 Antonella Granieri
Antonella Granieri Fanny Guglielmucci
Fanny Guglielmucci Antonino Costanzo2
Antonino Costanzo2 Adriano Schimmenti
Adriano Schimmenti- 1Department of Psychology, University of Turin, Turin, Italy
- 2Faculty of Human and Social Sciences, Kore University of Enna, Enna, Italy
- 3Department of Human Sciences, LUMSA University of Rome, Rome, Italy
Background: Extensive research has demonstrated the positive associations among the exposure to traumatic experiences, the levels of dissociation, and the severity of psychiatric symptoms in adults. However, it has been hypothesized in clinical literature that an excessive activation of the dissociative processes following multiple traumatic experiences may jeopardize the psychological and behavioral functioning of the individuals, fostering higher levels of maladaptive personality functioning.
Methods: The study involved 322 adult volunteers from Italy. Participants completed measures on traumatic experiences, dissociation, and maladaptive personality traits.
Results: The number of traumatic experiences reported by participants were positively associated with dissociation scores and maladaptive personality scores. Mediation analyses showed that dissociation acted as a partial mediator in the relationship between traumatic experiences and overall maladaptive personality functioning. Regression curve analyses showed that the positive association between maladaptive personality functioning and dissociation was stronger among participants with higher exposure to traumatic experiences.
Conclusion: Exposure to multiple traumatic experiences may increase the risk for an excessive activation of the dissociative processes, which in turn may generate severe impairments in multiple domains of personality functioning.
Introduction
Dissociation is a mental process already available in early stages of development, which allows an individual to tolerate distressing events by splitting off highly incoherent or overwhelming thoughts, memories, and feelings (1–7). The dissociative process could be conceptualized as a primary response to stress, which protects the mind from disorganization and feelings of fragmentation through a temporary selective exclusion of mental contents from consciousness and through multiple disconnections between mental states (3, 5, 8, 9).
However, when an individual is exposed to multiple traumatic experiences, and especially when such experiences started to occur during childhood—when a child has little capacity for self-regulation—dissociation may become a “psychological organizer” of the entire personality of the individual (5, 9–12). In these circumstances, the excessive activation of dissociative processes jeopardizes the mental and behavioral functioning of the individual so that dissociation becomes pathological and pervasive, and it may lead to severe psychiatric symptoms (5).
This conceptualization of dissociation as a protective function of the mind, which is, however, sensitive to the experiences of chronic traumatization to the point that it can even generate a functional reorganization of personality into distinct structures not fully integrated between them, has been widely endorsed in clinical literature (13–16) and is consistent with contemporary neurobiological findings, supporting the view that trauma is often linked to pathological dissociation (17–22).
Indeed, extensive research has reported a positive association between exposure to different types of trauma (e.g., emotional, physical, sexual) and the severity of dissociation (5, 23–26). Moreover, higher numbers of traumatic experiences in life seem to be associated with an increased risk for psychopathological conditions (5, 27–29).
Notably, exposure to multiple traumatic experiences has also been associated with less flexible, and more maladaptive, personality patterns (30–32), and longitudinal studies have shown a mediating role of personality features in the relationship between traumatic experiences and psychopathology (33, 34).
This study is part of a wider research program aimed at exploring the relationships among trauma, dissociation, and adult psychopathology. In previous research, we have described and empirically tested with positive results a conceptual model in which dissociation plays a mediating role between different types of traumatic experiences and psychopathology (5). A basic tenet of this model is that psychological trauma can be considered as a complex factor, in which different types of distressing experiences have different probability to co-occur and to generate an excessive activation of the dissociative process, with, however, higher numbers of distressing experiences being more likely related to excessive dissociation and psychopathology.
In fact, this model postulates that among the many contextual, social, and psychological variables that are associated with an increased risk for trauma exposure, the probability of experiencing a trauma is also related with the other traumata that occurred in an individual's life. Noteworthy, this particularly applies when trauma exposure starts in childhood. Just to make an example here: a child who loses a parent (trauma n. 1) will have an increased probability of being neglected (trauma n. 2) by the other parent (for example, because the living parent struggles to cope with his or her own depressive feelings, and/or because the death of his or her spouse generated financial problems in the family); being neglected at home, in turn, increases the probability that the child will be exposed to abuses (trauma n. 3) outside the family (e.g., being bullied at school), because he or she lacks a loving and protective figure who can help him or her to adequately cope with difficulties and problems. It is rather clear that this sequence of consecutive exposure to multiple traumatic experiences can continue. However, what is critical here is that the psychological and behavioral functioning of this child will be intensely affected by such negative experiences, to the point that his or her development will be deviated toward atypical trajectories, involving the development of maladaptive personality features.
Therefore, in the present study we hypothesized that the mediating role of dissociation already observed in the relationship between trauma and adult symptomatology (5) can also be observed in the relationship between trauma and maladaptive personality functioning.
