 Tania Sapre1
Tania Sapre1 Haylie L. Miller1Anna Schwartz1
Haylie L. Miller1Anna Schwartz1 Leah R. Ketcheson2Alanna Price3Kerry Winkelseth1Jeanne M. Barcelona2
Leah R. Ketcheson2Alanna Price3Kerry Winkelseth1Jeanne M. Barcelona2 Ronald F. Zernicke1,4
Ronald F. Zernicke1,4 Rebecca E. Hasson1*
Rebecca E. Hasson1*- 1School of Kinesiology, University of Michigan, Ann Arbor, MI, United States
- 2College of Education, Wayne State University, Detroit, MI, United States
- 3Detroit Public School Community District, Detroit, MI, United States
- 4Department of Orthopaedic Surgery, School of Medicine, University of Michigan, Ann Arbor, MI, United States
Purpose: While it is common practice for schools across the United States to include neurodivergent children in physical education classes, many programs outside of school—such as those at home or in the community—are not effectively tailored to meet their support needs. This gap contributes to lower levels of physical activity among neurodivergent children. Our objective was to address this issue by systematically adapting the InPACT (Interrupting Prolonged sitting with ACTivity) at Home program to enable neurodivergent children to safely engage in physical activity at home.
Methods: The rapid-cycle research adaptation process involved several key steps: (1) sorting and grouping video content based on different types of skills and exercises (problem exploration); (2) assembling an expert team to guide the development of the instructions (knowledge exploration); and (3) using generative artificial intelligence (AI) to create concise instructions and cue words for each skill/exercise (solution development). These outputs were then fine-tuned by the expert team. The refinements were guided by the Universal Design for Learning (UDL) principle of “Representation,” which acknowledges that learners perceive and understand information in diverse ways.
Results: From the 132 InPACT at Home videos, over 500 activities were identified and categorized into main skill groups: jumping, core, lateral, sport, upper body, lower body, and compound movements. Expert meetings emphasized the importance of the “Three C’s”—consistency, conciseness, and clarity—in crafting instructions, along with the use of simple, elementary sight words. AI was employed to generate and refine prompts like “Provide simplified step-by-step instructions for a jumping jack, suitable for a neurodivergent child” and “Condense the step-by-step instructions for a jumping jack, suitable for a neurodivergent child”.
Discussion: The adaptation of the existing InPACT at Home program was guided by dissemination and implementation science frameworks, aiming to increase equitable access to structured youth physical activity opportunities for neurodivergent children. By incorporating AI and UDL principles, we aim to further enhance the program’s accessibility. Our next steps include evaluating the effectiveness of our program adaptations in encouraging participation in the InPACT at Home program and subsequently increasing physical activity levels among neurodivergent children.
Introduction
The role of physical activity in child development
Physical activity plays a critical role in shaping children’s physical health, social development, and cognitive abilities. For neurotypical children, participation in physical activity is associated with improved physical health, higher self-esteem, and the development of a strong social identity through sports (Logan et al., 2019; Piercy and Troiano, 2018). Similarly, children with intellectual and developmental disabilities experience comparable benefits. For instance, neurodivergent children (e.g., those diagnosed with autism, developmental delay, intellectual disability, or similar) who participate in programs like Special Olympics show greater fitness, strength, aerobic capacity, self-esteem, confidence, social competence, and friendships compared to their peers who are not involved in such activities (Logan et al., 2019). Autistic children can also benefit from physical activity and exercise (Ceccarelli et al., 2020; Monteiro et al., 2022; Ruggeri et al., 2020), specifically experiencing positive changes in communication, social interaction, social cognition, social motivation, regulation of repetitive behaviors and awareness (Huang et al., 2020; Koh, 2024; Liang et al., 2022; Rafie et al., 2017). Physical activities like sports can also expose children to varied external stimuli, engaging multiple senses—sight, hearing, touch, and smell—and promoting sensory integration through nervous system activation and neural development (Rafie et al., 2017). Exercise further supports motor skill development, executive function, and overall quality of life for neurodivergent children (Bremer et al., 2016; St John et al., 2020; Sun et al., 2022). Collectively, this evidence underscores the profound impact of physical activity in fostering the development and wellbeing of all children, with especially significant benefits for neurodivergent children.
Current challenges in youth physical activity participation
Despite these benefits, few children and youth are regularly physically active (Piercy and Troiano, 2018). According to the 2024 United States Report Card on Physical Activity for Children and Youth, only 20%–28% of children aged 6 to 17 meet the recommended 60 min of daily physical activity (Alliance, 2024). These data, drawn from the National Survey of Children’s Health and National Health and Nutrition Examination Survey, show even lower levels of activity among neurodivergent children, with just 19% meeting the recommended amount (Alliance, 2024; Case et al., 2020). These findings are consistent with previous research using large datasets (McCoy et al., 2016) or objective measurements (Liang et al., 2020) and highlight the urgent need for targeted interventions to increase physical activity levels, particularly among neurodivergent children.
Low motor competence plays a significant role in these low physical activity levels. Research shows that neurotypical children with motor competence below an “average” threshold are unlikely to meet recommended physical activity guidelines (De Meester et al., 2018). Additionally, many neurodivergent children exhibit fundamental motor skill differences, such as delays or challenges in balance, aiming, catching, and strength (Staples and Reid, 2010). However, findings in the neurodivergent population are mixed (Taylor et al., 2024). Some studies show only a weak association between low motor competence and physical activity levels, with motor competence varying across specific domains (e.g., upper limb coordination versus running speed). These domain-specific difficulties may influence participation in certain types of activities.
Perceived motor competence is particularly important for motivating autistic youth to engage in physical activity (Wong et al., 2024) but appears less influential for children with intellectual disabilities or ADHD. This highlights the need for programs that address not only motor skills but also the diverse psychological needs of neurodivergent children to support their engagement in physical activity.
Although person-centered factors like motor competence affect participation, features of the social and physical environment also exacerbate disparities in physical activity participation among neurodivergent children (Wong et al., 2024; King et al., 2003). One major issue is the limited understanding among instructors and coaches about neurodivergent children’s abilities. Caregivers, instructors, and physical educators may not be comfortable modifying exercise instructions for a person with high communication or cognitive support needs (McDermott et al., 2022; Parsons et al., 2024). Playground design poses another barrier, since most fail to accommodate the needs of neurodivergent children (Johnson et al., 2021). Key features such as wayfinding systems, stable surfacing, flush transitions, and sensory elements are often missing, making spontaneous physical activity less safe, engaging, and accessible. Finally, there is a notable shortage of evidence-based, free resources, including specialized curricula and community programs, to support parents in addressing their children’s physical activity needs (Rimmer and Rowland, 2008). These gaps further exacerbate the barriers to physical activity faced by neurodivergent children.
Strategies for inclusive physical activity
Addressing these challenges requires developing targeted strategies to promote inclusive physical activity for neurodivergent children (Lakowski and Long, 2011; Murphy and Carbone, 2008). However, creating new interventions from scratch can be time-consuming and resource-intensive, making it more efficient to adapt existing evidence-based interventions (Wang et al., 2018). Adapting interventions involves modifying evidence-based interventions while maintaining their core components to ensure effectiveness (Baumann et al., 2018). This process has previously involved consideration of factors such as race, ethnicity, service setting, location, and organizational characteristics (Wiltsey Stirman et al., 2015). Yet, few researchers have applied adaptation frameworks to enhance equity and inclusion in physical activity interventions (Hasson et al., 2022; Scott-Andrews et al., 2021).
The current project: InPACT for Everyone
The main objective of the current project was to systematically adapt the Interrupting Prolonged sitting with ACTivity (InPACT) at Home program to enable neurodivergent children to engage in physical activity at home safely. This adaptation effort, named InPACT for Everyone, was guided by two key principles: rapid-cycle research and the Universal Design for Learning (UDL) principle of Representation (Johnson et al., 2015; Meyer et al., 2014). Rapid-cycle research is a systematic process where research teams identify barriers and address them using practice-based evidence, facilitating a swift transition from concept development to implementation in practice (Johnson et al., 2015). We previously used this approach to adapt a classroom-based physical activity intervention for delivery in the home (Hasson et al., 2022). The UDL principle of Representation emphasizes the need to represent information in multiple ways (e.g., through differing modalities such as text, images, and audio) to maximize accessibility of instructional content for learners with diverse backgrounds and support needs (Lieberman et al., 2021; Lieberman and Houston-Wilson, 2018). Multiple means of representation should also be provided in the assessment process, so that learners have a variety of opportunities to demonstrate skills.
The current paper describes key steps in the systematic adaptation of the InPACT at Home program, leveraging these frameworks to increase access to health-enhancing physical activity for neurodivergent children. By enhancing flexibility while maintaining fidelity, InPACT for Everyone seeks to address health equity and foster inclusive environments for physical activity.
