 James G. Scott1,2,3*Lori Matuschka1,2Solja Niemelä4,5
James G. Scott1,2,3*Lori Matuschka1,2Solja Niemelä4,5 Jouko Miettunen6,7Brett Emmerson1,3
Jouko Miettunen6,7Brett Emmerson1,3 Antti Mustonen6,7
Antti Mustonen6,7- 1Faculty of Medicine, The University of Queensland, Herston, QLD, Australia
- 2Queensland Centre for Mental Health Research, Wacol, QLD, Australia
- 3Metro North Mental Health, Royal Brisbane and Women's Hospital, Herston, QLD, Australia
- 4Faculty of Medicine, University of Turku, Turku, Finland
- 5Department of Psychiatry, South-Western Hospital District, Turku, Finland
- 6Center for Life Course Health Research, University of Oulu, Oulu, Finland
- 7Medical Research Center Oulu, Oulu University Hospital and University of Oulu, Oulu, Finland
There has been emerging evidence of an association between tobacco smoking and schizophrenia spectrum disorders (SSD). Two meta-analyses have reported that people who smoke tobacco have an ~2-fold increased risk of incident schizophrenia or psychosis, even after adjusting for confounding factors. This study aimed to critically appraise the research which has examined the association between tobacco smoking and SSD against the Bradford Hill criteria for causality, to determine the strength of the evidence for a causal relationship. Eight longitudinal studies (seven cohort studies and one case control study) were identified which examined tobacco smoking as an exposure and psychosis as an outcome. All seven cohort studies were assessed as being of high quality using the Newcastle-Ottawa Scale. Six of the eight studies found a statistically significant positive association between tobacco smoking and onset of SSD. These studies reported a consistent association with a moderate to large effect size and a dose response relationship. The studies adjusted for multiple potential confounders including age, sex, socioeconomic status, shared genetic risk, prodromal symptoms, and comorbid cannabis and other substance use. The studies did not adjust for exposure to childhood trauma or prenatal tobacco. There was substantial though inconclusive evidence supporting a causal relationship between tobacco smoking and increased risk of SSD. If a causal relationship does exist, nicotine is most likely responsible for this association. This raises serious public health concerns about the increasing use of e-cigarettes and other products, particularly by adolescents whose nicotine use may increase their risk of SSD. Research is urgently needed to examine the association between e-cigarette use and incident psychosis, particularly in adolescents and young adults.
Introduction
Schizophrenia spectrum disorders (SSD) are heterogeneous syndromes with well-established risk factors including exposure to childhood adversity, cannabis use during adolescence, a history of obstetric complications, stressful events during adulthood, and low maternal serum folate level (1). In recent years, there has been a growing interest in tobacco smoking as a risk factor for SSD (2, 3).
Tobacco smoking is known to cause a wide range of physical health problems. It is the leading cause of preventable death, through increasing the risk of lung and other malignancies, chronic obstructive pulmonary disease (COPD), coronary heart disease, cerebrovascular disease, asthma and diabetes (4). Two systematic reviews and meta-analyses have examined the association between tobacco smoking and psychotic disorders (2, 3). In pooling longitudinal studies (n = 5), Gurillo and colleagues reported a 2-fold increase in the risk of incident psychotic disorders in people who were daily tobacco smokers compared to those who were not (RR = 2.18; 95% CI 1.23–3.85). Similarly, Hunter et al. (3) who pooled data from studies identified using inclusion criteria with the outcome restricted to schizophrenia (N = 5) also reported smoking tobacco was associated with a 2-fold risk of schizophrenia (RR = 1.99; 95% CI 1.10–3.61). Both studies concluded that further research was needed to examine the potential causal role of tobacco smoking in the onset of SSD.
The association between tobacco smoking and SSD is of growing significance. There is evidence that nicotine alters signaling in the dopaminergic, cholinergic, and glutamatergic neurotransmitter systems, particularly in adolescence (5). Whilst the smoking of tobacco by young people has declined in many high income countries, there has been an increase in exposure to nicotine by this demographic through the availability of e-cigarettes (6). It is therefore important to critically examine the evidence for a causal relationship between tobacco smoking and SSD.
In this review we aimed to evaluate the relationship between tobacco smoking and SSD which we defined as any non-affective psychotic disorder against causal criteria based on the Bradford Hill Framework (7, 8). The Bradford Hill Framework provides nine criteria for establishing a causal relationship between an exposure and outcome. This review examined longitudinal studies identified from the two recent systematic reviews of tobacco smoking and incident SSD and other identified studies. The evidence for a causal relationship between tobacco smoking and SSD, alternative explanations for the association and the health implications are discussed.
Methods
Literature Search
We used the results of the two recently conducted systematic reviews (2, 3) to identify studies which examined tobacco smoking as an exposure and SSD as an outcome. As the review by Hunter et al. (3) restricted the outcome to a diagnosis of schizophrenia, we used the broader search strategy of Gurillo et al. (2) to identify studies from January 2014 to May 2018 that included the broader outcome of psychosis. These psychosis outcomes included schizophrenia, schizophreniform disorder, schizoaffective disorder, delusional disorder, non-affective psychotic disorder, atypical psychosis, psychotic depression, and bipolar mania with psychotic features.
