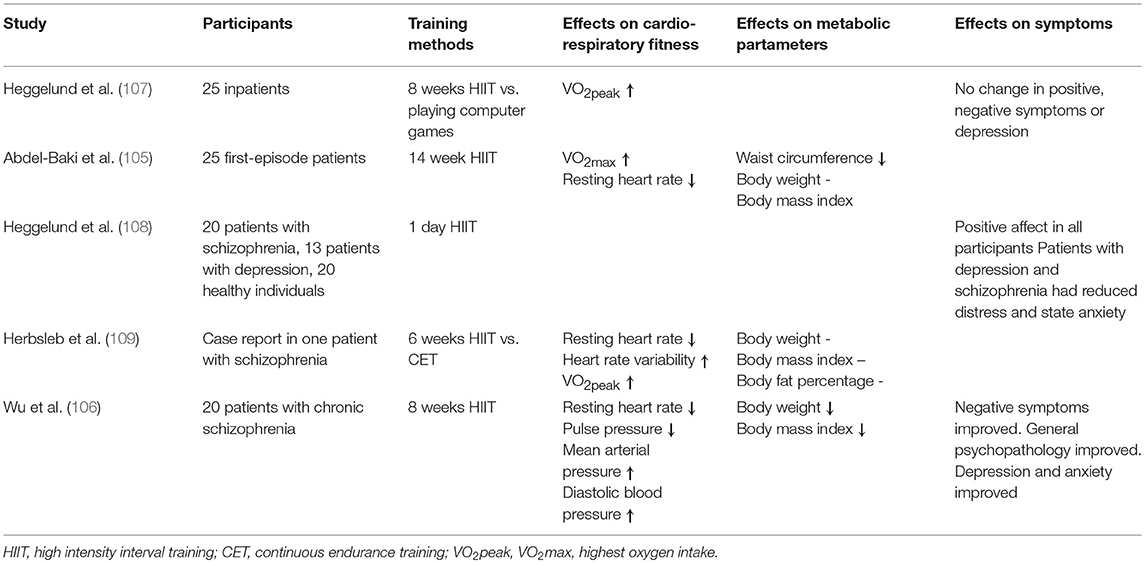
Table 4. Effects of high-intensity interval training on metabolic risk factors and symptoms of the disease in patients with schizophrenia.
In the general population, improving cardiorespiratory fitness is a key factor in preventing CVD and mortality (110, 111). Cardiorespiratory fitness can be measured by the highest oxygen intake (referred to as VO2max or VO2peak) and peak work rate/power output (Wpeak). Aerobic exercise interventions seeking to improve cardiorespiratory fitness can prevent CVD and the associated mortality (112). In a randomized study in obese and overweight patients with severe mental illness, including schizophrenia, schizoaffective disorder, bipolar disorder, and major depression, participation in group exercise classes was associated with improved short- and long-term cardiorespiratory fitness, as indicated by a lower heart rate response (92). Significant increases in VO2max, as a measure of aerobic capacity, and power output (Wpeak) have been reported in schizophrenia patients after continuous exercise training compared with control conditions, such as occupational therapy or table soccer (73, 79, 82, 88, 89, 91, 113) (Table 3). In a meta-analysis, cardiorespiratory fitness was improved in schizophrenia patients after aerobic exercise (g = 0.43, 95% CI 0.05–0.82). Furthermore, in schizophrenia patients improved cardiorespiratory fitness was correlated with an increased volume of the hippocampus (88, 114), with decreased ventricular and increased cerebral gray matter volume, and with thickening in the frontal, temporal, and cingulate cortex of the left hemisphere (113).
In a meta-analysis of HIIT vs. moderate-intensity continuous training, HIIT was more likely to increase VO2peak in adults with coronary heart disease, hypertension, metabolic syndrome, and obesity (115). In obese adults with hypertension, HIIT and continuous training both improved cardiorespiratory fitness, whereby an exercise intervention lasting at least 12 or 16 weeks was needed to achieve these effects (116). In schizophrenia patients, HIIT improved VO2peak by 12% compared with playing computer games (107), and in a case report of a patient with schizophrenia HIIT was more effective than moderate continuous training in increasing heart rate variability and reduing resting heart rate (109). A decrease in resting heart rate and 38% increase in VO2max was detected after a 14-week HIT program in schizophrenia patients (105). In summary, aerobic exercise is capable of improving cardiorespiratory fitness and thereby reducing risk factors for CVD and associated mortality (Table 4).
Reduction of symptoms may help to decrease suicidality in patients with schizophrenia (see above), and there is evidence that aerobic exercise interventions can improve schizophrenia symptoms and cognitive deficits. Published data from our group show that a structured endurance training programme is feasible in multi-episode schizophrenia patients (70). Previously, we demonstrated that 3 x 30 min aerobic exercise per week alleviated negative symptoms, significantly improved short-term memory and increased hippocampal volumes in patients with schizophrenia (88). Furthermore, when we added cognitive training to aerobic exercise from week 6 up to 3 months negative symptoms and working memory improved (90). Importantly, in 45% of the multi-episode schizophrenia patients who performed aerobic exercise the Global Assessment of Functioning (GAF) score improved by about 20% from baseline to month 3 (90); thus, this study showed that aerobic exercise as add-on therapy fosters patients' capacity to improve in multi-epsode schizophrenia. In this study, we did not replicate the increase of hippocampal volume after aerobic exercise, although we did detect increased volume of the left temporal cortex (117). In a randomized clinical trial, a 6-month structured aerobic exercise intervention reduced total symptoms of schizophrenia, positive symptoms, disorganization, excitement, emotional distress, symptoms of depression, and need of care significantly more than occupational therapy (79). In first-episode patients, an individualized exercise training program revealed improvement of negative and positive symptoms, psychosocial functioning and verbal short-term memory (93).
