 Joseph A. Vitriol
Joseph A. Vitriol- 1Stony Brook University, Stony Brook, NY, United States
- 2Lehigh University, Bethlehem, PA, United States
Sustained and coordinated social action is needed to combat the spread of the novel coronavirus disease 2019 (COVID-19). Health practitioners and governments around the world have issued recommendations and mandates designed to reduce the transmission of COVID-19 by influencing the social behaviors of the general public. Why and when are some people unwilling to take action to protect themselves and others from the effects of this public health crisis? We find that belief in COVID-19 consensus information (by the self or perceptions of scientists’ beliefs), are consequential predictors of COVID-19 mitigation behaviors. Importantly, support for COVID-19 conspiracy theories predicted decreased, whereas perceived understanding of COVID-19 predicted increased, belief in COVID-19 consensus information. We also implemented an Illusion of Explanatory depth paradigm, an approach to examining knowledge overestimation shown to reduce confidence in one’s understanding of complex phenomena. By requiring participants to elaborate upon COVID-19 conspiracies, we experimentally increased understanding of these theories, which led, in turn, to ironic increases in support for the conspiracy theories and undermined perceived understanding of COVID-19 information for a notable portion of our participants. Together, our results suggest that attention given to COVID-19 conspiracies may be misguided; describing or explaining the existence of COVID-19 conspiracies may ironically increase support for these accounts and undermine knowledge about and willingness to engage in COVID-19 mitigation.
Introduction
Sustained and coordinated social action is needed to combat the spread of the coronavirus disease 2019 (COVID-19; Van Bavel et al., 2020), a pandemic that has claimed the lives of millions and will continue to threaten the safety and well-being of many more in the foreseeable future (World Health Organization, 2020a). Health organizations, medical professionals, and governments around the world have issued recommendations and mandates designed to reduce the transmission of COVID-19 by influencing the social behaviors of the general public (Centers for Disease Control, 2020; Götz et al., 2020). These initiatives—such as frequent handwashing, the use of protective facemasks, and social distancing—have indeed been effective at slowing the transmission of the virus and reducing the likelihood of illness (Anderson et al., 2020; Cohen and Corey, 2020; Haushofer and Metcalf, 2020; Prather et al., 2020).
The success with which behavioral mitigation is able to reduce disease contagion largely depends on widespread and voluntary compliance among individual members of the general public (Bish and Michie, 2010; West et al., 2020). While large majorities of the general public in the U.S. support and engage in behavioral mitigation measures (Pew Research Center, 2020a; Pew Research Center, 2020b), there nonetheless remains a sizable minority who do not (cf. Motta et al., 2020). Why and when are some people unwilling to take action to protect themselves and others from the effects of the COVID-19 pandemic? With the widespread dissemination of inaccurate or unreliable information about COVID-19 (Brennen et al., 2020), where conspiracy theories run amok (Miller, 2020), and prominent political leaders misrepresent the severity of the pandemic and the efficacy of purported treatments (Sharma et al., 2017; Woodward, 2020), understanding how individuals acquire and use knowledge about COVID-19 is of central importance to containing its spread.
Predictors of COVID-19 Mitigation Beliefs and Behaviors
A literature examining predictors of COVID-19 beliefs about and voluntary compliance with behavioral mitigation recommendations is burgeoning. Engaging in mitigation behaviors is predicted by perceptions of the self (Bruine de Bruin and Bennett, 2020); perceptions of key others (Pfattheicher et al., 2020; Merkley and Loewen, 2021); individual traits such as thinking style (Pennycook et al., 2020; Teovanovic et al., 2020) and partisanship (Calvillo et al., 2020; Clinton et al., 2020; Druckman et al., 2020; Gollwitzer et al., 2020); as well as consumption of mainstream media outlets (Allington et al., 2020; Bridgman et al., 2020; Motta et al., 2020).
Much research has also focused on the implications of what some have described as an “infodemic” (Bridgman et al., 2020; World Health Organization, 2020b; Teovanovic et al., 2020), which refers to the widespread acceptance of unreliable and unverified information regarding the COVID-19 pandemic (for a review, see van Mulukom et al., 2020 preprint; Depoux et al., 2020; Kouzy et al., 2020; Mian and Khan, 2020; Motta and Callaghan, 2020). Such misperceptions of COVID-19 and distrust in experts who provide COVID-19 information reduce perceptions of risk and social distancing compliance (Bridgman et al., 2020; Merkley and Loewen, 2021). Furthermore, distrust in expertise promotes COVID-19 conspiracy theories (Uscinski et al., 2020), with belief in COVID-19 conspiracy theories being found to be the most consistent predictor of not engaging in protective health behaviors (Teovanovic et al., 2020). In short, misinformation and misperceptions can have deleterious consequences for accurate COVID-19 beliefs, with pernicious effects on behavioral mitigation.
Given the importance of accurate knowledge concerning the risk, transmission, and mitigation of COVID-19, a primary goal of public health recommendations and communication during the pandemic is to increase public understanding and align belief with consensus scientific information (Finset et al., 2020; Van Bavel et al., 2020). Even during the peak of the pandemic, some still underestimate the risk or severity of disease, or otherwise lack sophisticated knowledge concerning COVID-19 (e.g., Al-Hasan et al., 2020; Allcott et al., 2020; Druckman et al., 2020; Grossman et al., 2020). Understanding what factors keep people from accepting scientific information about COVID-19, and how this shapes mitigation behavior, is therefore needed.
Current Research
In this paper, we examine beliefs about scientifically supported COVID-19 information and its implications for COVID-19 mitigation behaviors. In a Pilot Study (see Supplemental Materials) that utilized data from an Amazon MTurk survey (N = 261), we find that belief in consensus information concerning COVID-19, and the perceptions that scientists also hold these beliefs, are associated with past and future COVID-19 mitigation behaviors, net a host of constructs known to covary with COVID-19 mitigation behaviors (Hypothesis 1). These results are largely consistent with prior research concerning the most proximate and consequential predictors of COVID-19 mitigation behaviors (Clark et al., 2020; Hornik et al., 2020; Marsh et al., 2021).
Importantly, the Pilot Study also demonstrates that support for conspiracy theories about COVID-19 correlated with significantly decreased, whereas perceived understanding of COVID-19 information correlated with significantly increased, belief in COVID-19 consensus information. The main focus of the current research is to better understand how these factors---conspiracy theories about and perceived understanding of COVID-19--shape belief in consensus COVID-19 information. We approach this issue in two ways.
First, we examine if the perception that one understands information related to COVID-19 correlates with belief in and engagement with mitigation behaviors. Prior research suggests that laypeople’s understanding of disease symptomology can shape their perception of effective treatment (Marsh and Zeveney, 2015; Marsh and Romano, 2016). Further, self-perceived causal understanding is closely tied to perceptions of causal understanding among scientists or experts (Sloman and Rabb, 2016; Rabb et al., 2019), the latter of which has been directly implicated in COVID-19 mitigation behaviors (Marsh et al., 2021). These findings suggest that perceived understanding, by both the self and scientists, of how COVID-19 spreads could translate to increased belief in and compliance with behavioral mitigation. We found evidence consistent with this prediction in the Pilot Study, and the current research provides an additional test of this hypothesis (Hypothesis 2).
However, perceived understanding of COVID-19 consensus information may not necessarily result in adopting mitigation behaviors. In general, people often hold a shallow or incorrect understanding of how things in the world actually work (Rozenblit and Keil, 2002). Instead, people are frequently overconfident in their own knowledge, perceiving themselves as able to understand the causal underpinnings of many complex phenomenon in daily life, despite lacking the ability to properly ascertain their own competence in many domains (Wilson and Keil, 1998; Rozenblit and Keil, 2002; Dunning et al., 2003; Fernbach et al., 2013; Zeveney and Marsh, 2016). Overestimation of one’s knowledge about the causes of autism relative to medical experts, for example, is associated with low levels of actual knowledge and reduced vaccine uptake (Motta et al., 2018). Similarly, Teovanovic et al. (2020) demonstrated that individuals who overestimate their knowledge (indexed as deviation between self-reported and objective levels of knowledge) about COVID-19 reported reduced compliance with COVID-19 behavioral guidelines. Other investigations in the political domain indicate that those with inflated confidence in their causal understanding of political phenomena adopt more extreme issue-positions and are more likely to endorse conspiracy theories (Fernbach et al., 2013; Raimi and Leary, 2014; Marsh and Vitriol, 2018; Vitriol and Marsh, 2018). Given these findings, the relationship between perceived understanding and beliefs about COVID-19 deserve more empirical investigation.
