 Rafaella Mendes Zambetta1*
Rafaella Mendes Zambetta1* Étore De Favari Signini1
Étore De Favari Signini1 Gabriela Nagai Ocamoto1,2
Gabriela Nagai Ocamoto1,2 Aparecida Maria Catai1
Aparecida Maria Catai1 Nicoly Ribeiro Uliam1Emiliano Santarnecchi3
Nicoly Ribeiro Uliam1Emiliano Santarnecchi3 Thiago Luiz Russo1*
Thiago Luiz Russo1*- 1Physical Therapy Department, Federal University of São Carlos, UFSCar, São Carlos, SP, Brazil
- 2Brain4care Inc., São Carlos, SP, Brazil
- 3Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States
Background: The microgravity environment has a direct impact on the cardiovascular system due to the fluid shift and weightlessness that results in cardiac dysfunction, vascular remodeling, and altered Cardiovascular autonomic modulation (CAM), deconditioning and poor performance on space activities, ultimately endangering the health of astronauts.
Objective: This study aimed to identify the acute and chronic effects of microgravity and Earth analogues on cardiovascular anatomy and function and CAM.
Methods: CINAHL, Cochrane Library, Scopus, Science Direct, PubMed, and Web of Science databases were searched. Outcomes were grouped into cardiovascular anatomic, functional, and autonomic alterations, and vascular remodeling. Studies were categorized as Spaceflight (SF), Chronic Simulation (CS), or Acute Simulation (AS) based on the weightlessness conditions. Meta-analysis was performed for the most frequent outcomes. Weightlessness and control groups were compared.
Results: 62 articles were included with a total of 963 participants involved. The meta-analysis showed that heart rate increased in SF [Mean difference (MD) = 3.44; p = 0.01] and in CS (MD = 4.98; p < 0.0001), whereas cardiac output and stroke volume decreased in CS (MD = −0.49; p = 0.03; and MD = −12.95; p < 0.0001, respectively), and systolic arterial pressure decreased in AS (MD = -5.20; p = 0.03). According to the qualitative synthesis, jugular vein cross-sectional area (CSA) and volume were greater in all conditions, and SF had increased carotid artery CSA. Heart rate variability and baroreflex sensitivity, in general, decreased in SF and CS, whereas both increased in AS.
Conclusion: This review indicates that weightlessness impairs the health of astronauts during and after spaceflight, similarly to the effects of aging and immobility, potentially increasing the risk of cardiovascular diseases.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42020215515.
Background
Interplanetary travel has become a significant objective for humanity, but it presents an enormous challenge: protecting the human body. Astronauts are exposed to several stressful situations, including cosmic radiation, sleep deprivation, low levels of physical activity, and microgravity (Hughson et al., 2018). The human body, especially the cardiovascular system, relies on the Earth’s gravity for proper function. Microgravity exposure leads to substantial changes in this system, which can endure for months after astronauts return to the ground (Demontis et al., 2017; Hughson et al., 2018).
Spaceflight experiments are rare and costly; hence, investigators seek to comprehend the impacts of microgravity on the cardiovascular system adaptation by implementing ground models including head-down tilt bed rest and immersion (Oluwafemi and Neduncheran, 2022). On Earth, there is a hydrostatic gradient, which is implicated in fluid pressures according to gravity. For example, the pressure is higher in the lower limbs than in the intracranial cavity. The lack of gravity in space leads to a fluid shift in the hydrostatic gradient, resulting in a uniform pressure of fluid throughout the body, which causes fluids to move upwards (Demontis et al., 2017; Hughson et al., 2018).
Astronauts may experience symptoms associated with the fluid shift, such as puffy face, swollen jugular veins, heart chamber distension, headaches and head “stuffing,” flu-like symptoms, and bird legs (thinner lower limbs), due to a reduction of around 10% in the blood volume of the lower limbs (Norsk, 2020). The literature suggests that long-duration space missions lead to an increase in venous return and cardiac preload (Fortrat et al., 2017), resulting in an increase in cardiac output (Norsk et al., 2015; Hughson et al., 2016; Marshall-Goebel et al., 2019). Cardiovascular dynamics changes may contribute to cardiac atrophy, as a cardiac muscle adaptation (Aubert et al., 2005; Shen and Frishman, 2019). In this sense, microgravity effects in heart rate (HR), blood pressure (BP) and stroke volume (SV) responses are still discussed. Some authors suggest that HR and SV tend to increase (Norsk et al., 2015; Mulavara et al., 2018; Marshall-Goebel et al., 2019; Wood et al., 2019), while systolic arterial pressure (SAP) decreases (Hughson et al., 2016; Fu et al., 2019), as a potential consequence of cardiac adaptation.
Arterial morphology and function can also be modified by microgravity, especially in the intracranial cavity (Arbeille et al., 2016; Lee et al., 2020). The mechanical stress in these arteries causes an enlargement of the artery circumference and thickness of tunica intima and media (Kotovskaya and Fomina, 2010; Grigoriev et al., 2011; Arbeille et al., 2017a). Additionally, weightlessness causes plasmatic hypovolemia and dehydration, leading to a compensatory increase in the sympathetic component to maintain stable cardiac output (Di Rienzo et al., 2008; Jimenez et al., 2012). Chronically, peripheral baroreceptors tend to accommodate, impairing baroreflex sensitivity (BRS) (Di Rienzo et al., 2008). Studies propose that the sympathetic component of Cardiovascular autonomic modulation (CAM) is predominant in both spaceflights and Earth simulation experiments, with reduction of heart rate variability (HRV) and baroreflex sensitivity (BRS) (Verheyden et al., 1985; Arzeno et al., 2013; Xu et al., 2013; Rusanov et al., 2020). On the contrary, Vandeput and colleagues (Vandeput et al., 2013) documented a reduction in both the sympathetic and parasympathetic components of HRV following prolonged spaceflight, indicating distinct delayed adaptation to microgravity. As a result, the available evidence on CAM regulation is not entirely conclusive.
Finally, the aforementioned cardiovascular alterations lead to orthostatic intolerance, resulting in inadequate cerebral perfusion and deconditioning in astronauts (Shen and Frishman, 2019; Gallo et al., 2020). This situation raises concern in circumstances that require precise performance, like in exploratory missions, emergencies, or extravehicular activities. Moreover, astronauts may experience health implications, including visual impairment and intracranial pressure syndrome (Platts et al., 2014), an increased risk of arrhythmia and cardiovascular diseases, even upon returning to Earth (Gallo et al., 2020). Therefore, this meta-analysis and systematic review seeks to identify the acute and chronic effects of microgravity (or corresponding analog models on Earth) on the anatomy and function of the cardiovascular system.
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Page et al., 2021). To systematize and simplify the search and data collection process, we utilized the State of the Art through Systematic Review (StArt) tool (available at http://lapes.dc.ufscar.br/tools/start_tool). Furthermore, we registered this systematic review in the International Prospective Register of Systematic Reviews (PROSPERO) with the identifier CRD42020215515.
Data sources and search strategy
Literature searches were conducted utilizing the subsequent databases: CINAHL with Full Text (EBSCO), Cochrane Library, Scopus, Science Direct, PubMed (via National Library of Medicine) and Web of Science (Thomson Scientific/ISI Web Services). MeSH terms were utilized to identify relevant keywords, and the resulting string of terms was subsequently employed. During the searched period from January 2013 to 2023, database searches were conducted for publications in English language containing the following keywords: “humans'' OR “astronauts” AND “weightlessness” OR “weightlessness Simulation” OR “space flight” AND “cardiovascular system” OR “hemodynamics” OR “fluid shifts.” An update was made in October 2023. Supplementary Table S1 illustrates all the applied filters, combinations, and searches.
Eligibility criteria
The main question of this study was based on the PICOS structure (P: population; I: intervention; C: comparison; O: outcomes; and S: study design). The subjects of interest were astronauts and healthy adult humans. Three weightlessness simulation experiments—Head-Down Tilt (HDT), Dry Immersion (DI) and Parabolic Flight (PF)—were selected due to the presence of fluid shift in each model, albeit at varying magnitudes. They are suitable models for investigating the physiological alterations resulting from weightlessness, particularly concerning the cardiovascular system (Norsk et al., 2015; Ploutz-Snyder, 2016). Comparisons using control groups or pre-post interventions were assessed. The cardiovascular outcomes considered were grouped into functional or anatomical modifications. Only quantitative studies were accepted.
Accordingly, the inclusion criteria were healthy adult humans and weightlessness effects on the cardiovascular system. We excluded studies with animal models, children, elderly population, and diseases; studies focusing solely in hypergravity or hypogravity, such as Martian and lunar gravity, and not microgravity; and qualitative studies, narrative reviews, meta-analysis, and systematic reviews, gray literature (e.g., governmental reports, theses, etc.), theoretical and opinion articles, conference abstracts, personal blogs, and social media were excluded.
Selection process
After removing duplicates, two reviewers (RMZ and EFS) independently selected articles that met the eligibility criteria based on their titles and abstracts. The selected articles were then retrieved for full-text reading to confirm that they met all inclusion criteria. Any disagreements between the two reviewers were resolved by consulting a third reviewer (GNO) to determine whether the study was eligible.
Data analysis
Data extraction and synthesis
We divided the studies into three categories: spaceflight (SF), chronic simulations (CS), and acute simulations (AS) (Tables 1–3). No specific timeframe was defined for spaceflight and weightlessness simulations. Studies with a duration exceeding 24 h were classified as CS due to the involvement of later blood pressure regulation mechanisms, including renal ones (Hall and Guyton, 2011). Studies with a duration of less than 24 h (<24 h) were categorized as AS.
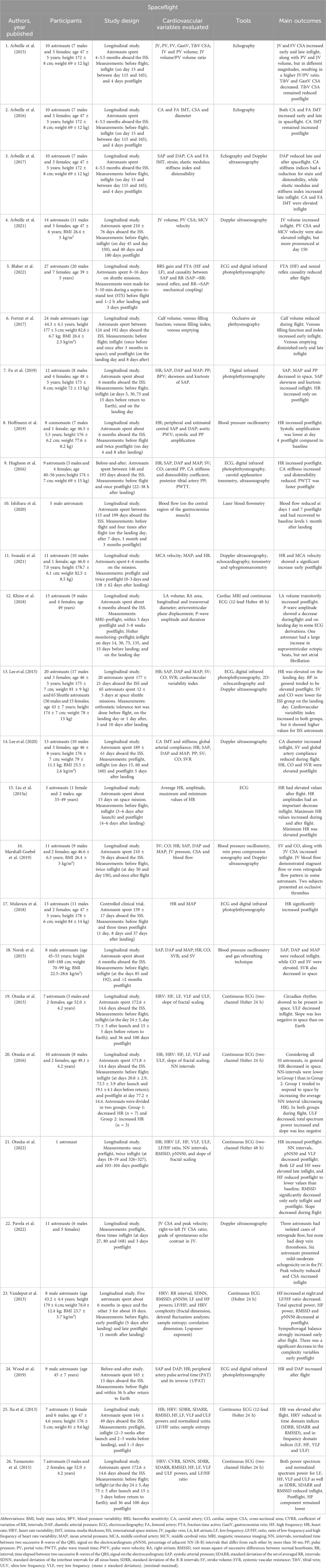
Table 1. Summary of main findings in spaceflight studies.

Table 2. Summary of main findings in chronic simulation studies.
