
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Psychiatry , 30 January 2017
Sec. Public Mental Health
Volume 8 - 2017 | https://doi.org/10.3389/fpsyt.2017.00010
This article is part of the Research Topic Computers and games for mental health and well-being View all 35 articles
 Rosa M. Baños1,2,3*
Rosa M. Baños1,2,3* Ernestina Etchemendy1,2,4
Ernestina Etchemendy1,2,4 Adriana Mira2,5
Adriana Mira2,5 Giuseppe Riva6,7
Giuseppe Riva6,7 Andrea Gaggioli6,7
Andrea Gaggioli6,7 Cristina Botella1,2,5
Cristina Botella1,2,5
Numerous studies have shown an alarming prevalence of depression, anxiety, and behavior disorders in youth. Thus, prevention of psychological problems in this population becomes crucial. According to the World Health Organization (1), prevention should also include the promotion and development of the individual’s strengths in order to reduce vulnerability to suffering from mental disorders. In addition, other key elements of prevention are the reach, adoption, implementation, and maintenance of interventions. The information and communication technologies, especially the Internet, have much to offer in terms of the prevention and promotion of positive mental health in adolescents. This paper reviews these fields of research—prevention, positive psychology, Internet, and adolescents—and discusses the potential of positive interventions delivered over the Internet as effective and sustainable health promotion tools. The paper provides a brief description of the systems developed so far and a summary of selected features of the studies detected in the literature review. The overall conclusions are that there is a need for more controlled studies with long-term follow-ups, the interventions should be designed considering the specific features of the target users and the specific contexts where the interventions will be delivered, and they could be enhanced by the use of other technologies, such as smartphones, sensors, or social networks.
Mental health disorders represent a large proportion of the disease burden (2), decreasing quality of life, and increasing the vulnerability to developing severe disabling diseases. Moreover, they have an important economic impact on society (career, family cost, low productivity, etc.) (3, 4). For the adolescent population, these problems take on special importance. Numerous studies have shown an alarming prevalence of depression, anxiety, and behavior disorders in youth (5, 6), and both retrospective and prospective research has shown that most adulthood psychiatric disorders begin in childhood and adolescence (7–10).
Estimates indicate that about 10–20% of children and adolescents suffer from mental health problems worldwide, but large differences in prevalence estimates across countries have also been noted (1). Thus, prevention of psychological problems in the youth population is crucial, and the promotion of young people’s mental health and well-being is considered a key priority in the EU Framework for Action and H2020 (11). Evidence shows that mental illness can be prevented in both adult and youth populations (12–15), and that intervening during childhood and adolescence maximizes the benefits of prevention tasks (16, 17).
According to the World Health Organization (1), prevention involves different actions aimed to reduce risk factors, interrupt the disease’s progress, and reduce its consequences. However, mental health is more than just the absence of mental illness; instead, it is “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively, and is able to make a contribution to his or her community …” [(18), p.1]. Mental health also implies a positive emotional state, positive expectations for the future, and an adaptive way of interpreting reality (19). Therefore, prevention should also include the promotion and development of the individual’s strengths, encouraging protective variables that empower the person and act as barriers and shields that can reduce vulnerability to suffering from mental disorders (1).
Evidence points out that some human strengths act as buffers against mental illness (20). Nevertheless, literature on adolescents and a prevention approach addressed to fostering individual strengths and protective variables, such as resilience, optimism, and positive emotions, is scarce (21). Although support for interventions designed to enhance these variables in adolescence is steadily growing, more research is needed (22).
Another key element of prevention involves reaching as many people in need as possible (23). The information and communication technologies (ICTs), especially the Internet and mobile devices, offer important advantages for reaching different target groups (24). ICTs offer accessibility with an attractive cost-effective relationship for the challenges of mental disorders and prevention.
In the case of adolescents, these advantages have even greater potential because they are considered “digital natives.” Therefore, this population is not as hindered by potential obstacles and barriers, such as acceptability of technology, self-concordance, digital format, etc. Most adolescents are fully immersed in digital worlds, and their activities, relationships, and concerns are being defined by technologies.
In sum, ICTs can offer several advantages for fostering individual competencies, resources, and psychological strengths during adolescence. However, this area of research has hardly been considered. Thus, this paper seeks to contribute to this research gap and clarify the current state of the art. The paper starts with an explanation of the role of positive psychology (PP) in preventing mental health problems and promoting well-being and resilience in the adolescent population. Then, it presents an overview of the advantages of ICTs, specifically focusing on delivering mental health interventions for youth via the Internet. Finally, the results of a literature review combining the three fields of research—PP and Internet interventions in youth—are presented, providing a brief description of the systems developed so far and a summary of selected features of these studies.