The second way we examine the underpinning of belief in consensus COVID-19 information is by investigating the role of conspiratorial beliefs. Consistent with other research examining the implications of COVID-19 misperceptions (Bridgman et al., 2020; Roozenbeek et al., 2020; Teovanovic et al., 2020) and the result of our Pilot Study, we hypothesize that COVID-19 conspiracy theories will undermine belief in consensus information concerning COVID-19 (Hypothesis 3). More importantly, we try to experimentally undermine belief in conspiracy theories by exposing to people what they do not understand about these theories. To do this, we use an Illusion of Explanatory Depth paradigm (IOED; Rozenblit and Keil, 2002), a paradigm robustly shown to help expose people to the shallowness and limits of their explanatory understanding (Alter et al., 2010; Zeveney and Marsh, 2016). Specifically, in the IOED paradigm, the act of generating a causal explanation for a phenomenon exposes the limitations of one’s knowledge, resulting in a drop in confidence in one’s understanding.
In the political domain, those who maintain high levels of confidence in their understanding of politics and public policy, post-explanation, are also more extreme and conspiratorial in their political views (Fernbach et al., 2013; Vitriol and Marsh, 2018). We hypothesize that the act of explaining the causal logic behind prominent COVID-19 conspiracies will reduce confidence in one’s perceived understanding of these theories, which in turn should be correlated with decreased overall endorsement of COVID-19 conspiracies (Hypothesis 4). If this hypothesis is confirmed, then the current study may be the first to demonstrate how revealing illusions of explanatory depth regarding specific conspiracy theories can reduce support for these beliefs and, as a result, minimize some of its more pernicious implications. Nonetheless, we advance our predictions with caution because, to date, the IOED paradigm has only been used to explain well-known or mainstream phenomena (e.g., faucets, election outcomes). As such, it is an open question of how explaining a conspiracy theory may influence understanding and uptake of that theory.
Experimental Study
In summary, our Experimental Study was designed with two goals: 1) to examine the underpinnings of COVID-19 conspiracy theories by utilizing an IOED paradigm to experimentally manipulate perceived understanding of COVID-19 conspiracies, and 2) to replicate the correlational observations of the Pilot Study on an independent sample. To achieve these two goals, we used a two-wave panel study. At Wave 1 (W1; November 30th to December 1st in 2020) participants completed measures of perceived understanding of and beliefs in consensus COVID-19 information, and a battery of measures known to correlate with endorsement of conspiracy theories. We also had participants rate their familiarity with a series of COVID-19 conspiracy theories.
At Wave 2 (W2; December 2nd−December 4th in 2020), we experimentally manipulated perceived understanding of COVID-19 conspiracies using an IOED paradigm (Rozenblit and Keil, 2002). After engaging in the IOED task, participants completed our understanding and belief measures for consensus COVID-19 information. We additionally had participants rate their support for COVID-19 conspiracy theories tested at W1 and the extent to which they were engaging in and planning to engage in COVID-19 mitigation behaviors. These measures will allow us to see how completing a task that should expose limited understanding of conspiracy theories and reveal the illusion of understanding changes endorsement of those theories. This design also allows us to examine if the IOED paradigm influences perceived understanding and belief for COVID-19 consensus information that stands in conflict with those conspiracy theories.
Overview of Hypotheses
We investigate the following hypotheses:
1. Belief in consensus information concerning COVID-19, and the perceptions that scientists also hold these beliefs, will correlate positively with past and future COVID-19 mitigation behaviors.
2. Perceived understanding, by both the self and scientists, of COVID-19 consensus information, will correlate with increased belief in COVID-19 consensus information.
3. Support for COVID-19 conspiracy theories will undermine belief in consensus information concerning COVID-19.
4. The act of explaining the causal logic behind prominent COVID-19 conspiracies will reduce confidence in one’s perceived understanding of these theories, which in turn should correlated with decreased overall endorsement of COVID-19 conspiracies.
Participants and Procedures
We recruited 399 U.S. Citizens participants from Amazon MTurk in November of 2020 (57.3% females; age M = 42.81, SD = 13.49; 74% identify as White; and 78.4% have earned at least a Bachelor’s degree). Of W1 participants, 58% or 232 were retained at W21. Participants who did or did not return for the W2 survey did not significantly differ in mean-levels of W1 belief in consensus COVID-19 information, perceived understanding of consensus COVID-19 information, cognitive sophistication, conspiratorial predispositions, and partisanship (ps > 0.05). However, participants who returned for W2 were significantly more ideologically conservative than participants who did not (W1 Only M = 3.51, SD = 1.93; W1 and W2 M = 3.93, SD = 1.88; t = 2.17, p = 0.031). The demographic characteristics of the two waves are highly similar (see Supplementary Table S4 in the Supplemental Materials).
At W1, participants completed measures of 1) perceived understanding of consensus COVID-19 information, 2) beliefs in consensus COVID-19 information, 3) cognitive sophistication, 4) conspiratorial predispositions, and 5) familiarity with different COVID-19 conspiracies2, and 6) control variables. Measures of belief and understanding were assessed first, in random order, followed by the remaining set of measures. Participants were then contacted two days after data collection for W1 was complete to participate in the W2 survey.
At the start of W2, participants completed the IOED paradigm developed by Rozenblit and Keil (2002; see Fernbach et al., 2013; Zeveney and Marsh, 2016). All participants first learned how to rate their understanding of phenomena on a 7-point scale (1 = very vague understanding, 7 = very thorough understanding) using the same instructions we provided before evaluating perceived understanding of consensus COVID-19 information (see Supplemental Materials). Participants then reported how well they understood three COVID-19 conspiracies, presented in random order; 1) “How the Chinese government engineered the coronavirus (COVID-19) as a bioweapon to wage war on America and Western countries”, 2) “How powerful people have used coronavirus (COVID-19) to orchestrate panic, close down businesses, and destroy capitalism”, and 3) “How the actual infection rate for the coronavirus (COVID-19) has been misreported in order to cover up how many people have been infected”. These conspiracies were selected because they had the highest mean-level support in the Pilot Study.
After reporting their level of understanding of the three COVID-19 conspiracies, participants were randomly assigned to one of two IOED conditions. In the “explanation” condition, participants engaged in a traditional IOED paradigm in which they were asked to explain how each conspiracy theory works as follows (adapted from Rozenblit and Keil (2002); see Supplemental Materials). In contrast, participants who were assigned to the “description” condition, which served as our control group, were asked to list all of the characteristics of each conspiracy they could think of (adapted from Zeveney and Marsh, 2016).
We used these two different IOED manipulations because traditionally generating a causal explanation is what reveals the limitation of one’s causal understanding (Zeveney and Marsh, 2016). For example, Vitriol and Marsh (2018) asked people to explain how a range of public policies work, using instructions with a strong emphasis on explicitly identifying causal connections. Fernbach et al. (2013) adopted a similar approach but compared participants in the explanation condition to participants who listed reasons they agreed or disagreed with a policy. Only when participants were required to explain the policies was the illusion revealed. However, we are uncertain how the act of description will function with implausible beliefs like conspiracy theories. Accordingly, we originally conceived of the description condition as a control group for the effect of explanation, but are open to how it may function in this context.
After generating an explanation or description of a single conspiracy, participants then again rated their level of understanding for that conspiracy. This process was repeated for each of the remaining conspiracies, in random order. Participants’ pre-IOED ratings were averaged across the three conspiracies for each participant to form an indicator of self-reported confidence in one’s understanding of COVID-19 conspiracies. Participants’ post-IOED ratings were similarly averaged to form an indicator of self-reported confidence in one’s understanding of COVID-19 conspiracies post-explanation or post-description.
After the IOED paradigm, participants again completed measures of 1) perceived understanding of consensus COVID-19 information, 2) beliefs in consensus COVID-19 information, and also completed measures of 3) endorsement of COVID-19 conspiracy theories and 4) COVID-19 mitigation behavior.
Measures
Means (SD), alphas, and intercorrelations of all measures are available in Table 1. All continuous variables were rescaled to run from 0–1 for easier interpretation and comparison of effect sizes. Full wording, items, and instructions can be found in the Supplemental Materials if it is not in the main text.
