 Katharina Bachmann
Katharina Bachmann Alexandra P. Lam
Alexandra P. Lam Alexandra Philipsen1,2,3*
Alexandra Philipsen1,2,3*

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Psychiatry , 27 June 2016
Sec. Neuroimaging
Volume 7 - 2016 | https://doi.org/10.3389/fpsyt.2016.00117
This article is part of the Research Topic Third-generation neuroimaging: translating research into clinical utility View all 22 articles
Attention-deficit/hyperactivity disorder (ADHD) is a recognized serious mental disorder that often persists into adulthood. The symptoms and impairments associated with ADHD often cause significant mental suffering in affected individuals. ADHD has been associated with abnormal neuronal activity in various neuronal circuits, such as the dorsofrontostriatal, orbitofrontostriatal, and frontocerebellar circuits. Psychopharmacological treatment with methylphenidate hydrochloride is recommended as the first-line treatment for ADHD. It is assumed that medication ameliorates ADHD symptoms by improving the functioning of the brain areas affected in the condition. However, side effects, contraindications, or non-response can limit the effectiveness of a psychopharmacological treatment for ADHD. It is therefore necessary to develop non-pharmacological interventions that target neuronal mechanisms associated with the condition in the same way as pharmacological treatment. We think that mindfulness meditation employed as a neuropsychotherapeutic intervention could help patients with ADHD to regulate impaired brain functioning and thereby reduce ADHD symptoms. In this paper, we highlight the mechanisms of such mindfulness meditation, and thus provide a rationale for further research and treatment development from a neuropsychotherapeutic perspective. We conclude that mindfulness meditation employed as a neuropsychotherapeutic intervention in therapy is a promising treatment approach in ADHD.
Attention deficit/hyperactivity disorder (ADHD) is a serious mental disorder characterized by three core symptoms: inattention, impulsivity, and hyperactivity. In up to 60% of cases, ADHD symptoms persist into adulthood (1). It has been estimated that about 3.4% of the adult population is affected by ADHD (2). The clinical picture of the condition is quite heterogeneous with respect to the expression and severity of symptoms, as well as its pathogenesis (3, 4).
It is assumed that the disorder relies strongly on impairments to neurobiological function (5, 6). Individuals with ADHD show abnormal neuronal activity in dorsofrontostriatal, orbitofrontostriatal, and frontocerebellar circuits (6). Furthermore, abnormal functional connectivity in the default-mode network (DMN) has been suggested (7).
Adults with ADHD often suffer from comorbid disorders (e.g., depression or anxiety disorders) and negative psychosocial consequences (8). Therefore, a multimodal treatment approach that takes into consideration both the ADHD and the comorbid disorders and psychosocial functioning is currently the gold standard in the treatment of adult ADHD (9).
Psychopharmacological treatment with methylphenidate hydrochloride is recommended as the first-line treatment for ADHD core symptoms (9). Methylphenidate influences dopaminergic and noradrenergic systems of the striatum, prefrontal cortex, locus coeruleus, and somatosensory cortex. Dopamine plays an important role in drive and motivation, and noradrenalin in attentional processes (10–12). Therefore, it has been suggested that the positive effects of methylphenidate on ADHD can be attributed to improving the functioning of brain areas involved in attentional and motivational processes (13). These positive effects can be augmented when combined with individual or group cognitive behavioral therapy (14).
However, while psychopharmacological treatment with methylphenidate has undoubted positive effects on ADHD symptoms, it also has significant limitations. About 20–50% of adult ADHD patients are non-responders (15). Also, a study by Tucha et al. (16) showed that although methylphenidate reduced deficits in attentional processes, it did not achieve normalization. Furthermore, contraindications such as hyperthyroidism, pregnancy, hypertonia, or substance abuse can prohibit treatment with methylphenidate (9, 17, 18). For instance, in a study investigating the efficacy of a combination of cognitive behavioral group psychotherapy, individual clinical management, and methylphenidate in a clinical sample, contraindications in about 20% of participants meant that they could not be treated with methylphenidate (14). Even if treatment with methylphenidate is possible, adverse side effects can occur. These most frequently include headaches, loss of appetite and weight, insomnia, internal unrest, and increased blood pressure and pulse (10). As a result, some patients prefer non-medical treatment.
Given the limitations of treatment with methylphenidate, it is worth considering alternative treatment approaches that target both the underlying neurobiological mechanisms and the psychosocial difficulties of patients with ADHD. From our point of view, this is best achieved by administering treatment from a neuropsychotherapeutic perspective. Such an approach incorporates neurobehavioral interventions to enhance the functioning of brain regions affected in ADHD and specific cognitive behavioral interventions. In mindfulness-based cognitive therapy (MBCT), conventional cognitive behavioral interventions are combined with mindfulness meditation, which can be understood as a form of mental training (19). Mindfulness signifies an open and alert state of mind. The person’s attention stays in the present moment, and sensations such as thoughts and feelings that arise are perceived and observed non-judgmentally (20). There is preliminary evidence that mindfulness meditation can improve the functioning of brain mechanisms underlying neuropsychological capacities impaired in ADHD, such as attention control and emotion regulation (19). We think that mindfulness meditation in patients with ADHD could help them to regulate brain functioning and thereby ameliorate their symptoms.