Materials and Methods
Participants
The study involved 322 adult volunteers (111 males, 34.4%; 221 females, 65.6%) from Sicily (Italy). Participants ranged in age from 18 to 64 years old (M = 33.48; SD = 13.53), and showed an average level of education of 15.45 years (SD = 3.50). One hundred forty-three of them (44.4%) were in a marital relationship, while the others were either single, divorced, or widowed. There were no gender differences in relation to age of participants [t(320) = 0.35, p = 0.73], their years of education [t(320) = 0.69, p = 0.49], and their marital status [ = 1.23, p = 0.27].
Procedures
Participants were recruited in Sicily (Italy) through public and electronic advertisements (flyers in public places and posts in social network pages). People who contacted the research office via e-mail or by phone were asked to participate in a study on personality and its features in relation to life events, and those who expressed their potential willingness to participate (N = 407) were sent an anonymous electronic link that allowed them to take part in the study. Inclusion criteria were as follows: (1) age between 18 and 65 years; (2) native or fluent Italian speaker; (3) no current diagnosis of severe psychiatric disorders (such as psychotic disorders, bipolar disorders, dementia); (4) not being in treatment with psychotropic medication within the past 3 months. Three hundred and twenty-two participants met the inclusion criteria and signed the informed consent. They were administered measures for the assessment of traumatic experiences, dissociation, and maladaptive personality. The study obtained ethical permission from the last author's university Internal Review Board for psychological research. Participants did not receive any compensation for their involvement in the study.
Measures
The Traumatic Experiences Checklist (TEC) (35) is a self-report measure addressing 29 types of potentially traumatic events (e.g., “Loss of a family member when you were a child”). It is used in both clinical practice and research and has been validated in many countries, including Italy, with the Italian translation showing adequate reliability and validity even at the item level (5). Different scores can be calculated on the TEC. Consistent with previous research (36), in this study we used the cumulative score of the TEC as an index of total trauma. The KR-20 index of TEC scores in this study was 0.57.
The Dissociative Experiences Scale–II (DES-II) (37) is a 28-item self-report measure of dissociative experiences (e.g., experiences of absorption, emotional detachment, amnesia, depersonalization, derealization, identity confusion, and compartmentalization). The subject is asked to circle the number to show what percentage of the time he or she experiences these symptoms (e.g., “Some people have the experience of looking in a mirror and not recognizing themselves. Circle the number to show what percentage of the time this happens to you”). The overall score ranges from 0 to 100% and is the average score obtained by adding up the 28 item scores and dividing by 28. International research shows that the psychometric properties of the DES-II are excellent (38), and the Italian translation of the DES-II similarly showed high internal consistency, adequate item-to-scale homogeneity, good split-half reliability, and good convergent validity (3). In this study, Cronbach's alpha of the DES-II was 0.94.
The Personality Inventory for DSM-5-Brief Form-Adult (PID-5-BF) (39) is a 25-item self-report measure assessing five maladaptive personality-trait domains (i.e., negative affectivity, detachment, antagonism, disinhibition, and psychoticism) according to the alternative DSM-5 model for personality disorders (40). Measures range from 0 to 75, with higher scores indicating greater overall personality dysfunction. Each trait domain includes five items and ranges from 0 to 15, with higher scores indicating greater dysfunction in the specific personality-trait domain. The PID-5-BF has been validated in many countries, including Italy (41), with positive results. In the present study, Cronbach's alpha for the PID-5-BF total score was 0.86, whereas Cronbach's alpha for the PID-5-BF domains were 0.63 (Negative affectivity), 0.66 (Detachment), 0.77 (Antagonism), 0.66 (Disinhibition), 0.73 (Psychoticism).
Statistical Analysis
Descriptive statistics were calculated for all the investigated variables. An independent sample t-test was used to examine gender differences. Pearson's r correlations were used to examine potential associations among traumatic experiences, dissociation, and maladaptive personality domains. Mediation analyses testing whether dissociation mediated between the number of traumatic experiences and maladaptive personality domains were performed using the Process Macro for SPSS (42), applying Model 4 with 5,000 bias-corrected bootstrap samples and controlling for gender, age, years of education, and marital status of participants. Finally, participants' scores on the TEC were split at the 50th percentile to obtain two subgroups with low and high levels of traumatic experiences, respectively. We tested whether regression curves for global maladaptive personality scores as a function of dissociation scores fit differently with respect to these two subgroups.
Results
Descriptive statistics are presented in Table 1, for the full sample and differentiated by gender, along with levels of significance for gender differences. Males reported higher scores in the PID-5-BF antagonistic domain (p = 0.001), whereas females reported higher scores in the PID-5-BF negative affectivity domain (p < 0.001). No other gender differences were observed in the sample.
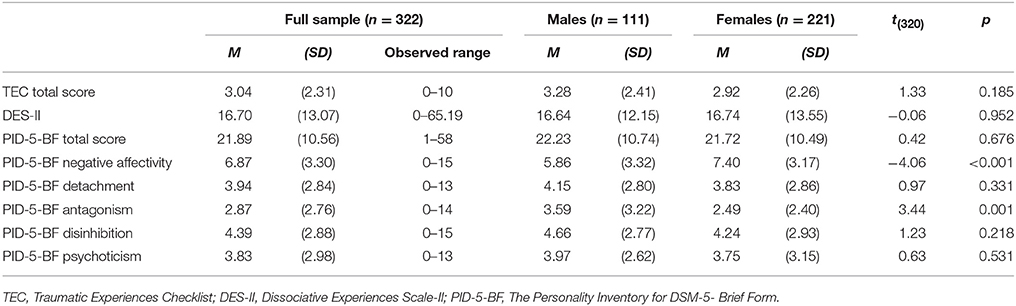
Table 1. Descriptive statistics and gender differences.
