 Ze-Fei Jiang
Ze-Fei Jiang Guang Liu
Guang Liu Xiao-Xiang Sun
Xiao-Xiang Sun Na Zhi
Na Zhi- Acupuncture and Tuina School, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, China
Introduction: Auricular acupressure (AA) has been widely utilized in the management of constipation, with several studies suggesting its efficacy in treating constipation patients. However, the safety and effectiveness of AA in constipation remain uncertain. Hence, the aim of this study was to assess the effectiveness and safety of AA for constipation.
Methods and analysis: A total of eight electronic databases and three clinical trial registration platforms were searched from their inception to April 2023 for randomized controlled trials (RCTs) of AA for constipation. The included studies were appraised for quality using the Cochrane Collaboration’s Risk of Bias Assessment tool. The quality of evidence was assessed by two independent reviewers employing the Grading of Recommendations Assessment, Development, and Evaluation System (GRADE) evaluation tool. Meta-analysis of data and assessment of publication bias were performed using RevMan 5.4 and STATA 13.0 software, respectively.
Results: This review included 34 randomized controlled trials conducted between 2007 and 2023, involving 2,465 participants. The findings of the study indicate that overall, AA is significantly associated with improved CSBMs (MD = 1.22, 95% CI [0.68, 1.77], p < 0.0001, I2 = 0%), BSF (MD = 0.72, 95%CI: [0.15,1.28], p = 0.01, I2 = 82%), CAS (MD = -3.28, 95%CI: [−5.95, −0.60], p = 0.02, I2 = 80%), responder rate (RR = 1.27, 95%CI: [1.16, 1.38], p < 0.00001, I2 = 79%), cure rate (RR = 1.84, 95% CI [1.56, 2.15], p < 0.00001, I2 = 0%), and PAC-QOL (MD = −2.73, 95% CI: [−3.41, −2.04], p < 0.00001, I2 = 98%) compared to the control group. However, no difference in PAC-SYM (MD = −0.15, 95%CI: [−0.38,0.07], p = 0.19, I2 = 67%) was found between the two groups. Additionally, there was no significant difference in adverse events (RR = 0.53, 95% CI: [0.24, 1.21], p = 0.13, I2 = 38%).
Conclusion: Based on the available evidence, auricular acupressure appears to be a potentially safe and effective intervention for managing constipation in adults. Nonetheless, the overall quality of evidence for the identified outcomes was assessed as low to very low, highlighting the need for additional high-quality randomized controlled trials to further validate these findings.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero, identifier CRD42023425033.
1 Introduction
Constipation, characterized by difficult and infrequent bowel movements accompanied by symptoms like bloating and abdominal pain (Vriesman et al., 2020), has a higher prevalence in older adults due to age-related factors (Barberio et al., 2021). The estimated overall prevalence of constipation in older adults is 18.9% [95% CI (14.7%–23.9%)] (Salari et al., 2023). Among the available treatment options, saline laxatives have shown robust evidence of effectiveness (Serra et al., 2020). However, concerns persist regarding the long-term safety of this approach (Serra et al., 2020), as laxative misuse and abuse can lead to weight loss, electrolyte imbalances, laxative dependence, and visceral organ dysfunction (Daniali et al., 2020). Non-pharmacological interventions, such as dietary guidance, regular physical activity, and potty training, are considered the initial management strategy for constipation (Vriesman et al., 2020). Nevertheless, successful implementation of these interventions relies heavily on patient compliance and persistence. Therefore, it is crucial to develop an effective, safe, and feasible therapy to alleviate constipation.
Auricular acupressure (AA) is a non-invasive therapy rooted in Traditional Chinese Medicine (TCM) that involves applying pressure to specific acupoints on the ear using Vaccaria seeds or magnetic pellets. AA offers several advantages over other therapies, including affordability, painlessness, and high patient acceptance. Under the guidance of a doctor, patients can easily complete the treatment procedure. Each organ in the body has a reflex point on the outer ear’s surface, and acupoint stimulation aims to restore balance between yin and yang, harmonize the flow of vital energy (qi) and blood, and alleviate various ailments within the body (Zhu, 2014). The vagus nerve plays a crucial regulatory role in controlling smooth muscle contractions and glandular secretions in the intestines (Breit et al., 2018). AA may potentially have a similar effect on constipation as auricular vagal nerve stimulation (Shi et al., 2021; Zhang et al., 2021).
Several clinical studies have found it to be effective in treating constipation (Li et al., 2014; Shin and Park, 2018; Jung and Chang, 2020; Aminizadeh et al., 2023). To date, two systematic reviews (SRs) have been published demonstrating that AA can be used for the treatment of constipation in leukemia patients undergoing chemotherapy (Chen et al., 2018a; Jing et al., 2018a), however, both reviews included only five studies, and the overall quality of evidence was low. The safety and efficacy of AA on constipation are still unclear, hence a SR and meta-analysis regarding AA for constipation is necessary. Consequently, we aimed to evaluate the efficacy of AA for constipation through this meta-analysis of randomized controlled trials (RCTs) to provide evidence-based support for managing constipation.
2 Methods
This study was conducted in accordance with the PRISMA 2020 statement: an updated guideline for reporting systematic reviews. (Page et al., 2021). and the PRISMA for acupuncture checklist (Wang et al., 2019). The study was registered on the PROSPERO website (https://www.crd.york.ac.uk/prospero/) with the registration number: CRD42023425033.
2.1 Inclusion criteria
(1) Types of studies: Only RCTs with parallel group designs published in English or Chinese were included in this study. Non-RCTs, such as controlled before-and-after studies, historically controlled studies, cohort studies, and cross-sectional studies, among others, were excluded.
(2) Types of participants: Adult patients (ages 18 years or older) who meet the diagnostic criteria of functional constipation Rome II (Drossman, 1999), Rome III (Drossman, 2006), Rome Ⅳ (Drossman, 2016) or other recognized diagnostic criteria were included, regardless of gender, age and race. Pregnant and lactating women were excluded in this study.
(3) Types of interventions: Auricular acupressure, defined as the application of pressure to ear acupoints using metallic beads (or actual seeds, ceramic beads, or magnetic beads), was considered. The study included the use of auricular acupressure alone in the experimental group or in combination with the treatment in the control group. Other acupuncture therapies, such as manual acupuncture, electrical acupoint stimulation, acupoint embedding needle, and acupoint application, were excluded. There were no restrictions on the frequency and duration of the interventions.
(4) Types of comparison: Control groups included those who received basic or conventional treatment, placebo-control (sham acupressure.), and no treatment. Conventional treatment included various western medicines, no treatment consists of waiting for treatment, usual care means that control patients receive health education (no drugs involved), such as diet, exercise, emotional management, and bowel habits advice.
(5) Types of outcome measures:
1) Primary outcomes: The primary outcome measures of the study were following:
a) Patient Assessment of Constipation-Sym ptom (PAC-SYM)
b) Complete spontaneous bowel movements (CSBMs)
c) Bristol Stool Form (BSF)
d) Cleveland Clinic Score (CCS)
e) Other indicators that may reflect improvement in spontaneous constipation.
2) Secondary outcomes: The secondary outcome measures of the study were as follows:
a) Responder rate, defined as the percentage of responders among the total number of participants in each group.
b) Cure rate.
c) Patient Assessment of Constipation-Quality of Life (PAC-QOL) questionnaires.
d) Adverse events related to acupressure therapy, such as tenderness or pain, dizziness, local discomfort, skin contusions, and others.
Studies were included if they report at least one of the above outcome indicators.
2.2 Data sources and search strategy
A comprehensive literature search was conducted from the inception of the databases until April 2023. The search was limited to articles published in Chinese and English. Eight electronic databases were searched, including four Chinese databases: China National Knowledge Infrastructure (CNKI), Wanfang, Cqvip (VIP), and Chinese Biomedical (CBM); and four English databases: PubMed, Embase, CENTRAL (Cochrane Central Register of Controlled Trials), and Web of Science. Additionally, three clinical trial registration platforms were searched: World Health Organization (WHO) International Clinical Trials Registry Platform (http://www.who.int/ictrp/en/), Chinese Clinical Trial Registry (http://www.chictr.org/en/), and ClinicalTrials.gov (https://www.clinicaltrials.gov/). The detailed retrieval process is provided in the Supplementary Material S1.
2.3 Study selection
Using NoteExpress 3.2.0, the literature retrieved from the different databases was imported, and duplicate records were identified and removed. Two independent researchers conducted an initial screening of titles, abstracts, and other relevant information. Following the initial screening, the full texts of potentially eligible studies were obtained, and the two researchers independently assessed the full texts against the predefined inclusion and exclusion criteria. In cases of disagreement between the two researchers, a third reviewer was consulted to resolve discrepancies and make a final decision. A PRISMA flowchart illustrating the study selection process is included as Figure 1.
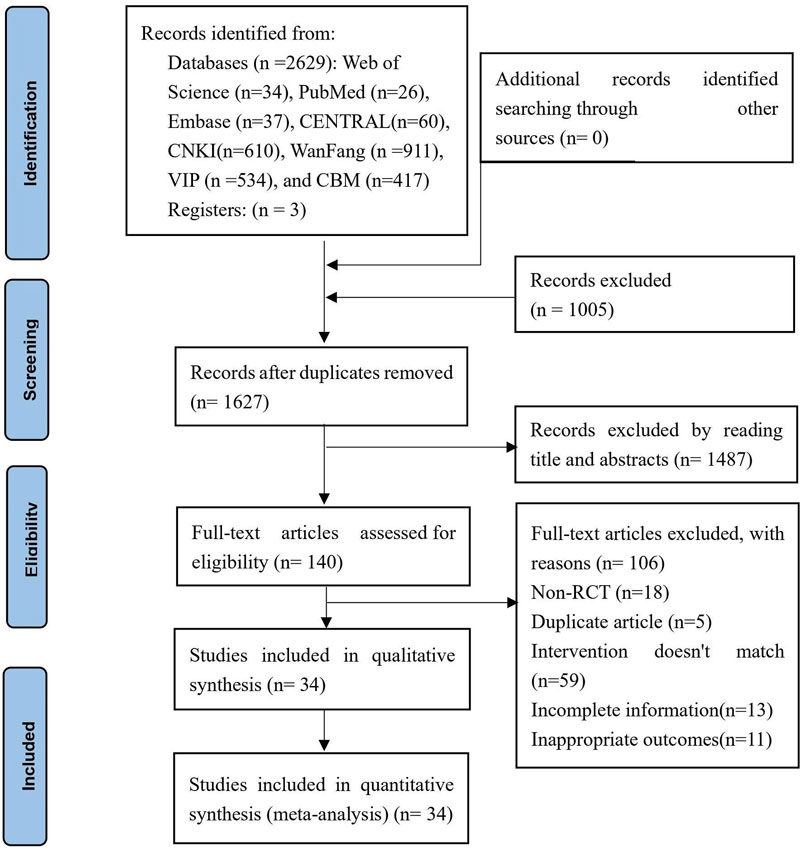
FIGURE 1. PRISMA flow diagram of the study selection process.
