 Xiangwen Chang
Xiangwen Chang Yan Sun
Yan Sun Yang Zhang
Yang Zhang Jiana Muhai
Jiana Muhai Lin Lu
Lin Lu Jie Shi
Jie Shi
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry, 16 November 2018
Sec. Addictive Disorders
Volume 9 - 2018 | https://doi.org/10.3389/fpsyt.2018.00603
This article is part of the Research TopicMethamphetamine–Related Psychosis: Symptoms, Epidemiology, Risk Factors and InterventionView all 6 articles
The illegal use of methamphetamine (MA) is a growing public health concern globally and results in a series of negative effects. The prominent detrimental effect of MA use is MA-related psychiatric symptoms (MAP) and is observed at a much higher incidence compared to the general population. MAP often includes multiple dimensions of cognitive impairment and induces adverse consequences such as, violence and suicide. However, the assessment methods for MAP are not standardized. Hence, it is necessary to investigate factors that affect the progression of psychiatric symptoms in individuals who use MA. A review of published studies was performed by searching the following databases: PubMed, EMBASE, and PsycINFO from inception to 31 May, 2018. The search strategy included methamphetamine, dependence, psychiatric symptoms, and risk factor terms. We reviewed the different features of MAP and the various types of assessment instruments and summarized MAP risk factors from MA use-related factors, socio-demographic characteristics, life events, and genetic factors. We found that MAP was consistently and causally associated with MA use, particularly as it relates to the frequency and amount of MA use. Other MAP-related risk factors like life events and genetics were relatively inconsistent in their association with MAP. Hence, causal and longitudinal studies that focus on multilateral comparisons are required. This review provides high quality evidence for MAP risk factors and would be helpful for developing early prevention and treatment strategies for MAP.
Methamphetamine (MA) is a potent and addictive synthetic central nervous system stimulant. MA production and supply appears to be on the rise, particularly in East and South-East Asia 1. Based on the World Drug Report in 2018, around 34 million people are reported to be using an Amphetamine Type Stimulant (ATS) worldwide (1). Illegal MA use frequently leads to harmful physical and potentially debilitating mental health consequences (1, 2). Methamphetamine-related psychiatric symptoms (MAP) are the most common adverse consequences among MA users, with recent estimates of up to ~40% of MA users affected (3). The prevalence of psychiatric symptoms among MA users is 11 times higher compared to the general population (4). Several studies have reported that the prevalence of MAP in cohorts of MA abusers ranged between 15 and 23% in recreational or community settings, and up to 60% in MA addicts in treatment settings (5–8). MAP can exacerbate distress among individuals using MA and contribute to significant burden on health care services (9, 10). However, the risk factors for MAP beyond MA use are unknown with no effective indicators for early MAP warning.
MAP consists of transient psychiatric symptoms, persistent psychiatric syndromes, and long-lasting substance-induced psychiatric disorders (11). The transient MAP symptoms always manifest among people who use MA and gradually relieve after stopping using MA, last hours to months, and mainly include hallucinations and persecutory delusions (4, 12, 13). In contrast, persisting psychiatric symptoms generally involve irritability, anxiety, and depression (12). Compared to MA-associated psychosis symptoms which are acute, long-lasting MAP leads to a greater burden for individuals, family members, and even society (11, 14). In addition, MAP results in progressive social and occupational deterioration (15, 16), with several adverse effects including violence (17) and suicide (18). The likelihood of experiencing MAP is associated with a larger or higher frequency of MA dose (19, 20) and other MA-related factors. In co-morbidity psychiatric disorders, concurrent use of alcohol or other drugs and family history have also been associated with MAP risk (11). It is critical to understand to what extent MAP is attributable to MA use and identify additional risk factors for MAP. We reviewed comprehensively all MAP-related studies, particularly for studies that had persistent MAP. We then subsequently reviewed MAP related assessment and risk factors (based on classification, including: pharmacological, genetic, and environmental factors). We aimed to incorporate the latest reports and reviews in the field to provide high quality evidence for MAP risk factors.
An extensive literature search was performed using PubMed, EMBASE, and PsycINFO databases from inception to 31 May, 2018. The search strategy included methamphetamine, psychiatric symptoms, and risk factors terms. Detailed search terms for methamphetamine include “MA dependence” or “amphetamine dependence,” and search terms for psychiatric symptoms contained “drug induced psychiatric symptoms,” “substance induced psychiatric symptoms,” and “psychiatric disorder,” and search terms for risk factors included “risk factors” and “vulnerability factors.”
To be considered for inclusion in this review, studies were required to have the following criteria:(1) human clinical study; (2) adults (>17 years) study; (3) studies where individuals using MA with current or lifetime MAP and were compared to those using MA without psychiatric symptoms; (4) MA was the primary drug; (5) studies which focus on MAP-related risk factors and describe the results clearly.
We read the title and abstract of the papers for the initial screening. Then we did the second screening after reading the full text. Finally, we included the studies according to the inclusion criteria and extracted information from them. Two researchers independently completed the literature screening process. Any disagreements about study inclusion were resolved by discussion.
A total of 17 papers met the inclusion criteria and their characteristics were summarized in Table 1, which were sorted into four categories of MAP-related risk factors: MA use-related factors (10 studies), socio-demographic variables (10 studies), Life events(2 studies), Psychiatric co-morbidity(4 studies), and genetic factors (2 studies). Among them, there are 10 studies that focused on more than one category of risk factors.
