 Guoqing Miao
Guoqing Miao Qi Yan1*†
Qi Yan1*† Houyuan Zhu
Houyuan Zhu- 1China Institute of Sport Science, Beijing, China
- 2School of Physical Education, Hebei Normal University, Shijiazhuang, Hebei, China
Objective: To explore the feasibility of post-exercise heart rate recovery indicators for predicting maximum oxygen uptake (VO2max) in healthy adults aged 30–60 years.
Methods: 260 healthy adults who did not perform regular exercise were randomly recruited and divided into a model group (n = 200) and a verification group (n = 60). Measure body fat percentage, weight, height and other indicators, and complete a cardiopulmonary exercise test as required to measure VO2max and heart rate recovery (HRR1, HRR2) in the first and second minutes after exercise. Equations are established through stepwise regression method, and the selected optimal equation is tested for back substitution.
Results: The optimal equation is:
Conclusion: The regression equation established through heart rate recovery after exercise can be used to predict VO2max in healthy adults aged 30–60 years.
1 Introduction
Cardiorespiratory endurance is an important indicator that reflects physical health (Writing Committee et al., 2012; Toulouse et al., 2021; Di Prampero, 2003) and is highly correlated with all-cause mortality (Lee et al., 2010), cardiovascular disease mortality (Ren et al., 2020) and the incidence of various tumors (Neto et al., 2019). In 2016, the American Heart Association ranked cardiorespiratory endurance as the fifth vital sign of the human body (Ross et al., 2016). Maximum oxygen uptake (VO2max) is the golden index for evaluating the human cardiorespiratory endurance level (Levine, 2008; Hawkins et al., 2007; Skattebo et al., 2021). VO2max refers to the maximum rate at which an individual can take in and utilize oxygen at maximum exercise intensity. As an important indicator for evaluating cardiorespiratory endurance, it has been widely used in competitive sports, mass sports, etc. (Guazzi et al., 2017; Molinari et al., 2020; Crowley et al., 2022). VO2max testing can be divided into two methods: direct testing and indirect testing. Direct measurement of VO2max is usually done through a cardiopulmonary exercise test. Subjects were required to complete incremental load exercises on a power bike or treadmill (Beltz et al., 2016). This method requires professional equipment and operators, and the test cost is high. It is difficult to popularize it among the public. It requires subjects to reach a state of exhaustion, which involves certain risks. It is also not suitable for the elderly and people with poor physical fitness. The indirect measurement method uses an exercise intensity lower than the maximum load and predicts VO2max from the test results. Although the indirect testing method is not as accurate as the direct testing method, it has attracted much attention due to its relatively low requirements on test sites, equipment, and operators, low economic cost, and easy operation. Indirect testing of VO2max usually uses the subject’s basic physical information and exercise capacity information as independent variables (Hansen et al., 2016; Jalili et al., 2018; Eisenberger et al., 2022).
Heart Rate Recovery (HRR) after exercise refers to the difference between the heart rate at different time periods after exercise and the peak heart rate during exercise. Commonly used measurement times include 1, 2, 3, 4, 5, and 7 min (recorded as HRRt, t corresponds to 1, 2, 3, 4, 5, and 7 min) refers to the individual’s heart rate gradually returning from the level during high-intensity exercise to the heart rate in the resting state after physical activity (Zhu and Lin, 2017). Studies have shown that VO2max tested in cardiopulmonary exercise testing has a positive linear correlation with HRR (Vicente-Campos et al., 2014). The purpose of this study is to establish an evaluation method for maximum oxygen uptake. Using variables such as HRR, body fat percentage, weight, and gender as independent variables, VO2max is evaluated through multiple linear stepwise regression.
2 Research objects and research methods
2.1 Research objects
Subject inclusion criteria: (1) Age 30–60 years old; (2) No exercise habit; (3) Voluntarily cooperate with the experimental process. Exclusion criteria: (1) suffering from cardiovascular disease and family history of sudden death; (2) suffering from physical pain, trauma, etc. Finally, after screening and data cleaning, the data of 260 subjects (164 males, 96 females) were selected. The above subjects’ data were randomly divided into two groups, of which 200 (120 males, 80 females) were In the model group, 60 people (44 men and 16 women) served as the validation group. The choice to allocate 200 participants to the model group and 60 to the validation group was based on statistical soundness. A larger model group sample size helps ensure the accuracy and stability of the model, while a smaller validation group sample size is sufficient to evaluate the model’s generalizability. This division complies with common rules of thumb and takes into account the effective use of resources and the scientific nature of the model (Table 1).
