 Birgit Kleim
Birgit Kleim Andrea B. Horn
Andrea B. Horn Rainer Kraehenmann
Rainer Kraehenmann Matthias R. Mehl
Matthias R. Mehl Anke Ehlers
Anke Ehlers- 1Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, United Kingdom
- 2Department of Psychology, University of Zurich, Zurich, Switzerland
- 3Department of Psychiatry, Psychotherapy and Psychosomatics, University of Zurich, Zurich, Switzerland
- 4University Research Priority Program “Dynamics of Healthy Aging,” University of Zurich, Zurich, Switzerland
- 5Department of Psychology, University of Arizona, Tucson, AZ, United States
- 6Department of Experimental Psychology, Oxford University, Oxford, United Kingdom
Identifying early predictors for psychiatric disorders, such as post-traumatic stress disorder (PTSD), is crucial for effective treatment and prevention efforts. Obtaining such predictors is challenging and methodologically limited, for example by individuals' distress, arousal, and reduced introspective ability. We investigated the predictive power of language-based, implicit markers of psychological processes (N = 163) derived from computerized text-analysis of trauma and control narratives provided within 18 days post-trauma. Trauma narratives with fewer cognitive processing words (indicating less cognitive elaboration), more death-related words (indicating perceived threat to life), and more first-person singular pronouns (indicating self-immersed processing) predicted greater PTSD symptoms at 6 months. These effects were specific to trauma narratives and held after controlling for early PTSD symptom severity and verbal intelligence. When self-report questionnaires of related processes were considered together with the trauma narrative linguistic predictors, use of more first-person singular pronouns remained a significant predictor alongside self-reported mental defeat. Language-based processing markers may complement questionnaire measures in early forecasting of post-trauma adjustment.
Early Linguistic Markers of Trauma-Specific Processing Predict Post-trauma Adjustment
There is large heterogeneity in psychological responding following exposure to traumatic events [e.g., (1)]. Trauma impact and recovery are not randomly distributed. Many survivors show a high degree of resilience and ultimately (and sometimes quickly) return to normal lives whilst others develop psychological disorders, such as post-traumatic stress disorder (PTSD). These survivors could benefit from professional help to mitigate the long-term social, emotional, and health impact of experiencing trauma (2). Fortunately, treatment options exist. Over the last decades, trauma researchers have made big strides in developing successful interventions and delivery of such interventions early after trauma has been shown to be effective (3).
A particularly important scientific question therefore is to identify early predictors of adjustment trajectories. To the extent that clinicians can reliably identify who is likely going to do well and who is at a high risk for developing chronic PTSD, limited therapeutic resources can be allocated to where they are most needed. In the context of trauma, identification of predictors at an early stage is an important objective. Survivors often have contact with professional services in the initial aftermath of a trauma, whereas such contact appears much more difficult to establish later, when disorders are chronic, often comorbid and more difficult to treat (4, 5).
Ideally, predictors of later chronic PTSD would be (a) early markers that can facilitate optimization of treatment initiation and resource allocation (b), naturally observable for clinicians—so that assessment burden can be kept to a necessary minimum at a distressing and vulnerable time for trauma survivors, and (c) trauma-specific—so that prediction errors are minimized. Finally, as the validity of self-report questionnaires may be undermined by factors such as high distress, emotional arousal, and limited introspective ability—factors that characterize information processing in the aftermath of a trauma- such markers would ideally be independent of the survivor's explicit self-report and could thus significantly complement such measures.
Natural language markers derived from individuals' spontaneous word use have recently received increased scientific attention (6). Use of certain words in individuals' writing or speech has been related to psychological aspects of their personal health and psychopathology [e.g. (7–10)]. Following trauma, maladaptive processing of traumatic memories may contribute to the development of PTSD. Linguistic features indexed in trauma survivors' personal accounts of their experience may offer more direct, “unfiltered” access to the way this experience is processed than self-report or interview measures. Unobtrusive indices of patterns of word use in such accounts may thus be good candidates to complement existing internal process measures for forecasting post-trauma adjustment [cf. (11, 12)]. Finally, linguistic measures reflect spontaneous behavior and thus do not share method variance with self-reported symptom outcomes, hence providing more unique and robust estimates of potential associations with PTSD symptoms.