The beneficial effects of physical exercise on brain function and structure and cognitive performance have been repeatedly reported in healthy individuals [e.g., (118)]. Beyond this, a meta-analysis showed that in schizophrenia patients aerobic exercise improves negative, positive, and depressive symptoms and global functioning, as measured by the GAF (119). Another meta-analysis focusing on cognition demonstrated improved global cognition, working memory, social cognition, and attention after aerobic exercise in schizophrenia patients (120). Findings from the literature are contradictory, but a meta-analysis of exercise interventions in schizophrenia indicated that symptoms improve with a higher intensity of training (81). Symptom improvement was prominent in interventions of 90 min of moderate exercise per week (81). In healthy adults, elderly people, or individuals with obesity, HIIT improved executive function and verbal and short-term memory (95, 121). A meta-analysis in healthy normal-weight and obese individuals showed that HIIT training improved affective psychological responses (122). In a first study in a small group of patients with different diagnoses that included only some schizophrenia patients, 8 weeks of HIIT did not decrease psychopathological symptoms, but it did have positive effects on physical fitness and anxiety (107, 108). In 18 patients with schizophrenia, an 8-week HIIT program significantly improved negative symptoms, general psychopathology, depression, and anxiety (106) (Table 4).
In summary, add-on therapy of endurance training combined with psychosocial interventions or diet may improve symptoms of the metabolic syndrome in schizophrenia patients, thereby reducing the prevalence of CVD and mortality. It has been shown that aerobic exercise programs are feasible in populations with severe mental illness and are accepted by schizophrenia patients who have weight gain and reduced physical fitness. However, specific complicating characteristics of patients with schizophrenia in comparison to the healthy population include fatigue and sedation (e.g., due to antipsychotic treatment), symptoms of the disease, a high level of anxiety and depression, antipsychotic-induced weight gain, a lower level of education, little experience with sport, and a lack of motivation for physical activity in case of negative symptoms (70). To increase patients' motivation to adhere to training sessions, a sports scientist must provide supervision, which in turn increases the cost of otherwise cheap training methods, such as biking and walking. Nevertheless, aerobic exercise programs still have a good cost-benefit ratio when one considers the high socioeconomic costs of metabolic risk factors in these patients. To date, physical exercise has no known serious side effects or safety issues that might pose any risk to the patients. Aerobic exercise can significantly contribute to improving symptoms of the disease, including cognitive deficits and psychosocial functioning. In addition, it may have positive effects on the residual symptoms that are known to be treatment resistant even after long-term therapy with antipsychotics; however, treatment recommendations will be given when the optimal dose and duration of the intervention has been found in randomized clinical trials. The reversibility of structural alterations in the brain and improvement of symptoms suggest that aerobic exercise may induce a regenerative process in patients with schizophrenia (123). Finally, HIIT can be hypothesized to have greater potential than conventional, aerobic endurance training to improve cognitive deficits, overall symptoms, and metabolic parameters in schizophrenia patients. Future studies should investigate the effects of HIIT on neuroplastic changes in the brain. Furthermore, treatment recommendations should include aerobic exercise in multimodal therapy regimes. The German S3 guideline “Schizophrenia” (124) and the NICE guideline (125) recommend exercise programs for patients with schizophrenia and weight gain. However, positive effects of aerobic exercise may be limited to the training periods (90), and long-term improvement of metabolic risk factors may require continuation of aerobic training in certified sports clubs. Overall, further high quality clinical trials are needed before statements can be made about the optimal length and type of aerobic exercise programs for routine clinical care.
PF, BM, AS, and IM designed this manuscript. ST, DK, BR, AS, BM, IM, MR, AR, AH, ML, MvW, and PF managed the literature searches, interpreted the data and prepared the manuscript. All authors contributed to and approved the final manuscript and reviewed it critically for important intellectual content.
This research was funded by the following grants from the Deutsche Forschungsgemeinschaft (DFG): Klinische Forschergruppe (KFO) 241 and PsyCourse to PF (FA241/16-1). Further funding was received from the German Federal Ministry of Education and Research (BMBF) through the research network on psychiatric diseases ESPRIT (grant number 01EE1407E) to PF, AH, and AS.
AH received funding from Lundbeck, Janssen-Cilag, and Pfizer and a paid speakership from Desitin, Otsuka, and Lundbeck and was a member of a Roche advisory board. PF has been an honorary speaker for AstraZeneca, Bristol Myers Squibb, Lilly, Essex, GE Healthcare, GlaxoSmithKline, Janssen Cilag, Lundbeck, Otsuka, Pfizer, Servier, and Takeda and a member of the advisory boards of Janssen-Cilag, AstraZeneca, Lilly, and Lundbeck. AS was an honorary speaker for TAD Pharma and Roche and a member of Roche advisory boards.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank Jacquie Klesing, Board-certified Editor in the Life Sciences (ELS), for editing assistance with the manuscript.
2. Perala J, Suvisaari J, Saarni SI, Kuoppasalmi K, Isometsa E, Pirkola S, et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population. Arch Gen Psychiatry (2007) 64:19–28. doi: 10.1001/archpsyc.64.1.19
3. Murray CJ, Lopez AD. Evidence-based health policy–lessons from the Global Burden of Disease Study. Science (1996) 274:740–3.
