
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol., 02 May 2023
Sec. Vascular Physiology
Volume 14 - 2023 | https://doi.org/10.3389/fphys.2023.1139658
This article is part of the Research TopicCerebral Blood Flow Hemodynamics and Cerebral Spinal Fluid Dynamics using Multi-Modality Monitoring in Neurological Intensive CareView all 9 articles
 Alberto Giardina1†Danilo Cardim2,3†Pietro Ciliberti1†
Alberto Giardina1†Danilo Cardim2,3†Pietro Ciliberti1† Denise Battaglini4
Denise Battaglini4 Lorenzo Ball1,4
Lorenzo Ball1,4 Magdalena Kasprowicz5Erta Beqiri6Peter Smielewski6Marek Czosnyka6,7Shirin Frisvold8
Magdalena Kasprowicz5Erta Beqiri6Peter Smielewski6Marek Czosnyka6,7Shirin Frisvold8 Matjaž Groznik9Paolo Pelosi1,4
Matjaž Groznik9Paolo Pelosi1,4 Chiara Robba1,4*‡
Chiara Robba1,4*‡Background: Cerebral autoregulation is the mechanism that allows to maintain the stability of cerebral blood flow despite changes in cerebral perfusion pressure. Maneuvers which increase intrathoracic pressure, such as the application of positive end-expiratory pressure (PEEP), have been always challenged in brain injured patients for the risk of increasing intracranial pressure (ICP) and altering autoregulation. The primary aim of this study is to assess the effect of PEEP increase (from 5 to 15 cmH2O) on cerebral autoregulation. Secondary aims include the effect of PEEP increase on ICP and cerebral oxygenation.
Material and Methods: Prospective, observational study including adult mechanically ventilated patients with acute brain injury requiring invasive ICP monitoring and undergoing multimodal neuromonitoring including ICP, cerebral perfusion pressure (CPP) and cerebral oxygenation parameters obtained with near-infrared spectroscopy (NIRS), and an index which expresses cerebral autoregulation (PRx). Additionally, values of arterial blood gases were analyzed at PEEP of 5 and 15 cmH2O. Results are expressed as median (interquartile range).
Results: Twenty-five patients were included in this study. The median age was 65 years (46–73). PEEP increase from 5 to 15 cmH2O did not lead to worsened autoregulation (PRx, from 0.17 (−0.003–0.28) to 0.18 (0.01-0.24), p = 0.83). Although ICP and CPP changed significantly (ICP: 11.11 (6.73–15.63) to 13.43 (6.8–16.87) mm Hg, p = 0.003, and CPP: 72.94 (59.19–84) to 66.22 (58.91–78.41) mm Hg, p = 0.004), these parameters did not reach clinically relevant levels. No significant changes in relevant cerebral oxygenation parameters were observed.
Conclusion: Slow and gradual increases of PEEP did not alter cerebral autoregulation, ICP, CPP and cerebral oxygenation to levels triggering clinical interventions in acute brain injury patients.
A large number of patients with brain damage require mechanical ventilation when admitted to the intensive care unit (ICU). The goal of mechanical ventilation is to optimize oxygen delivery and minimize lung and brain injury (Frisvold et al., 2019). The use of lung-protective ventilation strategies has been shown to reduce morbidity and mortality in critically ill patients (Sutherasan et al., 2014; Serpa Neto et al., 2015; Simonis et al., 2018). However, no specific recommendations are available on the optimal levels of positive end expiratory pressure (PEEP) to be applied in patients with acute brain injury (Robba et al., 2020).
PEEP can potentially cause an increase in intrathoracic pressures leading to a reduction in cerebral venous outflow and a consequent increase in intracranial pressure (ICP) and hemodynamic instability with reduction of cerebral perfusion pressure (CPP). On the other hand, alveolar overdistension can lead to an increase in arterial partial pressure of carbon dioxide (PaCO2) resulting in cerebral vasodilation. Thus, strategies involving the use of elevated PEEP are still controversial in brain-injured patients (Nemer et al., 2011; Borsellino et al., 2016; Robba et al., 2020). Previous studies from our group (Robba et al., 2021a; Robba et al., 2022) demonstrated that even high testing values of PEEP can be safe for ICP, as long as it promotes lung recruitment and improves lung compliance without causing hypotension. However, the effects of PEEP increase on more complex cerebral parameters such as cerebral autoregulation or cerebral oxygenation have not been completely elucidated. Assessment of these parameters is gaining particular interest in the context of multimodal monitoring of neurocritical care patients, as autoregulation impairment and brain hypoxia can reduce the tolerance to increased ICP, and can be associated with worse outcomes (Aries et al., 2012; Tas et al., 2021).