Positive psychology is the study of the conditions and processes that contribute to the flourishing or optimal functioning of people, groups, and institutions (25). Its main areas of study can be grouped in four categories (26): (a) positive emotions (e.g., happiness, flow, etc.) and their effects on psychological and physical functioning; (b) positive individual traits (e.g., values, talents, etc.) and their protective role in different physical and psychological disorders; (c) positive interpersonal relationships (e.g., friendship, marriage, etc.); and (d) positive institutions (e.g., family, school, business, etc.).
Positive psychology has also been interested in the development of positive psychology interventions (PPIs). Sin and Lyubomirsky (27) defined them as intentional activities specifically addressed to cultivate positive feelings, cognition, and behaviors. PPIs are exercises (e.g., counting your blessings, practicing kindness, expressing gratitude, using personal strengths, etc.), which have demonstrated empirically to increase positive emotions, satisfaction with life, or other positive states. In this sense, PPIs are not activities focused on remedying or healing pathological or negative aspects, but on contributing to well-being and health through activities aimed to enhance positive affect, cognitions, and behaviors, and they may be considered as a complementary strategy in mental health promotion and treatment (28).
Currently, there is substantial evidence about their effectiveness in improving well-being, reducing depressive symptoms (27, 28), and increasing the effectiveness of available psychological treatments (29). PPIs have also emerged as promising tools in the promotion and prevention of mental health (30–33).
Due to the high prevalence of emotional problems in young people worldwide (7), skills for improving well-being and happiness should be taught to teenagers as well (34, 35). Adolescence is an optimal stage to do this because it is a crucial period in human personal and emotional development (identity construction, social relationships, etc.). PP tries to create a fresh conceptual framework that allows the development of interventions focused on human strengths and individuals’ potential, rather than on their deficits or the troubled image traditionally associated with adolescence (34). However, it is necessary to further investigate the development and application of PP interventions in young people because the evidence is still scarce (36–38). Research with PPIs has mostly been carried out with adult populations (28), and although some studies have shown the effectiveness of PPIs in increasing well-being in adolescents (39, 22), the need for more specific knowledge about the application of PPIs in the young population is evident (22).
The use of ICTs to enhance health services is increasing due to numerous advantages they offer to the health-care system. Increased accessibility to interventions, reliability (efficacy/effectiveness), and financial efficiency in health-care systems have been identified as relevant benefits of e-health in different studies (40–43). Its contributions to the five dimensions postulated by the RE-AIM model (reach, efficacy/effectiveness, adoption, implementation, and maintenance), a framework extensively used to assess the public health impact of interventions (44), are supported by a large body of literature. Moreover, in the case of adolescents, ICTs facilitate access to their habits, culture, communications, social connection, etc. (45, 46). A comprehensive report elaborated in 2010 detected that young people consume technological devices for at least the same amount of time an adult spends daily at his/her work place, they use ICTs 7 days a week, and several devices simultaneously (47). Therefore, using ICTs to approach adolescents could facilitate the implementation of preventive interventions. Recent studies highlight the advantages of technologies to engage this population, monitor their behaviors, and provide them with information, interventions, etc., although literature on effectiveness is limited (48–50).
The brief duration of PPIs makes them good candidates for administration over the Internet, and online administration improves their dissemination. Proposals have been made to capture the fruitful relationship between PPIs and ICTs, and different terms have been suggested. Mitchell et al. (51) offered the term online positive psychological intervention and defended the potential of these interventions as an effective and sustainable health promotion tool within a comprehensive approach to mental health care. Riva et al. (52) and Botella et al. (53) proposed the term Positive Technologies to refer to the “scientific and applied approach that uses the technology for improving the quality of our personal experience with the goal of increasing wellness, and generating strengths and resilience in individuals, organizations, and society” [(53), pp. 1]. This field tries to combine and enhance the objectives of PP using all the possibilities offered by ICTs. Currently, there is already evidence of the effectiveness of these positive technologies in adult populations (28, 51), For example, Baños et al. (54) reported positive results of a self-guided Internet intervention to induce positive emotions and reinforce psychological resources. Shapira and Mongrain (55) also tested positively the effectiveness of two online exercises to help individuals experience self-compassion and optimism. Gander et al. (56) reported the impact of nine strengths-based positive interventions on well-being and depression in an Internet-based randomized placebo-controlled study, and these authors also offered data about the efficacy of PPIs via the Internet for older age groups (57). However, little work has been done in adolescence. Whereas there is a range of Internet-based well-being programs based on PP available to the general public (28, 51), there are not many Internet interventions specifically designed to promote well-being and resilience in adolescents and youth.