4. Judd LL, Akiskal HS, Schettler PJ, Endicott J, Leon AC, Solomon DA, et al. Psychosocial disability in the course of bipolar I and II disorders: a prospective, comparative, longitudinal study. Arch Gen Psychiatry (2005) 62:1322–30. doi: 10.1001/archpsyc.62.12.1322
5. an der Heiden W, Häfner H. Course and Outcome. In: Weinberger D, Harrison PJ, editors Schizophrenia. 3rd. ed. Oxford: Blackwell Publishing (2011). p. 104–41.
6. Leal J, Luengo-Fernandez R, Gray A, Petersen S, Rayner M. Economic burden of cardiovascular diseases in the enlarged European Union. Eur Heart J. (2006) 27:1610–9. doi: 10.1093/eurheartj/ehi733
7. GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (2018). 392:1789–1858. doi: 10.1016/S0140-6736(18)32281-5
8. Gustavsson A, Svensson M, Jacobi F, Allgulander C, Alonso J, Beghi E, et al. Cost of disorders of the brain in Europe 2010. Eur Neuropsychopharmacol. (2011) 21:718–79. doi: 10.1016/j.euroneuro.2011.08.008
9. Heinrichs RW, Zakzanis KK. Neurocognitive deficit in schizophrenia: a quantitative review of the evidence. Neuropsychology (1998) 12:426–45.
10. van Erp TG, Hibar DP, Rasmussen JM, Glahn DC, Pearlson GD, Andreassen OA, et al. Subcortical brain volume abnormalities in 2028 individuals with schizophrenia and 2540 healthy controls via the ENIGMA consortium. Mol Psychiatry (2016) 21:547–53. doi: 10.1038/mp.2015.63
11. Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry (1996) 153:321–30.
12. Hoff AL, Svetina C, Shields G, Stewart J, DeLisi LE. Ten year longitudinal study of neuropsychological functioning subsequent to a first episode of schizophrenia. Schizophr Res. (2005) 78:27–34. doi: 10.1016/j.schres.2005.05.010
13. Green MF, Horan WP, Lee J. Social cognition in schizophrenia. Nat Rev Neurosci. (2015) 16:620–31. doi: 10.1038/nrn4005
14. Jirsaraie RJ, Sheffield JM, Barch DM. Neural correlates of global and specific cognitive deficits in schizophrenia. Schizophr Res. (2018). 201:237–42. doi: 10.1016/j.schres.2018.06.017
15. Weinberger DR. On the plausibility of “the neurodevelopmental hypothesis” of schizophrenia. Neuropsychopharmacology (1996) 14:1–11S. doi: 10.1016/0893-133X(95)00199-N
16. Haijma SV, Van Haren N, Cahn W, Koolschijn PC, Hulshoff Pol HE, Kahn RS. Brain volumes in schizophrenia: a meta-analysis in over 18 000 subjects. Schizophr Bull. (2013) 39:1129–38. doi: 10.1093/schbul/sbs118
17. Schmitt A, Steyskal C, Bernstein HG, Schneider-Axmann T, Parlapani E, Schaeffer EL, et al. Stereologic investigation of the posterior part of the hippocampus in schizophrenia. Acta Neuropathol. (2009) 117:395–407. doi: 10.1007/s00401-008-0430-y
18. Falkai P, Malchow B, Wetzestein K, Nowastowski V, Bernstein HG, Steiner J, et al. Decreased oligodendrocyte and neuron number in anterior hippocampal areas and the entire hippocampus in schizophrenia: a stereological postmortem study. Schizophr Bull. (2016) 42(Suppl. 1):S4–12. doi: 10.1093/schbul/sbv157
19. Ellison-Wright I, Bullmore E. Meta-analysis of diffusion tensor imaging studies in schizophrenia. Schizophr Res. (2009) 108:3–10. doi: 10.1016/j.schres.2008.11.021
20. Voineskos AN, Felsky D, Kovacevic N, Tiwari AK, Zai C, Chakravarty MM, et al. Oligodendrocyte genes, white matter tract integrity, and cognition in schizophrenia. Cereb Cortex (2013) 23:2044–57. doi: 10.1093/cercor/bhs188
21. Spangaro M, Mazza E, Poletti S, Cavallaro R, Benedetti F. Obesity influences white matter integrity in schizophrenia. Psychoneuroendocrinology (2018) 97:135–42. doi: 10.1016/j.psyneuen.2018.07.017
22. Schmitt A, Malchow B, Hasan A, Falkai P. The impact of environmental factors in severe psychiatric disorders. Front Neurosci. (2014) 8:19. doi: 10.3389/fnins.2014.00019
23. Arnsten AF. Stress signalling pathways that impair prefrontal cortex structure and function. Nat Rev Neurosci. (2009) 10:410–22. doi: 10.1038/nrn2648
24. Penzes P, Cahill ME, Jones KA, VanLeeuwen JE, Woolfrey KM. Dendritic spine pathology in neuropsychiatric disorders. Nat Neurosci. (2011) 14:285–93. doi: 10.1038/nn.2741
25. Hayes RD, Chang CK, Fernandes AC, Begum A, To D, Broadbent M, et al. Functional status and all-cause mortality in serious mental illness. PLoS ONE (2012) 7:e44613. doi: 10.1371/journal.pone.0044613
26. Vancampfort D, Probst M, Scheewe T, De Herdt A, Sweers K, Knapen J, et al. Relationships between physical fitness, physical activity, smoking and metabolic and mental health parameters in people with schizophrenia. Psychiatry Res. (2013) 207:25–32. doi: 10.1016/j.psychres.2012.09.026
27. Hallgren J, Osby U, Westman J, Gissler M. Mortality trends in external causes of death in people with mental health disorders in Sweden, 1987-2010. Scand J Public Health (2018). doi: 10.1177/1403494818758912. [Epub ahead of print].