The inclusion criteria of the current review were: (a) longitudinal case control or cohort studies; (b) study populations of participants with psychosis or schizophrenia as the outcome (defined as those who meet the diagnostic criteria by structured interview or diagnosed by treating clinician); (c) presence of tobacco smoking prior to psychosis or schizophrenia diagnosis. Studies which were cross sectional in design or only provided sub-diagnostic outcomes of psychosis (e.g., psychotic symptoms, hallucinations, delusions) were excluded.
Data Extraction
Titles and abstracts of the articles were reviewed to identify studies that met the eligibility criteria. The following characteristics were extracted from each study when available: (a) study methodology (including author, publication year, location, study design, follow-up period, sample numbers, loss to follow-up, age at baseline, tobacco smoking measures, and assessment of psychosis or schizophrenia), and (b) study findings (effect size metrics, 95% CI, and confounders adjusted for).
The quality or the studies assessing for risk of bias was evaluated using Newcastle–Ottawa Scale (NOS) (9) as shown in Supplementary Table 1. The NOS is a method recommended by the Cochrane Non-randomized Studies Methods Working Group to evaluate the quality of the study. Points are assigned based on the selection process of cohorts (0–4 points), the comparability of the cohorts (0–2 points) and the identification of the exposures and the outcomes of research participants (0–3 points). A score of 7 or greater out of 9 was defined as high quality. Studies were assessed independently by two reviewers (LM and JS).
Assessment of Causality
Studies that met inclusion and exclusion criteria were assessed using causal criteria based on the Bradford Hill Framework shown in Supplementary Table 2. Of the nine criteria, five were chosen as most relevant for the purposes of this study (strength of association, consistency, temporality, dose-response, and biological plausibility). Given that smoking is known to cause a wide range of health problems, the criteria of specificity was not applicable. No studies have performed experimental manipulation exposing adolescents to tobacco because of the known harmful effects therefore this criteria was not included. Coherence was not included because of the lack of homogenous pathology evident in psychosis. In relation to analogy, the association between cannabis use and psychosis, reported to be causal (1) has some analogy to that of tobacco and psychosis. However, it is widely recognized that adolescents who smoke tobacco are more likely to smoke cannabis (10–12). Thus, cannabis rather than being analogous to tobacco in its relationship with psychosis may in fact be an important confounder. Similarly there are other important environmental factors which might confound the relationship between tobacco smoking and incident psychotic disorder. To address this concern, for the purpose of assessing evidence of causality, we included an extra criteria “accounted for confounding.” These six criteria were deemed appropriate by the research team in order to grade the associations reported between adolescent tobacco smoking and future risk of SSD as a basis for causality discussion (7).
Results
Gurillo and colleagues (2) identified four studies which met the specified inclusion criteria (13–16). One of the longitudinal studies (17) which they included in their pooled analysis did not determine the presence of tobacco smoking before the schizophrenia diagnosis and was therefore excluded. Hunter et al. (3) included another study (18) and the updated search identified a further three studies which met inclusion criteria (13, 19–21). In total, eight studies (seven cohort and one case-control studies) were included for assessment of a causal relationship between tobacco smoking in adolescence and incident SSD. Using the NOS, all seven cohort studies scored 7/9 or greater demonstrating they were of high quality (Table 1).
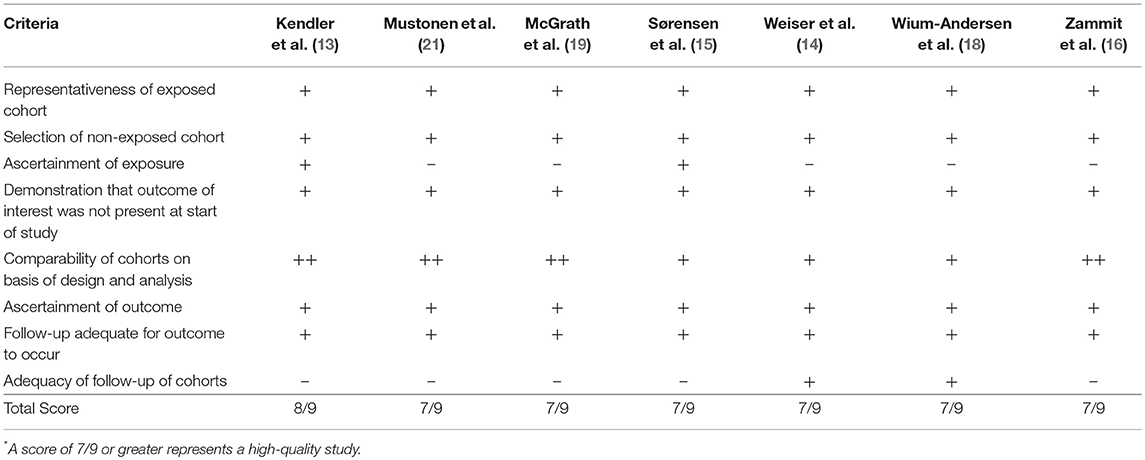
Table 1. Assessment of study quality using the Newcastle Ottowa Scale*.