Methods
The InPACT at Home program was chosen for adaptation due to its extensive reach across the state of Michigan. Specifically, when the program launched, website reach included all 83 counties and the daily viewership on public television ranged from 15,000–20,000 (Hasson et al., 2022). The InPACT at Home program was developed during the COVID-19 pandemic to provide equitable opportunities for physical activity in the home environment and address growing concerns of inactivity and obesity during the shelter-in-place restriction. Adapted from an existing classroom-based physical activity intervention, the InPACT at Home program retained key elements such as use of exercise videos, maintenance of intervention dose, and instructor-led physical activities (Hasson et al., 2021). The program features 132, 8-min exercise videos created by physical education teachers, pediatric exercise physiologists, athletes, and other fitness professionals. These videos focus on four main types of exercise: cardio, strength, sports skills, and mindfulness. The videos have been evaluated as high quality regarding their production (Beemer et al., 2023). Children have rated the program as enjoyable and can feasibly complete two videos at home (Beemer et al., 2022; Beemer et al., 2024).
Rapid adaptation of the InPACT at Home program
In June 2023, an expert in neurodivergent movement (H.L.M.) reached out to the program director of the InPACT at Home program (R.E.H.) to discuss increasing inclusive physical activity opportunities for youth. The principal investigator agreed and formed an interdisciplinary team of researchers and practitioners with expertise in motor development, pediatric exercise physiology, inclusive physical activity practices, and adapted physical education to address this issue (see Table 1). The InPACT program director contacted each team member via email to confirm their involvement in the adaptation team. Approximately 55% of the team members identified as women of color (including African American, Asian, Hispanic, and Middle East and North Africa [MENA]), and the entire team was composed of women. In addition, one of the team members identified as neurodivergent and had a neurodivergent immediate family member.
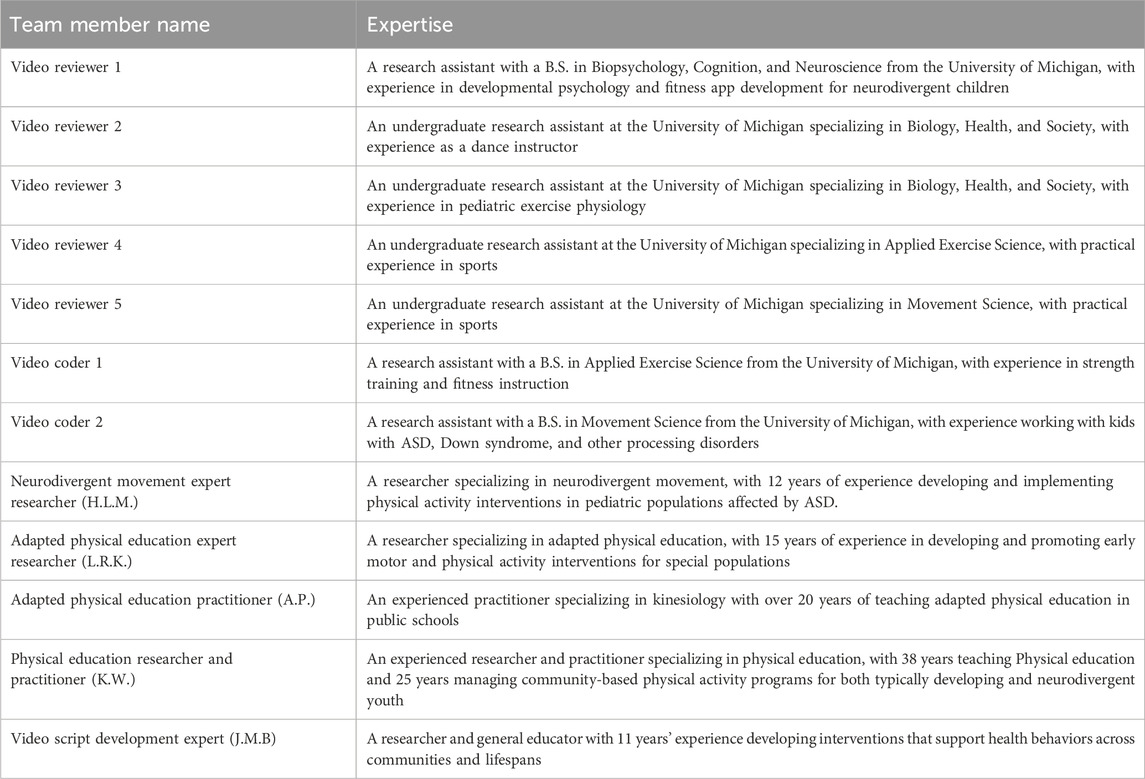
Table 1. Team member expertise. The specific expertise of each member of the video review team and expert team.
This diversity played a pivotal role in shaping the adaptation process by bringing together multiple cultural and experiential perspectives. The team’s varied social backgrounds and professional expertise ensured the adapted intervention would be inclusive and accessible to a wide range of neurodivergent children. With women of color from diverse cultural and neurodivergent backgrounds on the team, the adaptations were crafted with an enhanced sensitivity to how social, cultural, and cognitive factors affect engagement, comprehension, and comfort for children from different backgrounds. This inclusivity, paired with interdisciplinary expertise, enabled the team to create a nuanced, culturally sensitive adapted intervention to meet the unique needs of neurodivergent children.
Rapid adaptation of the InPACT at Home program
The six steps of rapid-cycle research provide a structured approach to developing, testing, and scaling solutions. These steps are based on the Framework for Rapid-Cycle Research developed by the Agency for Healthcare Research and Quality, which outlines the phases of the adaptation and research process from conceptualization to implementation (Johnson et al., 2015). The process begins with preparation, where partner organizations are identified, along with individuals within those organizations who will champion the program. This is followed by problem exploration, which involves understanding key problems that need to be solved. This stage emphasizes dialogue and sharing diverse perspectives to deepen the understanding of the issue. Next is knowledge exploration, which examines the problem from multiple angles. This includes characterizing the problem, identifying industries that face similar challenges, pinpointing organizations within those industries that have successfully addressed the problem, and analyzing the processes or activities that set these organizations apart.
Solution development then focuses on identifying the simplest, least invasive, and most scalable solutions that can be applied. Once potential solutions are developed, the solution testing phase evaluates their effectiveness. Project team members assess the importance of and progress on various evaluation dimensions (Reach, Effectiveness, Adoption, Implementation, Maintenance or RE-AIM). Based on these assessments, teams prioritize one or two RE-AIM dimensions, set proximal goals, and implement strategies to improve their progress. This step follows an iterative process to refine the solutions. Finally, the dissemination phase ensures the findings and effective solutions are shared, facilitating broader adoption and scaling.
This project specifically focused on the second through fourth phases: problem exploration, knowledge exploration, and solution development. Each of these three steps of rapid-cycle research and their associated activities are described in Table 2. The fifth and sixth phases (solution testing and dissemination) were beyond the scope of this project and the preparation phase was accomplished prior to the adoption of the rapid cycle framework through the formation of the adaptation team.
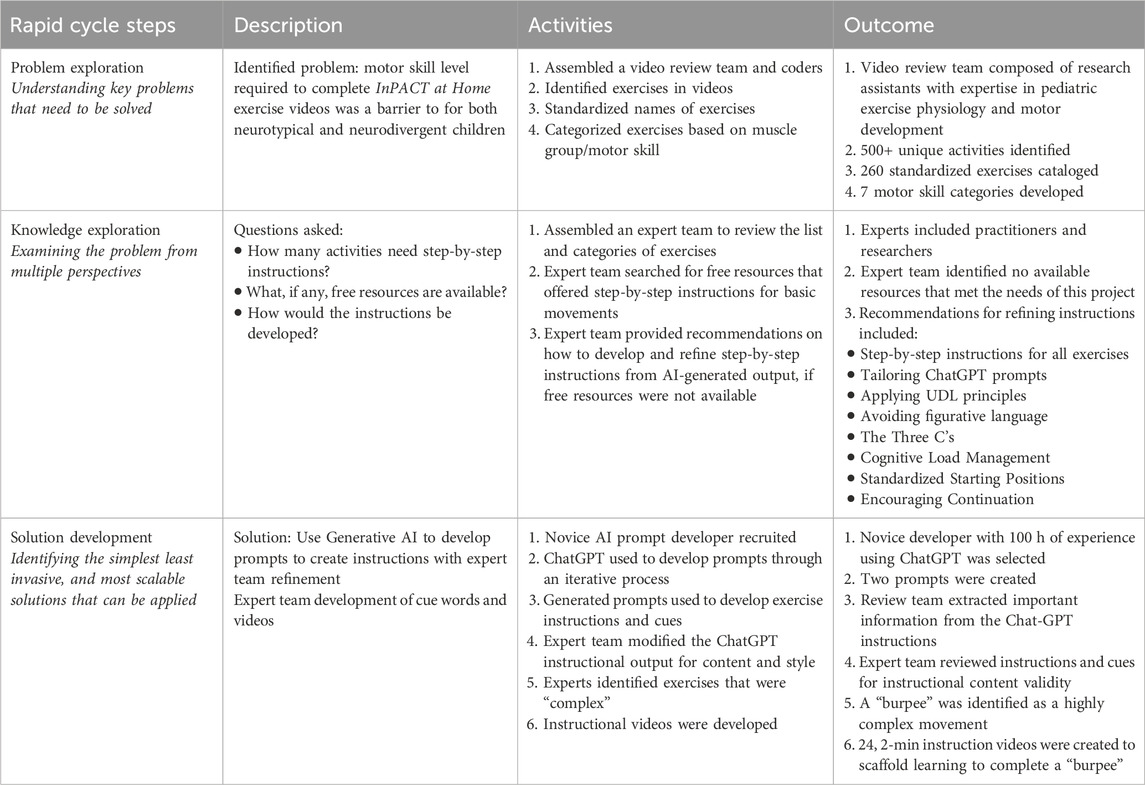
Table 2. Key cycle steps to adapt the InPACT at Home program for use in neurodivergent pediatric populations.
