 Shervin Assari
Shervin Assari Maryam Moghani Lankarani
Maryam Moghani Lankarani- 1Department of Psychiatry, School of Medicine, University of Michigan, Ann Arbor, MI, USA
- 2Center for Research on Ethnicity, Culture and Health, School of Public Health, University of Michigan, Ann Arbor, MI, USA
- 3Medicine and Health Promotion Institute, Tehran, Iran
Background: Despite the existing knowledge on the association between discrimination and poor mental health, very few studies have explored gender differences in this association in Arab Americans.
Objective: The current study aimed to investigate whether gender moderates the association between the experience of discrimination and psychological distress in a representative sample of Arab Americans in Michigan.
Methods: Using data from the Detroit Arab American Study (DAAS), 2003, this study recruited Arab Americans (337 males, 385 females) living in Michigan, United States. The main independent variable was discrimination. The main outcome was psychological distress. Covariates included demographic factors (age), socioeconomic status (education, employment, and income), and immigration characteristics (nativity and years living in United States). Gender was the focal moderator. We used multivariable regression with and without discrimination × gender interaction term.
Results: In the pooled sample, discrimination was positively associated with psychological distress [B = 0.62, 95% confidence interval (CI) = 0.22–1.03, p = 0.003]. We found a significant gender × discrimination interaction in the pooled sample (B = 0.79, 95% CI = 0.01–1.59, p = 0.050), suggesting a stronger association in males than females. In our gender-specific model, higher discrimination was associated with higher psychological distress among male (B = 0.87, 95% CI = 0.33–1.42, p = 0.002) but not female (B = 0.18, 95% CI = −0.43 to 0.78, p = 0.567) Arab Americans.
Conclusion: While discrimination is associated with poor mental health, a stronger link between discrimination and psychological symptoms may exist in male compared to female Arab Americans. While efforts should be made to universally reduce discrimination, screening for discrimination may be a more salient component of mental health care for male than female Arab Americans.
Introduction
Discrimination can be defined as the unfair treatment of different categories of people based on race, gender, age, religion, sexual orientation, and other characteristics (1–4). Given that discrimination operates as a stressor, it may increase the risk of a wide range of undesired physical and mental health outcomes (5–9). Some of the undesired consequences of discrimination include depression (10), anxiety (11), substance use (12), suicide (13, 14), and psychological distress (15).
From a population perspective, most of the United States literature on the association between the discrimination and mental health of racial and ethnic minorities is written about discrimination against Blacks (3, 8, 16–22) and Hispanics (23–25). Thus, more is yet to be learned about populations such as Arab Americans (26, 27) who also experience considerable levels of discrimination in their everyday life (28).
Regarding causes of discrimination, most of the current literature is written about discrimination because of race and ethnicity; however, religion is also a source of discrimination (13, 14). This is especially important for Muslim Americans, a population commonly exposed to discrimination for reasons other than race and ethnicity, specifically their belief in Islam (26–28). Particularly, discrimination against the Muslim American community increased considerably following September 11 attacks (29, 30).
Regardless of whether it is overt or perceived, general or specific, related to race, ethnicity, race, or religion, exposure to discrimination is a risk factor for poor mental health (3, 9, 16, 31–35). Perceived discrimination influences may have long-term effects on mental health (31). This notion proposes perceived racial discrimination as a distinct stressor (31). Perceived discrimination can lead to a wide range of adverse mental outcomes including depression (10), anxiety (11), substance use (12), suicidal ideation (13, 14), and psychological distress (15).
Discrimination may have similar effects as other stressors (3). There are studies that suggest discrimination may even have a more powerful effect on psychological distress compared with general stressful life events (9, 36). Baseline perceived discrimination better predicts future adverse mental health outcomes than vice versa, suggesting a causal link between discrimination and poor mental health (16).
From a long list of potential moderators that alter the effects of discrimination on mental health (10, 37, 38), gender has received little attention (12). Gender interferes with experiencing discrimination (39–42). For instance, among Blacks, men report higher rates of perceived discrimination compared to women (43, 44). Concerning the gender gap in discrimination, multiple hypotheses are proposed. The race–gender intersectionality hypothesis suggests that life experiences are shaped by the intersection of race and gender, rather than merely race or gender alone, and discrimination may be more common among Black men (41). This is also in line with mass incarceration and police brutality against Black men (45, 46). Based on the subordinate male hypothesis, discrimination is more detrimental for men than women, as men have a higher preference for dominance and hierarchy. In this view, masculinity ideologies may increase mental health costs associated with perceived discrimination (47).
The current study was performed to investigate whether gender moderates the association between discrimination and psychological distress in a representative sample of Arab Americans in the United States.
Materials and Methods
Design and Setting
Data came from the 2003 Detroit Arab American Study (DAAS) survey (48). The DAAS is a representative survey conducted from July to December 2003 in Wayne, Oakland, and Macomb counties, Michigan. The DAAS survey was designed through a partnership and collaboration between the academic affiliates and community members where both Muslim Arab and Chaldean (Christian) Arab groups were represented.
Main Study
The DAAS data collection was conducted between July and December 2003. The DAAS included all adults of Arab or Chaldean descent living in Michigan’s Wayne, Oakland, and Macomb counties. Approximately 490,000 Arabs resided in Michigan at the time of study, of whom more than 80% lived in the above listed counties (49). Arab Americans are the third largest ethnic group in Michigan, with a history dating back multiple generations (30, 50, 51).
Some of this population are Christian, and some are Muslim. For instance, Chaldean Americans are Catholic Christians and are descendants of people from the northern Tigris-Euphrates Valley, with their own language. Although they share some aspects of culture and experience with other Arab Americans, they may also represent a distinct ethnic group (52, 53). Thus, although participants in this study represent distinct ethnic groups, they share major aspects of Arab cultures and are all recognized as Arab Americans (30).