The present study conducts a narrative review that describes and discusses the state of the art of this field. Specifically, the purpose of this paper is to review the scientific literature on PPIs delivered through technological systems for promoting health and well-being in adolescent and youth populations.
In April 2016, a bibliographic search was conducted on the PsychINFO and PubMed databases. In addition, experts in the field were contacted for information on relevant material. Studies were eligible if: they have been focused on prove the efficacy of an online PPI to promote well-being and resilience in adolescent population; they were published until April 2016; they were English studies, and they were randomized controlled trials (RCTs). Studies were excluded if they were review articles. The search was limited to RCTs because a recent meta-analysis suggested that effectiveness of PPIs could be overestimated in not controlled studies (28). The key terms used were: “Positive Psychology” OR well-being OR wellbeing OR resilience OR happiness AND adolescent OR youth OR teenager AND “Internet intervention” OR online OR “Internet-based” OR “web-based” AND prevention OR “mental health.” Two independent evaluators reviewed and selected the studies. Those who were finally selected were reviewed by a third expert evaluator. Finally seven studies were identified about Internet-based PP programs for adolescents and youth. Consultation with international experts in the area identified one additional study (58), and one unpublished doctoral thesis (59) (Figure 1).
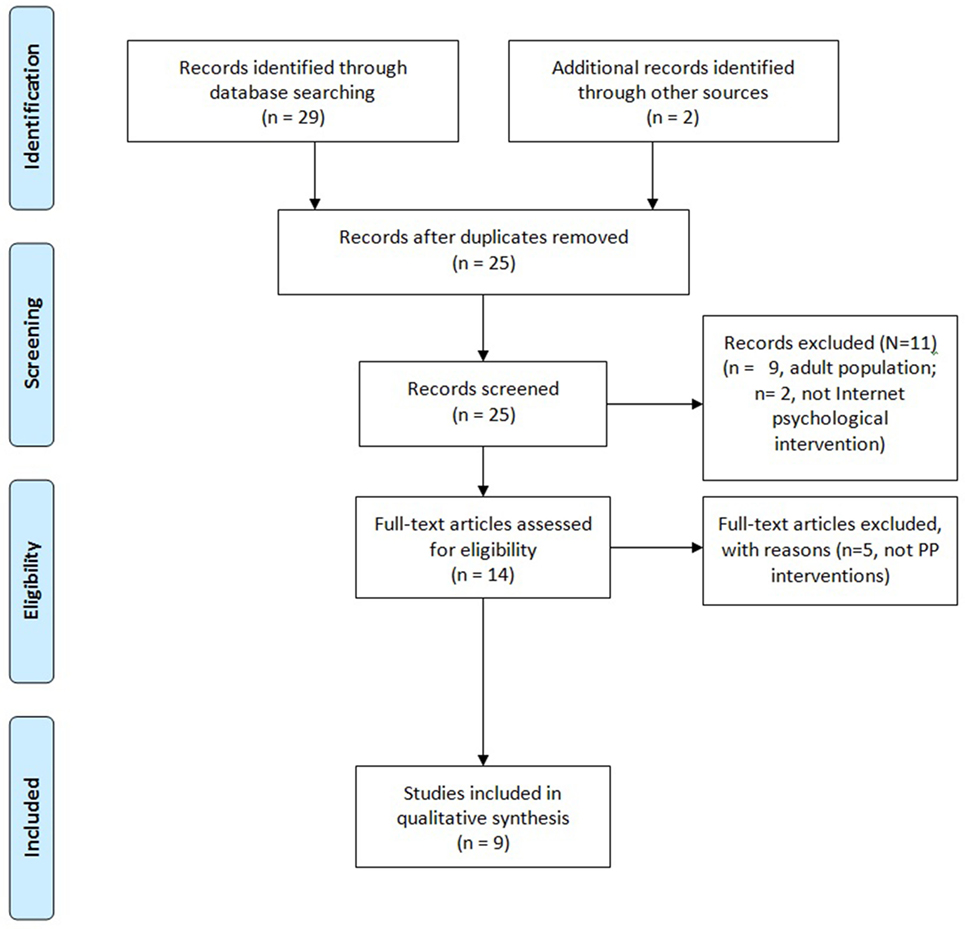
Figure 1. Flow chart.
The literature review identified seven technological systems that include PPIs to promote well-being in adolescent and youth populations, which efficacy was tested in nine studies. All studies used a website to deliver the PPIs, one study also used social network (Facebook) and email (60), and another one also used text messages reminders (61). Regarding the efficacy of the interventions, in general all studies showed positive results, decreasing anxiety and depression scores, and increasing well-being.
A brief description of the systems and a summary of these studies are presented in Table 1.