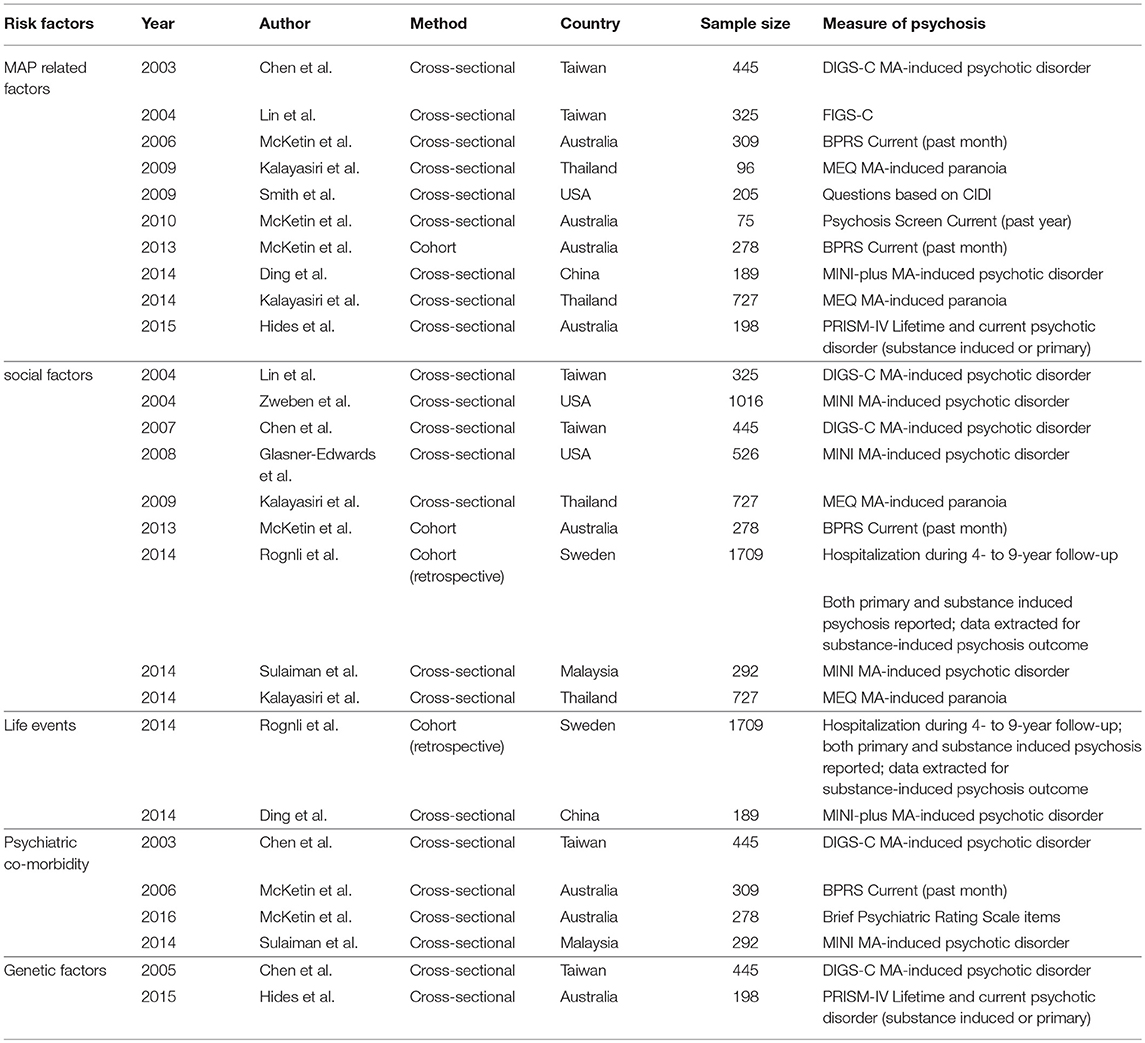
Table 1. Studies identifying risk factors for methamphetamine-related psychiatric symptoms.
Studies on MAP are sparse. They are mainly from existing data gathered from community hospitals or other research centers. Assessment of MAP is primarily based on clinician judgment. In targeted studies, investigators usually select appropriate research tools to assess certain type or types of mental disorders or symptoms and specific risk factors for which they are interested. Positive and Negative Syndrome Scale (PANSS) is used to assess MAP when clinical manifestations of MAP, especially transient MAP, are similar to schizophrenia (21–23). Beck Depression Inventory (BDI) is used to assess specific depression symptoms (24–26). Additionally, there are several other assessments used in MAP research, including the Beck Anxiety Inventory (BAI) (27, 28), Hamilton Depression Rating Scale (HDRS) (29, 30), and other scales (31–33). There is inconsistency in MAP definition when several assessments are compared (34–36). For example, the Mini International Neuropsychiatric Interview (MINI) could be used to assess lifetime MAP (16, 37, 38), while the list of psychiatric symptoms (Symptom Checklist 90, SCL-90) (39–41) could be used to assess recent MAP.
Earlier onset and longer duration (42, 43) are associated with increased risk of long-lasting MAP. Studies that associated these risk factors with MAP used lifetime measures of psychiatric disorders or symptoms (19, 44, 45). The severity of sustained MAP apparently related to earlier and longer exposure to MA, which reflects a “threshold” effect of stimulant use on the development of psychiatric symptoms (46).
Higher frequency and larger doses of MA use are closely associated with lifetime MAP (19, 20, 47). In a longitudinal prospective cohort study there was a five-fold increase in the likelihood of psychiatric symptoms during periods of MA use compared to sober periods (2). Frequent MA use had a relatively higher risk for longer-lasting MAP (44, 45, 48). Similarly, a higher dose of MA correlated with greater lifetime substance-induced psychotic disorders (19, 37) and psychiatric symptoms (19, 45, 49). These studies illustrate the dose-dependence relationship between MA use and the occurrence of psychiatric symptoms during periods of MA use (2, 50).