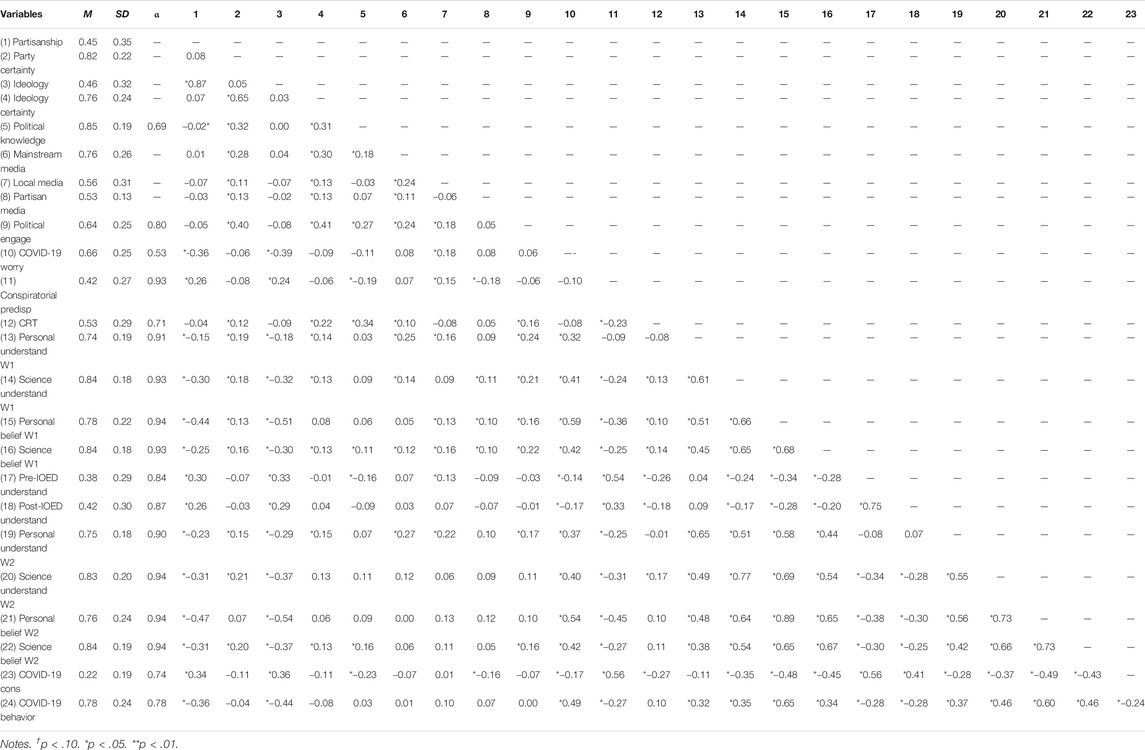
TABLE 1. Mean, SD, Cronbach’s alpha, and correlations between all continuous variables used in study one.
Perceived Understanding of Consensus COVID-19 Information.
At the start of W1 and after the IOED paradigm at W2, participants completed a set of questions that measured their perceived understanding of nine different elements of COVID-19 that tapped understanding of the disease’s transmission, prevention measures, and effects on the body. We refer to these nine items as measuring consensus COVID-19 information. Participants reported in random order the extent to which they understood these consensus pieces of information, as well as how well “scientists and public health experts” understood this information. Participants were provided with instructions based on those used in the illusion of explanatory depth literature to guide their rating of understanding. Higher values represented increased perceived understanding of consensus COVID-19 information.
Perceived Belief in Consensus COVID-19 Information
At the start of W1 and after the IOED paradigm at W2, participants rated how much they believed the same nine consensus COVID-19 pieces of information, again for themselves and for “scientists and public health experts”, in random order (see Supplemental Materials for items). An independent measure of “belief” was computed for each referent group, separately, by taking mean responses across all items. Higher values represented increased belief in consensus COVID-19 information.
Cognitive Sophistication
At the start of W1, participants completed a measure of the Cognitive Reflection Test (CRT; Frederick, 2005), following the procedure used by Pennycook and Rand (2019), which combined modified versions of the original CRT items with additional non-numeric items from Thomson and Oppenheimer (2016). Participants were asked to provide an answer to seven items, such as: “If you’re running a race and you pass the person in second place, what place are you in?”, “A farmer had 15 sheep and all but eight died. How many are left?”, and “If it takes 10 s for 10 printers to print out 10 pages of paper, how many seconds will it take for 50 printers to print out 50 pages of paper?”. Correct responses were coded as a “1” and incorrect responses were coded as a “0”. Responses were averaged across items and scaled such that higher values correspond with higher levels of cognitive sophistication.
Conspiratorial Predispositions
At the start of W1, participants completed a measure of conspiratorial predisposition (Edelson et al., 2017). Participants indicated, on a 7-point scale (1 = strongly disagree, 2 = disagree, 3 = somewhat disagree, 4 = neither agree nor disagree, 5 = somewhat agree, 6 = agree, 7 = strongly agree) the extent to which they agree or disagree with the following statements: 1) “Much of our lives are being controlled by plots hatched in secret places”, 2) “Even though we live in a democracy, a few people will always run things anyway”, 3) “The people who really run the country are not known to the voters”, and 4) “Big events like wars, economic recessions, and the outcomes of elections are controlled by small groups of people who are working in secret against the rest of us”. Responses were averaged across items and scaled such that higher values correspond with higher levels of conspiratorial predispositions.
Covid-19 Conspiracy Theories
Participants were asked to report the extent to which they believe in each of six different COVID-19 conspiracies (selected from Miller, 2020), including the belief that 1) “the government is hiding the vaccine”, 2) “COVID-19” is a bioweapon engineered by the Chinese government to wage war on America and Western countries”, 3) “the coronavirus (COVID-19) originated from drinking Corona beer”, 4) “the coronavirus (COVID-19) panic has been an orchestrated effort by powerful people to close down businesses and destroy capitalism. Others do not believe this”, 5) “the coronavirus (COVID-19) was originally engineered by the U.S. military”, and 6) “that the infection rate in your country from coronavirus (COVID-19) is much higher than is reported, so as to cover up how many people have been infected. Others do not believe this”. The items were presented in random order, and responses were coded such that higher values represent increased endorsement of conspiracy theories.
COVID-19 Mitigation Behaviors
At W2, participants indicated whether they had engaged in 11 different COVID-19 mitigation behaviors. Items included social distancing behaviors, sanitization behaviors, and mask wearing. This measure was computed by calculating the total number of “Yes” responses and dividing by the total number all items. Higher values indicate increased engagement in COVID-19 mitigation behavior.
Control Variables
We included in our analysis a set of control variables including: 1) political knowledge, 2) ideological self-placement, partisan identification, and certainty in both, 3) political engagement, 4) media consumption, and 5) concern about COVID-19. These variables were controlled for in all models unless explicitly noted otherwise. The Supplemental Materials provides complete information for how these constructs were measured and computed. High values correspond with higher level of knowledge, engagement, media consumption, COVID-19 concern, conservatism, republicanism, and ideological certainty.
Results
Hypothesis 1: Does Belief in Consensus COVID-19 Information Correlate With Increased COVID-19 Mitigation?
We first sought to replicate the results of the Pilot Study that belief in COVID-19 consensus information (by the self or by scientists) would correlate with COVID-19 mitigation behaviors. To do so, we regressed using ordinary least-squares W2 COVID19 mitigation behavior on our control variables and either W1 or W2 independent variables. The results of this analysis are summarized in Table 2. Personal beliefs in consensus COVID-19 information correlated with mitigation behaviors at both time points (W1 personal beliefs, b = 0.65, CI 95% (0.48, 0.82), p < 0.001; W2 personal beliefs, b = 0.42, CI 95% (0.18, 0.59), p < 0.001) and perceptions of scientists’ beliefs correlated with mitigation behaviors at W1 (b = −0.19, CI 95% (−0.37, −0.01), p = 0.040), but not W2 (b = 0.07, CI 95% (−0.12, 0.26), p = 0.464)3. Omitting personal belief from the model, perceptions of scientists correlated with mitigation behaviors, although this only obtained significance in W2 (W1, b = 0.13, CI 95% (−0.04, 0.31), p = 0.142; W2, b = 0.32, CI 95% (0.16, 0.61), p < 0.001). While perception of scientists’ beliefs has an inconsistent relationship when accounting for other competing predictors of behavior (Table 2), both personal beliefs and perceptions of scientists’ beliefs about COVID-19, at both W1 and W2, significantly correlated with increased COVID-19 mitigation behaviors without our control variables (see Table 1).
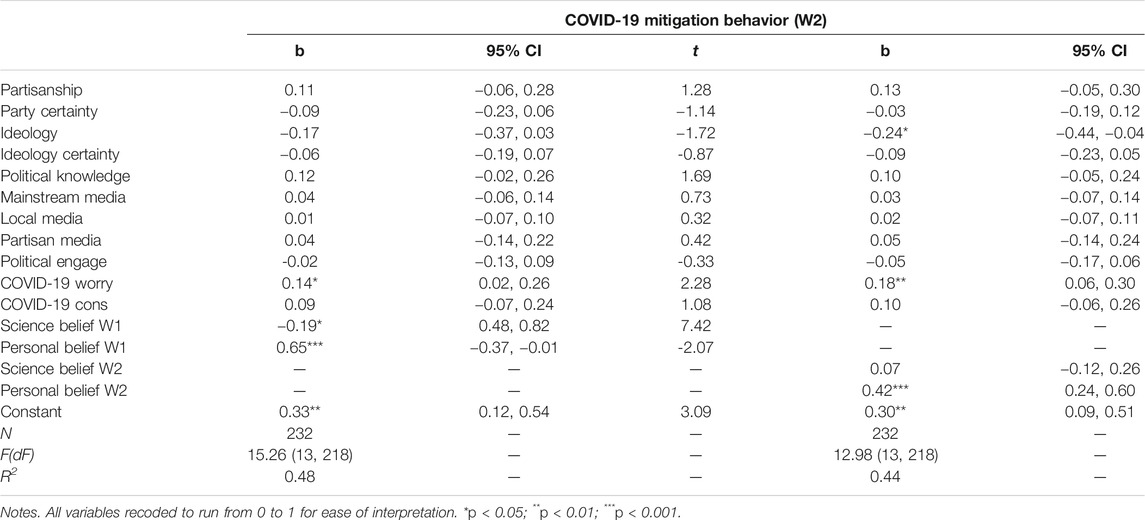
TABLE 2. COVID-19 mitigation behavior (W2).