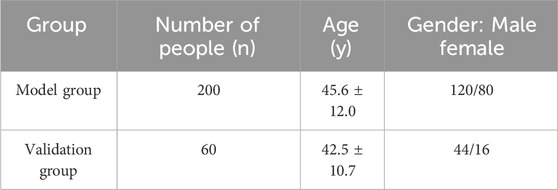
Table 1. Basic information on the indicators of the model group and validation group.
2.2 Research methods
2.2.1 Morphological information measurement
Use the Inbody720 body composition tester to test height, weight, and body fat percentage. The test methods refer to the “National Physical Fitness Measurement Standards (Revised in 2023)” promulgated by the National Physical Fitness Monitoring Center. Calculate the subject’s body mass index (BMI) = weight/height2 based on the height and weight tested by Inbody720.
2.2.2 Cardiopulmonary exercise test
Testing equipment: cardiopulmonary exercise function tester (China, Hanya, model SMAX58CE-SP); treadmill (Sweden, RODBY, model RL2000E); heart rate belt (Finland, POLAR, model H10); respiratory mask (United States, HANS RUDOLPH, Model 2797).
The VO2max test plan adopts Bruce’s incremental load treadmill plan. After the tester is ready for the test, he or she puts on the heart rate monitor, respiratory mask, and fastens the safety protection device while standing on the treadmill. The tester once again informed the tester of the testing process and precautions. After the VO2max test, the tester stood still on the treadmill, and HRR1 and HRR2 were measured through the heart rate belt.
Criteria for judging the end of the VO2max test: (1) The heart rate reaches 180 b/min or no longer rises within 2 min; (2) Respiratory quotient ≥1.10; (3) As the exercise intensity increases, the subject’s oxygen uptake plateaus or declines; (4) The subject is unable to maintain the existing exercise intensity despite his best efforts. The equation model group reaches the limit state during the test, and the back-substitution test group stops testing when the test center rate reaches 180 b/min or no longer rises within 2 min.
2.3 Statistical analysis
Input the data into spss25.0 statistical software for relevant statistical processing, and the statistical results are expressed in the form of ‾x ± s. Correlation analysis was conducted on the normality of the data and the factors affecting VO2max through the Kolmogorov-Smirnov test and the Pearson correlation coefficient test. Four stepwise regressions were performed, and the best equation for goodness of fit was selected through goodness-of-fit test, VIF test, Durbin-Watson test, etc. The differences between the measured values and the predicted values of the optimal equation were analyzed through paired sample t test, Pearson correlation analysis, and Bland-Altman test. The significance level is P < 0.05, and the very significant level is P < 0.01.
3 Results
3.1 Body shape test results
The test results are shown in Table 2. The height, weight and BMI of men are significantly higher than that of women (p < 0.01); their body fat rate is significantly lower than that of women (p < 0.01).
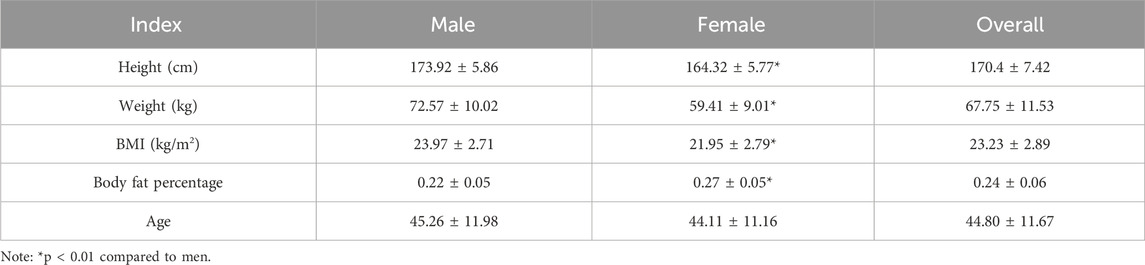
Table 2. Body shape test results.
3.2 Cardiopulmonary exercise test results
The test results are shown in Table 3. VO2max is 3.23 ± 0.67 L/min for men and 2.10 ± 0.45 L/min for women; HRR1 is 21.79 ± 5.19 beats/min for men and 19.41 ± 5.61 beats/min for women; HRR2 is 43.30 ± 8.38 beats/min for men. 37.59 ± 9.10 beats/min for women.