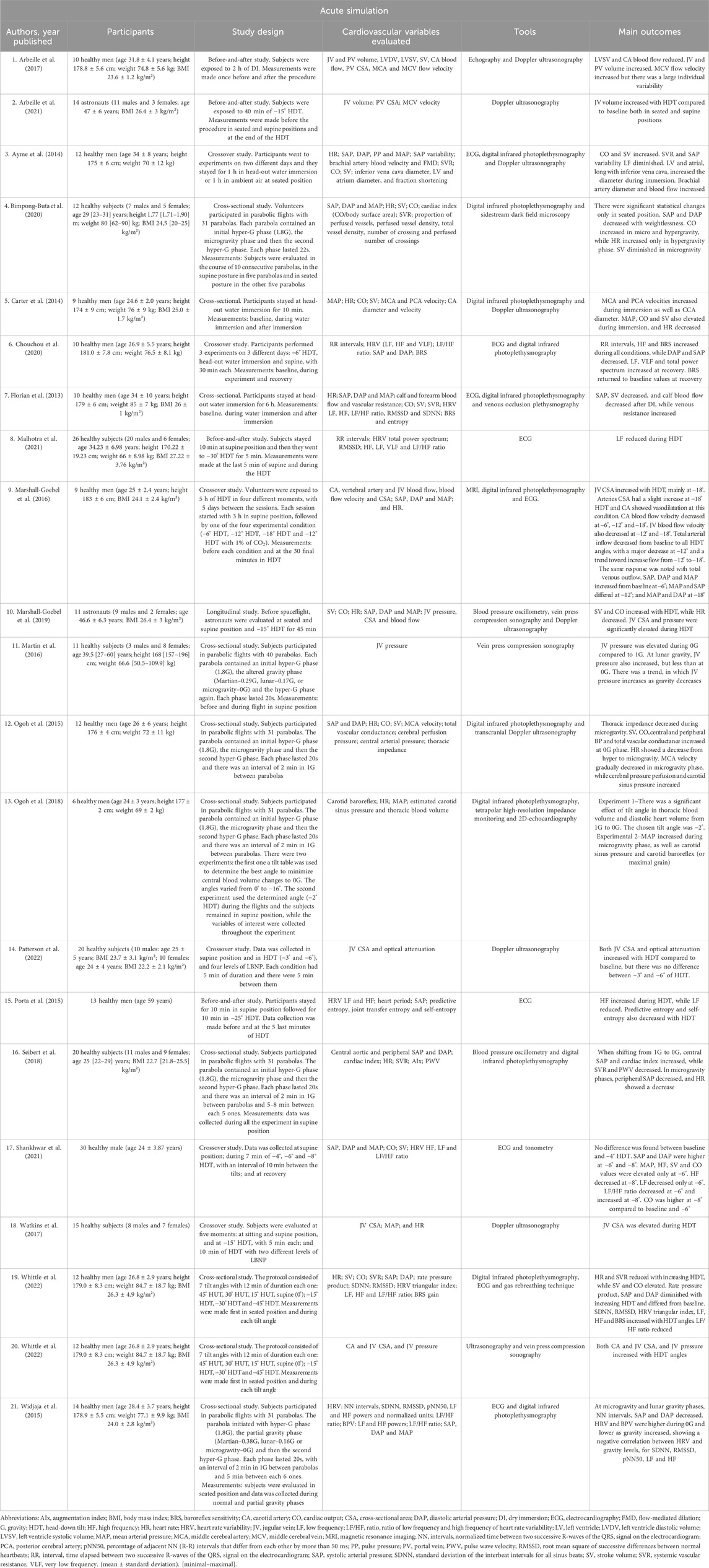
Table 3. Summary of main findings in acute simulation studies.
The outcomes were classified into three categories: anatomical, functional, and CAM outcomes, depending on the assessment method used. Anatomical outcomes were measured through imaging tests like echography, ultrasonography, and magnetic resonance imaging (MRI). Functional outcomes consisted of measures of cardiac function and blood flow, obtained through techniques like photoplethysmography, doppler ultrasonography, blood pressure oscillometry, and electrocardiogram (ECG), when used for measuring HR. When the ECG and photoplethysmography data allowed the derivation of the HRV and BRS, respectively, they were categorized as CAM.
Meta-analysis
Meta-analysis was performed with the included articles using the Cochrane Collaboration software (Review Manager 5.4.1) (Ryan and Cochrane Consumers and Communication Review Group, 2016). In order to have a robust meta-analysis, the outcome had to be observed in at least three studies for each condition (SF, CS and AS) to be considered for the meta-analysis (Higgins et al., 2011). Outcomes that did not appear in all types of studies, were not used for meta-analysis, once the comparison is fragile. Means and standard deviations were extracted from studies. Standard deviation was computed for studies where data was presented in standard error or interquartile intervals (Ried, 2006; Higgins et al., 2011; Ryan and Cochrane Consumers and Communication Review Group, 2016).
Comparisons were conducted between the weightlessness group and the control group (not exposed to weightlessness). In studies where no control group was presented, the baseline measurements of the participants were considered as the control. For meta-analysis, the final measurement during weightlessness was used. In studies without evaluations during the intervention, values immediately after the intervention were used. Data extraction was standardized in the supine position. Data collected from the positioning of seating or functional testing were not included. The random effects model was used for analysis due to the methodological heterogeneity in the studies. Mean difference (MD) and a 95% confidence interval were calculated to measure effects.
Results
A total of 749 studies were identified, with 722 articles retrieved from the databases, and a further 27 articles from other sources, mainly through a review of the references used in the included articles from the databases. After the database search update, two more studies were included. Sixty-two articles were included in this review (Figure 1), in which 58 used exclusively one type of weightlessness model, and other 4 studies utilized both SF and CS or SF and AS. A summary table was created as a qualitative synthesis for each type of study, presenting the main findings of all the 62 included studies. For the quantitative synthesis, the meta-analysis, only 34 of these studies were included.
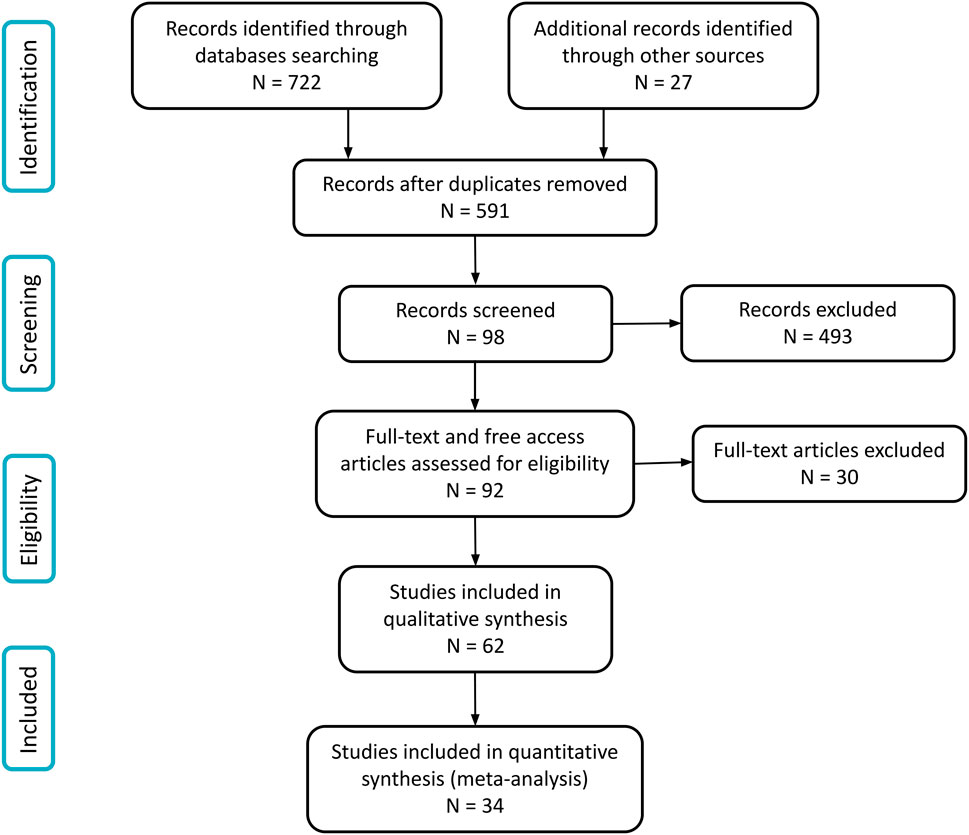
Figure 1. Study flow diagram.
Twenty-six studies were included in the spaceflight condition, with an average duration of 163.7 days (about 5 and a half months) and ranging from 12 to 327 days (about 10 and a half months). Nineteen studies were considered as CS. Among these, 16 studies used HDT, which 15 considered −6° of inclination, and one study was conducted with −12° HDT. Only three studies used DI. The average duration of CS studies was 37.8 days (ranging between one to 70 days). For AS, 21 studies were included. Of these studies, six employed parabolic flight, with variations in the number of parabolas used; each parabola featured a mean microgravity phase lasting 20 s. In eleven studies, HDT was utilized, with a range of 5 min–6 h of exposure. DI was utilized only in one study, while an alternative DI approach, referred to as “head-out water immersion” (WI), was used in three other studies, with exposure periods ranging from 10 min to 6 h.
All the included articles and their main findings of studies are summarized and presented on Tables 1–3. It was considered only the weightlessness group without any countermeasure or other intervention.
Population
In this review, a total of 963 participants were enrolled across all three conditions of weightlessness investigated. This value was calculated considering the sample size (n) of each study; therefore, it is possible that there are overlapping participants among the studies. Of the participants, 346 were involved in the SF studies. The sample size ranged from one to 85 subjects, with a mean of 13 (10 male and 3 female) astronauts per study. The CS studies involved 329 participants, with a varying sample size ranging from 6 to 63 individuals and a mean of 17 (15 male and 2 female) subjects per study. Two hundred and eighty-eight participants took part in the AS studies, with the sample size varying from 6 to 30 per study, and a mean of 14 participants (11 males and 3 females) per study. Table 4 displays the demographic characteristics of the participants.
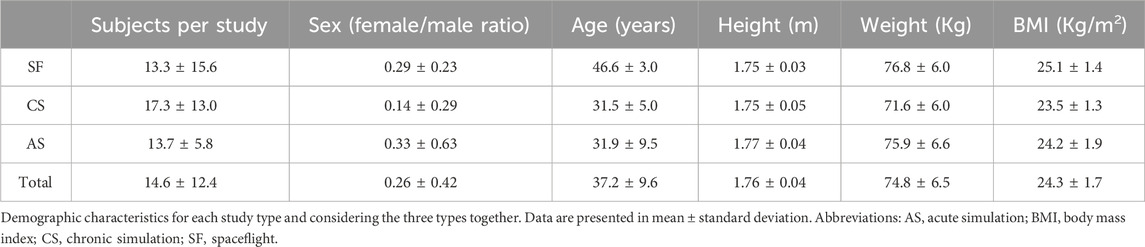
Table 4. Participants’ demographic characterization.
Cardiac outcomes
Cardiac function
Heart rate (HR): HR had a significant increase during spaceflight (Xu et al., 2013; Liu Z. et al., 2015; Lee et al., 2015; Hughson et al., 2016; Mulavara et al., 2018; Fu et al., 2019; Hoffmann et al., 2019; Wood et al., 2019; Lee et al., 2020; Iwasaki et al., 2021; Otsuka et al., 2022), and right after CS (Adami et al., 2013; Liu J. et al., 2015; Palombo et al., 2015; Westby et al., 2016a; Ogoh et al., 2017; Mulavara et al., 2018; Martín-Yebra et al., 2019; Ogoh et al., 2020; Möstl et al., 2021). Conversely, some studies with AS showed a decrease in HR (Carter et al., 2014; Ogoh et al., 2015; Seibert et al., 2018; Marshall-Goebel et al., 2019; Whittle et al., 2022).