However, these relationships do not completely relate to all MA users. For example, there are certain subsets of individuals who do not appear to develop psychiatric symptoms with frequent MA use, while others suffer from chronic psychosis with limited exposure to the drug (51, 52).
Severity of MA dependence is closely associated with MAP. However, we found that the association was not consistent for all the studies evaluated. It is estimated that MA-dependent individuals were 2–3 times more likely to develop acute MAP symptoms compared to non-dependent individuals (19, 45, 53, 54). Nakama et al. found that the craving degree for MA use was correlated with the occurrence of persistent MAP (55). However, Hides et al. found that the severity of MA dependence was not associated with the risk of psychosis (6).
There are several routes of MA administration, including intravenous injection and snorting. Individuals who use MA intravenously are more likely to develop persistent MAP (47, 56). However, some studies did not find any relationship between route of MA administration and MAP. Of these studies, there was one study that investigated recreational drug use and found a comparatively low rate of injecting use (57). Two of the studies reported current psychiatric symptoms (4, 57), with one reporting hospitalization for substance-induced psychiatric disorder (58) and the other describing lifetime substance-induced psychiatric disorder (37). In summary, additional studies should be conducted to validate the relationship between MAP and the route of MA administration.
Concurrent use of other non-stimulant drugs and alcohol is associated with an increased risk of persistent MAP (19, 59, 60), especially cannabis and alcohol use or dependence (2, 19, 45, 61). Ketamine may exacerbate persisting psychiatric symptoms of MA users, like anxiety or depression and anergia symptoms (62). To date, there is no agreement regarding the association between a lifetime history of other drug use and MAP. This may be due to ethnic differences or religion. There was one study conducted on cohorts from inpatient psychiatric and rehabilitation centers in a Muslim country (where consumption of alcohol is prohibited) and found that alcohol dependence was not associated with lifetime and current MAP (37).
We found that several socio-demographic events had a correlation with MAP. However, certain controversies regarding the gender divergence of MAP has been noted. Several studies found that men were more prone to both transient and lifetime MAP (63–65), however other studies have demonstrated that transient MAP for both genders were similar (66–68). Regarding the age of onset, we found that young people with MA dependence were more vulnerable to acute and chronic MAP56 (69). Compared to non-MAP patients, patients with lifetime MAP were more likely to be single (65), unemployed (65), less educated (54, 65), and homeless (56, 58). Additional studies validating these findings need to be conducted.
MA users with worse life experiences are likely to suffer from MAP, however there are inconsistencies with these findings. Studies have found that sexual abuse and risky sexual behaviors (56) of MA users are associated with developing persistent MAP (56), however several other studies have not found any association (58). One study investigated the impact of adverse childhood experiences (ACEs) on the development of transient MAP and found that individuals with three or more ACEs had a strikingly higher risk of MAP lifetime risk (44). One study documented that pre-morbid schizoid/schizotypal personality predisposes MA users to develop lifetime MAP (19). Several studies have supported the positive correlation of lifetime and current MAP and the diagnosis of antisocial personality and other behavior disorders (37, 45, 70).
There are inconsistencies regarding the association between concurrent psychosis and MAP. Pre-existing psychiatric symptoms in MA users are difficult to identify. Factors associated with susceptibility to schizophrenia appear to similarly predict MAP. McKetin et al. evaluated co-morbid affective and anxiety disorders among dependent methamphetamine users and found both transient and persistent psychiatric symptoms were associated with co-morbidity anxiety disorders and major depression (63). Additionally, MA users with a history of psychotic disorders (schizophrenia, schizoaffective, or bipolar disorder) were more likely to develop acute psychiatric symptoms (57, 65). Patients with severe symptoms of attention deficit hyperactivity disorder (ADHD) were more susceptible to transient MAP after agreeing to MA treatment (71), and MAP was more severe in patients with ADHD who underwent treatment that were previously consuming higher doses of MA (52).
Genetic and family factors also contribute to MAP. The MA users whose family members have a history of psychosis have a higher susceptibility to MAP. Relatives of persistent MAP patients had a higher risk of suffering from schizophrenia compared to relatives of transient MAP patients (72). Moreover, the degree of familial loading for schizophrenia could predict the onset and duration of MA psychosis (3). Several studies have demonstrated that first-degree relatives of individuals with MA psychosis were five times more likely to be schizophrenic (19, 72). McKetin et al. demonstrated that a family history of schizophrenia was associated with persistent MAP in MA users (70).
Currently, several classic substance dependence or psychiatric-related genes associated with MAP have been reported. Variations in GRIN1 have been identified as a risk factor for schizophrenia and drug dependence, supporting the hypotheses of glutamatergic dysfunction in these disorders. The genetic variation of GRIN1 provides a good example for the genetic association with MA dependence and its resultant psychosis (73). Ezaki et al. found that 5-HTTLPR polymorphism were significantly associated with MAP, particularly among patients with prolonged MAP (74). In addition, polymorphisms in DTNBP1 (75), SOD2 (76), COMT (77, 78) may be associated with psychiatric disorders or symptoms caused by MA. A recent MAP GWAS analysis of Japanese cohorts appears to provide evidence that MAP shares genetic risk with schizophrenia, whereas no significant genome-wide SNP has been found (79).