This paper aims to illustrate our concept of a neuropsychotherapeutic approach for ADHD in adulthood.
A search for trials on treatment, mindfulness, neuropsychotherapy, and psychotherapy in adult ADHD was conducted in the following bibliographic databases: PubMed, Embase, Medline, and Central (The Cochrane Central Register of Controlled Trials). The following terms were used: (ADHD OR (attention deficit) OR (attention deficit) OR hyperactivity*) AND (non-psychopharmacological treatment OR treatment OR therapy OR mindfulness OR psychotherapy OR neuropsychotherapy OR neuropsychology) AND (adult). Studies were selected and included according to their relevance for the subject.
The concept of neuropsychotherapy represents the link between neuropsychology and psychotherapy. A neuropsychotherapeutic approach brings a neuroscientific perspective to therapeutic issues and aims to target underlying brain mechanisms that could be an obstacle to recovery in traditional therapy (21, 22).
We define “neuropsychotherapy” as an approach that integrates cognitive behavioral therapy with neurobehavioral treatment. Neurobehavioral treatment refers to behavioral interventions that deliberately target neuronal mechanisms associated with psychiatric disorders, in the same way as pharmacological or surgical treatments (22).
Since neuropsychotherapy targets neurobiological mechanisms, as well as observable symptoms or cognitive, behavioral manifestations of underlying neurobiological mechanisms, multiple therapeutic interventions are used. As in conventional psychotherapy, cognitive and behavioral interventions are employed for psychoeducative purposes and to bring about change in problematic cognitive and behavioral patterns. In addition, neuropsychological interventions are used. That is, affected neuronal structures are identified through neuropsychological assessment and neuroimaging. Subsequently, neurobehavioral interventions are employed to strengthen the functioning of those neuronal structures via concrete, intensive, and repetitive stimulation (21).
There is evidence that intensive and repetitive targeting of dysfunctional neuronal structures can ameliorate psychiatric disorders and improve brain functioning. In one study, patients with severe unipolar depression received neurobehavioral “cognitive control training” for 2 weeks, aimed at activating the prefrontal cortex, which it has been suggested plays an important role in depressive symptoms such as rumination. They were compared to a control group who received treatment as usual. Participants in the intervention group displayed a significantly greater decrease in depressive symptoms and rumination than participants in the control group. In addition, participants who received the cognitive control training showed normalization of brain functions targeted by the intervention (22).
Furthermore, it has been proposed that the success of cognitive behavioral therapy in treating anxiety disorders may be attributable to the modification of underlying, dysfunctional neuronal systems, as a result of the concrete, intense, and repetitive stimulation induced by exposure sessions (21). For instance, neuroimaging studies in OCD (obsessive compulsive disorder) samples (23, 24) revealed that exposure is associated with improved activity in brain areas involved in obsessive compulsive behavior.
It is recognized that, owing to neuronal plasticity, altered brain functioning can be modified by intense, prolonged, and regular therapeutic interventions (21, 22, 25), leading to improved psychological functioning. Therefore, the neuroscientifically informed implementation of neurobehavioral interventions in conventional psychotherapy appears to be a promising approach to improving treatment outcomes (22). It would appear particularly promising for treatment of a condition such as ADHD, which is known to be significantly related to structural, functional, and neurochemical brain abnormalities (26).
There is growing evidence that ADHD psychopathology is closely related to dysfunctions in multiple neuronal systems implicated in higher-level cognitive functions, as well as sensorimotor processes and the DMN (a brain network that is active in the resting state and inactive during task performance), which causes impairments in executive functioning (26), including in attentional processes such as sustained attention and set-shifting, impulse control, and working memory. ADHD symptoms are thought to reflect altered connectivity within and among several neural networks, rather than abnormal functioning of discrete, isolated brain regions (5). It has been suggested that mostly prefrontal–striatal–cerebellar circuits are impaired in ADHD in adulthood, specifically the prefrontal cortex, basal ganglia, and cerebellum are associated with ADHD (27, 28). The first of these neural circuits are frontostriatal loops, involved in response output control/response suppression, working memory, and response selection. Impairments are also found in frontocerebellar loops, responsible for the temporal information processing needed in timing and alerting the brain to new information. Finally, frontolimbic loops involved in avoidance conditioning and reinforcement learning are relevant to ADHD (27) (see Figure 1).