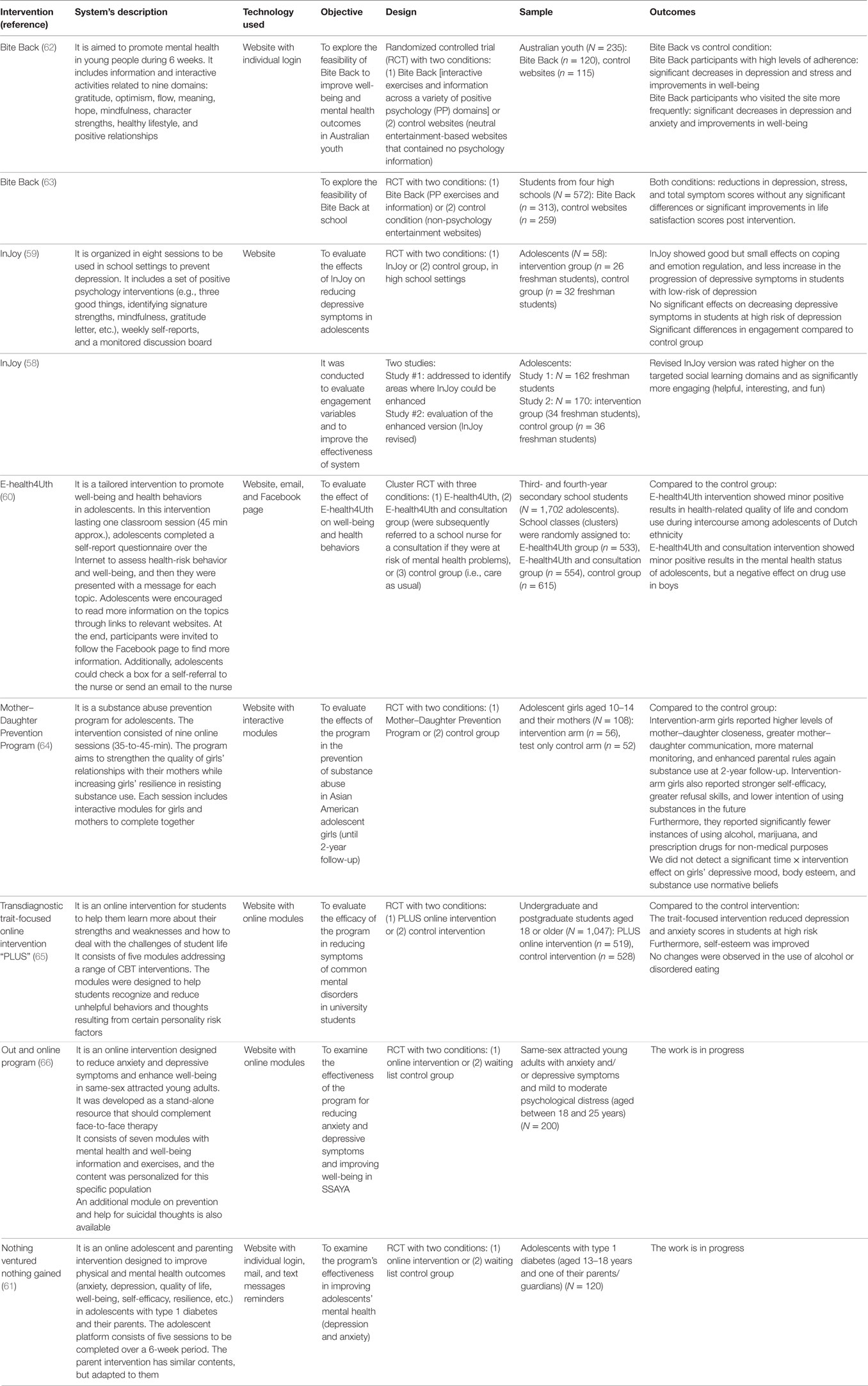
Table 1. Summary of findings.
Only seven ICT-based PPI for promoting health and well-being in adolescent and youth populations were identified in the literature review, and only nine studies testing their efficacy. Therefore, our first conclusion is that more controlled studies are needed. Furthermore, no longitudinal studies were identified, and these ICT-based prevention interventions should also prove their effectiveness through longitudinal studies that can clearly demonstrate whether the protective factors (virtues, strengths, etc.) are maintained in adulthood. Only one intervention (Mother–Daughter Prevention Program) reported data from a 2-year follow-up (64).