We found that MAP was significantly associated with MA-related use factors, especially with the frequency and amount of MA use. Combined with the use of other addictive drugs, particularly novel synthetic drugs, like ketamine, may sharply increase the risk of MAP development. Although the number of studies regarding the association of life events and MAP were sparse, there was concordance with regards to adverse life events and MAP exacerbation. Substance dependence-related psychosis and psychiatric symptoms may usually affected by polygenic and genetic–environmental interactions. We did not cover all of these MAP risk factors. Other biological factors, such as serum brain-derived neurotrophic factor levels ≤ 1,251.0 pg/ml (24), disordered plasma immune factors (80), and HIV infection (81) of MA users have also been reported to be associated with MAP.
This review mainly focused on MAP rather than MA-associated psychosis that mostly represents acute symptoms. Although numerous studies and reviews have reported risk factors associating with MAP (3, 14, 82), several inconsistencies regarding these risk factors have made it difficult to conclusively determine their importance. The latest systematic review by Arunogiri et al. summarized the risk factors for methamphetamine associated psychosis from socio-demographic variables, methamphetamine use variables, other substance use, and family history (14), while other studies roughly described potential related risk factors (3, 82). Our review comprehensively outlines the risk factors for long-lasting psychiatric symptoms. In addition, to better understand MAP, we devoted greater attention to assessing MAP. The definition of MAP in this review is more extensive compared to simply defining it as psychosis. The risk factors we focused on were more comprehensive, and included genetic factors and ADHD.
However, these risk factors do not completely apply to all MA users. In addition to small or poorly representative sample cohorts, several confounding factors would affect the consistency of these findings. Firstly, poly-drug use is a common problem. The combined use of different drugs, like ketamine and cannabis, cause persistent psychiatric symptoms (62, 83), or cause transient intoxication states when cocaine is used (59). Secondly, only self-reported information from addicts was sometimes obtained. These reports do not help determine whether these addicts have MA exposure or not, or may not include other psychoactive substances including new (novel) synthetic drugs. In addition, most of the studies are cross-sectional, and the causal and prospective effects of MA use and pre-existing psychiatric symptoms could not be assessed. Hence these findings are not suitable for testing causality and predictive ability. In addition, the detrimental effects of MA use would be affected by purity and content of the drug itself. In addition, MAP assessments would be affected by recall or selection bias.
Psychosocial treatment for MA dependence is strongly evidence based and is the optimal first-line treatment strategy to reduce psychiatric symptoms in MA patients (3, 84). In addition, Cognitive-Behavioral Treatment (CBT) may be used to target multiple psychiatric disorders and symptoms, and emerging evidence supports the use of CBT to treat psychiatric symptoms associated with schizophrenia (85). For the treatment of acute MAP, guidance for clinical practice can be obtained from case studies. Numerous studies have reported the efficacy of antipsychotics including risperidone and aripiprazole for the management of acute MA-induced psychiatric symptoms (86). The treatment for long-lasting substance-induced psychiatric disorders should focus on MA abstinence to prevent future episodes of psychosis (3).
Early intervention can prevent MA users from progressing to disabling diseases like MA addiction and MAP (87). Future MAP-related studies should include individuals from community and treatment centers with a wide range of MA use histories to achieve more accurate and reliable study outcomes. Longitudinal, high-quality, and integrated studies which focus on risk factors for transient and long-lasting MAP are required. In addition, these studies should pay more attention to control confounding factors that affect the reliability of study findings.
JS, LL, and YS conceptualized and organized the review study. XC, YZ, and JM performed the online study search and analysis. XC and YS wrote the manuscript. All authors edited and accepted the final version of the manuscript.
This work was supported by the National Basic Research Program of China (No. 2015CB553503), the National Natural Science Foundation of China (No. U1402226, 81521063, 81601165, 31571099), the National Key Research and Development Program of China (No. 2017YFC0803608 and No. 2017YFC0803609). Beijing Municipal Science & Technology Commission (Z181100001518005 and Z161100002616006). And we appreciatively thank YS for helping us to proofread the language of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
2. McKetin R, Lubman DI, Baker AL, Dawe S, Ali RL. Dose-related psychotic symptoms in chronic methamphetamine users: evidence from a prospective longitudinal study. JAMA Psychiatry (2013) 70:319–24. doi: 10.1001/jamapsychiatry.2013.283
3. Glasner-Edwards S, Mooney LJ. Methamphetamine psychosis: epidemiology and management. CNS Drugs (2014) 28:1115–26. doi: 10.1007/s40263-014-0209-8
4. McKetin R, McLaren J, Lubman DI, Hides L. The prevalence of psychotic symptoms among methamphetamine users. Addiction (2006) 101:1473–8. doi: 10.1111/j.1360-0443.2006.01496.x