2.4 Data extraction and management
Data was independently extracted by two reviewers using a standardized form, which including the following elements: basic information (title, year of publication, first author, language, country of implementation), participant characteristics at baseline (sample size, age, gender, consistency), study design (randomization method, allocation concealment, blinding procedures, diagnostic criteria, intervention frequency and duration, acupoint composition), and outcomes. In the case of multi-arm RCTs, they were reclassified as dual-arm RCTs to ensure compatibility for result synthesis. The two reviewers conducted data extraction and cross-checking, and any discrepancies were resolved through consultation with the corresponding authors.
2.5 Risk of bias assessment
Two independent reviewers evaluated the quality of the included studies using the Cochrane Collaboration’s Risk of Bias Assessment tool (Cumpston et al., 2019). This assessment covered several domains, including random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other potential sources of bias. For instance, in the assessment of random sequence generation, the use of pseudo-random methods such as consultation dates, dates of birth, or ID numbers was considered a “high risk” of bias, while the use of true random methods such as simple random number tables or computerized random number generation was regarded as “low risk” of bias. If no specific method of randomization was stated, the risk was classified as “unclear."
2.6 Confidence in cumulative evidence
The Grading of Recommendations Assessment, Development, and Evaluation System (GRADE) evaluation tool (Guyatt et al., 2011) was independently used by two reviewers to assess the quality of evidence in terms of five dimensions: risk of bias, inconsistency, indirectness, imprecision, and publication bias. The quality of evidence will be classified as high, moderate, low, or very low. In the event of any disagreement, a third reviewer will be consulted to facilitate consensus.
2.7 Assessment of heterogeneity
Statistical heterogeneity between studies was considered acceptable when p ≥ 0.1 or I2 ≤ 50%. p < 0.1 or I2>50% means that the statistical heterogeneity is deemed significant, indicating the need for an analysis to identify the source of the heterogeneity. Sensitivity analysis or subgroup analysis was used for the assessment.
2.8 Data synthesis
In this study, RevMan software (version 5.4, the Nordic Cochrane Centre, Copenhagen, Denmark) was used for data synthesis and analysis. Mean difference (MD) was employed as the effect size for continuous variables, while relative risk (RR) was used for dichotomous variables. The 95% confidence interval (CI) was calculated. A significance level of p < 0.05 was considered statistically significant. Statistical heterogeneity was assessed using chi-squared tests and the Higgins I2 test. If p ≥ 0.1 and I2 ≤ 50%, indicating a high degree of homogeneity, a fixed-effects model was applied for the pooled analysis. Conversely, if p < 0.1 or I2 > 50%, indicating a significant degree of heterogeneity, a random-effects model was used. Significant clinical heterogeneity was addressed through methods such as subgroup analysis, sensitivity analysis, or a narrative summary if necessary. If the outcome data could not be pooled for meta-analysis, a narrative summary was provided instead. If there was significant heterogeneity between studies and the data were available, subgroup analyses were performed based on the varying characteristics of the included studies. If more than 10 studies were included in the analysis, the funnel plot method was used to assess publication biases. Additionally, an Egger’s test was conducted to further evaluate publication bias. The analysis for publication bias was performed using STATA software (version 16.0, Stata Corp LP, United States). A significance level of p < 0.05 was considered indicative of significant publication bias.
3 Results
3.1 Study selection
A total of 2,632 potentially relevant articles were identified through a systematic search across eight databases and three clinical trial registration platforms. After removing 1,005 duplicates, a preliminary screening of titles and abstracts resulted in the exclusion of 1,487 studies. From the remaining 140 studies, 106 were excluded after reading the full text. Ultimately, 34 RCTs (Zhong, 2007; Zhang, 2009; Liu et al., 2011; Chen et al., 2012; Qian, 2012; Xu et al., 2013; Yang and Fu, 2013; Hu et al., 2014; Li et al., 2014; Yang et al., 2014; Ye and He, 2014; Ji et al., 2015; Shen et al., 2015; Chen and Hou, 2016; Huang, 2016; Ji et al., 2016; Qu and Ye, 2016; Liu and Jiang, 2017; Du and Xu, 2018; Li et al., 2018; Liu, 2018; Shin and Park, 2018; Wang, 2019; Xu, 2019; Jung and Chang, 2020; Wang et al., 2020; Chen et al., 2021; Fu et al., 2021; Jie et al., 2021; Wu et al., 2021; Wang et al., 2022; Zhao and Wang, 2022; Aminizadeh et al., 2023; Xu, 2023) met the inclusion criteria, with sample sizes ranging from 25 to 50 participants, involving a total of 2,465 patients. The screening process is presented in Figure 1, illustrating the flow diagram.
3.2 Study characteristics
The main characteristics of the included RCTs are showed in Table 1. The studies, conducted between 2007 and 2023, were predominantly carried out in China, with one study conducted in Hong Kong (Li et al., 2014)), Iran (Aminizadeh et al., 2023), and the Republic of Korea (Shin and Park, 2018; Jung and Chang, 2020). Thirty-two studies were published in Chinese (Zhong, 2007; Zhang, 2009; Liu et al., 2011; Chen et al., 2012; Qian, 2012; Xu et al., 2013; Yang and Fu, 2013; Hu et al., 2014; Yang et al., 2014; Ye and He, 2014; Ji et al., 2015; Shen et al., 2015; Chen and Hou, 2016; Huang, 2016; Ji et al., 2016; Qu and Ye, 2016; Liu and Jiang, 2017; Du and Xu, 2018; Li et al., 2018; Liu, 2018; Wang, 2019; Xu, 2019; Wang et al., 2020; Chen et al., 2021; Fu et al., 2021; Jie et al., 2021; Wu et al., 2021; Wang et al., 2022; Zhao and Wang, 2022; Xu, 2023) while four were published in English (Li et al., 2014; Shin and Park, 2018; Jung and Chang, 2020; Aminizadeh et al., 2023). Among the included studies, 34 were two-arm studies (Zhong, 2007; Zhang, 2009; Liu et al., 2011; Chen et al., 2012; Qian, 2012; Xu et al., 2013; Yang and Fu, 2013; Hu et al., 2014; Yang et al., 2014; Ye and He, 2014; Ji et al., 2015; Shen et al., 2015; Chen and Hou, 2016; Huang, 2016; Ji et al., 2016; Qu and Ye, 2016; Liu and Jiang, 2017; Du and Xu, 2018; Li et al., 2018; Liu, 2018; Shin and Park, 2018; Wang, 2019; Xu, 2019; Jung and Chang, 2020; Wang et al., 2020; Chen et al., 2021; Fu et al., 2021; Jie et al., 2021; Wu et al., 2021; Wang et al., 2022; Zhao and Wang, 2022; Aminizadeh et al., 2023; Xu, 2023), and one was a three-arm study (Li et al., 2014). The age range of patients with constipation was 18 years and older, with seven studies specifically including elderly patients (Zhang, 2009; Yang and Fu, 2013; Ye and He, 2014; Chen and Hou, 2016; Fu et al., 2021; Wang et al., 2022; Aminizadeh et al., 2023). Some studies included patients with additional conditions, such as subarachnoid hemorrhage (Qian, 2012), post-fracture (Yang and Fu, 2013; Liu and Jiang, 2017), stroke (Xu et al., 2013; Ji et al., 2015; Ji et al., 2016), post-craniotomy (Wu et al., 2021), opioid use (Yang et al., 2014), morphine use (Qu and Ye, 2016), diabetes (Hu et al., 2014), schizophrenia (Ye and He, 2014; Jie et al., 2021; Xu, 2023), hemodialysis (Shen et al., 2015; Jung and Chang, 2020; Fu et al., 2021), heart failure (Li et al., 2018), hypertension (Chen and Hou, 2016), and breast cancer patients receiving chemotherapy (Shin and Park, 2018). The treatment duration ranges from 1 week to 8 weeks. Adverse reactions were reported in seven studies (Zhong, 2007; Yang et al., 2014; Liu, 2018; Fu et al., 2021; Zhao and Wang, 2022; Aminizadeh et al., 2023; Xu, 2023), while two studies (Zhong, 2007; Xu, 2023) specifically mentioned that AA had no adverse reactions. The four most commonly selected auricular acupoints in the included studies were the Large intestine (n = 33), Spleen (n = 27), San Jiao (n = 26), and Rectum (n = 23).