Sampling
Eligibility was based on Arab or Chaldean ancestry from adults living in Michigan. Most countries included were Egypt, Iraq, Jordan, Palestine, Lebanon, Libya, Saudi Arabia, Syria, and Yemen. Although these countries are all Arab, they are not all Muslim countries. A large proportion of participants were also Chaldean Christians. Individuals residing in institutions, in group quarters, or on military bases were excluded (54). A total of 1,389 eligible households were identified; 1,016 adults from these eligible households completed the study interview. Participation rate was 73% (30).
A dual-frame probability sample design was used in DAAS. An area probability frame was employed to select area segments from year 2000 census tracts in which 10% or more of individuals self-identified as Arab or Chaldean in ancestry. Then a list frame was used to select housing units from the mailing and membership lists of 13 Arab American and Chaldean American community organizations. The area probability component was based on the following stages: (1) area segment units, (2) housing units within area segments, and (3) selection of an eligible adult from each household. Within the list frame, a systematic random sample of individual addresses was employed, with random selection of one eligible adult respondent in each household (30).
Process
The DAAS administered surveys via face-to-face interviews for data collection. Data were collected on demographic and socioeconomic factors, discrimination, attitudes and beliefs, and health. The main predictor of interest was discrimination. The main outcome was psychological distress. Confounders included demographic and socioeconomic factors and health status (30).
Measures
Demographic Factors
Data were collected on gender (male as the referent group) and age (younger than 30 years, 30–55 years, older than 55 years).
Socioeconomic Characteristics
We collected data on education level (less than high school, some college, and advanced degree), marital status, and household income (less than $30,000, $30,000–$75,000, and above $75,000).
Immigration-Related Factors
Data were collected on the country of origin, nativity, and years of residence in the United States.
Discrimination
The study collected data on self-report of personal abuse against individuals or their household members by answering yes or no to the question “In the last 2 years, have you personally, or anyone in your household, experienced verbal insults or abuse, threatening words or gestures, physical attack, vandalism or destruction of property, or loss of employment, due to your race, ethnicity, or religion?” Participants were also asked if they had experienced post-September 11 discrimination by the following question “Since 9/11, have you personally had a bad experience due to your Arab or Chaldean ethnicity?” Respondents were also asked to rate their level of agreement, on a 5-point Likert-type scale, with the statement “Arab Americans are not respected by the broader American society.” Fourth, they were asked “How much—if any—have the events of 9/11 shaken your own personal sense of safety and security?” Responses were gathered on a 4-point Likert-type scale.
Self-rated Health (SRH)
To measure SRH, all respondents were asked “How would you describe your overall state of health these days? Would you say it is excellent, very good, good, fair, or poor?” This single-item measure of SRH has been shown to be an independent predictor of mortality risk above and beyond baseline physical health status and lifestyle (55, 56).
Psychological Distress
The main outcome variable was psychological distress measured by the Kessler Psychological Distress Scale (K10) (57). The K10 results have been previously validated as a screening tool comparable with the General Health Questionnaire (58). The Cronbach alpha coefficient for the K10 in our sample was 0.89. We computed a K10 score for each respondent, with a higher score reflecting more distress.
Data Analysis
Data analysis was conducted in SPSS 20.0 for Windows (IBM Inc., Armonk, NY, USA). For descriptive statistics, we presented frequency and relative frequency for categorical and mean measures, and SD for continuous measures, both in the pooled sample, and based on gender. We used the Pearson correlation test for bivariate analysis, in the pooled sample, and based on gender.
For our multivariable analysis, we ran a series of multiple linear regressions. First, we ran our models in the pooled sample. In these models, discrimination was the main independent variable of interest, and psychological distress was the dependent variable. Age, education, income, marital status, employment, and SRH were covariates. Gender was the focal moderator. Regression coefficients (B), SE, 95% confidence interval (CI), and p value were reported.
In the first regression model, we only included demographic factors (age, gender, and nativity). In model 2, we also added socioeconomic factors (education, family income, married, and employment). In model 3, we also controlled for health (SRH) added discrimination and included gender by discriminate interaction. Then we ran gender-specific models with the same order (models 1–4).
Ethics
The research followed the tenets of the Declaration of Helsinki. This project was approved by the Institutional Review Board of the University of Michigan, Ann Arbor. All participants provided written informed consent, and all data were kept confidential.
Results
Univariate Analysis
Table 1 shows descriptive statistics in the pooled sample. As this table shows, mean (SD) of age of the participants was 43.63 (16.48). Most of the participants were women, immigrants (non-United States born), married, and unemployed.
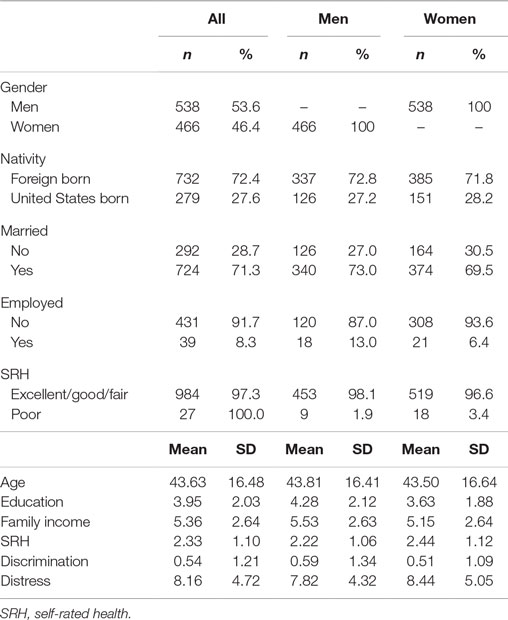
Table 1. Summary of descriptive statistics in the pooled sample and based on gender in Arab Americans.
Table 1 also shows descriptive statistics based on gender. While education and income were higher in men than in women, SRH and psychological distress were worse in women than in men. Men reported higher levels of discrimination than women.
Bivariate Analysis
Table 2 shows bivariate correlations in the pooled sample. As this table shows, discrimination and psychological distress showed a weak, yet positive association (r = 0.16). In the pooled sample, psychological distress was also associated with gender, education, income, marital status, and SRH.