28. Laursen TM, Munk-Olsen T, Gasse C. Chronic somatic comorbidity and excess mortality due to natural causes in persons with schizophrenia or bipolar affective disorder. PLoS ONE (2011) 6:e24597. doi: 10.1371/journal.pone.0024597
29. Lawrence D, Hancock KJ, Kisely S. The gap in life expectancy from preventable physical illness in psychiatric patients in Western Australia: retrospective analysis of population based registers. BMJ (2013) 346:f2539. doi: 10.1136/bmj.f2539
30. Ringen PA, Engh JA, Birkenaes AB, Dieset I, Andreassen OA. Increased mortality in schizophrenia due to cardiovascular disease - a non-systematic review of epidemiology, possible causes, and interventions. Front Psychiatry (2014) 5:137. doi: 10.3389/fpsyt.2014.00137
31. Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry (2015) 72:334–41. doi: 10.1001/jamapsychiatry.2014.2502
32. Foguet-Boreu Q, Fernandez San Martin MI, Flores Mateo G, Zabaleta Del Olmo E, Ayerbe Garcia-Morzon L, Perez-Pinar Lopez M, et al. Cardiovascular risk assessment in patients with a severe mental illness: a systematic review and meta-analysis. BMC Psychiatry (2016) 16:141. doi: 10.1186/s12888-016-0833-6
33. De Hert M, Detraux J, Vancampfort D. The intriguing relationship between coronary heart disease and mental disorders. Dialogues Clin Neurosci. (2018) 20:31–40.
34. Simon GE, Stewart C, Yarborough BJ, Lynch F, Coleman KJ, Beck A, et al. Mortality rates after the first diagnosis of psychotic disorder in adolescents and young adults. JAMA Psychiatry (2018) 75:254–60. doi: 10.1001/jamapsychiatry.2017.4437
35. Clapham E, Boden R, Brandt L, Jonsson EG, Bahmanyar S, Ekbom A, et al. Suicide ideation and behavior as risk factors for subsequent suicide in schizophrenia: a nested case-control study. Suicide Life Threat Behav. (2018). doi: 10.1111/sltb.12499. [Epub ahead of print].
36. Bornheimer LA. Suicidal Ideation in First-Episode Psychosis (FEP): examination of symptoms of depression and psychosis among individuals in an early phase of treatment. Suicide Life Threat Behav. (2018). doi: 10.1111/sltb.12440. [Epub ahead of print].
37. Zhang XY, Du X, Yin G, Zhang Y, Chen D, Xiu M, et al. Prevalence and clinical correlates of and cognitive function at the time of suicide attempts in first-episode and drug-naive patients with schizophrenia. J Clin Psychiatry (2018) 79:17m11797. doi: 10.4088/JCP.17m11797
38. Canal-Rivero M, Lopez-Morinigo JD, Setien-Suero E, Ruiz-Veguilla M, Ayuso-Mateos JL, Ayesa-Arriola R, et al. Predicting suicidal behaviour after first episode of non-affective psychosis: the role of neurocognitive functioning. Eur Psychiatry (2018) 53:52–7. doi: 10.1016/j.eurpsy.2018.06.001
39. Cassidy RM, Yang F, Kapczinski F, Passos IC. Risk factors for suicidality in patients with schizophrenia: a systematic review, meta-analysis, and meta-regression of 96 studies. Schizophr Bull. (2018) 44:787–97. doi: 10.1093/schbul/sbx131
40. Alberti KG, Zimmet P, Shaw J. Metabolic syndrome–a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med. (2006) 23:469–80. doi: 10.1111/j.1464-5491.2006.01858.x
41. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA (2001) 285:2486–97. doi: 10.1001/jama.285.19.2486
42. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation (2005) 112:2735–52. doi: 10.1161/CIRCULATIONAHA.105.169404
43. Hanley AJ, Karter AJ, Williams K, Festa A, D'Agostino RBJr, Wagenknecht LE, et al. Prediction of type 2 diabetes mellitus with alternative definitions of the metabolic syndrome: the Insulin Resistance Atherosclerosis Study. Circulation (2005) 112:3713–21. doi: 10.1161/CIRCULATIONAHA.105.559633
44. Gami AS, Witt BJ, Howard DE, Erwin PJ, Gami LA, Somers VK, et al. Metabolic syndrome and risk of incident cardiovascular events and death: a systematic review and meta-analysis of longitudinal studies. J Am Coll Cardiol. (2007) 49:403–14. doi: 10.1016/j.jacc.2006.09.032
45. Vancampfort D, Stubbs B, Mitchell AJ, De Hert M, Wampers M, Ward PB, et al. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: a systematic review and meta-analysis. World Psychiatry (2015) 14:339–47. doi: 10.1002/wps.20252
46. Correll CU, Frederickson AM, Kane JM, Manu P. Metabolic syndrome and the risk of coronary heart disease in 367 patients treated with second-generation antipsychotic drugs. J Clin Psychiatry (2006) 67:575–83.