Blood pressure (BP): during SF, two studies showed reduction of systolic arterial pressure (SAP) (Norsk et al., 2015; Fu et al., 2019), diastolic arterial pressure (DAP) (Norsk et al., 2015; Arbeille et al., 2017a) and mean arterial pressure (MAP) (Norsk et al., 2015; Fu et al., 2019), one reported an increase in BP in general (Lee et al., 2015) and also only study reported an increase in DAP (Wood et al., 2019), and the others remained unchanged (Hughson et al., 2016; Mulavara et al., 2018; Hoffmann et al., 2019; Marshall-Goebel et al., 2019; Lee et al., 2020; Iwasaki et al., 2021). Regarding CS models, SAP decreased in two studies (Arzeno et al., 2013; Linnarsson et al., 2015) and increased in other two (Ogoh et al., 2017; Robin et al., 2023). DAP was diminished in one study (Arzeno et al., 2013) and elevated in other two as well (Möstl et al., 2021; Robin et al., 2023). MAP also decreased in one study (Adami et al., 2013) and increased in another one (Liu J. et al., 2015). In AS, SAP, DAP and MAP were reduced in six studies (Florian et al., 2013; Widjaja et al., 2015; Seibert et al., 2018; Bimpong-Buta et al., 2020; Chouchou et al., 2020; Whittle et al., 2022), while five studies reported a significant increase (Carter et al., 2014; Ogoh et al., 2015; Marshall-Goebel et al., 2016; Ogoh et al., 2018; Shankhwar et al., 2021). Pulse pressure reduced in one study with SF (Fu et al., 2019) and in two studies with CS (Palombo et al., 2015; Möstl et al., 2021). In addition, two studies found higher isovolumetric contraction (Möstl et al., 2021) and relaxation time (Westby et al., 2016a), suggesting central systolic and diastolic dysfunction.
Stroke volume (SV): Five studies evaluated SV in SF (Lee et al., 2015; Norsk et al., 2015; Hughson et al., 2016; Marshall-Goebel et al., 2019; Lee et al., 2020). Two studies reported an increase in SV (Norsk et al., 2015; Marshall-Goebel et al., 2019), while the other two studies reported a reduction in SV (Lee et al., 2015; Lee et al., 2020). In CS studies, SV was diminished in all studies with this outcome (Adami et al., 2013; Palombo et al., 2015; Westby et al., 2016a; Möstl et al., 2021), while in AS, six studies reported an increase (Ayme et al., 2014; Carter et al., 2014; Ogoh et al., 2015; Marshall-Goebel et al., 2019; Shankhwar et al., 2021; Whittle et al., 2022), and two presented lower SV values compared to baseline (Florian et al., 2013; Bimpong-Buta et al., 2020).
Cardiac output (CO): CO increased in three of the five SF studies (Norsk et al., 2015; Marshall-Goebel et al., 2019; Lee et al., 2020) and decreased in only one study (Lee et al., 2015). CO was markedly decreased in two studies using CS (Adami et al., 2013; Ogoh et al., 2017) and was elevated in seven studies with AS (Ayme et al., 2014; Carter et al., 2014; Ogoh et al., 2015; Marshall-Goebel et al., 2019; Bimpong-Buta et al., 2020; Shankhwar et al., 2021; Whittle et al., 2022).
Cardiac dimension and morphology
One study with AS identified increments of the left ventricle end-diastolic diameter and atrium diameter (Ayme et al., 2014). Studies with CS described a decrease of left ventricle mass and blood volume, both in systole and diastole (Westby et al., 2016a; Orter et al., 2022).
Cardiac electrophysiology
Two CS studies identified alterations in the cardiac electrophysiology, including a reduction in T-wave area, an increase in apex and amplitude, and a decrease in QRS-T angle (Caiani et al., 2013; Martín-Yebra et al., 2019). Another study, conducted with SF, investigated atrial alterations and found increased left atrial blood volume post-flight (Khine et al., 2018). Additionally, some derivations of the electrocardiogram (ECG) showed a decrease in P-wave amplitude (Khine et al., 2018). One astronaut had a significant increase in supraventricular ectopic beats but no evidence of atrial fibrillation (Khine et al., 2018).
Vascular outcomes
Vascular hemodynamics and morphology
Middle cerebral artery (MCA) velocity increased in one study with SF (Iwasaki et al., 2021) and in one with AS (Carter et al., 2014). In addition, in AS, one study had a decrease in MCA velocity (Ogoh et al., 2015). Both carotid artery and femoral artery cross-sectional area (CSA) and intima-media thickness (IMT) increased in space (Arbeille et al., 2016; Arbeille et al., 2017a). In AS, two studies identified an increase in carotid artery CSA as well (Whittle and Diaz-Artiles, 1985; Marshall-Goebel et al., 2016), while one CS study found an increase in carotid artery diameter (Ogoh et al., 2017). Jugular vein CSA and volume were higher in all the three conditions (Whittle and Diaz-Artiles, 1985; Arbeille et al., 2015; Marshall-Goebel et al., 2016; Arbeille et al., 2017b; Watkins et al., 2017; Marshall-Goebel et al., 2018; Marshall-Goebel et al., 2019; Arbeille et al., 2021; Patterson et al., 2022; Pavela et al., 2022). Systemic vascular resistance increased in one study in space (Lee et al., 2020) and decreased in other studies with SF, CS and AS (Adami et al., 2013; Ayme et al., 2014; Norsk et al., 2015; Seibert et al., 2018; Whittle et al., 2022). Additionally, aortic pulse wave velocity decreased in AS (Seibert et al., 2018), while no differences were observed in SF and CS (Palombo et al., 2015; Hoffmann et al., 2019; Möstl et al., 2021).
Cardiovascular autonomic modulation (CAM) outcomes
CAM in frequency domain
The cardiovascular autonomic modulation was influenced by microgravity. During SF, the low frequency (LF) of the heart rate variability (HRV) reduced in two of six studies (Xu et al., 2013; Yamamoto et al., 2015), and increased in one (Otsuka et al., 2022), while in the other three studies there was no difference (Vandeput et al., 2013; Otsuka et al., 2015; Otsuka et al., 2016). For high frequency (HF) of HRV, four studies showed a reduction (Vandeput et al., 2013; Xu et al., 2013; Yamamoto et al., 2015; Otsuka et al., 2022), and two had no difference (Otsuka et al., 2015; Otsuka et al., 2016). The LF/HF ratio was reduced in one study (Vandeput et al., 2013). In CS, two studies showed a reduction of the HF (Arzeno et al., 2013; Liang et al., 2014) and one of the LF (Liang et al., 2014), and LF increased in one study (Arzeno et al., 2013). In AS, five studies showed an increase in the HF band of HRV (Porta et al., 2015; Widjaja et al., 2015; Chouchou et al., 2020; Shankhwar et al., 2021; Whittle et al., 2022). LF had an increase in three studies (Widjaja et al., 2015; Chouchou et al., 2020; Whittle et al., 2022) and a decrease in other three studies (Porta et al., 2015; Malhotra et al., 2021; Shankhwar et al., 2021). The LF/HF ratio was diminished in two studies (Shankhwar et al., 2021; Whittle et al., 2022).
CAM in time domain
HRV in time domain in space had decrease in the following variables: pNN50 (percentage of adjacent NN (R-R) intervals that differ from each other by more than 50 ms) (Vandeput et al., 2013; Otsuka et al., 2022), SDRR (standard deviation of the R-R intervals) (Xu et al., 2013; Yamamoto et al., 2015), SDARR (standard deviation of the set of averaged RR intervals) (Xu et al., 2013; Yamamoto et al., 2015), and RMSSD (root mean square of successive differences between normal heartbeats) (Vandeput et al., 2013; Xu et al., 2013; Yamamoto et al., 2015; Otsuka et al., 2022). For CS studies, pNN50 was reduced (Rusanov et al., 2020), and during AS, pNN50, SDNN and RMSSD were increased (Widjaja et al., 2015; Whittle et al., 2022).
Baroreflex sensitivity
Blood pressure variability did not change during SF and CS (Arzeno et al., 2013; Fu et al., 2019) but increased during AS (Widjaja et al., 2015). Baroreflex sensitivity decreased in CS (Arzeno et al., 2013; Liu J. et al., 2015) but increased in AS in two studies (Chouchou et al., 2020; Whittle et al., 2022). Most studies showed no changes in RR intervals (Caiani et al., 2013; Vandeput et al., 2013; Liu J. et al., 2015; Rusanov et al., 2020; Malhotra et al., 2021), but one CS study identified a reduction (Arzeno et al., 2013) and another AS study showed an increase (Chouchou et al., 2020).
Meta-analysis
Meta-analysis was conducted for the following variables: HR, SAP, CO and SV. The results of SF and CS are presented both separately and grouped due to their chronic exposure characteristics. Nevertheless, AS data was presented separately.
Eleven studies with HR in SF were included in meta-analysis (Figure 2). Heterogeneity was I2 = 56%, and it presented a significant effect size (131 subjects, MD = 3.44, 95% CI 0.82 to 6.06, Z = 2.58, p = .010). For CS, nine studies with HR were included. One of them was repeated three times in the graphic, once it had three groups with different duration of weightlessness simulation. Heterogeneity was I2 = 11%, and it showed a significant effect size (173 subjects, MD = 4.98, 95% CI 2.54 to 7.41, Z = 4.01, p < .0001). When HR was grouped for SF and CS meta-analysis showed a significant increase (effect size: MD = 4.02, 95% CI 2.17 to 5.86, Z = 4.26, p < .0001), with low heterogeneity (I2 = 42%). Concerning the HR in AS studies, nine studies were included, and one was repeated three times as well as in the CS group. Heterogeneity was low (I2 = 27%) with no effect size (133 subjects, MD = −1.56, 95% CI −4.35 to 1.23, Z = 1.10, p = .27).
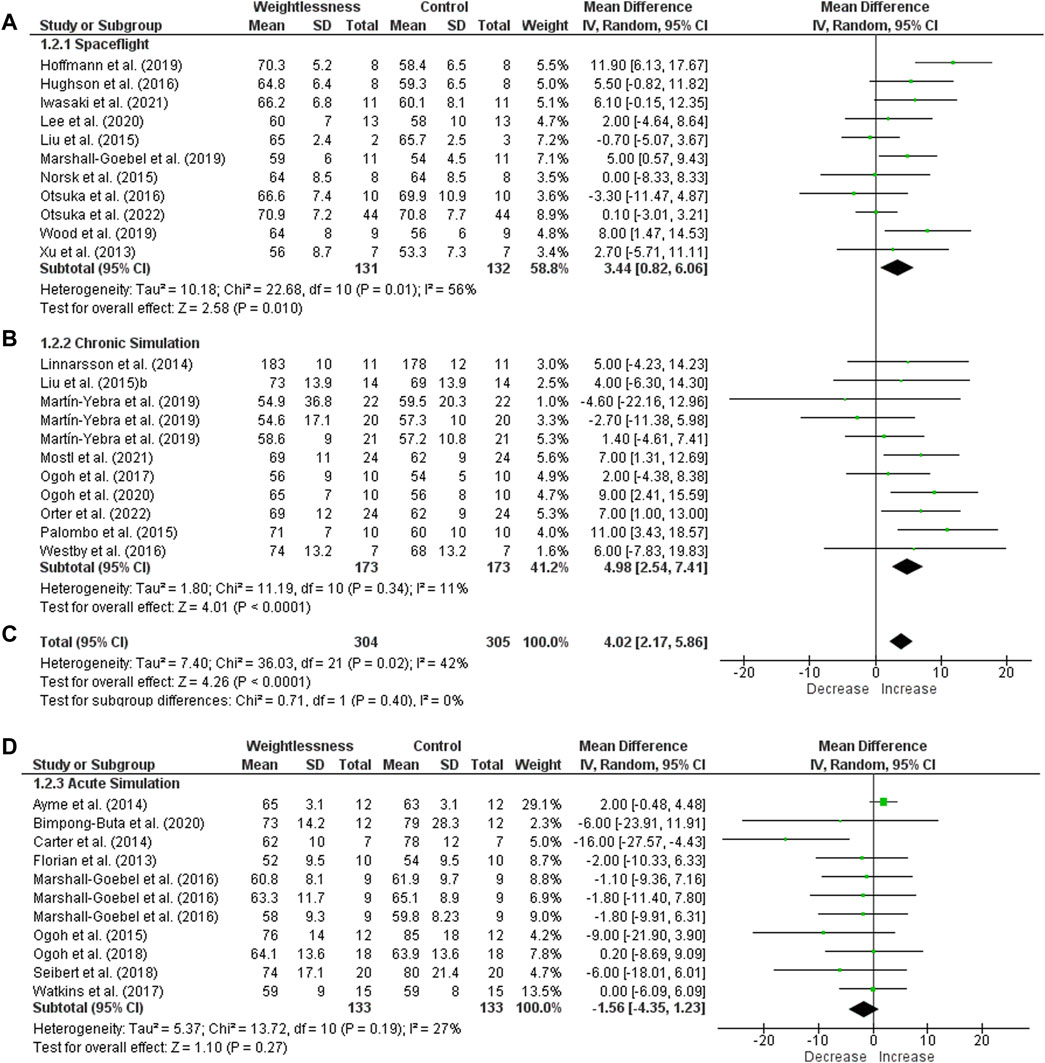
Figure 2. Forest plot of Heart Rate. Effect sizes after weightlessness exposure compared to control group or baseline. (A) Spaceflight; (B) Chronic Simulation; (C) Total effect size of the Spaceflight and Chronic Simulation; (D) Acute Simulation. The left side of the forest plot represents a decrease in the value of the outcome. The right side of the forest plot represents an increase in the value of the outcome.