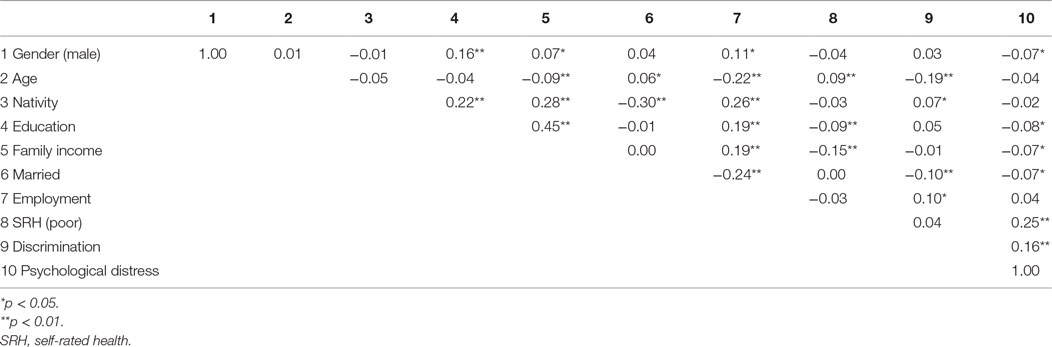
Table 2. Summary of bivariate correlations in the pooled sample of Arab Americans.
Table 3 shows bivariate correlations based on gender. As this table shows, discrimination and psychological distress were correlated in males (r = 0.22) and females (r = 0.10).
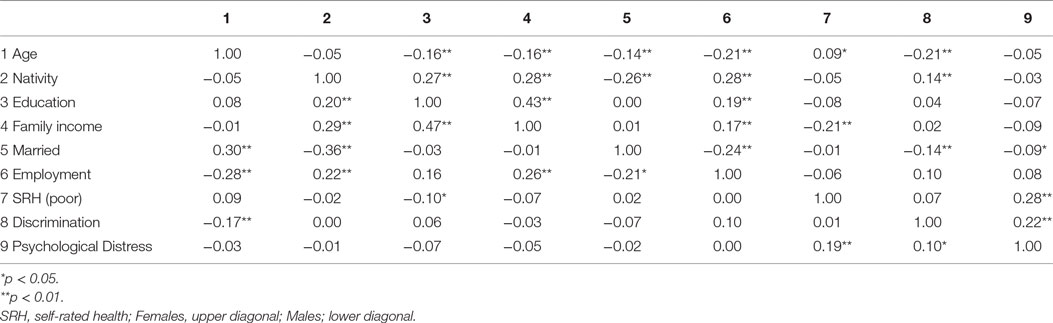
Table 3. Summary of bivariate correlations based in Arab American male and females.
Multivariable Analysis
As Table 4 shows, in the pooled sample, discrimination was positively associated with psychological distress (B = 0.62, 95% CI = 0.22–1.03, p = 0.003). We found a significant gender × discrimination interaction in the pooled sample (B = 0.79, 95% CI = 0.01–1.59, p = 0.050), suggesting a stronger association in males than in females.
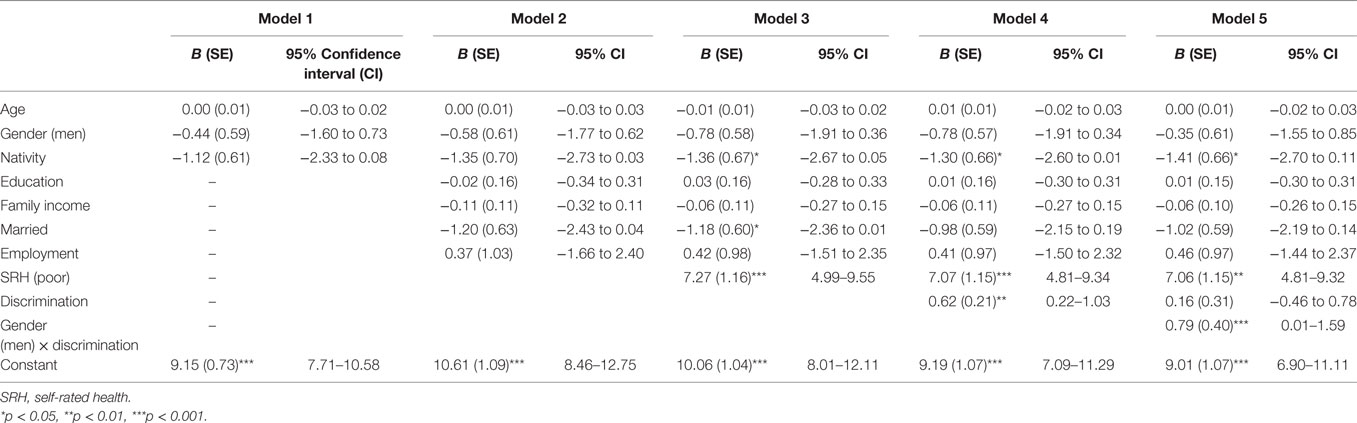
Table 4. Summary of linear regression analysis between discrimination and psychological distress in the pooled sample of Arab Americans.
As Table 5 shows, in our gender-specific model, higher discrimination was associated with higher psychological distress among male (B = 0.87, 95% CI = 0.33–1.42, p = 0.002), but not female (B = 0.18, 95% CI = −0.43 to 0.78, p = 0.567), Arab Americans.