Study Characteristics
Table 2 summarizes the study characteristics. They utilized birth cohort studies of offspring (19, 21) or mothers (15), cohorts of young male conscripts from defense forces (14, 16), two cohorts combined, the first consisting of mothers recruited from a birth cohort, the second were male conscripts Kendler et al. (13) and two general population cohorts to assess cardiovascular risk factors (18). The longitudinal case control study was of participants at clinical high risk of psychosis (20). All studies were from high income countries. The follow-up period of all cohort studies was adequate to ascertain incident cases of SSD, ranging from a minimum of 4 years (14) to a maximum of 48 years (15). Two of the studies were genetically informed with one examining psychosis risk in family members discordant for smoking (13), the other examining schizophrenia in people with different alleles of the rs1051730 genotype in the nicotinic acetylcholine receptor gene stratified by smoking status (18).
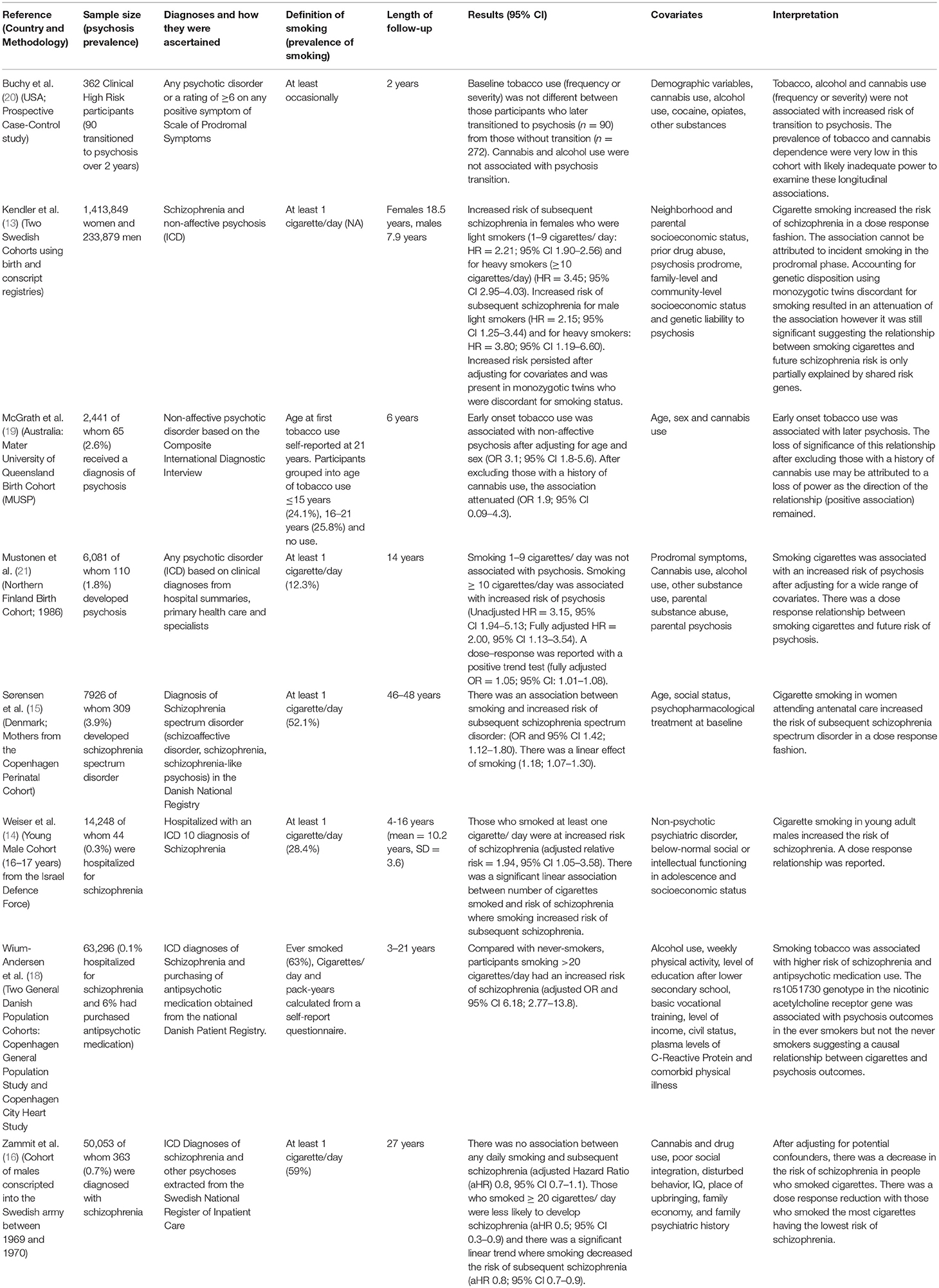
Table 2. Longitudinal studies examining the association between tobacco smoking and later schizophrenia and related disorders.