Considering SF, seven studies investigated SAP and were included for meta-analysis (Figure 3). Heterogeneity was 53%, and it had no significant effect size (65 subjects, MD = 1.39, 95% CI −3.73 to 6.51, Z = 0.53, p = .59). About CS studies, five were included, and SAP also had no significant difference (78 subjects, MD = −0.23, 95% CI −3.59 to 3.12, Z = 0.14, p = .89), with heterogeneity of I2 = 0%. When both SF and CS were grouped, heterogeneity was I2 = 25% and had no significant effect size (143 subjects, MD = 0.31, 95% CI −2.51 to 3.14, Z = 0.22, p = .83). Nine of AS studies were considered, and they showed a significant decrease (effect size: MD = −5.29, 95% CI −10.20 to −0.39, Z = 2.11, p = .03), but with high heterogeneity (I2 = 81%).
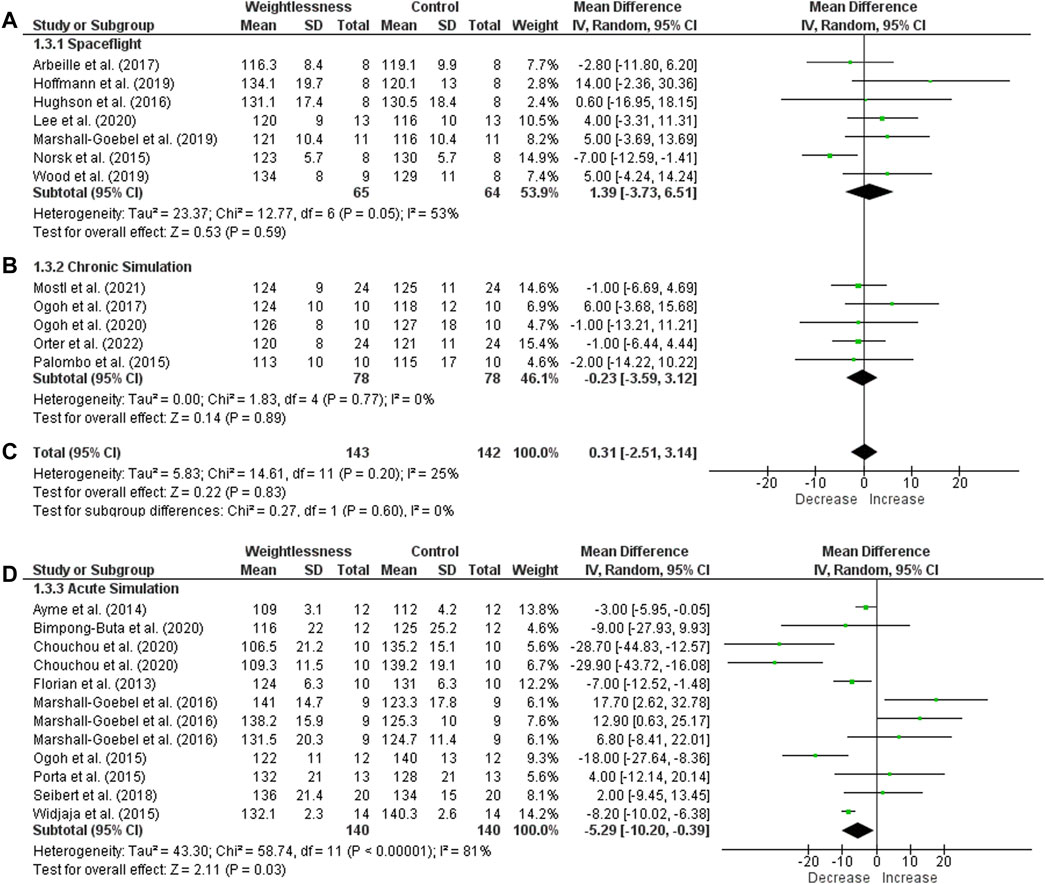
Figure 3. Forest plot of Systolic Arterial Pressure. Effect sizes after weightlessness exposure compared to control group or baseline. (A) Spaceflight; (B) Chronic Simulation; (C) Total effect size of the Spaceflight and Chronic Simulation; (D) Acute Simulation. The left side of the forest plot represents a decrease in the value of the outcome. The right side of the forest plot represents an increase in the value of the outcome.
Regarding CO in SF, four studies were included and there was no statistical significance (heterogeneity of I2 = 74%, and effect size of 40 subjects, MD = 0.91, 95% CI −0.13 to 1.94, Z = 1.72, p = .09). There was a significant decrease of CO in CS, with 3 studies included (I2 = 0% and effect size: MD = −0.49, 95% CI -0.94 to −0.04, Z = 2.15, p = .03). The total heterogeneity of the groups SF and CS was high (I2 = 79%) with no significant effect size (81 subjects, MD = 0.22, 95% CI −0.56 to 0.99, Z = 0.54, p = .59), as seen in Figure 4. No difference was found for AS studies (heterogeneity of I2 = 0% and no significant effect size of 41 subjects, MD = 0.06, 95% CI −0.34 to 0.45, Z = 0.28, p = .78), with four studies included.
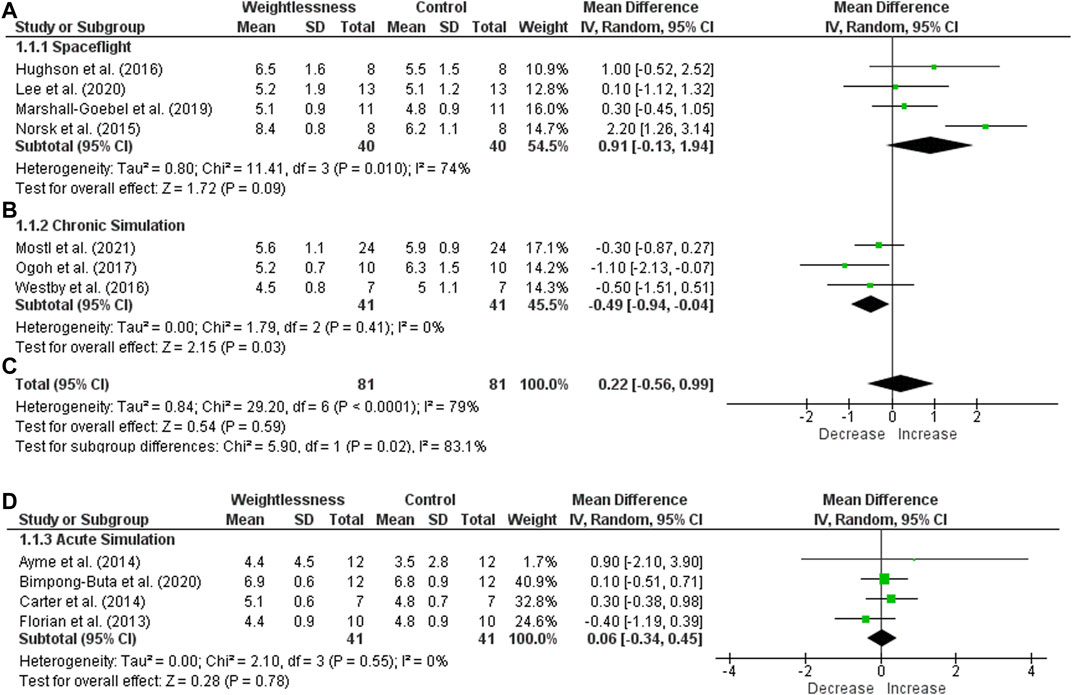
Figure 4. Forest plot of Cardiac Output. Effect sizes after weightlessness exposure compared to control group or baseline. (A) Spaceflight; (B) Chronic Simulation; (C) Total effect size of the Spaceflight and Chronic Simulation; (D) Acute Simulation. The left side of the forest plot represents a decrease in the value of the outcome. The right side of the forest plot represents an increase in the value of the outcome.
Finally, SV was unchanged in space (heterogeneity of I2 = 0% and effect size of 32 subjects, MD = −4.14, 95% CI −11.14 to 2.86, Z = 1.16, p = .25) (Figure 5). SV was significantly reduced in CS (heterogeneity of I2 = 0% and significant effect size of 41 subjects, MD = −12.95, 95% CI −18.77 to −7.12, Z = 4.36, p < .0001). For the two groups (SF and CS), heterogeneity was I2 = 0% and there was significant effect size, indicating a decrease of SV (73 subjects, MD = −9.35, 95% CI −13.82 to −4.87, Z = 4.09, p < .0001). About AS studies, four of ten studies were included in meta-analysis, and SV had a significant increase (heterogeneity of I2 = 69% and effect size of 39 subjects, MD = 11.21, 95% CI 0.63 to 21.78, Z = 2.08, p = .04).
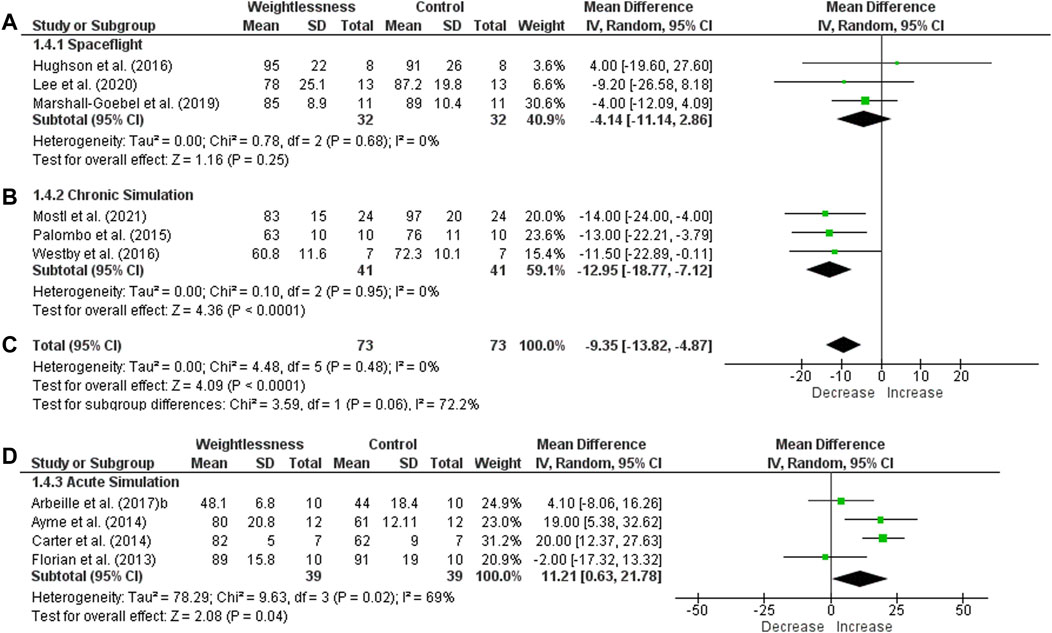
Figure 5. Forest plot of Stroke Volume. Effect sizes after weightlessness exposure compared to control group or baseline. (A) Spaceflight; (B) Chronic Simulation; (C) Total effect size of the Spaceflight and Chronic Simulation; (D) Acute Simulation. The left side of the forest plot represents a decrease in the value of the outcome. The right side of the forest plot represents an increase in the value of the outcome.