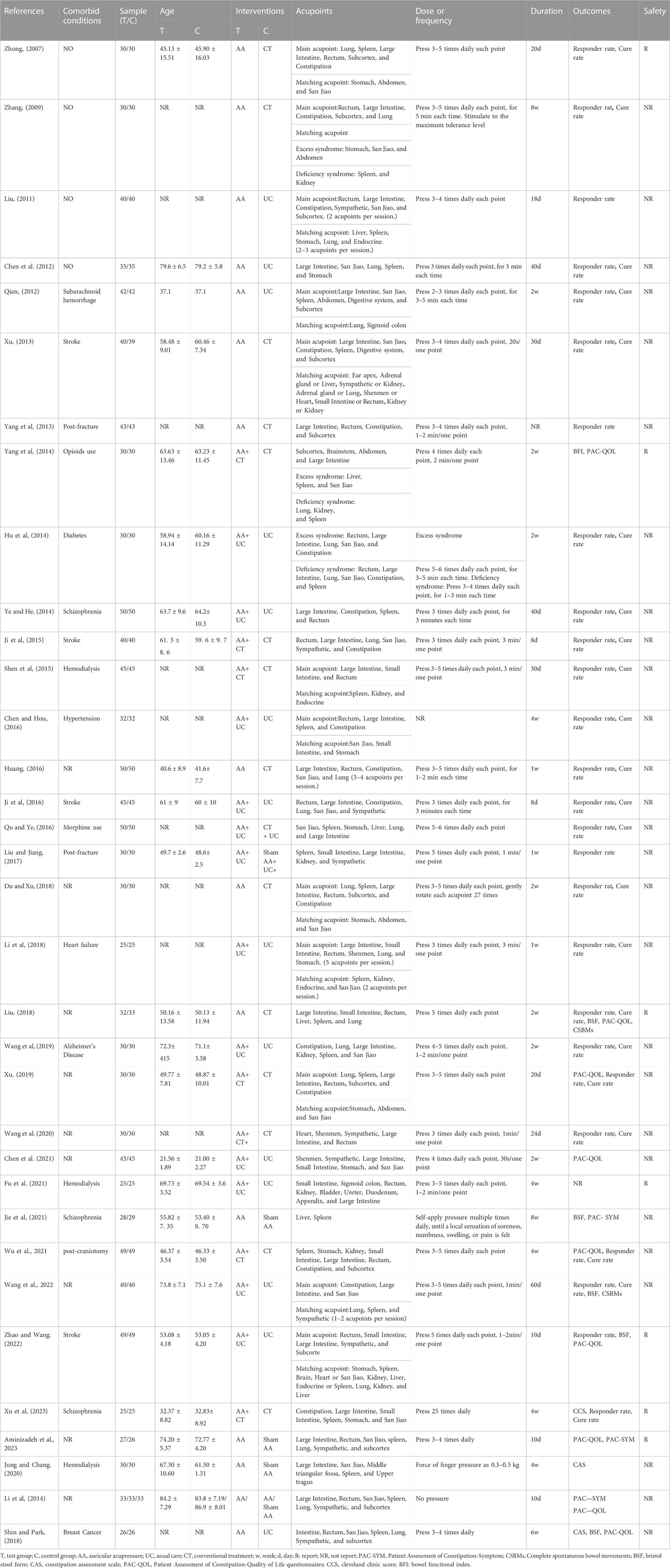
TABLE 1. Basic characteristics of the included studies.
3.3 Risk of bias
All the included studies mentioned the term “randomized” or “random” in their methodology. One of the RCTs (Shin and Park, 2018)included in the study implemented concealed allocation and received a “low risk” rating for allocation concealment. The majority of the included RCTs received an “unclear” rating for blinding of participants and personnel, with the exception of two studies (Li et al., 2014; Aminizadeh et al., 2023) that utilized a sham AA procedure. One (Li et al., 2014) of the RCTs included in the study implemented blinding of outcome assessment and received a “low risk”. Two studies (Ji et al., 2015; Wang et al., 2022) were classified as “high risk” due to without providing a description of the reasons for dropout. In terms of other biases, four studies were classified as high risk. Among them, two studies (Liu et al., 2011; Li et al., 2018) did not report baseline consistency, and two studies (Yang and Fu, 2013; Qu and Ye, 2016) did not report treatment duration. The detailed results are depicted in Figure 2.
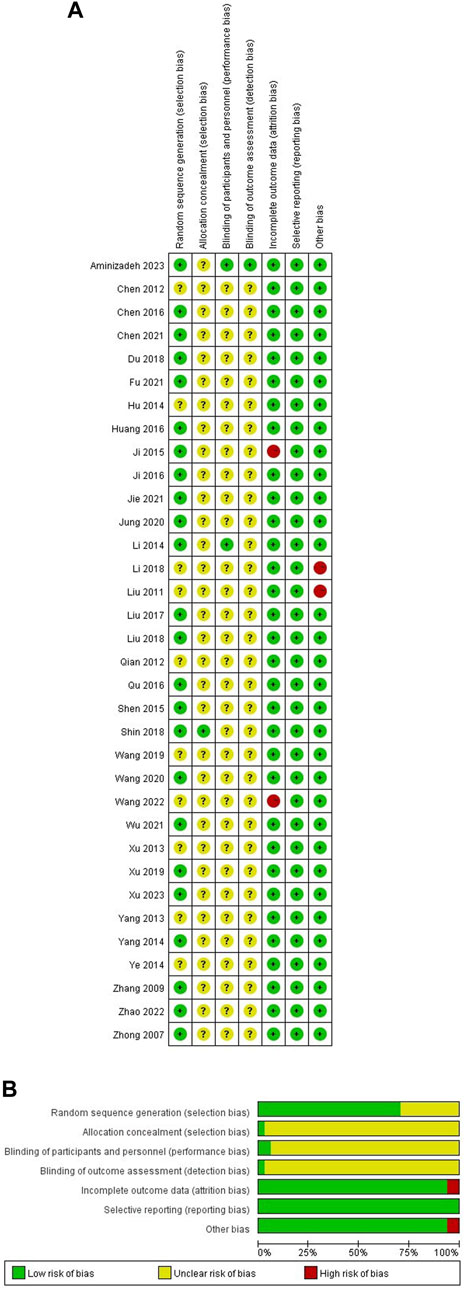
FIGURE 2. Risk of bias of RCTs (A) Risk of bias summary; (B) Risk of bias graph.
3.4 Meta-analysis
The summary of the meta-analysis results is provided in Table 2, with a detailed explanation below.
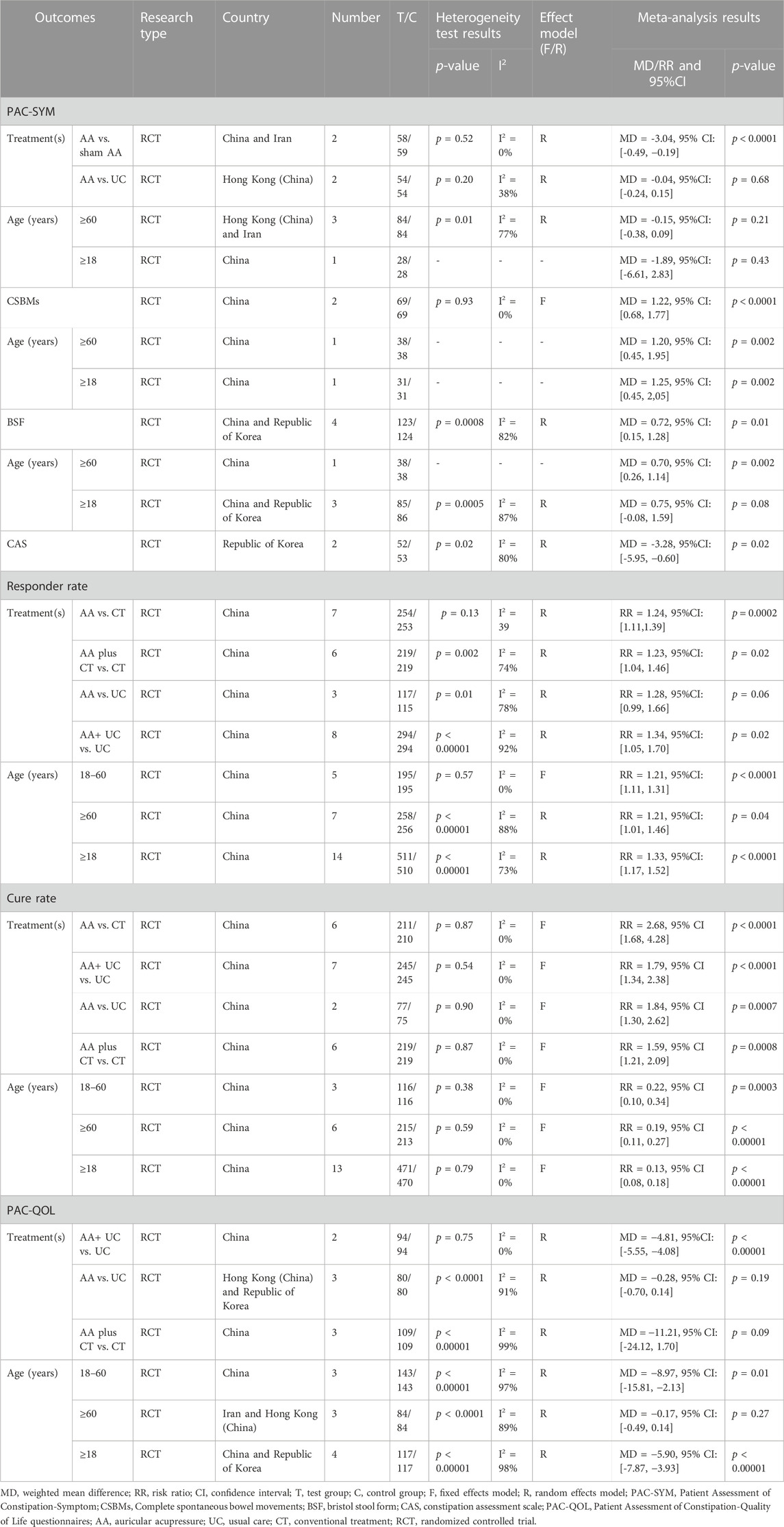
TABLE 2. Summary of meta-analysis results.
3.4.1 Primary outcome
3.4.1.1 PAC-SYM
Among the included RCTs, three studies (Li et al., 2014; Jie et al., 2021; Aminizadeh et al., 2023) reported PAC-SYM as an outcome measure, with one of them (Li et al., 2014) being a three-arm study. The pooled data analysis revealed that there was no significant decrease in PAC-SYM overall (MD = −0.15, 95% CI: [-0.38, 0.07], p = 0.19, I2 = 67%) (Figure 3). A subgroup analysis was conducted based on different comparators, and the results indicated that Auricular acupressure (AA) was more effective than sham AA (MD = −0.34, 95% CI: [-0.49, −0.19], p < 0.0001, I2 = 0%). However, no significant difference was observed when comparing AA to usual care (MD = −0.04, 95% CI: [-0.24, 0.15], p = 0.68, I2 = 38%). When subgroup analysis based on patient age was conducted, no statistically significant differences in PAC-SYM improvement were observed across all age groups with AA (Table 2).