Which trauma memory processing styles have been associated with later PTSD? According to cognitive models [e.g. (13, 14), survivors who engage primarily in surface-level processing of sensory and perceptual characteristics without elaboration of context and meaning of the event are more prone to develop PTSD than those who engage in more in-depth elaborate cognitive processing during trauma. Use of cognitive words in trauma narratives might reflect this elaboration process (15, 16). Peritraumatic mental defeat, a peritraumatic process, consisting of complete loss of inner resistance has also been implicated in the development in PTSD (14, 17, 18) as well as perceived threat to life (19). Earlier studies have indexed the use of death-related words in trauma narratives as linguistic indicator and proxy of these processes, which was related to PTSD as expected (20, 21). A meta-analysis of PTSD predictors highlighted survivors' emotional response to the trauma, such as fear, helplessness, horror, guilt, and shame, during trauma as one of the strongest PTSD predictors (19), a process captured by the use of negative emotion words in trauma narratives (22, 23). Finally, the use of first-person singular pronouns (“I,” “me.” “my”), a proposed measure of self-immersed processing (24, 25) has emerged as a predictor of depression (9, 26, 27) and general psychopathology (28) in prior research. Whilst working through the trauma memory is beneficial for constructing an elaborated and organized perspective of the event, a narrow and self-immersed perspective and focus on recounting details and personal reactions might undermine adaptive self-reflection (29) as well as the resolution of initial post-traumatic stress reactions.
Whereas, some studies have investigated language use following exposure to national traumatic events in the general population (30, 31) or in smaller samples of indirectly exposed individuals (32), no study has yet investigated whether such linguistic markers indexed in the early aftermath of trauma predict later chronic PTSD in a large sample of trauma survivors and how specific such linguistic predictors are in forecasting trauma adaptation and PTSD, over and above self-report questionnaires, as well as in complement to such self-report measures.
The present study investigated four candidate linguistic predictors, assessed early after assault, a trauma with increased PTSD risk relative to other potentially traumatic events (4). We indexed linguistic measures in trauma narratives provided on average 18 days post-trauma by a large sample of directly exposed trauma survivors. Knowledge about such early predictors is sparse, although it may help identify those survivors that could effectively be treated to prevent later chronic PTSD. In order to establish process-specificity of linguistic characteristics, we indexed linguistic markers in trauma narratives, as well as in non-traumatic control narratives. Specifically, we hypothesized that linguistic measures of (1) less elaboration and cognitive processing, (2) more mental defeat and threat to life, (3) more negative emotionality, and (4) more self-immersed processing in early accounts of the assault would be associated with more PTSD symptoms at 6 months follow-up. We then determined the extent to which significant trauma-specific linguistic predictors complement corresponding self-report questionnaires in predicting PTSD.
Method
Participants and Procedures
The local ethics board approved the study. Participants were assault survivors who attended the Emergency Department of a large urban teaching hospital. Exclusion criteria, assessed by an initial screening interview, were current psychosis, alcohol dependence, ongoing domestic violence, and no memory of the assault. Two hundred and twenty-two individuals were recruited and consented to participate in a research session conducted by a research psychologist, which took place around 18 days post-assault, SD = 9.7 days. During this session, 163 (67% male, mean age = 34 years, SD = 11.4) provided a narrative of their trauma and a negative, non-traumatic control event from around the same time of the assault. The latter was used to examine trauma-specificity of linguistic process measures1,2. Participants were asked to remember both events as vividly and in as much details as possible and to provide a detailed verbal report of their trauma including sensory impressions and cognitions during trauma. Narrative length was highly variable between participants, with mean narrative length of 786 words (SD = 584) for the trauma and 211 words (SD = 203) for the negative event narrative. Nearly all assaults were physical assaults; only 2% were sexual assaults. See Table 1 for descriptive statistics and correlations among study variables.