Hypothesis 2: Does Perceived Understanding Correlate With Increased Belief in Consensus COVID-19 Information?
Next, we tested what correlated with belief in COVID-19 consensus information (by the self or perceptions of scientists’ beliefs). Our primary focus is to examine whether these two variables are associated with 1) perceived understanding of consensus COVID-19 information and 2) COVID-19 conspiracy theories, net the effect of our controls using ordinary least squares regression. The results of this analysis are summarized in Tables 3, 4.
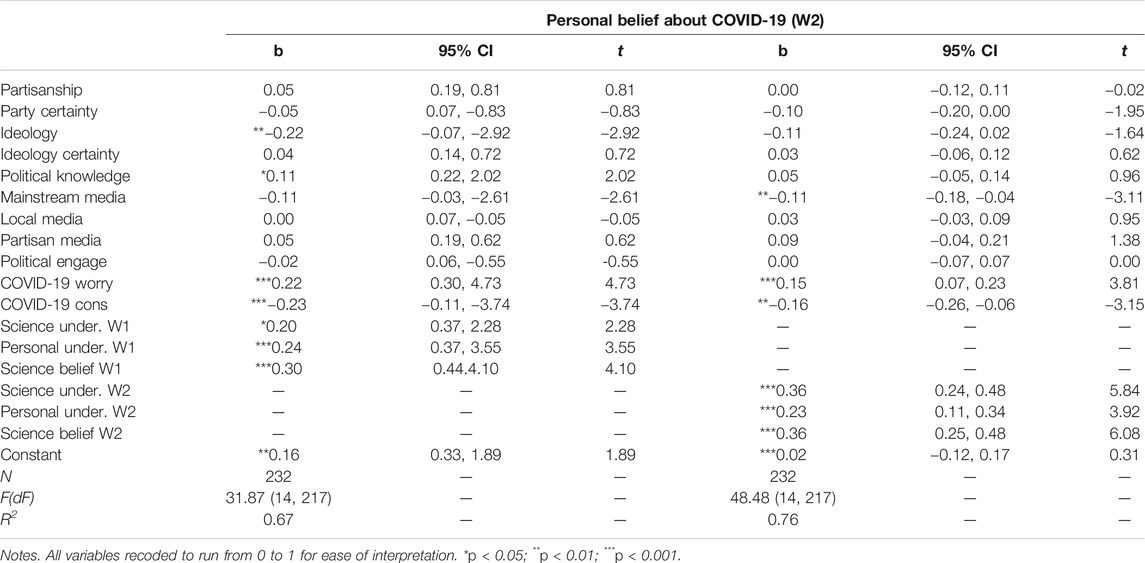
TABLE 3. Personal belief about COVID-19 (W2).
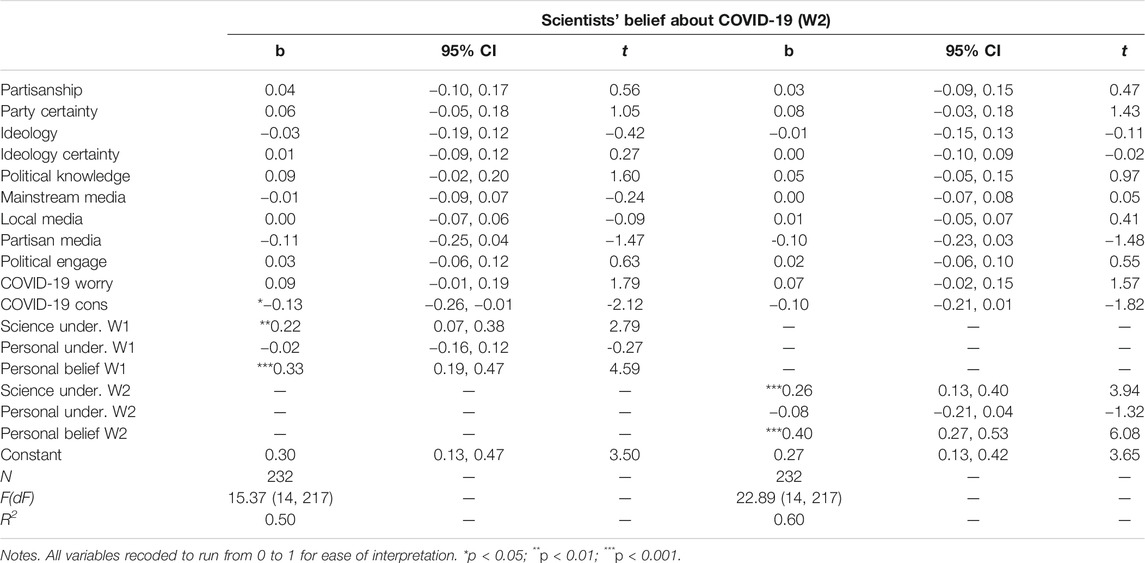
TABLE 4. Scientists’ belief about COVID-19 (W2).
We regressed W2 personal belief and W2 perceptions of scientists’ beliefs about COVID-19, separately, across a range of model specifications. In all models, we include our full set of control variables measured at W1 as well as W2 COVID-19 conspiracy theory endorsement. In our first model, we use W1 measures of perceived understanding and beliefs about COVID-19 as predictors, and in our second model we use W2 measures of perceived understanding and beliefs about COVID-19.
Consistent with the Pilot Study, our results indicate that believing consensus COVID-19 information at W2 was correlated with 1) higher personal understanding of COVID-19, measured at both W1 and W2, and 2) higher perceptions of scientists’ understanding and beliefs about COVID-19, measured at both W1 and W2. Similarly, W2 perceptions of scientists’ beliefs about consensus COVID-19 information was correlated with 1) increased perceptions that scientists understand consensus COVID-19 information, measured at both W1 and W2, and 2) increased personal beliefs in consensus COVID-19 information, measured at both W1 and W2. Personal understanding of consensus COVID-19 information did not correlate with perceptions of scientists’ belief in consensus COVID-19 information.
Hypothesis 3: Does Belief in COVID-19 Conspiracy Theories Correlate With Decreased Belief in Consensus COVID-19 Information?
Importantly, however, belief in COVID-19 conspiracy theories at W2 correlated with significantly reduced personal belief, and perceptions of scientists’ belief, in consensus COVID-19 information. Moving from the lowest to the highest levels of support for COVID-19 conspiracies corresponded with a decrease of approximately 16–23% and 10–14% in personal beliefs and perceptions of scientists’ beliefs in COVID-19 consensus information, respectively.
Summary of Observational Findings
Overall, we have provided evidence that mitigation behaviors are correlated with belief in consensus COVID-19 information. Belief in this consensus information was strengthened by self and expert understanding of the information, and, importantly, weakened by endorsement of conspiracy theories. We next turn to exploring what could reduce endorsement of conspiracy theories.
Hypothesis 4: Will Revealing the Illusion of Explanatory Depth Reduce Perceived Understanding of COVID-19 Consensus Information and Support for COVID-19 Conspiracies?
We examined the IOED for both the explanation and description condition. To do so, a mixed 2 (time point: pre-IOED rating vs. post-IOED rating; within) x 2 (condition: explanation vs. description; between) ANOVA was used to compare differences in self-reported understanding of COVID-19 conspiracy theories, pre-IOED to post-IOED. This analysis indicated a significant main effect of time point (F (1, 230) = 9.33, p = 0.002; Overall pre-IOED M = 0.38, SD = 0.39; Overall post-IOED M = 0.42, SD = 0.30). There was no main effect of condition and there was not a significant interaction (ps > 0.21; Explanation pre-IOED M = 0.35, SD = 0.29; Explanation post-IOED M = 0.40, SD = 0.30; Description pre-IOED M = 0.40, SD = 0.30; Description post-IOED M = 0.44, SD = 0.30). Thus, we observe change in perceived understanding of conspiracies as a function of the IOED task. But, and in contrast to prior work on the IOED, instead of revealing the illusion and reducing perceived understanding, we observe significant increases in perceived understanding (see Figure 1).