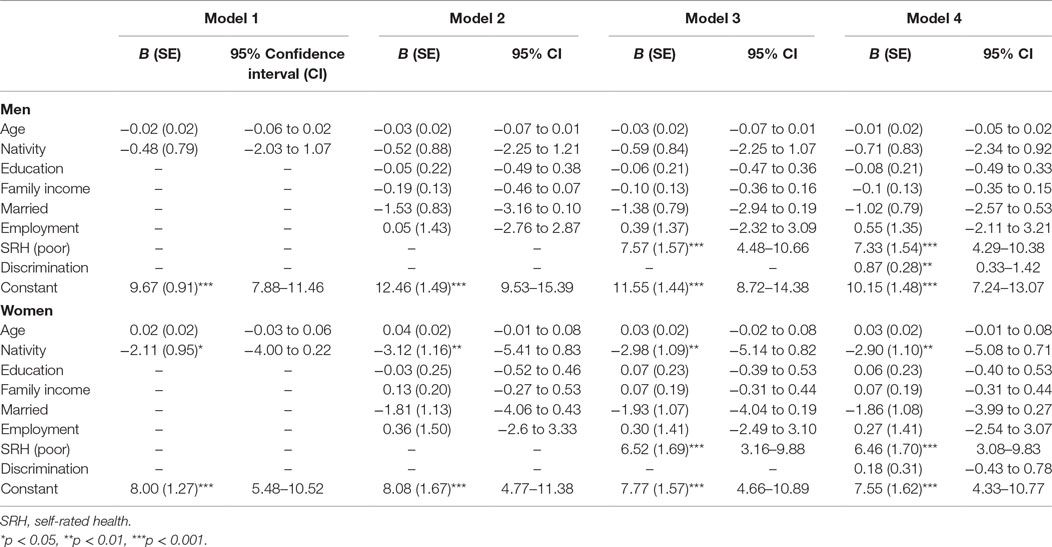
Table 5. Summary of linear regression analysis between discrimination and psychological distress among male and female Arab Americans.
Discussion
Our study revealed two main findings; first, discrimination was associated with psychological distress among Arab Americans. Second, gender moderates the association between perceived discrimination and psychological distress in the Arab American community, with the association being stronger for males than for females.
Our first finding that discrimination is associated with psychological distress is in line with previous studies (15). Discrimination is also associated with other undesired physical and mental health outcomes (5–9) including but not limited to depression (10), anxiety (11), substance use (12), and suicide (13, 14). Most of the published literature on mental health correlates of discrimination in the United States is, however, limited to Blacks (3, 8, 16–22) and Hispanics (23–25). This study extends the limited literature on Arab Americans (26–28).
Our second finding on gender as a moderator of the association between discrimination and psychological distress is also in line with findings in other ethnic groups. In studies that have mostly enrolled Black Americans, men have reported higher rates of perceived discrimination compared with women (41, 43, 44). Building on multiracial feminist theories, Harnois and Ifatunji (59) offered a theoretical framework to understand interpersonal racial discrimination as gendered measures, gendered models, and gendered phenomena. The intersectional framework that Harnois and Ifatunji proposed suggests that, while there are some discriminatory practices that are directed at both male and female minorities, some forms of discrimination will affect men more than women, some will affect women more than men, and some forms may be gender-specific (59). For instance, due to controlling images that are gendered, among Blacks, men are content with stereotypes such as the lower-class, hyper-sexual “thug,” while women face stereotypes of mammies, matriarchs, jezebels, and welfare queens (60–63). There is evidence suggesting that some racial stereotypes are indeed gender-specific (64, 65). Men of color may be more commonly discriminated against when they look for a job; as in some racial groups, women may have better job opportunities than men (66).
Multiple hypotheses have been proposed to explain the gender gap in perceived discrimination among minorities. The subordinate male target hypothesis argues that minority men are subject to more experiences of discrimination (41). The race–gender intersectionality hypothesis also argues that it is neither race nor gender, but their intersection that shapes experiences such as discrimination (41, 59). According to recent work by Ifatunji and Harnois on data from the National Survey of American Life as well as the Detroit Area Study, everyday discrimination could justify the subordinate male hypothesis, while major life discrimination could better fit with the intersectionality hypothesis (41). In the case of Blacks, more negative attitudes toward Black males compared with Black females as a result of stereotypes that exist around race and gender may be due to the attribution of aggression and anti-intellectuality to Black males (40, 42, 67, 68). It has been shown that in schools, Black boys more commonly receive negative treatment compared to Black girls (42, 69–73). This may be in part due to differences in attending to threat, perceived threat, and stereotype threat for Black men that may also be in part reinforced by their body size, appearance, or behaviors (74–76). Such differences can be seen in neuroimaging studies (77) or neurocognitive tests (78). Such threat attention may also have implications in interactions between minority men and police (79). In the case of Arab Americans, with the same reasoning, men may be more frequently exposed to discrimination due to stereotype threat.
Among minorities, gender may shape the frequency of messages around race, racism, discrimination, immigration, and religion in families. For instance, among Black families, boys and girls receive different levels of parental messages considering discrimination and racial barriers (80, 81). Differential messages that are being communicated to boys and girls may cause differential awareness or attention toward factors such as discrimination and associated cues in one gender. Such practices may influence perception as well as impact of discrimination between males and females. Another factor may be masculine role norms that may moderate the link between discrimination and psychological distress in minorities (10, 82). Yet another explanation is restricted emotion expression in men in general, and in men of color in particular. Men of color who live under oppression learn to have a higher self-reliance that may increase psychological distress (82). Sex and gender role, self-image, peer appraisal, gender identity, and access to social support may also have a differential role for male and females (42). In addition, males and females use different coping styles to deal with stressors, including discrimination (42, 83). Overall, the interaction of gender and culture/ethnicity should be considered when studying the mental health of minority individuals (42).
Our findings should be interpreted in the context of Arab American culture that shapes traditional gender roles, norms, and identities. In many Arab and Muslim countries, gender roles are very distinct for men and women. Major decisions are made by men, as men are very authoritative toward women, who are more submissive. Men are the main breadwinners and are involved with the labor market, so they get more involved with the society in general. Instead, women’s social lives are more limited, as they spend most of their time inside with their children and close relatives. Men endorse high levels of hegemonic masculinities and are not expected to share their emotions. As a result, men internalize their emotional problems, do not seek emotional social support, and do not communicate about their problems. This increases vulnerability of men compared to women, who can easily seek emotional support and share and communicate about their emotional problems and stressors (84–89).
Research has shown that in addition to distress, discrimination is also associated with drug use; an effect which seems to be stronger for males than for females (12). Brondolo et al. (90) showed that discrimination may differently influence substance use of men and women, with stronger effects in men compared with women. Our study, however, did not explore gender differences in the effects of discrimination on substance use in the Arab community.