5. Arunogiri S, Petrie M, Sharkey M, Lubman DI. Key differences in treatment-seeking stimulant users attending a specialised treatment service: a means of early intervention? Australas Psychiatry (2017) 25:246–9. doi: 10.1177/1039856216684737
6. Hides L, Dawe S, McKetin R, Kavanagh DJ, Young RM, Teesson M, et al. Primary and substance-induced psychotic disorders in methamphetamine users. Psychiatry Res. (2015) 226:91–6. doi: 10.1016/j.psychres.2014.11.077
7. Lapworth K, Dawe S, Davis P, Kavanagh D, Young R, Saunders J. Impulsivity and positive psychotic symptoms influence hostility in methamphetamine users. Addict Behav. (2009) 34:380–5. doi: 10.1016/j.addbeh.2008.11.014
8. Schuckit MA. Comorbidity between substance use disorders and psychiatric conditions. Addiction (2006) 101:76–88. doi: 10.1111/j.1360-0443.2006.01592.x
9. Arunogiri S, Gao CX, Lloyd B, Smith K, Lubman DI. The role of methamphetamines in psychosis-related ambulance presentations. Aust N Z J Psychiatry (2015) 49:939–40. doi: 10.1177/0004867415585323
10. McKetin R, Degenhardt L, Shanahan M, Baker AL, Lee NK, Lubman DI. Health service utilisation attributable to methamphetamine use in Australia: patterns, predictors and national impact. Drug Alcohol Rev. (2018) 37:196–204. doi: 10.1111/dar.12518
11. Bramness JG, Rognli EB. Psychosis induced by amphetamines. Curr Opin psychiatry (2016) 29:236–41. doi: 10.1097/yco.0000000000000254
12. Zweben JE, Cohen JB, Christian D, Galloway GP, Salinardi M, Parent D, et al. Psychiatric symptoms in methamphetamine users. Am J Addict. (2004) 13:181–90. doi: 10.1080/10550490490436055
13. Harris DSLB. Stimulant psychosis: symptom profile and acute clinical course. (2000) Am J Addict. 9:28–37. doi: 10.1080/10550490050172209
14. Arunogiri S, Foulds JA, McKetin R, Lubman DI. A systematic review of risk factors for methamphetamine-associated psychosis. Aust N Z J Psychiatry (2018) 52:514–29. doi: 10.1177/0004867417748750
15. Glasner-Edwards S, Mooney LJ, Marinelli-Casey P, Hillhouse M, Ang A, Rawson R, et al. Clinical course and outcomes of methamphetamine-dependent adults with psychosis. J Subst Abuse Treat. (2008) 35:445–50. doi: 10.1016/j.jsat.2007.12.004
16. Glasner-Edwards S, Mooney LJ, Marinelli-Casey P, Hillhouse M, Ang A, Rawson RA. Psychopathology in methamphetamine-dependent adults 3 years after treatment. Drug Alcohol Rev. (2010) 29:12–20. doi: 10.1111/j.1465-3362.2009.00081.x
17. Khalkhali SMR, Najafi K, Ahmadi R, Yousefnezhad A, Hamidi A, Ellahi M, et al. Domestic violence in methamphetamine psychotic users, psychiatric inpatients, and healthy people: a comparative study. Iran J Med Sci. (2016) 41:486–93.
18. Kuo CJ, Tsai SY, Liao YT, Conwell Y, Lin SK, Chang CL, et al. Risk and protective factors for suicide among patients with methamphetamine dependence: a nested case-control study. J Clin Psychiatry (2011) 72:487–93. doi: 10.4088/JCP.09m05360gry
19. Chen CK, Lin SK, Sham PC, Ball D, Loh EW, Hsiao CC, et al. Pre-morbid characteristics and co-morbidity of methamphetamine users with and without psychosis. Psychol Med. (2003) 33:1407–14. doi: 10.1017/S0033291703008353
20. Matsumoto T, Kamijo A, Miyakawa T, Endo K, Yabana T, Kishimoto H, et al. Methamphetamine in Japan: the consequences of methamphetamine abuse as a function of route of administration. Addiction (2002) 97:809–17. doi: 10.1046/j.1360-0443.2002.00143.x
21. Alexander PD, Gicas KM, Willi TS, Kim CN, Boyeva V, Procyshyn RM, et al. A comparison of psychotic symptoms in subjects with methamphetamine versus cocaine dependence. Psychopharmacology (2017) 234:1535–47. doi: 10.1007/s00213-017-4551-7
22. Hajebi A, Amini H, Kashani L, Sharifi V. Twelve-month course and outcome of methamphetamine-induced psychosis compared with first episode primary psychotic disorders. Early Interv Psychiatry (2016) 12:928–34. doi: 10.1111/eip.12404
23. Medhus S, Mordal J, Holm B, Morland J, Bramness JG. A comparison of symptoms and drug use between patients with methamphetamine associated psychoses and patients diagnosed with schizophrenia in two acute psychiatric wards. Psychiatry Res. (2013) 206:17–21. doi: 10.1016/j.psychres.2012.09.023
24. Ren WW, Luan XQ, Zhang J, Gutteea P, Cai Y, Zhao JY, et al. Brain-derived neurotrophic factor levels and depression during methamphetamine withdrawal. J Affect Disord. (2017) 221:165–71. doi: 10.1016/j.jad.2017.06.017
25. Reback CJ, Kamien JB, Amass L. Characteristics and HIV risk behaviors of homeless, substance-using men who have sex with men. Addictive Behav. (2007) 32:647–54. doi: 10.1016/j.addbeh.2006.06.008
26. Dyer KR, Cruickshank CC. Depression and other psychological health problems among methamphetamine dependent patients in treatment: implications for assessment and treatment outcome. Aust Psychol. (2005) 40:96–108. doi: 10.1080/00050060500094647
27. Zhang J, Su H, Tao JY, Xie Y, Sun YM, Li LR, et al. Relationship of impulsivity and depression during early methamphetamine withdrawal in Han Chinese population. Addictive Behav. (2015) 43:7–10. doi: 10.1016/j.addbeh.2014.10.032
28. Hartwell EE, Moallem NR, Courtney KE, Glasner-Edwards S, Ray LA. Sex Differences in the association between internalizing symptoms and craving in methamphetamine users. J Addict Med. (2016) 10:395–401. doi: 10.1097/Adm.0000000000000250
29. Eslami-Shahrbabaki M, Fekrat A, Mazhari S. A Study of the prevalence of psychiatric disorders in patients with methamphetamine-induced psychosis. Addict Health (2015) 7:37–46.