Discussion
This study evaluated the impact of microgravity on the cardiovascular system of healthy subjects, specifically focusing on structural, physiological, and functional properties. The study conducted a systematic review of existing literature and a meta-analysis of both acute and chronic effects of weightlessness on the cardiovascular system, providing new evidence to support medical research in space. It was observed that weightlessness has an impact on the cardiovascular system, causing changes to cardiac function, vascular health, and cardiovascular autonomic modulation.
Advantages and disadvantages of each model of microgravity
Considering the impact of weightlessness on the cardiovascular system, there were some specificities inherent for each study condition, with corresponding strengths and limitations for data interpretation. The main advantage of SF research lies in real environment, which promotes trustworthy findings about microgravity effects. However, several aspects must be considered before data generalization. For instance, the small sample size of Space Shuttle and Space Station missions due to their expensive nature and the need for a specific and well-trained crew, mostly consisting of male subjects, means that the results are highly influenced by inter-individual variability. Additionally, astronauts are subject to various factors associated with spaceflight, including exposure to cosmic radiation, confinement, sleep deprivation, altered nutrition, and high concentrations of CO2 on the spacecraft. Equally significant, astronauts often partake in multiple studies, potentially impacting the outcomes under investigation (Lee et al., 2015; Hughson et al., 2016; Fu et al., 2019).
Interestingly, chronic models that simulate spaceflight (DI and HDT) demonstrate similar outcomes to those seen in long-duration spaceflights, as observed in the meta-analysis. These models offer certain advantages, such as a controlled environment that allows for a concentrated focus on the primary outcomes with minimal interference from external factors, thereby enabling testing of countermeasures to ensure their effectiveness in space missions (Hargens and Vico, 1985). It is impossible to fully eliminate the effects of gravitational force, making the results of experiments conducted in space less reliable and reproducible. Additionally, chronic simulations share certain drawbacks with spaceflight studies, including a small sample size and a predominance of male volunteers. The literature reports high costs associated with long protocols, including those lasting 70 days in HDT (Shen and Frishman, 2019). This kind of study typically requires numerous specialized professionals to guarantee safety measures, along with multiple concurrent research experiments that involve enrolling the same individuals (Shen and Frishman, 2019).
Acute models of microgravity simulation allow for more intense and focused observation of effects while avoiding the accommodation effect. Though exposure time is brief in comparison to actual spaceflight, acute effects are valuable for representing the initial phase of flight (Shen and Frishman, 2019). DI and HDT acute simulations offer practical and low-cost advantages. It is important to note that the Earth’s gravitational influence, akin to CS, is present in both types of models. It has the potential to affect the outcomes (Ploutz-Snyder, 2016). Parabolic flight enables a real microgravity experience on Earth. However, due to the brief duration of the parabolic phase (typically lasting only 20 s), conducting cardiovascular assessments can be challenging. Other factors that may impact microgravity responses include the hypergravity phase, small sample sizes, and the higher likelihood of motion sickness among participants, for which medication may be necessary (Shen and Frishman, 2019).
Cardiovascular impairments and astronaut physiology
During SF, astronauts suffer from generalized deconditioning, which impacts different systems such as musculoskeletal, immune, cardiovascular, vestibular systems, among others. Specifically, weightlessness can modify different aspects of the cardiovascular system, including fluid balance, renal hemodynamics, vascular adaptation, and cardiovascular autonomic neural control (Aubert et al., 2005). This review has identified cardiac remodeling, as an indicative of atrophy, decreased SV, and impaired baroreflex sensitivity as significant findings. Previous studies during Neurolab and Spacelab Missions had similar findings (Cooke et al., 1985; Perhonen et al., 1985; Levine et al., 2002; Eckberg et al., 2010). A summary of the main results is presented in Figure 6.
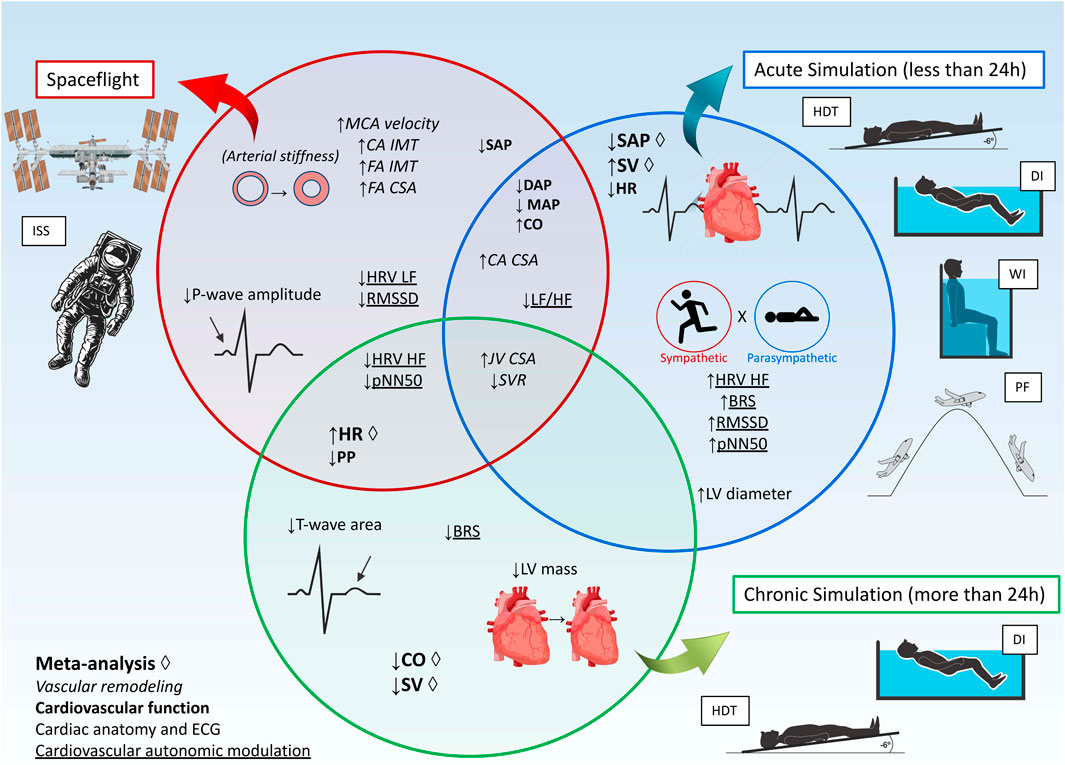
Figure 6. Summary of results. Abbreviations: BRS, baroreflex sensitivity; CA, carotid artery; CO, cardiac output; CSA, cross-sectional area; DAP, diastolic arterial pressure; DI, dry immersion; ECG, electrocardiography; FA, Femoral artery; HDT, head-down tilt; HF, high frequency; HR, heart rate; HRV, heart rate variability; IMT, Intima-media thickness; ISS, International Space Station; JV, jugular vein; LF, low frequency; LF/HF ratio, ratio of low frequency and high frequency of heart rate variability; LV, left ventricle; MAP, mean arterial pressure; MCA, middle cerebral artery; PF, Parabolic Flight; pNN50, percentage of adjacent NN (R-R) intervals that differ from each other by more than 50 ms; PP, pulse pressure; RMSSD, root mean square of successive differences between normal heartbeats; SAP, systolic arterial pressure; SV, stroke volume; SVR, systemic vascular resistance; WI, Head-out water immersion.
During the first 24 h in space, the absence of gravity results in a decrease in intrathoracic pressure due to chest expansion. Studies of European Space Agency parabolic flight campaigns (Pump et al., 1985; Videbaek and Norsk, 1985) have suggested an increase in transmural cardiac pressure, cardiac preload, and atrial stretching, that could be primarily caused by an elevation in plasma volume in the trunk (Aubert et al., 2005; Norsk, 2020). Atrial stretching results in an elevation of atrial natriuretic peptide levels. This, in conjunction with decreased blood vessel tension due to the absence of gravity, leads to vasodilation and enhanced permeability (Norsk, 2020). Moreover, based on the Frank Starling mechanism, distension of the cardiac chambers enhances the final diastolic volume, thereby increasing the SV. The present review’s meta-analysis observed a considerable rise in SV in AS, consistent with existing literature (Aubert et al., 2005; Norsk, 2020).
Increased SV is typically followed by an expected increase in CO shortly after exposure to microgravity. However, the meta-analysis displayed no changes to CO or HR, and a decrease in SAP during AS. Lower SAP values can trigger greater activation of the Renin Angiotensin Aldosterone System, which results in the reabsorption of sodium and water, and an increase in vascular resistance in arterioles as an attempt to regulate SAP (Aubert et al., 2005). Furthermore, the initial increase in plasma volume in the trunk leads to an attempt to return to baseline state through a greater process of natriuresis and diuresis (Norsk, 2020). Chronically, this process leads to dehydration (Norsk, 2020).
Extended exposure to weightlessness significantly decreases plasma volume, potentially due to systemic vascular resistance and peripheral arterial vasoconstriction (Norsk, 2020). This may prompt high venous compliance, which contributes to the maintenance of SAP reduction during prolonged weightlessness as reflected in the majority of the studies included in this review (Norsk, 2020). The reduction of blood pressure, in general, can be observed in both SF and AS, as illustrated in Figure 6. According to our meta-analysis findings, SAP tends to stabilize over time, while SV decreases after CS (the same pattern observed during SF). Furthermore, our results show a decrease in left ventricular mass and blood volume, along with systemic hypovolemia and shrinkage of the cardiac cavity. These changes may contribute to systolic and diastolic dysfunction (Caiani et al., 2013; Westby et al., 2016a; Martín-Yebra et al., 2019). Literature suggests that cardiac atrophy and deconditioning occur in both SF and CS conditions as a form of adaptation (Dorfman et al., 1985a; Dorfman et al., 1985b; Perhonen et al., 1985; Westby et al., 2016), similar to the effects of aging, sedentary behavior, and immobility (Hart, 2023; Malhan et al., 2023). Of particular concern for cardiac deconditioning is the slow process of reconditioning after return to Earth (Solbiati et al., 2020).
Electrocardiographic alterations, such as reduced P-wave amplitude and T-wave area, should not be overlooked since they can pose a potential risk to atrial fibrillation and arrhythmia (Caiani et al., 2013; Khine et al., 2018). Also, these alterations can be associated with fluid loss and hypovolemia, which may also affect cardiovascular autonomic modulation (Caiani et al., 2013; Martín-Yebra et al., 2019). Our findings are consistent with the previous literature and other studies not included in this review, which indicates a decrease in both sympathetic and parasympathetic components of HRV, however, there is a significant reduction in parasympathetic responses, resulting in a relative predominance of sympathetic activity (Cooke et al., 1985; Iwasaki et al., 2004; Norsk, 2020). Total power spectrum and BRS also seems to decrease in space (Cooke et al., 1985; Iwasaki et al., 2004), probably due to baroreceptor overload and saturation, making it difficult for the ANS to modulate HR and blood pressure (Norsk et al., 2015). The accumulation of blood volume in the trunk also increases cerebrovascular pressure and engorgement of the neck vasculature, which stimulates aortic and carotid baroreceptors, affecting their saturation levels (Shen and Frishman, 2019). Thus, BRS decreases, probably, as a consequence of the regulation failure (Shen and Frishman, 2019).