47. Mitchell AJ, Vancampfort D, Sweers K, van Winkel R, Yu W, De Hert M. Prevalence of metabolic syndrome and metabolic abnormalities in schizophrenia and related disorders–a systematic review and meta-analysis. Schizophr Bull. (2013) 39:306–18. doi: 10.1093/schbul/sbr148
48. Sicras-Mainar A, Maurino J, Ruiz-Beato E, Navarro-Artieda R. Prevalence of metabolic syndrome according to the presence of negative symptoms in patients with schizophrenia. Neuropsychiatr Dis Treat. (2015) 11:51–7. doi: 10.2147/NDT.S75449
49. Bora E, Akdede BB, Alptekin K. The relationship between cognitive impairment in schizophrenia and metabolic syndrome: a systematic review and meta-analysis. Psychol Med. (2017) 47:1030–40. doi: 10.1017/S0033291716003366
50. Mitchell AJ, Vancampfort D, De Herdt A, Yu W, De Hert M. Is the prevalence of metabolic syndrome and metabolic abnormalities increased in early schizophrenia? A comparative meta-analysis of first episode, untreated and treated patients. Schizophr Bull. (2013) 39:295–305. doi: 10.1093/schbul/sbs082
51. Hasan A, Falkai P, Wobrock T, Lieberman J, Glenthoj B, Gattaz WF, et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for Biological Treatment of Schizophrenia, part 1: update 2012 on the acute treatment of schizophrenia and the management of treatment resistance. World J Biol Psychiatry (2012) 13:318–78. doi: 10.3109/15622975.2012.696143
52. Leucht S, Cipriani A, Spineli L, Mavridis D, Orey D, Richter F, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet (2013) 382:951–62. doi: 10.1016/S0140-6736(13)60733-3
53. Ray WA, Chung CP, Murray KT, Hall K, Stein CM. Atypical antipsychotic drugs and the risk of sudden cardiac death. N Engl J Med. (2009) 360:225–35. doi: 10.1056/NEJMoa0806994
54. Agelink MW, Majewski T, Wurthmann C, Lukas K, Ullrich H, Linka T, et al. Effects of newer atypical antipsychotics on autonomic neurocardiac function: a comparison between amisulpride, olanzapine, sertindole, and clozapine. J Clin Psychopharmacol. (2001) 21:8–13.
55. Bär KJ. Cardiac autonomic dysfunction in patients with schizophrenia and their healthy relatives - A small review. Front Neurol. (2015) 6:139. doi: 10.3389/fneur.2015.00139
56. Leucht S, Komossa K, Rummel-Kluge C, Corves C, Hunger H, Schmid F, et al. A meta-analysis of head-to-head comparisons of second-generation antipsychotics in the treatment of schizophrenia. Am J Psychiatry (2009) 166:152–63. doi: 10.1176/appi.ajp.2008.08030368
57. Ma X, Maimaitirexiati T, Zhang R, Gui X, Zhang W, Xu G, et al. HTR2C polymorphisms, olanzapine-induced weight gain and antipsychotic-induced metabolic syndrome in schizophrenia patients: a meta-analysis. Int J Psychiatry Clin Pract. (2014) 18:229–42. doi: 10.3109/13651501.2014.957705
58. Heald A, Pendlebury J, Anderson S, Narayan V, Guy M, Gibson M, et al. Lifestyle factors and the metabolic syndrome in Schizophrenia: a cross-sectional study. Ann Gen Psychiatry (2017) 16:12. doi: 10.1186/s12991-017-0134-6
59. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet (2012) 380:219–29. doi: 10.1016/S0140-6736(12)61031-9
60. Vancampfort D, Probst M, Knapen J, Carraro A, De Hert M. Associations between sedentary behaviour and metabolic parameters in patients with schizophrenia. Psychiatry Res. (2012) 200:73–8. doi: 10.1016/j.psychres.2012.03.046
61. Nyboe L, Vestergaard CH, Moeller MK, Lund H, Videbech P. Metabolic syndrome and aerobic fitness in patients with first-episode schizophrenia, including a 1-year follow-up. Schizophr Res. (2015) 168:381–7. doi: 10.1016/j.schres.2015.07.053
62. Vancampfort D, Guelinkcx H, Probst M, Stubbs B, Rosenbaum S, Ward PB, et al. Associations between metabolic and aerobic fitness parameters in patients with schizophrenia. J Nerv Ment Dis. (2015) 203:23–7. doi: 10.1097/NMD.0000000000000229
63. Stubbs B, Williams J, Gaughran F, Craig T. How sedentary are people with psychosis? A systematic review and meta-analysis. Schizophr Res. (2016) 171:103–9. doi: 10.1016/j.schres.2016.01.034
64. Stubbs B, Firth J, Berry A, Schuch FB, Rosenbaum S, Gaughran F, et al. How much physical activity do people with schizophrenia engage in? A systematic review, comparative meta-analysis and meta-regression. Schizophr Res. (2016) 176:431–40. doi: 10.1016/j.schres.2016.05.017
65. Ohi K, Kataoka Y, Shimada T, Kuwata A, Okubo H, Kimura K, et al. Meta-analysis of physical activity and effects of social function and quality of life on the physical activity in patients with schizophrenia. Eur Arch Psychiatry Clin Neurosci. (2018). doi: 10.1007/s00406-018-0903-5. [Epub ahead of print].