We also examined the prevalence of traumatic experiences reported in the sample. Only 32 participants (9.9%) did not report any exposure to traumatic experiences in their life. However, the number of traumatic experiences among participants in this sample was low, with most participants reporting 1 (n = 65, 20.2%), 2 (n = 66, 20.5%), or 3 (n = 45, 14.0%) traumata. The most frequent traumatic experiences occurring in the sample were parentification (i.e., looking after parents and/or brothers and sisters during childhood; n = 108, 33.5%) and intense pain (e.g., due to an injury or a surgery, n = 106, 32.9%), the less frequent were war experiences (n = 1, 0.3%) and sexual harassment/abuse by family members (n = 1, 0.3%). Considering the experiences of abuse, 99 participants (30.7%) reported emotional abuse, 40 participants (12.4%) reported physical abuse, and 20 participants (6.2%) reported sexual abuse. Data concerning the age at which the first trauma was experienced was available for 274 participants (because responses such as “during my entire childhood,” “during adolescence,” “it started some years ago,” “as long as I can remember,” “I cannot exactly remember how old I was,” and the like, were excluded from this analysis). Among these participants, mean age of first trauma was 14.17 years (SD = 10.87), ranging from 0 (a life-saving surgery immediately after birth) to 55 years old.
Subsequently, the patterns of associations among TEC scores, DES-II scores, and PID-5-BF total and domain scores were examined. The results of this analysis are presented in Table 2. TEC scores were modestly but significantly and positively associated with DES-II and PID-5-BF scores, whereas the positive correlations between DES-II and PID-5-BF were stronger.
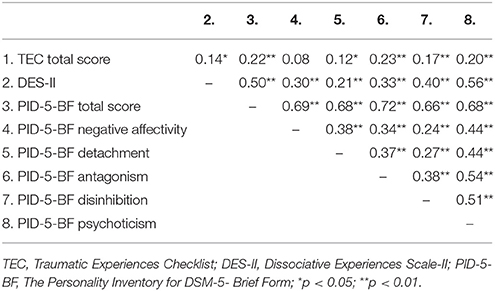
Table 2. Pearson's r correlations between traumatic experiences, dissociative experiences and maladaptive personality domains.
A mediation analysis controlling for gender, age, years of education, and marital status of participants showed that DES-II scores acted as partial mediators in the relationship between TEC scores (predictor) and PID-5-BF total scores (outcome). The hypothesized predictor (TEC total scores) was positively and significantly linked with both the proposed mediator (B = 1.07, se = 0.33) and the outcome (B = 1.10, se = 0.26). DES-II scores (mediator) were also positively related (B = 0.40, se = 0.04) with PID-5-BF total scores (outcome). The inclusion of DES-II scores in the model predicting PID-5-BF total scores by TEC total scores lowered the impact of TEC scores on PID-5-BF total scores (B = 0.68, se = 0.24), which, however, remained significant. The explained variance increased from 7.3%, F(5, 316) = 4.44, p = 0.001, to 29.3%, F(6, 315) = 31.33, p < 0.001 with the inclusion of dissociation in the model. Bootstrap analyses showed that the indirect effect of TEC scores on PID-5-BF total scores via DES-II scores was significant (C.I. 95%: 0.19–0.72), which was also confirmed by Sobel's test (z = 3.03, p = 0.002). Results from this mediation analysis are summarized in Figure 1.
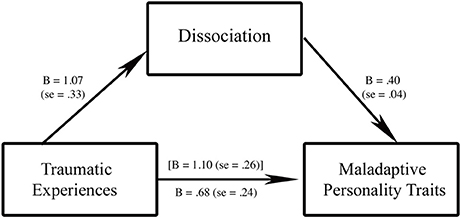
Figure 1. The mediating role of dissociation in the relationship between traumatic experiences and maladaptive personality traits. Traumatic experiences, Traumatic Experiences Checklist total score; Dissociation, Dissociative Experiences Scale–II total score; Maladaptive Personality Traits, The Personality Inventory for DSM-5-Brief Form total score; values in bracket square indicate the relationship between traumatic experiences (predictor) and maladaptive personality traits (outcome) without the inclusion of dissociation (mediator); all p < 0.01.
Further mediation analyses were performed to examine the potentially mediating role of DES-II scores in the relationship between TEC scores and PID-5-BF domain scores. Table 3 summarizes the findings from these analyses. As shown in Table 3, DES-II scores acted as partial mediators in the relationship between TEC scores and PID-5-BF domain scores concerning antagonism, disinhibition, and psychoticism, and as total mediators in the relationship between tec scores and pid-5-bf domain scores concerning negative affectivity and detachment.
