
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol. , 25 March 2025
Sec. Lipid and Fatty Acid Research
Volume 16 - 2025 | https://doi.org/10.3389/fphys.2025.1537484
This article is part of the Research Topic Lipids and Wasting Disorders in Disease and Aging View all articles
 Wassim Benouali1†
Wassim Benouali1† Adeline Dolly2†Aurore Bleuzen1
Adeline Dolly2†Aurore Bleuzen1 Stéphane Servais2Jean-François Dumas2‡
Stéphane Servais2Jean-François Dumas2‡ Christophe Vandier2
Christophe Vandier2 Caroline Goupille2,3†
Caroline Goupille2,3† Lobna Ouldamer2,3*†
Lobna Ouldamer2,3*†Background: Advanced epithelial ovarian cancer (EOC) patients often receive neoadjuvant platinum-based chemotherapy (NAC), with interval surgery (after three cycles of chemotherapy) considered as a major prognostic factors. We examined how changes in body composition (muscle and adipose tissue) during NAC influence prognosis.
Objective: Using CT images acquired before and during NAC in a cohort of women with advanced EOC, the aim of this study was to analyze body composition (muscle and fat mass) and see whether these parameters, at diagnosis or as they evolve during chemotherapy, can be linked to recurrence-free survival and overall survival (RFS and OS).
Material and methods: The study included 53 patients with FIGO stage III-IV epithelial ovarian cancer. CT images were analyzed to calculate skeletal muscle index (SMI), subcutaneous adipose tissue index visceral adipose tissue index estimated lean body mass (LBM) and estimated whole-body fat mass (WFM). Changes in tissue composition were normalized for 100 days and expressed as % change to account for intervals between scans at baseline and after three cycles of chemotherapy. The impact on survival was assessed by Log-rank test.
Results: At diagnosis, clinical criteria such as age or BMI did not correlate with RFS or OS. 60% of patients were considered sarcopenic (low SMI), including mainly underweight and normal-weight patients. Low SMI was not associated with RFS or OS. Twenty-six patients who underwent interval surgery demonstrated longer relapse-free intervals (p = 0.01). Notably, while muscle parameters showed minimal changes (−2%), parameters assessing adipose tissue showed significant decreases of 10, 12% and 7.6% per 100 days (VATI, SATI and estimated WFM, respectively). Obese patients were particularly affected by this loss of muscle and fat, compared with patients in other BMI categories. Rapid and severe loss of VATI (−28% per 100 days) and estimated WFM (−18% per 100 days) were significantly associated with shorter OS (p = 0.031 and p = 0.046 respectively).
Conclusion: Our findings suggests that early and substantial loss of visceral adipose tissue during NAC is a significant predictor of poor survival in advanced EOC. This highlights an urgent need for targeted nutritional or pharmaceutical strategies to mitigate fat loss and improve patients outcomes.
In addition to new targeted therapies (anti-angiogenic and PARP inhibitors), the treatment of epithelial ovarian cancer consists of primary excision surgery followed by chemotherapy (Armstrong et al., 2021). However, in patients with advanced disease, platinum-based neoadjuvant chemotherapy has been introduced as an option to decrease tumor burden and increase the optimal cytoreduction rate for complete surgery. Excisional surgery is then performed, if possible, after three or four cycles of chemotherapy, known as interval surgery. The International Federation of Gynecology and Obstetrics (FIGO) stage and residual disease after surgery remain well-recognized factors in survival prognosis (Hennessy et al., 2009), and NAC helps reduce the risk of early mortality (Melamed et al., 2021). However, epithelial ovarian cancer (EOC) is often diagnosed at an advanced stage, and the overall 5-year survival rate remains very low, at around 50% (Melamed et al., 2021; Siegel et al., 2018). These high mortality rates underline the need for new therapeutic strategies (Nikolaidi et al., 2022), and the search for markers associated with relapse or survival can help identify patients with the poorest prognosis, promote individual management and guide the search for new therapeutic targets.
Used as a standard method of managing cancer staging and follow-up, CT imaging can also provide a more accurate analysis of body composition than weight or BMI alone. Using thresholds commonly used in the literature (Martin et al., 2013a), muscle and fat areas can be quantified. After normalization for patient height, the SMI (Skeletal Muscle Index), ATI (Adipose Tissue Index), estimated LBM (Lean Body Mass) and estimated WFM (Whole-Body Fat mass) can be calculated (Shen et al., 2004; Mourtzakis et al., 2008a; Prado et al., 2008a). Clinically, the diagnosis of cancer-related sarcopenia (loss of muscle mass and functionality) may go undetected if weight loss is masked by ascites accumulation or adiposity. CT analysis provides a more precise and specific picture of body composition.
Numerous studies have attempted to identify body composition parameters at baseline (cancer diagnosis), associated with relapse and survival. A low muscular index has already been associated with poorer survival, as in pancreatic (Klassen et al., 2023) and colorectal (Hopkins et al., 2019) cancers. In ovarian cancer, the meta-analysis by Ubachs et al. (Ubachs et al., 2019) showed a significant association between low SMI and overall survival, while McSharry et al. identified only a link between muscle attenuation and survival (McSharry et al., 2020). Recently, the meta-analysis by Jin et al. (Jin et al., 2023) showed that low SMI is associated with progression-free survival, 5-year overall survival and highlighted its association with advanced FIGO stage and low BMI (<25 kg/m2) but not with histological types or chemotherapy toxicity.
Several studies show that this body composition can change progressively with muscle and/or fat loss during cancer follow-up. The origins and kinetics of these losses remain unclear (Klassen et al., 2023; Vazeille et al., 2017; Cuello et al., 2023). Associations between muscle and fat loss and outcome have been demonstrated in patients with foregut cancers, for example, (Daly et al., 2018). In a tumor-bearing rat model, adipose tissue loss and the onset of lipolysis occur before muscle loss and reduced food intake (Byerley et al., 2010). In cancer patients, weight loss is also associated with lipolysis, and the kinetics of adipose tissue loss appear to be greater than those of lean body mass. This fat loss is also accompanied by changes in circulating lipids (Murphy et al., 2010; Fouladiun et al., 2005). This lipolysis was also observed in our previous study of ovarian cancer patients. Loss of n-6 and n-3 polyunsaturated fatty acids in adipose tissue was associated with earlier relapse (Salaun et al., 2023).
While several studies suggest the importance of fatty acid metabolism in ovarian cancer progression (Cai et al., 2015; Ladanyi et al., 2018; Mukherjee et al., 2020), few clinical studies with CT analysis report the amount of adipose tissue at baseline, its evolution during treatment and its prognostic value. In 2013, Torres et al. showed that low amounts of subcutaneous adipose tissue (SAT) and intermuscular adipose tissue (IMAT) at diagnosis were associated with poorer overall survival (Torres et al., 2013). In 2022, Nakayama et al. concluded that fat loss was not associated with disease-free survival and overall survival (Nakayama et al., 2022). Huang et al. reported that muscle loss but not fat loss was associated with poor survival in a homogeneous population of stage III ovarian cancer patients (Huang et al., 2020). The latter two studies excluded patients for whom NAC was indicated. Only Rutten et al. in 2016 reported that loss of visceral adipose tissue and muscle during neoadjuvant chemotherapy negatively influenced overall survival (Rutten et al., 2016).