66. Wang J, Fan X, Liu D, Yi Z, Freudenreich O, Goff D, et al. Both physical activity and food intake are associated with metabolic risks in patients with schizophrenia. Schizophr. Res. (2012) 140:260–1. doi: 10.1016/j.schres.2012.05.008
67. Gurusamy J, Gandhi S, Damodharan D, Ganesan V, Palaniappan M. Exercise, diet and educational interventions for metabolic syndrome in persons with schizophrenia: a systematic review. Asian J Psychiatr. (2018) 36:73–85. doi: 10.1016/j.ajp.2018.06.018
68. Soundy A, Freeman P, Stubbs B, Probst M, Vancampfort D. The value of social support to encourage people with schizophrenia to engage in physical activity: an international insight from specialist mental health physiotherapists. J Ment Health (2014) 23:256–60. doi: 10.3109/09638237.2014.951481
69. Vancampfort D, De Hert M, Stubbs B, Ward PB, Rosenbaum S, Soundy A, et al. Negative symptoms are associated with lower autonomous motivation towards physical activity in people with schizophrenia. Compr Psychiatry (2015a) 56:128–32. doi: 10.1016/j.comppsych.2014.10.007
70. Keller-Varady K, Hasan A, Schneider-Axmann T, Hillmer-Vogel U, Adomssent B, Wobrock T, et al. Endurance training in patients with schizophrenia and healthy controls: differences and similarities. Eur Arch Psychiatry Clin Neurosci. (2016) 266:461–73. doi: 10.1007/s00406-015-0651-8
71. Callaghan P. Exercise: a neglected intervention in mental health care? J Psychiatr Ment Health Nurs. (2004) 11:476–83. doi: 10.1111/j.1365-2850.2004.00751.x
72. Ellis N, Crone D, Davey R, Grogan S. Exercise interventions as an adjunct therapy for psychosis: a critical review. Br J Clin Psychol. (2007) 46:95–111.
73. Dodd KJ, Duffy S, Stewart JA, Impey J, Taylor N. A small group aerobic exercise programme that reduces body weight is feasible in adults with severe chronic schizophrenia: a pilot study. Disabil Rehabil. (2011) 33:1222–9. doi: 10.3109/09638288.2010.526162
74. Vancampfort D, Probst M, Scheewe T, Knapen J, De Herdt A, De Hert M. The functional exercise capacity is correlated with global functioning in patients with schizophrenia. Acta Psychiatr Scand. (2012) 125:382–7. doi: 10.1111/j.1600-0447.2011.01825.x
75. Malchow B, Reich-Erkelenz D, Oertel-Knochel V, Keller K, Hasan A, Schmitt A, et al. The effects of physical exercise in schizophrenia and affective disorders. Eur Arch Psychiatry Clin Neurosci. (2013) 263:451–67. doi: 10.1007/s00406-013-0423-2
76. Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. (2011) 43:1334–59. doi: 10.1249/MSS.0b013e318213fefb
77. Chekroud SR, Gueorguieva R, Zheutlin AB, Paulus M, Krumholz HM, Krystal JH, et al. Association between physical exercise and mental health in 1.2 million individuals in the USA between 2011 and 2015: a cross-sectional study. Lancet Psychiatry (2018) 5:739–46. doi: 10.1016/S2215-0366(18)30227-X
78. Ball MP, Coons VB, Buchanan RW. A program for treating olanzapine-related weight gain. Psychiatr Serv. (2001) 52:967–9. doi: 10.1176/appi.ps.52.7.967
79. Scheewe TW, Backx FJ, Takken T, Jorg F, van Strater AC, Kroes AG, et al. Exercise therapy improves mental and physical health in schizophrenia: a randomised controlled trial. Acta Psychiatr Scand. (2013) 127:464–73. doi: 10.1111/acps.12029
80. Pearsall R, Smith DJ, Pelosi A, Geddes J. Exercise therapy in adults with serious mental illness: a systematic review and meta-analysis. BMC Psychiatry (2014) 14:117. doi: 10.1186/1471-244X-14-117
81. Firth J, Cotter J, Elliott R, French P, Yung AR. A systematic review and meta-analysis of exercise interventions in schizophrenia patients. Psychol Med. 45:1343–61. doi: 10.1017/S0033291714003110
82. Bredin SS, Warburton DE, Lang DJ. The health benefits and challenges of exercise training in persons living with schizophrenia: a pilot study. Brain Sci. (2013) 3:821–48. doi: 10.3390/brainsci3020821
83. Daumit GL, Dickerson FB, Wang NY, Dalcin A, Jerome GJ, Anderson CA, et al. A behavioral weight-loss intervention in persons with serious mental illness. N Engl J Med. (2013) 368:1594–602. doi: 10.1056/NEJMoa1214530
84. Krogh J, Speyer H, Norgaard HC, Moltke A, Nordentoft M. Can exercise increase fitness and reduce weight in patients with schizophrenia and depression? Front Psychiatry (2014) 5:89. doi: 10.3389/fpsyt.2014.00089
85. Methapatara W, Srisurapanont M. Pedometer walking plus motivational interviewing program for Thai schizophrenic patients with obesity or overweight: a 12-week, randomized, controlled trial. Psychiatry Clin Neurosci. (2011) 65:374–80. doi: 10.1111/j.1440-1819.2011.02225.x