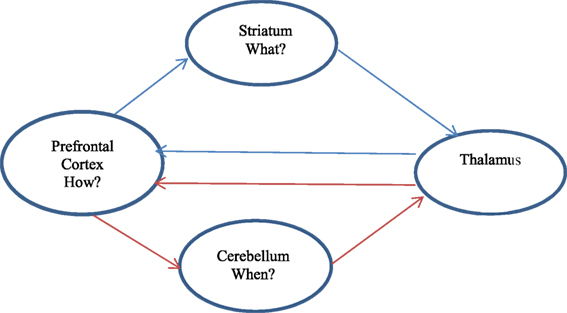
Figure 1. Cerebellar pathways affected in ADHD.
A meta-analysis of neuroimaging studies of ADHD in adulthood revealed ADHD-related hypoactivation located in the frontoparietal network, which includes the lateral frontal pole, anterior cingulate cortex (ACC), dorsolateral prefrontal cortex (dlPFC), anterior PFC (aPFC), lateral cerebellum, anterior insula, and the caudate and inferior parietal lobe (5, 29). The frontoparietal network is known as the executive control circuit (30). It guides decision making by integrating external information with internal representations (5). It provides the flexibility to configure information processing when task demands change, and is involved in goal-directed executive processes (31). Hypoactivation in the frontoparietal network is consistent with executive dysfunction in ADHD in adulthood (26).
The functioning of the dorsal and ventral attentional networks, which are central parts of the attentional regulatory system, also seems to be impaired in ADHD (5, 32). The ventral attentional network includes the temporoparietal junction, the supramarginal gyrus, frontal operculum, and anterior insula (32). It is involved in attentional reorienting to relevant external stimuli and in interrupting ongoing activity when necessary. To prevent shifts of attention to irrelevant objects, suppression of this network is needed (33). It has been suggested that hyperactivation of the ventral attentional network may explain distractibility, which is a main symptom of ADHD (26). The dorsal attentional network, which is anchored by the intraparietal sulcus and the frontal eye fields, also shows ADHD-related abnormalities. The dorsal attentional network is associated with attention shifting and the control of spatial attention (32).
Furthermore, impairments in the visual network have been proposed (34). This network includes the visual cortex and the middle temporal area complex, both of which are connected to the dorsal attentional network. The middle temporal area complex is also functionally correlated to frontal regions, as well as to primary visual areas (5, 35).
There is also evidence that the motor network (e.g., primary motor cortex, primary sensory cortex, putamen, thalamus, and cerebellum) may be affected in ADHD (5).
Attention deficit/hyperactivity disorder has also been conceptualized as a disorder of dysfunctional DMN activity. The DMN includes the medial prefrontal cortex (mPFC), ACC, and posterior cingulate cortex (PCC) (36). It has been suggested that in ADHD the inter-regulation between the DMN and networks activated during task performance (e.g., frontoparietal, ventral, or dorsal attentional networks) is disturbed. During task performance, DMN activity is typically suppressed. According to one hypothesis, in ADHD the DMN is hyperactive during task performance, which may cause the disruption in cognitive performance and fluctuation in attention that characterize the condition (26, 37). For example, the regulation of DMN activity by stimulant medication has been shown to improve cognitive performance in ADHD (38, 39).
Given these neurobiological functional impairments in ADHD, it seems rational to employ principles of neuroscience in treatment, which we discuss next.
A promising approach to improve the outcome of therapy in ADHD involves the neuropsychotherapeutic administration of meditation practice in MBCT. MBCT combines methods of cognitive behavioral therapy with mindfulness meditation. The treatment aims to provide the patient with an explanation for his symptoms, as well as information about ADHD. Behavioral interventions are designed to develop planning skills such as time management or problem solving. With cognitive methods, patients learn to identify and modify problematic thinking patterns (40). Besides cognitive behavioral interventions, patients engage in mindfulness meditation, which can be defined as a form of mental training that can improve neuropsychological deficits in ADHD, such as attention control and emotion regulation, by strengthening the function of brain regions believed to underlie these deficits (19).
It has been proposed that mindfulness meditation can help reduce mind wandering and distractibility in ADHD by improving the functioning of the DMN. For example, experienced meditators show reduced activation of the DMN during meditation and stronger functional connectivity of brain regions implicated in cognitive control and self-monitoring (41).
A further possible beneficial effect of mindfulness meditation in ADHD is that it teaches patients not to act out but rather to observe emotional states as temporary and passing events, thereby helping patients to improve their regulation of emotion. Emotion regulation refers to strategies that help to exert influence on the occurrence, experience, and expression of emotions (19, 42). Even though emotional dysregulation is not a core diagnostic feature of ADHD, it often contributes to considerable impairment (43–45). Neuroimaging studies have found neuroplastic changes in the structure and function of brain regions supporting emotion regulation (19).