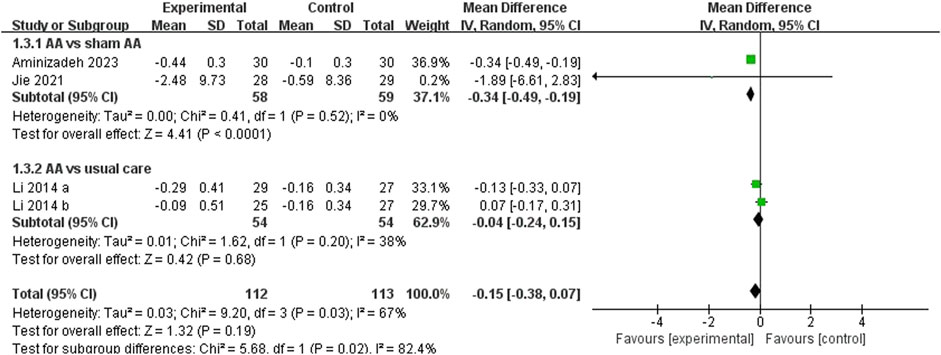
FIGURE 3. Meta-analysis and forest plot for PAC-SYM.
3.4.1.2 CSBMs
Among the included RCTs, two studies (Liu, 2018; Wang et al., 2022) reported CSBMs as an outcome, the pooled data analysis indicated that AA could increase CSBMs [MD = 1.22, 95% CI (0.68, 1.77), p < 0.0001, I2 = 0%] (Figure 4).

FIGURE 4. Meta-analysis and forest plot for CSBMs.
3.4.1.3 BSF
Five studies (Liu, 2018; Shin and Park, 2018; Jie et al., 2021; Wang et al., 2022; Zhao and Wang, 2022) reported BSF as an outcome, however, one study (Zhao and Wang, 2022) with a different scoring rule was excluded from the meta-analysis. The pooled data indicated a significant improvement in BSF (MD = 0.72, 95%CI: [0.15,1.28], p = 0.01, I2 = 82%) (Figure 5). Given to the high heterogeneity, a sensitivity analysis was conducted. When one study (Jie et al., 2021) was removed, the heterogeneity decreased (MD = 0.92, 95%CI: [0.60, 1.23], p < 0.00001, I2 = 1%) (Figure 6).

FIGURE 5. Meta-analysis and forest plot for BSF.

FIGURE 6. Meta-analysis and forest plot for BSF (a study has been excluded).
3.4.1.4 Constipation Assessment Scale (CAS)
CAS was measured after AA treatment in two studies (Shin and Park, 2018; Jung and Chang, 2020), due to the high heterogeneity (I2 = 80%), an analysis was conducted using a random-effects model. The meta-analysis indicated a significant decrease in CAS (MD = -3.28, 95%CI: [-5.95, −0.60], p = 0.02, I2 = 80%) (Figure 7).

FIGURE 7. Meta-analysis and forest plot for CAS.
3.4.2 Secondary outcomes
3.4.2.1 Responder rate
Twenty-six studies (Zhong, 2007; Zhang, 2009; Liu et al., 2011; Chen et al., 2012; Qian, 2012; Xu et al., 2013; Yang and Fu, 2013; Hu et al., 2014; Ye and He, 2014; Ji et al., 2015; Shen et al., 2015; Chen and Hou, 2016; Huang, 2016; Ji et al., 2016; Qu and Ye, 2016; Liu and Jiang, 2017; Du and Xu, 2018; Li et al., 2018; Liu, 2018; Wang, 2019; Xu, 2019; Wang et al., 2020; Wu et al., 2021; Wang et al., 2022; Zhao and Wang, 2022; Xu, 2023) reported the responder rate. The pooled results indicated that overall, there was a significantly higher responder rate in the experimental group compared to the control group (RR = 1.27, 95%CI: [1.16, 1.38], p < 0.00001, I2 = 79%). A subgroup analysis was performed based on different comparators. The results suggested that AA alone (RR = 1.24, 95%CI: [1.11, 1.39], p = 0.0002, I2 = 39%) or plus conventional treatment (RR = 1.23, 95%CI: [1.04, 1.46], p = 0.02, I2 = 74%) was superior to conventional treatment. AA combined with usual care was superior to usual care (RR = 1.34, 95%CI: [1.05, 1.70], p = 0.02, I2 = 92%), and removing the article by Chen et al. (Chen and Hou, 2016) reduced the heterogeneity (RR = 1.32, 95%CI: [1.16, 1.49], p < 0.0001, I2 = 36%). Similarly, the combination of AA with usual care demonstrated superior outcomes compared to combining usual care with conventional treatment (RR = 1.31, 95%CI: [1.08, 1.60], p = 0.007, I2 = not applicable). However, no significant difference in responder rate was observed when AA compared to usual care (RR = 1.28, 95%CI: [0.99, 1.66], p = 0.06, I2 = 78%) or combined with usual care compared to usual care plus sham AA (RR = 1.27, 95%CI: [1.01, 1.61], p = 0.05, I2 = not applicable) (Figure 8). In addition, when subgroup analysis based on patient age was performed, AA showed statistically significant differences in improving responder rate among different age groups (Table 2).
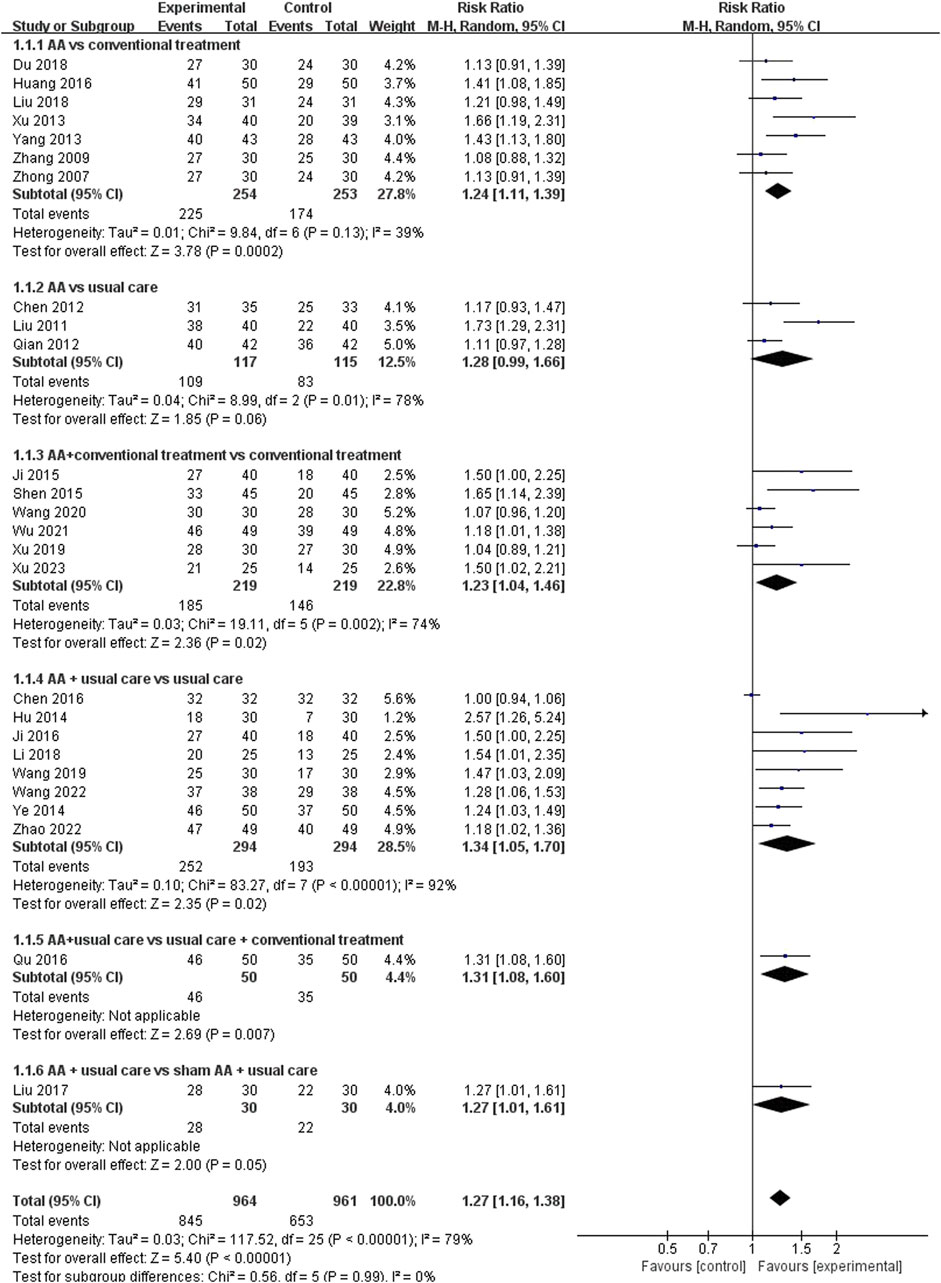
FIGURE 8. Meta-analysis and forest plot for responder rate.
3.4.2.2 Cure rate
There are twenty-two studies (Zhong, 2007; Zhang, 2009; Chen et al., 2012; Qian, 2012; Xu et al., 2013; Hu et al., 2014; Ye and He, 2014; Ji et al., 2015; Shen et al., 2015; Chen and Hou, 2016; Huang, 2016; Ji et al., 2016; Qu and Ye, 2016; Du and Xu, 2018; Li et al., 2018; Liu, 2018; Wang, 2019; Xu, 2019; Wang et al., 2020; Wu et al., 2021; Wang et al., 2022; Xu, 2023) reported the cure rate as an outcome. The fixed-effect model was employed based on the results of heterogeneity test (p = 0.93, I2 = 0%). Meta-analysis showed that the treatment group can significantly increase cure rate among patients with constipation (RR = 1.84, 95% CI [1.56, 2.15], p < 0.00001). Subgroup analysis was performed according to different comparators, indicating that AA alone (RR = 2.68, 95% CI [1.68, 4.28], p < 0.0001, I2 = 0%) or combined with conventional treatment (RR = 1.59, 95% CI [1.21, 2.09], p = 0.0008, I2 = 0%) was superior to conventional treatment. Similarly, AA alone (RR = 1.84, 95% CI [1.30, 2.62], p = 0.0007, I2 = 0%) or combined with usual care (RR = 1.79, 95% CI [1.34, 2.38], p < 0.0001, I2 = 0%) could increase the cure rate when compared with usual care, however, there was no significant difference was observed when AA combined with usual care compared to conventional treatment combined with usual care (RR = 1.63, 95%CI: [0.74, 3.58], p = 0.23, I2 = not applicable) (Figure 9). Additionally, when conducting subgroup analysis by patient age, there were statistically significant differences in the cure rate of AA among different age groups (Table 2).