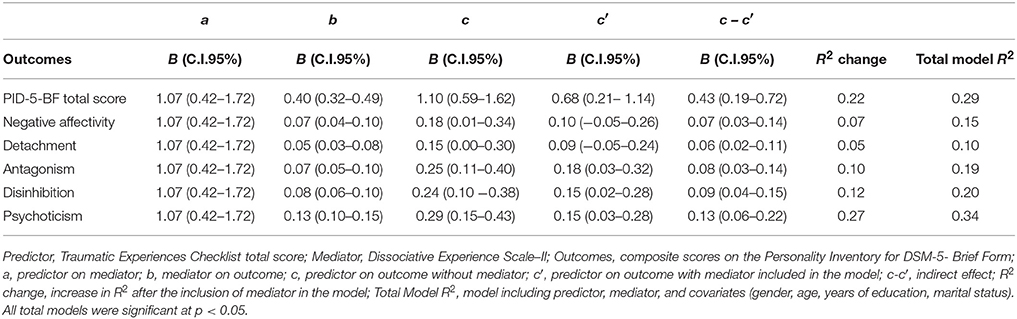
Table 3. Mediation models of the relationships between traumatic experiences (predictor) and maladaptive personality domains (outcomes) via dissociation (mediator).
Finally, because linear regression analyses showed that DES-II scores predicted PID-5-BF total scores, F(1, 320) = 107.35, p < 0.001, R2 = 0.251, the group of participants was split at the 50th percentile (median) of the TEC score distribution. This in order to identify participants in the sample who displayed low (TEC scores ≤ 2) and high (TEC scores > 2) levels of traumatization in this sample, and to examine whether the magnitude of the predictive association between DES-II scores and PID-5-BF total scores was related to different levels of traumatization. Different regression curves (linear, quadratic, cubic, exponential, and logistic) were tested, and it was verified that the relationship between dissociation and maladaptive personality features followed two distinct paths for people with low and high levels of trauma, with the best fitting curve for the data being a quadratic curve. In detail, the quadratic model was significant in the entire sample and in the two subgroups, F(2, 319) = 56.36, p < 0.001, R2 = 0.261, and it explained 1% of additional variance with respect to the linear model. This analysis also showed that the predictive association between DES-II scores and PID-5-BF scores was stronger in the subgroup with high levels of traumatization (R2 = 0.292) than in the subgroup with low levels of traumatization (R2 = 0.209), and that the two regression curves followed different pathways (see Figure 2). The curve of those with high levels of traumatization was almost a straight line with no visible inflection while the parabola of the curve of those with low levels of traumatization showed a clear deflection at DES-II scores above 45.
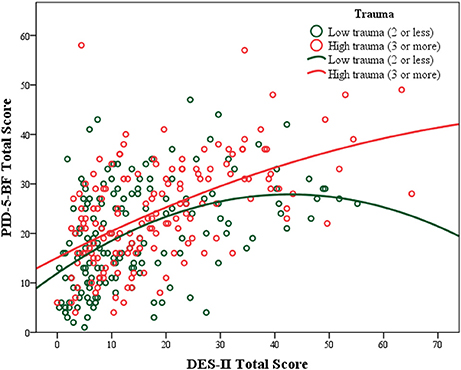
Figure 2. Predictive associations between dissociation scores and maladaptive personality scores at low and high levels of traumatization.
Discussion
The present study explored the relationships among psychological trauma, dissociation, and maladaptive personality domains. Consistent with previous studies on other nonclinical samples from the same country, our sample reported only low to moderate levels of psychological trauma (36), maladaptive personality traits (43, 44), and dissociative symptoms (3). Also consistent with the literature, males reported higher antagonistic features than females, and females reported higher negative affectivity than males (44). The main aim of our study was to test a conceptual model in which the predictive association between trauma and maladaptive personality functioning would be mediated by dissociation. The results of the mediation analyses supported this model.
In line with previous empirical findings and clinical considerations on the close relationship between complex trauma and dissociative experiences (45–47), we observed that increased numbers of traumatic experiences were associated with increased levels of dissociation in our study. Furthermore, we observed that traumatic experiences had both direct and indirect effects on global maladaptive personality functioning. Traumatic experiences significantly and positively predicted all maladaptive personality domains after controlling for sociodemographic variables (gender, age, years of education, and marital status), and they continued to significantly predict the domains of disinhibition, psychoticism, and antagonism after the inclusion of dissociation in the mediation models. Therefore, our results are generally consistent with previous studies showing that traumatic experiences can have a significant impact on the development of specific maladaptive personality domains, and especially those domains linked with self-regulation, identity integration, and difficulties with relatedness.
We also found that dissociative experiences always acted as significant mediators in the relationships between levels of traumatization and maladaptive personality domains scores. This result mirrors findings from a previous study on the relationships among trauma, dissociation, and psychopathology (5), and supports a wealth of clinical literature (1, 7–10, 14, 48, 49) suggesting that the development of maladaptive personality traits may result from complex traumatization (50–55) via an excessive activation of the dissociative processes (11, 16).