Table 3. Cardiopulmonary exercise test results.
3.3 Correlation analysis between VO2max and various indicators
Through correlation analysis, it was found that, as shown in Table 4, VO2max has a significant correlation with HRR1, HRR2, body fat rate, height, weight and gender of the overall data (p < 0.01). The correlation between age and VO2max is not significant (p > 0.05).
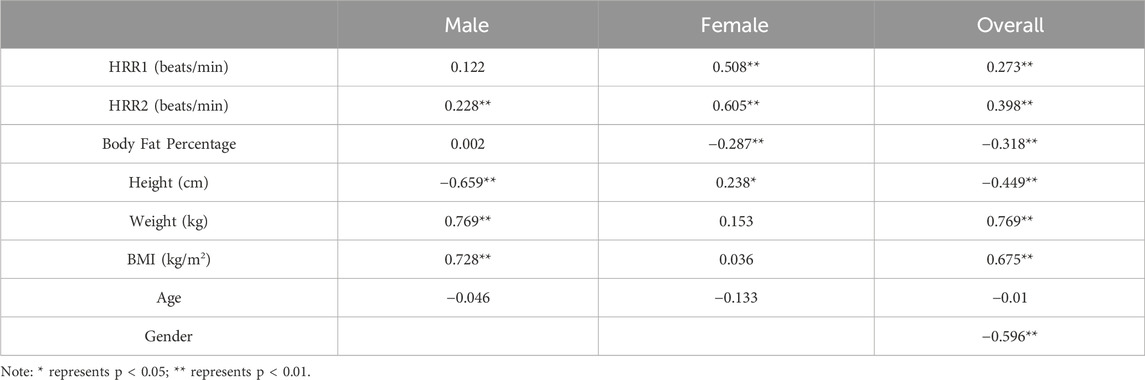
Table 4. Correlation between VO2max and various indicators.
3.4 Establishment of regression equation
Through stepwise regression analysis, HRR1, HRR2, body fat percentage, height, weight, BMI and gender were brought into the regression equation. The regression analysis results are shown in Tables 5, 6.

Table 5. Summary of regression equations.
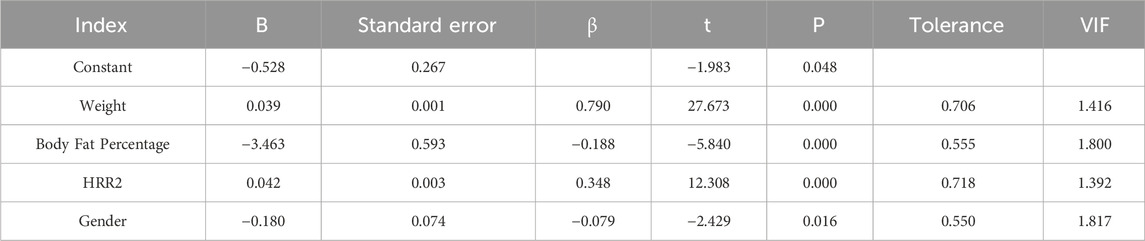
Table 6. Correlation coefficient in Equation 4.
According to the regression results, the estimated VO2max equation can be finally obtained:
As (Equation 1) can be seen from Table 5, the correlation coefficient (R) of model 1 is 0.769, indicating that there is a moderate positive correlation between VO2max and body weight. The coefficient of determination (R2) is 0.592, indicating that this model can explain 59.2% of VO2max. The adjusted coefficient of determination (adjusted R2) is 0.590. Taking into account the influence of the number of independent variables and sample size in the model, the explanatory power of the model has improved. The standard error is 0.708 and the Durbin-Watson test is 1.511.
The correlation coefficient (R) of model 2 is 0.870, indicating that there is a strong positive correlation between VO2max (Equation 2), body weight and body fat percentage. The coefficient of determination (R2) is 0.758, indicating that this model can explain 75.8% of VO2max. The adjusted coefficient of determination (adjusted R2) is 0.756. Taking into account the influence of the number of independent variables and sample size in the model, the explanatory power of the model has improved. The standard error is 0.546 and the Durbin-Watson test is 1.581.
The correlation coefficient (R) of model 3 is 0.922, indicating (Equation 3) that there is a strong positive correlation between VO2max and body weight, body fat rate and HRR2. The coefficient of determination (R2) is 0.850, indicating that this model can explain 85.0% of VO2max. The adjusted coefficient of determination (adjusted R2) is 0.848. Taking into account the influence of the number of independent variables and sample size in the model, the explanatory power of the model has improved. The standard error is 0.431 and the Durbin-Watson test is 1.625.