We therefore conducted a prospective observational study with the objective to evaluate cerebral hemodynamics including cerebral autoregulation, cerebral oxygenation and ICP using a brain multimodal monitoring approach at two different levels of PEEP in a cohort of acute brain injured patients.
This is a prospective, observational study including adult mechanically ventilated brain injured patients requiring invasive ICP monitoring. The local ethics review board (Comitato Etico Regione Liguria, protocol n. CER Liguria: 23/2020) approved this study, and written consent was obtained from patients’ next of kin. We adhered to the “Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)” statement guidelines for observational cohort studies (von Elm et al., 2014) (Additional file 1: ESM Supplementary Table S1).
Patients were screened for inclusion from 1 February 2021 to 1 September 2022 at San Martino Policlinic Hospital, IRCCS for Oncology and Neurosciences, Genoa, Italy, and were considered eligible if they were 1) older than 18 years-old; 2) admitted to ICU for acute brain injury, i.e., traumatic brain injury (TBI), subarachnoid hemorrhage (SAH) or intracranial hemorrhage (ICH); 3) required invasive ICP monitoring and mechanical ventilation at ICU admission, and 4) underwent multimodal neuromonitoring (according to clinical severity and based on bed availability) including ICP, cerebral autoregulation and cerebral oxygenation during a PEEP test from 5 to 15 cmH2O. Our unit is a mixed general and neuro-ICU, composed of 28 level 3 beds, of which 12 are equipped with ICM + software. Patients without multimodal neuromonitoring, not mechanically ventilated or those patients whose next of kins refused to agree about inclusion in the study were excluded.
Electronic medical records were used to collect patients’ information, and included admission demographics (e.g., age, sex, body mass index (BMI), pre-injury comorbidities (respiratory, cardiovascular, liver and kidney disease, cancer, diabetes mellitus and hypertension), reason for ICU admission (TBI, SAH, ICH), neurological status at admission as for Glasgow coma scale (GCS) and pupils characteristics (reactivity, iso or anisocoria), ICU complications (acute distress respiratory syndrome (ARDS), ventilator-associated pneumoniae, acute kidney injury, sepsis, vasospasm) and patients’ clinical outcomes, such as ICU length of stay, number of days with mechanical ventilation, ICU mortality and neurological status (as for Glasgow Outcome Score-Extended (GOSE)), type of ICP monitoring (intraparenchymal or external ventricular drain).
Data on ventilatory mechanics, i.e., tidal volume, plateau pressure, and arterial blood gases (partial pressure of oxygen (PaO2) and of carbon dioxide (PaCO2) and multimodal neuromonitoring data before and after PEEP test were also collected.
In the ICU, patients were sedated with propofol (3–6 mg/kg/h) and/or midazolam (0.03–0.2 mg/kg/h) and fentanyl (0.1–0.8 μg/kg/min), intubated and mechanically ventilated in pressure or volume-controlled ventilation. Tidal volume was targeted to 6–8 mL per kg of predicted body weight (PBW), but higher values of tidal volume were tolerated, if driving pressure was maintained below 15 cmH2O. Invasive ICP monitoring was inserted according to our local policies and clinical practice, following latest Brain Trauma Foundation Guidelines (Carney et al., 2017), as well as patients’ clinical management.
The decision to perform a PEEP test was based on clinicians’ evaluation if optimization of mechanical ventilation was required, to set the best PEEP level, according to local protocol (Robba et al., 2022) and our previous experience.
PEEP test was performed in volume-controlled ventilation in all patients, without using neuromuscular blockade. PEEP was slowly increased from 5 to 15 cmH2O, about 2 cmH2O every minute, evaluating the changes in respiratory mechanics and cerebral hemodynamics, with the aim to set the best PEEP value. Our local protocol is based on our previous clinical experience which suggested that these PEEP values are safe in brain injured patients (Robba et al., 2021a), and on a recent consensus on mechanical ventilation in brain injured patients, which suggested to use the same level of PEEP applied in the non-brain injured population (Robba et al., 2020).
Data were obtained at PEEP of 5 (T0) and at 15 cmH2O (T1) after allowing 5 min for stabilization, as previously described (Cressoni et al., 2017), and the chosen levels of PEEP (5 and 15 cmH2O) represent the standard levels of PEEP used to estimate response to PEEP in general ICU patients (Gattinoni et al., 2006).