Problem exploration-understanding the problems that were important to solve
The adaptation team identified that the difficulty level of the InPACT at Home exercises posed a barrier to engagement for both neurotypical and neurodivergent children. Previous research found that the skill level needed to complete the exercises was a challenge for neurotypical children (Beemer et al., 2022). This suggested that skill level may also be a barrier for neurodivergent children. To improve program engagement for both neurotypical and neurodivergent children, it became necessary to identify which exercises featured in the videos required additional instructions, cues, and demonstrations to support participation. The following sections outline the activities conducted during the problem exploration phase.
Activity 1: assemble a video review team
During the problem exploration phase, the adaptation team formed a video review team to identify and categorize exercises in the InPACT at Home videos that required additional instructions, cues, and demonstrations (see Table 1). For this project, an exercise was defined as “a series of skills or movements performed to strengthen one or more muscle groups”.
The video review team had two distinct roles: “video reviewers”, who systematically documented exercise names in the videos, and “coders”, who standardized these names by grouping similar exercises under a single term. Standardizing exercise names aimed to reduce variations in terminology and concepts, minimizing the cognitive load on the learner’s working memory (van Merrienboer and Sweller, 2010). As a result, children could focus more on performing the movements rather than processing different terms or ideas.
Activity 2: identify exercises in videos
Each InPACT at Home video was reviewed to identify the exercises included. Each reviewers watched a subsection of the video catalog, noting every exercise taught and any unique exercise names that needed standardization. This process produced a comprehensive list of movements and exercises found in all InPACT at Home videos.
Activity 3: standardize exercise names
The coders then assigned each unique exercise a more standardized name (e.g., “stand-up sit-downs” were grouped under “squats”). To accomplish this, the coders examined each uniquely named exercise, watched the corresponding video segments, and identified its key movements. If those movements matched an exercise already on the standardized list, the coders grouped the activity under the appropriate name, eliminating the unique names from the final list.
Activity 4: categorize standardized exercises by muscle group or motor skill
After standardizing the exercise names, exercises were categorized based on the muscle group or movement skill they primarily targeted. The team coded the standardized list of exercises from the InPACT at Home videos, focusing on the main body parts and skills activated during the movements. Recognizing that no exercise exclusively targets a single body part or skill, the video review team determined which body part was most activated or which skill was most integral to each movement.
Knowledge exploration—Exploring the problem from different perspectives
The following sections outline the activities conducted during the knowledge exploration phase.
Activity 1: assemble an expert team
Drawing from insights gained during the problem exploration phase, the adaptation team brought together a group of experts—comprising researchers and practitioners from within the team—during the knowledge exploration phase. This team (A.P., H.L.M., K.W., and L.K.) reviewed the list and categories of exercises and provided guidance on developing step-by-step movement instructions tailored to meet the needs of neurodivergent children.
Activity 2: expert consultations to identify existing free resources
Members of the adaptation team (A.S., T.S., and R.E.H.) conducted a series of meetings with practitioners (A.P. and K.W.) from the expert team to explore the availability of free resources offering step-by-step instructions for fundamental movement skills. These discussions also addressed potential strategies for developing such instructions if free resources were not available. The team specifically considered the utility of generative artificial intelligence (AI) for creating tailored resources for neurodivergent children.
ChatGPT 3.5, a free AI chatbot developed by OpenAI, emerged from the discussions as a promising tool due to its ability to quickly provide accurate information and enable customization through interactive prompts (Ray, 2023). This capability allows users to tailor outputs to specific needs, making it a valuable resource for developing inclusive instructional materials. Additionally, using generative AI software would enable the adaptation team to efficiently develop and refine instructions for hundreds of activities—a task that would have otherwise taken months to complete.
In reviewing the literature, the adaptation team confirmed that generative AI had already been successfully used in fitness and medicine to instruct and inform users. For example, researchers in Finland used ChatGPT 4.0 to generate personalized workout plans that participants found to be high quality, engaging, and useful (Logacheva et al., 2014). Another study showed that medical students in Canada were more successful at learning surgical skills in simulations when tutored and given feedback by an AI tutor rather than an expert instructor (Fazlollahi et al., 2022).
While AI technologies are not yet recommended as replacements for personalized, progressive, and health condition-specific guidance from healthcare and fitness professionals, they can serve as valuable supplementary tools. In their current form, AI technologies enhance accessibility, particularly for individuals who cannot afford professional advice. Consequently, the practitioners discussed using generative AI alongside expert feedback to develop step-by-step instructions for inclusive physical activity.
Activity 3: expert recommendations for developing and refining instructions and cue words
If new resources needed to be developed, the expert team agreed to provide recommendations on how to develop and refine instructions and cue words from AI-generated output.
Solution development—identifying the simplest possible solution to be applied
The following sections outline the activities conducted during the solution development phase.
Activity 1: novice AI prompt developer recruitment
To assist in developing new instructions and cue words, a novice AI prompt developer was recruited. The decision to use a novice developer instead of a professional prompt engineer was intentional, aimed at simulating the experience of an average user with limited or no experience using ChatGPT. This approach ensured that generating instructions would be feasible for parents and families.
Activity 2: ChatGPT prompt development
The process of developing ChatGPT prompts was iterative. Initially, the bot was asked to provide instructions for a sample exercise (lateral lunge), and the outputs were then refined to match the desired content and format. For instance, if ChatGPT produced lengthy instructions (more than 10 steps), it was prompted to condense them. If the language used was not straightforward (e.g., using metaphors or elaborate sentences to describe the step) or was too verbose, it was instructed to simplify the wording. Subsequently, ChatGPT was asked, “What prompt should I use to get this output?” The returned output would then be used as a template prompt for each exercise on the standardized list by substituting “lateral lunge” for the exercise of interest (Prompt 1).
A similar process was used to develop a prompt that further shortened the length of the instructions, helping the content become more digestible (Prompt 2). The combination of both prompts allowed for the instructional content to be accurate (Prompt 1) and concise (Prompt 2). Figure 1 displays the series of ChatGPT inputs used in the form of a decision tree to generate prompts for creating inclusive step-by-step instructions. Supplementary Appendix S1 provides an example of the iterative process used to generate and refine exercise instructions from ChatGPT.
Step 1: Development of step-by-step instructions and cue words
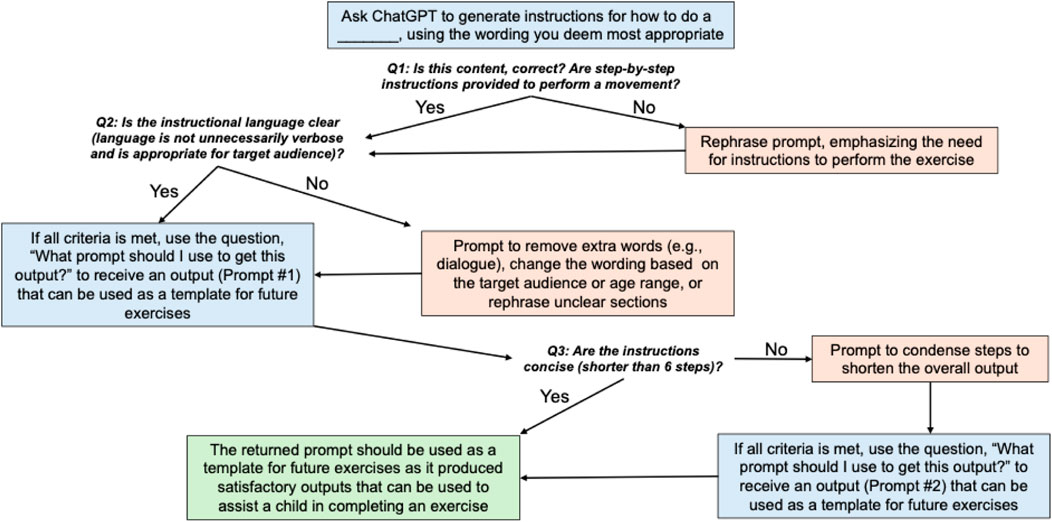
Figure 1. The decision tree used to initially generate ChatGPT prompts that return satisfactory exercise instructions. *Note: This study uses Prompt #1 and Prompt #2 in conjunction to generate instructions for each exercise. However, for replication purposes, users may be able to use only Prompt #1 or Prompt #2 to generate satisfactory results depending on what is returned by ChatGPT.