The correlation coefficient (R) of model 4 is 0.924 (Equation 4), indicating that there is a strong positive correlation between VO2max and body weight, body fat rate and HRR2. The coefficient of determination (R2) is 0.853, indicating that this model can explain 85.3% of VO2max. The adjusted coefficient of determination (adjusted R2) is 0.851. Taking into account the influence of the number of independent variables and sample size in the model, the explanatory power of the model has improved. The standard error is 0.427 and the Durbin-Watson test is 1.624.
In summary, Model 4 has strong explanatory power, with higher R2 and higher adjusted R2, taking into account the effects of weight, body fat rate, HRR2 and gender. The standard error is small. The Durbin-Watson test is close to the ideal range, indicating that the residuals in this model are independent of each other. Comprehensive analysis results show that body weight, body fat percentage, HRR2 and gender have a significant impact on the ability to explain VO2max. The explanatory power of these models is relatively strong, the standard errors are small, and the research results have certain reference value.
3.5 Backward elimination test
Substitute various indicators of the verification group (n = 60) into the optimal equation to predict the VO2max value and analyze and compare it with the measured VO2max value. Through paired sample t test and Pearson correlation analysis test, the test results show that the measured value and predicted value The difference is not significant (p > 0.05) and there is a high positive correlation (r = 0.889, p < 0.01) (Table 7).

Table 7. Comparative analysis of actual measured values and predicted values.
4 Discussion
Using stepwise regression analysis, four regression equations for inferring VO2max were established. Test through goodness of fit test, VIF test, Durbin-Watson and other methods. The best equation is adopted based on the test results. The best equation is
The independent variables included in the optimal equation of this study are weight, body fat percentage, HRR2 and gender. There is a significant positive correlation between absolute VO2max and body weight. Onetti-Onetti et al. (2020) proposed that body weight is an important influencing factor for VO2max. This is consistent with the research results of Tangkudung et al. (2020). In this study, body weight was used as the natural factor. Variables are included in the regression equation. There is a significant negative correlation between body fat rate and absolute VO2max, This means that a lower body fat percentage is beneficial to an individual’s VO2max. Kai et al. (2024) used 48 subjects as the research subjects, and the results showed that body fat rate is beneficial to the individual’s aerobic exercise ability. There was a significant negative correlation between fat percentage and absolute VO2max (r = −0.55, p < 0.001), which is consistent with the research results of Mondal and Mishra (2017). Absolute VO2max has a significant positive correlation with HRR2. As heart rate recovery ability increases, aerobic exercise capacity will also be enhanced. Yifan et al. (2014) divided HRR242bmp into one group, and divided HRR2 < 42bmp into another group. One group, a comparative analysis of the VO2max and other indicators of the two groups found that the VO2max of the high HRR2 group was significantly higher than the other group. Gender is an important influencing factor on VO2max. Research by Xiaoyun and Meng (2005) and others pointed out that differences in gender will cause differences in VO2max. Women are usually lower than men, which is related to the fact that men have higher heart volume, hemoglobin content and cardiac output than women (Santisteban et al., 2022). The study by Wiebe et al. (1998) also found that women’s VO2max is significantly lower than men.
The validity of the equation is tested by substituting the data of the validation group into the model group, and the measured and predicted values of the validation group are analyzed using paired sample t-test, Pearson correlation analysis and Bland Altman test. Bland-Altman analysis is a method used to evaluate the consistency between two measurement methods. It is usually used to compare the deviation and consistency of two measurement methods (Gerke, 2020) and is intuitively reflected through graphics. In this study, the value calculated by the optimal equation was slightly lower than the measured value, which may be related to the individual differences of the subjects. At the same time, the paired sample t test showed that there was no significant difference between the measured value and the predicted value (Figure 1), Pearson product-moment correlation analysis suggests that the two are highly correlated (Figure 2). The normality test was performed on the difference between the measured value and the predicted value in the verification group, and the results showed that the difference was normally distributed (Figure 3). The actual measured values and predicted values of the validation group were further evaluated. Through the Bland-Altman consistency test, it was found that the mean VO2max difference of 58 of the 60 subjects in the validation group was within the Mean ± 1.96*SD interval. Only two subjects had mean differences outside the Mean ± 1.96*SD interval (Figure 4), which shows that the optimal equation used in this study has good validity.