In contrast to our study, which did not find an association between discrimination and distress among females, other studies have found such association between experiences of discrimination and poor mental health in female minorities (91). Coping, however, may explain some gender differences in the consequences of discrimination. Among Blacks, women have a higher tendency to use avoidant coping mechanisms in response to race-related stress, rather than recruiting more combative forms of coping, such as using one’s voice as power (83). Avoidant coping may mediate the association of gendered racism with heightened distress (83).
Gender may mitigate how exposure to the same discriminatory experience is perceived as stressful (21). Gender influences the decision to seek emotional support following exposure to discrimination and other stressors, with women having a higher tendency to seek social support than men; this support, sought from a wide range of sources including family and friends, is used as a coping strategy against racism (92–95), which is in line with the notion that women are better users of social support in general than are men (96). Family members and friends may also be differently available as a source of social support for men and women (10).
Our findings indicating gender differences in the psychological correlates of perceived discrimination have implications for public health and clinical practice with the Arab American community. Perceived discrimination may be a more salient contributor to poor mental health for male compared to female Arab Americans. Asking about perceived discrimination may be an important aspect of mental health screening both in community and clinical settings and may be an important step toward the diagnosis and treatment of psychopathology for Arab Americans, particularly men.
Our findings may also have implications for future research on the intersection of race and ethnicity, discrimination, and health. Further research is needed to better understand mechanisms by which male and female Arab Americans respond differently to similar discrimination experiences. Differential coping mechanisms may be a hypothetical explanation for worse effects of discrimination on the mental health of male minorities.
This study is subject to a few limitations. First, we measured psychological distress rather than clinical diagnosis of psychiatric disorders. Although we used a valid measure of psychological symptoms, structural interviews could have provided more accurate results. Second, we did not account for a previous diagnosis of psychopathology, or the use of anti depressant or anxiolytic medications which may interfere with the psychological symptoms. Third, we did not account for discrimination due to other factors such as gender and age. Although previous research exists on the link between discrimination and the mental health outcomes of Arab Americans, the current study was one of the first attempts to understand gender differences in these links. Using a representative sample of Arab Americans is also a point of strength in this study.
In conclusion, the current study showed that there is an association between perceived discrimination and psychological distress among Arab Americans. This study also showed major gender differences in this link, with stronger association displayed among men than women. Given the lack of research on processes and of mental health in Arab American communities, further investigation is needed to study how sociodemographic factors, identity, discrimination, acculturation, access to health care, and coping shape the psychopathology of this demographic group. Such findings have clinical and public health implications for the mental health promotion of Arab American communities.
Author Contributions
The original idea of this analysis was developed by SA; SA also analyzed the data. ML drafted the manuscript. SA and ML approved the final version of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
SA is supported by the Tam Foundation as well as the Heinz C. Prechter Bipolar Research Fund at the University of Michigan Depression Center.
Funding
This study was funded by the Russell Sage Foundation (91-03-06) as well as Andrew W. Mellon Foundation. The content of this article does not reflect the views or policies of the funding agencies.
References
1. Forsyth J, Schoenthaler A, Chaplin WF, Ogedegbe G, Ravenell J. Perceived discrimination and medication adherence in black hypertensive patients: the role of stress and depression. Psychosom Med (2014) 76(3):229–36. doi: 10.1097/PSY.0000000000000043
2. Jackson JS, Brown TN, Williams DR, Torres M, Sellers SL, Brown K. Racism and the physical and mental health status of African Americans: a thirteen year national panel study. Ethn Dis (1995) 6(1–2):132–47.
3. Pascoe EA, Smart Richman L. Perceived discrimination and health: a meta-analytic review. Psychol Bull (2009) 135(4):531. doi:10.1037/a0016059
4. Williams DR, Neighbors HW, Jackson JS. Racial/ethnic discrimination and health: findings from community studies. Am J Public Health (2003) 93(2):200–8. doi:10.2105/AJPH.93.2.200
5. Banks KH, Kohn-Wood LP, Spencer M. An examination of the African American experience of everyday discrimination and symptoms of psychological distress. Community Ment Health J (2006) 42(6):555–70. doi:10.1007/s10597-006-9052-9
6. Brondolo E, Ver Halen NB, Pencille M, Beatty D, Contrada RJ. Coping with racism: a selective review of the literature and a theoretical and methodological critique. J Behav Med (2009) 32(1):64–88. doi:10.1007/s10865-008-9193-0
7. Ong AD, Fuller-Rowell T, Burrow AL. Racial discrimination and the stress process. J Pers Soc Psychol (2009) 96(6):1259. doi:10.1037/a0015335
8. Schulz AJ, Gravlee CC, Williams DR, Israel BA, Mentz G, Rowe Z. Discrimination, symptoms of depression, and self-rated health among African American women in Detroit: results from a longitudinal analysis. Am J Public Health (2006) 96(7):1265–70. doi:10.2105/AJPH.2005.064543