The accumulation of blood in the neck region, and consequently increase of blood vessels pressure, is particularly worrisome for middle cerebral artery, CA and JV, once it involves impaired cerebral perfusion, stiffness of cerebral arteries and increased intracranial pressure. It is interesting to note that JV CSA have the same behavior in the three conditions, as shown in Figure 6. This indicates that the accumulation of blood in the neck is present both acutely and chronically, regardless of the microgravity model used. Some astronauts even presented JV stagnant or reversed venous flow (Marshall-Goebel et al., 2019). In this case, intracranial pressure is the main cause of Spaceflight Associated Neuro-Ocular Syndrome (SANS). More than half of astronauts exhibit at least one symptom of SANS, which symptoms are the same as patients with idiopathic intracranial hypertension (Norsk et al., 2015) and could cause permanent deficits in vision (Wojcik et al., 2020).
Another important issue is orthostatic intolerance (OI), a frequent occurrence resulting from reduced cardiac filling, inadequate SV, and/or compensatory neurohumoral responses (Goswami et al., 2017; Jordan et al., 2022). This leads to a failure in the maintenance of cerebral perfusion during postural alterations, such as transitions from sitting to standing or during more intensive physical activity (Mulavara et al., 2018; Jordan et al., 2022). As suggested by Neurolab and WISE-2005 studies (Arbeille et al., 1985; Dyson et al., 2007; Guinet et al., 2009), possible causes of OI include hypovolemia, increased vascular compliance, impaired arterial resistance and venous return, and cardiac atrophy (Goswami et al., 2017; Shen and Frishman, 2019; Jordan et al., 2022), very similarly to aging and immobility. Also, reduced BRS may contribute to OI (Jordan et al., 2022). Therefore, OI poses a relevant concern not only during emergency spacecraft landings, but also when returning to normogravity.
Also of interest, some biomarkers associated with the aging process (De Favari Signini et al., 2022), including mitochondrial dysfunction, deoxyribonucleic acid (DNA) damage, telomere shortening, and cellular senescence, have been observed in astronauts (Capri et al., 2023). One such study was the National Aeronautics and Space Administration (NASA) Twin Study (Garrett-Bakelman et al., 2019), which found that the astronaut twin had more noticeable aging indications compared to his ground-based twin, suggesting accelerated aging in the astronaut (Garrett-Bakelman et al., 2019). Interestingly, these biomarker changes, along with inflammation, arterial stiffness and significant risk of cardiovascular diseases, have been observed in both aging and spaceflight (Jaruchart et al., 2016; De Favari Signini et al., 2022; Capri et al., 2023; Hart, 2023; Malhan et al., 2023). Finally, it is noteworthy that the astronauts in the included articles were nearly 15 years older than the subjects in simulations. Thus, in addition to radiation exposure, sleep deprivation, and other stressors inherent to SF, the age difference may also have influenced the astronauts’ outcomes. Accordingly, the results of this review should be regarded with caution, and the findings of simulations cannot be fully extrapolated to astronauts.
There were several limitations in this review, including the small sample sizes used in the included studies, high variability in time exposure to microgravity or models/simulation, varied control groups, and the use of the same volunteers for different outcome measurements. Nonetheless, the challenge of conducting this kind of research justifies such limitations. Moreover, the systematic extraction and classification of outcomes, as well as the meta-analysis undertaken, produced robust and convincing evidence.
Future studies should consider the physical deconditioning of astronauts and its negative impact on their performance at work, in daily life in the spacecraft and especially during extravehicular exploratory activities. Therefore, understanding what happens to the physiology of the human body when exposed to microgravity is essential for monitoring and creating countermeasure strategies for the harmful mechanisms caused by fluid shift, supporting humanity to reach new planets.
Conclusion
This review identified that weightlessness can negatively affect cardiac functions, vascular health, and cardiovascular autonomic modulation. These changes impact the health of astronauts during spaceflight and persist even after returning to Earth, resembling the aging process and prolonged immobility, potentially increasing the risk of cardiovascular diseases and other aging-related conditions. Further research is necessary to develop countermeasures against weightlessness to facilitate long space travels.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Author contributions
RM: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing–original draft, Writing–review and editing. ÉS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing–original draft, Writing–review and editing. GO: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Writing–original draft, Writing–review and editing. AC: Formal Analysis, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing. NU: Formal Analysis, Validation, Visualization, Writing–original draft, Writing–review and editing. ES: Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing. TR: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This review was financially supported by São Paulo Research Foundation – FAPESP (grant #2017/22173-5, #2019/14877-8, #2019/25569-2, #2023/00839-2, #2023/04712-7, #2018/25082-3, and #2023/09582-4), and National Council for Scientific and Technological Development - CNPq (grant #141311/2023-1 and 312042/2023-0).
Acknowledgments
The authors would like to acknowledge the Coordination for the Improvement of Higher Education Personnel–CAPES (Postgraduate Program in Physiotherapy, Grant: 001).
Conflict of interest
Author GO was employed by Brain4care Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2024.1438089/full#supplementary-material
References
Adami A., Pizzinelli P., Bringard A., Capelli C., Malacarne M., Lucini D., et al. (2013). Cardiovascular re-adjustments and baroreflex response during clinical reambulation procedure at the end of 35-day bed rest in humans. Appl. Physiol. Nutr. Metab. 38 (6), 673–680. doi:10.1139/apnm-2012-0396
Arbeille P., Avan P., Treffel L., Zuj K., Normand H., Denise P. (2017). Jugular and portal vein volume, middle cerebral vein velocity, and intracranial pressure in dry immersion. Aerosp. Med. Hum. Perform. 88 (5), 457–462. doi:10.3357/AMHP.4762.2017
Arbeille P., Kerbeci P., Mattar L., Shoemaker J. K., Hughson R. L. (1985)2008). WISE-2005: tibial and gastrocnemius vein and calf tissue response to LBNP after a 60-day bed rest with and without countermeasures. J. Appl. Physiol. 104 (4), 938–943. doi:10.1152/japplphysiol.01021.2007
Arbeille P., Provost R., Zuj K. (2016). Carotid and femoral artery intima-media thickness during 6 Months of spaceflight. Aerosp. Med. Hum. Perform. 87 (5), 449–453. doi:10.3357/AMHP.4493.2016
Arbeille P., Provost R., Zuj K. (2017). Carotid and femoral arterial wall distensibility during long-duration spaceflight. Aerosp. Med. Hum. Perform. 88 (10), 924–930. doi:10.3357/AMHP.4884.2017
Arbeille P., Provost R., Zuj K., Vincent N. (2015). Measurements of jugular, portal, femoral, and calf vein cross-sectional area for the assessment of venous blood redistribution with long duration spaceflight (Vessel Imaging Experiment). Eur. J. Appl. Physiol. 115 (10), 2099–2106. doi:10.1007/s00421-015-3189-6
Arbeille P., Zuj K. A., Macias B. R., Ebert D. J., Laurie S. S., Sargsyan A. E., et al. (2021). Lower body negative pressure reduces jugular and portal vein volumes and counteracts the elevation of middle cerebral vein velocity during long-duration spaceflight. J. Appl. Physiology 131 (3), 1080–1087. doi:10.1152/japplphysiol.00231.2021
Arzeno N. M., Stenger M. B., Lee S. M. C., Ploutz-Snyder R., Platts S. H. (2013). Sex differences in blood pressure control during 6° head-down tilt bed rest. Am. J. Physiology-Heart Circulatory Physiology 304 (8), H1114–H1123. doi:10.1152/ajpheart.00391.2012
Aubert A. E., Beckers F., Verheyden B. (2005). Cardiovascular function and basics of physiology in microgravity. Acta Cardiol. 60 (2), 129–151. doi:10.2143/AC.60.2.2005024
Ayme K., Gavarry O., Rossi P., Desruelle A. V., Regnard J., Boussuges A. (2014). Effect of head-out water immersion on vascular function in healthy subjects. Appl. Physiol. Nutr. Metab. 39 (4), 425–431. doi:10.1139/apnm-2013-0153
Bimpong-Buta N. Y., Muessig J. M., Knost T., Masyuk M., Binneboessel S., Nia A. M., et al. (2020). Comprehensive analysis of macrocirculation and microcirculation in microgravity during parabolic flights. Front. Physiol. 11, 960. doi:10.3389/fphys.2020.00960
Blaber A. P., Goswami N., Xu D. (2022). Prolonged unloading of the cardiovascular system during bedrest and spaceflight weakens neural coupling between blood pressure and heart rate. Acta Astronaut. 195, 567–573. doi:10.1016/j.actaastro.2022.03.009
Caiani E. G., Pellegrini A., Bolea J., Sotaquira M., Almeida R., Vaïda P. (2013). Impaired T-wave amplitude adaptation to heart-rate induced by cardiac deconditioning after 5-days of head-down bed-rest. Acta Astronaut. 91, 166–172. doi:10.1016/j.actaastro.2013.05.016
Capri M., Conte M., Ciurca E., Pirazzini C., Garagnani P., Santoro A., et al. (2023). Long-term human spaceflight and inflammaging: does it promote aging? Ageing Res. Rev. 87, 101909. doi:10.1016/j.arr.2023.101909
Carter H. H., Spence A. L., Pugh C. J. A., Ainslie P., Naylor L. H., Green D. J. (2014). Cardiovascular responses to water immersion in humans: impact on cerebral perfusion. Am. J. Physiology-Regulatory, Integr. Comp. Physiology 306 (9), R636–R640. doi:10.1152/ajpregu.00516.2013
Chouchou F., Pichot V., Costes F., Guillot M., Barthélémy J. C., Bertoletti L., et al. (2020). Autonomic cardiovascular adaptations to acute head-out water immersion, head-down tilt and supine position. Eur. J. Appl. Physiol. 120 (2), 337–347. doi:10.1007/s00421-019-04278-4
Cooke W. H., Ames J. E. I. V., Crossman A. A., Cox J. F., Kuusela T. A., Tahvanainen K. U., et al. (1985). Nine months in space: effects on human autonomic cardiovascular regulation. J. Appl. Physiol. 89 (3), 1039–1045. doi:10.1152/jappl.2000.89.3.1039
De Favari Signini É., Castro A., Rehder-Santos P., Cristina Millan-Mattos J., Magalhães de Oliveira J., Minatel V., et al. (2022). Integrative perspective of the healthy aging process considering the metabolome, cardiac autonomic modulation and cardiorespiratory fitness evaluated in age groups. Sci. Rep. 12 (1), 21314. doi:10.1038/s41598-022-25747-5
Demontis G. C., Germani M. M., Caiani E. G., Barravecchia I., Passino C., Angeloni D. (2017). Human pathophysiological adaptations to the space environment. Front. Physiol. 8, 547. doi:10.3389/fphys.2017.00547
Di Rienzo M., Castiglioni P., Iellamo F., Volterrani M., Pagani M., Mancia G., et al. (2008). Dynamic adaptation of cardiac baroreflex sensitivity to prolonged exposure to microgravity: data from a 16-day spaceflight. J. Appl. Physiology 105 (5), 1569–1575. doi:10.1152/japplphysiol.90625.2008
Dorfman T. A., Levine B. D., Tillery T., Peshock R. M., Hastings J. L., Schneider S. M., et al. (1985). Cardiac atrophy in women following bed rest. J. Appl. Physiol. 103 (1), 8–16. doi:10.1152/japplphysiol.01162.2006
Dorfman T. A., Rosen B. D., Perhonen M. A., Tillery T., McColl R., Peshock R. M., et al. (1985). Diastolic suction is impaired by bed rest: MRI tagging studies of diastolic untwisting. J. Appl. Physiol. 104 (4), 1037–1044. doi:10.1152/japplphysiol.00858.2006
Dyson K. S., Arbeille P., Shoemaker J. K., Custaud M. A., Hughson R. L. (2007). WISE 2005: flow and nitroglycerin mediated dilation following 56 days of head down tilt bed rest with and without an exercise countermeasure. J. Gravit. Physiol. 14 (1), P55–P56. PMID: 18372697.