Given the limited amount of research in this specific area of NAC in ovarian cancer patients, we sought to assess body composition parameters (skeletal muscle and adipose tissue), at baseline and their evolution, in a cohort of women treated with NAC for advanced epithelial ovarian cancer and to determine whether these parameters or their changes during the first cycles of chemotherapy have prognostic value.
We collected data on all women with presumed advanced-stage EOC and FIGO 2009 final stage III-IV cancer (Pecorelli, 2009) managed at the University Hospital of Tours from January 2016 to December 2019. The care pathway of patients included in this study is presented in Figure 1A. During the diagnostic period, an extension workup is performed, notably using CT scans and laparoscopic biopsies. CT images acquired during this period are considered the patient’s baseline image (C0). Patients who were not eligible for primary reduction surgery were included in our study and received neoadjuvant chemotherapy (NAC) consisting of carboplatin (AUC 5) and paclitaxel (175 mg/m2) every 21 days. Women under 65 years old received a maximum of 750 mg paclitaxel per cycle, while women over 65 years old received a maximum of 600 mg per cycle. Including patients over 65 years old was essential to reflect the real-world demographic of advanced epithelial ovarian cancer (EOC), as older age is a significant factor in both disease prevalence and treatment outcomes. While older age is associated with increased sarcopenia, it also represents a critical subgroup that may experience differential responses to neoadjuvant chemotherapy (NAC) and body composition changes.
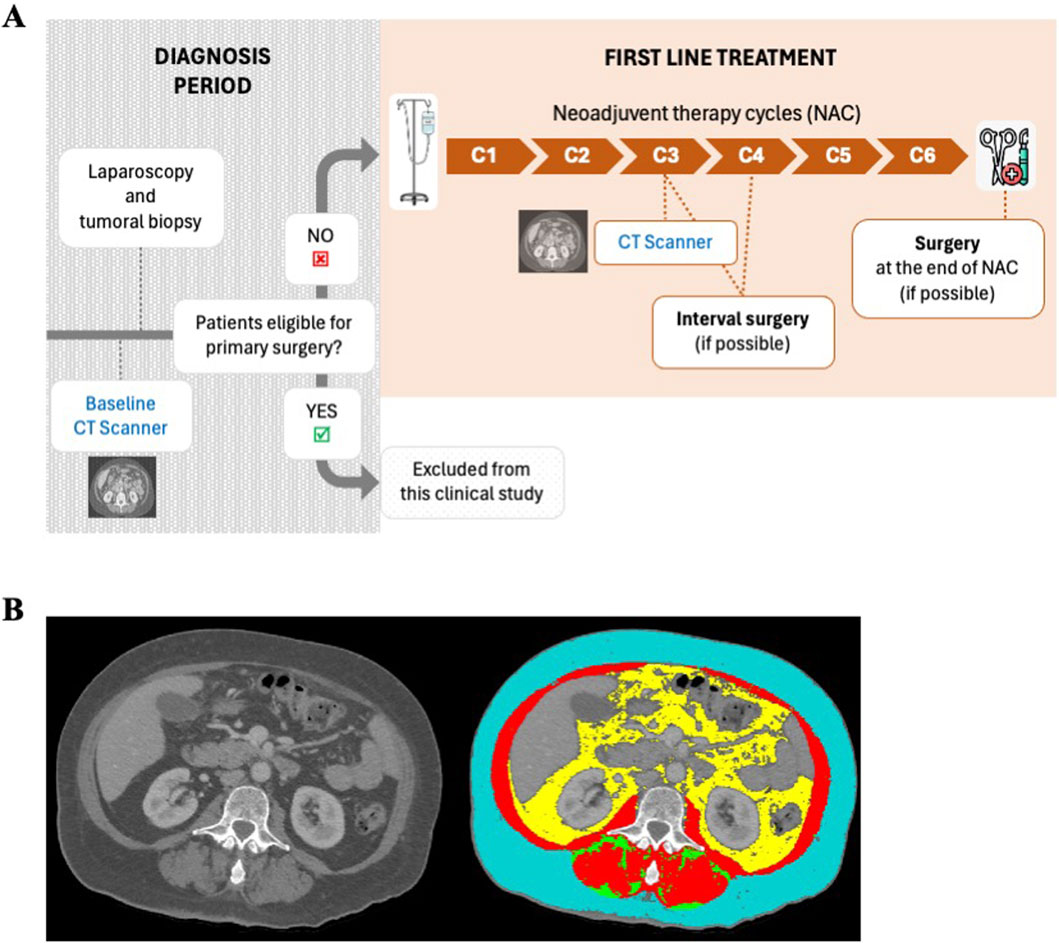
Figure 1. Care pathway and CT scans analysis of ovarian cancer patients included in our retrospective clinical study. (A) During the diagnostic period, CT scan (defined as the reference CT scan) and laparoscopy were performed to allow staging of the cancer, definition of tumor histology and operability. When not eligible for primary surgery (unsatisfactory debulking), patients underwent neoadjuvant platinum-based chemotherapy. After three to four cycles of chemotherapy, further CT imaging (defined as C3-C4 CT scan) was performed to decide whether interval surgery was possible. Fifty-three women with available CT scans (at baseline and C3-C4) were included in this retrospective clinical study. Patients eligible for primary surgery were excluded. (B) Body composition analyzed on a patient’s CT scan using SliceOmatic software (Tomovision). Tissues are identified according to their contrast in Hounsfield Units (HU): skeletal muscle in red (−29 to +150 HU), subcutaneous adipose tissue in blue (−190 to −30 HU), intermuscular adipose tissue in green (−190 to −30 HU) and visceral adipose tissue in yellow (−150 to −50 HU).
Patients eligible for primary surgery were excluded to focus on a homogeneous cohort of advanced EOC patients who required NAC. This exclusion ensures that the study population reflects those with the highest disease burden, for whom NAC is most relevant. While this limits the generalizability of findings to all EOC patients, it strengthens the internal validity of the study by reducing heterogeneity.
After three cycles of NAC, a new CT-scan was performed to assess tumor response and validate the possibility of interval surgery. CT-scan images acquired at this time are identified as C3 images. If patients were still not eligible for full surgery after three or four cycles, NAC was continued for a total of six to eight cycles.
The research protocol using anonymized CT images was approved by the institutional review board.
We retrieved the abdominopelvic CT scans initially used for cancer diagnosis/follow-up to assess patients’ body composition. An axial image of the third lumbar vertebra (L3) was selected for analysis of total muscle and fat cross-sectional areas (cm2) (Mourtzakis et al., 2008b; Prado et al., 2008b; Shen et al., 1985; Mitsiopoulos et al., 1985). Tissues were anatomically identified and quantified in predefined Hounsfield Unit (HU) ranges (Mitsiopoulos et al., 1985): skeletal muscle (−29 to +150 HU); subcutaneous adipose tissue (SAT) (−190 to −30 HU); intermuscular adipose tissue (IMAT) (−190 to −30 HU); visceral adipose tissue (VAT) (−150 to −50 HU), using Slice-O-Matic software (v.6.0; Tomovision, Magog, Canada) (Figure 1B). Measurements were performed by a radiologist, who was blinded to the patients’ treatment status.
Cross-sectional area of total muscle was normalized for stature, and skeletal muscle index (SMI; cm2/m2) was calculated (Mourtzakis et al., 2008b; Prado et al., 2008b). We used validated cut points for sarcopenia (Martin et al., 2013a): SMI <41 cm2/m2 for women. Patients with a SMI below this cut-point were considered sarcopenic. Total fat cross-sectional area was calculated as the sum of VAT, SAT and IMAT areas. For lean body mass (LBM; kg) and whole-body fat mass (WFM; kg) calculation, previously validated regression equations were used (Mourtzakis et al., 2008b; Shen et al., 1985).