After finalizing the two template ChatGPT prompts, the AI prompt developer used the prompts to generate step-by-step exercise instructions for each activity on the standardized list of exercises.
Step 2: Refinement of step-by-step instructions
Once the AI-generated exercise instructions were created, members of the expert team reviewed and approved them for both content validity and style consistency. Based on this review, a set of expert recommendations was compiled to assist parents and families in using generative AI to develop their own instructions for additional exercises beyond those included in the InPACT at Home program.
Step 3: Cue word development and refinement
After the expert team reviewed and approved the AI-generated instructions for content and style, the video review team began developing short cue words (2-3 words) to reinforce key concepts from the instructions. The focus was on content validity, ensuring that the cue words were derived directly from the longer instructions.
The video review team assessed the instructions to identify critical words related to physical form or specific body movements. For example, the AI-generated instructions for a squat exercise might read:
Starting Position: 1) Stand with feet hip-width apart. 2) Bend Knees: Slowly bend knees, like sitting in a chair. 3) Keep Back Straight: Maintain a straight back. 4) Go Down Comfortably: Lower body as far as comfortable. 5) Push Up: Push through heels to stand straight.
From this, the expert feedback led to refined instructions: 1) Stand with feet hip width apart; 2) Pretend you’re sitting in a chair; 3) Push through heels to stand.
The corresponding cue words, developed by the review team, would then be: 1. Feet apart; 2. Pretend chair sit; 3. Push to stand.
The expert team then verified that each cue word reinforced essential information for completing the movement. By combining AI-generated instructions with expert feedback to refine the cues, the new resources were reviewed at multiple levels—iteratively refined by AI, the video review team, and the expert team—to ensure the content was accurate and beneficial for both neurotypical and neurodivergent children.
Step 4: Expert identification of “complex” exercises
After developing the step-by-step exercise instructions and cue words, the expert team identified which exercises were “complex”. These exercises were deemed particularly challenging for children due to the involvement of multiple compound movements. For these exercises it was recommended that children would benefit from demonstration videos to better understand these movements. This aligned with the UDL principle of Representation, which emphasizes presenting information in multiple formats to support diverse ways of learning and engaging with instructional content (Meyer et al., 2014).
The expert team identified specific complex exercises in the InPACT at Home videos that could be broken down into individual movements and then scaffolded into a video series teaching comprehensive whole-body complex movements. Additionally, it was determined that these step-by-step instructional videos could serve as introductory videos for both neurodivergent and neurotypical youth who are new to the InPACT at Home program. This approach ensured that all participants, regardless of their developmental background, could effectively learn and engage with the InPACT at Home exercises.
Step 5: Video development
A member of the expert team, A.P., was chosen to appear in the instructional videos due to her previous experience in exercise video production. An expert in video script development (J.B.) was recruited to join the expert team to create the video content, while R.E.H., the InPACT program director, served as the scientific advisor to ensure the accuracy of the video content. All videos were filmed at a community location using professional equipment and staff.
Results
Problem exploration
Outcome 1: composition of the video review team
The video review team consisted of graduate and undergraduate research assistants from the adaptation team with expertise in pediatric exercise physiology and motor development. Five assistants were assigned as video reviewers, while the other two served as video coders.
Outcome 2: identification of unique exercises
From the 132 videos in the InPACT at Home program, more than 500 unique exercises were identified.
Outcome 3: standardization of exercises
The 500+ unique exercises were consolidated into a list of 259 standardized exercises.
Outcome 4: standardized exercises categorized by muscle group or motor skill
The list of standardized exercises was then coded into one of seven fundamental motor skill categories based on the skill that was performed: jumping, lateral movement, core, upper body, lower body, sports skills, and compound movement. Table 3 describes the key features and examples of each category. For example, the “squat” exercise was initially identified to target glutes and quadriceps muscles. This was then coded into the lower body category, as the muscles predominantly involved were part of lower body muscle groups. This coding process helped the team visualize the distribution of exercises across motor skills categories. From this analysis, there were 11 jumping exercises, 4 lateral movement exercises, 28 core exercises, 61 upper body exercises, 68 lower body exercises, 48 sports skill movements, and 39 compound movement exercises.
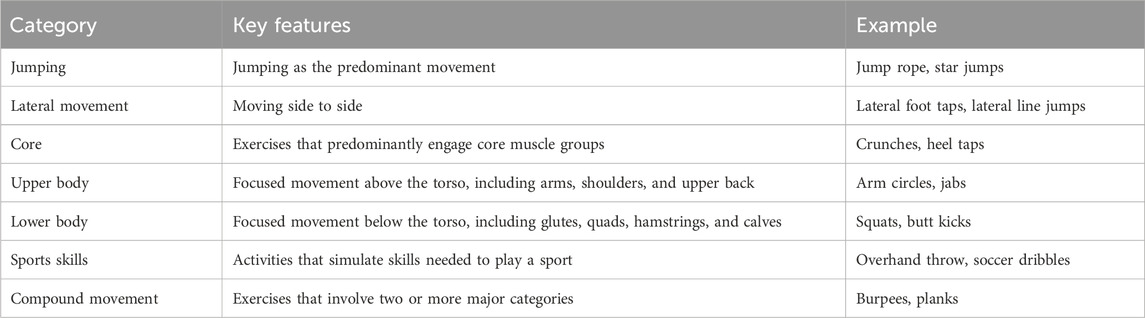
Table 3. InPACT at Home Exercise Categories. This table displays each category of exercise present in the InPACT at Home program. Each category includes distinct key features that help determine which category each exercise belongs in. The table also provides examples of exercises in each category.
Knowledge exploration
Outcome 1: expert team assembled
The expert team consisted of four researchers and/or practitioners with expertise in neurodivergent movement, adapted physical education, and physical education. This team reviewed a subset of the compiled list of activities and developed a strategy for creating a glossary of exercise instructions.
Outcome 2: expert identification of available resources
Consultations with the practitioners on the expert team revealed that while validated adapted physical activity resources exist, many come with associated costs and are not freely accessible to the public. The free resources that are available do not include step-by-step instructions for teaching fundamental motor skills. As a result, the decision was made to use ChatGPT to generate step-by-step instructions.
Outcome 3: expert recommendations for developing and refining instructions from AI-generated output
Throughout the project, nine meetings with the expert team were conducted, leading to several key recommendations for developing and refining the AI-generated exercise instructions:
Step-by-Step instructions for all exercises
Early discussions with researchers H.L.M. and L.R.K. led to the recommendation that all exercises, regardless of complexity, should include step-by-step instructions. This approach was chosen due to the lack of a clear definition for complex exercises and the need to address individual differences, particularly for neurodivergent children.
Tailoring ChatGPT prompts for neurodivergent children
The team emphasized the importance of adjusting ChatGPT prompts to meet the unique needs of neurodivergent children, who often have different body awareness compared to neurotypical peers (Fears et al., 2023). The researchers highlighted that any movement is beneficial, even if it does not perfectly match the cue words and instructions.
Applying UDL principles
A strong focus was placed on UDL principles. The team stressed the need to include both written descriptions and visual aids (e.g., pictures and videos) to accommodate diverse learning preferences and enhancing accessibility. Accordingly, the expert team recommended presenting instructional content in three formats: detailed instructions, short cues, and videos. This variety allows children to learn in the format that best suits their needs, whether through text or visual aids, and helps ensure accessibility for all learners (Meyer et al., 2014).
Avoiding figurative language
Practitioners A.P. and K.W. advised against using figurative language (e.g., metaphors like “keep your eyes on the target”) in the instructions (Holt and Ratliffe, 2004), as neurodivergent children often struggle with figurative language. Instead, they recommended clear, straightforward language to improve understanding (Kalandadze et al., 2018).