However, dissociation acted as a partial mediator, not as a full mediator, in the relationship between trauma score and overall maladaptive personality scores. A possible explanation of this finding is rooted in the fact that not all distressing experiences are processed through dissociation. Many traumatic experiences occur in fact in normal consciousness and are retained in accessible and retrievable memory (56–58). Thus, consistent with recent theory conceiving psychological trauma as a complex factor in which specific traumatic experiences may have different probability to combine and may relate differently to dissociative processes and psychopathology (5), it could be possible that several types of distressing experiences are tolerable to an individual's mind—perhaps because they occurred just once in life and/or at an adult age (when the personality and the capacity for affect regulation and mentalization are already developed) and/or when effective social support was available to buffer their effects. Such experiences may be encoded and processed at a conscious level, although they also may continue to constitute a source of distress for the individual. Other distressing experiences, which perhaps occurred more frequently, and/or started at an early age generating a maladaptive developmental cascade, and/or were extremely disorganizing, could be instead coded in altered and dissociative states of consciousness, with a stronger influence on the development of maladaptive personality functioning (4, 7, 13, 44, 59).
In this respect, dissociation may represent a mental process that can be used in adaptive or maladaptive ways in response to distressing experiences occurring in an individual's life. In fact, regression curve analyses showed two different pathways for the relationship between dissociation and maladaptive personality functioning, in which the numbers of trauma played a pivotal role. For individuals exposed to low numbers of traumatic experiences, personality functioning was only barely linked to dissociation, and actually the highest scores on dissociation corresponded to a decrease in maladaptive personality scores, suggesting that dissociation in this situation can act as a normal and even positive function of the mind, likely related to normal self-absorption phenomena and creative responses to distressing events (60). Thus, we could hypothesize that when the mind is exposed to low numbers of distressing experiences, dissociation can be used flexibly as a defense mechanism that protects the self from being overwhelmed by distressing stimuli or by excessive anxiety. On the contrary, for highly traumatized individuals, dissociation may become pervasive, jeopardizing their entire mental life (3). In these circumstances, the mind seems to keep the score (61) of previous traumata, and dissociation may become a psychological organizer of the entire self (11, 13), playing a key role in the development and consolidation of maladaptive personality domains.
Cumulatively, these considerations may suggest that dissociation as a psychological process maintains its own specific role in personality functioning, with different levels of trauma-related dissociation (or, better to say, with different levels of activation of the dissociative process following different levels of traumatization) linked to different levels of impairments in personality functioning.
In conclusion, our study supports the general hypothesis that maladaptive personality functioning is linked with trauma-related dissociation. However, as with all research, the present study comes with a number of limitations. First, the sample is constituted only by adult volunteers from an Italian isle, which limits the generalizability of our results. Second, causal interpretations of the relationships among traumatic experiences, dissociation, and personality are invoked based on theory, but the findings should be cautiously interpreted, and it is impossible to directly extend them to other samples due to the cross-sectional design of the study and the nonclinical nature of the sample. In this respect, longitudinal studies with clinical and nonclinical samples are warranted. Third, we did not distinguish between different types of trauma and the age at which they occurred, and actually we weighed all traumatic experiences equally, while research and clinical experiences suggest that different types of trauma might differently affect the development of personality. This approach to research data was clearly useful to empirically test the theoretical model on complex traumatization (5, 10) already illustrated in the present work and in other articles with respect to personality functioning, but we are aware that such approach to hypothesis-testing was taken at the price of potentially obscuring the relationships between specific characteristics of traumatic experiences and specific domains of maladaptive personality.
Conclusions
Even considering its limitations, this study shed some new light on how trauma and dissociation may undermine an individual's personality functioning. From a psychodynamic perspective, clinical work with traumatized patients is aimed at reestablishing the unity and uniqueness of self and personal identity by fostering mentalization, affect regulation, and a basic sense of safety and trust toward interpersonal relationships (4, 10–12, 14, 16, 62–69). So, understanding whether the excessive activation of the dissociative process has been so pervasive for an individual to deviate his or her entire organization of personality is a first step in uncovering the impact (and sometimes even the presence, in some cases of dissociative functioning with severe amnesia) of psychological trauma. This kind of knowledge can certainly help clinicians choose the best treatment available for people who display maladaptive personality traits.
Ethics Statement
This study was carried out in accordance with the recommendations of the American Psychological Association (APA) and the Italian Association of Psychology (AIP). The protocol was approved by the Internal Review Board for Psychological Research (IRB) of the UKE-Kore University of Enna (10th October 2016). All subjects were given a complete description of the study and provided written informed consent in accordance with the Declaration of Helsinki.
Author Contributions
AS designed the study and managed the research process. FG and AC collected and analyzed the data. AG, FG, and AC performed the literature review. AG, FG, and AS took primary responsibility for initial drafting. VC contributed with relevant theoretical and clinical inputs. AG and AS were responsible for subsequent collation of inputs and redrafting. All authors critically revised the manuscript and approved its final version.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Dell PF, O'Neil JA (eds.). Dissociation and the Dissociative Disorders: DSM-V and Beyond. New York, NY: Routledge (2009).