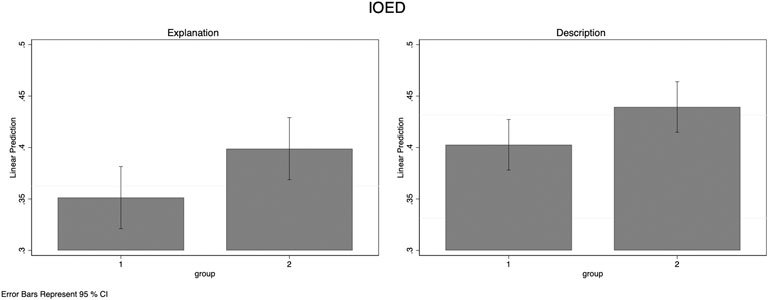
FIGURE 1. Between-subject comparison of mean-level perceived understanding of COVID-19 conspiracy theories, pre and post IOED, for participants in the explanation or description conditions.
We next explored whether an increase in understanding of COVID-19 conspiracy theories was common across all of our participants or, alternatively, driven by a subset of our participants. Across both conditions, 30.17% showed increased post-IOED ratings (description condition, 29.75%; explanation condition, 30.63%), 40.52% reported decreases in their ratings post-IOED (description condition, 41.32%; explanation condition, 39.64%), and 29.3% of participants showed zero change in their understanding ratings pre to post-IOED (description condition, 28.93%; explanation condition, 29.73%). In short, we find that the increase in post-IOED ratings is driven by a subset of our participants.
What differentiates people who increased their perceived understanding of conspiracies after the IOED task from people who did not? We examined whether overall cognitive sophistication and conspiratorial predisposition, known correlates of endorsement for conspiracies more generally, correlated with change in perceived understanding. We computed a difference score between perceived understanding (post-IOED minus pre-IOED), such that positive values correspond with increases in perceived understanding.4 We regressed the IOED difference score (collapsed across IOED condition given the lack of differences found for that manipulation) on a model including all of our control variable measures and W1 measures of perceived understanding of and beliefs in consensus COVID-19 information, and both conspiratorial predispositions and cognitive sophistication (see Table 5). Whereas conspiratorial predispositions significantly correlated with increased perceived understanding of COVID-19 conspiracies after the IOED task (b = 0.16, CI 95% (0.08, 0.24), p < 0.001), cognitive sophistication was not significantly related to change in perceived understanding (b = 0.01, CI 95% (−0.07, 0.08), p = 0.876).
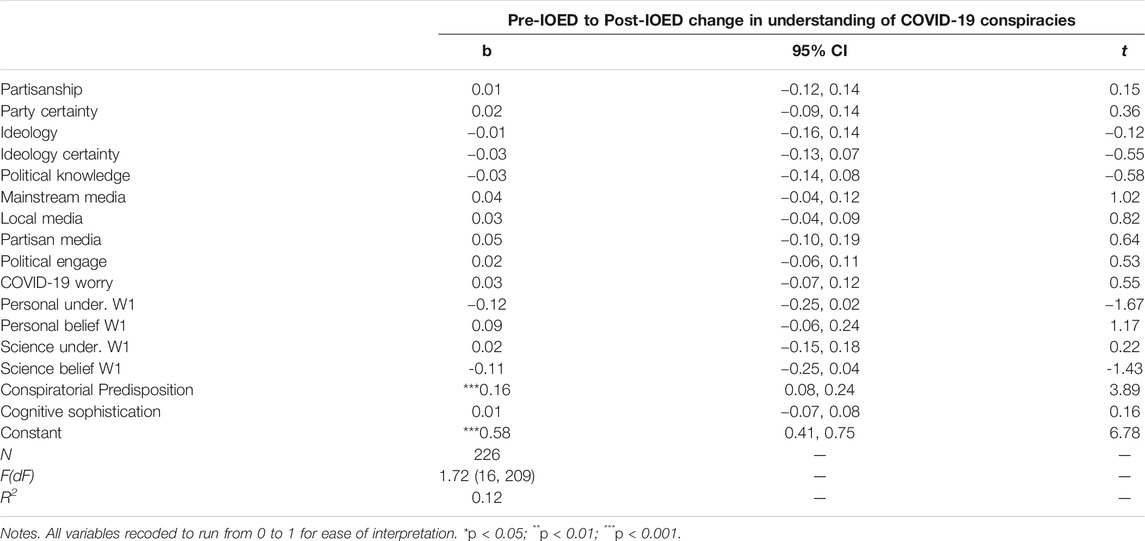
TABLE 5. Pre-IOED to Post-IOED change in understanding of COVID-19 conspiracies.
Does change in understanding of conspiracies correlate with their endorsement? For this analysis, we regress support for COVID-19 conspiracies (measured at W2) on the full set of W1 controls variables and the IOED difference variable. This analysis is graphically represented in Figure 2. Results indicate that increased perceived understanding of conspiracies significantly correlated with increased support for COVID-19 conspiracies (b = 0.22, CI 95% (0.06, 0.37), p = 0.007; Table 6). To strengthen our inferences concerning whether increases or decreases in understanding of COVID-19 conspiracy theories, post-IOED, is driving this relationship, we computed two dummy-variables with categorization as “increase” or “decrease” coded as a “1”, and the “no change” group as the referent, coded as a “0”. This allows for a comparison between “increase” and “no change” or “decrease” and “no change”. Compared to participants who did not show change in understanding post-IOED, those who increased understanding post-IOED were more likely to endorse COVID-19 conspiracies (b = 0.06, CI 95% (0.00, 0.12), p = 0.053); however, those who decreased understanding post-IOED were not any more or less likely to endorse COVID-19 conspiracies then those who did not change understanding post-IOED (b = 0.003, CI 95% (−0.05, 0.06), p = 0.926).
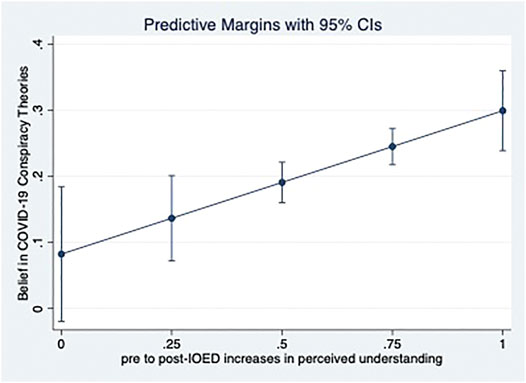
FIGURE 2. Pre to post IOED change in perceived understanding of COVID-19 conspiracy theories and belief in COVID-19 conspiracies.
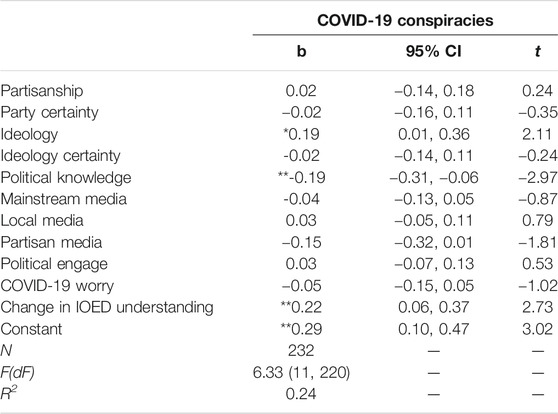
TABLE 6. COVID-19 conspiracies.
Finally, we examined the extent to which change in perceived understanding of COVID-19 conspiracies correlated with perceived understanding of consensus COVID-19 information. Here, we are able to take advantage of the panel design of our measures that straddled the IOED. We examined whether changes post-IOED in understanding of COVID-19 conspiracy theories correlated with W1 to W2 change in perceptions of one’s own or scientists’ understanding of consensus COVID-19 information, separately. For this analysis, we regress W2 dependent variables on W1 control variables, W1 and W2 measures of understanding and belief (other than what is estimated as the dependent variables), and the IOED difference score, interpreting coefficients for the latter as predicting W1 to W2 change in the dependent variables. Results indicate that an increase post-IOED in perceived understanding of COVID-19 conspiracies correlated with significantly reduced perceived understanding of consensus COVID-19 information from W1 to W2 (b = −0.21, CI 95% (−0.33, −0.10), p < 0.001). In contrast, we did not observe a significant relationship between the IOED difference score and perceptions of scientists’ understanding (b = 0.03, CI 95% (−0.07, 0.13), p = 0.51). These results are summarized in Table 7.