Eckberg D. L., Halliwill J. R., Beightol L. A., Brown T. E., Taylor J. A., Goble R. (2010). Human vagal baroreflex mechanisms in space. J. Physiol. 588 (Pt 7), 1129–1138. doi:10.1113/jphysiol.2009.186650
Florian J. P., Simmons E. E., Chon K. H., Faes L., Shykoff B. E. (2013). Cardiovascular and autonomic responses to physiological stressors before and after six hours of water immersion. J. Appl. Physiology 115 (9), 1275–1289. doi:10.1152/japplphysiol.00466.2013
Fortrat J. O., De Holanda A., Zuj K., Gauquelin-Koch G., Gharib C. (2017). Altered venous function during long-duration spaceflights. Front. Physiol. 8, 694. doi:10.3389/fphys.2017.00694
Fu Q., Shibata S., Hastings J. L., Platts S. H., Hamilton D. M., Bungo M. W., et al. (2019). Impact of prolonged spaceflight on orthostatic tolerance during ambulation and blood pressure profiles in astronauts. Circulation 140 (9), 729–738. doi:10.1161/CIRCULATIONAHA.119.041050
Gallo C., Ridolfi L., Scarsoglio S. (2020). Cardiovascular deconditioning during long-term spaceflight through multiscale modeling. npj Microgravity 6 (1), 27. doi:10.1038/s41526-020-00117-5
Garrett-Bakelman F. E., Darshi M., Green S. J., Gur R. C., Lin L., Macias B. R., et al. (2019). The NASA Twins Study: a multidimensional analysis of a year-long human spaceflight. Science 364 (6436), eaau8650. doi:10.1126/science.aau8650
Goswami N., Blaber A. P., Hinghofer-Szalkay H., Montani J. P. (2017). Orthostatic intolerance in older persons: etiology and countermeasures. Front. Physiol. 8, 803. doi:10.3389/fphys.2017.00803
Grigoriev A. I., Kotovskaya A. R., Fomina G. A. (2011). The human cardiovascular system during space flight. Acta Astronaut. 68, 1495–1500. doi:10.1016/j.actaastro.2009.11.013
Guinet P., Schneider S. M., Macias B. R., Watenpaugh D. E., Hughson R. L., Le Traon A. P., et al. (2009). WISE-2005: effect of aerobic and resistive exercises on orthostatic tolerance during 60 days bed rest in women. Eur. J. Appl. Physiol. 106 (2), 217–227. doi:10.1007/s00421-009-1009-6
Hall J. E., Guyton A. C. (2011). Guyton and Hall textbook of medical physiology. Amsterdam: Saunders/Elsevier, 1091.
Hargens A. R., Vico L. (1985)2016). Long-duration bed rest as an analog to microgravity. J. Appl. Physiol. 120 (8), 891–903. doi:10.1152/japplphysiol.00935.2015
Hart D. A. (2023). Homo sapiens—a species not designed for space flight: health risks in low earth orbit and beyond, including potential risks when traveling beyond the geomagnetic field of earth. Life 13 (3), 757. doi:10.3390/life13030757
Higgins J. P. T., Altman D. G., Gøtzsche P. C., Jüni P., Moher D., Oxman A. D., et al. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343, d5928. doi:10.1136/bmj.d5928
Hoffmann F., Möstl S., Luchitskaya E., Funtova I., Jordan J., Baevsky R., et al. (2019). An oscillometric approach in assessing early vascular ageing biomarkers following long-term space flights. Int. J. Cardiol. Hypertens. 2, 100013. doi:10.1016/j.ijchy.2019.100013
Hughson R. L., Helm A., Durante M. (2018). Heart in space: effect of the extraterrestrial environment on the cardiovascular system. Nat. Rev. Cardiol. 15 (3), 167–180. doi:10.1038/nrcardio.2017.157
Hughson R. L., Robertson A. D., Arbeille P., Shoemaker J. K., Rush J. W. E., Fraser K. S., et al. (2016). Increased postflight carotid artery stiffness and inflight insulin resistance resulting from 6-mo spaceflight in male and female astronauts. Am. J. Physiology-Heart Circulatory Physiology 310 (5), H628–H638. doi:10.1152/ajpheart.00802.2015
Ishihara A., Terada M., Kouzaki M., Hagio S., Higashibata A., Yamada S., et al. (2020). Blood flow in astronauts on Earth after long space stay. Acta Astronaut. 175, 462–464. doi:10.1016/j.actaastro.2020.05.017
Iwasaki K., Ogawa Y., Kurazumi T., Imaduddin S. M., Mukai C., Furukawa S., et al. (2021). Long-duration spaceflight alters estimated intracranial pressure and cerebral blood velocity. J. Physiol. 599 (4), 1067–1081. doi:10.1113/JP280318
Iwasaki K. I., Zhang R., Perhonen M. A., Zuckerman J. H., Levine B. D. (2004). Reduced baroreflex control of heart period after bed rest is normalized by acute plasma volume restoration. Am. J. Physiol. Regul. Integr. Comp. Physiol. 287 (5), R1256–R1262. doi:10.1152/ajpregu.00613.2002
Jaruchart T., Suwanwela N. C., Tanaka H., Suksom D. (2016). Arterial stiffness is associated with age-related differences in cerebrovascular conductance. Exp. Gerontol. 73, 59–64. doi:10.1016/j.exger.2015.11.006
Jimenez C., Fortrat J. O., Delapierre B., Melin B. (2012). Moderate exercise effects on orthostatic intolerance while wearing protective clothing. Aviat. Space Environ. Med. 83 (6), 570–576. doi:10.3357/asem.3141.2012
Jordan J., Limper U., Tank J. (2022). Cardiovascular autonomic nervous system responses and orthostatic intolerance in astronauts and their relevance in daily medicine. Neurol. Sci. 43 (5), 3039–3051. doi:10.1007/s10072-022-05963-7
Khine H. W., Steding-Ehrenborg K., Hastings J. L., Kowal J., Daniels J. D., Page R. L., et al. (2018). Effects of prolonged spaceflight on atrial size, atrial electrophysiology, and risk of atrial fibrillation. Circ Arrhythmia Electrophysiol. 11 (5), e005959. doi:10.1161/CIRCEP.117.005959
Kotovskaya A. R., Fomina G. A. (2010). Characteristics of adaptation and maladaptation of human cardiovascular system under space flight conditions. Hum. Physiol. 36 (2), 190–197. doi:10.1134/S0362119710020106
Lee S. M. C., Feiveson A. H., Stein S., Stenger M. B., Platts S. H. (2015). Orthostatic intolerance after ISS and space Shuttle missions. Aerosp. Med. Hum. Perform. 86 (12), A54–A67. doi:10.3357/AMHP.EC08.2015
Lee S. M. C., Ribeiro L. C., Martin D. S., Zwart S. R., Feiveson A. H., Laurie S. S., et al. (2020). Arterial structure and function during and after long-duration spaceflight. J. Appl. Physiology 129 (1), 108–123. doi:10.1152/japplphysiol.00550.2019
Levine B. D., Pawelczyk J. A., Ertl A. C., Cox J. F., Zuckerman J. H., Diedrich A., et al. (2002). Human muscle sympathetic neural and haemodynamic responses to tilt following spaceflight. J. Physiol. 538 (Pt 1), 331–340. doi:10.1113/jphysiol.2001.012575
Liang X., Zhang L., Shen H., Chen X., Wan Y., Li L., et al. (2014). Effects of a 45-day head-down bed rest on the diurnal rhythms of activity, sleep, and heart rate. Biol. Rhythm Res. 45 (4), 591–601. doi:10.1080/09291016.2014.882093
Linnarsson D., Hughson R. L., Fraser K. S., Clément G., Karlsson L. L., Mulder E., et al. (2015). Effects of an artificial gravity countermeasure on orthostatic tolerance, blood volumes and aerobic power after short-term bed rest (BR-AG1). J. Appl. Physiology 118 (1), 29–35. doi:10.1152/japplphysiol.00061.2014
Liu J., Li Y., Verheyden B., Chen Z., Wang J., Li Y., et al. (2015). Orthostatic intolerance is independent of the degree of autonomic cardiovascular adaptation after 60 Days of head-down bed rest. BioMed Res. Int. 2015, 896372–896410. doi:10.1155/2015/896372
Liu Z., Wan Y., Zhang L., Tian Y., Lv K., Li Y., et al. (2015). Alterations in the heart rate and activity rhythms of three orbital astronauts on a space mission. Life Sci. Space Res. 4, 62–66. doi:10.1016/j.lssr.2015.01.001
Malhan D., Schoenrock B., Yalçin M., Blottner D., Relόgio A. (2023). Circadian regulation in aging: implications for spaceflight and life on earth. Aging Cell 22 (9), e13935. doi:10.1111/acel.13935
Malhotra V., Thakare A., Hulke S., Wakode S., Parashar R., Ravi N. (2021). Effect of head down tilt on heart rate variability. J. Fam. Med. Prim. Care 10 (1), 439–442. doi:10.4103/jfmpc.jfmpc_1642_20
Marshall-Goebel K., Ambarki K., Eklund A., Malm J., Mulder E., Gerlach D., et al. (2016). Effects of short-term exposure to head-down tilt on cerebral hemodynamics: a prospective evaluation of a spaceflight analog using phase-contrast MRI. J. Appl. Physiology 120 (12), 1466–1473. doi:10.1152/japplphysiol.00841.2015
Marshall-Goebel K., Laurie S. S., Alferova I. V., Arbeille P., Auñón-Chancellor S. M., Ebert D. J., et al. (2019). Assessment of jugular venous blood flow stasis and thrombosis during spaceflight. JAMA Netw. Open 2 (11), e1915011. doi:10.1001/jamanetworkopen.2019.15011
Marshall-Goebel K., Stevens B., Rao C. V., Suarez J. I., Calvillo E., Arbeille P., et al. (2018). Internal jugular vein volume during head-down tilt and Carbon dioxide exposure in the SPACECOT study. Aerosp. Med. Hum. Perform. 89 (4), 351–356. doi:10.3357/AMHP.4934.2018
Martin D. S., Lee S. M. C., Matz T. P., Westby C. M., Scott J. M., Stenger M. B., et al. (2016). Internal jugular pressure increases during parabolic flight. Physiol. Rep. 4 (24), e13068. doi:10.14814/phy2.13068
Martín-Yebra A., Monasterio V., Landreani F., Laguna P., Pablo Martínez J., Caiani E. G. (2019). Assessment of ventricular repolarization instability in terms of T-wave alternans induced by head-down bed-rest immobilization. Physiol. Meas. 40 (10), 104001. doi:10.1088/1361-6579/ab4c18
Möstl S., Orter S., Hoffmann F., Bachler M., Hametner B., Wassertheurer S., et al. (2021). Limited effect of 60-days strict head down tilt bed rest on vascular aging. Front. Physiol. 12, 685473. doi:10.3389/fphys.2021.685473
Mulavara A. P., Peters B. T., Miller C. A., Kofman I. S., Reschke M. F., Taylor L. C., et al. (2018). Physiological and functional alterations after spaceflight and bed rest. Med. Sci. Sports Exerc. 50 (9), 1961–1980. doi:10.1249/MSS.0000000000001615
Norsk P. (2020). Adaptation of the cardiovascular system to weightlessness: surprises, paradoxes and implications for deep space missions. Acta Physiol. (Oxf) 228 (3), e13434. doi:10.1111/apha.13434
Norsk P., Asmar A., Damgaard M., Christensen N. J. (2015). Fluid shifts, vasodilatation and ambulatory blood pressure reduction during long duration spaceflight: vasodilatation and ambulatory blood pressure during spaceflight. J. Physiol. 593 (3), 573–584. doi:10.1113/jphysiol.2014.284869