2. Porges SW. The polyvagal theory: phylogenetic substrates of a social nervous system. Int J Psychophysiol. (2001) 42:123–46. doi: 10.1016/S0167-8760(01)00162-3
3. Schimmenti A. Dissociative experiences and dissociative minds: exploring a nomological network of dissociative functioning. J Trauma Dissoc. (2016) 17:338–61. doi: 10.1080/15299732.2015.1108948
4. Schimmenti A. The developmental roots of dissociation: a multiple mediation analysis. Psychoanal Psychol. (2017) 34:96–105. doi: 10.1037/pap0000084
5. Schimmenti A. The trauma factor: examining the relationships among different types of trauma, dissociation, and psychopathology. J Trauma Dissoc. (2017) 11:1–20. doi: 10.1080/15299732.2017.1402400
7. Schore AN. Attachment trauma and the developing right brain: origins of pathological dissociation. In: Dell PF, O'Neil JA, editors. Dissociation and the Dissociative Disorders: DSM-V and Beyond. New York, NY: Routledge (2009). p. 141–53.
8. Bromberg PM. Standing in the Spaces: Essays on Clinical Process, Trauma and Dissociation. Hillsdale, MI: The Analytic Press (1998).
9. Bromberg PM. Dissociation and personality organization: reflections on Peter Goldberg's essay. Psychoanal Dialogues (1995) 5:511–28. doi: 10.1080/10481889509539089
10. Schimmenti A, Caretti V. Linking the overwhelming with the unbearable: developmental trauma, dissociation, and the disconnected self. Psychoanal Psychol. (2016) 33:106–28. doi: 10.1037/a0038019
11. Chefetz RA. Intensive Psychotherapy for Persistent Dissociative Processes: The Fear of Feeling Real. New York, NY: WW Norton (2015).
13. Bromberg PM. The Shadow of the Tsunami and the Growth of the Relational Mind. London: Routledge (2012).
14. Sar V, Öztürk E. Functional dissociation of the self: a sociocognitive approach to dissociation. J Trauma Dissoc. (2007) 8:69–89. doi: 10.1300/J229v08n04_05
15. Schimmenti A. Elena: a case of dissociative identity disorder from the 1920s. Bull Menninger Clin. (2017) 81:281–98. doi: 10.1521/bumc_2017_81_08
17. Farina B, Speranza AM, Dittoni S, Gnoni V, Trentini C, Vergano CM, et al. Memories of attachment hamper EEG cortical connectivity in dissociative patients. european archives of Psychiatry Clin Neurosci. (2014) 264:449–58. doi: 10.1007/s00406-013-0461-9
18. Lanius RA, Vermetten E, Loewenstein RJ, Brand B, Schmahl C, Bremner JD, et al. Emotion modulation in PTSD: clinical and neurobiological evidence for a dissociative subtype. Am J Psychiatry (2010) 167:640–47. doi: 10.1176/appi.ajp.2009.09081168
19. Lanius UF, Paulsen SL, Corrigan FM. Neurobiology and Treatment of Traumatic Dissociation: Towards an Embodied Self. New York, NY: Springer (2014).
20. Mutluer T, Sar V, Kose-Demiray C, Arslan H, Tamer S, Ünal S, et al. Lateralization of neurobiological response in adolescents with PTSD related to severe childhood sexual abuse: the Tri-Modal Reaction (T-MR) model of protection. J Trauma Dissoc. (2017) 10:1–18.
21. Reinders AATS, Willemsen ATM, Vissia EM, Vos HPJ, Den Boer JA, Nijenhuis ERS. The psychobiology of authentic and simulated dissociative personality states: The full monty. J Nervous Mental Dis. (2016) 204:445–57. doi: 10.1097/NMD.0000000000000522
22. Ross CA, Goode C, Schroeder E. Hippocampal volumes in a sample of trauma patients: a possible neuro-protective effect of dissociation. Open Psychiatry J. (2015) 9:7–10. doi: 10.2174/1874354401509010007
23. Amos J, Furber G, Segal L. Understanding maltreating mothers: a synthesis of relational trauma, attachment disorganization, structural dissociation of the personality, and experiential avoidance. J Trauma Dissoc. (2011) 12:495–509. doi: 10.1080/15299732.2011.593259
24. Brand BL, Classen CC, McNary SW, Zaveri P. A review of dissociative disorders treatment studies. J Nervous Mental Dis. (2009) 197:646–54. doi: 10.1097/NMD.0b013e3181b3afaa
25. Schalinski I, Teicher MH. Type and timing of childhood maltreatment and severity of shutdown dissociation in patients with schizophrenia spectrum disorder. PLoS ONE (2015) 10:e0127151. doi: 10.1371/journal.pone.0127151