Assessment of Studies Against Bradford Hill Criteria
Using causal criteria, based on the Bradford Hill Framework Hill (8), of the eight studies examined, six reported a positive association between tobacco smoking and risk of schizophrenia spectrum disorder. The strength of the associations were robust ranging from an almost 50% increased risk (15) to a 6-fold increased risk of schizophrenia in heavy smokers (18). In these six studies, all reported a temporal association with appropriate adjustment for confounding variables, particularly comorbid substance use. All but one (19) demonstrated a dose response relationship between tobacco use and SSD. By contrast, one study (16) reported that smoking tobacco reduced the risk of schizophrenia and the case control study (20) found no association.
Discussion
Two meta-analyses have demonstrated that smoking tobacco is associated with a 2-fold increase in risk of incident schizophrenia (3) or broader psychosis (2). Based on these systematic reviews and our own literature search, we identified eight studies that examined the longitudinal association between tobacco smoking and incident SSD of which six demonstrated a positive association (13–15, 18, 19, 21), one a negative association (16) and the final study showed no association (20). Using the Bradford Hill framework, a causal association between tobacco smoking and onset of SSD is discussed on the basis of strength of association, temporality, dose-response, adjustment for confounding factors, biological plausibility, and consistency of the association.
Strength
Of the six studies that found a positive association (13–15, 18, 19, 21), five reported moderate to large effect sizes (22) (Tables 2, 3) consistent with a causal relationship (8). Sørensen et al. (15) reported a smaller effect size with a 42% increase in the odds of schizophrenia spectrum disorder in people who smoked cigarettes.
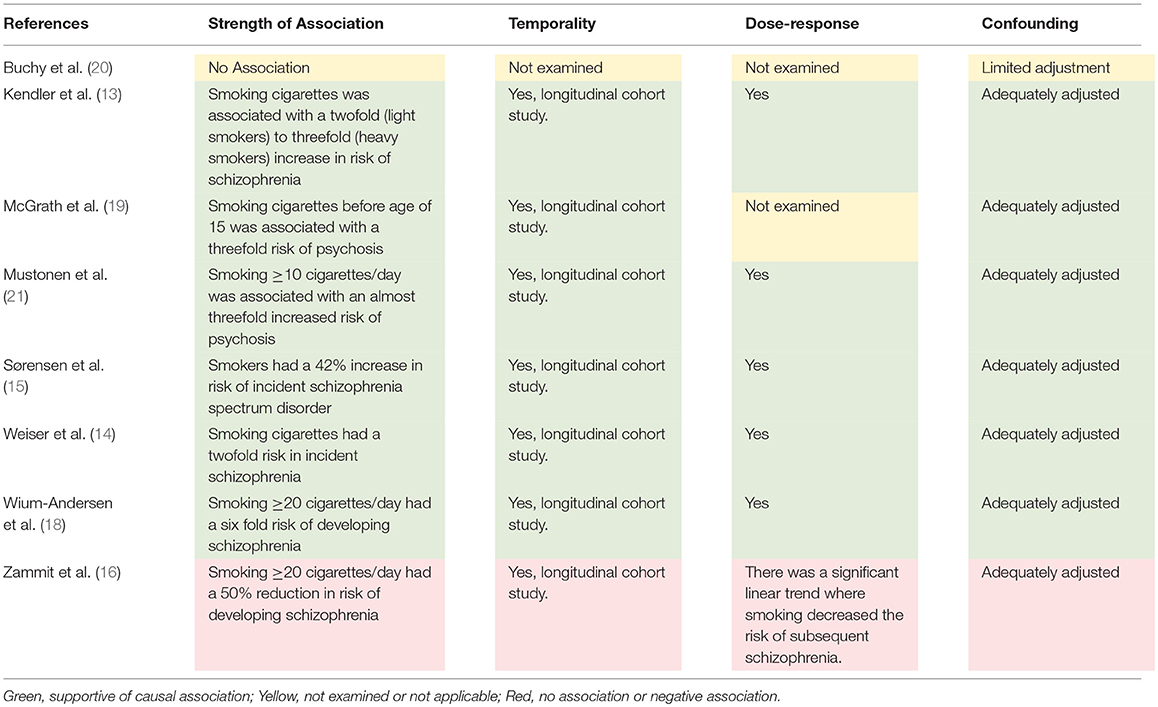
Table 3. Assessment of studies against Bradford Hill criteria.
Consistency
Consistency of the association is assessed through multiple studies of independent cohorts confirming the same result. In the eight longitudinal studies, six reported a positive association between tobacco smoking and incident SSD. Of the two which did not report a positive association, one was a case-control study of participants at clinical high risk for psychosis which found that neither tobacco nor cannabis smoking were associated with transition to psychosis. The prevalence of tobacco and cannabis dependence in this cohort was low and the study may have been underpowered to examine the effects of these substances on transition to psychosis. Zammit et al. (16) reported that smoking tobacco was associated with a lower risk of future schizophrenia, and was therefore inconsistent with the main body of research. The overwhelming majority of studies showed a positive relationship fulfilling criteria for consistency.