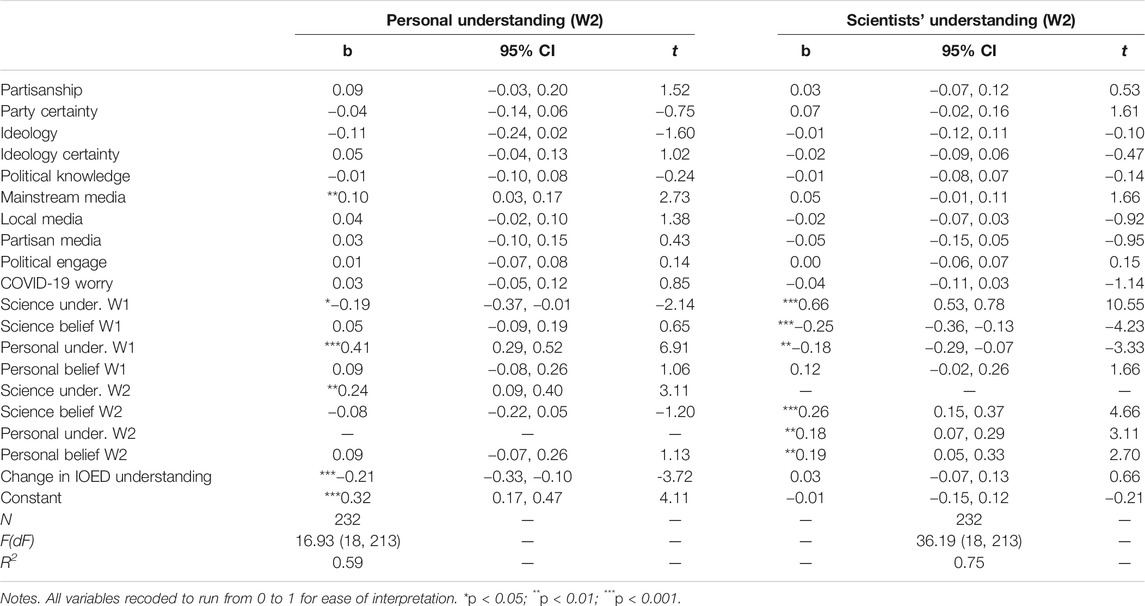
TABLE 7. Personal and Scientists Understanding (W2).
Again, we estimated the same models above for perceived understanding, but swapped in the two dummy-variables as an alternative to the IOED difference score. Results indicate that, compared to participants who did not show change in understanding post-IOED, those who increased understanding post-IOED were more likely to report W1 to W2 decreases in perceived understanding of consensus COVID-19 information (b = −0.06, CI 95% (−0.10, −0.01), p = 0.013); however, those who decreased understanding post-IOED were not significantly different from those who did not change understanding post-IOED (b = 0.01, CI 95% (−0.03, 0.05), p = 0.745).
Discussion
We examined beliefs about consensus COVID-19 information and its implications for COVID-19 mitigation behaviors. We find that belief in COVID-19 consensus information (by the self or perceptions of scientists’ beliefs) correlates with COVID-19 mitigation behaviors. Importantly, belief in COVID-19 consensus information was correlated with perceived understanding of COVID-19 consensus information. We also demonstrate that belief in COVID-19 conspiracies correlated with significantly reduced belief in and perceptions of scientists’ belief in COVID-19 consensus information. While we do observe significant bivariate correlations, perceived understanding and COVID-19 conspiracies do not correlate with COVID-19 behavioral mitigation independent of our control variables, consistent with the observations reported by Hornick et al. (2020). Together, these results indicate that perceived understanding and COVID-19 conspiracy theories may indirectly influence compliance with COVID-19 mitigation through its relationship to beliefs about COVID-19.
Importantly, we also implemented an IOED paradigm (Rozenblit and Keil, 2002) to experimentally manipulate perceived understanding of COVID-19 conspiracies and, consequently, influence support for these theories. Our findings with the IOED paradigm are important for two reasons. First, we provide a novel demonstration of how explanation or description influences understanding of phenomena generally seen as implausible or improbable. Prior research indicates that the act of explanation leads to reductions in belief confidence (Rozenblit and Keil, 2002; Fernbach et al., 2013; Vitriol and Marsh, 2018). However, for COVID-19 conspiracy theories, the act of explanation or description increased perceived understanding. While previous research has consistently shown a decrease in understanding after explanation alone (vs. description), we observed an equivalent increase for both the explanation and description conditions. We think that the lack of difference between our conditions helps illustrate why we find an overall increase. Our tested conspiracy theories are phenomena that people should have much less familiarity with than phenomena usually tested in IOED work (e.g., how a faucet works). Participants may have so little self-perceived knowledge about these conspiracy theories that the act of reflecting on conspiracy theories in any way may help generate information that was not previously believed or increased cognitive fluency in one’s understanding of COVID-19 conspiracy theories in a way that inflates perceived validity (e.g., DiFonzo et al., 2016). This in turn may lead to greater perceptions of understanding. In this way, instead of revealing the limitations of one’s causal understanding, being tasked with explaining or describing the existence of implausible or improbable phenomena may ironically raise perceived causal understanding. Future research should seek to replicate and extend these observations across a broader range of conspiracy theories and epistemically suspect beliefs, using both description and explanation prompts, to better understand this phenomenon.
Our findings with the IOED paradigm are also important because we gain some leverage for causal inference regarding the consequences of COVID-19 conspiracies for perceived understanding and beliefs about COVID-19. Not all of our participants showed a pre to post-IOED increase despite an overall mean increase in ratings; while almost a third showed increased post-IOED ratings, 40% reported decreases in their ratings post-IOED, and less than a third of participants showed zero change in their understanding ratings pre to post-IOED. Pre to post-IOED increases were correlated with high levels of conspiratorial predispositions. Increases in understanding correlated with increased endorsement of COVID-19 conspiracies and reduced perceived understanding of COVID-19 consensus information. These results strengthen our claim that COVID-19 conspiracy theories are consequential for COVID-19 beliefs and behaviors. Our results also suggest that time and attention given to COVID-19 conspiracies may be misguided; describing or explaining the existence of COVID-19 conspiracies may ironically increase support for these accounts and undermine knowledge about, belief in, and willingness to engage in COVID-19 mitigation for those people already predisposed to believing in conspiracies. Instead, communications and recommendations from public health experts should focus, first and foremost, on increasing belief in and acceptance of consensus COVID-19 information and, secondarily, increasing understanding of this information (also see Rabb et al., 2019; Clark et al., 2020; Marsh et al., 2021).
Despite the strength of our evidence across both samples, our study is nonetheless limited by its exclusive reliance upon MTurk samples. MTurk samples may be older and more diverse than student samples, and more nationally representative than typical internet samples (e.g., Berinsky et al., 2012), but are not a representative, random sample of the American public. This limitation is particularly notable for correlational or observational studies. Further, our sample was limited to U.S. citizens. Future research should investigate the generalizability of our observations to samples more representative of the U.S. and the international community (e.g., Vitriol et al., 2019) in order to better understand beliefs about COVID-19 and its implications for COVID-19 mitigation behaviors. By understanding lay beliefs about COVID-19, public health practitioners can better identify who is likely to resist their advice and target those individuals with more effective messages designed to increase compliance. Doing so will help both individuals and their communities combat the spread of COVID-19 and the pandemics after that.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Lehigh University Institutional Review Board (project title: The Illusion of Explanatory Depth).
Author Contributions
JV and JM jointly generated the original research question and developed the project concept. Data preparation was conducted by JM and analysis was conducted by JV. JV generated the first draft of the manuscript and JM provided critical oversight and revision. All authors contributed to interpreting the results, drafting the manuscript, and approving the final version for submission.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpos.2021.648082/full#supplementary-material
Footnotes
1Due to a coding error, only 27% of participants in the Pilot Study and 80% of participants in the main Study completed demographic measures. For these reasons, we use these data to describe our sample but do not control for demographic characteristics in our model specification.
2Participants were asked to rate how familiar (1 = Not familiar at all, 2 = Slightly familiar, 3 = Moderately familiar, 4 = Very familiar, 5 = Extremely familiar) they were with each of the three COVID-19 conspiracies used in the W2 IOED paradigm (M = 3.23, SD = 1.03) and a non-conspiratorial item (“Some people believe that the coronavirus (COVID-19) panic originated in Wuhan China. Others do not believe this”; M = 4.05, SD = 1.04). Thus, familiarity with the conspiracy theories was lower than the non-conspiratorial item and below the mid-point, but not so low as to constrain variability in responding.
3These results are unchanged when including measures of perceived understanding of consensus COVID-19 information as covariates, suggesting that belief correlates with COVID-19 mitigation behavior independent of these constructs.
4We arrive at statistically similar results and conclusions when, instead of using a difference score, we control for pre-IOED perceived understanding and use post-IOED understanding as the predictor.