26. Twaite JA, Rodriguez-Srednicki O. Childhood sexual and physical abuse and adult vulnerability to PTSD: The mediating effects of attachment and dissociation. J Child Sex Abuse (2004) 13:17–38. doi: 10.1300/J070v13n01_02
27. Brown RC, Berenz EC, Aggen SH, Gardner CO, Knudsen GP, Reichborn-Kjennerud T, et al. Trauma exposure and Axis I psychopathology: a cotwin control analysis in Norwegian young adults. Psychol Trauma (2014) 6:652–60. doi: 10.1037/a0034326
28. Fink DS, Galea S. Life course epidemiology of trauma and related psychopathology in civilian populations. Curr Psychiatry Rep. (2015) 17:5–9. doi: 10.1007/s11920-015-0566-0
29. Schalinski I, Teicher MH, Nischk D, Hinderer E, Müller O, Rockstroh B. Type and timing of adverse childhood experiences differentially affect severity of PTSD, dissociative and depressive symptoms in adult inpatients. BMC Psychiatry (2016) 16:295. doi: 10.1186/s12888-016-1004-5
30. Brents LK, Tripathi SP, Young J, James GA, Kilts CD. The role of child- hood maltreatment in the altered trait and global expression of personality in cocaine addiction. J Psychiatry Res. (2015) 64:23–31. doi: 10.1016/j.jpsychires.2015.02.015
31. Kim J, Cicchetti D, Rogosch FA, Manly JT. Child maltreatment and trajectories of personality and behavioral functioning: implications for the development of personality disorder. Dev Psychopathol. (2009) 21:889–912. doi: 10.1017/S0954579409000480
32. Rogosch FA, Cicchetti D. Child maltreatment and emergent personality organization: Perspectives from the five-factor model. J Abnorm Child Psychol. (2004) 32:123–45. doi: 10.1023/B:JACP.0000019766.47625.40
33. Oshri A, Rogosch FA, Cicchetti D. Child maltreatment and mediating influences of childhood personality types on the development of adolescent psychopathology. J Clin Child Adolesc Psychol. (2013) 42:287–301. doi: 10.1080/15374416.2012.715366
34. Spinhoven P, Elzinga BM, Van Hemert AM, de Rooij M, Brenda W., Penninx BW. Childhood maltreatment, maladaptive personality types and level and course of psychological distress: a six-year longitudinal study. J Affect Disord. (2016) 191:100–8. doi: 10.1016/j.jad.2015.11.036
35. Nijenhuis ERS, Van der Hart O, Kruger K. The psychometric characteristics of the Traumatic Experiences Checklist (TEC): First findings among psychiatric outpatients. Clin Psychol Psychother. (2002) 9:200–10. doi: 10.1002/cpp.332
36. Schimmenti A, Passanisi A, Caretti V, La Marca L, Granieri A, Iacolino C, et al. Traumatic experiences, alexithymia, and Internet addiction symptoms among late adolescents: a moderated mediation analysis. Addict Behav. (2017) 64:314–20. doi: 10.1016/j.addbeh.2015.11.002
37. Carlson EB, Putnam FW, Ross CA, Torem M, Coons P, Dill DL, et al. Validity of the Dissociative experiences scale in screening for multiple personality disorder: a multicenter study. Am J Psychiatry (1993) 150:1030–6. doi: 10.1176/ajp.150.7.1030
38. Van Ijzendoorn MH, Schuengel C, Bakermans-Kranenburg MJ. Disorganized attachment in early childhood: meta-analysis of precursors, concomitants, and sequelae. Dev Psychopathol. (1999) 11:225–49. doi: 10.1017/S0954579499002035
39. Krueger RF, Derringer J, Markon KE, Watson D, Skodol AE. Initial construction of a maladaptive personality trait model and inventory for DSM-5. Psychol Med. (2012) 42:1879–90. doi: 10.1017/S0033291711002674
40. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5th edn. Arlington, TX: American Psychiatric Publishing (2013).
41. Fossati A, Krueger RF, Markon KE, Borroni S, Maffei C, Somma A. The DSM-5 alternative model of personality disorders from the perspective of adult attachment: a study in community-dwelling adults. J Nervous Mental Dis. (2015) 203:252–8. doi: 10.1097/NMD.0000000000000274
42. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis. A Regression-Based Approach. New York, NY: Guilford Publications (2013).
43. Gervasi AM, La Marca L, Lombardo EMC, Mannino G, Iacolino C, Schimmenti A. Maladaptive personality traits and internet addiction symptoms among young adults: A study based on the alternative DSM-5 model for personality disorders. Clin Neuropsychiatry (2017) 14:20–8.