Temporality
The six studies that reported a positive association demonstrated a clear temporal relationship with the exposure of tobacco smoking preceding the onset of SSD. Schizophrenia spectrum disorders frequently have an insidious onset with a long prodrome. In order to address this concern, (21), adjusted for prodromal psychotic symptoms at baseline and Kendler et al. (13) accounted for the possible prodrome by conducting a subanalysis restricting the onset of SSD to at least 5 years following initial exposure to tobacco. The relationship between tobacco smoking and onset of schizophrenia was largely attenuated after accounting for the prodrome rendering reverse causality an unlikely explanation for the association between tobacco use and SSD thus suggesting tobacco smoking precedes the illness.
Dose-Response
A dose response between tobacco smoking and incident SSD was reported in five of the six studies reporting a positive association. In three studies (14, 15, 21) a significant linear trend was demonstrated where the risk of SSD increased with the an increase in tobacco smoking. In two studies (13, 18), those who smoked more daily tobacco had an increase in the odds of developing SSD.
Potential Confounders
The relationship between tobacco use and SSD remained significant even after adjusting for factors that might confound the relationship including family socio-economic status, cannabis use (1), parental substance abuse and parental psychosis (23–27). A shared genetic liability was also accounted for in two genetically informed studies (13, 18). Adjustment for confounders attenuated the strength of the association but significance was maintained in all but one study (19), probably due to a lack of power for the analysis. None of the studies adjusted for childhood trauma (28).
Biological Plausibility
Tobacco and tobacco smoke contain almost 5,000 different chemicals. Nicotine is the most important pharmacologically active and psychotogenic compound in tobacco smoke because of its interaction with nicotinic acetylcholine receptors (29). Previous reports on tobacco smoking suggests that nicotine could alter signaling of dopaminergic, cholinergic, and glutamatergic neurotransmitter systems (5, 30) and thus could potentially influence brain development as suggested by studies of adolescent nicotine exposure and neurodevelopmental trajectories (5). Also, excess nicotine intake during early adolescence is associated with abnormal white matter maturation in adults (31), and chronic cigarette smoking has been linked to structural brain changes such as gray matter decreases in the prefrontal cortex, which correspond with areas where functional alterations occur from nicotine exposure (32).
Furthermore, recent evidence suggest that adolescent nicotine use could have persistent effects on nicotine receptor responsiveness, which results in the strengthening of negative emotional changes and alterations in cognitive functioning (5).
Alternative Explanations
There are other explanations for the positive association between tobacco smoking and SSD. Individuals who develop schizophrenia are more likely to have externalizing symptoms in childhood and adolescence (33, 34) and children with externalizing symptoms are more likely to smoke tobacco during adolescence (35). There may be unmeasured confounding. None of the studies adjusted for childhood trauma, a well-established risk factor for SSD (1, 28) and for tobacco use (36). Similarly there was no adjustment for prenatal tobacco smoking exposure which is associated with both an increased risk of smoking in adolescence (37) and an increased risk of schizophrenia even after adjusting for life time smoking (3, 38). Furthermore, recent studies have suggested bidirectional associations by revealing single nucleotide polymorphisms associated with nicotine dependence (CHRNA5) that are also associated with schizophrenia (39, 40).
Limitations
Each study included in this review is observational in methodology, and the majority of cohort studies included had significant attrition. Participants who are most likely to be lost to follow up are more likely to be socioeconomically disadvantaged and be at increased risk of both tobacco smoking and mental illness. Therefore, it is unlikely that attrition would significantly affect reported associations. Measurement of tobacco smoking has been measured via self-report or by interview, generally at one point in time and often retrospectively recalled. Only one study measured the long-term smoking exposure prior the psychotic illness using pack-years (18) which provides a more precise measurement of tobacco smoke exposure. Further, no studies have used biological markers for tobacco smoking such as expired air carbon monoxide (41) or serum cotinine measurement (42). These limitations are inherent to large cohort and registry studies and are difficult to overcome. Finally, as two recent systematic reviews had been published on this topic, we relied on these to identify the studies included in this review rather than replicating the searches in these studies.
Implications
Given tobacco is known to have widespread adverse health outcomes and governments around the world are adopting policies to reduce tobacco smoking, why is it important to clarify if smoking tobacco has a causal role in the onset of SSD? The first reason is that better understanding the aetiopathogenesis of SSD will inform our knowledge of this syndrome which may lead to better treatments. The second, a much more urgent consideration is the growing availability of electronic (e) cigarettes. These have been developed as a safer alternative to cigarettes by enabling nicotine use without the exposure to carcinogenic chemicals associated with smoking tobacco.