86. Kuo FC, Lee CH, Hsieh CH, Kuo P, Chen YC, Hung YJ. Lifestyle modification and behavior therapy effectively reduce body weight and increase serum level of brain-derived neurotrophic factor in obese non-diabetic patients with schizophrenia. Psychiatry Res. (2013) 209:150–4. doi: 10.1016/j.psychres.2012.11.020
87. Amiaz R, Rubinstein K, Czerniak E, Karni Y, Weiser M. A diet and fitness program similarly affects weight reduction in schizophrenia patients treated with typical or atypical medications. Pharmacopsychiatry (2016) 49:112–6. doi: 10.1055/s-0035-1569416
88. Pajonk FG, Wobrock T, Gruber O, Scherk H, Berner D, Kaizl I, et al. Hippocampal plasticity in response to exercise in schizophrenia. Arch Gen Psychiatry (2010) 67:133–43. doi: 10.1001/archgenpsychiatry.2009.193
89. Scheewe TW, Takken T, Kahn RS, Cahn W, Backx FJ. Effects of exercise therapy on cardiorespiratory fitness in patients with schizophrenia. Med Sci Sports Exerc. (2012) 44:1834–42. doi: 10.1249/MSS.0b013e318258e120
90. Malchow B, Keller K, Hasan A, Dorfler S, Schneider-Axmann T, Hillmer-Vogel U, et al. Effects of endurance training combined with cognitive remediation on everyday functioning, symptoms, and cognition in multiepisode schizophrenia patients. Schizophr Bull. (2015) 41:847–58. doi: 10.1093/schbul/sbv020
91. Armstrong HF, Bartels MN, Paslavski O, Cain D, Shoval HA, Ballon JS, et al. The impact of aerobic exercise training on cardiopulmonary functioning in individuals with schizophrenia. Schizophr Res. (2016) 173:116–7. doi: 10.1016/j.schres.2016.03.009
92. Jerome GJ, Young DR, Dalcin AT, Wang NY, Gennusa J III, Goldsholl S, Appel LJ, et al. Cardiorespiratory benefits of group exercise among adults with serious mental illness. Psychiatry Res. (2017) 256:85–7. doi: 10.1016/j.psychres.2017.06.019
93. Firth J, Carney R, Elliott R, French P, Parker S, McIntyre R, et al. Exercise as an intervention for first-episode psychosis: a feasibility study. Early Interv Psychiatry (2018) 12:307–15. doi: 10.1111/eip.12329
94. Kessler HS, Sisson SB, Short KR. The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Med. (2012) 42:489–509. doi: 10.2165/11630910-000000000-00000
95. Drigny J, Gremeaux V, Dupuy O, Gayda M, Bherer L, Juneau M, et al. Effect of interval training on cognitive functioning and cerebral oxygenation in obese patients: a pilot study. J Rehabil Med. (2014) 46:1050–4. doi: 10.2340/16501977-1905
96. Batacan RBJr, Duncan MJ, Dalbo VJ, Tucker PS, Fenning AS. Effects of high-intensity interval training on cardiometabolic health: a systematic review and meta-analysis of intervention studies. Br J Sports Med. (2017) 51:494–503. doi: 10.1136/bjsports-2015-095841
97. Wewege M, van den Berg R, Ward RE, Keech A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: a systematic review and meta-analysis. Obes Rev. (2017) 18:635–46. doi: 10.1111/obr.12532
98. Thivel D, Masurier J, Baquet G, Timmons BW, Pereira B, Berthoin S, et al. High-intensity interval training in overweight and obese children and adolescents: systematic review and meta-analysis. J Sports Med Phys Fitness (2018). doi: 10.23736/S0022-4707.18.08075-1. [Epub ahead of print].
99. Vissers D, Hens W, Taeymans J, Baeyens JP, Poortmans J, Van Gaal L. The effect of exercise on visceral adipose tissue in overweight adults: a systematic review and meta-analysis. PLoS ONE (2013) 8:e56415. doi: 10.1371/journal.pone.0056415
100. Jelleyman C, Yates T, O'Donovan G, Gray LJ, King JA, Khunti K, et al. The effects of high-intensity interval training on glucose regulation and insulin resistance: a meta-analysis. Obes Rev. (2015) 16:942–61. doi: 10.1111/obr.12317
101. Keating SE, Johnson NA, Mielke GI, Coombes JS. A systematic review and meta-analysis of interval training versus moderate-intensity continuous training on body adiposity. Obes Rev. (2017) 18:943–64. doi: 10.1111/obr.12536
102. Roy M, Williams SM, Brown RC, Meredith-Jones KA, Osborne H, Jospe M, et al. High-intensity interval training in the real world: outcomes from a 12-month intervention in overweight adults. Med Sci Sports Exerc. (2018) 50:1818–26. doi: 10.1249/MSS.0000000000001642
103. Maillard F, Pereira B, Boisseau N. Effect of high-intensity interval training on total, abdominal and visceral fat mass: a meta-analysis. Sports Med. (2018) 48:269–88. doi: 10.1007/s40279-017-0807-y
104. De Strijcker D, Lapauw B, Ouwens DM, Van de Velde D, Hansen D, Petrovic M, et al. High intensity interval training is associated with greater impact on physical fitness, insulin sensitivity and muscle mitochondrial content in males with overweight/obesity, as opposed to continuous endurance training: a randomized controlled trial. J Musculoskelet Neuronal Interact. (2018) 18:215–26.