Another conclusion has to do with the design of the ICT-based PPIs. They should be designed considering the specific features of the target users. Both the contents (language, instructions, images, etc.) and other format and design elements are crucial in engaging teens. For example, InJoy was modified to improve its effectiveness and enhance its ability to engage. Compared to the initial version, the recent one was rated higher by students on the targeted social learning domains and found to be significantly more engaging (helpful, interesting, and fun) (58). Another example of adapting the systems to young people’s characteristics is the use of Internet social networks. E-health4Uth uses social networks (Facebook). The use of these resources could increase the attractiveness of these programs for young people and their adherence to them (47).
This review also identifies the importance of considering the contexts where the interventions will be delivered. For example, Bite Black was not more effective than the control task when used in schools, perhaps because teens perceived the application as an additional “school task” (63). This finding suggests the need to explore which technological systems and which PPIs best fit the different settings (school, family, leisure, etc.). Schools offer the possibility of reaching a large number of users, but the adaptation of interventions to increase their effectiveness should be considered.
Another relevant issue is the role of different technologies to deliver PPIs. Technological advances, especially related to smartphones, sensors, and virtual/augmented reality in daily life, could be very useful in promoting well-being. In our revision, it draws attention the limited number of ICTs used. It is important to explore this field because young people use ICTs every day through several mobile devices simultaneously (47) and this trend is expected that increases in the coming years. Currently, smartphones are main channels of communication, socialization, and entertainment for adolescents, and therefore to use them as devices to deliver PPIs could be appropriate. In this review, no system uses mobile phone resources to carry out the interventions and nurture interpersonal relationships. However, since smartphones or similars were not considered as keywords it is possible that some systems were not detected. This is a limitation in our search that should be considered.
This paper focuses on the benefits of using ICT-based PPIs to promote wellbeing in adolescents and youth. However, it should be highlighted that these interventions could also have some negative effects and potential dangers, if misused. It is necessary to be cautious when designing a prevention program, as people with more severe mental disorders might consider these programs to be substitutes to psychological treatments. In addition, other important aspects should also be taken into account in the e-mental health field (67), including confidentiality, privacy, and rigor of contents. Further work needs to consider all these issues, because despite limitations and potential dangers, ICT-based PPIs offer new mental health opportunities, especially for adolescents, and important benefits in terms of sustainability and accessibility. This review shows that some controlled studies have already been conducted, but much more research is required to establish the efficacy of these preventive interventions, including long-term follow-up studies. Successful prevention of mental disorders and mental health promotion are priorities worldwide, and ICTs can be a great ally, especially among young people.
All authors (RB, EK, AM, GR, AG, and CB) jointly contributed to write the manuscript and all of them approved the final version for submission. Literature search has been done by EK and AM. Studies selected were reviewed by a third expert evaluator (RB). All authors contribute to the discussion of the literature review.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This study was funded in part by the Excellence in Research Program PROMETEO II (Generalitat Valenciana, Conselleria de Educación, 2013/003) and CIBER of Physiopathology of Obesity Nutrition, an initiative of ISCIII (ISC III CB06 03/0052).
1. World Health Organization. Prevention of Mental Disorders: Effective Interventions and Policy Options: Summary Report/a Report of the World Health Organization Department of Mental Health and Substance Abuse; in Collaboration with the Prevention Research Centre of the Universities of Nijmegen and Maastricht. Geneva: World Health Organization (2004).
2. Mihalopoulos C, Vos T, Pirkis J, Carter R. The economic analysis of prevention in mental health programs. Annu Rev Clin Psychol (2011) 7:169–201. doi: 10.1146/annurev-clinpsy-032210-104601
3. Merikangas KR, Kalaydjian A. Magnitude and impact of comorbidity of mental disorders from epidemiologic surveys. Curr Opin Psychiatry (2007) 20(4):353–8. doi:10.1097/YCO.0b013e3281c61dc5
4. Luppa M, Heinrich S, Angermeyer MC, König H-H, Riedel-Heller SG. Cost-of-illness studies of depression: a systematic review. J Affect Disord (2007) 98(1–2):29–43. doi:10.1016/j.jad.2006.07.017
5. Costello E, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch Gen Psychiatry (2003) 60(8):837. doi:10.1001/archpsyc.60.8.837
6. Merikangas KR, Nakamura EF, Kessler RC. Epidemiology of mental disorders in children and adolescents. Dialogues Clin Neurosci (2009) 11(1):7–20.