The neurobiological mechanism of mindfulness meditation is currently not fully understood. It has been hypothesized that mindfulness meditation changes brain structure and function by myelinogenesis, synaptogenesis, dendritic branching, or adult neurogenesis (19). Furthermore, it seems possible that mindfulness meditation has a positive effect on neuronal preservation, restoration, and/or inhibition of apoptosis (46–48).
Besides these findings from neuroimaging studies, treatment studies have provided promising preliminary support for the feasibility and acceptability of mindfulness meditation in the treatment of ADHD. Recent studies indicate that mindfulness meditation training has ameliorating effects on ADHD symptoms and improves executive functioning, as well as emotion regulation (ISRCTN12722296 in preparation) (49, 50). Furthermore, participants show notable levels of compliance and report a high degree of satisfaction with the treatment (51). In addition, mindfulness meditation is a core component of a modified Dialectical Behavior Therapy group program for adults with ADHD. Mindfulness meditation seems to be well accepted by the patients and a very useful component of the program (52, 53) (see Table 1).
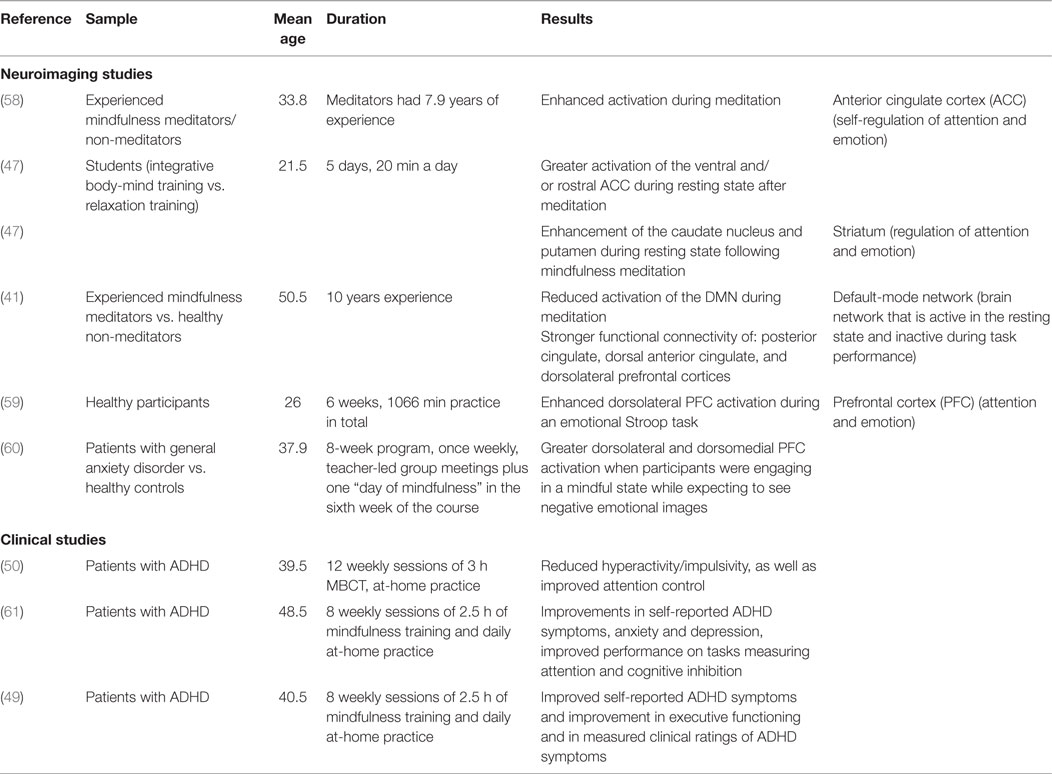
Table 1. Evidence of changes after mindfulness meditation.
Given this evidence, we conclude that engagement in mindfulness meditation is associated with functional changes in brain areas suggested to be impaired in adults with ADHD. In addition, patients readily accept mindfulness meditation. Thus, mindfulness meditation appears to be a promising neurobehavioral intervention, with several potential pathways to improving neuropsychological functioning in patients with ADHD.
There is emerging evidence that mindfulness meditation ameliorates ADHD symptoms and may cause neuroplastic changes in brain regions impaired in ADHD. However, the study of the neurobiological mechanisms of mindfulness meditation and its beneficial effects in ADHD is still in its infancy. This allows only speculative statements about possible future treatment directions. The following limitations have to be considered, along with recommendations arising out of them.
Research is needed that uses larger sample sizes, active control conditions, and longitudinal, randomized research designs (19, 51).
To our knowledge, no neuroimaging study has investigated the effects of mindfulness meditation on the adult ADHD brain. Future research should aim to expand understanding of the neurobiological effects of mindfulness meditation in ADHD and to connect neuroscientific findings with behavioral data.