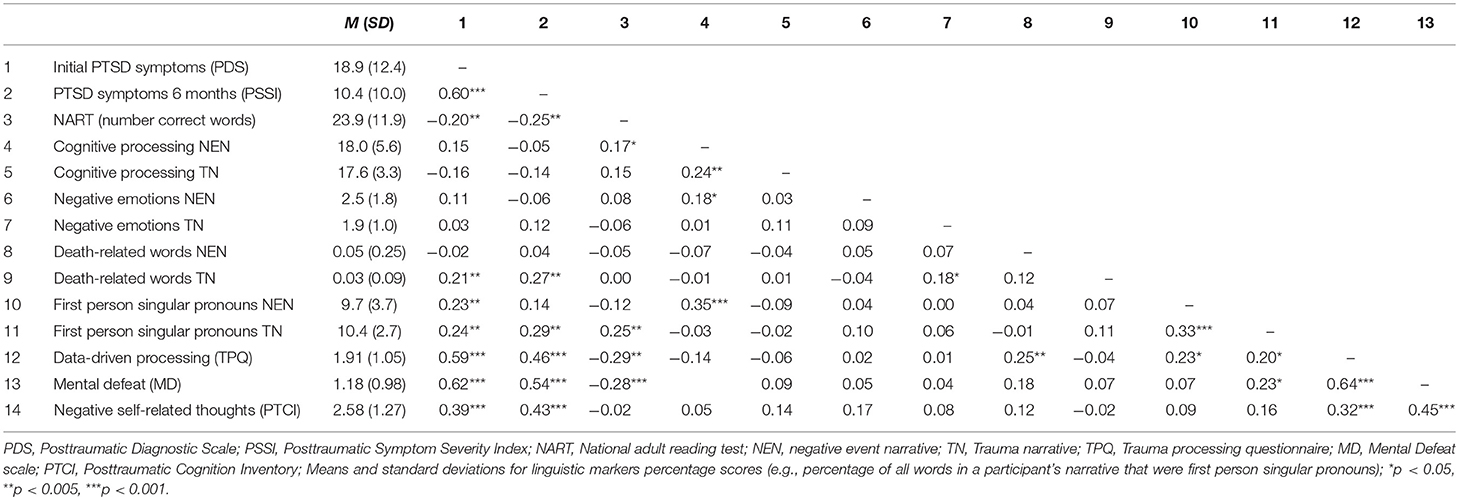
Table 1. Descriptive statistics and correlations among study variables.
Measures
PTSD Symptoms
PTSD symptom severity at 2 weeks was assessed using the self-report Post-traumatic Diagnostic Scale [PDS, (35); α =.92], symptom severity at 6 months was assessed with the PTSD Symptom Scale, a semi-structured interview with 17 items, each corresponding to one of the DSM-IV criteria for PTSD [PSSI, (36); interrater reliability, κ = 0.82]. We also indexed PTSD diagnosis using the PTSD Symptom Scale- Interview (PSS-I), a 17-item structured (36) and it was established that 18.9% of the sample fulfilled diagnostic criteria for PTSD at 6 months.
Verbal Intelligence
Participants also completed the National Adult Reading Test [NART, (37)], a widely accepted measure of verbal intelligence. The NART requires participants to read out loud a list of 50 irregularly spelled words in order of increasing difficulty. The number of words read correctly comprises the final score. The NART has excellent reliability and construct validity (38). It correlates highly with other measures of intelligence and allows the prediction of full-scale IQ scores (37).
Trauma-Specific and Non-specific Linguistic Markers
Verbatim transcripts of the narratives were analyzed using Linguistic Inquiry and Word Count [LIWC, (39)], an extensively validated computerized text-analysis tool. LIWC analyses texts by calculating the percentage of words in a given text that fall into a set of pre-defined psychological and grammatical categories. Based on prior research and cognitive PTSD theory, we limited our analysis to the categories cognitive processes (e.g., “cause,” “know,” “ought”) as an index of elaboration and cognitive processing, death-related words (e.g., “dead,” “kill,” “grave”) as an index of mental defeat and death salience, negative emotions (e.g., “angry,” “sad,” “cry”), as an index of negative emotionality, and first person singular pronouns (e.g., “I,” “me,” “my”) as an index of self-immersed processing. To address the question of process specificity, we computed separate word-use variables for the trauma and negative event narratives. Sample excerpts illustrating these four language variables in both types of narratives are provided in the Appendix.