Ogoh S., Hirasawa A., de Abreu S., Denise P., Normand H. (2017). Internal carotid, external carotid and vertebral artery blood flow responses to 3 days of head-out dry immersion. Exp. Physiol. 102 (10), 1278–1287. doi:10.1113/EP086507
Ogoh S., Hirasawa A., Raven P. B., Rebuffat T., Denise P., Lericollais R., et al. (2015). Effect of an acute increase in central blood volume on cerebral hemodynamics. Am. J. Physiology-Regulatory, Integr. Comp. Physiology 309 (8), R902–R911. doi:10.1152/ajpregu.00137.2015
Ogoh S., Marais M., Lericollais R., Denise P., Raven P. B., Normand H. (2018). Interaction between graviception and carotid baroreflex function in humans during parabolic flight-induced microgravity. J. Appl. Physiology 125 (2), 634–641. doi:10.1152/japplphysiol.00198.2018
Ogoh S., Sato K., Abreu S., Denise P., Normand H. (2020). Arterial and venous cerebral blood flow responses to long-term head-down bed rest in male volunteers. Exp. Physiol. 105 (1), 44–52. doi:10.1113/EP088057
Oluwafemi F. A., Neduncheran A. (2022). Analog and simulated microgravity platforms for life sciences research: their individual capacities, benefits and limitations. Adv. Space Res. 69 (7), 2921–2929. doi:10.1016/j.asr.2022.01.007
Orter S., Möstl S., Bachler M., Hoffmann F., Mayer C. C., Kaniusas E., et al. (2022). A comparison between left ventricular ejection time measurement methods during physiological changes induced by simulated microgravity. Exp. Physiol. 107 (3), 213–221. doi:10.1113/EP090103
Otsuka K., Cornelissen G., Furukawa S., Kubo Y., Hayashi M., Shibata K., et al. (2016). Long-term exposure to space’s microgravity alters the time structure of heart rate variability of astronauts. Heliyon 2 (12), e00211. doi:10.1016/j.heliyon.2016.e00211
Otsuka K., Cornelissen G., Furukawa S., Shibata K., Kubo Y., Mizuno K., et al. (2022). Unconscious mind activates central cardiovascular network and promotes adaptation to microgravity possibly anti-aging during 1-year-long spaceflight. Sci. Rep. 12 (1), 11862. doi:10.1038/s41598-022-14858-8
Otsuka K., Cornelissen G., Kubo Y., Hayashi M., Yamamoto N., Shibata K., et al. (2015). Intrinsic cardiovascular autonomic regulatory system of astronauts exposed long-term to microgravity in space: observational study. npj Microgravity 1 (1), 15018. doi:10.1038/npjmgrav.2016.37
Page M. J., McKenzie J. E., Bossuyt P. M., Boutron I., Hoffmann T. C., Mulrow C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71. doi:10.1136/bmj.n71
Palombo C., Morizzo C., Baluci M., Lucini D., Ricci S., Biolo G., et al. (2015). Large artery remodeling and dynamics following simulated microgravity by prolonged head-down tilt bed rest in humans. BioMed Res. Int. 2015, 342565–342567. doi:10.1155/2015/342565
Patterson C. A., Amelard R., Saarikoski E., Heigold H., Hughson R. L., Robertson A. D. (2022). Sex-dependent jugular vein optical attenuation and distension during head-down tilt and lower body negative pressure. Physiol. Rep. 10 (3), e15179. doi:10.14814/phy2.15179
Pavela J., Sargsyan A., Bedi D., Everson A., Charvat J., Mason S., et al. (2022). Surveillance for jugular venous thrombosis in astronauts. Vasc. Med. 27 (4), 365–372. doi:10.1177/1358863X221086619
Perhonen M. A., Franco F., Lane L. D., Buckey J. C., Blomqvist C. G., Zerwekh J. E., et al. (1985)2001). Cardiac atrophy after bed rest and spaceflight. J. Appl. Physiol. 91 (2), 645–653. doi:10.1152/jappl.2001.91.2.645
Platts S. H., Bairey Merz C. N., Barr Y., Fu Q., Gulati M., Hughson R., et al. (2014). Effects of sex and gender on adaptation to space: cardiovascular alterations. J. Womens Health (Larchmt) 23 (11), 950–955. doi:10.1089/jwh.2014.4912
Ploutz-Snyder L. (2016). Evaluating countermeasures in spaceflight analogs. J. Appl. Physiol. (1985) 120 (8), 915–921. doi:10.1152/japplphysiol.00860.2015
Porta A., Faes L., Marchi A., Bari V., De Maria B., Guzzetti S., et al. (2015). Disentangling cardiovascular control mechanisms during head-down tilt via joint transfer entropy and self-entropy decompositions. Front. Physiol. 6, 301. doi:10.3389/fphys.2015.00301
Pump B., Videbaek R., Gabrielsen A., Norsk P. (1985). Arterial pressure in humans during weightlessness induced by parabolic flights. J. Appl. Physiol. 87 (3), 928–932. doi:10.1152/jappl.1999.87.3.928
Ried K. (2006). Interpreting and understanding meta-analysis graphs--a practical guide. Aust. Fam. Physician 35 (8), 635–638. PMID: 16894442.
Robin A., Van Ombergen A., Laurens C., Bergouignan A., Vico L., Linossier M. T., et al. (2023). Comprehensive assessment of physiological responses in women during the ESA dry immersion VIVALDI microgravity simulation. Nat. Commun. 14 (1), 6311. doi:10.1038/s41467-023-41990-4
Rusanov V. B., Pastushkova L.K, Larina I. M., Chernikova A. G., Goncharova A. G., Nosovsky A. M., et al. (2020). The effect of five-day dry immersion on the nervous and metabolic mechanisms of the circulatory system. Front. Physiol. 11, 692. doi:10.3389/fphys.2020.00692
Ryan R.Cochrane Consumers and Communication Review Group (2016). Cochrane Consumers and communication group: meta-analysis. Available at: https://cccrg.cochrane.org/.
Seibert F. S., Bernhard F., Stervbo U., Vairavanathan S., Bauer F., Rohn B., et al. (2018). The effect of microgravity on central aortic blood pressure. Am. J. Hypertens. 31 (11), 1183–1189. doi:10.1093/ajh/hpy119
Shankhwar V., Singh D., Deepak K. K. (2021). Immediate changes in cardiac autonomic tone and stroke volume during microgravity simulation using head-down tilt. IJPP 65, 86–93. doi:10.25259/IJPP_2_2021
Shen M., Frishman W. H. (2019). Effects of spaceflight on cardiovascular physiology and health. Cardiol. Rev. 27 (3), 122–126. doi:10.1097/CRD.0000000000000236
Solbiati S., Landreani F., Turcato M., Martin-Yebra A., Costantini L., Vaida P., et al. (2020). Analysis of changes in cardiac circadian rhythms of RR and QT induced by a 60-day head-down bed rest with and without nutritional countermeasure. Eur. J. Appl. Physiol. 120 (7), 1699–1710. doi:10.1007/s00421-020-04404-7
Vandeput S., Widjaja D., Aubert A. E., Van Huffel S. (2013). Adaptation of autonomic heart rate regulation in astronauts after spaceflight. Med. Sci. Monit. 19, 9–17. doi:10.12659/MSM.883724
Verheyden B., Liu J., Beckers F., Aubert A. E. (1985)2010). Operational point of neural cardiovascular regulation in humans up to 6 months in space. J. Appl. Physiol. 108 (3), 646–654. doi:10.1152/japplphysiol.00883.2009
Videbaek R., Norsk P. (1985)1997). Atrial distension in humans during microgravity induced by parabolic flights. J. Appl. Physiol. 83 (6), 1862–1866. doi:10.1152/jappl.1997.83.6.1862
Watkins W., Hargens A. R., Seidl S., Clary E. M., Macias B. R. (2017). Lower-body negative pressure decreases noninvasively measured intracranial pressure and internal jugular vein cross-sectional area during head-down tilt. J. Appl. Physiology 123 (1), 260–266. doi:10.1152/japplphysiol.00091.2017
Westby C. M., Martin D. S., Lee S. M. C., Stenger M. B., Platts S. H. (2016a). Left ventricular remodeling during and after 60 days of sedentary head-down bed rest. J. Appl. Physiology 120 (8), 956–964. doi:10.1152/japplphysiol.00676.2015
Whittle R. S., Diaz-Artiles A. (1985)2023). Gravitational effects on carotid and jugular characteristics in graded head-up and head-down tilt. J. Appl. Physiol. 134 (2), 217–229. doi:10.1152/japplphysiol.00248.2022
Whittle R. S., Keller N., Hall E. A., Vellore H. S., Stapleton L. M., Findlay K. H., et al. (2022). Gravitational dose-response curves for acute cardiovascular hemodynamics and autonomic responses in a tilt paradigm. JAHA 11 (14), e024175. doi:10.1161/JAHA.121.024175
Widjaja D., Vandeput S., Van Huffel S., Aubert A. E. (2015). Cardiovascular autonomic adaptation in lunar and martian gravity during parabolic flight. Eur. J. Appl. Physiol. 115 (6), 1205–1218. doi:10.1007/s00421-015-3118-8
Wojcik P., Kini A., Othman B. A., Galdamez L. A., Lee A. G. (2020). Spaceflight associated neuro-ocular syndrome. Curr. Opin. neurology 33 (1), 62–67. doi:10.1097/WCO.0000000000000778
Wood K. N., Greaves D. K., Hughson R. L. (2019). Interrelationships between pulse arrival time and arterial blood pressure during postural transitions before and after spaceflight. J. Appl. Physiology 127 (4), 1050–1057. doi:10.1152/japplphysiol.00317.2019
Xu D., Shoemaker J. K., Blaber A. P., Arbeille P., Fraser K., Hughson R. L. (2013). Reduced heart rate variability during sleep in long-duration spaceflight. Am. J. Physiology-Regulatory, Integr. Comp. Physiology 305 (2), R164–R170. doi:10.1152/ajpregu.00423.2012
Yamamoto N., Otsuka K., Kubo Y., Hayashi M., Mizuno K., Ohshima H., et al. (2015). Effects of long-term microgravity exposure in space on circadian rhythms of heart rate variability. Chronobiology Int. 32 (3), 327–340. doi:10.3109/07420528.2014.979940
Glossary

Keywords: cardiovascular system, fluid shift, hemodynamics, spaceflight, weightlessness conditions, ground-based simulations
Citation: Mendes Zambetta R, Signini ÉDF, Ocamoto GN, Catai AM, Uliam NR, Santarnecchi E and Russo TL (2024) Effects of weightlessness on the cardiovascular system: a systematic review and meta-analysis. Front. Physiol. 15:1438089. doi: 10.3389/fphys.2024.1438089
Received: 25 May 2024; Accepted: 02 July 2024;
Published: 26 July 2024.
Edited by:
Costantino Balestra, Haute École Bruxelles-Brabant (HE2B), BelgiumReviewed by:
Peter Germonpre, Centre for Hyperbaric Oxygen Therapy, BelgiumSebastian Klapa, University of Kiel, Germany
Copyright © 2024 Mendes Zambetta, Signini, Ocamoto, Catai, Uliam, Santarnecchi and Russo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rafaella Mendes Zambetta, cmFmYS5tLnphbWJldHRhQGdtYWlsLmNvbQ==; Thiago Luiz Russo, cnVzc29AdWZzY2FyLmJy