Statistical analyses were performed using GraphPad Prism software for Windows (v.10.3.1, Boston, Massachusetts, United States). Categorical variables were summarized using frequency counts and percentages, and differences between groups were tested using Chi2 or Fisher’s exact tests as appropriate. Continuous variables were summarized using median and interquartile range (IQR). We used nonparametric Wilcoxon-Mann-Whitney tests (with median and interquartile range (IQR)) to compare continuous variables. Outliers were excluded using Grubbs’ test (α = 0.05).
Survival analysis was performed using Kaplan-Meier estimates to estimate the event-time distributions for recurrence-free survival (RFS) and overall survival (OS). Differences between risk groups were compared using the log-rank. Cox proportional hazards models were used to assess the multivariate effect of covariates. Statistical significance was set at a p-value less than 0.05.
We considered a p-value ≤0.05 to be statistically significant.
Fifty-three women were included in this retrospective clinical study. They received platinum-based neoadjuvant chemotherapy (NAC) for advanced epithelial ovarian cancer (EOC) and had available CT-Scans at baseline and C3 (Figure 1A). Patient characteristics are presented in Table 1. The median age was 68 years, with a wide range from 23 to 84 years. The median BMI was 24.7 kg/m2 (Interquartile Range (IQR) 21.9–27.9), with eight obese patients (15%) included in the cohort. Seventeen patients (32%) experienced body weight loss 2–6 months prior to the inclusion. Regarding tumor histology: 43 women (81%) had pure high-grade serous ovarian cancer (HGSOC) and 10 (19%) had EOC types (2 women had HGSOC mixed with undifferentiated type, two had carcinosarcomas, two had endometrioid type and three had clear-cell carcinoma type). Twenty-one (40%) had ascites removed during diagnostic laparoscopy. After three to four cycles of NAC, 49% of patients were eligible for surgery (interval surgery), while 19% could only be operated on after six cycles of chemotherapy, and 32% were not operated on at all, showing that around 50% of patients responded poorly or not at all to chemotherapy.
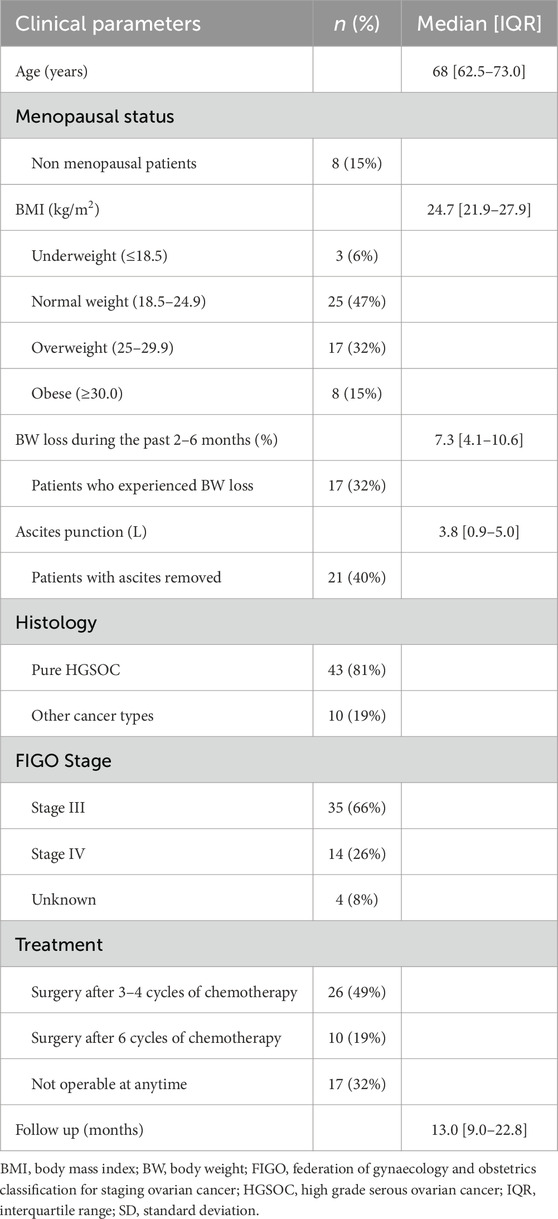
Table 1. Patient characteristics (n = 53).
We investigated the association between clinical and body composition parameters at baseline (C0) and survival in our cohort. Results are presented in Table 2 and Figure 2. For most parameters, patients were divided into tertiles, and we compared recurrence-free survival (RFS) and overall survival (OS) between tertiles 1 and 3. For BMI, patients were classified as underweight (BMI <18.5 kg/m2), normal weight (18.5 ≤ BMI <25 kg/m2), overweight (25 ≤ BMI <30 kg/m2) and obese (BMI ≥30 kg/m2). We also compared sarcopenic and non-sarcopenic patients on the basis of their skeletal muscle index (SMI<41 cm2/m2), as described in the methods section.
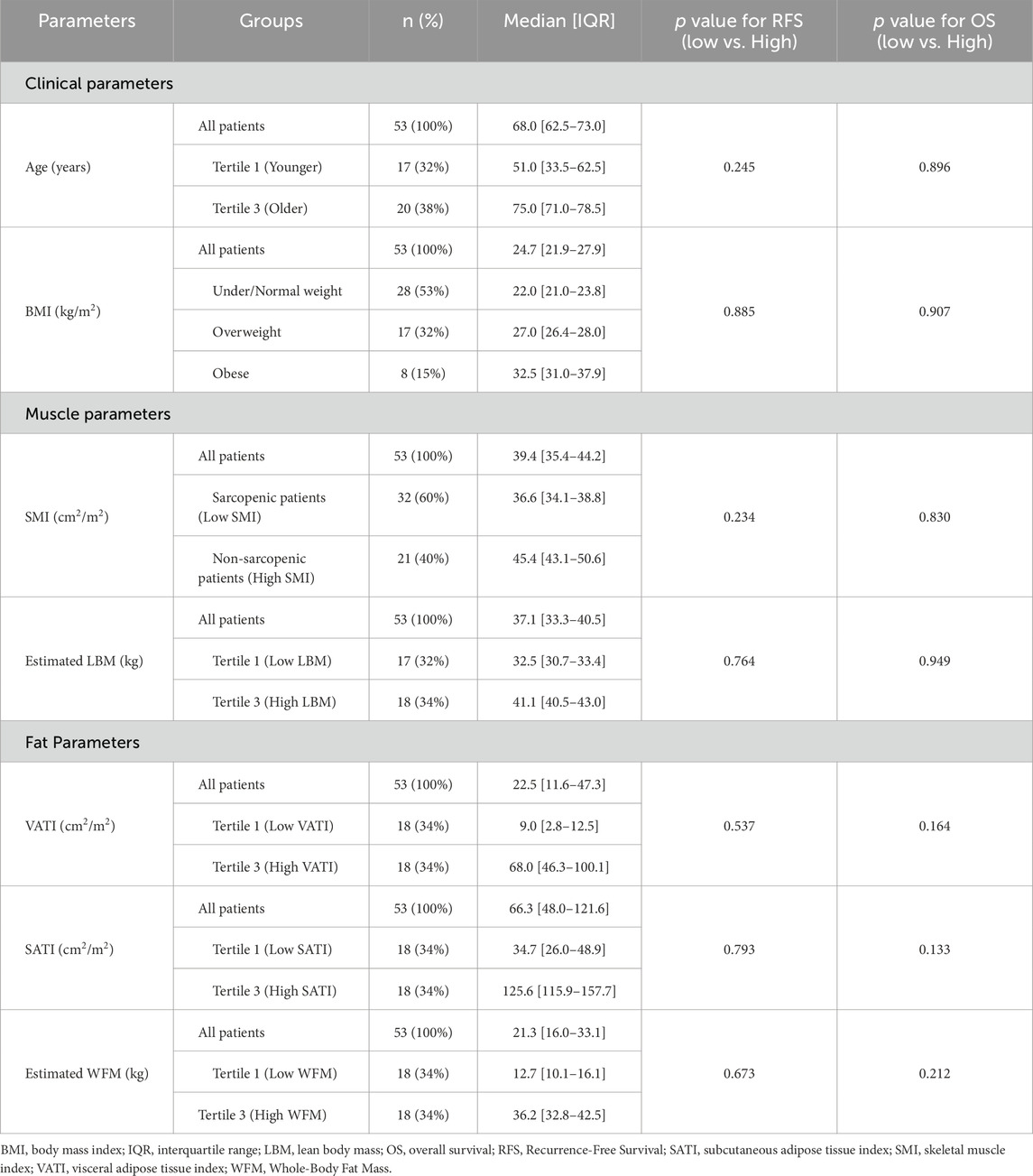
Table 2. Clinical and body composition parameters at baseline and their association with survival in ovarian cancer patients treated with NAC.