9. Utsey SO, Giesbrecht N, Hook J, Stanard PM. Cultural, sociofamilial, and psychological resources that inhibit psychological distress in African Americans exposed to stressful life events and race-related stress. J Couns Psychol (2008) 55(1):49. doi:10.1037/0022-0167.55.1.49
10. Caldwell CH, Antonakos CL, Tsuchiya K, Assari S, De Loney EH. Masculinity as a moderator of discrimination and parenting on depressive symptoms and drinking behaviors among nonresident African-American fathers. Psychol Men Masc (2013) 14(1):47. doi:10.1037/a0029105
11. Soto JA, Dawson-Andoh NA, BeLue R. The relationship between perceived discrimination and generalized anxiety disorder among African Americans, Afro Caribbeans, and non-Hispanic Whites. J Anxiety Disord (2011) 25(2):258–65. doi:10.1016/j.janxdis.2010.09.011
12. Brodish AB, Cogburn CD, Fuller-Rowell TE, Peck S, Malanchuk O, Eccles JS. Perceived racial discrimination as a predictor of health behaviors: the moderating role of gender. Race Soc Probl (2011) 3(3):160–9. doi:10.1007/s12552-011-9050-6
13. Sutter M, Perrin PB. Discrimination, mental health, and suicidal ideation among LGBTQ people of color. J Couns Psychol (2016) 63(1):98–105. doi:10.1037/cou0000126
14. Stahlman S, Grosso A, Ketende S, Pitche V, Kouanda S, Ceesay N, et al. Suicidal ideation among MSM in three West African countries: associations with stigma and social capital. Int J Soc Psychiatry (2016) 62(6):522–31. doi:10.1177/0020764016663969
15. Yip T, Gee GC, Takeuchi DT. Racial discrimination and psychological distress: the impact of ethnic identity and age among immigrant and United States-born Asian adults. Dev Psychol (2008) 44(3):787–800. doi:10.1037/0012-1649.44.3.787
16. Brown TN, Williams DR, Jackson JS, Neighbors HW, Torres M, Sellers SL, et al. “Being black and feeling blue”: the mental health consequences of racial discrimination. Race Soc (2000) 2(2):117–31. doi:10.1016/S1090-9524(00)00010-3
17. Canady RB, Bullen BL, Holzman C, Broman C, Tian Y. Discrimination and symptoms of depression in pregnancy among African American and White women. Womens Health Issues (2008) 18(4):292–300. doi:10.1016/j.whi.2008.04.003
18. Foynes MM, Shipherd JC, Harrington EF. Race and gender discrimination in the Marines. Cultur Divers Ethnic Minor Psychol (2013) 19(1):111. doi:10.1037/a0030567
19. Odom EC, Vernon-Feagans L. Buffers of racial discrimination: links with depression among rural African American mothers. J Marriage Fam (2010) 72(2):346–59. doi:10.1111/j.1741-3737.2010.00704.x
20. Torres L, Ong AD. A daily diary investigation of Latino ethnic identity, discrimination, and depression. Cultur Divers Ethnic Minor Psychol (2010) 16(4):561. doi:10.1037/a0020652
21. Wagner J, Abbott G. Depression and depression care in diabetes relationship to perceived discrimination in African Americans. Diabetes Care (2007) 30(2):364–6. doi:10.2337/dc06-1756
22. Walker RL, Salami TK, Carter SE, Flowers K. Perceived racism and suicide ideation: mediating role of depression but moderating role of religiosity among African American adults. Suicide Life Threat Behav (2014) 44(5):548–59. doi:10.1111/sltb.12089
23. Basáñez T, Unger JB, Soto D, Crano W, Baezconde-Garbanati L. Perceived discrimination as a risk factor for depressive symptoms and substance use among Hispanic adolescents in Los Angeles. Ethn Health (2013) 18(3):244–61. doi:10.1080/13557858.2012.713093
24. Torres L, Driscoll MW, Voell M. Discrimination, acculturation, acculturative stress, and Latino psychological distress: a moderated mediational model. Cultur Divers Ethnic Minor Psychol (2012) 18(1):17–25. doi:10.1037/a0026710
25. Walker JL, Ruiz RJ, Chinn JJ, Marti N, Ricks TN. Discrimination, acculturation and other predictors of depression among pregnant Hispanic women. Ethn Dis (2012) 22(4):497–503.
26. Abdulrahim S, Baker W. Differences in self-rated health by immigrant status and language preference among Arab Americans in the Detroit Metropolitan Area. Soc Sci Med (2009) 68(12):2097–103. doi:10.1016/j.socscimed.2009.04.017
27. Read JG, Amick B, Donato KM. Arab immigrants: a new case for ethnicity and health? Soc Sci Med (2005) 61(1):77–82. doi:10.1016/j.socscimed.2004.11.054
28. Abdulrahim S, James SA, Yamout R, Baker W. Discrimination and psychological distress: does Whiteness matter for Arab Americans? Soc Sci Med (2012) 75(12):2116–23. doi:10.1016/j.socscimed.2012.07.030
29. Kulwicki A, Khalifa R, Moore G. The effects of September 11 on Arab American nurses in metropolitan Detroit. J Transcult Nurs (2008) 19(2):134–9. doi:10.1177/1043659607313071
30. Padela AI, Heisler M. The association of perceived abuse and discrimination after September 11, 2001, with psychological distress, level of happiness, and health status among Arab Americans. Am J Public Health (2010) 100(2):284–91. doi:10.2105/AJPH.2009.164954
31. Brondolo E, Brady N, Thompson S, Tobin JN, Cassells A, Sweeney M, et al. Perceived racism and negative affect: analyses of trait and state measures of affect in a community sample. J Soc Clin Psychol (2008) 27(2):150. doi:10.1521/jscp.2008.27.2.150
32. Clark R, Anderson NB, Clark VR, Williams DR. Racism as a stressor for African Americans: a biopsychosocial model. Am Psychol (1999) 54(10):805. doi:10.1037/0003-066X.54.10.805
33. Kessler RC, Mickelson KD, Williams DR. The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. J Health Soc Behav (1999) 40(3):208–30. doi:10.2307/2676349
34. Landrine H, Klonoff EA. The schedule of racist events: a measure of racial discrimination and a study of its negative physical and mental health consequences. J Black Psychol (1996) 22(2):144–68. doi:10.1177/00957984960222002
35. Levine DS, Himle JA, Abelson JM, Matusko N, Dhawan N, Taylor RJ. Discrimination and social anxiety disorder among African-Americans, Caribbean blacks, and non-Hispanic whites. J Nervous Ment Dis (2014) 202(3):224–30. doi:10.1097/NMD.0000000000000099