Furthermore, it has been suggested that ADHD is a heterogeneous condition, which probably includes different diagnostic subtypes (54), possibly caused by different neurobiological impairments. In addition, owing to the high comorbidity with other psychiatric disorders, common comorbid psychiatric disorders may rely on the same dysfunctional neuronal mechanisms as ADHD does. For example, ADHD and bipolar disorder show an overlap in diagnostic criteria, such as inattention and irritability (55). Also, a significantly higher prevalence of ADHD among relatives of persons with bipolar disorder and a significantly higher prevalence of bipolar I disorder among relatives of persons with ADHD has been reported (56). This co-occurrence may be associated with impairments in the same underlying neuronal mechanisms. Knowledge of these underlying neuronal mechanisms could help in developing a more specific assessment and classification of psychiatric disorders, as well as improved treatment interventions.
Another area for future research is investigation of the optimum amount of mindfulness meditation practice in ADHD. Neurobehavioral interventions are known to involve intense, prolonged, and regular stimulation of the targeted brain areas to effectively change neuronal structures (21). However, it is as yet not known how much mindfulness meditation is needed to evoke changes in neuroplasticity and psychological functioning in ADHD. For example, a study in a non-ADHD sample compared the effects of an 8-week mindfulness training course in a high- vs. low-practice group. The results indicate that high engagement in mindfulness (total time practice over 8 weeks: M = 11 h, SD = 7 h) compared to low engagement in mindfulness (total time practice over 8 weeks: M = 2.5 h, SD = 1 h) is associated with improved working memory control and improved positive affect (57).
Although studies indicate that mindfulness meditation has positive effects on ADHD in adulthood, the exact working mechanisms of mindfulness meditation are unclear. For example, patients may learn to relate and react more functionally to their thoughts thanks to mindful awareness of their cognitions, or to decenter from thoughts and view them as passing events that do not have to be acted upon. Furthermore, it is possible that mindfulness meditation causes changes in other areas of life, such as better self-care (e.g., improved diet, regular exercise), which could contribute to improved treatment outcomes.
Attention-deficit/hyperactivity disorder, in adulthood is a serious mental condition with a strong neurobiological component that causes a wide range of impairments in affected individuals. Psychopharmacological medication is the first-line treatment for ADHD. However, not all patients respond well to it, and others have a preference for non-psychopharmacological treatment. Healthy psychological functioning in ADHD seems to rely greatly on the well-coordinated functioning of neuronal networks. There is promising preliminary evidence that mindfulness meditation employed as a neurobehavioral intervention in therapy can help ADHD patients to regulate impaired brain functioning and thereby improve self-regulation of attention and emotion control.
KB: literature research and writing, AL: literature research and writing, AP: literature research and writing, supervision.
AP (MD) declares that she has served on advisory boards, given lectures, performed phase three studies, or received travel grants within the last 3 years from Eli Lilly and Co., Lundbeck, MEDICE Arzneimittel Pütter GmbH and Co. KG, Novartis, Servier, and Shire; and has authored books and articles on psychotherapy published by Elsevier, Hogrefe, Schattauer, Kohlhammer, Karger, and Springer. KB declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. AL (MD) declares that she received travel grants within the last year from MEDICE Arzneimittel Pütter GmbH and Co. KG.
1. Kessler RC, Adler LA, Barkley R, Biederman J, Conners CK, Faraone SV, et al. Patterns and predictors of attention-deficit/hyperactivity disorder persistence into adulthood: results from the national comorbidity survey replication. Biol Psychiatry (2005) 57(11):1442–51. doi:10.1016/j.biopsych.2005.04.001
2. Fayyad J, De Graaf R, Kessler R, Alonso J, Angermeyer M, Demyttenaere K, et al. Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br J Psychiatry (2007) 190:402–9. doi:10.1192/bjp.bp.106.034389
3. Mostert JC, Onnink AM, Klein M, Dammers J, Harneit A, Schulten T, et al. Cognitive heterogeneity in adult attention deficit/hyperactivity disorder: a systematic analysis of neuropsychological measurements. Eur Neuropsychopharmacol (2015) 25(11):2062–74. doi:10.1016/j.euroneuro.2015.08.010
4. Wahlstedt C, Thorell LB, Bohlin G. Heterogeneity in ADHD: neuropsychological pathways, comorbidity and symptom domains. J Abnorm Child Psychol (2009) 37(4):551–64. doi:10.1007/s10802-008-9286-9
5. Castellanos FX, Proal E. Large-scale brain systems in ADHD: beyond the prefrontal-striatal model. Trends Cogn Sci (2012) 16(1):17–26. doi:10.1016/j.tics.2011.11.007
6. Durston S, van Belle J, de Zeeuw P. Differentiating frontostriatal and fronto-cerebellar circuits in attention-deficit/hyperactivity disorder. Biol Psychiatry (2011) 69(12):1178–84. doi:10.1016/j.biopsych.2010.07.037
7. Konrad K, Herpertz S, Herpertz-Dahlmann B. Aufmerksamkeitsdefizit-Hyperaktivitätssyndrom. In: Fink GR, Schneider F, editors. Funktionelle MRT in Psychiatrie und Neurologie. Berlin, Heidelberg: Springer Verlag (2013). p. 716–25.