7. Copeland W, Shanahan L, Costello EJ, Angold A. Cumulative prevalence of psychiatric disorders by young adulthood: a prospective cohort analysis from the Great Smoky Mountains Study. J Am Acad Child Adolesc Psychiatry (2011) 50(3):252–61. doi:10.1016/j.jaac.2010.12.014
8. Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, Ustün TB. Age of onset of mental disorders: a review of recent literature. Curr Opin Psychiatry (2007) 20(4):359–64. doi:10.1097/YCO.0b013e32816ebc8c
9. Kessler R, Berglund P, Demler O, Jin R, Merikangas K, Walters E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry (2005) 62(6):593. doi:10.1001/archpsyc.62.6.593
10. Kim-Cohen J, Caspi A, Moffitt T, Harrington H, Milne B, Poulton R. Prior juvenile diagnoses in adults with mental disorder. Arch Gen Psychiatry (2003) 60(7):709. doi:10.1001/archpsyc.60.7.709
11. Stengård E, Appelqvist-Schmidlechner K. Mental Health Promotion in Young People – An Investment for the Future. Copenhagen: World Health Organisation (2010).
12. Calear AL, Christensen H. Review of internet-based prevention and treatment programs for anxiety and depression in children and adolescents. Med J Aust (2010) 192(11):12.
13. Cuijpers P, Beekman A, Reynolds C. Preventing depression. JAMA (2012) 307(10):1033. doi:10.1001/jama.2012.271
14. Muñoz RF, Cuijpers P, Smit F, Barrera A, Leykin Y. Prevention on major depression. Annu Rev Clin Psychol (2010) 6:181–212. doi:10.1146/annurev-clinpsy-033109-132040
15. van Zoonen K, Buntrock C, Ebert D, Smit F, Reynolds C, Beekman A, et al. Preventing the onset of major depressive disorder: a meta-analytic review of psychological interventions. Int J Epidemiol (2014) 43(2):318–29. doi:10.1093/ije/dyt175
16. Gladstone T, Beardslee W, O’Connor E. The prevention of adolescent depression. Psychiatr Clin North Am (2011) 34(1):35–52. doi:10.1016/j.psc.2010.11.015
17. O’Connell M, Boat T, Warner K. Preventing Mental, Emotional, and Behavioral Disorders among Young People. Washington, DC: National Academies Press (2009).
18. World Health Organization. Mental Health: Strengthening Our Response. (2014). Available from: http://www.who.int/mediacentre/factsheets/fs220/en/
19. Edmondson OJH, MacLeod AK. Psychological well-being and anticipated positive personal events: their relationship to depression. Clin Psychol Psychother (2015) 22(5):418–25. doi:10.1002/cpp.1911
20. Joseph S. Positive Psychology in Practice: Promoting Human Flourishing In Work, Health, Education, and Everyday Life. Hoboken: John Wiley & Sons, Inc (2015).
21. Huebner ES, Gilman R, Furlong MJ. A conceptual model for research in positive psychology in children and youth. In: Gilman R, Huebner ES, Furlong MJ, editors. Handbook of Positive Psychology in Schools. New York: Routledge (2009). p. 3–8.
22. Norrish JM, Vella-Brodrick DA. Positive psychology and adolescents: where are we now? Where to from here? Aust Psychol (2009) 44(4):270–8. doi:10.1080/00050060902914103
23. Barak A, Hen L, Boniel-Nissim M, Shapira N. A comprehensive review and a meta-analysis of the effectiveness of internet-based psychotherapeutic interventions. J Techno Hum Serv (2008) 26(2–4):109–60. doi:10.1080/15228830802094429
24. Griffiths KM, Christensen H. Internet-based mental health programs: a powerful tool in the rural medical kit. Aust J Rural Health (2007) 15(2):81–7. doi:10.1111/j.1440-1584.2007.00859.x
25. Seligman M, Csikszentmihalyi M. Positive psychology: an introduction. Am Psychol (2000) 55(1):5–14. doi:10.1037//0003-066x.55.1.5
26. Park N, Peterson C, Sun JK. La psicología positiva: investigación y aplicaciones. Terapia Psicologica (2013) 31(1):11–9. doi:10.4067/S0718-48082013000100002
27. Sin NL, Lyubomirsky S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J Clin Psychol (2009) 65(5):467–87. doi:10.1002/jclp.20593
28. Bolier L, Haverman M, Westerhof GJ, Riper H, Smit F, Bohlmeijer E. Positive psychology interventions: a meta-analysis of randomized controlled studies. BMC Public Health (2013) 13(1):119. doi:10.1186/1471-2458-13-119
30. Barry MM. Promoting positive mental health: theoretical frameworks for practice. Int J Ment Health Promot (2001) 3(1):25–34.
31. Fava GA, Ruini C, Rafanelli C, Finos L, Salmaso L, Mangelli L, et al. Well-being therapy of generalized anxiety disorder. Psychother Psychosom (2005) 74(1):26–30. doi:10.1159/000082023
32. Seligman MEP, Rashid T, Parks A. Positive psychotherapy. Am Psychol (2006) 8:774–88. doi:10.1037/0003-066X.61.8.774
33. Vázquez C, Hervás G, Ho SMY. Intervenciones clínicas basadas en la psicología positiva: Fundamentos y aplicaciones. Psicología Conductual (2006) 14:401–32.