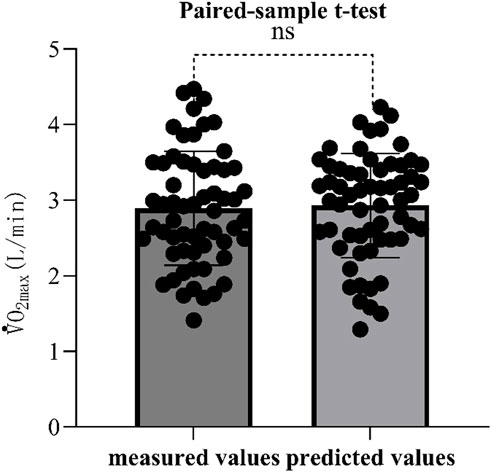
Figure 1. Paired sample t-test of measured values and predicted values. Note: ns means p > 0.05, no significant difference.

Figure 2. Pearson correlation analysis between actual measured values and predicted values.
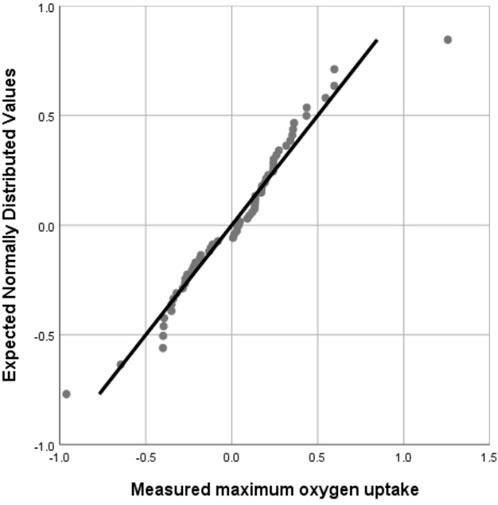
Figure 3. Normal Q-Q plot of the difference between actual measured value and predicted value.
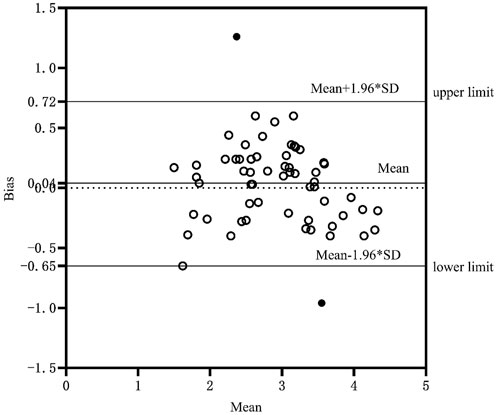
Figure 4. Mean systematic error between measured values and predicted values.
Although the equation has included some major factors such as weight, body fat percentage, HRR2 and gender, there are also some potential confounding variables that may not have been taken into account, such as age, height, training status, genetic factors and lifestyle factors. These potential confounding variables may affect the accuracy of VO2max prediction. In practical applications, it is recommended to further examine and control these potential confounding variables to improve the reliability and validity of the model.
HRR is an important indicator of cardiovascular health (Dimkpa, 2009), which reflects the heart’s ability to recover from a high-intensity state to a resting state after exercise and reflects the body’s ability to adapt to exercise load. HRR not only has the feasibility of evaluating aerobic capacity, but has also been proven to be an effective independent indicator for predicting the occurrence of cardiovascular disease and cardiovascular events (Cole et al., 2000; Cole and Lauer, 1999; Nishime et al., 2000). This is one of the reasons why this study uses HRR as a predictor of VO2max. In addition, and most importantly, HRR measurement is relatively simple, usually just recording the heart rate drop after high-intensity exercise, without the need for complex equipment. This makes the inferred VO2max equation established through HRR highly operable, practical and easy to popularize.