8. Pitts M, Mangle L, Asherson P. Impairments, diagnosis and treatments associated with attention-deficit/hyperactivity disorder (ADHD) in UK adults: results from the lifetime impairment survey. Arch Psychiatr Nurs (2015) 29(1):56–63. doi:10.1016/j.apnu.2014.10.001
9. NICE. Attention Deficit Hyperactivity Disorder: Diagnosis and Management of ADHD in Children, Young People and Adults. NICE Guideline 72. (2013). Available from: https://www.nice.org.uk/guidance/cg72
10. Epstein T, Patsopoulos NA, Weiser M. Immediate-release methylphenidate for attention deficit hyperactivity disorder (ADHD) in adults. Cochrane Database Syst Rev (2014) 9:Cd005041. doi:10.1002/14651858.CD005041.pub2
11. Del Campo N, Chamberlain SR, Sahakian BJ, Robbins TW. The roles of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Biol Psychiatry (2011) 69(12):e145–57. doi:10.1016/j.biopsych.2011.02.036
12. Krause J, Krause KH. ADHS im Erwachsenenalter: Symptome, Differenzialdiagnose, Therapie. Schattauer (2014).
13. ter Huurne N, Fallon SJ, van Schouwenburg M, van der Schaaf M, Buitelaar J, Jensen O, et al. Methylphenidate alters selective attention by amplifying salience. Psychopharmacology (Berl) (2015) 232(23):4317–23. doi:10.1007/s00213-015-4059-y
14. Philipsen A, Jans T, Graf E, Matthies S, Borel P, Colla M, et al. Effects of group psychotherapy, individual counseling, methylphenidate, and placebo in the treatment of adult attention-deficit/hyperactivity disorder: a randomized clinical trial. JAMA Psychiatry (2015) 72(12):1199–210. doi:10.1001/jamapsychiatry.2015.2146
15. Wilens TE, Spencer TJ, Biedermann J. A review of the pharmacotherapy of adults with attention-deficit/hyperactivity disorder. J Atten Disord (2002) 5(4):189–202. doi:10.1177/108705470100500401
16. Tucha O, Mecklinger L, Laufkotter R, Klein HE, Walitza S, Lange KW. Methylphenidate-induced improvements of various measures of attention in adults with attention deficit hyperactivity disorder. J Neural Transm (Vienna) (2006) 113(10):1575–92. doi:10.1007/s00702-005-0437-7
17. Eich-Höchli D, Seifritz E, Eich P. Pharmakotherapie bei ADHS im Erwachsenenalter: Eine Bestandsaufnahme. Zeitschrift für Psychiatrie Psychologie Psychotherapie (2015) 63(1):15–24. doi:10.1024/1661-4747/a000215
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol (2005) 61(5):589–606. doi:10.1002/jclp.20122
19. Tang YY, Hölzel BK, Posner MI. The neuroscience of mindfulness meditation. Nat Rev Neurosci (2015) 16(4):213–25. doi:10.1038/nrn3916
20. Kabat-Zinn J. Gesund durch Meditation: das große Buch der Selbstheilung. New York, NY: Otto Wilhelm Barth Verlag (2000).
22. Siegle GJ, Ghinassi F, Thase ME. Neurobehavioral therapies in the 21st century: summary of an emerging field and an extended example of cognitive control training for depression. Cognit Ther Res (2007) 31(2):235–62. doi:10.1007/s10608-006-9118-6
23. Morgieve M, N’Diaye K, Haynes WI, Granger B, Clair AH, Pelissolo A, et al. Dynamics of psychotherapy-related cerebral haemodynamic changes in obsessive compulsive disorder using a personalized exposure task in functional magnetic resonance imaging. Psychol Med (2014) 44(7):1461–73. doi:10.1017/S0033291713002237
24. Schiepek G, Tominschek I, Heinzel S, Aigner M, Dold M, Unger A, et al. Discontinuous patterns of brain activation in the psychotherapy process of obsessive-compulsive disorder: converging results from repeated FMRI and daily self-reports. PLoS One (2013) 8(8):e71863. doi:10.1371/journal.pone.0071863
25. Chavan CF, Mouthon M, Draganski B, van der Zwaag W, Spierer L. Differential patterns of functional and structural plasticity within and between inferior frontal gyri support training-induced improvements in inhibitory control proficiency. Hum Brain Mapp (2015) 36(7):2527–43. doi:10.1002/hbm.22789