30. Landabaso MA, Iraurgi I, Jimenez-Lerma JM, Calle R, Sanz J, Gutierrez-Fraile M. Ecstasy-induced psychotic disorder: six-month follow-up study. Eur Addict Res. (2002) 8:133–40. doi: 10.1159/000059383
31. McKetin R, McLaren J, Lubman DI, Hides L. Hostility among methamphetamine users experiencing psychotic symptoms. Am J Addict. (2008) 17:235–40. doi: 10.1080/10550490802019816
32. Akiyama K. Longitudinal clinical course following pharmacological treatment of methamphetamine psychosis which persists after long-term abstinence. Ann N Y Acad Sci. (2006) 1074:125–34. doi: 10.1196/annals.1369.012
33. Sekine Y, Minabe Y, Ouchi Y, Takei N, Iyo M, Nakamura K, et al. Association of dopamine transporter loss in the orbitofrontal and dorsolateral prefrontal cortices with methamphetamine-related psychiatric symptoms. Am J Psychiatry (2003) 160:1699–701. doi: 10.1176/appi.ajp.160.9.1699
34. Gunter TD, Black DW, Zwick J, Arndt S. Drug and alcohol treatment services effective for methamphetamine abuse. Ann Clin Psychiatry (2004) 16:195–200. doi: 10.1080/10401230490522007
35. Srisurapanont M, Ali R, Marsden J, Sunga A, Wada K, Monteiro M. Psychotic symptoms in methamphetamine psychotic in-patients. Int J Neuropsychopharmacol. (2003) 6:347–52. doi: 10.1017/s1461145703003675
36. Singer LT, Linares TJ, Ntiri S, Henry R, Minnes S. Psychosocial profiles of older adolescent MDMA users. Drug Alcohol Depend. (2004) 74:245–52. doi: 10.1016/j.drugalcdep.2003.12.015
37. Sulaiman AH, Said MA, Habil MH, Rashid R, Siddiq A, Guan NC, et al. The risk and associated factors of methamphetamine psychosis in methamphetamine-dependent patients in Malaysia. Compr Psychiatry (2014) 55:S89–94. doi: 10.1016/j.comppsych.2013.01.003
38. Kittirattanapaiboon P, Mahatnirunkul S, Booncharoen H, Thummawomg P, Dumrongchai U, Chutha W. Long-term outcomes in methamphetamine psychosis patients after first hospitalisation. Drug Alcohol Rev. (2010) 29:456–61. doi: 10.1111/j.1465-3362.2010.00196.x
39. Zhang Y, Zhong BL, Li Y, Ma ZL, Tian Y. Brain event-related potentials associated with psychiatric symptoms in amphetamine-type stimulant dependent patients. Int J Psychiat Med. (2012) 43:189–96. doi: 10.2190/PM.43.2.g
40. King G, Alicata D, Cloak C, Chang L. Psychiatric symptoms and HPA axis function in adolescent methamphetamine users. J Neuroimmune Pharmacol. (2010) 5:582–91. doi: 10.1007/s11481-010-9206-y
41. Parrott AC, Milani RM, Parmar R, Turner JD. Recreational ecstasy/MDMA and other drug users from the UK and Italy: psychiatric symptoms and psychobiological problems. Psychopharmacology (2001) 159:77–82. doi: 10.1007/s002130100897
42. Lecomte T, Mueser KT, MacEwan W, Thornton AE, Buchanan T, Bouchard V, et al. Predictors of persistent psychotic symptoms in persons with methamphetamine abuse receiving psychiatric treatment. J Nerv Ment Dis. (2013) 201:1085–9. doi: 10.1097/nmd.0000000000000059
43. Sekine Y, Iyo M, Ouchi Y, Matsunaga T, Tsukada H, Okada H, et al. Methamphetamine-related psychiatric symptoms and reduced brain dopamine transporters studied with PET. Am J Psychiatry (2001) 158:1206–14. doi: 10.1176/appi.ajp.158.8.1206
44. Ding Y, Lin H, Zhou L, Yan H, He N. Adverse childhood experiences and interaction with methamphetamine use frequency in the risk of methamphetamine-associated psychosis. Drug Alcohol Depend. (2014) 142:295–300. doi: 10.1016/j.drugalcdep.2014.06.042
45. Kalayasiri R, Mutirangura A, Verachai V, Gelernter J, Malison RT. Risk factors for methamphetamine-induced paranoia and latency of symptom onset in a Thai drug treatment cohort. Asian Biomed. (2009) 3:635–43.
46. Lichlyter B, Purdon S, Tibbo P. Predictors of psychosis severity in individuals with primary stimulant addictions. Addictive Behav. (2011) 36:137–9. doi: 10.1016/j.addbeh.2010.08.019
47. Grant KM, Kelley SS, Agrawal S, Meza JL, Meyer JR, Romberger DJ. Methamphetamine use in rural midwesterners. Am J Addict. (2007) 16:79–84. doi: 10.1080/10550490601184159
48. Hall W, Hando J, Darke S, Ross J. Psychological morbidity and route of administration among amphetamine users in Sydney, Australia. Addiction (1996) 91:81–7.