44. Granieri A, La Marca L, Mannino G, Giunta S, Guglielmucci F, Schimmenti A. The relationship between defense patterns and DSM-5 maladaptive personality domains. Front Psychol. (2017) 8:1926. doi: 10.3389/fpsyg.2017.01926
45. Carlson EB, Dalenberg C, McDade-Montez E. Dissociation in posttraumatic stress disorder part I: Definitions and review of research. Psychol Trauma (2012) 4:479–89. doi: 10.1037/a0027748
46. Dalenberg CJ, Brand BL, Gleaves DH, Dorahy MJ, Loewenstein RJ, Cardeña E, et al. Evaluation of the evidence for the trauma and fantasy models of dissociation. Psychol Bull. (2012) 138:550–88. doi: 10.1037/a0027447
47. Dalenberg CJ, Brand BL, Loewenstein RJ, Gleaves DH, Dorahy MJ, Cardeña E, et al. Reality versus fantasy: reply to Lynn et al. Psychol Bull. (2014) 140:911–20. doi: 10.1037/a0036685
48. Blum H. Dissociation and its disorders. Psychoanal Inquiry (2013) 33:427–38. doi: 10.1080/07351690.2013.815058
50. Forbes D, Elhai JD, Miller MW, Creamer M. Internalizing and externalizing classes in posttraumatic stress disorder: a latent class analysis. J Traum Stress (2010) 23:340–9. doi: 10.1002/jts.20526
51. James LM, Anders SL, Peterson CK, Engdahl BE, Krueger RF, Georgopoulos AP. DSM-5 personality traits discriminate between posttraumatic stress disorder and control groups. Exp Brain Res. (2015) 233:2021–8. doi: 10.1007/s00221-015-4273-1
52. Jang KL, Stein MB, Taylor S, Asmundson GJG, Livesley WJ. Exposure to traumatic events and experiences: aetiological relationships with personality function. Psychiatry Res. (2003) 120:61–9. doi: 10.1016/S0165-1781(03)00172-0
53. Li XB, Wanga ZM, Houa YZ, Wanga Y, Liub JT, Wanga CY. Effects of childhood trauma on personality in a sample of Chinese adolescents. Child Abuse Neglect (2014) 38:788–96. doi: 10.1016/j.chiabu.2013.09.002
54. Veith AC, Russell TD, King AR. PID-5 trait mediation of childhood maltreatment effects. Pers Individ Differ. (2017) 104:58–63. doi: 10.1016/j.paid.2016.07.024
55. Yan YY, Meng XZ. The study of child abuse and trauma experience on adult mental health. Chin J Clin Psychol. (2005) 13:208–9.
56. Frewen PA, Lanius RA. Trauma-related altered states of consciousness: exploring the 4-D model. J Trauma Dissoc. (2014) 15:436–56. doi: 10.1080/15299732.2013.873377
57. Frewen PA, Hegadoren K, Coupland NJ, Rowe BH, Neufeld RW J, Lanius RA. Trauma-related altered states of consciousness (TRASC) and functional impairment I: prospective study in acutely traumatized persons. J Trauma Dissoc. (2015) 16:500–19. doi: 10.1080/15299732.2015.1022925
58. Sar V. Parallel-distinct structures of internal world and external reality: disavowing and re-claiming the self-identity in the aftermath of trauma-generated dissociation. Front Psychol. (2017) 8:216. doi: 10.3389/fpsyg.2017.00216
59. Mahoney D, Markel B. An integrative approach to conceptualizing and treating complex trauma. Psychoanal Soc Work (2016) 23:1–22. doi: 10.1080/15228878.2015.1104640
60. Butler LD. Normative dissociation. Psychiatr Clin North Am. (2006) 29:45–62. doi: 10.1016/j.psc.2005.10.004
61. Van der Kolk BA. The body keeps the score. Memory and the evolving of psychobiology of posttraumatic stress. Harvard Rev Psychiatry (1994) 1:253–65. doi: 10.3109/10673229409017088
62. Allen JG, Fonagy P, Bateman AL. Mentalizing in Clinical Practice. Washington, DC: American Psychiatric Publishing (2008).
63. Chefetz RA. Healing haunted hearts - toward a model for integrating subjectivity: Commentary on papers by Philip Bromberg and Gerald Stechler. Psychoanal Dialog.(2003) 13:727–42. doi: 10.1080/10481881309348766
64. Fonagy P, Gergely G, Jurist EL, Target M. Affect Regulation, Mentalization, and the Development of the Self. New York, NY: Other Press (2002).
65. Granieri A. Corporeo, Pensiero, Affetti. Intreccio tra Psicoanalisi e Neurobiologia. [Body, Affects and Thinking. The Link between Psychoanalysis and Neurobiology]. Torino: UTET Università (2011). Italian.
66. Granieri A. The drive for self assertion and the reality principle in a patient with mesothelioma: the history of Giulia. Am J Psychoanal. (2017) 77:285–94. doi: 10.1057/s11231-017-9099-0
67. Granieri A, Schimmenti A. Mind–body splitting and eating disorders: a psychoanalytic perspective. Psychoanal Psychother. (2014) 28:52–70. doi: 10.1080/02668734.2013.872172
68. Howell EF. Inside and outside: “Trauma/dissociation/relationality” as a framework for understanding psychic structure and problems in living. Psychoanal Perspect. (2007) 5:47–67.
Keywords: trauma, dissociation, personality, alternative DSM-5 model for personality disorder, defense mechanisms
Citation: Granieri A, Guglielmucci F, Costanzo A, Caretti V and Schimmenti A (2018) Trauma-Related Dissociation Is Linked With Maladaptive Personality Functioning. Front. Psychiatry 9:206. doi: 10.3389/fpsyt.2018.00206
Received: 12 February 2018; Accepted: 03 May 2018;
Published: 25 May 2018.
Edited by:
Danny Horesh, Bar-Ilan University, IsraelReviewed by:
Antonio Bruno, Università degli Studi di Messina, ItalyRachel Lev-Wiesel, University of Haifa, Israel
Copyright © 2018 Granieri, Guglielmucci, Costanzo, Caretti and Schimmenti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fanny Guglielmucci, ZmFubnkuZ3VnbGllbG11Y2NpQGxpdmUuaXQ=