Self-reported Peri- and Post-traumatic Processing
Data driven processing was assessed as an index of lacking elaboration and cognitive processing with the 8-items data-driven processing subscale from the Cognitive Processing Scale (40). The scale assesses the extent to which individuals engage in surface-level, perceptual processing during the assault (“I could not think clearly,” “I was confused and could not fully make sense of what was happening”), each on a scale from 0 (not at all) to 4 (very strongly). Internal consistency in the present sample was good, Cronbach's α = 0.87.
The Mental Defeat Scale (41), an 11-items self-report questionnaire, was used to index mental defeat. Participants rated the extent to which statements such as “I no longer felt like a human being” or “In my mind, I gave up” applied to them at some time during the assault, each on a scale from 0 (not at all) to 4 (very strongly). Internal consistency in the present sample was high, Cronbach's α = 0.90.
The Negative thoughts about the self subscale of the Post-traumatic cognition inventory [PTCI, (42)] was used to index self-related thoughts in context of the assault, each on a scale from 1 (totally agree) to 7 (totally disagree). The PTCI indexes generalized negative appraisals of the trauma and its aftermath and has been shown to have good reliability and convergent validity (42). Internal consistency of the 21-items negative self subscale in the present sample was high, Cronbach's α = 0.93.
Data Analysis
We calculated a hierarchical linear regression analysis in order to determine whether trauma-specific linguistic markers predict PTSD symptom severity at 6 months, over and above initial PTSD symptoms, verbal intelligence and non-trauma linguistic variables. From the significant trauma-specific linguistic variables and corresponding self-report questionnaires, we determined the best set of variables to predict PTSD symptom severity using a stepwise linear regression and a forward selection method. All analyses were conducted using SPSS 20.0.
Results
Results from the linear regression analyses are shown in Table 2. Less use of cognitive processing words in negative event narratives predicted PTSD symptom severity at 6 months after controlling for initial PTSD symptom severity and verbal intelligence. No other negative event linguistic characteristics predicted PTSD. However, when trauma-specific linguistic characteristics were introduced in the regression model, general cognitive processing from the negative event narrative was no longer significant. Instead, the linguistic trauma narrative characteristics, with exception of negative emotion words, significantly predicted later PTSD symptom severity. Less cognitive processing, use of more death-related words and more first person singular pronouns in trauma narratives were predictive of more PTSD symptoms at follow-up. Together, the linguistic predictors from the trauma narrative accounted for 7% additional variance in later PTSD symptoms, over and above initial PTSD symptoms, verbal intelligence and general linguistic predictors from non-trauma narratives.
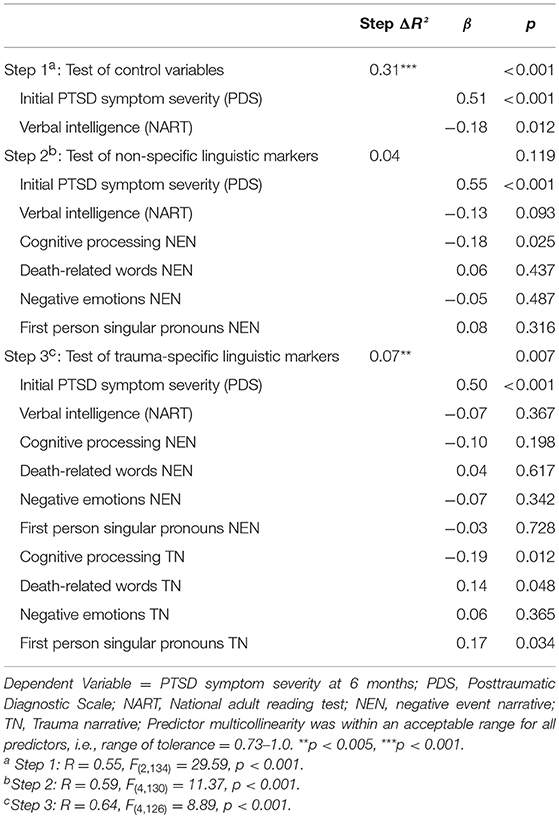
Table 2. Trauma-specific linguistic markers predict posttraumatic stress disorder symptom severity at 6 months beyond initial symptom severity, verbal intelligence and non-specific linguistic markers.