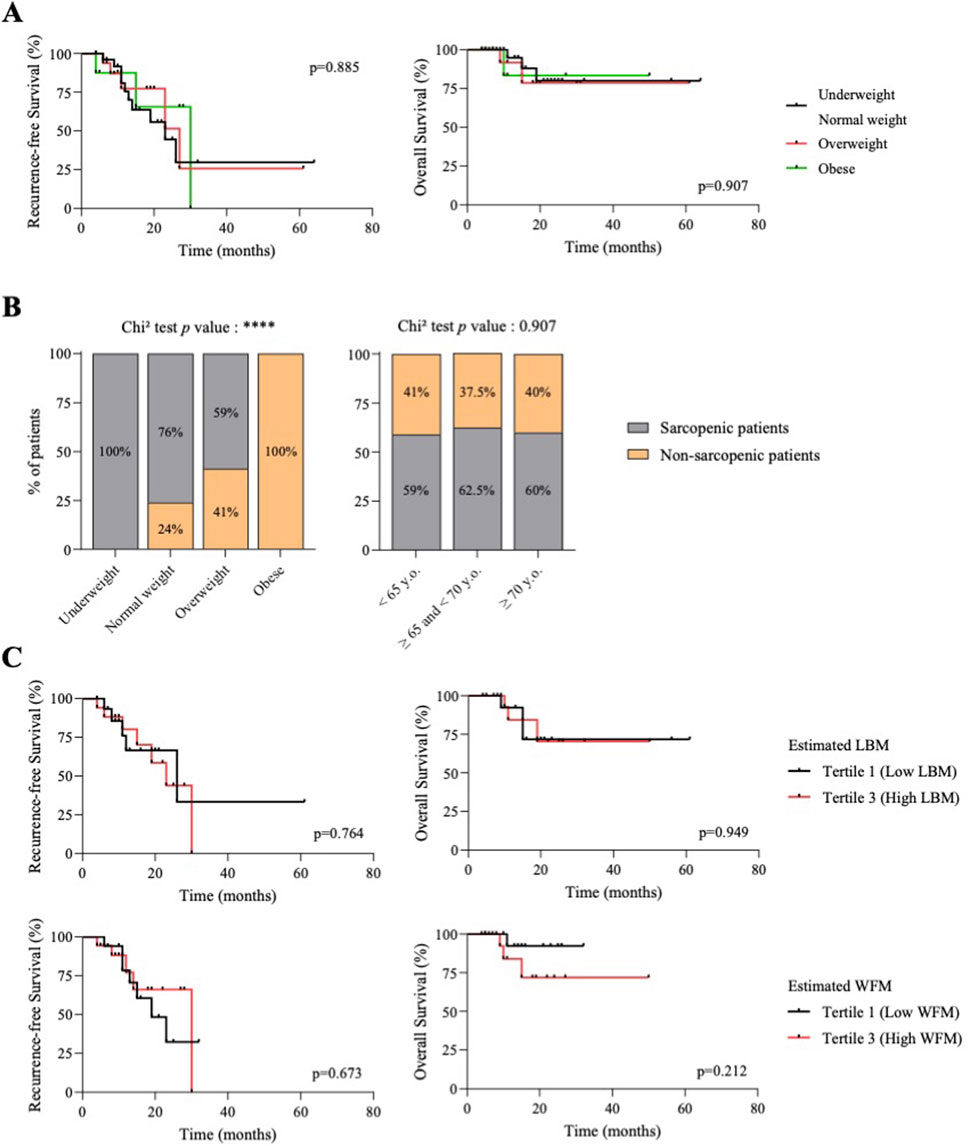
Figure 2. BMI and body composition parameters at baseline do not influence the survival of patients with ovarian cancer. (A) Kaplan-Meier curves of recurrence-free survival (left) and overall survival (right). Patients were divided into BMI categories. P value were calculated by Log-rank tests. (B) Proportion of sarcopenic and non-sarcopenic patients by body mass index category (BMI - left) or age tertiles (right). Chi2 tests were used to generate p values. (C) Kaplan-Meier curves of recurrence-free survival (left) and overall survival (right). Patients were divided according to baseline body composition parameters: lean body mass (LBM) or whole-body fat mass (WFM). Black lines represent patients with low LBM (<34.3 kg, tertile 1) or low WFM (<17.6 kg, tertile 1). Red lines represent patients with high LBM (>38.6 kg, tertile 3) or high WFM (>26.4 kg, tertile 3). P value were calculated by Log-rank tests.
Age and BMI had no significant influence on RFS and OS in our cohort (Table 2; Figure 2A). Regarding skeletal muscle parameters, median estimated LBM was 37.1 kg (IQR 33.3–40.5) and median SMI was 39.4 cm2/m2 (IQR 35.4–44.2). Thirty-two patients (60%) were classified as sarcopenic at diagnosis (C0), with median SMI being 36.6 cm2/m2 (IQR 34.1–38.8) (Table 2). The proportion of sarcopenic patients differed significantly according to BMI category (p < 0.0001) (Figure 2B): 100% of underweight patients, 76% of normal-weight patients and 59% of overweight patients were sarcopenic. The eight obese patients were not sarcopenic. The proportion of sarcopenic patients remained unchanged across all age categories (p = 0.90) (Figure 2B). There was no association between estimated LBM or sarcopenic status at baseline and patients survival (RFS and OS) (Table 2; Figure 2C). When looking at adipose tissue parameters at baseline, whether subcutaneous adipose tissue index (SATI), visceral adipose tissue index (VATI) or estimated whole body fat mass (WFM), none were associated with RFS or OS (Table 2; Figure 2C).
Altogether, this first set of results shows that patients’ body composition at baseline (whether muscle or adipose tissue parameters) was not associated with survival (RFS/OS) in our cohort of advanced EOC patients treated with NAC.