105. Abdel-Baki A, Brazzini-Poisson V, Marois F, Letendre E, Karelis AD. Effects of aerobic interval training on metabolic complications and cardiorespiratory fitness in young adults with psychotic disorders: a pilot study. Schizophr Res. (2013) 149:112–5. doi: 10.1016/j.schres.2013.06.040
106. Wu MH, Lee CP, Hsu SC, Chang CM, Chen CY. Effectiveness of high-intensity interval training on the mental and physical health of people with chronic schizophrenia. Neuropsychiatr Dis Treat. (2015) 11:1255–63. doi: 10.2147/NDT.S81482
107. Heggelund J, Nilsberg GE, Hoff J, Morken G, Helgerud J. Effects of high aerobic intensity training in patients with schizophrenia: a controlled trial. Nord J Psychiatry (2011) 65:269–75. doi: 10.3109/08039488.2011.560278
108. Heggelund J, Kleppe KD, Morken G, Vedul-Kjelsas E. High aerobic intensity training and psychological States in patients with depression or schizophrenia. Front Psychiatry (2014) 5:148. doi: 10.3389/fpsyt.2014.00148
109. Herbsleb M, Muhlhaus T, Bär KJ. Differential cardiac effects of aerobic interval training versus moderate continuous training in a patient with schizophrenia: a case report. Front Psychiatry (2014) 5:119. doi: 10.3389/fpsyt.2014.00119
110. Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA (2009) 301:2024–35. doi: 10.1001/jama.2009.681
111. Myers J, McAuley P, Lavie CJ, Despres JP, Arena R, Kokkinos P. Physical activity and cardiorespiratory fitness as major markers of cardiovascular risk: their independent and interwoven importance to health status. Prog Cardiovasc Dis. (2015) 57:306–14. doi: 10.1016/j.pcad.2014.09.011
112. Barry VW, Baruth M, Beets MW, Durstine JL, Liu J, Blair SN. Fitness vs. fatness on all-cause mortality: a meta-analysis. Prog Cardiovasc Dis. (2014) 56:382–90. doi: 10.1016/j.pcad.2013.09.002
113. Scheewe TW, van Haren NE, Sarkisyan G, Schnack HG, Brouwer RM, de Glint M, et al. Exercise therapy, cardiorespiratory fitness and their effect on brain volumes: a randomised controlled trial in patients with schizophrenia and healthy controls. Eur Neuropsychopharmacol. (2013) 23:675–85. doi: 10.1016/j.euroneuro.2012.08.008
114. Papiol S, Popovic D, Keeser D, Hasan A, Schneider-Axmann T, Degenhardt F, et al. Polygenic risk has an impact on the structural plasticity of hippocampal subfields during aerobic exercise combined with cognitive remediation in multi-episode schizophrenia. Transl Psychiatry (2017) 7:e1159. doi: 10.1038/tp.2017.131
115. Weston KS, Wisloff U, Coombes JS. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: a systematic review and meta-analysis. Br J Sports Med. (2014) 48:1227–34. doi: 10.1136/bjsports-2013-092576
116. Jurio-Iriarte B, Maldonado-Martin S. Effects of different exercise training programs on cardiorespiratory fitness in overweight/obese adults with hypertension: a pilot study. Health Promot Pract. (2018). doi: 10.1177/1524839918774310. [Epub ahead of print].
117. Malchow B, Keeser D, Keller K, Hasan A, Rauchmann BS, Kimura H, et al. Effects of endurance training on brain structures in chronic schizophrenia patients and healthy controls. Schizophr Res. (2016) 173:182–91. doi: 10.1016/j.schres.2015.01.005
118. Erickson KI, Voss MW, Prakash RS, Basak C, Szabo A, Chaddock L, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci USA. (2011) 108:3017–22. doi: 10.1073/pnas.1015950108
119. Dauwan M, Begemann MJ, Heringa SM, Sommer IE. Exercise improves clinical symptoms, quality of life, global functioning, and depression in schizophrenia: a systematic review and meta-analysis. Schizophr Bull. (2016) 42:588–99. doi: 10.1093/schbul/sbv164
120. Firth J, Stubbs B, Rosenbaum S, Vancampfort D, Malchow B, Schuch F, et al. Aerobic exercise improves cognitive functioning in people with schizophrenia: a systematic review and meta-analysis. Schizophr Bull. (2017) 43:546–56. doi: 10.1093/schbul/sbw115
121. Berryman N, Bherer L, Nadeau S, Lauziere S, Lehr L, Bobeuf F, et al. Multiple roads lead to Rome: combined high-intensity aerobic and strength training vs. gross motor activities leads to equivalent improvement in executive functions in a cohort of healthy older adults. Age (2014) 36:9710. doi: 10.1007/s11357-014-9710-8
122. Oliveira BRR, Santos TM, Kilpatrick M, Pires FO, Deslandes AC. Affective and enjoyment responses in high intensity interval training and continuous training: a systematic review and meta-analysis. PLoS ONE (2018) 13:e0197124. doi: 10.1371/journal.pone.0197124
123. Falkai P, Rossner MJ, Schulze TG, Hasan A, Brzozka MM, Malchow B, et al. Kraepelin revisited: schizophrenia from degeneration to failed regeneration. Mol Psychiatry (2015) 20:671–6. doi: 10.1038/mp.2015.35
124. Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde S3 Leitlinie Schizophrenie, Konsultationsfassung (2018). Available online at: https://www.awmf.org/fileadmin/user_upload/Leitlinien/038_D_G_f_Psychiatrie__Psychotherapie_und_Nervenheilkunde/038-009l_S3_Konsultationsfassung_Schizophrenie_2018-09.pdf
125. NICE. Psychosis and Schizophrenia in Adults: Prevention and Management Clinical Guideline [CG178] (2014). Available online at: https://www.nice.org.uk/guidance/cg178.
Keywords: aerobic exercise, endurance training, high-intensity interval training, metabolic syndrome, mortality, schizophrenia, cognition, positive and negative symptoms
Citation: Schmitt A, Maurus I, Rossner MJ, Röh A, Lembeck M, von Wilmsdorff M, Takahashi S, Rauchmann B, Keeser D, Hasan A, Malchow B and Falkai P (2018) Effects of Aerobic Exercise on Metabolic Syndrome, Cardiorespiratory Fitness, and Symptoms in Schizophrenia Include Decreased Mortality. Front. Psychiatry 9:690. doi: 10.3389/fpsyt.2018.00690
Received: 31 August 2018; Accepted: 27 November 2018;
Published: 21 December 2018.
Edited by:
Andrea Fiorillo, Università degli Studi della Campania Luigi Vanvitelli Naples, ItalyReviewed by:
Gaia Sampogna, Università degli Studi della Campania Luigi Vanvitelli Naples, ItalyCopyright © 2018 Schmitt, Maurus, Rossner, Röh, Lembeck, von Wilmsdorff, Takahashi, Rauchmann, Keeser, Hasan, Malchow and Falkai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Schmitt, YW5kcmVhLnNjaG1pdHRAbWVkLnVuaS1tdWVuY2hlbi5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.