34. Giménez M, Vázquez C, Hervás G. El análisis de las fortalezas psicológicas en la adolescencia: Más allá de los modelos de vulnerabilidad. Psychol Soc Educ (2010) 2(2):97–116.
35. Seligman MEP, Ernst RM, Gillham J, Reivich K, Linkins M. Positive education: positive psychology and classroom interventions. Oxf Rev Educ (2009) 35(3):293–311. doi:10.1080/03054980902934563
36. Austin DB. The Effects of a Strengths Development Intervention Program upon the Self Perception of Students’ Academic Abilities. (2005). Available from: http://ir.library.oregonstate.edu/xmlui/handle/1957/30550
37. Froh JJ, Sefick WJ, Emmons RA. Counting blessings in early adolescents: an experimental study of gratitude and subjective well-being. J Sch Psychol (2008) 46(2):213–33. doi:10.1016/j.jsp.2007.03.005
38. Otake K, Shimai S, Tanaka-Matsumi J, Otsui K, Fredrickson BL. Happy people become happier through kindness: a counting kindnesses intervention. J Happiness Stud (2006) 7(3):361–75. doi:10.1007/s10902-005-3650-z
39. Haworth CM, Nelson SK, Layous K, Carter K, Bao KJ, Lyubomirsky S, et al. Stability and change in genetic and environmental influences on well-being in response to an intervention. Plos one (2016) 11(5):e0155538. doi:10.1371/journal.pone.0155538
40. Andersson G. Internet-delivered psychological treatments. Annu Rev Clin Psychol (2016) 12:157–79. doi:10.1146/annurev-clinpsy-021815-093006
41. Johansson R, Andersson G. Internet-based psychological treatments for depression. Expert Rev Neurother (2012) 12(7):861–9. doi:10.1586/ern.12.63
42. Richards D, Richardson T. Computer-based psychological treatments for depression: a systematic review and meta-analysis. Clin Psychol Rev (2012) 32(4):329–42. doi:10.1016/j.cpr.2012.02.004
43. World Health Organization. Atlas of Ehealth Country Profile: The Use of Ehealth in Support of Universal Health Coverage: Based on the Findings of the Third Global Survey on Ehealth 2015. Geneva, Switzerland: WHO Library Cataloguing-in-Publication Data (2016).
44. Glasgow R, McKay H, Piette J, Reynolds K. The RE-AIM framework for evaluating interventions: what can it tell us about approaches to chronic illness management? Patient Educ Couns (2001) 44(2):119–27. doi:10.1016/s0738-3991(00)00186-5
45. Giedd J. The digital revolution and adolescent brain evolution. J Adolesc Health Care (2012) 51(2):101–5. doi:10.1016/j.jadohealth.2012.06.002
46. Hyden C, Cohall A. Innovative approaches to using new media and technology in health promotion for adolescents and young adults. Adolesc Med State Art Rev (2011) 22(3):498–520.
47. Rideout VJ, Foehr UG, Roberts D. Generation M: Media in the Lives of 8- to 18-Year-Olds: A Kaiser Family Foundation Study. California: The Henry J. Kaiser Family Foundation (2010).