In a separate model, we determined the best predictors of later PTSD symptom severity from the three significant trauma narrative linguistic variables (cognitive processing, use of death-related words, first person singular pronouns) and the corresponding self-report questionnaire scores (data-driven processing, mental defeat, and negative self-related thoughts) using linear regression and a forward selection procedure. First person singular pronouns in trauma narratives significantly predicted PTSD at 6 months, β = 0.17, p < 0.031, alongside self-reported mental defeat, β = −0.52, p < 0.001. No other significant predictor emerged in this analysis. Together, the variables explained 34% of PTSD symptom severity, R = 0.58, F(1, 125) = 31.92, p < 0.001. There were no significant sex differences in magnitude in any of the linguistic predictors under study (all p > 122).
Discussion
Linguistic markers of trauma-specific processing indexed in the early aftermath of a trauma uniquely predicted later chronic PTSD symptoms. Less cognitive processing words (as marker of less elaboration), use of more death-related words (as marker of mental defeat), use of more first person singular pronouns (as marker of self-immersed processing) assessed in the first 2 weeks after trauma predicted more severe PTSD symptoms at 6 months follow-up. Importantly, these linguistic predictors uniquely emerged from trauma-narrative competing against language markers of general emotional processing derived from non-traumatic, negative event narratives and predicted PTSD over and above established risk factors such as verbal intelligence and initial levels of PTSD symptoms.
The use of less cognition words in those with increased PTSD symptoms is in accord with cognitive theories of PTSD and the proposed beneficial nature of elaborative cognitive processing during trauma (13, 14) and complements earlier findings of increased cognition words predicting fewer distress symptoms following emotional events (15, 25). Although references to death were low overall, their relative frequencies predicted later PTSD, hence indicating the sensitivity of this index and its potential for clinical use. The finding is in line with studies showing perceived threat to life as an important aspect of trauma [for a review see (19)]. More reference to death and dying in trauma narratives may also reflect mental defeat and the result of giving up all efforts to retain one's identity as a human being during trauma. Negative emotion use in trauma narratives was, however, not predictive of later PTSD, a finding that replicates earlier results by Jones et al. (43) and may indicate limited usefulness of this index early post-trauma yet leaves open the possibility that PTSD-specific differences emerge gradually at a later time. Focus on specific emotional categories, such as shame or anger could be more predictive than a broad negative emotion category. Finally, more first-person singular pronoun use in trauma narratives predicted later PTSD and may indicate unmitigated self-immersion which may hamper emotion regulation and has been associated with greater impairment of mental and social functioning (9, 26).
Use of more first-person singular pronouns remained a significant predictor alongside self-reported mental defeat, when corresponding questionnaire measures were included. Assessment of such candidate early linguistic predictors, along with self-report questionnaires is thus one way to capture psychological processes after exposure to trauma and to predict later psychological adjustment. Self-report questionnaires may often provide practically the most efficient way of indexing psychological processing, despite their potential limitations when administered early after of trauma. However, patients routinely report on aspects of their trauma and such narratives could readily be subjected to automatic linguistic analyses as part of routine clinical practice.
The current study is not without limitations. Our sample consisted of assault survivors (who suffer a relatively high risk for chronic PTSD) and generalizability to other trauma types needs to be established. The potentially lower reliability of the negative event narrative markers due to their lower word count might have to some extent constrained their regression weights. Yet, LIWC variables are based on proportions and 50 or less words have proven sufficient to yield reliable estimates in prior research (44). Although, some of the narratives were rather short, minimum requirements for establishing LIWC scores were met for those narratives at the lower end of the word count. The results should nevertheless be replicated in another sample and specificity established, as well as reliability of the linguistic markers. Moreover, the linguistic predictors were conceptualized as proxies of psychological processes (e.g., mental defeat), which usually only partially convergence with questionnaire scores [see also (45)], owing, in part, also to methodological differences between these two methods of measurement. A fruitful approach could thus be to use both measures in complement to forecast trauma adaptation and development of later PTSD.