Twenty-six women (49%) underwent interval surgery after three cycles of NAC. This suggested a good tumor response. Indeed, patients eligible for interval surgery showed a prolonged time to cancer relapse (median RFS 27 months vs. 15 months for eligible and non-eligible patients respectively - p = 0.013), but a survival time close to that of patients who were not eligible (OS - p = 0.336) (Table 3; Figure 3A).

Table 3. Changes in clinical parameters and body composition between C0 and C3 and their association with survival in ovarian cancer patients treated with NAC.
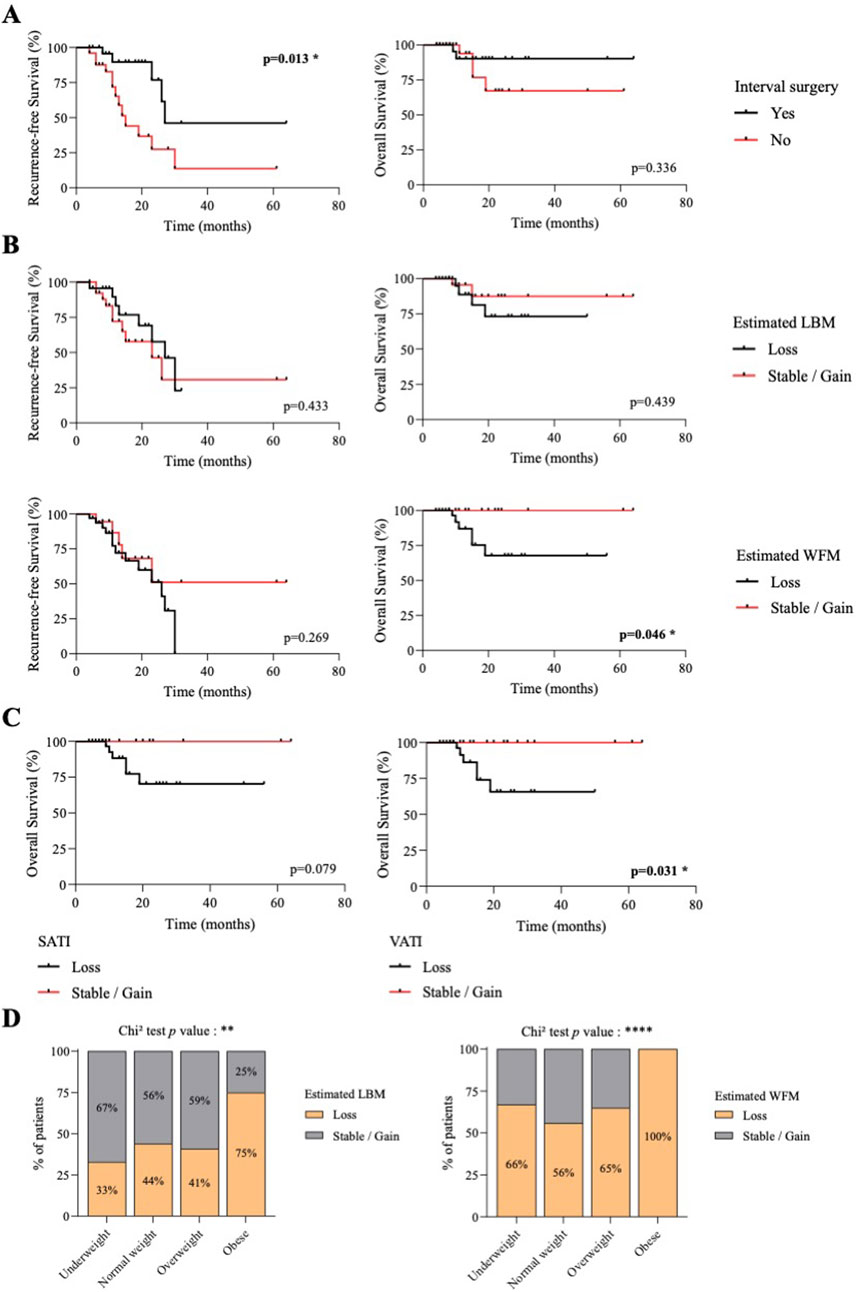
Figure 3. Loss of body fat, but not lean body mass, during neoadjuvant chemotherapy is associated with shorter survival for ovarian cancer patients. (A) Kaplan-Meier curves of recurrence-free survival (left) and overall survival (right) according to interval surgery eligibility. Black lines, patients with interval surgery. Red lines, patients without interval surgery. P value were calculated by Log-rank tests. (B) Kaplan-Meier curves of recurrence-free survival (left) and overall survival (right) according to changes in LBM or WFM during NAC. Black lines, patients who lost LBM or WFM. Red lines, patients who gained or had stable LBM or WFM. p value were calculated by Log-rank tests. (C) Kaplan-Meier curves of overall survival according to changes in subcutaneous (left) or visceral (right) adipose tissue index (SATI/VATI) during NAC. Black lines, patients who lost SATI or VATI. Red lines, patients who gained or had stable SATI or VATI. p value were calculated by Log-rank tests. (D) Proportion of patients with loss or gained/stable lean body mass (LBM - left) or whole-body fat mass (WFM - right) during NAC according to BMI category. Chi2 tests were used to generate p values.
The 53 patients included in this cohort had a second CT-Scan at C3 with a median duration interval of 103 days (Min 55; Max 220). Data for change over time were normalized to 100 days. For muscle and fat parameters, patients who experienced tissue loss greater than the 2% measurement error (MacDonald et al., 2011), were categorized as tissue losers. Other patients were categorized as stable/gaining tissue over time. Tissue changes are detailed in Table 3.
Skeletal muscle loss resulted in two women becoming sarcopenic. In line with these results, SMI remained relatively stable between diagnosis (C0) and C3 chemotherapy cycles, with a median variation of −2.2% (IQR -8.4% to +6.5%) (Table 3), suggesting that these first chemotherapy cycles did not drastically worsen sarcopenia.
We compared patients who lost SMI (−7.8%; IQR -12.8% to −4.3%) or LBM (−6.9%; IQR -12.3% to −3.9%), and those who gained or has stable SMI (+6.5%; IQR +3.0% to +9.0%) or LBM (+4.5%; IQR +2.2% to +7.6%). We found no association with RFS and OS (Table 3; Figure 3B).
Adiposity parameters changed more markedly between C0 and C3, with median losses of −10.5% (IQR -32.5% to +6.6%) for VATI, −12.1% (IQR -27.3% to +1.4%) for SATI and −7.6% (IQR -20.8% to +2.0%) for WFM estimation (Table 3). We observed no significant association between changes in body fat and recurrence-free survival (Table 3; Figure 3B). Only loss of SATI tended to be associated with shorter RFS (p = 0.075) (Table 3). On the other hand, loss of body fat seems to be a prognostic factor for OS. We observed that patients had shorter overall survival if they had lost VATI (p = 0.031) or WFM (p = 0.046). The same tends to apply to SATI (p = 0.079) (Table 3; Figures 3B,C). Patients with rapid and severe loss of VATI (−27.7%, IQR -39.6% to −10.8%), SATI (−19.0%, IQR -32.5% to −10.6%) and estimated WFM (−17.0%, IQR -24.7% to −7.6%) within 100 days had shortened overall survival.
During their first three cycles of neoadjuvant chemotherapy, obese patients were particularly affected by tissue loss, whether lean or fat mass (Figure 3D), with 75% and 100% of obese patients losing more than 2% of their estimated lean and fat mass respectively.