26. Cortese S, Kelly C, Chabernaud C, Proal E, Di Martino A, Milham MP, et al. Towards systems neuroscience of ADHD: a meta-analysis of 55 fMRI studies. Am J Psychiatry (2012) 169(10):1038–55. doi:10.1176/appi.ajp.2012.11101521
27. Nigg JT, Casey BJ. An integrative theory of attention-deficit/hyperactivity disorder based on the cognitive and affective neurosciences. Dev Psychopathol (2005) 17(03):785–806. doi:10.1017/S0954579405050376
28. Cubillo A, Halari R, Smith A, Taylor E, Rubia K. A review of fronto-striatal and fronto-cortical brain abnormalities in children and adults with attention deficit hyperactivity disorder (ADHD) and new evidence for dysfunction in adults with ADHD during motivation and attention. Cortex (2012) 48(2):194–215. doi:10.1016/j.cortex.2011.04.007
29. Vincent JL, Kahn I, Snyder AZ, Raichle ME, Buckner RL. Evidence for a frontoparietal control system revealed by intrinsic functional connectivity. J Neurophysiol (2008) 100(6):3328–42. doi:10.1152/jn.90355.2008
30. Menon V. Large-scale brain networks and psychopathology: a unifying triple network model. Trends Cogn Sci (2011) 15(10):483–506. doi:10.1016/j.tics.2011.08.003
31. Liston C, Matalon S, Hare TA, Davidson MC, Casey BJ. Anterior cingulate and posterior parietal cortices are sensitive to dissociable forms of conflict in a task-switching paradigm. Neuron (2006) 50(4):643–53. doi:10.1016/j.neuron.2006.04.015
32. Corbetta M, Patel G, Shulman GL. The reorienting system of the human brain: from environment to theory of mind. Neuron (2008) 58(3):306–24. doi:10.1016/j.neuron.2008.04.017
33. Corbetta M, Shulman GL. Control of goal-directed and stimulus-driven attention in the brain. Nat Rev Neurosci (2002) 3(3):201–15. doi:10.1038/nrn755
34. Ahrendts J, Rusch N, Wilke M, Philipsen A, Eickhoff SB, Glauche V, et al. Visual cortex abnormalities in adults with ADHD: a structural MRI study. World J Biol Psychiatry (2011) 12(4):260–70. doi:10.3109/15622975.2010.518624
35. Yeo BT, Krienen FM, Sepulcre J, Sabuncu MR, Lashkari D, Hollinshead M, et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol (2011) 106(3):1125–65. doi:10.1152/jn.00338.2011
36. Tang YY, Rothbart MK, Posner MI. Neural correlates of establishing, maintaining, and switching brain states. Trends Cogn Sci (2012) 16(6):330–7. doi:10.1016/j.tics.2012.05.001
37. Sonuga-Barke EJ, Castellanos FX. Spontaneous attentional fluctuations in impaired states and pathological conditions: a neurobiological hypothesis. Neurosci Biobehav Rev (2007) 31(7):977–86. doi:10.1016/j.neubiorev.2007.02.005
38. Peterson BS, Potenza MN, Wang Z, Zhu H, Martin A, Marsh R, et al. An FMRI study of the effects of psychostimulants on default-mode processing during Stroop task performance in youths with ADHD. Am J Psychiatry (2009) 166(11):1286–94. doi:10.1176/appi.ajp.2009.08050724
39. Liddle EB, Hollis C, Batty MJ, Groom MJ, Totman JJ, Liotti M, et al. Task-related default mode network modulation and inhibitory control in ADHD: effects of motivation and methylphenidate. J Child Psychol Psychiatry (2011) 52(7):761–71. doi:10.1111/j.1469-7610.2010.02333.x
40. Safren SA, Sobanski E. Kognitive Verhaltenstherapie der ADHS des Erwachsenenalters. Berlin: Med. Wiss. Verlag-Ges (2009).
41. Brewer JA, Worhunsky PD, Gray JR, Tang YY, Weber J, Kober H. Meditation experience is associated with differences in default mode network activity and connectivity. Proc Natl Acad Sci U S A (2011) 108(50):20254–9. doi:10.1073/pnas.1112029108
42. Ochsner KN, Gross JJ. The cognitive control of emotion. Trends Cogn Sci (2005) 9(5):242–9. doi:10.1016/j.tics.2005.03.010