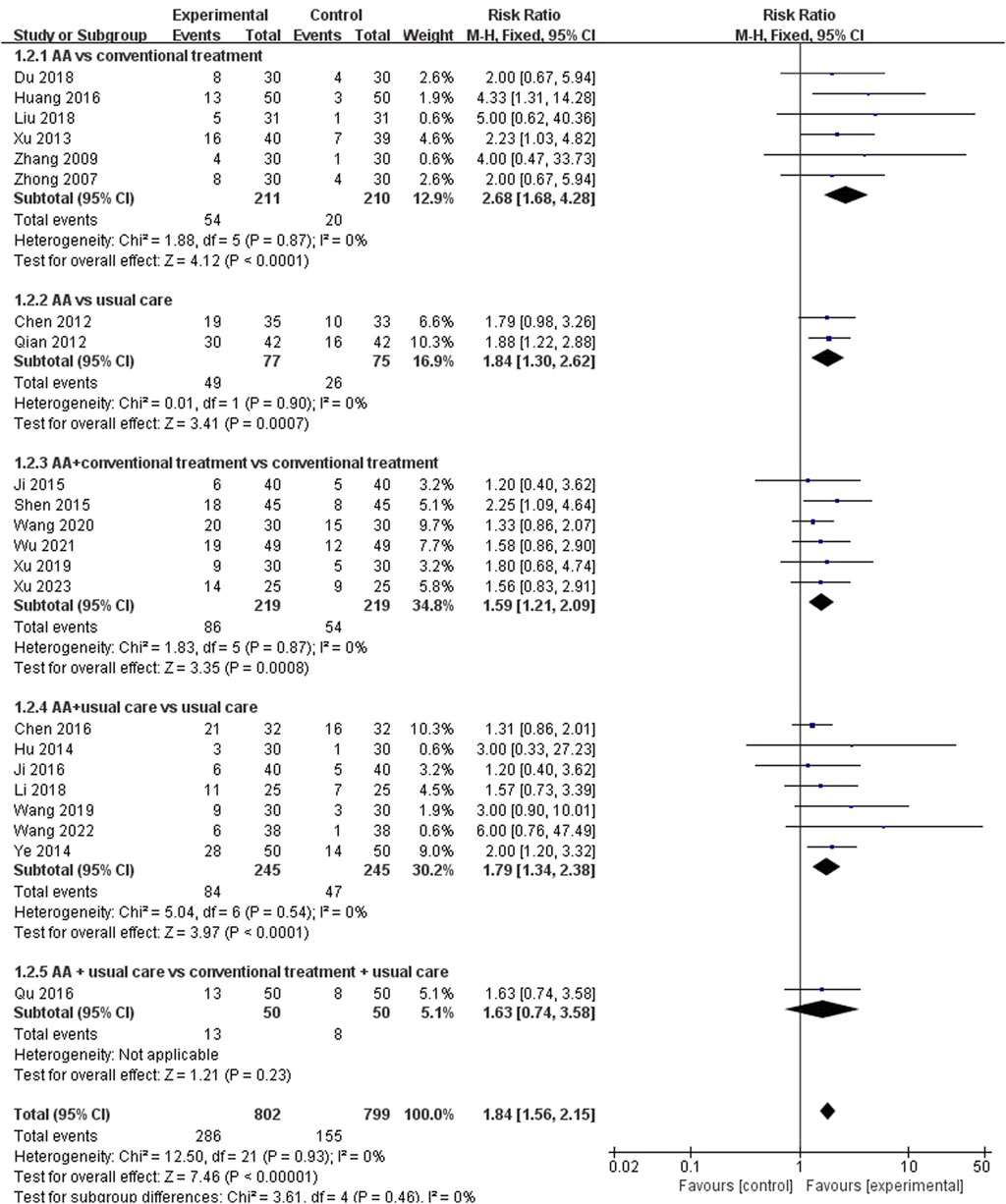
FIGURE 9. Meta-analysis and forest plot for cure rate.
3.4.2.3 PAC-QOL
Nine studies (Li et al., 2014; Yang et al., 2014; Liu, 2018; Shin and Park, 2018; Xu, 2019; Chen et al., 2021; Wu et al., 2021; Zhao and Wang, 2022; Aminizadeh et al., 2023) reported the PAC-QOL. The results meta-analysis showed a greater improvement in the experimental group compared to the control group (MD = −2.73, 95% CI: [-3.41, −2.04], p < 0.00001, I2 = 98%). A subgroup analysis was performed according to different comparators, the results showed there was no significant improvement in PAC-QOL between AA combined with conventional treatment and conventional treatment (MD = −11.21, 95% CI: [-24.12,1.70], p = 0.09, I2 = 99%). Given the significant heterogeneity, a sensitivity analysis was employed. When removing the article by Yang et al. (Yang et al., 2014) the heterogeneity decreased from 99% to 0%. Additionally, there was no significant improvement between AA and usual care groups (MD = −0.28, 95% CI: [-0.70, 0.14], p = 0.19, I2 = 91%). However, AA was superior to conventional treatment (p < 0.00001) or sham AA (p < 0.00001) in terms of PAC-QOL, furthermore, the decrease in PAC-QOL score was more significant in the AA combined with usual care group (MD = −4.81, 95%CI: [-5.55, −4.08], p < 0.00001, I2 = 0%) than in the usual care group (Figure 10). Additionally, when performing subgroup analysis based on patient age, except for the elderly group aged 60 and above, AA showed statistical significance in improving PAC-QOL for constipated patients (Table 2).
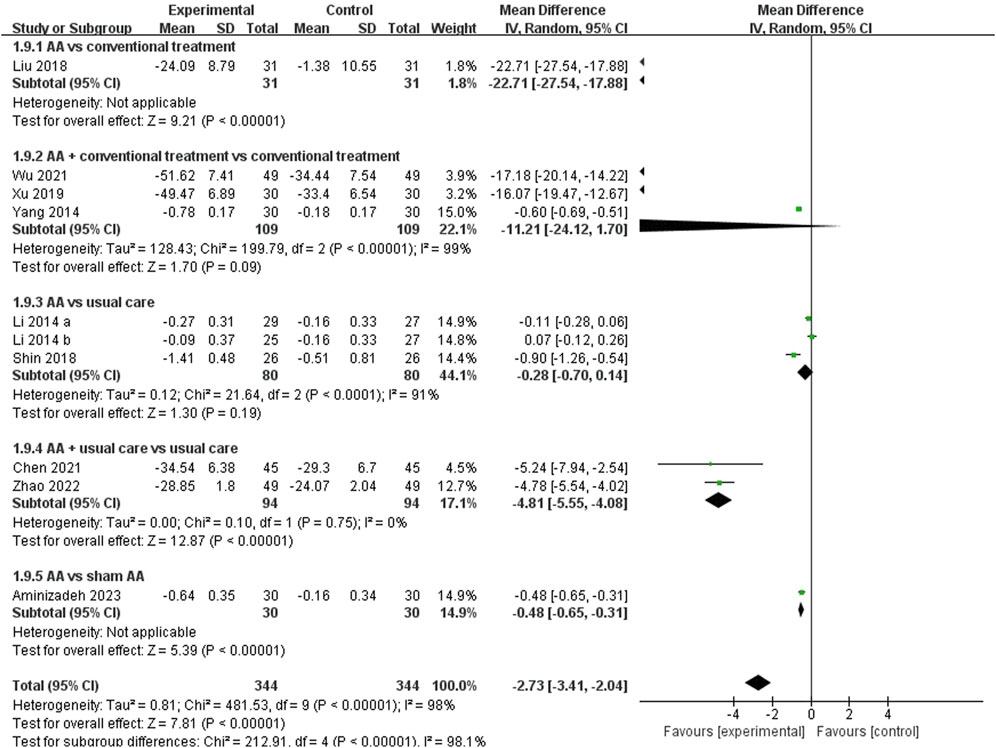
FIGURE 10. Meta-analysis and forest plot for PAC-QOL.
3.4.2.4 Adverse events
A total of seven articles (Zhong, 2007; Yang et al., 2014; Liu, 2018; Fu et al., 2021; Zhao and Wang, 2022; Aminizadeh et al., 2023; Xu, 2023) mentioned adverse events, of these, one study (Aminizadeh et al., 2023) could not be included for meta-analysis due to poor description. The results of meta-analysis showed AA alone or in combination with other treatments was equally safe compared to other treatments (RR = 0.53, 95% CI: [0.24, 1.21], p = 0.13, I2 = 38%) (Figure 11). The adverse reactions were mostly minor, such as skin lesions or itching at the site of pressure, which typically resolved within a few days.
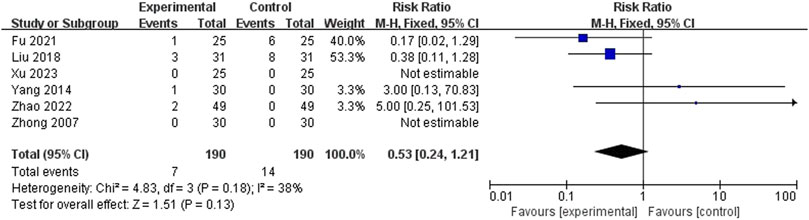
FIGURE 11. Meta-analysis and forest plot for adverse events.
3.5 Quality of evidence
Table 3 presents the quality evaluation of each outcome of AA on constipation. The GRADE system was used to assess the evidence quality based on different intervention measures. The results revealed one outcome with moderate-quality evidence, nine with low-quality evidence, seven with very low-quality evidence, and no evidence with high quality. Most studies had limitations in their experimental design, such as inadequate description of random sequence generation, allocation concealment, and blinding. Consequently, they were downgraded. Additionally, the presence of publication bias in most studies contributed to their downgrading.