36. Williams DR, Mohammed SA. Discrimination and racial disparities in health: evidence and needed research. J Behav Med (2009) 32(1):20–47. doi:10.1007/s10865-008-9185-0
37. Assari S, Watkins DC, Caldwell CH. Race attribution modifies the association between daily discrimination and major depressive disorder among blacks: the role of gender and ethnicity. J Racial Ethn Health Disparities (2015) 2(2):200–10. doi:10.1007/s40615-014-0064-9
38. Noh S, Kaspar V. Perceived discrimination and depression: moderating effects of coping, acculturation, and ethnic support. Am J Public Health (2003) 93(2):232–8. doi:10.2105/AJPH.93.2.232
39. Coll CG, Crnic K, Lamberty G, Wasik BH, Jenkins R, Garcia HV, et al. An integrative model for the study of developmental competencies in minority children. Child Dev (1996) 67(5):1891–914. doi:10.2307/1131600
40. Cunningham M. African American adolescent males’ perceptions of their community resources and constraints: a longitudinal analysis. J Community Psychol (1999) 27(5):569–88. doi:10.1002/(SICI)1520-6629(199909)27:5<569::AID-JCOP5>3.0.CO;2-6
41. Ifatunji MA, Harnois CE. An explanation for the gender gap in perceptions of discrimination among African Americans considering the role of gender bias in measurement. Sociol Race Ethn (2015) 2(3):263–88. doi:10.1177/2332649215613532
42. Swanson DP, Cunningham M, Spencer MB. Black males’ structural conditions, achievement patterns, normative needs, and “opportunities”. Urban Educ (2003) 38(5):608–33. doi:10.1177/0042085903256218
43. Broman CL, Mavaddat R, Hsu S-y. The experience and consequences of perceived racial discrimination: a study of African Americans. J Black Psychol (2000) 26(2):165–80. doi:10.1177/0095798400026002003
44. Sellers RM, Shelton JN. The role of racial identity in perceived racial discrimination. J Pers Soc Psychol (2003) 84(5):1079. doi:10.1037/0022-3514.84.5.1079
45. Wang EA, Aminawung JA, Wildeman C, Ross JS, Krumholz HM. High incarceration rates among black men enrolled in clinical studies may compromise ability to identify disparities. Health Aff (Millwood) (2014) 33(5):848–55. doi:10.1377/hlthaff.2013.1325
46. Moore LD, Elkavich A. Who’s using and who’s doing time: incarceration, the war on drugs, and public health. Am J Public Health (2008) 98(9 Suppl):S176–80. doi:10.2105/AJPH.98.Supplement_1.S176
47. Hosoda M, Stone DL, Stone-Romero EF. The interactive effects of race, gender, and job type on job suitability ratings and selection decisions. J Appl Soc Psychol (2003) 33(1):145–78. doi:10.1111/j.1559-1816.2003.tb02077.x
48. Baker W, Stockton R, Howell S, Jamal A, Chih A, Shryock A, et al. ICPSR04413-v2. Ann Arbor, MI: Inter-University Consortium for Political and Social Research [Distributor] (2003).
49. Arab American Institute. Arab American demographics. (2009). Available from: http://www.aaiusa.org/arabamericans/22/demographics
50. Hassoun RJ. Arab Americans in Michigan. East Lansing, MI: Michigan State University Press (2005).
51. Arab American Institute. Arab Americans. Washington, DC (2003). Available from: http://www.aaiusa.org
52. Sengstock M. Chaldean Americans. (2009). Available from: http://www.everyculture.com/multi/Bu-Dr/Chaldean-Americans.html
53. Free Press. 100 Questions and Answers about Arab Americans: A Journalist’s Guide. Detroit, MI (2001). Available from: www.bintjbeil.com/E/news/100q
54. Heeringa S, Adams T. Technical Documentation: (2003) Detroit Arab American Study. Ann Arbor, MI: University of Michigan Institute for Social Research (2004).
55. Idler EL, Kasl S. Health perceptions and survival: do global evaluations of health status really predict mortality? J Gerontol (1991) 46(2):S55–65. doi:10.1093/geronj/46.2.S55
56. Ware JE Jr. Improvements in short-form measures of health status: introduction to a series. J Clin Epidemiol (2008) 61(1):1–5. doi:10.1016/j.jclinepi.2007.08.008
57. Andrews G, Slade T. Interpreting scores on the Kessler psychological distress scale (K10). Aust N Z J Public Health (2001) 25(6):494–7. doi:10.1111/j.1467-842X.2001.tb00310.x
58. Goldberg D, Williams P. A User’s Guide to the General Health Questionnaire. Windsor, England: NFER-Nelson (1988).
59. Harnois CE, Ifatunji M. Gendered measures, gendered models: toward an intersectional analysis of interpersonal racial discrimination. Ethn Racial Stud (2011) 34(6):1006–28. doi:10.1080/01419870.2010.516836
60. Beauboeuf-Lafontant T. Behind the Mask of the Strong Black Woman. Philadelphia: Temple University Press (2009).
62. Kelley RDG. Confessions of a nice Negro or why I shaved my head. In: Belton D, editor. Speak My Name: Black Men on Masculinity and the American Dream. Boston: Beacon Press (1995). p. 12–22.
64. Timberlake JM, Estes SB. Do racial and ethnic stereotypes depend on the sex of the target group members? Evidence from a survey-based experiment’. Sociol Q (2007) 48(3):399–433. doi:10.1111/j.1533-8525.2007.00083.x
65. Shih J. “Yeah, I could hire this one, but I know it’s gonna be a problem”: how race, nativity and gender affect employers’ perceptions of the manageability of job seekers’. Ethn Racial Stud (2002) 25(1):99–199. doi:10.1080/01419870120112076
66. Browne I, Misra J. The intersection of gender and race in the labor market. Annu Rev Sociol (2003) 29:487–513. doi:10.1146/annurev.soc.29.010202.100016
67. Chavous T, Harris A, Rivas D, Helaire L, Green L. Racial stereotypes and gender in context: an examination of African American college student adjustment. Sex Roles (2004) 51:1–16. doi:10.1023/B:SERS.0000032305.48347.6d
68. Van Laar C, Sidanius J. Social status and the academic achievement gap: a social dominance perspective. Soc Psychol Educ (2001) 4(3–4):235–58. doi:10.1023/A:1011302418327
69. Davis JE. Early schooling and academic achievement of African American males. Urban Educ (2003) 38(5):515–37. doi:10.1177/0042085903256220
70. Honora DT. The relationship of gender and achievement to future outlook among African American adolescents. Adolescence (2002) 37(146):301.