43. Wender PH. Attention-Deficit Hyperactivity Disorder in Adults. Oxford: Oxford University Press (1995).
44. Barkley RA, Fischer M. The unique contribution of emotional impulsiveness to impairment in major life activities in hyperactive children as adults. J Am Acad Child Adolesc Psychiatry (2010) 49(5):503–13. doi:10.1097/00004583-201003000-00002
45. Shaw P, Stringaris A, Nigg J, Leibenluft E. Emotional dysregulation and attention-deficit/hyperactivity disorder. Am J Psychiatry (2014) 171(3):276–93. doi:10.1176/appi.ajp.2013.13070966
46. Tang YY, Ma Y, Wang J, Fan Y, Feng S, Lu Q, et al. Short-term meditation training improves attention and self-regulation. Proc Natl Acad Sci U S A (2007) 104(43):17152–6. doi:10.1073/pnas.0707678104
47. Tang YY, Ma Y, Fan Y, Feng H, Wang J, Feng S, et al. Central and autonomic nervous system interaction is altered by short-term meditation. Proc Natl Acad Sci U S A (2009) 106(22):8865–70. doi:10.1073/pnas.0904031106
48. Gray JD, Milner TA, McEwen BS. Dynamic plasticity: the role of glucocorticoids, brain-derived neurotrophic factor and other trophic factors. Neuroscience (2013) 239:214–27. doi:10.1016/j.neuroscience.2012.08.034
49. Mitchell JT, McIntyre EM, English JS, Dennis MF, Beckham JC, Kollins SH. A pilot trial of mindfulness meditation training for attention-deficit/hyperactivity disorder in adulthood: impact on core symptoms, executive functioning, and emotion dysregulation. J Atten Disord (2013). doi:10.1177/1087054713513328
50. Schoenberg PL, Hepark S, Kan CC, Barendregt HP, Buitelaar JK, Speckens AE. Effects of mindfulness-based cognitive therapy on neurophysiological correlates of performance monitoring in adult attention-deficit/hyperactivity disorder. Clin Neurophysiol (2014) 125(7):1407–16. doi:10.1016/j.clinph.2013.11.031
51. Mitchell JT, Zylowska L, Kollins SH. Mindfulness meditation training for attention-deficit/hyperactivity disorder in adulthood: current empirical support, treatment overview, and future directions. Cogn Behav Pract (2015) 22(2):172–91. doi:10.1016/j.cbpra.2014.10.002
52. Hesslinger B, Philipsen A, Richter H. Psychotherapie der ADHS im Erwachsenenalter: ein Arbeitsbuch. Göttingen: Hogrefe (2004).
53. Philipsen A, Richter H, Peters J, Alm B, Sobanski E, Colla M, et al. Structured group psychotherapy in adults with attention deficit hyperactivity disorder: results of an open multicentre study. J Nerv Ment Dis (2007) 195(12):1013–9. doi:10.1097/NMD.0b013e31815c088b
54. Philipsen A, Hesslinger B, Tebartz van Elst L. Attention deficit hyperactivity disorder in adulthood: diagnosis, etiology and therapy. Dtsch Arztebl Int (2008) 105(17):311–7. doi:10.3238/arztebl.2008.0311
55. Youngstrom EA, Arnold LE, Frazier TW. Bipolar and ADHD comorbidity: both artifact and outgrowth of shared mechanisms. Clin Psychol (New York) (2010) 17(4):350–9. doi:10.1111/j.1468-2850.2010.01226
56. Faraone SV, Biederman J, Wozniak J. Examining the comorbidity between attention deficit hyperactivity disorder and bipolar I disorder: a meta-analysis of family genetic studies. Am J Psychiatry (2012) 169(12):1256–66. doi:10.1176/appi.ajp.2012.12010087
57. Jha AP, Stanley EA, Kiyonaga A, Wong L, Gelfand L. Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion (2010) 10(1):54–64. doi:10.1037/a0018438
58. Hölzel BK, Ott U, Hempel H, Hackl A, Wolf K, Stark R, et al. Differential engagement of anterior cingulate and adjacent medial frontal cortex in adept meditators and non-meditators. Neurosci Lett (2007) 421(1):16–21. doi:10.1016/j.neulet.2007.04.074
59. Allen M, Dietz M, Blair KS, van Beek M, Rees G, Vestergaard-Poulsen P, et al. Cognitive-affective neural plasticity following active-controlled mindfulness intervention. J Neurosci (2012) 32(44):15601–10. doi:10.1523/jneurosci.2957-12.2012
60. Hölzel BK, Hoge EA, Greve DN, Gard T, Creswell JD, Brown KW, et al. Neural mechanisms of symptom improvements in generalized anxiety disorder following mindfulness training. Neuroimage Clin (2013) 2:448–58. doi:10.1016/j.nicl.2013.03.011
Keywords: neuropsychotherapy, ADHD, adult, MBCT, non-psychopharmacological treatment
Citation: Bachmann K, Lam AP and Philipsen A (2016) Mindfulness-Based Cognitive Therapy and the Adult ADHD Brain: A Neuropsychotherapeutic Perspective. Front. Psychiatry 7:117. doi: 10.3389/fpsyt.2016.00117
Received: 09 March 2016; Accepted: 14 June 2016;
Published: 27 June 2016
Edited by:
Stefan Borgwardt, University of Basel, SwitzerlandReviewed by:
Gianluca Serafini, University of Genoa, ItalyCopyright: © 2016 Bachmann, Lam and Philipsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandra Philipsen, YWxleGFuZHJhLnBoaWxpcHNlbkB1bmktb2xkZW5idXJnLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.