Overall, these results show that after three cycles of neoadjuvant chemotherapy, obese patients are more likely to lose muscle mass and fat mass. However, it was patients with rapid and marked fat loss who had a significantly shorter overall survival time.
Multivariate Cox regression analysis demonstrated that visceral fat loss remained an independent prognostic factor for overall survival (HR = 2.45, 95% CI: 1.32–4.56, p = 0.004), after adjusting for age, BMI, and surgical status.
Eligibility for interval surgery suggests a better tumor response to NAC and is known to influence a better prognosis, in particular by increasing time to relapse. We retrospectively examined whether patients eligible for interval surgery had specific clinical and body composition characteristics. We compared clinical and body composition parameters at baseline, as well as changes in body composition parameters during NAC, and found no significant differences between patients eligible and ineligible for interval surgery (Supplementary Table 1). Patients with the best tumor response to NAC had no specific clinical or body composition characteristics.
The aim of our study was to assess body composition parameters in women with advanced epithelial ovarian cancer eligible for NAC, and to determine whether these parameters had an impact on prognosis. Low BMI, but not age, was a primary clinical indicator associated with sarcopenic patients, since 100% of underweight women and 76% of normal-weight women, but none of the obese women, were sarcopenic at baseline. No clinical (age, BMI) or body composition parameters at baseline were associated with recurrence-free survival or overall survival. After three cycles of NAC, 26 patients underwent interval surgery. This indicator of good tumor response was associated with a significantly longer time to relapse, but not with a specific change in body composition. During the first three cycles of NAC, the loss of body fat (around −10%) was more marked than the loss of muscle mass (−2%). Obese patients were the most affected by these losses, with 100% showing a reduction in fat mass and 75% a reduction in muscle mass. Nevertheless, it was the patients who had a severe and rapid loss of VATI (−28% per 100 days) and fat mass (−17% per 100 days) who had a significantly shorter overall survival.
In this study, the most commonly used threshold, SMI<41 cm2/m2, was chosen as the reference to identify 32 sarcopenic patients (Martin et al., 2013b) (60% of patients). Using the reference supported by the Haute Autorité de Santé (HAS), SMI<38.5 cm2/m2 (Prado et al., 2008c), only 21 women (40%) should be considered sarcopenic prior to the implementation of NAC. The relevance of the chosen threshold is debatable, as thresholds defined for American populations may not be directly applicable to European or Asian populations. A sensitivity analysis using an alternative threshold (SMI <38.5 cm2/m2) yielded similar results, confirming the robustness of our findings.
However, analyses using this other threshold or a tertile analysis also failed to establish a link between sarcopenia, low SMI or loss of SMI and survival in our study. Several hypotheses can be put forward: i/the patients we included were first-line patients, whereas several studies have reported a loss of muscle mass during palliative chemotherapy; ii/the loss of muscle mass, with a median variation of −2%, remained low. Sarcopenia is characterized by progressive muscle loss. The time between the two scans (median 103 days) may not be sufficient to show a significant reduction in muscle mass and impact on survival; iii/this pilot study included 53 patients, which may be too small a number to demonstrate the effect of low muscle mass or loss of muscle mass on survival. However, the literature is not yet in complete agreement on the association between sarcopenia and survival in EOC (McSharry et al., 2020; Jin et al., 2023; Huang et al., 2020). As shown by Jin et al. (Jin et al., 2023), body composition, and in particular muscle mass, can change with disease stage: a low muscle mass index is more frequently associated with advanced stages (stage III/IV). The fact that only patients eligible for NAC were included in this study led to a selection of patients in advanced stages, and therefore perhaps also to a selection of patients who already had a high rate of sarcopenia (60%). The low heterogeneity of patients with regard to stage may lead to a narrower range of values for SMI, making it impossible to demonstrate its involvement in survival.
To our knowledge, we have identified only one article reporting body composition before and after three cycles of NAC in patients with EOC (Rutten et al., 2016). Compared with our study, we might note a difference in patient selection, since we only included patients eligible for interval surgery. The authors identified muscle loss and visceral fat loss as factors negatively related to overall survival. In line with this study, our results report a link between fat loss, particularly visceral fat loss, and overall survival. It is difficult to determine whether fat loss is associated with tumor progression, the effect of chemotherapy or some other mechanism. However, in our study, the favorable evolution of the tumor under chemotherapy, which makes it possible to space out surgical interventions, is not linked to these changes in body fat (Supplementary Table 1). Without ruling out the possibility of chemotherapy-related toxicity, we may wonder why the loss of body fat occurs mainly at the visceral level. In the event of a reduction in food intake, it has been shown that, physiologically, caloric restriction preferentially reduces visceral over subcutaneous fat (Janssen and Ross, 1999). Nevertheless, it cannot be ruled out that the particular localization of ovarian cancer in the abdominal cavity may favour privileged interactions between these cancer cells and abdominal adipose tissue. It constitutes a source of energy (by delipidation of adipocytes) and a metabolic/cytokinic support for their proliferation and local and distant implantation (Motohara et al., 2019). Moreover, the proximity of ovarian tumour cells to adipocytes may induce a metabolic shift towards fatty acid consumption and beta-oxidation, which may be associated with tumour progression (Chen et al., 2019; Wang et al., 2017).
The prognostic significance of adiposity is still debated. Our results indicate that obese patients are particularly affected by fat and lean mass loss. Nevertheless, there is no link between BMI and survival (RFS and OS). This ambiguity has already been noted in the literature. In 2023, Cuello’s publication showed that high visceral fat mass and metabolic dysfunction, not BMI, are associated with poorer survival in patients with EOC (Cuello et al., 2023). Furthermore, our results showed that patients with poorer survival had a rapid and severe decrease in body fat (over 100 days, −28% for VATI and −18% for WFM), suggesting specific metabolic changes and a strong energy imbalance. Some hypotheses can be put forward: i/an increase in inflammatory processes that could lead to a greater reduction in food intake, placing these patients in an energy deficit (Martin et al., 2021). Measures of inflammation and caloric intake should therefore be evaluated in future studies; ii/a decrease in food intake could be coupled with hypermetabolism leading to rapid loss of adipose tissue. Although never demonstrated in ovarian cancer, hypermetabolism has already been measured in cancer patients, affecting over a third of patients and having a major impact on patient survival (Vazeille et al., 2017). To manage these patients, who are rapidly losing body fat and whose risk of death is particularly high, the literature suggests two options: either nutritional supplementation to compensate for the energy deficit (Cotogni et al., 2022; Jouinot et al., 2020) or nutritional or drug management to rebalance lipid metabolism (Cuello et al., 2023). Only the identification of the mechanism(s) responsible for fat loss, using simple, validated markers or biomarkers, can guide the clinician in the choice of nutritional or medicinal support.
One of the strengths of our work is the homogeneity and representativeness of our cohort, since all patients had advanced stage III-IV FIGO EOC, and were treated with the same drugs and protocol at the same center. However, our study also has certain limitations, including its retrospective nature and the fact that our sample size (patients with NAC) decreased considerably, which limited the power of statistical analyses. We acknowledge that the small sample size, particularly the limited number of obese patients (N = 8), may have reduced the reliability of subgroup analyses. While our findings suggest that obese patients are particularly susceptible to fat and muscle loss during NAC, these results should be interpreted with caution. Future multicenter studies with larger cohorts are needed to validate these observations and to further explore the impact of NAC on body composition parameters and prognostic implications. Nutritional supplementation and pharmacological management of lipid metabolism represent promising strategies to mitigate fat loss and improve survival outcomes. However, the efficacy of these interventions must be validated in prospective clinical trials.