49. Du J, Sun H, Huang D, Jiang H, Zhong N, Xu D, et al. Use trajectories of amphetamine-type stimulants (ATS) in Shanghai, China. Drug Alcohol Depend. (2014) 143:44–50. doi: 10.1016/j.drugalcdep.2014.06.031
50. Willi TS, Honer WG, Thornton AE, Gicas K, Procyshyn RM, Vila-Rodriguez F, et al. Factors affecting severity of positive and negative symptoms of psychosis in a polysubstance using population with psychostimulant dependence. Psychiatry Res. (2016) 240:336–42. doi: 10.1016/j.psychres.2016.04.059
51. Akiyama K, Saito A, Shimoda K. Chronic methamphetamine psychosis after long-term abstinence in Japanese incarcerated patients. Am J Addict. (2011) 20:240–9. doi: 10.1111/j.1521-0391.2011.00124.x
52. Salo R, Fassbender C, Iosif AM, Ursu S, Leamon MH, Carter C. Predictors of methamphetamine psychosis: history of ADHD-relevant childhood behaviors and drug exposure. Psychiatry Res. (2013) 210:529–35. doi: 10.1016/j.psychres.2013.06.030
53. Kalayasiri R, Verachai V, Gelernter J, Mutirangura A, Malison RT. Clinical features of methamphetamine-induced paranoia and preliminary genetic association with DBH-1021C. T in a Thai treatment cohort. Addiction (2014) 109:965–76. doi: 10.1111/add.12512
54. Lappin JM, Roxburgh A, Kaye S, Chalmers J, Sara G, Dobbins T, et al. Increased prevalence of self-reported psychotic illness predicted by crystal methamphetamine use: evidence from a high-risk population. Int J Drug Policy (2016) 38:16–20. doi: 10.1016/j.drugpo.2016.10.018
55. Nakama H, Chang L, Cloak C, Jiang C, Alicata D, Haning W. Association between psychiatric symptoms and craving in methamphetamine users. Am J Addict. (2008) 17:441–6. doi: 10.1080/10550490802268462
56. Semple SJ, Strathdee SA, Zians J, McQuaid J, Patterson TL. Psychosocial and behavioral correlates of anxiety symptoms in a sample of HIV-positive, methamphetamine-using men who have sex with men. AIDS care (2011) 23:628–37. doi: 10.1080/09540121.2010.525608
57. McKetin R, Hickey K, Devlin K, Lawrence K. The risk of psychotic symptoms associated with recreational methamphetamine use. Drug Alcohol Rev. (2010) 29:358–63. doi: 10.1111/j.1465-3362.2009.00160.x
58. Rognli EB, Hakansson A, Berge J, Bramness JG. Does the pattern of amphetamine use prior to incarceration predict later psychosis?–a longitudinal study of amphetamine users in the Swedish criminal justice system. Drug Alcohol Depend. (2014) 143:219–24. doi: 10.1016/j.drugalcdep.2014.07.037
59. Smith MJ, Thirthalli J, Abdallah AB, Murray RM, Cottler LB. Prevalence of psychotic symptoms in substance users: a comparison across substances. Compr Psychiatry (2009) 50:245–50. doi: 10.1016/j.comppsych.2008.07.009
60. Medina KL, Shear PK. Anxiety, depression, and behavioral symptoms of executive dysfunction in ecstasy users: contributions of polydrug use. Drug Alcohol Depend. (2007) 87:303–11. doi: 10.1016/j.drugalcdep.2006.09.003
61. Daumann J, Hensen G, Thimm B, Rezk M, Till B, Gouzoulis-Mayfrank E. Self-reported psychopathological symptoms in recreational ecstasy (MDMA) users are mainly associated with regular cannabis use: further evidence from a combined cross-sectional/longitudinal investigation. Psychopharmacology (2004) 173:398–404. doi: 10.1007/s00213-003-1719-0
62. Liu X, Zhang Y, Wang X, Hao W. The synergistic effect of dual use of amphetamine-type stimulants and ketamine on drug-induced psychotic symptoms in Chinese synthetic drug users. Oncotarget (2017) 8:66569–75. doi: 10.18632/oncotarget.16474
63. McKetin R, Gardner J, Baker AL, Dawe S, Ali R, Voce A, et al. Correlates of transient versus persistent psychotic symptoms among dependent methamphetamine users. Psychiatry Res. (2016) 238:166–71. doi: 10.1016/j.psychres.2016.02.038
64. Akindipe T, Wilson D, Stein DJ. Psychiatric disorders in individuals with methamphetamine dependence: prevalence and risk factors. Metab Brain Dis. (2014) 29:351–7. doi: 10.1007/s11011-014-9496-5
65. Farnia V, Shakeri J, Tatari F, Juibari TA, Bajoghli H, Golshani S, et al. Demographic and mental history-related data predicted occurrence of psychosis in metamphetamine users. Psychiatry Res. (2016) 240:431–4. doi: 10.1016/j.psychres.2016.04.053
66. Polcin DL, Buscemi R, Nayak M, Korcha R, Galloway G. Gender differences in psychiatric symptoms among methamphetamine dependent residents in sober living houses. Addict Disord Their Treat. (2012) 11:53–63. doi: 10.1097/ADT.0b013e3182213ef1
67. Mahoney JJ III, Hawkins RY, De La Garza R II, Kalechstein AD, Newton TF. Relationship between gender and psychotic symptoms in cocaine-dependent and methamphetamine-dependent participants. Gend Med. (2010) 7:414–21. doi: 10.1016/j.genm.2010.09.003
68. Yen CF, Su YC. The associations of early-onset methamphetamine use with psychiatric morbidity among Taiwanese adolescents. Subst Use Misuse (2006) 41:35–44. doi: 10.1080/10826080500318616
69. Cloutier RL, Hendrickson RG, Fu RR, Blake B. Methamphetamine-related psychiatric visits to an urban academic emergency department: an observational study. J Emerg Med. (2013) 45:136–42. doi: 10.1016/j.jemermed.2012.11.094