48. Struthers A, Charette C, Bapuji SB, Winters S, Ye X, Metge C, et al. The acceptability of e-mental health services for children, adolescents, and young adults: a systematic search and review. Can J Commun Ment Health (2015) 34(2):1–21. doi:10.7870/cjcmh-2015-006
49. Ye X, Bapuji S, Winters S, Struthers A, Raynard M, Metge C, et al. Effectiveness of internet-based interventions for children, youth, and young adults with anxiety and/or depression: a systematic review and meta-analysis. BMC Health Serv Res (2014) 14(1):313. doi:10.1186/1472-6963-14-313
50. Yonker LM, Zan S, Scirica CV, Jethwani K, Kinane TB. “Friending” teens: systematic review of social media in adolescent and young adult health care. J Med Internet Res (2015) 17(1):e4. doi:10.2196/jmir.3692
51. Mitchell J, Vella-Brodrick D, Klein B. Positive psychology and the internet: a mental health opportunity. SENSORIA (2010) 6(2):30–41. doi:10.7790/ejap.v6i2.230
52. Riva G, Baños RM, Botella C, Wiederhold BK, Gaggioli A. Positive technology: using interactive technologies to promote positive functioning. Cyberpsychol Behav Soc Netw (2012) 15(2):69–77. doi:10.1089/cyber.2011.0139
53. Botella C, Riva G, Gaggioli A, Wiederhold BK, Alcañiz M, Baños RM. The present and future of positive technologies. Cyberpsychol Behav Soc Netw (2012) 15(2):78–84. doi:10.1089/cyber.2011.0140
54. Baños RM, Etchmendy E, Farfallini L, García-Palacios A, Quero S, Botella C. EARTH of well-being system: a pilot study of an information and communication technology-based positive psychology intervention. The J Positive Psychol (2014) 9(6):482–8. doi:10.1080/17439760.2014.927906
55. Shapira LH, Mongrain M. The benefits of self-compassion and optimism exercises for individuals vulnerable to depression. J Posit Psychol (2010) 5:377–89. doi:10.1080/17439760.2010.516763
56. Gander F, Proyer RT, Ruch W, Wyss T. Strength-based positive interventions: further evidence for their potential in enhancing well-being and alleviating depression. J Happiness Stud (2013) 14124:1–1259. doi:10.1007/s10902-012-9380-0
57. Proyer RT, Gander F, Wellenzohn S, Ruch W. Positive psychology interventions in people aged 50–79 years: long-term effects of placebo-controlled online interventions on well-being and depression. Aging Ment Health (2014) 18:997–1005. doi:10.1080/13607863.2014.899978
58. Redzic NM, Taylor K, Chang V, Trockel M, Shorter A, Taylor CB. An internet-based positive psychology program: strategies to improve effectiveness and engagement. J Posit Psychol (2014) 9(6):494–501. doi:10.1080/17439760.2014.936966
59. Redzic NM. The Effects of an Internet-Based Psychoeducational Program On Reducing Depressive Symptoms in Adolescents. ProQuest Dissertations & Theses A&I (1435619958) (2012). Available from: http://search.proquest.com/docview/1435619958?accountid=14777
60. Bannink R, Broeren S, Joosten-van Zwanenburg E, van As E, van de Looij-Jansen P, Raat H. Effectiveness of a web-based tailored intervention (E-health4Uth) and consultation to promote adolescents’ health: randomized controlled trial. J Med Internet Res (2014) 16(5):e143. doi:10.2196/jmir.3163
61. Hackworth NJ, Matthews J, Burke K, Petrovic Z, Klein B, Northam EA, et al. Improving mental health of adolescents with type 1 diabetes: protocol for a randomized controlled trial of the nothing ventured nothing gained online adolescent and parenting support intervention. BMC Public Health (2013) 13(1):1. doi:10.1186/1471-2458-13-1185
62. Manicavasagar V, Horswood D, Burckhardt R, Lum A, Hadzi-Pavlovic D, Parker G. Feasibility and effectiveness of a web-based positive psychology program for youth mental health: randomized controlled trial. J Med Internet Res (2014) 16(6):e140. doi:10.2196/jmir.3176
63. Burckhardt R, Manicavasagar V, Batterham PJ, Miller LM, Talbot E. A web-based adolescent positive psychology program in schools: randomized controlled trial. J Med Internet Res (2015) 17:7. doi:10.2196/jmir.4329
64. Fang L, Schinke SP. Two-year outcomes of a randomized, family-based substance use prevention trial for Asian American adolescent girls. Psychol Addict Behav (2013) 27(3):788. doi:10.1037/a0030925
65. Musiat P, Conrod P, Treasure J, Tylee A, Williams C, Schmidt U. Targeted prevention of common mental health disorders in university students: randomised controlled trial of a transdiagnostic trait-focused web-based intervention. PLoS One (2014) 9(4):e93621. doi:10.1371/journal.pone.0093621
66. Abbott JAM, Klein B, McLaren S, Austin DW, Molloy M, Meyer D, et al. Out & online; effectiveness of a tailored online multi-symptom mental health and wellbeing program for same-sex attracted young adults: study protocol for a randomised controlled trial. Trials (2014) 15(1):1. doi:10.1186/1745-6215-15-504
Keywords: adolescents, mental health, prevention, positive psychology, online interventions, Internet
Citation: Baños RM, Etchemendy E, Mira A, Riva G, Gaggioli A and Botella C (2017) Online Positive Interventions to Promote Well-being and Resilience in the Adolescent Population: A Narrative Review. Front. Psychiatry 8:10. doi: 10.3389/fpsyt.2017.00010
Received: 29 July 2016; Accepted: 13 January 2017;
Published: 30 January 2017
Edited by:
Stéphane Bouchard, Université du Québec en Outaouais, CanadaReviewed by:
Caroline Vandeleur, Centre hospitalier universitaire vaudois, SwitzerlandCopyright: © 2017 Baños, Etchemendy, Mira, Riva, Gaggioli and Botella. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosa M. Baños, YmFub3NAdXYuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.