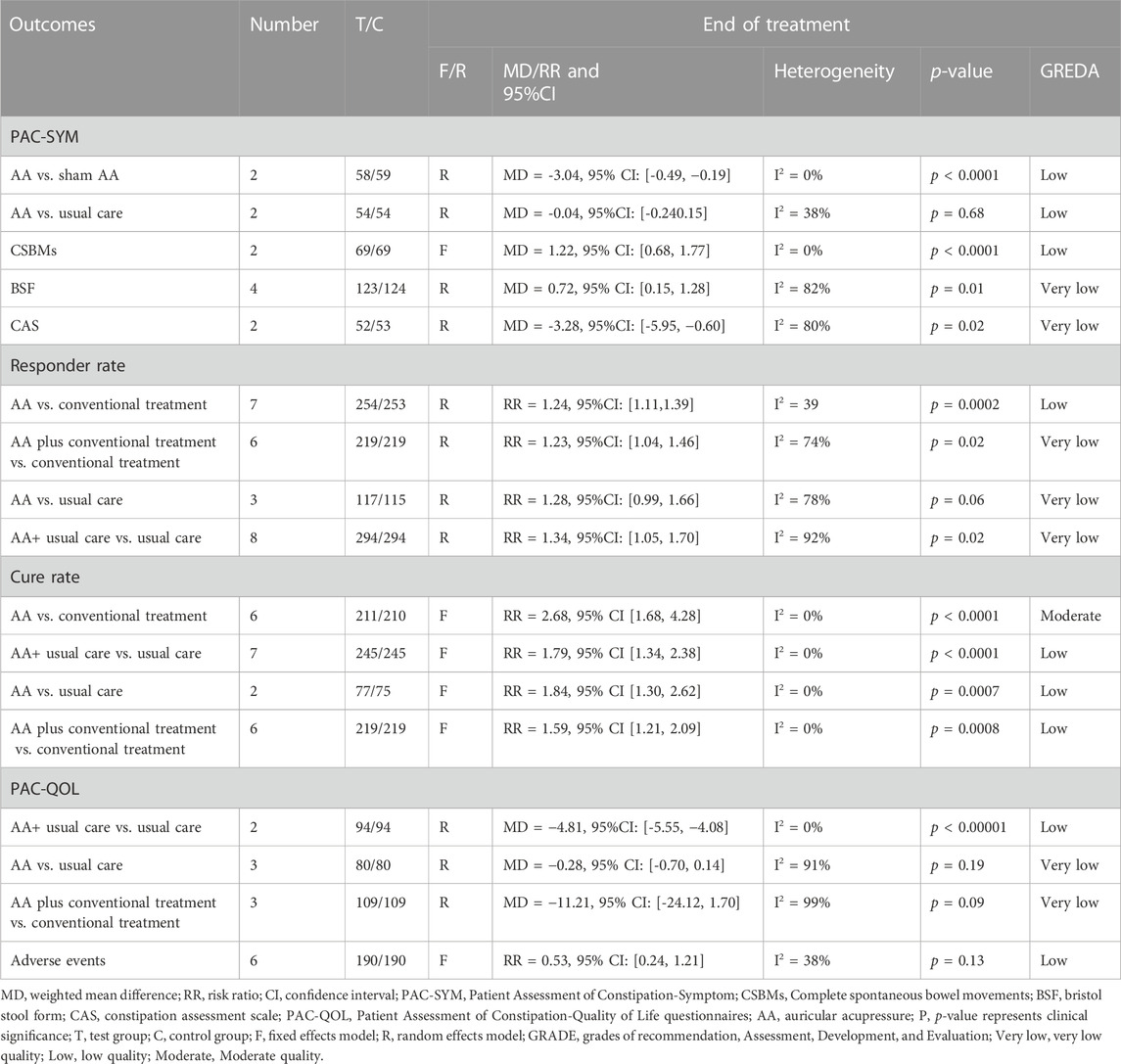
TABLE 3. Quality of evidence included RCTs by GRADE.
3.6 Reporting bias
Due to the limited number of studies reporting outcome results, funnel plots and Egger’s tests were conducted only for response rate and cure rate. The funnel plot of included studies on responder rate displays an asymmetrical distribution, with four studies lying outside the pseudo 95% CI, indicating significant publication bias (Figure 12A). The funnel plot of included studies on cure rate indicates a roughly symmetrical distribution, suggesting a certain degree of publication bias and the presence of a small sample size effect (Figure 12B). Egger’s tests revealed significance levels of p < 0.05 for both response rate (p = 0.00) and cure rate (p = 0.003) (Figure 13).
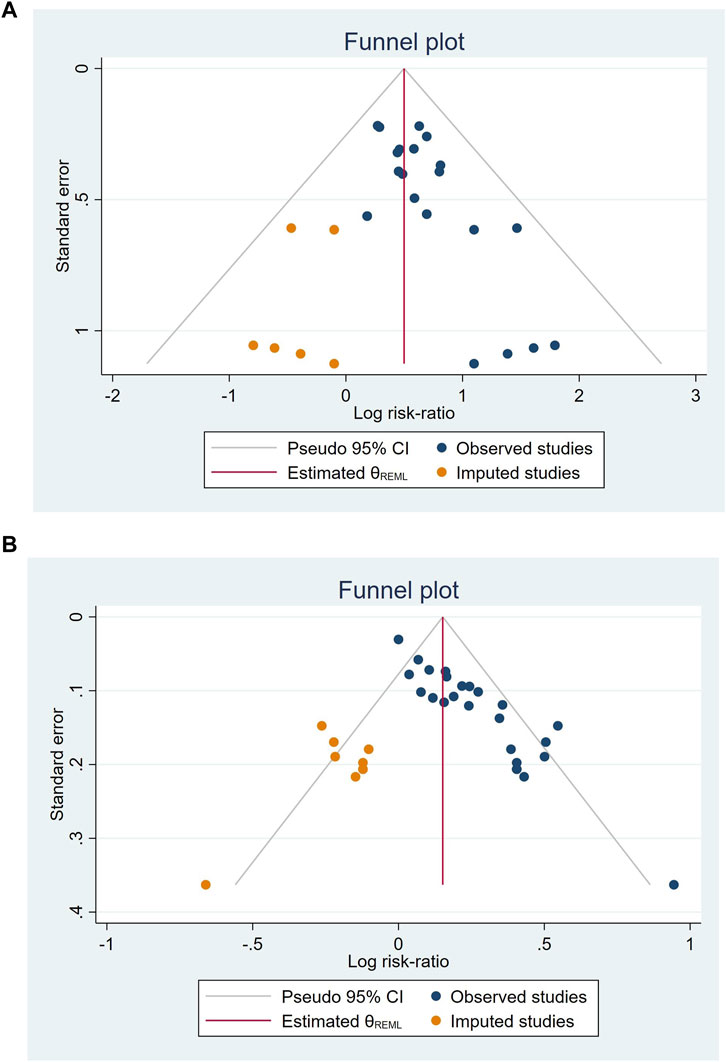
FIGURE 12. Funnel plots of included studies on responder rate (A), cure rate (B).
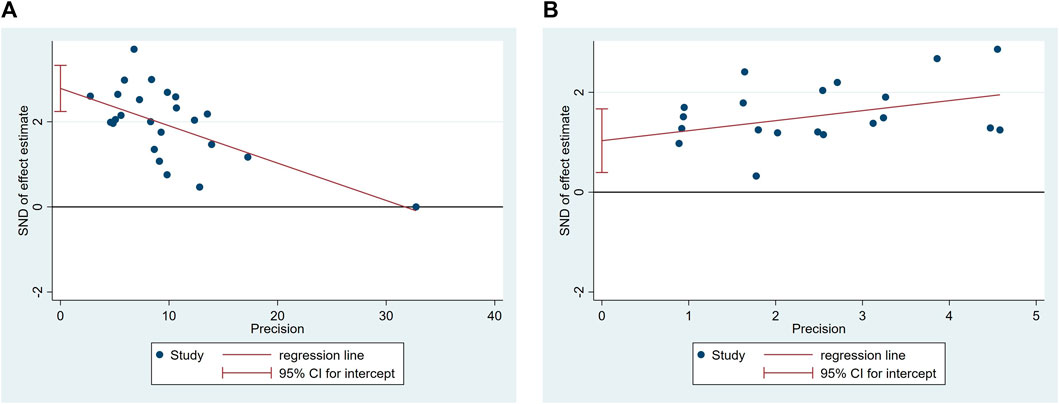
FIGURE 13. Egger’s test of included studies on responder rate (A), cure rate (B).
4 Discussion
Constipation, a prevalent gastrointestinal condition, is characterized by persistent difficulties in bowel movements, incomplete defecation, and decreased frequency of bowel movements. This condition significantly impacts patients’ daily lives and can impair social functioning, leading to work or education limitations in a considerable proportion of individuals (Rao et al., 2007). Initial management strategies for constipation in both children and adults typically involve non-pharmacological approaches, as they have demonstrated beneficial effects in many cases (Daniali et al., 2020; Vriesman et al., 2020). AA, a non-invasive and non-pharmacological treatment modality, has gained widespread utilization for managing various chronic conditions, including constipation. Several studies have reported positive outcomes of AA in alleviating constipation symptoms (Li et al., 2014; Shin and Park, 2018; Jung and Chang, 2020; Aminizadeh et al., 2023). However, the safety and efficacy of AA for constipation in adults remain uncertain.
As is widely known, SRs and meta-analyses generate the highest level of clinical evidence (Izzo et al., 2016). Therefore, we conducted this study to assess the efficacy and safety of AA for constipation in adults. Overall, our study revealed statistically significant differences between the AA and control groups in terms of CSBMs, BSF, CAS, PAC-QOL, responder rate and cure rate, whereas it showed no statistical difference in PAC-SYM. However, when comparing AA with sham AA, AA could significantly reduce the PAC-SYM score (MD = -3.04, 95% CI: [-0.49, −0.19], p < 0.0001). These findings suggest that AA has the potential to alleviate constipation symptoms, increase the frequency of spontaneous bowel movements, improve stool consistency, and enhance overall quality of life. These results are consistent with previous studies examining the effects of AA on constipation in leukemia patients undergoing chemotherapy (Chen et al., 2018a; Jing et al., 2018a). Adverse events reported in seven studies were primarily mild, such as itching at the application site, with no serious adverse reactions documented.