Despite these limitations, our findings have important clinical implications. We identified early linguistic markers of later PTSD assessed in narratives provided by survivors at 18 days post-trauma and found that they predicted 7% of later variance in PTSD over and above initial symptom severity. Self-immersed processing assessed by a linguistic index and mental defeat indexed by self-report questionnaire emerged as the best set of early predictors of later PTSD in the present study. Linguistic markers can thus make a clinically significant contribution and help identify those individuals at risk of developing chronic PTSD. Early provision of trauma-focused psychotherapy for these individuals at risk can prevent chronic PTSD (3). Linguistic markers, assessed early after trauma, may complement self-report questionnaires and help identify those at risk that could effectively be treated with such early psychological treatment, and they predicted over and above initial symptom severity. Reducing dysfunctional self-focus, self-immersed processing and putting the experience of mental defeat in perspective, as well as working through the trauma memory to enhance elaboration and cognitive processing comprise useful targets for such interventions.
Ethics Statement
The protocol was approved by the IRB of King's College Hospital. All subjects gave written informed consent in accordance with the Declaration of Helsinki.
Author Contributions
BK and AE developed the study concept and the study design. Testing and data collection were performed by BK. BK, AH, and AE performed the data analysis and interpretation. BK, RK, AH, and MM drafted the paper, and AE and MM provided critical revisions. All authors approved the final version of the paper for submission.
Funding
The study was funded by grants from the Psychiatry Research Trust and the Wellcome Trust (grant 069777). BK and AH were funded by grants from the Swiss National Science Foundation (PZ00P1_126597, PZ00P1_150812 to BK, PMPDP1_164470 to AH).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank Laure Coates and Linda Horrell for their help with narrative transcription. Correspondence concerning this paper should be addressed to Birgit Kleim, Department of Psychiatry, University of Zurich, Lenggstrasse 31, CH-8032 Zurich, Switzerland. Email: YmlyZ2l0LmtsZWltQHV6aC5jaA==, Phone: (+41) 44-635 7377.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2018.00645/full#supplementary-material
Footnotes
1. ^Data are reported for those 136 participants who provided both narratives initially and who were reassessed at 6 months later. This subgroup did not differ from the total sample in terms of age, sex, or initial PTSD symptom severity.
2. ^Other measures from the current sample are reported in (33, 34). None of these papers analyzed trauma or negative event narratives.
References
1. Bonanno GA, Westphal M, Mancini AD. Resilience to loss and potential trauma. Ann Rev Clin Psychol. (2011) 7:511–35. doi: 10.1146/annurev-clinpsy-032210-104526
2. Visser E, Gosens T, DenOudsten BL, De Vries J. The course, prediction, and treatment of acute and posttraumatic stress in trauma patients: a systematic review. J Trauma Acute Care Surg. (2017) 82:1158–83. doi: 10.1097/TA.0000000000001447
3. Kearns MC, Ressler KJ, Zatzick D, Rothbaum BO. Early interventions for PTSD: a review. Depression Anxiety (2012) 10:833–42. doi: 10.1002/da.21997
4. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry (1995) 52:1048–60. doi: 10.1001/archpsyc.1995.03950240066012
5. Wang PS, Lane MS, Olfson M, Pincus HA, Wells KD, Kessler RC. Twelve-month use of mental health services in the United States: results from the National Comorbidity Survey Replication. Arch Gen Psychiatry (2005) 62:629–40. doi: 10.1001/archpsyc.62.6.629
6. Pennebaker JW, Mehl MR, Niederhoffer KG. Psychological aspects of natural language use: our words, our selves. Ann Rev Psychol. (2003) 54:547–77. doi: 10.1146/annurev.psych.54.101601.145041
7. Fast LA, Funder DC. Gender differences in the correlates of self-referent word use: authority, entitlement, and depressive symptoms. J Pers. (2010) 78:313–38. doi: 10.1111/j.1467-6494.2009.00617.x
8. Rohrbaugh MJ, Mehl MR, Shoham V, Reilly ES, Ewy G. Prognostic significance of spouse we talk in couples coping with heart failure. J Consult Clin Psychol. (2008) 76:781–9. doi: 10.1037/a0013238