References
Al-Hasan, A., Yim, D., and Khuntia, J. (2020). Citizens’ Adherence to COVID-19 Mitigation Recommendations by the Government: A 3-country Comparative Evaluation Using Web-Based Cross-Sectional Survey Data. J. Med. Internet Res. 22 (8), e20634. doi:10.2196/20634
Allcott, H., Boxell, L., Conway, J., Gentzkow, M., Thaler, M., and Yang, D. Y. (2020). Polarization and Public Health: Partisan Differences in Social Distancing during COVID-19. SSRN J. doi:10.2139/ssrn.3570274
Allington, D., Duffy, B., Wessely, S., Dhavan, N., and Rubin, J. (2020). Health-Protective Behaviour, Social Media Usage and Conspiracy Belief During the COVID-19 Public Health Emergency. Psychol. med., 1–7. doi:10.1017/S003329172000224X
Alter, A. L., Oppenheimer, D. M., and Zemla, J. C. (2010). Missing the Trees for the forest: A Construal Level Account of the Illusion of Explanatory Depth. J. Personal. Soc. Psychol. 99 (3), 436–451. doi:10.1037/a0020218
Anderson, R. M., Heesterbeek, H., Klinkenberg, D., and Hollingsworth, T. D. (2020). How Will Country-Based Mitigation Measures Influence the Course of the COVID-19 Epidemic? The Lancet, 395 (10228), 931–934. doi:10.1016/S0140-6736(20)30567-5
Berinsky, A. J., Huber, G. A., and Lenz, G. S. (2012). Evaluating Online Labor Markets for Experimental Research: Amazon.Com's Mechanical Turk. Polit. Anal. 20 (3), 351–368. doi:10.1093/pan/mpr057
Bish, A., and Michie, S. (2010). Demographic and Attitudinal Determinants of Protective Behaviours during a Pandemic: A Review. Br. J. Health Psychol. 15 (4), 797–824. doi:10.1348/135910710X485826
Brennen, J. S., Howard, P. N., Nielsen, R. K., and Nielsen, R. K. (2020). “Balancing Product Reviews, Traffic Targets, and Industry Criticism: UK Technology Journalism in Practice,”. in Types, Sources, and Claims of COVID-19 Misinformation. Journalism Pract. 7. Reuters Institute, 1–18. doi:10.1080/17512786.2020.1783567
Bridgman, A., Merkley, E., Loewen, P. J., Owen, T., Ruths, D., Teichmann, L., et al. (2020). “The Causes and Consequences of Covid-19 Misperceptions: Understanding the Role of News and Social media”. The Harvard Kennedy School (HKS) Misinformation Review. doi:10.37016/mr-2020-028
Bruine de Bruin, W., and Bennett, D. (2020). Relationships between Initial COVID-19 Risk Perceptions and Protective Health Behaviors: A National Survey. Am. J. Prev. Med. 59 (2), 157–167. doi:10.1016/j.amepre.2020.05.001
Bruine de Bruin, W., Saw, H.-W., and Goldman, D. P. (2020). Political Polarization in US Residents' COVID-19 Risk Perceptions, Policy Preferences, and Protective Behaviors. J. Risk Uncertain 61, 177–194. doi:10.1007/s11166-020-09336-3
Calvillo, D. P., Ross, B. J., Garcia, R. J. B., Smelter, T. J., and Rutchick, A. M. (2020). Political Ideology Predicts Perceptions of the Threat of Covid-19 (And Susceptibility to Fake News about it). Soc. Psychol. Personal. Sci. 11 (8), 1119–1128. doi:10.1177/1948550620940539
Centers for Disease Control (2020). Prevent getting sick. Centers for Disease Control and Prevention. Retrieved from: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/socialdistancing.html (Accessed December 1, 2020).
Clark, C., Davila, A., Regis, M., and Kraus, S. (2020). Predictors of COVID-19 Voluntary Compliance Behaviors: An International Investigation. Glob. Transitions 2, 76–82. doi:10.1016/j.glt.2020.06.003
Clinton, J., Cohen, J., Lapinski, J. S., and Trussler, M. (2020). Partisan Pandemic: How Partisanship and Public Health Concerns Affect Individuals' Social Distancing during COVID-19. SSRN J. doi:10.2139/ssrn.3633934
Cohen, M. S., and Corey, L. (2020). Combination Prevention for COVID-19. Science 368 (6491), 551. doi:10.1126/science.abc5798
Depoux, A., Martin, S., Karafillakis, E., Preet, R., Wilder-Smith, A., and Larson, H. (2020). The Pandemic of Social media Panic Travels Faster Than the COVID-19 Outbreak. J. Trav. Med. 27 (3), taaa031. doi:10.1093/jtm/taaa031
DiFonzo, N., Beckstead, J. W., Stupak, N., and Walders, K. (2016). Validity Judgments of Rumors Heard Multiple Times: The Shape of the Truth Effect. Social Influence 11 (1), 22–39. doi:10.1080/15534510.2015.1137224
Druckman, J. N., Klar, S., Krupnikov, Y., Levendusky, M., and Ryan, J. B. (2020). Affective Polarization, Local Contexts and Public Opinion in America. Nat. Hum. Behav. 5, 28–38. doi:10.1038/s41562-020-01012-5
Dunning, D., Johnson, K., Ehrlinger, J., and Kruger, J. (2003). Why People Fail to Recognize Their Own Incompetence. Curr. Dir. Psychol. Sci. 12 (3), 83–87. doi:10.1111/1467-8721.01235
Edelson, J., Alduncin, A., Krewson, C., Sieja, J. A., and Uscinski, J. E. (2017). The Effect of Conspiratorial Thinking and Motivated Reasoning on Belief in Election Fraud. Political Res. Q. 70, 933–946. doi:10.1177/1065912917721061
Fernbach, P. M., Rogers, T., Fox, C. R., and Sloman, S. A. (2013). Political Extremism Is Supported by an Illusion of Understanding. Psychol. Sci. 24 (6), 939–946. doi:10.1177/0956797612464058
Finset, A., Bosworth, H., ButowGulbrandsen, P. P., Gulbrandsen, P., Hulsman, R. L., Pieterse, A. H., et al. (2020). Effective Health Communication - a Key Factor in Fighting the COVID-19 Pandemic. Patient Educ. Couns. 103 (5), 873–876. doi:10.1016/j.pec.2020.03.027
Frederick, S. (2005). Cognitive Reflection and Decision Making. J. Econ. Perspect. 19, 25–42. doi:10.1257/089533005775196732
Gollwitzer, A., Martel, C., Brady, W. J., Pärnamets, P., Freedman, I. G., Knowles, E. D., et al. (2020). Partisan Differences in Physical Distancing Are Linked to Health Outcomes during the COVID-19 Pandemic. Nat. Hum. Behav. 4 (11), 1186–1197. doi:10.1038/s41562-020-00977-7
Götz, F. M., Gvirtz, A., Galinsky, A. D., and Jachimowicz, J. M. (2020). How Personality and Policy Predict Pandemic Behavior: Understanding Sheltering-In-Place in 55 Countries at the Onset of COVID-19. Am. Psychol. 76 (999), 39–49. doi:10.1037/amp0000740
Grossman, G., Kim, S., Rexer, J. M., and Thirumurthy, H. (2020). Political Partisanship Influences Behavioral Responses to Governors' Recommendations for COVID-19 Prevention in the United States. Proc. Natl. Acad. Sci. USA 117, 24144–24153. doi:10.1073/pnas.2007835117
Haushofer, J., and Metcalf, C. J. E. (2020). Which Interventions Work Best in a Pandemic? Science 368, 1063–1065. doi:10.1126/science.abb6144
Hornik, R., Kikut, A., Jesch, E., Woko, C., Siegel, L., and Kim, K. (2020). Association of COVID-19 Misinformation with Face Mask Wearing and Social Distancing in a Nationally Representative U.S. Sample. PsyArXiv. Retrieved from: https://psyarxiv.com/k8pds/ (Accessed December 1, 2020).
Hornik, R., Woko, C., Siegel, L., Kim, K., Kikut, A., and Jesch, E. (2020). What Beliefs are Associated with COVID Vaccination Intentions? Implications for Campaign Planning. doi:10.31234/osf.io/t3kyx
Kouzy, R., Abi Jaoude, J., Kraitem, A., El Alam, M. B., Karam, B., Adib, E., et al. (2020). Coronavirus Goes Viral: Quantifying the COVID-19 Misinformation Epidemic on Twitter. Cureus 12 (3), e7255. doi:10.7759/cureus.7255
Marsh, J. K., and Romano, A. L. (2016). Lay Judgments of Mental Health Treatment Options. MDM Pol. Pract. 1 (1), 238146831666936. doi:10.1177/2381468316669361
Marsh, J. K., and Vitriol, J. A. (2018). “Explanation Hubris and Conspiracy Theories: A Case of the 2016 Presidential Election,” in Proceedings of the 40th Annual Conference of the Cognitive Science Society. Editors T. T. Rogers, M. Rau, X. Zhu, and C. W. Kalish (Austin, TX: Cognitive Science Society), 2090–2095.