It is worth noting that various outcome measures have been employed to assess the efficacy of constipation treatments. Some measures focus on single-item scores related to constipation (e.g., CSBMs), while others provide a comprehensive evaluation of different aspects of constipation (e.g., CAS). However, certain measures may not precisely reflect specific treatment efficacy, such as response rate or cure rate. To ensure the selected measures adequately capture the effectiveness of constipation treatments, future studies are recommended to include CSBMs per week as one of the outcome measures. This measure provides a straightforward and intuitive reflection of treatment effectiveness and has been widely adopted in recent high-quality clinical studies (Camilleri et al., 2022; Rao et al., 2023; Wang et al., 2023). In our study, AA was found to increase the number of complete spontaneous bowel movements [MD = 1.22, 95% CI (0.68, 1.77), p < 0.0001], with low heterogeneity (I2 = 0%).
AA, derived from traditional Chinese Medicine (acupuncture), focuses on manipulating specific acupoints on the ear to achieve therapeutic effects. This technique is based on the concept of Qi, the vital energy flow within the body. Through applying pressure to these acupoints, practitioners aim to regulate Qi and restore balance (Yang et al., 2013). During auricular acupressure, individuals may experience sensations such as soreness, tingling, or numbness, indicating the activation of acupoints and the desired therapeutic response. Among the included studies, only one study (Li et al., 2014) did not require pressure application to achieve the intended stimulation of Qi. In most other studies, participants were instructed to apply pressure 3–5 times daily. This practice is widely accepted in China (Bao et al., 2017). Furthermore, based on the included research findings, AA involves applying pressure to the acupoints on one side at a time and alternating between both sides. However, there is considerable variation in treatment duration among the studies, ranging from 1 week to 8 weeks. Further research is needed to evaluate the optimal duration and effectiveness of AA. The selection of ear acupoints primarily follows the TCM Zang-fu theory (Liu et al., 2021). The most frequently used acupoints include the Large Intestine and Rectum points to increase intestinal peristalsis, the Spleen point to strengthen transportation and transformation functions, and the San Jiao point to regulate the flow of qi and fluid in the body. When these points are used together, they are believed to promote smooth qi flow in the Large Intestine, ensuring normal transmission function.
However, it is important to acknowledge the limitations of this study. The variations in selected acupoints, comorbid conditions, treatment courses, and number of compressions may introduce significant clinical heterogeneity. Additionally, the restriction to English and Chinese clinical trials may introduce publication bias, as only four out of the 35 included studies were published in English. Most studies did not provide specific details regarding randomization, allocation concealment, and blinding methods, and some failed to comprehensively report trial details according to standard reporting guidelines such as CONSORT. As a result, the quality of evidence for the majority of outcomes was deemed low or very low.
5 Conclusion
Our findings suggest that AA may be a safe and effective treatment for constipation in adults to improving symptoms of constipation and increasing the frequency of spontaneous bowel movements. Nevertheless, it is important to note that the current evidence quality is considered insufficient, and further validation is required through a greater number of high-quality RCTs.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
Z-FJ: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Writing–original draft, Writing–review and editing. GL: Data curation, Software, Writing–review and editing. X-XS: Data curation, Formal Analysis, Software, Writing–review and editing. NZ: Writing–review and editing. X-ML: Writing–review and editing. RS: Writing–review and editing. HZ: Funding acquisition, Writing–review and editing.
Funding
This study was supported by the “Xinglin Scholars” Subject Talent Research Promotion Plan of Chengdu University of Traditional Chinese Medicine (XKTD2021004) and the State Administration of Traditional Chinese Medicine 2022 National Famous Old Chinese Medicine Expert Inheritance Studio Construction Project.
Acknowledgments
The authors would like to express their gratitude to the “Xinglin Scholars” Subject Talent Research Promotion Plan of Chengdu University of Traditional Chinese Medicine (XKTD2021004) and the State Administration of Traditional Chinese Medicine 2022 National Famous Old Chinese Medicine expert Inheritance Studio construction project for their support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2023.1257660/full#supplementary-material
References
Aminizadeh M., Tirgari B., Rashtabadi O. R., Jahani Y., Tajadini H. (2023). Effectiveness of auricular acupressure on constipation and related quality of life among the older people in the residential care home: a randomized clinical trial. Bmc Geriatr. 23, 171. doi:10.1186/s12877-023-03881-7
Bao N., Wang Q., Jia Y. J., Yang K., Kong L. J., Sun Y. H., et al. (2017). Research of characteristics of stimulation methods and application of acupoint in auricular needle therapy based on data mining. Zhen Ci Yan Jiu 42, 372–376. doi:10.13702/J.1000-0607.2017.04.018
Barberio B., Judge C., Savarino E. V., Ford A. C. (2021). Global prevalence of functional constipation according to the rome criteria: a systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 6, 638–648. doi:10.1016/S2468-1253(21)00111-4
Breit S., Kupferberg A., Rogler G., Hasler G. (2018). Vagus nerve as modulator of the brain-gut axis in psychiatric and inflammatory disorders. Front. Psychiatry 9, 44. doi:10.3389/fpsyt.2018.00044
Camilleri M., Subramanian T., Pagan F., Isaacson S., Gil R., Hauser R. A., et al. (2022). Oral ent-01 targets enteric neurons to treat constipation in Parkinson disease: a randomized controlled trial. Ann. Intern Med. 175, 1666–1674. doi:10.7326/M22-1438
Chen C. Y., Lin X. X., Wang X. (2018a). Efficacy of non-invasive auricular acupressure for treating constipation in leukemia patients undergoing chemotherapy: a systematic review. Complement. Med. Res. 25, 406–412. doi:10.1159/000491693
Chen J., Li F., Han W. Y., Ju X. M. (2021). Automatic consistency assurance for literature-based gene ontology annotation. Chin. J. Sch. Health 42, 565–568. doi:10.1186/s12859-021-04479-9
Chen J. H., Hou L. M. (2016). Curative effect and health economics comparison of combining ear acupuncture point buries bean with health education in the treatment of elderly hypertensive patients with functional constipation. J. Sichuan Traditional Chin. Med. 34, 203–205.
Chen Y. F., Zhan X. L., Chen X. H. (2012). Clinical nursing observation of the improvement of constipation due to Qi deficiency in the elderly through auricular-bean embedding. Fujian J. Traditional Chin. Med. 43, 62. doi:10.13260/j.cnki.jfjtcm.010354
Cumpston M., Li T., Page M. J., Chandler J., Welch V. A., Higgins J. P., et al. (2019). Updated guidance for trusted systematic reviews: a new edition of the cochrane handbook for systematic reviews of interventions. Cochrane Database Syst. Rev. 10, ED000142. doi:10.1002/14651858.ED000142
Daniali M., Nikfar S., Abdollahi M. (2020). An overview of interventions for constipation in adults. Expert Rev. Gastroenterol. Hepatol. 14, 721–732. doi:10.1080/17474124.2020.1781617
Drossman D. A. (2016). Functional gastrointestinal disorders: history, pathophysiology, clinical features and rome iv. Gastroenterology 150, 1262–1279.e2. doi:10.1053/j.gastro.2016.02.032
Drossman D. A. (1999). The functional gastrointestinal disorders and the rome ii process. Gut 45 (2), I1–I5. doi:10.1136/gut.45.2008.ii1
Drossman D. A. (2006). The functional gastrointestinal disorders and the rome iii process. Gastroenterology 130, 1377–1390. doi:10.1053/j.gastro.2006.03.008
Du B. L., Xu Z. M. (2018). Clinical observation on 30 cases of asthenia constipation of lung and spleen treated with auricular acupoint pressing. Chin. Community Dr. 34, 101–102. doi:10.3969/j.issn.1007-614x.2018.09.063
Fu J. R., Li Y. L., Wu S. F. (2021). Effect of auricular bean embedding therapy on constipation in elderly patients undergoing hemodialysis. Shenzhen J. Integr. Traditional Chin. West. Med. 31, 71–73. doi:10.16458/j.cnki.1007-0893.2021.10.032
Guyatt G. H., Oxman A. D., Schunemann H. J., Tugwell P., Knottnerus A. (2011). Grade guidelines: a new series of articles in the journal of clinical epidemiology. J. Clin. Epidemiol. 64, 380–382. doi:10.1016/j.jclinepi.2010.09.011
Hu J., Gu W. P., Zhai M., Liang Y., Tang X., Chen K. (2014). Stent placement for treatment of long-segment (≥40 mm) carotid atherosclerotic stenosis: results and long-term follow-up in a single-center experience. J. Extern. Ther. Traditional Chin. Med. 23, 32–36. doi:10.1016/j.clineuro.2014.06.025
Huang R. (2016). Clinical study on the curative effect of auricular-point-pressing therapy with heat colon dryness type constipation. J. Pract. Traditional Chin. Intern. Med., 20–22. doi:10.13729/j.issn.1671-7813.2016.10.09
Izzo A. A., Hoon-Kim S., Radhakrishnan R., Williamson E. M. (2016). A critical approach to evaluating clinical efficacy, adverse events and drug interactions of herbal remedies. Phytother. Res. 30, 691–700. doi:10.1002/ptr.5591
Ji J., Ren S. L., Wang Y. W. (2015). Effect observation of auricular-plaster therapy in the treatment of constipation in the acute stage of stroke. Beijing J. Traditional Chin. Med. 34, 661–663. doi:10.16025/j.1674-1307.2015.08.024
Ji J., Wang Y. W., Ren S. L. (2016). Therapeutic observation of auricular point sticking plus basic nursing for constipation of excessive syndrome in acute stage of stroke. Shanghai J. Acupunct. Moxibustion 35, 276–278. doi:10.13460/j.issn.1005-0957.2016.03.0276
Jie Y., Jiang Y. Q., Xu A. H. (2021). Clinical research of auricular pellet acupressure on constipation in patients with chronic schizophrenia. Hebei J. Traditional Chin. Med. 43, 843–846. doi:10.3969/j.issn.1002-2619.2021.05.030
Jing X., Liu J., Wang C., Ji M., Chen X., Mei Y., et al. (2018a). Auricular acupressure is an alternative in treating constipation in leukemia patients undergoing chemotherapy: a systematic review and meta-analysis. Complement. Ther. Clin. Pract. 31, 282–289. doi:10.1016/j.ctcp.2018.03.005
Jung E. S., Chang A. K. (2020). Effects of auricular acupressure in patients on hemodialysis. J. Nurs. Res. 28, e106. doi:10.1097/jnr.0000000000000378
Li M. K., Lee T. F., Suen K. P. (2014). Complementary effects of auricular acupressure in relieving constipation symptoms and promoting disease-specific health-related quality of life: a randomized placebo-controlled trial. Complement. Ther. Med. 22, 266–277. doi:10.1016/j.ctim.2014.01.010
Li W., Jia L., Zhao X., Wu X., Tang H. (2018). Efficacy and safety of tenofovir in preventing mother-to-infant transmission of hepatitis B virus: a meta-analysis based on 6 studies from China and 3 studies from other countries. J. Clin. Med. 5, 121–122. doi:10.1186/s12876-018-0847-2
Liu H. Q., Jiang P. Y. (2017). Curative effect observation of seed-embedding at otopoints treating constipation after thoracolumbar compression fracture. China Mod. Med. 24, 120–122. doi:10.3969/j.issn.1674-4721.2017.36.039
Liu J. X., Sun Y. H., Zhang X., Du Y. Z., Jia C. S., Li X. F. (2021). Research status and thinking of auricular acupuncture theory. Zhen Ci Yan Jiu 46, 893–900. doi:10.13702/j.1000-0607.20210412
Liu S. Y., Lin F., Wang L. L. (2011). Clinical observation of Chen Yifeng, Zhan Xulan, Chen Xuehua auricular acupressure pills in the treatment of functional constipation. Chin. General Pract. Nurs. 9, 210–211. doi:10.3969/j.issn.1674-4748.2011.03.015
Liu X. J. (2018). Clinical observation on auricular acupressure treatment of functional constipation of liver Qi stagnation thesis. Hubei. Hubei University of Chinese Medicine.