The three C’s
The expert team recommended focusing on the 3 C’s for instructional content—conciseness, clarity, and consistency—to reduce cognitive load and improve comprehension (Sweller et al., 2011). Conciseness refers to using as few words as possible, clarity involves using simple and unambiguous language, and consistency requires using the same terminology for each activity.
Cognitive load management
The team recommended limiting each exercise to three-to-five cues, with each cue being two-to-three words long. This helps prevent cognitive overload, as research indicates that working memory typically holds only three-to-four pieces of information (Farrington, 2011).
Standardized starting positions
To reduce unnecessary wording, the expert team established four standardized starting position names: “ready position” (stand upright, feet together), “stand comfortably” (stand upright, feet shoulder-width apart), “lie down” (lie on back with body parts flat on the ground), and “bend knees” (feet shoulder-width apart, in a half-squat position).
Encouraging continuation
The expert team also recommended adding the phrase “Keep Going!” at the end of instructions to signal that the movement should be repeated until the child feels comfortable.
Solution development
Outcome 1: novice AI prompt developer identified
A member of the adaptation team with approximately 100 h of experience using ChatGPT 3.5 was selected to create concise instructions and supplementary cue words for each exercise.
Outcome 2: ChatGPT prompts
Through the iterative process of developing ChatGPT prompts, the team identified two complementary prompts that, when used together, offered consistent and effective instructions. These two prompts were, “Provide simplified step-by-step instructions for a [insert exercise name here] suitable for a neurodivergent child” and “Condense the step-by-step instructions for a [insert exercise name here] suitable for a neurodivergent child.”
Outcome 3: step-by-step instruction and cue word development
These AI-generated prompts were inserted into ChatGPT one after the other, substituting the blank for an exercise name, to result in a set of instructions to perform the movement. The review team then extracted the important information from the ChatGPT-generated instructions to develop cue words. Table 4 displays a sample of the developed instructions and cue words.
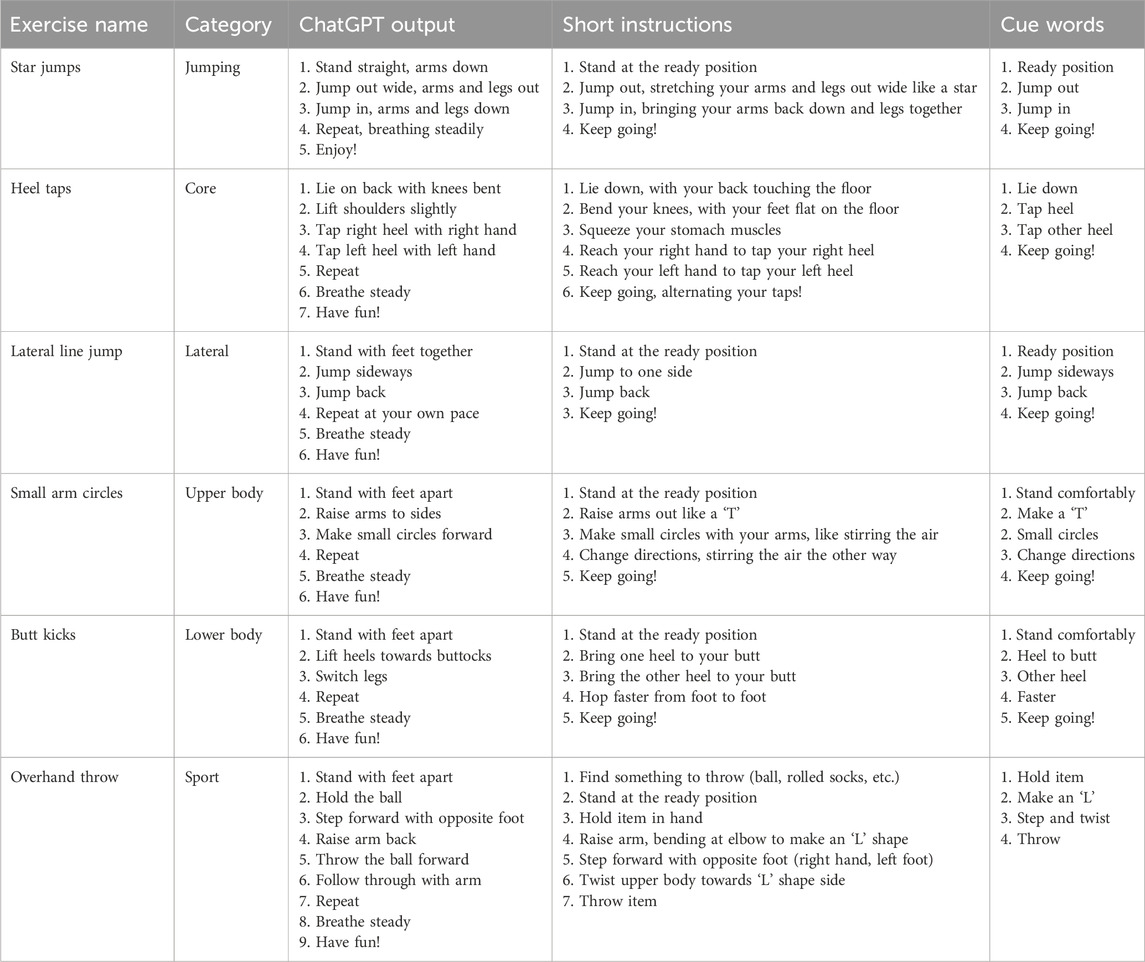
Table 4. A sample of exercises, the ChatGPT outputs, the corresponding instructions, and their cues. Short instructions and cue words were developed by the review team with expert input.
Outcome 4: step-by-step instruction and cue word refinement
After the initial development of cues and instructions, the expert team reviewed them for instructional content validity. They ensured that the wording for starting positions, signals for repetitions, and instructions for general movements remained consistent across each set of instructions and thoroughly covered all the necessary information to correctly perform the movement. This qualitative process helped to ensure the accuracy of the instructions and cues.
Outcome 5: expert identification of “complex” exercises
The burpee was identified as a highly complex movement due to its combination of multiple motor skills (e.g., jumping and balancing), compound movements (e.g., engaging the core, lower body, and jumping), and the need for precise coordination across nearly every muscle group. Given its complexity, the burpee was selected as an example for a demonstration video to guide participants in mastering the movement effectively.
Outcome 6: video development
Figure 2 shows a visual representation of several videos designed to teach children how to perform complex exercises by breaking the movements down into manageable steps. A total of 24 videos, each 2 minutes long, was created for this purpose. These videos were organized into four units, with each unit named after the specific complex exercise covered in its series of six videos. Within every unit, exercises were ordered so that each new skill could be scaffolded onto the next, ensuring that the fundamental skills needed to complete the complex exercise were mastered before moving on to the next component. For example, completing unit 1 meant that the child would be able to perform a straight arm jack, a complex version of a jumping jack. To do this, they are taught how to jump in video 1, how to move their legs side to side in video 2, how to jump in and out in video 3, how to move their arms in video 4, how to put everything together to perform a jumping jack in video 5, and then finally how to perform a straight jack in video 6.
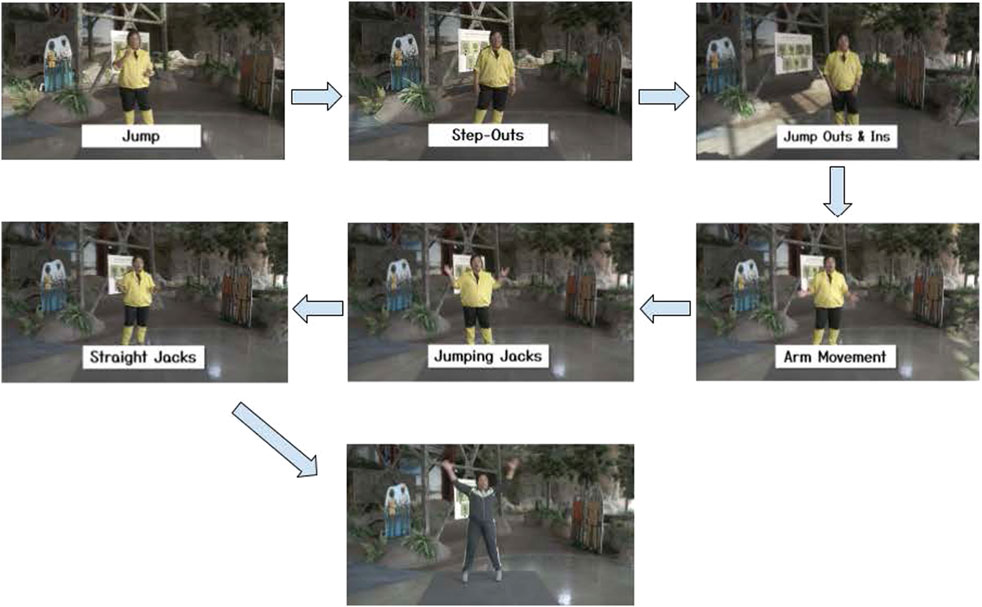
Figure 2. Screenshots from each of the videos in unit 1, leading up to straight jacks (a scaled-up version of jumping jacks). The last image shows the basic foundational exercise from unit 1, jumping jacks, serving as the warmup for unit 2 videos.