5 Conclusion
The prediction equation established in this study is:
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Beijing Hospital Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
GM: Writing–original draft, Writing–review and editing. HZ: Writing–review and editing, Data curation. FL: Writing–review and editing. QY: Funding acquisition, Writing–review and editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Beltz N. M., Gibson A. L., Janot J. M., Kravitz L., Mermier C. M., Dalleck L. C. (2016). Graded exercise testing protocols for the determination of VO2max: historical perspectives, progress, and future considerations. J. Sports Med. 2016 (1), 3968393. doi:10.1155/2016/3968393
Cole C. R., Foody J. M., Blackstone E. H., Lauer M. S. (2000). Heart rate recovery after submaximal exercise testing as a predictor of mortality in a cardiovascularly healthy cohort. Ann. Intern. Med. 132 (7), 552–5. doi:10.7326/0003-4819-132-7-200004040-00007
Cole C. R., Lauer M. S. (1999). Heart-rate recovery immediately after exercise as a predictor of mortality. N. Engl. J. Med. 341 (1), 1351–1357. doi:10.1056/NEJM199910283411804
Crowley E., Powell C., Carson B. P., W Davies R. (2022). The effect of exercise training intensity on VO2max in healthy adults: an overview of systematic reviews and meta-analyses. Transl. Sports Med. 2022, 9310710–10. doi:10.1155/2022/9310710
Dimkpa U. (2009). Post-exercise heart rate recovery: an index of cardiovascular fitness. J. Exerc. Physiol. Online 12 (1), 10–22.
Di Prampero P. E. (2003). Factors limiting maximal performance in humans. Eur. J. Appl. Physiol. 90 (3–4), 420–429. doi:10.1007/s00421-003-0926-z
Eisenberger L., Mayr B., Beck M., Venek V., Kranzinger C., Menzl A., et al. (2022). Development and validation of a 1-km cardio-trekking test to estimate cardiorespiratory fitness in healthy adults. Prev. Med. Rep. 30, 102039. doi:10.1016/j.pmedr.2022.102039
Gerke O. (2020). Reporting standards for a bland–altman agreement analysis: a review of methodological reviews. Diagnostics 10 (5), 334. doi:10.3390/diagnostics10050334
Guazzi M., Bandera F., Ozemek C., Systrom D., Arena R. (2017). Cardiopulmonary exercise testing. J. Am. Coll. Cardiol. 70 (13), 1618–1636. doi:10.1016/j.jacc.2017.08.012
Hansen D., Jacobs N., Thijs H., Dendale P., Claes N. (2016). Validation of a single-stage fixed-rate step test for the prediction of maximal oxygen uptake in healthy adults. Clin. Physiology Funct. Imaging 36 (5), 401–406. doi:10.1111/cpf.12243
Hawkins M. N., Raven P. B., Snell P. G., James S.-G., Benjamin D. L. (2007). Maximal oxygen uptake as a parametric measure of cardiorespiratory capacity. 39 (1), 103–107. doi:10.1249/01.mss.0000241641.75101.64
Jalili M., Nazem F., Sazvar A., Ranjbar K. (2018). Prediction of maximal oxygen uptake by six-minute walk test and body mass index in healthy boys. J. Pediatr. 200, 155–159. doi:10.1016/j.jpeds.2018.04.026
Kai W., Baichao X., Zhaoxin W., Jianjiao S. (2024). Effects of combined motion intervention on body composition, cardiovascular risk factors and cardiopulmonary fitness of obese female adolescents. Chin. General Pract. 27 (9), 1109–1117. doi:10.12114/j.issn.1007-9572.2023.0483
Lee D. chul, Artero E. G., Sui X., Blair S. N. (2010). Mortality trends in the general population: the importance of cardiorespiratory fitness. J. Psychopharmacol. Oxf. Engl. 24 (4_Suppl. ment), 27–35. doi:10.1177/1359786810382057
Levine B. D. (2008). What do we know, and what do we still need to know? J. Physiology 586 (1), 25–34. doi:10.1113/jphysiol.2007.147629
Molinari C. A., Edwards J., Billat V. (2020). Maximal time spent at VO2max from sprint to the marathon. Int. J. Environ. Res. Public Health 17 (24), 9250. doi:10.3390/ijerph17249250
Mondal H., Mishra S. P. (2017). Effect of BMI, body fat percentage and fat free mass on maximal oxygen consumption in healthy young adults. J. Clin. DIAGNOSTIC Res. 11, CC17–CC20. doi:10.7860/JCDR/2017/25465.10039