However, there is growing use of e-cigarettes and other nicotine products by adolescents (6) and it is acknowledged that the health effects of e-cigarettes on youth are not fully understood (43). In addition to tobacco and cannabis, there is now evidence that adolescents who use inhalants are at increased risk of psychotic disorders (44) suggesting that adolescence is the developmental period where adverse neuropsychiatric outcomes from psychoactive substances are most likely to occur. There is substantial though not conclusive evidence that the association between tobacco smoking and SSD is causal and may well be a result of the effects of nicotine on multiple neurotransmitter systems. Therefore, policy makers must be cautious when developing regulations for the availability of e-cigarettes, nicotine replacement therapy products and smokeless tobacco. Similarly, health practitioners who recommend e-cigarettes or smokeless tobacco products as a safe alternative to smoking need to consider the findings of the studies identified in this review, especially when providing advice to adolescents.
It is essential that future well designed observational studies are undertaken examining the risk of SSDs in those who use e-cigarettes, particularly in adolescence. A major challenge is the low prevalence of SSD. Recruiting samples large enough to examine the association between e-cigarettes and SSD will take many years. Previous longitudinal research has shown positive associations between cannabis, tobacco and alcohol use and psychotic experiences (PE) which are proxy markers for psychosis risk. PE have the advantage of being higher in prevalence compared to SSD thereby reducing the required sample size to identify associations. Schizophrenia endophenotypes may also have a role to inform the association between nicotine exposure through e-cigarettes and risk of SSD. Previous research has shown that smoking tobacco modulates the association between polymorphisms of transcription factor 4 and reduced sensory gating, an endophenotype of schizophrenia suggesting that the smoking of tobacco might play a role in early information processing deficits in schizophrenia (45). Use of research paradigms such as PE and endophenotypes PE would expedite research into the association between e-cigarette use and SSD risk. Further research is urgently needed to determine if nicotine is causally associated with incident SSD. In the interim, it is important that policy makers consider the available evidence between tobacco smoking and risk of schizophrenia when evaluating the potential health consequences that might arise from community access to e-cigarettes.
Author Contributions
JS and AM planned the review. LM conducted the initial literature search and JS and LM assessed papers for suitability for inclusion. JS and LM reviewed all the papers and assessed them for quality. JS, LM, and AM wrote the first draft of the manuscript and all authors contributed to further drafts. All authors reviewed and approved the final draft.
Funding
JS is supported by a National Health and Medical Research Council Practitioner Fellowship Grant APP1105807 and employed by The Queensland Centre for Mental Health Research which receives core funding from the Queensland Health. AM is supported by Juho Vainio Foundation, Scholarship Fund of the University of Oulu, Oulun Lääketieteellinen tutkimussäätiö and The Hospital District of South Ostrobothnia, Finland. JM is supported by Academy of Finland (#268336).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2018.00607/full#supplementary-material
References
1. Belbasis L, Köhler CA, Stefanis N, Stubbs B, Os Jv, Vieta E, et al. Risk factors and peripheral biomarkers for schizophrenia spectrum disorders: an umbrella review of meta-analyses. Acta Psychiatr Scand. (2018) 137:88–97. doi: 10.1111/acps.12847
2. Gurillo P, Jauhar S, Murray RM, MacCabe JH. Does tobacco use cause psychosis? Systematic review and meta-analysis. Lancet Psychiatry (2015) 2:718–25. doi: 10.1016/S2215-0366(15)00152-2
3. Hunter A, Murray R, Asher L, Leonardi-Bee J. The effects of tobacco smoking, and prenatal tobacco smoke exposure, on risk of schizophrenia: a systematic review and meta-analysis. Nicotine Tob Res. (2018). doi: 10.1093/ntr/nty160. [Epub ahead of print].
4. Collaborators GT. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet (2017) 389:1885–906. doi: 10.1016/s0140-6736(17)30819-x
5. Smith RF, McDonald CG, Bergstrom HC, Ehlinger DG, Brielmaier JM. Adolescent nicotine induces persisting changes in development of neural connectivity. Neurosci Biobehav Rev (2015) 55:432–43. doi: 10.1016/j.neubiorev.2015.05.019
6. Perikleous EP, Steiropoulos P, Paraskakis E, Constantinidis TC, Nena E. E-cigarette use among adolescents: an overview of the literature and future perspectives. Front Public Health (2018) 6:86. doi: 10.3389/fpubh.2018.00086
7. Fedak KM, Bernal A, Capshaw ZA, Gross S. Applying the bradford hill criteria in the 21st century: how data integration has changed causal inference in molecular epidemiology. Emerg Themes Epidemiol. (2015) 12:14. doi: 10.1186/s12982-015-0037-4