Page M. J., McKenzie J. E., Bossuyt P. M., Boutron I., Hoffmann T. C., Mulrow C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71. doi:10.1136/bmj.n71
Qian A. P. (2012). Treatment of 42 patients with subarachnoid hemorrhage and constipation using auricular acupressure. Chin. J. Traditional Med. Sci. Technol. 19, 469–470. doi:10.3969/j.issn.1005-7072.2012.05.063
Qu C. X., Ye Y. F. (2016). Effect observation of auricular acupressure combined with lactulose in the treatment of opioid-induced constipation. Chin. J. Woman Child Health Res., 567–568.
Rao S., Quigley E., Chey W. D., Sharma A., Lembo A. J. (2023). Randomized placebo-controlled phase 3 trial of vibrating capsule for chronic constipation. Gastroenterology 164, 1202–1210.e6. doi:10.1053/j.gastro.2023.02.013
Rao S. S., Seaton K., Miller M. J., Schulze K., Brown C. K., Paulson J., et al. (2007). Psychological profiles and quality of life differ between patients with dyssynergia and those with slow transit constipation. J. Psychosom. Res. 63, 441–449. doi:10.1016/j.jpsychores.2007.05.016
Salari N., Ghasemianrad M., Ammari-Allahyari M., Rasoulpoor S., Shohaimi S., Mohammadi M. (2023). Global prevalence of constipation in older adults: a systematic review and meta-analysis. Wien Klin Wochenschr. 135, 385. doi:10.1007/s00508-023-02156-w
Serra J., Pohl D., Azpiroz F., Chiarioni G., Ducrotte P., Gourcerol G., et al. (2020). European society of neurogastroenterology and motility guidelines on functional constipation in adults. Neurogastroenterol. Motil. 32, e13762. doi:10.1111/nmo.13762
Shen J. J., Wang X. D., Zhang Y. L. (2015). Effect of auricular-plaster therapy on constipation in patients with maintenance hemodialysis. J. Nursing(China), 62–64. doi:10.16460/j.issn1008-9969.2015.01.062
Shi X., Hu Y., Zhang B., Li W., Chen J. D., Liu F. (2021). Ameliorating effects and mechanisms of transcutaneous auricular vagal nerve stimulation on abdominal pain and constipation. JCI Insight 6, 6. doi:10.1172/jci.insight.150052
Shin J., Park H. (2018). Effects of auricular acupressure on constipation in patients with breast cancer receiving chemotherapy: a randomized control trial. West J. Nurs. Res. 40, 67–83. doi:10.1177/0193945916680362
Vriesman M. H., Koppen I., Camilleri M., Di Lorenzo C., Benninga M. A. (2020). Management of functional constipation in children and adults. Nat. Rev. Gastroenterol. Hepatol. 17, 21–39. doi:10.1038/s41575-019-0222-y
Wang L. J. (2019). Nursing observation of functional constipation of Alzheimer's disease treated with ear embedding beans. Shanxi J. Traditional Chin. Med. 35, 61–62. doi:10.3969/j.issn.1000-7156.2019.02.026
Wang W., Liu Y., Yang X., Sun J., Yue Z., Lu D., et al. (2023). Effects of electroacupuncture for opioid-induced constipation in patients with cancer in China: a randomized clinical trial. JAMA Netw. Open 6, e230310. doi:10.1001/jamanetworkopen.2023.0310
Wang X., Chen Y., Liu Y., Yao L., Estill J., Bian Z., et al. (2019). Reporting items for systematic reviews and meta-analyses of acupuncture: the prisma for acupuncture checklist. BMC Complement. Altern. Med. 19, 208. doi:10.1186/s12906-019-2624-3
Wang X. X., Liu X., Ke M. H. (2020). Clinical observation on auricular point sticking therapy for functional constipation combined with anxiety. Chin. Med. Mod. Distance Educ. China 18, 89–91. doi:10.3969/j.issn.1672-2779.2020.10.036
Wang Z. Y., Wang X. X., Jiao W. N., Hua S. W. (2022). Observation on therapeutic effect of auricular acupoint pressing in the treatment of community elderly functional constipation. Guangming J. Chin. Med. 37, 844–846. doi:10.3969/j.issn.1003-8914.2022.05.039
Wu H. J., Ren H. L., Wang Y., Lin C., Zhang Y. (2021). Therapeutic effect of ear acupoint pressing beans combined with comprehensive intervention in patients with constipation after craniocerebral surgery. J. Logist. Univ. PAP Med. Sci. 30, 72–74. doi:10.16548/j.2095-3720.2021.11.056
Xu H. M., Liu C. X., Wang C. X. (2013). Observation of therapeutic efficacy of auricular acupressure on constipation in 40 cases of stroke. Clin. J. Traditional Chin. Med., 1003–1004. doi:10.16448/j.cjtem.2013.11.014
Xu W. (2019). Observation on the treatment of functional defecation disorder due to spleen and lung deficiency with ear acupuncture point sticking the seed of vaccaria and biofeedback therapy [thesis]. Anhui University of Chinese Medicine. doi:10.26922/d.cnki.ganzc.2019.000186
Xu Y. Y. (2023). Clinical observation of auricular point compression bean in treating constipation caused by clozapine in patients with schizophrenia. Guide China Med. 21, 123–125. doi:10.15912/j.cnki.gocm.2023.11.050
Yang L. H., Duan P. B., Xu Y. N., Hou Q. M., Mei S. J., Wang X. Q., et al. (2014). Effect evaluation of auricular plaster therapy based on the pattern/syndrome differentiation in patients with constipation induced by strong opioid drugs for pain. Chin. J. Pract. Nurs. 30, 4–7. doi:10.3760/cma.j.issn.1672-7088.2014.05.002
Yang L. J., Fu S. D. (2013). Effect analysis of auricular acupressure treatment for constipation after elderly hip fracture. Chin. J. Traditional Med. Traumatology Orthop. 21, 58–59.
Yang X. Y., Shi G. X., Li Q. Q., Zhang Z. H., Xu Q., Liu C. Z. (2013). Characterization of deqi sensation and acupuncture effect. Evid. Based Complement. Altern. Med. 2013, 319734. doi:10.1155/2013/319734
Ye Z., He X. Y. (2014). Exploration of nursing effects of auricular acupressure on improving constipation in elderly patients with schizophrenia. Today Nurse · Spec. Ed., 123–124.
Zhang Y. (2009). Ear treatment of senile habitual constipation [thesis]. Shandong University of Traditional Chinese Medicine.
Zhang Y., Lu T., Meng Y., Maisiyiti A., Dong Y., Li S., et al. (2021). Auricular vagal nerve stimulation improves constipation by enhancing colon motility via the central-vagal efferent pathway in opioid-induced constipated rats. Neuromodulation 24, 1258–1268. doi:10.1111/ner.13406
Zhao Y. H., Wang H. Y. (2022). Analysis of application effect of auricular acupoint pressing bean combined nursing measures in constipation after stroke. Reflexology Rehabilitation Med. 3, 1–4.
Zhong X. (2007). Clinical study on auricular point sticking in the treatment of colon slow transit constipation with deficiency of lung-spleen qi thesis. Beijing. Beijing University of Chinese Medicine.
Keywords: auricular acupressure, constipation, effectiveness, meta-analysis, systematic review
Citation: Jiang Z-F, Liu G, Sun X-X, Zhi N, Li X-M, Sun R and Zhang H (2023) Auricular acupressure for constipation in adults: a systematic review and meta-analysis. Front. Physiol. 14:1257660. doi: 10.3389/fphys.2023.1257660
Received: 13 July 2023; Accepted: 03 October 2023;
Published: 16 October 2023.
Edited by:
Rüdiger Christoph Pryss, Julius Maximilian University of Würzburg, GermanyReviewed by:
HuangHsi Chen, Chung Shan Medical University Hospital, TaiwanWinfried Schlee, University of Regensburg, Germany
Copyright © 2023 Jiang, Liu, Sun, Zhi, Li, Sun and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Zhang, aHpoYW5nMDEyM0Bmb3htYWlsLmNvbQ==