70. McKetin R, Dawe S, Burns RA, Hides L, Kavanagh DJ, Teesson M, et al. The profile of psychiatric symptoms exacerbated by methamphetamine use. Drug Alcohol Depend. (2016) 161:104–9. doi: 10.1016/j.drugalcdep.2016.01.018
71. Jaffe C, Bush KR, Straits-Troster K, Meredith C, Romwall L, Rosenbaum G, et al. A comparison of methamphetamine-dependent inpatients childhood attention deficit hyperactivity disorder symptomatology. J Addict Dis. (2005) 24:133–52. doi: 10.1300/J069v24n03_11
72. Chen CK, Lin SK, Sham PC, Ball D, Loh el W, Murray RM. Morbid risk for psychiatric disorder among the relatives of methamphetamine users with and without psychosis. Am J Med Genet B Neuropsychiatr Genet. (2005) 136B:87–91. doi: 10.1002/ajmg.b.30187
73. Chanasong R, Thanoi S, Watiktinkorn P, Reynolds GP, Nudmamud-Thanoi S. Genetic variation of GRIN1 confers vulnerability to methamphetamine-dependent psychosis in a Thai population. Neuroscience Lett. (2013) 551:58–61. doi: 10.1016/j.neulet.2013.07.017
74. Ezaki N, Nakamura K, Sekine Y, Thanseem I, Anitha A, Iwata Y, et al. Short allele of 5-HTTLPR as a risk factor for the development of psychosis in Japanese methamphetamine abusers. Ann N Y Acad Sci. (2008) 1139:49–56. doi: 10.1196/annals.1432.011
75. Kishimoto M, Ujike H, Motohashi Y, Tanaka Y, Okahisa Y, Kotaka T, et al. The dysbindin gene (DTNBP1) is associated with methamphetamine psychosis. Biol Psychiatry (2008)63:191–6. doi: 10.1016/j.biopsych.2007.03.019
76. Nakamura K, Chen CK, Sekine Y, Iwata Y, Anitha A, Loh el W, et al. Association analysis of SOD2 variants with methamphetamine psychosis in Japanese and Taiwanese populations. Hum Genet. (2006) 120:243–52. doi: 10.1007/s00439-006-0189-y
77. Hosak L, Sery O, Beranek M, Alda M. Lack of association between the Val158Met catechol-O-methyltransferase gene polymorphism and methamphetamine dependence. Neuro Endocrinol Lett. (2011) 32:469–74. doi: 10.1016/S0924-9338(12)74207-4
78. Suzuki A, Nakamura K, Sekine Y, Minabe Y, Takei N, Suzuki K, et al. An association study between catechol-O-methyl transferase gene polymorphism and methamphetamine psychotic disorder. Psychiatr Genet. (2006) 16:133–8. doi: 10.1097/01.ypg.0000218613.35139.cd
79. Ikeda M, Okahisa Y, Aleksic B, Won M, Kondo N, Naruse N, et al. Evidence for shared genetic risk between methamphetamine-induced psychosis and schizophrenia. Neuropsychopharmacology (2013) 38:1864–70. doi: 10.1038/npp.2013.94
80. Huckans M, Fuller BE, Chalker AL, Adams M, Loftis JM. Plasma inflammatory factors are associated with anxiety, depression, and cognitive problems in adults with and without methamphetamine dependence: an exploratory protein array study. Front Psychiatry (2015) 6:178. doi: 10.3389/fpsyt.2015.00178
81. Semple SJ, Strathdee SA, Zians J, Patterson TL. Mother-son relationship as a risk factor for depressive symptoms among methamphetamine users. J Subst Use (2012) 17:51–60. doi: 10.3109/14659891.2010.519420
82. Bramness JG, Gundersen OH, Guterstam J, Rognli EB, Konstenius M, Loberg EM, et al. Amphetamine-induced psychosis–a separate diagnostic entity or primary psychosis triggered in the vulnerable? BMC Psychiatry (2012) 12:221. doi: 10.1186/1471-244x-12-221
83. Murray RM, Paparelli A, Morrison PD, Marconi A, Di Forti M. What can we learn about schizophrenia from studying the human model, drug-induced psychosis? Am J Med Genet B Neuropsychiatr Genet. (2013) 162b:661–70. doi: 10.1002/ajmg.b.32177
84. Lee NK, Rawson RA. A systematic review of cognitive and behavioural therapies for methamphetamine dependence. Drug Alcohol Rev. (2008) 27:309–17. doi: 10.1080/09595230801919494
85. Burns AM, Erickson DH, Brenner CA. Cognitive-behavioral therapy for medication-resistant psychosis: a meta-analytic review. Psychiatr Serv. (2014) 65:874–80. doi: 10.1176/appi.ps.201300213
86. Wang G, Zhang Y, Zhang S, Chen H, Xu Z, Schottenfeld RS, et al. Aripiprazole and risperidone for treatment of methamphetamine-associated psychosis in chinese patients. J Subst Abuse Treat. (2016) 62:84–8. doi: 10.1016/j.jsat.2015.11.009
Keywords: methamphetamine (MA), methamphetamine-related psychiatric symptoms (MAP), assessment instruments, risk factors, methamphetamine use related factors, socio-demographic variables and life events, genetic factors
Citation: Chang XW, Sun Y, Zhang Y, Muhai JN, Lu L and Shi J (2018) A Review of Risk Factors for Methamphetamine-Related Psychiatric Symptoms. Front. Psychiatry 9:603. doi: 10.3389/fpsyt.2018.00603
Received: 02 July 2018; Accepted: 29 October 2018;
Published: 16 November 2018.
Edited by:
Julia M. Lappin, University of New South Wales, AustraliaReviewed by:
Mercedes Lovrecic, National Institute for Public Health, SloveniaCopyright © 2018 Chang, Sun, Zhang, Muhai, Lu and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jie Shi, c2hpamllQGJqbXUuZWR1LmNu
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.