8. Hill AB. The environment and disease: association or causation? Proc R Soc Med. (1965) 58:295–300.
9. Wells G, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa: The Ottawa Hospital (2018).
10. Hindocha C, Shaban NDC, Freeman TP, Das RK, Gale G, Schafer G, et al. Associations between cigarette smoking and cannabis dependence: a longitudinal study of young cannabis users in the United Kingdom. Drug Alcohol Depend. (2015) 148:165–71. doi: 10.1016/j.drugalcdep.2015.01.004
11. Badiani A, Boden JM, De Pirro S, Fergusson DM, Horwood LJ, Harold GT. Tobacco smoking and cannabis use in a longitudinal birth cohort: evidence of reciprocal causal relationships. Drug Alcohol Depend. (2015) 150:69–76. doi: 10.1016/j.drugalcdep.2015.02.015
12. Weinberger AH, Platt J, Copeland J, Goodwin RD. Is cannabis use associated with increased risk of cigarette smoking initiation, persistence, and relapse? longitudinal data from a representative sample of US adults. J Clin Psychiatry (2018) 79:17m11522. doi: 10.4088/JCP.17m11522
13. Kendler KS, Lönn SL, Sundquist J, Sundquist K. Smoking and schizophrenia in population cohorts of swedish women and men: a prospective co-relative control study. Am J Psychiatry (2015) 172:1092–100. doi: 10.1176/appi.ajp.2015.15010126
14. Weiser M, Reichenberg A, Grotto I, Yasvitzky R, Rabinowitz J, Lubin G, et al. Higher rates of cigarette smoking in male adolescents before the onset of schizophrenia: a historical-prospective cohort study. Am J Psychiatry (2004) 161:1219–23. doi: 10.1176/appi.ajp.161.7.1219
15. Sørensen HJ, Mortensen EL, Reinisch JM, Mednick SA. A prospective study of smoking in young women and risk of later psychiatric hospitalization. Nordic J Psychiatry (2011) 65:3–8. doi: 10.3109/08039481003786386
16. Zammit S, Allebeck P, Dalman C, Lundberg I, Hemmingsson T, Lewis G. Investigating the association between cigarette smoking and schizophrenia in a cohort study. Am J Psychiatry (2003) 160:2216–21. doi: 10.1176/appi.ajp.160.12.2216
17. Riala K, Hakko H, Isohanni M, Pouta A, Räsänen P. Is initiation of smoking associated with the prodromal phase of schizophrenia? J Psychiatry Neurosci. (2005) 30:26–32.
18. Wium-Andersen MK, Orsted DD, Nordestgaard BG. Tobacco smoking is causally associated with antipsychotic medication use and schizophrenia, but not with antidepressant medication use or depression. Int J Epidemiol. (2015) 44:566–77. doi: 10.1093/ije/dyv090
19. McGrath JJ, Alati R, Clavarino A, Williams GM, Bor W, Najman JM, et al. Age at first tobacco use and risk of subsequent psychosis-related outcomes: a birth cohort study. Aust N Z J Psychiatry (2016) 50:577–83. doi: 10.1177/0004867415587341
20. Buchy L, Cadenhead KS, Cannon TD, Cornblatt BA, McGlashan TH, Perkins DO, et al. Substance use in individuals at clinical high risk of psychosis. Psychol Med. (2015) 45:2275–84. doi: 10.1017/S0033291715000227
21. Mustonen A, Ahokas T, Nordström T, Murray GK, Mäki P, Jääskeläinen E, et al. Smokin‘ hot: adolescent smoking and the risk of psychosis. Acta Psychiatr Scand. (2018) 138:5–14. doi: 10.1111/acps.12863
22. Rosenthal JA. Qualitative descriptors of strength of association and effect size. J Soc Serv Res. (1996) 21:37–59. doi: 10.1300/J079v21n04_02
23. McAdams TA, Neiderhiser JM, Rijsdijk FV, Narusyte J, Lichtenstein P, Eley TC. Accounting for genetic and environmental confounds in associations between parent and child characteristics: a systematic review of children-of-twins studies. Psychol Bull. (2014) 140:1138–73. doi: 10.1037/a0036416
24. Niemi-Pynttäri JA, Sund R, Putkonen H, Vorma H, Wahlbeck K, Pirkola SP. Substance-induced psychoses converting into schizophrenia: a register-based study of 18,478 Finnish inpatient cases. J Clin Psychiatry (2013) 74:e94–9. doi: 10.4088/JCP.12m07822
25. Patrick ME, Wightman P, Schoeni RF, Schulenberg JE. Socioeconomic status and substance use among young adults: a comparison across constructs and drugs. J Stud Alcohol Drugs (2012) 73:772–82. doi: 10.15288/jsad.2012.73.772
26. Radhakrishnan R, Wilkinson ST, D'Souza DC. Gone to pot - a review of the association between cannabis and psychosis. Front Psychiatry (2014) 5:54. doi: 10.3389/fpsyt.2014.00054
27. Starzer MSK, Nordentoft M, Hjorthøj C. Rates and predictors of conversion to schizophrenia or bipolar disorder following substance-induced psychosis. Am J Psychiatry (2018) 175:343–50. doi: 10.1176/appi.ajp.2017.17020223