In conclusion, our study highlights the high prevalence of sarcopenia in women with advanced ovarian cancer and identifies rapid and severe loss of visceral fat as a prognostic factor for poorer OS. These findings suggest the potential of early nutritional and/or pharmacological interventions to promote muscle and adipose tissue maintenance and improve outcomes for women with advanced ovarian cancer. Future research should focus on identifying the mechanisms underlying fat loss and evaluating the efficacy of targeted interventions in this high-risk population.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by review board of Centre hospitalier de tours. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
WB: Data curation, Formal Analysis, Investigation, Writing–original draft. AD: Data curation, Investigation, Writing–review and editing. AB: Investigation, Methodology, Resources, Software, Writing–review and editing. SS: Resources, Visualization, Writing–review and editing. J-FD: Resources, Supervision, Writing–review and editing. CV: Funding acquisition, Resources, Supervision, Visualization, Writing–review and editing. CG: Investigation, Resources, Supervision, Validation, Writing–review and editing. LO: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. AD received financial support from the French Ministry of Higher Education, Research and Innovation and the French Society of Clinical Nutrition and Metabolism (SFNCM, Exceptional Research Prize).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2025.1537484/full#supplementary-material
Armstrong D. K., Alvarez R. D., Bakkum-Gamez J. N., Barroilhet L., Behbakht K., Berchuck A., et al. (2021). Ovarian cancer, version 2.2020, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Canc Netw. 19 (2), 191–226. doi:10.6004/jnccn.2021.0007
Byerley L. O., Lee S. H., Redmann S., Culberson C., Clemens M., Lively M. O. (2010). Evidence for a novel serum factor distinct from zinc alpha-2 glycoprotein that promotes body fat loss early in the development of cachexia. Nutr. Cancer 62 (4), 484–494. doi:10.1080/01635580903441220
Cai Y., Wang J., Zhang L., Wu D., Yu D., Tian X., et al. (2015). Expressions of fatty acid synthase and HER2 are correlated with poor prognosis of ovarian cancer. Med. Oncol. 32 (1), 391. doi:10.1007/s12032-014-0391-z
Chen R. R., Yung M. M. H., Xuan Y., Zhan S., Leung L. L., Liang R. R., et al. (2019). Targeting of lipid metabolism with a metabolic inhibitor cocktail eradicates peritoneal metastases in ovarian cancer cells. Commun. Biol. 2 (1), 281. doi:10.1038/s42003-019-0508-1
Cotogni P., Bozzetti F., Goldwasser F., Jimenez-Fonseca P., Roelsgaard Obling S., Valle J. W. (2022). Supplemental parenteral nutrition in cancer care: why, who, when. Ther. Adv. Med. Oncol. 14, 17588359221113691. doi:10.1177/17588359221113691
Cuello M. A., Gómez F., Wichmann I., Suárez F., Kato S., Orlandini E., et al. (2023). Body composition and metabolic dysfunction really matter for the achievement of better outcomes in high-grade serous ovarian cancer. Cancers 15 (4), 1156. doi:10.3390/cancers15041156
Daly L. E., Ní Bhuachalla É. B., Power D. G., Cushen S. J., James K., Ryan A. M. (2018). Loss of skeletal muscle during systemic chemotherapy is prognostic of poor survival in patients with foregut cancer: muscle loss during chemotherapy is prognostic of poor survival. J. Cachexia Sarcopenia Muscle 9 (2), 315–325. doi:10.1002/jcsm.12267
Fouladiun M., Körner U., Bosaeus I., Daneryd P., Hyltander A., Lundholm K. G. (2005). Body composition and time course changes in regional distribution of fat and lean tissue in unselected cancer patients on palliative care—correlations with food intake, metabolism, exercise capacity, and hormones. Cancer 103 (10), 2189–2198. doi:10.1002/cncr.21013
Hennessy B. T., Coleman R. L., Markman M. (2009). Ovarian cancer. Lancet 374 (9698), 1371–1382. doi:10.1016/S0140-6736(09)61338-6
Hopkins J. J., Reif R. L., Bigam D. L., Baracos V. E., Eurich D. T., Sawyer M. B. (2019). The impact of muscle and adipose tissue on long-term survival in patients with stage I to III colorectal cancer. Dis. Colon Rectum 62 (5), 549–560. doi:10.1097/DCR.0000000000001352
Huang C., Yang Y., Chen T., Chen J., Chen Y., Wu M., et al. (2020). Muscle loss during primary debulking surgery and chemotherapy predicts poor survival in advanced-stage ovarian cancer. J. Cachexia Sarcopenia Muscle 11 (2), 534–546. doi:10.1002/jcsm.12524
Janssen I., Ross R. (1999). Effects of sex on the change in visceral, subcutaneous adipose tissue and skeletal muscle in response to weight loss. Int. J. Obes. 23 (10), 1035–1046. doi:10.1038/sj.ijo.0801038
Jin Y., Ma X., Yang Z., Zhang N. (2023). Low L3 skeletal muscle index associated with the clinicopathological characteristics and prognosis of ovarian cancer: a meta-analysis. J. Cachexia Sarcopenia Muscle 14 (2), 697–705. doi:10.1002/jcsm.13175
Jouinot A., Ulmann G., Vazeille C., Durand J. P., Boudou-Rouquette P., Arrondeau J., et al. (2020). Hypermetabolism is an independent prognostic factor of survival in metastatic non-small cell lung cancer patients. Clin. Nutr. 39 (6), 1893–1899. doi:10.1016/j.clnu.2019.08.003
Klassen P. N., Baracos V., Ghosh S., Martin L., Sawyer M. B., Mazurak V. C. (2023). Muscle and adipose wasting despite disease control: unaddressed side effects of palliative chemotherapy for pancreatic cancer. Cancers 15 (17), 4368. doi:10.3390/cancers15174368
Ladanyi A., Mukherjee A., Kenny H. A., Johnson A., Mitra A. K., Sundaresan S., et al. (2018). Adipocyte-induced CD36 expression drives ovarian cancer progression and metastasis. Oncogene 37 (17), 2285–2301. doi:10.1038/s41388-017-0093-z
MacDonald A. J., Greig C. A., Baracos V. (2011). The advantages and limitations of cross-sectional body composition analysis. Curr. Opin. Support Palliat. Care 5 (4), 342–349. doi:10.1097/SPC.0b013e32834c49eb
Martin L., Birdsell L., MacDonald N., Reiman T., Clandinin M. T., McCargar L. J., et al. (2013a). Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 31 (12), 1539–1547. doi:10.1200/JCO.2012.45.2722
Martin L., Birdsell L., MacDonald N., Reiman T., Clandinin M. T., McCargar L. J., et al. (2013b). Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 31 (12), 1539–1547. doi:10.1200/JCO.2012.45.2722
Martin L., Muscaritoli M., Bourdel-Marchasson I., Kubrak C., Laird B., Gagnon B., et al. (2021). Diagnostic criteria for cancer cachexia: reduced food intake and inflammation predict weight loss and survival in an international, multi-cohort analysis. J. Cachexia Sarcopenia Muscle 12 (5), 1189–1202. doi:10.1002/jcsm.12756