Each of the first three units focused on teaching different complex exercises that were about the same difficulty. Because the expert team determined that one of the most complex exercises present in the InPACT at Home videos was the burpee, exercises in units 1-3 focused on skills that would help perform a burpee in unit 4. These foundational skills were reinforced through each unit by making moves from the previous unit serve as the warm-up in the following unit (e.g., jumping jacks from unit 1 were the warm-up for exercises in unit 2).
To ensure equitable access, the videos are broadcast on the Michigan Learning Channel as part of their “Read, Write, ROAR!” program (https://www.michiganlearning.org). They are now also a complementary component of the InPACT at Home program (inpactathome.umich.edu). The instructions for all these exercises are also being compiled into a glossary and will be made available to families on the program website.
Discussion
Systematic adaptation process
To enhance the accessibility of the InPACT at Home program for neurodivergent children, a systematic adaptation approach was utilized. The process began with a video review team identifying and categorizing exercises by muscle group or skill (problem exploration). Following this, a series of meetings with an expert team established the criteria for creating step-by-step instructions (knowledge exploration). Generative AI was then used to generate initial instructions, which were reviewed, refined, and supplemented with short cues by the expert team. For exercises that were particularly complex, additional instructional videos were produced to offer further guidance (solution development).
This approach addressed a fundamental shortcoming of many at-home physical activity programs, which often lack options for children with diverse cognitive needs and may require financial resources or prior exercise knowledge (Rimmer and Rowland, 2008). By integrating generative AI with expert feedback, this adaptation process rapidly provided step-by-step instructions, ensuring that neurodivergent children have equitable opportunities to participate in physical activity at home. InPACT for Everyone includes prompts and guidelines that parents can use to generate instructions, sample instructions and cues for activities, and videos to further support participation. The outcome of this systematic process of adaptation provides families with the tools to support their children in completing virtual exercise routines without financial constraints or access barriers.
Collaborative expertise and adaptation
Similar to the initial adaptation of the InPACT program from the classroom to the home environment, the InPACT at Home program’s adaptation relied on collaboration with researchers and practitioners specializing in motor development, pediatric exercise physiology, inclusive physical activity practices, and adapted physical education. These experts were considered “physically educated” (Decorby et al., 2005), and contributed essential expertise to teach basic movement skills, apply UDL principles, and model a range of inclusive physical activities that promote lifelong participation in physical activity.
Role of generative AI in adaptation
In this study, ChatGPT was used to create step-by-step instructions for physical activities, leveraging a free and accessible platform to support neurodivergent children. While several programs offer evidence-based resources, their cost limits accessibility for many families. For example, Sports, Play, and Active Recreation for Kids (SPARK) is an evidence-based program that offers physical education resources and curricula to promote physical activity and healthy lifestyles in schools (McKenzie et al., 2016). SPARK is particularly useful as it breaks exercises down into manageable steps and includes inclusive physical education options. Similarly, the Effective Physical Education Curriculum (EPEC) program aims to create inclusive physical education environments and ensure accessibility for all children, including those with disabilities, by providing progressive exercises to reinforce new skills and apply them in various contexts (Michigan's Exemplary Physical Education Curriculum Project, 2000). However, both SPARK and EPEC are behind paywalls, limiting their accessibility for parents who want to guide their children in exercises.
OPEN (https://openphysed.org) provides high quality free curriculum resources to schools but this curriculum lacks specific instructor prompts for teaching fundamental motor skills. The National Center on Health, Physical Activity and Disability (https://www.nchpad.org) offers free information and exercise videos for people with physical, sensory, and cognitive disabilities, but provides limited guidance on teaching motor skills and complex movements to neurodivergent children who need additional support. Finally, resources like Steps to Inclusion (Tristani et al., 2019) provide theoretical guidance on making physical activity inclusive but can be challenging for parents without practical experience. By utilizing ChatGPT and integrating expert feedback, the current study demonstrated how AI can bridge these gaps, offering accessible and practical tools for parents and families.
Observations on AI output and inclusivity
An interesting observation made during the project was ChatGPT’s tendency to include motivational language when prompted to develop tailored instructions for neurodivergent children. This extra content was not consistently included when ChatGPT was asked to provide instructions alone or when the target audience was specified as “kids”. Although this motivational content was removed from the instructional materials for this project due to its lack of direct relevance to the movements, it is noteworthy that ChatGPT tends to add extra information based on assumptions about the needs of neurodivergent children.
That phenomenon highlights the importance of training AI models with diverse, inclusive datasets, as an AI model’s effectiveness depends on the training data it was developed with. Research on developing inclusive AI systems highlights that the problem-solving frameworks used for training often represent a single viewpoint, which can lead to homogenization and perpetuate stereotypes or biases (Hutson, 2024). For example, the above-mentioned scenario with ChatGPT implies that neurotypical children do not require additional motivation to complete exercises, whereas neurodivergent children do. Motivation levels vary among all individuals, regardless of whether they are neurodivergent or neurotypical. Thus, a neurotypical child who needs extra motivational content might not receive it, while a neurodivergent child with strong intrinsic motivation might receive unnecessary motivational content that could detract from the specific exercise. Hutson suggests that AI models like ChatGPT should be trained with broader, more diverse data sets, including those reflecting the viewpoints of neurodivergent individuals, to enhance inclusivity and expand the model’s utility in diverse contexts (Hutson, 2024). Future research should explore strategies for optimizing AI training to better reflect the nuanced needs of all users, ensuring equitable and accurate outputs.
UDL framework
UDL, a framework developed by the Center for Applied Special Technology (CAST), aims to enhance and optimize teaching and learning for everyone, drawing on scientific insights into how humans learn (CAST, 2024). UDL has been successfully applied in various contexts to enhance instructional content accessibility. For instance, UDL, combined with the inclusion spectrum, has helped general physical education teachers align learning goals with activities that enable neurodivergent children to interact with their peers while staying physically active (Grenier et al., 2017). Additionally, UDL, together with the Planning for All Learners (PAL) procedures, has improved the accessibility of high school reading comprehension programs (Meo, 2008). The PAL process provides a practical four-step approach for implementing UDL: (1) setting goals, (2) analyzing the current status of the curriculum and classroom, (3) applying the UDL framework to lesson and unit development, and (4) teaching these UDL-aligned lessons and units (Israel et al., 2014).
As generative AI becomes increasingly popular, more programs are beginning to combine AI with UDL to enhance inclusivity. For example, one initiative used AI to optimize UDL implementation in an online graduate course, enabling personalized learning and customized assessments and course content (Morgan et al., 2024). Another project employed AI to develop K-12 health education lesson plans incorporating UDL principles, allowing teachers with no prior experience in health education to effectively teach the content (Conrad and Rees, 2024). While generative AI has been used in education to enhance UDL applications, its combination with UDL principles for creating inclusive physical activity resources at home remains underexplored. This project addresses that gap by providing a model for integrating UDL and AI to enhance accessibility and inclusivity.
Strengths and limitations
This study highlights several key strengths. First, it utilized implementation and dissemination science frameworks along with universal design to systematically adapt the InPACT at Home program. The involvement of a diverse adaptation team was another major strength, ensuring that multiple perspectives were integrated into the resource development process, thereby enhancing the accessibility of the resources for the pediatric population in Michigan. Additionally, the innovative use of ChatGPT to create inclusive instructional content was validated by incorporating expert feedback, which further strengthened the content.
However, the study also has some limitations. Previous research has highlighted AI’s tendency to “confabulate” (i.e., to make up something without malicious intent), which may have affected the accuracy of ChatGPT’s output (Alkaissi and McFarlane, 2023). That limitation was mitigated by refining the AI-generated content through expert team feedback. Another limitation is that the effectiveness of the InPACT at Home adaptation—specifically its step-by-step instructions, cue words, and demonstration videos—in improving program participation among neurodivergent children has not yet been rigorously tested. Additionally, the current study focuses solely on children, creating a gap in research on how these adaptations might apply to other age groups. Furthermore, the adaptation focused exclusively on the UDL principle of “Representation.” Future research should explore how the UDL principles of “Engagement” and “Action and Expression” could be employed to further optimize inclusion within the InPACT at Home program. Finally, since the goal of InPACT for Everyone is to make the program accessible to all children, further testing is needed to determine whether this approach is effective for individuals with physical or cognitive disabilities beyond neurodivergence. It is our hope that the flexibility of this approach can be adapted to benefit a broader and more diverse community.