9. Sloan DM. It's all about me: self-focused attention and depressed mood. Cogn Ther Res. (2005) 29:279–88.
10. Simmons RA, Gordon PC, Chambless DL. Pronouns in marital interaction. Psychol Sci. (2005) 16:932–6. doi: 10.1111/j.1467-9280.2005.01639.x
11. Baumeister RF, Vohs KD, Funder DC. Psychology as the science of self-reports and finger movements: whatever happened to actual behavior? Perspect Psychol Sci. (2007) 2:396–403. doi: 10.1111/j.1745-6916.2007.00051.x
12. Küfner ACP, Back MD, Nestler S, Egloff B. Tell me a story and I will tell you who you are! Lens model analyses of personality and creative writing. J Res Pers. (2010) 44:427–35. doi: 10.1016/j.jrp.2010.05.003
13. Brewin CR. The nature and significance of memory disturbance in posttraumatic stress disorder. Ann Rev Clin Psychol. (2011) 7:203–27. doi: 10.1146/annurev-clinpsy-032210-104544
14. Ehlers A, Clark DM. A cognitive model of posttraumatic stress disorder. Behav Res Ther. (2000) 38:319–45. doi: 10.1016/S0005-7967(99)00123-0
15. Boals A, Klein K. Word use in emotional narratives about failed romantic relationships and subsequent mental health. J Lang Soc Psychol. (2005) 24:252–68. doi: 10.1177/0261927X05278386
16. Pennebaker JW, Mayne TJ, Francis ME. Linguistic predictors of adaptive bereavement. J Pers Soc Psychol. (1997) 72:863–71. doi: 10.1037/0022-3514.72.4.863
17. Ehlers A, Maercker A, Boos A. Posttraumatic stress disorder following political imprisonment: the role of mental defeat, alienation, and perceived permanent change. J Abnormal Psychol. (2000) 109:45–55. doi: 10.1037/0021-843X.109.1.45
18. Wilker S, Kleim B, Geiling A, Pfeiffer A, Elbert T, Kolassa I. Mental defeat and cumulative trauma experiences predict trauma-related psychopathology: evidence from a postconflict population in northern Uganda. Clin Psychol Sci. (2017) 5:974–84. doi: 10.1177/2167702617719946
19. Ozer EJ, Best SR, Lipsey TL, Weiss DS. Predictors of posttraumatic stress disorder and symptoms in adults: a meta-analysis. Psychol Bull. (2003) 129:52–73. doi: 10.1037/0033-2909.129.1.52
20. Alvarez-Conrad J, Zoellner LA, Foa EB. Linguistic predictors of trauma pathology and physical health. Appl Cogn Psychol. (2001) 15:S159–70. doi: 10.1002/acp.839
21. Dekel S, Bonanno GA. Changes in trauma memory and patterns of posttraumatic stress. Psychol Trauma Theory Res Pract Policy (2013) 5:26–34. doi: 10.1037/a0022750
22. Mundorf ES, Paivio SC. Narrative quality and disturbance pre- and post-emotion-focused therapy for child abuse trauma. J Traum Stress (2011) 24:643–50. doi: 10.1002/jts.20707
23. O‘Carroll Bantum E, Owen JE. Evaluating the validity of computerized content analysis programs for identification of emotional expression in cancer narratives. Psychol Assess. (2009) 21:79–88. doi: 10.1037/a0014643
24. Borelli JL, David DH, Sbarra DA, Mehl MR, Mayes LC. Language use in the adult attachment interview: evidence for attachment-specific emotion regulation. Pers Relat. (2012) 20:23–37. doi: 10.1111/j.1475-6811.2012.01394.x
25. Kross E, Ayduk O. Facilitating adaptive emotional analysis: distinguishing distanced-analysis of depressive experiences from immersed-analysis and distraction. Pers Soc Psychol Bull. (2008) 34:924–38. doi: 10.1177/0146167208315938
26. Mehl MR. The lay assessment of sub-clinical depression in daily life. Psychol Assess. (2006) 18:340–5. doi: 10.1037/1040-3590.18.3.340
27. Rude SS, Gortner EM, Pennebaker JW. Language use of depressed and depression-vulnerable college students. Cogn Emot. (2004) 18:1121–33. doi: 10.1080/02699930441000030
28. Junghaenel DU, Smyth JM, Santner L. Linguistic dimensions of psychopathology: a quantitative analysis. J Soc Clin Psychol. (2008) 27:36–55. doi: 10.1521/jscp.2008.27.1.36