Neto J. M. R., Tebexreni A. S., Alves A. N. F., Smanio P. E. P., de Abreu F. B., Thomazi M. C., et al. (2019). Cardiorespiratory fitness data from 18,189 participants who underwent treadmill cardiopulmonary exercise testing in a Brazilian population. PLOS ONE 14 (1), e0209897. doi:10.1371/journal.pone.0209897
Nishime E. O., Cole C. R., Blackstone E. H., Pashkow F. J., Lauer M. S. (2000). Heart rate recovery and treadmill exercise score as predictors of mortality in patients referred for exercise ECG. JAMA 284 (11), 1392–1398. doi:10.1001/jama.284.11.1392
Onetti-Onetti W., Molina-Sotomayor E., González-Jurado J. A., Castillo-Rodríguez A. (2020). Comparison between sexes of the relationships between body composition and maximum oxygen volume in elderly people. Sustainability 12 (8), 3156. doi:10.3390/su12083156
Ren C., Wu X. Y., Zhao W., Tao L. Y., Liu P., Gao W. (2020). Protective effect of cardiopulmonary fitness on patients with high risk of atherosclerotic cardiovascular disease. Beijing da xue xue bao Yi xue ban = J. Peking Univ. Health Sci. 52 (1), 152–157. doi:10.19723/j.issn.1671-167X.2020.01.024
Ross R., Blair S. N., Arena R., Church T. S., Després J. P., Franklin B. A., et al. (2016). Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American heart association. Circulation 134 (24), e653–e699. doi:10.1161/CIR.0000000000000461
Santisteban K. J., Lovering A. T., Halliwill J. R., Minson C. T. (2022). Sex differences in VO2max and the impact on endurance-exercise performance. Int. J. Environ. Res. Public Health 19 (9), 4946. doi:10.3390/ijerph19094946
Skattebo Ø., Johansen E. S., Capelli C., Hallén J. (2021). Effects of 150- and 450-mL acute blood losses on maximal oxygen uptake and exercise capacity. Med. Sci. Sports Exerc. 53, 1729–1738. doi:10.1249/MSS.0000000000002618
Tangkudung J., Haqiyah A., Puspitorini W., Tangkudung A. W. A., Riyadi D. N. (2020). The effect of body mass index and haemoglobin on cardiorespiratory endurance. Int. J. Innovation 11 (8).
Toulouse L., Mucci P., Pezé T., Zunquin G. (2021). Influence of grade of obesity on the achievement of VO2max using an incremental treadmill test in youths. J. Sports Sci. 39 (15), 1717–1722. doi:10.1080/02640414.2021.1898093
Vicente-Campos D., López A. M., Nuñez M. J., López Chicharro J. (2014). Heart rate recovery normality data recorded in response to a maximal exercise test in physically active men. Eur. J. Appl. Physiology 114 (6), 1123–1128. doi:10.1007/s00421-014-2847-4
Wiebe C. G., Gledhill N., Warburton D. E. R., Jamnik V. K., Ferguson S. (1998). Exercise cardiac function in endurance-trained males versus females. Clin. J. Sport Med. 8 (4), 272–279. doi:10.1097/00042752-199810000-00004
Writing Committee, EACPR Guazzi M., Conraads V., Halle M., Mezzani A., Vanhees L., et al. (2012). EACPR/AHA Joint Scientific Statement. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Eur. Heart J. 33 (23), 2917–2927. doi:10.1093/eurheartj/ehs221
Xiaoyun L. I., Meng W. (2005). Vital capacity of students of different majors and genders in colleges and universities, Comparative study of ventilation and maximum oxygen uptake. J. Jilin Inst. Phys. Educ. (2), 82–83.
Yifan ZHAO, Pan S., Wang L. (2014). Study on the correlation between heart rate recovery after exercise test and cardiopulmonary function and quality of life in patients with coronary heart disease. Chin. J. Rehabilitation Med. 29 (11), 1039–1043.
Keywords: heart rate recovery, maximum oxygen uptake, regression equation, healthy people aged 30∼50, cardiorespiratory endurance
Citation: Miao G, Yan Q, Zhu H and Li F (2024) Study on heart rate recovery index to predict maximum oxygen uptake in healthy adults aged 30 to 60 years old. Front. Physiol. 15:1437962. doi: 10.3389/fphys.2024.1437962
Received: 24 May 2024; Accepted: 29 November 2024;
Published: 24 December 2024.
Edited by:
Vincenzo Bonaiuto, University of Rome Tor Vergata, ItalyReviewed by:
Zixiang Gao, University of Calgary, CanadaAsgeir Mamen, Kristiania University College, Norway
Copyright © 2024 Miao, Yan, Zhu and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qi Yan, MTM1MDEzMDI5NDNAMTI2LmNvbQ==
†These authors share first authorship