Conclusions
In conclusion, this study provides valuable insights into the rapid adaptation of the InPACT at Home program for neurodivergent children by integrating generative AI with expert feedback and grounding the process in dissemination and implementation science frameworks. That systematic approach not only addressed barriers to accessibility that often limit participation in at-home physical activity programs but also offers a replicable model for families to create their own physical activity resources.
By following specific guidelines—such as using ChatGPT prompts to generate detailed instructions, ensuring the content is concise, clear, and consistent, and presenting the instructions in various forms—families can effectively support their children’s physical activity at home. While the study highlights promising outcomes, further research is needed to rigorously test the effectiveness of these adaptations and explore additional UDL principles to enhance inclusivity. Ultimately, this work sets a precedent for promoting health equity through the systematic and inclusive design of physical activity interventions, helping to reduce physical activity disparities and foster healthy habits among all children.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
TS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Writing–original draft, Writing–review and editing. HM: Conceptualization, Methodology, Supervision, Writing–review and editing. AS: Data curation, Investigation, Methodology, Writing–review and editing. LK: Formal Analysis, Investigation, Methodology, Supervision, Writing–review and editing. AP: Data curation, Investigation, Methodology, Writing–review and editing. KW: Methodology, Supervision, Writing–review and editing. JB: Data curation, Writing–review and editing. RZ: Funding acquisition, Writing–review and editing. RH: Funding acquisition, Project administration, Supervision, Writing–original draft, Writing–review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported in part by the National Institutes of Health (P30-AG024824) and the Michigan Health Endowment Fund (R-2204-150254)
Acknowledgments
The author would like to thank collaborators from the InPACT for Everyone adaptation team for their contributions and involvement in this project. The results of this study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. ChatGPT version 3.5 was used to edit the grammar and sentence structure of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2024.1496114/full#supplementary-material
References
Alkaissi H., McFarlane S. I. (2023). Artificial hallucinations in ChatGPT: implications in scientific writing. Cureus 15 (2), e35179. doi:10.7759/cureus.35179
Alliance P. A. (2024). The 2024 United States Report card on physical activity for children and youth.
Baumann A., Cabassa L., Stirman S. (2018). “Adaptation in dissemination and implementation science,” in Dissemination and implementation research in health: translating science to practice. Editors R. Brownson, G. A. Colditz, and E. Proctor 2nd Edn (Oxford University Press), 285–300.
Beemer L. R., Tackett W., Kinnet-Hopkins D., Hasson R. E. (2022). Child perceptions of a home-based, virtual, instructor-led, physical activity program. Med. Sci. Sports Exe. 54, 233. doi:10.1249/01.mss.0000877944.24309.dc
Beemer L. R., Tackett W., Schwartz A., Schliebe M., Miller A., Eisman A. B., et al. (2023). Use of a novel theory-based pragmatic tool to evaluate the quality of instructor-led exercise videos to promote youth physical activity at home: preliminary findings. Int. J. Environ. Res. Public Health 20 (16), 6561. doi:10.3390/ijerph20166561
Beemer L. R., Eisman A. B., Templin T., Robinson L. E., Miller A., Tackett W., et al. (2024). “Assessing children's adherence to the InPACT at Home intervention: A mixed methods study,” in Press at Journal of Teaching in Physical Education.
Bremer E., Crozier M., Lloyd M. (2016). A systematic review of the behavioural outcomes following exercise interventions for children and youth with autism spectrum disorder. Autism 20 (8), 899–915. doi:10.1177/1362361315616002
Case L., Ross S., Yun J. (2020). Physical activity guideline compliance among a national sample of children with various developmental disabilities. Disabil. Health J. 13 (2), 100881. doi:10.1016/j.dhjo.2019.100881
CAST (2024). Universal design for learning guidelines version 3.0. Available at: https://udlguidelines.cast.org (Accessed November 26, 2024).
Ceccarelli S. B., Ferrante C., Gazzola E., Marzocchi G. M., Nobile M., Molteni M., et al. (2020). Fundamental motor skills intervention for children with autism spectrum disorder: a 10-year narrative review. Children 7 (11), 250. doi:10.3390/children7110250
Conrad E. J., Rees L. K. (2024). Generative AI as a catalyst to elevate school health education. J. Phys. Educ. Recreat. Dance 95 (6), 45–51. doi:10.1080/07303084.2024.2355865
Decorby K., Halas J., Dixon S., Wintrup L., Janzen H. (2005). Classroom teachers and the challenges of delivering quality physical education. J. Educ. Res. 98 (4), 208–221. doi:10.3200/joer.98.4.208-221
De Meester A., Stodden D., Goodway J., True L., Brian A., Ferkel R., et al. (2018). Identifying a motor proficiency barrier for meeting physical activity guidelines in children. J. Sci. Med. Sport 21 (1), 58–62. doi:10.1016/j.jsams.2017.05.007
Farrington J. (2011). From the research: myths worth dispelling: seriously, the game is up. Perform. Improv. Q. 24, 105–110. doi:10.1002/piq.20114
Fazlollahi A. M., Bakhaidar M., Alsayegh A., Yilmaz R., Winkler-Schwartz A., Mirchi N., et al. (2022). Effect of artificial intelligence tutoring vs expert instruction on learning simulated surgical skills among medical students: a randomized clinical trial. Jama Netw. Open 5 (2), e2149008. doi:10.1001/jamanetworkopen.2021.49008
Fears N. E., Templin T. N., Sherrod G. M., Bugnariu N. L., Patterson R. M., Miller H. L. (2023). Autistic children use less efficient goal-directed whole body movements compared to neurotypical development. J. Autism Dev. Disord. 53 (7), 2806–2817. doi:10.1007/s10803-022-05523-0
Grenier M., Miller N., Black K. (2017). Applying universal design for learning and the inclusion spectrum for students with severe disabilities in general physical education. J. Phys. Educ. Recreat. Dan. 88 (6), 51–56. doi:10.1080/07303084.2017.1330167
Hasson R. E., Beemer L. R., Ajibewa T. A., Eisman A. B. (2021). Adapting the InPACT intervention to enhance implementation fidelity and flexibility. Prev. Sci. 22 (3), 324–333. doi:10.1007/s11121-020-01199-z
Hasson R. E., Eisman A. B., Wassmann A., Martin S., Pugh P., Winkelseth K., et al. (2022). Rapid cycle adaptation of a classroom-based intervention to promote equity in access to youth physical activity. Transl. Behav. Med. 12 (9), 945–955. doi:10.1093/tbm/ibac049
Holt B. J., Ratliffe T. (2004). Help children learn skills by using figurative language. Teach. Elem. Phys. Educ. 15 (3), 28–29. Available at: https://eric.ed.gov/?id=EJ757256
Huang J., Du C., Liu J., Tan G. (2020). Meta-analysis on intervention effects of physical activities on children and adolescents with autism. Int. J. Environ. Res. Public Health 17 (6), 1950. doi:10.3390/ijerph17061950
Hutson P. (2024). Embracing the irreplaceable: the role of neurodiversity in cultivating human-AI symbiosis in education. Int. J. Emerg. Dis. Innova. Educ. 2 (1), 5. doi:10.62608/2831-3550.1020
Israel M., Ribuffo C., Smith S. (2014). Universal design for learning: recommendations for teacher preparation and professional development (document No. IC-7). Available at: http://ceedar.education.ufl.edu/tools/innovation-configurations/. (Accessed August 25, 2024).
Johnson K., Gustafson D., Ewigman B., Provost L., Roper R. (2015). Using rapid-cycle research to reach goals: awareness, assessment, adaptation, acceleration.
Johnson M., Nocera V., Kaushal N., Simon L., Hasson R., Equity A. H. (2021). Why we must prioritize equitable access to physical activity for children with disabilities. Available at: https://www.acsm.org/blog-detail/acsm-blog/2021/03/22/prioritize-equitable-access-to-physical-activity-for-children-with-disabilities.