29. Kross E, Ayduk O. Making meaning out of negative experiences by self-distancing. Curr Dir Psychol Sci. (2011) 20:187–91. doi: 10.1177/0963721411408883
30. Cohn MA, Mehl MR, Pennebaker JW. Linguistic markers of psychological change surrounding September 11, 2001. Psychol Sci. (2004) 15:687–93. doi: 10.1111/j.0956-7976.2004.00741.x
31. Back MD, Küfner AC, Egloff B. The emotional timeline of September 11, 2001. Psychol Sci. (2010) 21:1417–9. doi: 10.1177/0956797610382124
32. D'Andrea W, Chiu PH, Casas BR, Deldin P. Linguistic predictors of post-traumatic stress disorder symptoms following 11 September 2001. Appl Cogn Psychol. (2012) 26:316–23. doi: 10.1002/acp.1830
33. Kleim B, Wilhelm F, Glucksman E, Ehlers A. Heart rate reactivity to script-driven imagery early after trauma predicts PTSD in female, but not in male assault survivors. Psychosom Med. (2010) 72:917–24. doi: 10.1097/PSY.0b013e3181f8894b
34. Kleim B, Ehlers A, Glucksman E. Prediction of chronic posttraumatic stress disorder after assault. Psychol Med. (2007) 37:1457–68. doi: 10.1017/S0033291707001006
35. Foa EB, Cashman L, Jaycox L, Perry K. The validation of a self-report measure of posttraumatic stress disorder: the posttraumatic diagnostic scale. Psychol Assess. (1997) 9:445–51. doi: 10.1037/1040-3590.9.4.445
36. Foa EB, Riggs DS, Dancu CV, Rothbaum BO. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J Traum Stress (1993) 6:459–73. doi: 10.1002/jts.2490060405
37. Nelson HE, Willison JR. The Revised National Adult Reading Test–Test Manual. Windsor: NFER-Nelson (1991).
38. Crawford JR, Parker DM, Allan KM, Jack AM, Morrison FM. The Short NART: cross-validation, relationship to IQ and some practical considerations. Br J Clin Psychol. (1991) 30:223–9. doi: 10.1111/j.2044-8260.1991.tb00940.x
39. Pennebaker JW, Booth RE, Francis ME. Linguistic Inquiry and Word Count: LIWC2007 – Operator's Manual. Austin, TX: LIWC.net (2007).
40. Halligan SL, Michael T, Clark DM, Ehlers A. Posttraumatic stress disorder following assault: the role of cognitive processing, trauma memory, and appraisals. J Consult Clin Psychol. (2003) 71:419–31. doi: 10.1037/0022-006X.71.3.419
41. Dunmore E, Clark DM, Ehlers A. A prospective investigation of the role of cognitive factors in persistent posttraumatic stress disorder (PTSD) after physical or sexual assault. Behav Res Ther. (2001) 39:1063–84. doi: 10.1016/S0005-7967(00)00088-7
42. Foa EB, Ehlers A, Clark DM, Tolin DF, Orsillo SM. The Posttraumatic Cognitions Inventory (PTCI): development and validation. Psychol Assess. (1999) 11:303–14. doi: 10.1037/1040-3590.11.3.303
43. Jones C, Harvey AG, Brewin CR. The organisation and content of trauma memories in survivors of road traffic accidents. Behav Res Ther. (2007) 45:151–62. doi: 10.1016/j.brat.2006.02.004
44. Pennebaker JW, Boyd RL, Jordan K, Blackburn K The Development and Psychometric Properties of LIWC 2015. Austin, TX: University of Texas at Austin (2015).
Keywords: post-traumatic stress disorder, early predictors, cognitive processing, LIWC, text analysis, linguistic
Citation: Kleim B, Horn AB, Kraehenmann R, Mehl MR and Ehlers A (2018) Early Linguistic Markers of Trauma-Specific Processing Predict Post-trauma Adjustment. Front. Psychiatry 9:645. doi: 10.3389/fpsyt.2018.00645
Received: 25 May 2018; Accepted: 15 November 2018;
Published: 05 December 2018.
Edited by:
Chantal Martin Soelch, Université de Fribourg, SwitzerlandReviewed by:
Tanja Michael, Saarland University, GermanySebastian Trautmann, Technische Universität Dresden, Germany
Copyright © 2018 Kleim, Horn, Kraehenmann, Mehl and Ehlers. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Birgit Kleim, Yi5rbGVpbUBwc3ljaG9sb2dpZS51emguY2g=