Marsh, J. K., and Zeveney, A. (2015). “Naïve Beliefs about Intervening on Causes and Symptoms in the Health Domain,” in Proceedings of the 37th Annual Conference of the Cognitive Science Society. Editors D. C. Noelle, R. Dale, A. S. Warlaumont, J. Yoshimi, T. Matlock, C. D. Jennings, and P. P. Maglio (Austin, TX:Cognitive Science Society), 1529–1534.
Marsh, J. K., Ungson, N. D., and Packer, D. J. (2021). Bring Out Your Experts: The Influence of Perceived Expert Causal Understanding on Pandemic Behaviors. Manuscript submitted for publication.
Merkley, E., and Loewen, P. J. (2021). Anti-intellectualism and the Mass Public’s Response to the COVID-19 Pandemic. Nat. Hum. Behav. doi:10.1038/s41562-021-01112-w
Mian, A., and Khan, S. (2020). Coronavirus. The Spread of Misinformation. BMC Med. 18 (1), 89. doi:10.1186/s12916-020-01556-3
Miller, J. M. (2020). Do COVID-19 Conspiracy Theory Beliefs Form a Monological Belief System? Can. J. Pol. Sci. 53 (2), 319–326. doi:10.1017/s0008423920000517
Motta, M., and Callaghan, T. (2020). The Pervasiveness and Policy Consequences of Medical Folk Wisdom in the US. Scientific Rep. 10. doi:10.1038/s41598-020-67744-6
Motta, M., Callaghan, T., and Sylvester, S. (2018). Knowing Less but Presuming More: Dunning-Kruger Effects and the Endorsement of Anti-vaccine Policy Attitudes. Soc. Sci. Med. 211, 274–281. doi:10.1016/j.socscimed.2018.06.032
Motta, M., Stecula, D., and Farhart, C. (2020). How Right-Leaning Media Coverage of COVID-19 Facilitated the Spread of Misinformation in the Early Stages of the Pandemic in the U.S. Can. J. Pol. Sci. 53, 335–342. doi:10.1017/S0008423920000396
Paolacci, G., and Chandler, J. (2014). Inside the Turk. Curr. Dir. Psychol. Sci. 23 (3), 184–188. doi:10.1177/0963721414531598
Pennycook, G., Cheyne, J. A., Koehler, D. J., and Fugelsang, J. A. (2020). On the Belief that Beliefs Should Change According to Evidence: Implications for Conspiratorial, Moral, Paranormal, Political, Religious, and Science Beliefs. Judgment Decis. making, 15 (4), 476. doi:10.31234/osf.io/a7k96
Pennycook, G., and Rand, D. G. (2019). Fighting Misinformation On Social Media Using Crowdsources Judgments Of News Source Quality. Proc. Natl. Acad Sci. 116, 2521–2526.
Pew Research Center (2020a). Public Assessments of the U.S. Coronavirus. Retrieved at: https://www.pewresearch.org/politics/2020/08/06/public-assessments-of-the-u-s-coronavirus-outbreak/ (Accessed December 1, 2020).
Pew Research Center (2020b). Most Americans Say Coronavirus Outbreak Has Impacted Their Lives. Retrieved from: https://www.pewsocialtrends.org/2020/03/30/most-americans-say-coronavirus-outbreak-has-impacted-their-lives/ (Accessed December 1, 2020).
Pfattheicher, S., Nockur, L., Böhm, R., Sassenrath, C., and Petersen, M. B. (2020). The Emotional Path to Action: Empathy Promotes Physical Distancing and Wearing of Face Masks during the COVID-19 Pandemic. Psychological Science 31, 1363–1373. doi:10.31234/osf.io/y2cg5
Prather, K. A., Wang, C. C., and Schooley, R. T. (2020). Reducing Transmission of SARS-CoV-2. Science 368, 1422–1424. doi:10.1126/science.abc6197
Rabb, N., Fernbach, P. M., and Sloman, S. A. (2019). Individual Representation in a Community of Knowledge. Trends Cogn. Sci. 23 (10), 891–902. doi:10.1016/j.tics.2019.07.011
Raimi, K. T., and Leary, M. R. (2014). Belief Superiority in the Environmental Domain: Attitude Extremity and Reactions to Fracking. J. Environ. Psychol. 40, 76–85. doi:10.1016/j.jenvp.2014.05.005
Roozenbeek, J., Schneider, C. R., Dryhurst, S., Kerr, J., Freeman, A. L. J., Recchia, G., et al. (2020). Susceptibility to Misinformation about COVID-19 Around the World. R. Soc. Open Sci. 7 (10), 201199. doi:10.1098/rsos.201199
Rozenblit, L., and Keil, F. (2002). The Misunderstood Limits of Folk Science: An Illusion of Explanatory Depth. Cogn. Sci. 26 (5), 521–562. doi:10.1207/s15516709cog2605_1
Sharma, M., Yadav, K., Yadav, N., and Ferdinand, K. C. (2017). Zika Virus Pandemic-Analysis of Facebook as a Social media Health Information Platform. Am. J. Infect. Control, 45 (3), 301–302. doi:10.1016/j.ajic.2016.08.022
Sloman, S. A., and Rabb, N. (2016). Your Understanding Is My Understanding. Psychol. Sci. 27 (11), 1451–1460. doi:10.1177/0956797616662271
Teovanovic, P., Lukic, P., Zupan, Z., Lazić, A., Ninković, M., and Zezelj, I. (2020). Irrational Beliefs Differentially Predict Adherence to Guidelines and Pseudoscientific Practices during the COVID-19 Pandemic. PsyArXiv. doi:10.31234/osf.io/gefhn
Thomson, K. S., and Oppenheimer, D. M. (2016). Investigating an alternate form of the cognitive reflection test. Judgment and Decision Making, Society for Judgment and Decision Making 11, 99–113.
Uscinski, J. E., Enders, A. M., Klofstad, C., Seelig, M., Funchion, J., Everett, C., et al. (2020). Why Do People Believe COVID-19 Conspiracy Theories? HKS Misinfo Rev. 1 (3). doi:10.37016/mr-2020-015
Bavel, J. J. V., Baicker, K., Boggio, P. S., Capraro, V., Cichocka, A., Cikara, M., et al. (2020). Using Social and Behavioural Science to Support COVID-19 Pandemic Response. Nat. Hum. Behav. 4 (5), 460–471. doi:10.1038/s41562-020-0884-z
van Mulukom, V., Pummerer, L., Čavojová, V., Šrol, J., Zezelj, I., Marinthe, G., et al. (2020). Antecedents and Consequences of COVID-19 Conspiracy Theories: a Rapid Review of the Evidence. PsyArXiv.
Vitriol, J. A., and Marsh, J. K. (2018). The Illusion of Explanatory Depth and Endorsement of Conspiracy Beliefs. Eur. J. Soc. Psychol. 48, 955–969. doi:10.1002/ejsp.2504
Vitriol, J. A., Larsen, E. G., and Ludeke, S. G. (2019). The Generalizability of Personality Effects in Politics. Eur. J. Pers 33 (6), 631–641. doi:10.1002/per.2222
West, R., Michie, S., Rubin, G. J., and Amlôt, R. (2020). Applying Principles of Behaviour Change to Reduce SARS-CoV-2 Transmission. Nat. Hum. Behav. 4 (May), 451–459. doi:10.1038/s41562-020-0887-9
Wilson, R. A., and Keil, F. (1998). The Shadows and Shallows of Explanation. Minds and Machines 8 (1), 137–159. doi:10.1023/A:1008259020140
World Health Organization (2020a). Coronavirus Disease (COVID-19) Pandemic. Retrieved from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019
World Health Organization (2020b). Munich Security Conference. Retrieved from: https://www.who.int/director-general/speeches/detail/munich-security-conference
Zeveney, A. S., and Marsh, J. K. (2016). “The Illusion of Explanatory Depth in a Misunderstood Field: The IOED in Mental Disorders,” in Proceedings of the 38th Annual Conference of the Cognitive Science Society. Editors A. Pagafragou, D. Grodner, D. Mirman, and J. C. Trueswell (Austin, TX: Cognitive Science Society), 1020–1025.
Keywords: conspiracy, fake news, COVID-19, health communication, causal reasoning and explanation
Citation: Vitriol JA and Marsh JK (2021) A Pandemic of Misbelief: How Beliefs Promote or Undermine COVID-19 Mitigation. Front. Polit. Sci. 3:648082. doi: 10.3389/fpos.2021.648082
Received: 31 December 2020; Accepted: 11 May 2021;
Published: 17 June 2021.
Edited by:
Eric Merkley, University of Toronto, CanadaReviewed by:
Joseph Uscinski, University of Miami, United StatesBenjamin Lyons, University of Exeter, United Kingdom
Copyright © 2021 Vitriol and Marsh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joseph Vitriol, joevitriol@gmail.com