Kalandadze T., Norbury C., Naerland T., Naess K. B. (2018). Figurative language comprehension in individuals with autism spectrum disorder: a meta-analytic review. Autism 22 (2), 99–117. doi:10.1177/1362361316668652
King G., Law M., King S., Rosenbaum P., Kertoy M. K., Young N. L. (2003). A conceptual model of the factors affecting the recreation and leisure participation of children with disabilities. Phys. Occup. Ther. Pediatr. 23 (1), 63–90. doi:10.1080/J006v23n01_05
Koh S. H. (2024). Analyzing the influence of physical exercise interventions on social skills in children with autism spectrum disorder: insights from meta-analysis. Front. Psychol. 15, 1399902. doi:10.3389/fpsyg.2024.1399902
Liang X., Li R., Wong S. H. S., Sum R. K. W., Sit C. H. P. (2020). Accelerometer-measured physical activity levels in children and adolescents with autism spectrum disorder: a systematic review. Prev. Med. Rep. 19, 101147. doi:10.1016/j.pmedr.2020.101147
Liang X., Li R., Wong S. H. S., Sum R. K. W., Wang P., Yang B., et al. (2022). The effects of exercise interventions on executive functions in children and adolescents with autism spectrum disorder: a systematic review and meta-analysis. Sports Med. 52 (1), 75–88. doi:10.1007/s40279-021-01545-3
Lieberman L. J., Grenier M., Brian A., Arndt K. (2021). Universal design for learning in physical education. 1st Edn. Champagne, IL: Human Kinetics.
Lieberman L. J., Houston-Wilson C. (2018). Strategies for inclusion:Physical education for everyone. 3rd Edn. Champagne, IL: Human Kinetics.
Logacheva E., Hellas A., Prather J., Sarsa S., Leinonen J. (2014). Evaluating contextually personalized programming exercises created with generative AI. Association for Computing Machinery, 95–113. Available at: https://arxiv.org/pdf/2407.11994v1.
Logan K., Cuff S., Council On Sports M., Brooks M. A., Canty G., Diamond A. B., et al. (2019). Organized sports for children, preadolescents, and adolescents. Pediatrics 143, e20190997. doi:10.1542/peds.2019-0997
McCoy S. M., Jakicic J. M., Gibbs B. B. (2016). Comparison of obesity, physical activity, and sedentary behaviors between adolescents with autism spectrum disorders and without. J. Autism Dev. Disord. 46 (7), 2317–2326. doi:10.1007/s10803-016-2762-0
McDermott G., Brick N. E., Shannon S., Fitzpatrick B., Taggart L. (2022). Barriers and facilitators of physical activity in adolescents with intellectual disabilities: an analysis informed by the COM-B model. J. Appl. Res. Intellect. Disabil. 35 (3), 800–825. doi:10.1111/jar.12985
McKenzie T. L., Sallis J. F., Rosengard P., Ballard K. (2016). The SPARK programs: a public health model of physical education research and dissemination. J. Teach. Phys. Educ. 35, 381–389. doi:10.1123/jtpe.2016-0100
Meo G. (2008). Curriculum planning for all learners: applying universal design for learning (UDL) to a high school reading comprehension program. Prev. Sch. Fail. Altern. Educ. Child. Youth 52 (2), 21–30. doi:10.3200/psfl.52.2.21-30
Meyer A., Rose D. H., Gordon D. (2014). Universal design for learning: theory and practice. Lynnfield, MA: CAST Professional Publishing.
Monteiro C. E., Da Silva E., Sodre R., Costa F., Trindade A. S., Bunn P., et al. (2022). The effect of physical activity on motor skills of children with autism spectrum disorder: a meta-analysis. Int. J. Environ. Res. Public Health 19 (21), 14081. doi:10.3390/ijerph192114081
Morgan A. (2024). “Unlocking learning potential with universal design in online learning environments,” in Leveraging generative artificial intelligence to expedite UDL implementation in online courses. Editors M. Bartlett, and S. Ehrlich (Hershey, PA: IGI Global), 171–195.
Murphy N. A., Carbone P. S. (2008). Promoting the participation of children with disabilities in sports, recreation, and physical activities. Pediatrics 121 (5), 1057–1061. doi:10.1542/peds.2008-0566
Parsons K., Payne S., Holt N., Wallace J. (2024). A qualitative study of physical activity drivers in autistic individuals using COM-B. Autistic and non-autistic perspectives. Res. Autism Spectr. Disord. 111, 102331. doi:10.1016/j.rasd.2024.102331
Piercy K. L., Troiano R. P. (2018). Physical activity guidelines for Americans from the US department of health and human services. Circ. Cardiovasc Qual. Outcomes 11 (11), e005263. doi:10.1161/CIRCOUTCOMES.118.005263
Michigan's Exemplary Physical Education Curriculum Project (2000). EPEC: exemplary physical education curriculum: lessons. Manual. Lansing, MI: Michigan Fitness Foundation.
Rafie F., Ghasemi A., Zamani Jam A., Jalali S. (2017). Effect of exercise intervention on the perceptual-motor skills in adolescents with autism. J. Sports Med. Phys. Fit. 57 (1-2), 53–59. doi:10.23736/S0022-4707.16.05919-3
Ray P. P. (2023). ChatGPT: a comprehensive review on background, applications, key challenges, bias, ethics, limitations and future scope. Internet Things Cyber-Physical Syst. 3, 121–154. doi:10.1016/j.iotcps.2023.04.003
Rimmer J. A., Rowland J. L. (2008). Physical activity for youth with disabilities: a critical need in an underserved population. Dev. Neur. 11 (2), 141–148. doi:10.1080/17518420701688649
Ruggeri A., Dancel A., Johnson R., Sargent B. (2020). The effect of motor and physical activity intervention on motor outcomes of children with autism spectrum disorder: a systematic review. Autism 24 (3), 544–568. doi:10.1177/1362361319885215
Scott-Andrews K. Q., Miller A. L., Templin T. J., Hasson R. E., Robinson L. E. (2021). The feasibility and challenges of conducting online research to examine movement behavior in parents and children during the COVID-19 pandemic. Front. Public Health 9, 720083. doi:10.3389/fpubh.2021.720083
Staples K. L., Reid G. (2010). Fundamental movement skills and autism spectrum disorders. J. Autism Dev. Disord. 40 (2), 209–217. doi:10.1007/s10803-009-0854-9
St John L., Borschneck G., Cairney J. (2020). A systematic review and meta-analysis examining the effect of exercise on individuals with intellectual disability. Am. J. Intellect. Dev. Disabil. 125 (4), 274–286. doi:10.1352/1944-7558-125.4.274
Sun W., Yu M., Zhou X. (2022). Effects of physical exercise on attention deficit and other major symptoms in children with ADHD: a meta-analysis. Psychiatry Res. 311, 114509. doi:10.1016/j.psychres.2022.114509
Sweller J., Ayres P., Kalyuga S. (2011). “Intrinsic and extraneous cognitive load. Cognitive load theory explorations in the learning sciences,” in Instructional systems and performance technologies (Springer), 1.
Taylor S. L., Downs S. J., Rudd J. R., McGrane B., Melville C. A., McGarty A. M., et al. (2024). Associations between motor competence and physical activity levels of children with intellectual disabilities and/or autism spectrum disorder: movement matters. J. Intellect. Disabil. 28 (4), 976–993. doi:10.1177/17446295231203764
Tristani L., Tomasone J., Gainforth H., Bassett-Gunter R. (2019). Taking steps to inclusion: a content analysis of a resource aimed to support teachers in delivering inclusive physical education. Int. J. Disabil. Dev. Educ. 68 (1), 116–135. doi:10.1080/1034912x.2019.1662890
van Merrienboer J. J., Sweller J. (2010). Cognitive load theory in health professional education: design principles and strategies. Med. Educ. 44 (1), 85–93. doi:10.1111/j.1365-2923.2009.03498.x
Wang Z., Norris S. L., Bero L. (2018). The advantages and limitations of guideline adaptation frameworks. Implement. Sci. 13 (1), 72. doi:10.1186/s13012-018-0763-4
Wiltsey Stirman S., Gutner C. A., Crits-Christoph P., Edmunds J., Evans A. C., Beidas R. S. (2015). Relationships between clinician-level attributes and fidelity-consistent and fidelity-inconsistent modifications to an evidence-based psychotherapy. Implement. Sci. 10, 115. doi:10.1186/s13012-015-0308-z
Keywords: generative AI, universal design for learning (UDL), adolescent and youth, exercise, implementation science
Citation: Sapre T, Miller HL, Schwartz A, Ketcheson LR, Price A, Winkelseth K, Barcelona JM, Zernicke RF and Hasson RE (2025) Enhancing home-based physical activity for neurodivergent children: adapting the InPACT at Home program with AI and universal design. Front. Physiol. 15:1496114. doi: 10.3389/fphys.2024.1496114
Received: 13 September 2024; Accepted: 13 December 2024;
Published: 07 January 2025.
Edited by:
Hassane Zouhal, University of Rennes 2, FranceReviewed by:
Akshata R. Naik, Oakland University, United StatesJose Manuel Salum Tome, Temuco Catholic University, Chile
Copyright © 2025 Sapre, Miller, Schwartz, Ketcheson, Price, Winkelseth, Barcelona, Zernicke and Hasson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rebecca E. Hasson, aGFzc29uckB1bWljaC5lZHU=