28. Varese F, Smeets F, Drukker M, Lieverse R, Lataster T, Viechtbauer W, et al. Childhood adversities increase the risk of psychosis: a meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr Bull. (2012) 38:661–71. doi: 10.1093/schbul/sbs050
29. Thielen A, Klus H, Müller L. Tobacco smoke: unraveling a controversial subject. Exp Toxicol Pathol. (2008) 60:141–56. doi: 10.1016/j.etp.2008.01.014
30. Davis J, Eyre H, Jacka FN, Dodd S, Dean O, McEwen S, et al. A review of vulnerability and risks for schizophrenia: Beyond the two hit hypothesis. Neurosci Biobehav Rev. (2016) 65:185–94. doi: 10.1016/j.neubiorev.2016.03.017
31. Gogliettino AR, Potenza MN, Yip SW. White matter development and tobacco smoking in young adults: a systematic review with recommendations for future research. Drug Alcohol Depend. (2016) 162:26–33. doi: 10.1016/j.drugalcdep.2016.02.015
32. Sutherland MT, Riedel MC, Flannery JS, Yanes JA, Fox PT, Stein EA, et al. Chronic cigarette smoking is linked with structural alterations in brain regions showing acute nicotinic drug-induced functional modulations. Behav Brain Funct. (2016) 12:16. doi: 10.1186/s12993-016-0100-5
33. Scott J, Martin G, Welham J, Bor W, Najman J, O'Callaghan M, et al. Psychopathology during childhood and adolescence predicts delusional-like experiences in adults: a 21-year birth cohort study. Am J Psychiatry (2009) 166:567–74. doi: 10.1176/appi.ajp.2008.08081182
34. Matheson SL, Shepherd AM, Laurens KR, Carr VJ. A systematic meta-review grading the evidence for non-genetic risk factors and putative antecedents of schizophrenia. Schizophr Rese. (2011) 133:133–42. doi: 10.1016/j.schres.2011.09.020
35. Miettunen J, Murray GK, Jones PB, Maki P, Ebeling H, Taanila A, et al. Longitudinal associations between childhood and adulthood externalizing and internalizing psychopathology and adolescent substance use. Psychol Med. (2014) 44:1727–38. doi: 10.1017/S0033291713002328
36. Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Med. (2012) 9:e1001349. doi: 10.1371/journal.pmed.1001349
37. Niemela S, Raisanen A, Koskela J, Taanila A, Miettunen J, Ramsay H, et al. The effect of prenatal smoking exposure on daily smoking among teenage offspring. Addiction (2017) 112:134–43. doi: 10.1111/add.13533
38. Niemela S, Sourander A, Surcel HM, Hinkka-Yli-Salomaki S, McKeague IW, Cheslack-Postava K, et al. Prenatal nicotine exposure and risk of schizophrenia among offspring in a national birth cohort. Am J Psychiatry (2016) 173:799–806. doi: 10.1176/appi.ajp.2016.15060800
39. Chen J, Bacanu SA, Yu H, Zhao Z, Jia P, Kendler KS, et al. Genetic relationship between schizophrenia and nicotine dependence. Sci Rep. (2016). 6:25671. doi: 10.1038/srep25671.
40. Hartz SM, Horton AC, Hancock DB, Baker TB, Caporaso NE, Chen LS, et al. Genetic correlation between smoking behaviors and schizophrenia. Schizophr Res. (2018) 194:86–90. doi: 10.1016/j.schres.2017.02.022
41. Jarvis MJ, Russell MA, Saloojee Y. Expired air carbon monoxide: a simple breath test of tobacco smoke intake. Br Med J. (1980) 281:484–5.
42. Vartiainen E, Seppala T, Lillsunde P, Puska P. Validation of self reported smoking by serum cotinine measurement in a community-based study. J Epidemiol Commun Health (2002) 56:167–70. doi: 10.1136/jech.56.3.167
43. National Academies of Sciences Engineering and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on the Review of the Health Effects of Electronic Nicotine Delivery Systems. Public Health Consequences of E-Cigarettes. In: Eaton DL, Kwan LY, Stratton K, editors. Washington, DC: National Academies Press (US) (2018).
44. Mustonen A, Niemela S, McGrath JJ, Murray GK, Nordstrom T, Maki P, et al. Adolescent inhalant use and psychosis risk-a prospective longitudinal study. Schizophr Res. (2018). doi: 10.1016/j.schres.2018.05.013. [Epub ahead of print].
Keywords: schizophrenia, psychosis, nicotine, smoking, causal, association, e-cigarette
Citation: Scott JG, Matuschka L, Niemelä S, Miettunen J, Emmerson B and Mustonen A (2018) Evidence of a Causal Relationship Between Smoking Tobacco and Schizophrenia Spectrum Disorders. Front. Psychiatry 9:607. doi: 10.3389/fpsyt.2018.00607
Received: 07 September 2018; Accepted: 30 October 2018;
Published: 20 November 2018.
Edited by:
David Jonathan Castle, The University of Melbourne, AustraliaReviewed by:
Peter Bosanac, St Vincent's Hospital (Melbourne), AustraliaBoris B. Quednow, University of Zurich, Switzerland
Copyright © 2018 Scott, Matuschka, Niemelä, Miettunen, Emmerson and Mustonen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: James G. Scott, amFtZXMuc2NvdHRAaGVhbHRoLnFsZC5nb3YuYXU=