71. Noguera PA. The trouble with Black boys: the role and influence of environmental and cultural factors on the academic performance of African American males. Urban Educ (2003) 38(4):431–59. doi:10.1177/0042085903038004005
72. Roderick M. What’s happening to the boys? Early high school experiences and school outcomes among African American male adolescents in Chicago. Urban Educ (2003) 38(5):538–607.
73. Simpson AW, Erickson MT. Teachers’ verbal and nonverbal communication patterns as a function of teacher race, student gender, and student race. Am Educ Res J (1983) 20(2):183–98. doi:10.3102/00028312020002183
74. Richeson JA, Trawalter S. The threat of appearing prejudiced and race-based attentional biases. Psychol Sci (2008) 19(2):98–102. doi:10.1111/j.1467-9280.2008.02052.x
75. Trawalter S, Todd AR, Baird AA, Richeson JA. Attending to threat: race-based patterns of selective attention. J Exp Soc Psychol (2008) 44(5):1322–7. doi:10.1016/j.jesp.2008.03.006
76. Skinner AL, Haas IJ. Perceived threat associated with police officers and Black men predicts support for policing policy reform. Front Psychol (2016) 7:1057. doi:10.3389/fpsyg.2016.01057
77. Chekroud AM, Everett JA, Bridge H, Hewstone M. A review of neuroimaging studies of race-related prejudice: does amygdala response reflect threat? Front Hum Neurosci (2014) 8:179. doi:10.3389/fnhum.2014.00179
78. Chae DH, Nuru-Jeter AM, Adler NE. Implicit racial bias as a moderator of the association between racial discrimination and hypertension: a study of Midlife African American men. Psychosom Med (2012) 74(9):961–4. doi:10.1097/PSY.0b013e3182733665
79. Najdowski CJ, Bottoms BL, Goff PA. Stereotype threat and racial differences in citizens’ experiences of police encounters. Law Hum Behav (2015) 39(5):463–77. doi:10.1037/lhb0000140
80. Bowman PJ, Howard C. Race-related socialization, motivation, and academic achievement: a study of Black youths in three-generation families. J Am Acad Child Psychiatry (1985) 24(2):134–41. doi:10.1016/S0002-7138(09)60438-6
81. Coard SI, Wallace SA, Stevenson HC Jr, Brotman LM. Towards culturally relevant preventive interventions: the consideration of racial socialization in parent training with African American families. J Child Fam Stud (2004) 13(3):277–93. doi:10.1023/B:JCFS.0000022035.07171.f8
82. Hammond WP. Taking it like a man: masculine role norms as moderators of the racial discrimination–depressive symptoms association among African American men. Am J Public Health (2012) 102(S2):S232–41. doi:10.2105/AJPH.2011.300485
83. Thomas AJ, Witherspoon KM, Speight SL. Gendered racism, psychological distress, and coping styles of African American women. Cultur Divers Ethnic Minor Psychol (2008) 14(4):307. doi:10.1037/1099-9809.14.4.307
84. Mensch BS, Ibrahim BL, Lee SM, el-Gibaly O. Gender-role attitudes among Egyptian adolescents. Stud Fam Plann (2003) 34(1):8–18. doi:10.1111/j.1728-4465.2003.00008.x
85. Jaffer YA, Afifi MM. Adolescent reproductive health and gender role attitudes in Oman. Saudi Med J (2005) 26(2):234–40.
86. Sayed H, El-Zanaty F. Male role in decision making in Egypt. Paper Presented at the annual International Union for the Scientific Study of Population (IUSSP) Conference; 24 August–1 September. Montreal (1993).
87. Kandiyoti D. The paradoxes of masculinity: some thoughts on segregated societies. In: Cornwall A, Lindisfarne N, editors. Dislocating Masculinity: Comparative Ethnographies. London; New York: Routledge (1994). p. 197–213.
88. Rugh A. Within the Circle: Parents and Children in an Arab Village. New York: Columbia University Press (1997).
89. Davis SS, Davis DA. Adolescence in a Moroccan Town: Making Social Sense. New Brunswick, NJ: Rutgers University Press (1989).
90. Brondolo E, Monge A, Agosta J, Tobin JN, Cassells A, Stanton C, et al. Perceived ethnic discrimination and cigarette smoking: examining the moderating effects of race/ethnicity and gender in a sample of Black and Latino urban adults. J Behav Med (2015) 38(4):689–700. doi:10.1007/s10865-015-9645-2
91. McLaughlin KA, Hatzenbuehler ML, Keyes KM. Responses to discrimination and psychiatric disorders among Black, Hispanic, female, and lesbian, gay, and bisexual individuals. Am J Public Health (2010) 100(8):1477–84.
92. Banyard VL, Graham-Bermann SA. A gender analysis of theories of coping with stress. Psychol Women Q (1993) 17(3):303–18. doi:10.1111/j.1471-6402.1993.tb00489.x
93. Everett JE, Hall JC, Hamilton-Mason J. Everyday conflict and daily stressors: coping responses of Black women. Affilia (2010) 25(1):30–42. doi:10.1177/0886109909354983
94. Lewis JA, Mendenhall R, Harwood SA, Huntt MB. Coping with gendered racial microaggressions among Black women college students. J Afr Am Stud (2013) 17(1):51–73. doi:10.1007/s12111-012-9219-0
95. Shorter-Gooden K. Multiple resistance strategies: how African American women cope with racism and sexism. J Black Psychol (2004) 30(3):406–25. doi:10.1177/0095798404266050
Keywords: Arab Americans, gender, discrimination, psychological symptoms, distress
Citation: Assari S and Lankarani MM (2017) Discrimination and Psychological Distress: Gender Differences among Arab Americans. Front. Psychiatry 8:23. doi: 10.3389/fpsyt.2017.00023
Received: 05 December 2016; Accepted: 31 January 2017;
Published: 20 February 2017
Edited by:
Mercedes Lovrecic, National Institute of Public Health, SloveniaReviewed by:
Sebastian Fischer, Leuphana University, GermanyRohan Dexter Jeremiah, University of Illinois at Chicago, USA
Copyright: © 2017 Assari and Lankarani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shervin Assari, YXNzYXJpQHVtaWNoLmVkdQ==