McSharry V., Mullee A., McCann L., Rogers A. C., McKiernan M., Brennan D. J. (2020). The impact of sarcopenia and low muscle attenuation on overall survival in epithelial ovarian cancer: a systematic review and meta-analysis. Ann. Surg. Oncol. 27 (9), 3553–3564. doi:10.1245/s10434-020-08382-0
Melamed A., Rauh-Hain J. A., Gockley A. A., Nitecki R., Ramirez P. T., Hershman D. L., et al. (2021). Association between overall survival and the tendency for cancer programs to administer neoadjuvant chemotherapy for patients with advanced ovarian cancer. JAMA Oncol. 7 (12), 1782–1790. doi:10.1001/jamaoncol.2021.4252
Mitsiopoulos N., Baumgartner R. N., Heymsfield S. B., Lyons W., Gallagher D., Ross R. (1985). Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J. Appl. Physiol. Bethesda Md 85 (1), 115–122. doi:10.1152/jappl.1998.85.1.115
Motohara T., Masuda K., Morotti M., Zheng Y., El-Sahhar S., Chong K. Y., et al. (2019). An evolving story of the metastatic voyage of ovarian cancer cells: cellular and molecular orchestration of the adipose-rich metastatic microenvironment. Oncogene 38 (16), 2885–2898. doi:10.1038/s41388-018-0637-x
Mourtzakis M., Prado C. M. M., Lieffers J. R., Reiman T., McCargar L. J., Baracos V. E. (2008a). A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 33 (5), 997–1006. doi:10.1139/H08-075
Mourtzakis M., Prado C. M. M., Lieffers J. R., Reiman T., McCargar L. J., Baracos V. E. (2008b). A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 33 (5), 997–1006. doi:10.1139/H08-075
Mukherjee A., Chiang C. Y., Daifotis H. A., Nieman K. M., Fahrmann J. F., Lastra R. R., et al. (2020). Adipocyte-Induced FABP4 expression in ovarian cancer cells promotes metastasis and mediates carboplatin resistance. Cancer Res. 80 (8), 1748–1761. doi:10.1158/0008-5472.CAN-19-1999
Murphy R. A., Wilke M. S., Perrine M., Pawlowicz M., Mourtzakis M., Lieffers J. R., et al. (2010). Loss of adipose tissue and plasma phospholipids: relationship to survival in advanced cancer patients. Clin. Nutr. 29 (4), 482–487. doi:10.1016/j.clnu.2009.11.006
Nakayama N., Nakayama K., Ishibashi T., Katayama S., Kyo S. (2022). Effect of muscle loss but not fat loss during primary debulking surgery and chemotherapy on prognosis of patients with ovarian cancer. J. Clin. Med. 11 (11), 3184. doi:10.3390/jcm11113184
Nikolaidi A., Fountzilas E., Fostira F., Psyrri A., Gogas H., Papadimitriou C. (2022). Neoadjuvant treatment in ovarian cancer: new perspectives, new challenges. Front. Oncol. 12, 820128. doi:10.3389/fonc.2022.820128
Pecorelli S. (2009). Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 105 (2), 103–104. doi:10.1016/j.ijgo.2009.02.012
Prado C. M., Lieffers J. R., McCargar L. J., Reiman T., Sawyer M. B., Martin L., et al. (2008a). Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 9 (7), 629–635. doi:10.1016/S1470-2045(08)70153-0
Prado C. M., Lieffers J. R., McCargar L. J., Reiman T., Sawyer M. B., Martin L., et al. (2008b). Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 9 (7), 629–635. doi:10.1016/S1470-2045(08)70153-0
Prado C. M., Lieffers J. R., McCargar L. J., Reiman T., Sawyer M. B., Martin L., et al. (2008c). Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 9 (7), 629–635. doi:10.1016/S1470-2045(08)70153-0
Rutten I. J. G., Van Dijk D. P. J., Kruitwagen RFPM, Beets-Tan R. G. H., Olde Damink S. W. M., Van Gorp T. (2016). Loss of skeletal muscle during neoadjuvant chemotherapy is related to decreased survival in ovarian cancer patients. J. Cachexia Sarcopenia Muscle 7 (4), 458–466. doi:10.1002/jcsm.12107
Salaun H., Poisson M., Dolly A., Arbion F., Servais S., Dumas J. F., et al. (2023). Total polyunsaturated fatty acid level in abdominal adipose tissue as an independent predictor of recurrence-free survival in women with ovarian cancer. Int. J. Mol. Sci. 24 (2), 1768. doi:10.3390/ijms24021768
Shen W., Punyanitya M., Wang Z., Gallagher D., St-Onge M. P., Albu J., et al. (1985). Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J. Appl. Physiol. Bethesda Md 97 (6), 2333–2338. doi:10.1152/japplphysiol.00744.2004
Shen W., Punyanitya M., Wang Z., Gallagher D., St.-Onge M. P., Albu J., et al. (2004). Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J. Appl. Physiol. 97 (6), 2333–2338. doi:10.1152/japplphysiol.00744.2004
Siegel R. L., Miller K. D., Jemal A. (2018). Cancer statistics, 2018. CA Cancer J. Clin. 68 (1), 7–30. doi:10.3322/caac.21442
Torres M. L., Hartmann L. C., Cliby W. A., Kalli K. R., Young P. M., Weaver A. L., et al. (2013). Nutritional status, CT body composition measures and survival in ovarian cancer. Gynecol. Oncol. 129 (3), 548–553. doi:10.1016/j.ygyno.2013.03.003
Ubachs J., Ziemons J., Minis-Rutten I. J. G., Kruitwagen R. F. P. M., Kleijnen J., Lambrechts S., et al. (2019). Sarcopenia and ovarian cancer survival: a systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 10 (6), 1165–1174. doi:10.1002/jcsm.12468
Vazeille C., Jouinot A., Durand J. P., Neveux N., Boudou-Rouquette P., Huillard O., et al. (2017). Relation between hypermetabolism, cachexia, and survival in cancer patients: a prospective study in 390 cancer patients before initiation of anticancer therapy. Am. J. Clin. Nutr. 105 (5), 1139–1147. doi:10.3945/ajcn.116.140434
Wang Y. Y., Attané C., Milhas D., Dirat B., Dauvillier S., Guerard A., et al. (2017). Mammary adipocytes stimulate breast cancer invasion through metabolic remodeling of tumor cells. JCI Insight 2 (4), e87489. Available online at: https://insight.jci.org/articles/view/87489doi:10.1172/jci.insight.87489 Accessed 2024 Nov 27).
Keywords: epithelial ovarian cancer, body composition, neoadjuvant chemotherapy, ovarian cancer, sarcopenia, visceral adipose tissue
Citation: Benouali W, Dolly A, Bleuzen A, Servais S, Dumas J-F, Vandier C, Goupille C and Ouldamer L (2025) Adipose tissue loss during neoadjuvant chemotherapy: a key prognostic factor in advanced epithelial ovarian cancer. Front. Physiol. 16:1537484. doi: 10.3389/fphys.2025.1537484
Received: 30 November 2024; Accepted: 07 March 2025;
Published: 25 March 2025.
Edited by:
Lindsay McDermott, University of Bedfordshire, United KingdomReviewed by:
Nurul Ratna Mutu Manikam, University of Indonesia, IndonesiaCopyright © 2025 Benouali, Dolly, Bleuzen, Servais, Dumas, Vandier, Goupille and Ouldamer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lobna Ouldamer, bC5vdWxkYW1lckBjaHUtdG91cnMuZnI=
†These authors have contributed equally to this work
‡ORCID: Jean-François Dumas, orcid.org/0000-0002-2293-6606
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.