Data collected at T0 and T1 included respiratory mechanics and arterial blood gases parameters including arterial partial pressure of oxygen (PaO2) and of carbon dioxide (PaCO2), tidal volume (VT), plateau pressure (Pplat), respiratory system compliance (CRS), driving pressure (DP), arterial saturation of oxygen (SaO2), as well as neuromonitoring data, i.e., ICP, pressure reactivity index (PRx, as means for cerebral autoregulation assessment), and data on cerebral oxygenation derived from near-infrared spectroscopy (NIRS).
Intracranial pressure was monitored continuously with a transducer into the brain parenchymal space or through an external cerebral fluid shunt, according to clinical practice. Arterial blood pressure was monitored in the radial or femoral artery zeroed at the level of the right atrium (Baxter Healthcare, CA, United States; Sidcup, United Kingdom). In patients with head elevation, no corrections were made for hydrostatic pressure differences.
For the assessment of cerebral oxygenation, we used non-invasive continuous regional cerebral oxygen saturation using the Root® with O3® regional oximetry device (Masimo, Irvine, CA, United States), with a bilateral sensor applied in the frontotemporal region. Final values of cerebral oxygenation measurements at T0 and T1 were calculated as the mean between single instant measurements obtained from the right and left frontotemporal sensors. Different parameters of cerebral oxygenation can be obtained from this monitor: a) rSO2, which represents the regional cerebral oxygen saturation, and is derived as the ratio of the concentration of oxyhemoglobin (O2Hb) and total hemoglobin (cHb = O2Hb + HHb, where HHb is deoxyhemoglobin); b) ΔO2Hbi, which is an index associated with changes of concentration of oxyhemoglobin, thus representing predominantly changes in the arterial component of regional oxygen saturation; c) ΔHHbi, an index reflecting changes in concentration of deoxyhemoglobin, approximately representing changes in the venous component of the oxygen saturation; d) ΔcHbi, an index representing the sum of ΔO2Hbi and ΔHHbi components (total hemoglobin content) (Gattinoni et al., 2006; Robba et al., 2021a).
All continuous physiological data were collected simultaneously and analyzed using ICM+ (Cambridge Enterprise, Cambridge, United Kingdom, https://icmplus.neurosurg.cam.ac.uk) (Smielewski et al., 2005), a clinical research software which can provide real-time analysis of multimodal monitoring modalities at the patient’s bedside. Data collected with ICM+ were sampled at 100 Hz. Artifacts were visually inspected and manually removed from the data time series using artifact removal tools on ICM+. Typical artifacts in the data consisted of spikes in ICP due to suction, or arterial line flushes. Cerebral autoregulation assessed through PRx and calculated over a 5-min moving window as the Pearson correlation of 30 consecutive 10-s average values of ABP and ICP as previously described (Czosnyka et al., 1997). A preserved autoregulation was defined as values of PRx below 0.05 averaged over a 10-min period, whereas higher values (above 0.25) are defined as altered autoregulation (Sorrentino et al., 2012). PRx was calculated from T0 (averaged value of a 10-min period before PEEP increase) and T1 (averaged value of a 10-min period immediately after PEEP increase to 15 cmH2O) periods.
The Shapiro-Wilk test was used to test the normality of the distribution of the variables. Continuous variables are reported as median and interquartile range (IQR = 25th −75th percentiles). Comparisons between different variables at T0 and T1 were made by repeated measures (paired) t-test for normally distributed variables, while non-normally distributed variables were compared by paired Wilcoxon signed-rank test. Graphical representations of these comparisons are presented as boxplots. Dependent variables were expressed as a change from baseline (T0) in absolute terms (Δ change = T1-T0). The correlations coefficients between systemic and the different neuromonitoring variables were verified using Pearson’s or Spearman’s method, for parametric and non-parametric variables, respectively. All statistical analyses were performed using RStudio software (version 4.1.1). A p-value <0.05 was considered statistically significant.
During the study period, a total of 110 patients were considered for inclusion. Fifty-two patients were excluded as they did not undergo multimodal neuromonitoring and 33 patients were not allocated to a specific bed with ICM+. A final number of 25 patients were included in the analysis. The characteristics of the patients are presented in Table 1. 60% were male, and the median age was 64.7 years (45.9-73.2). Thirteen patients (52%) were admitted for TBI, 7 (28%) for SAH, and 5 (20%) patients for ICH. Six patients (24%) had a history of hypertension. At ICU discharge, median GOSE was 3 (1.8-4.0), and 5 patients died (20%).
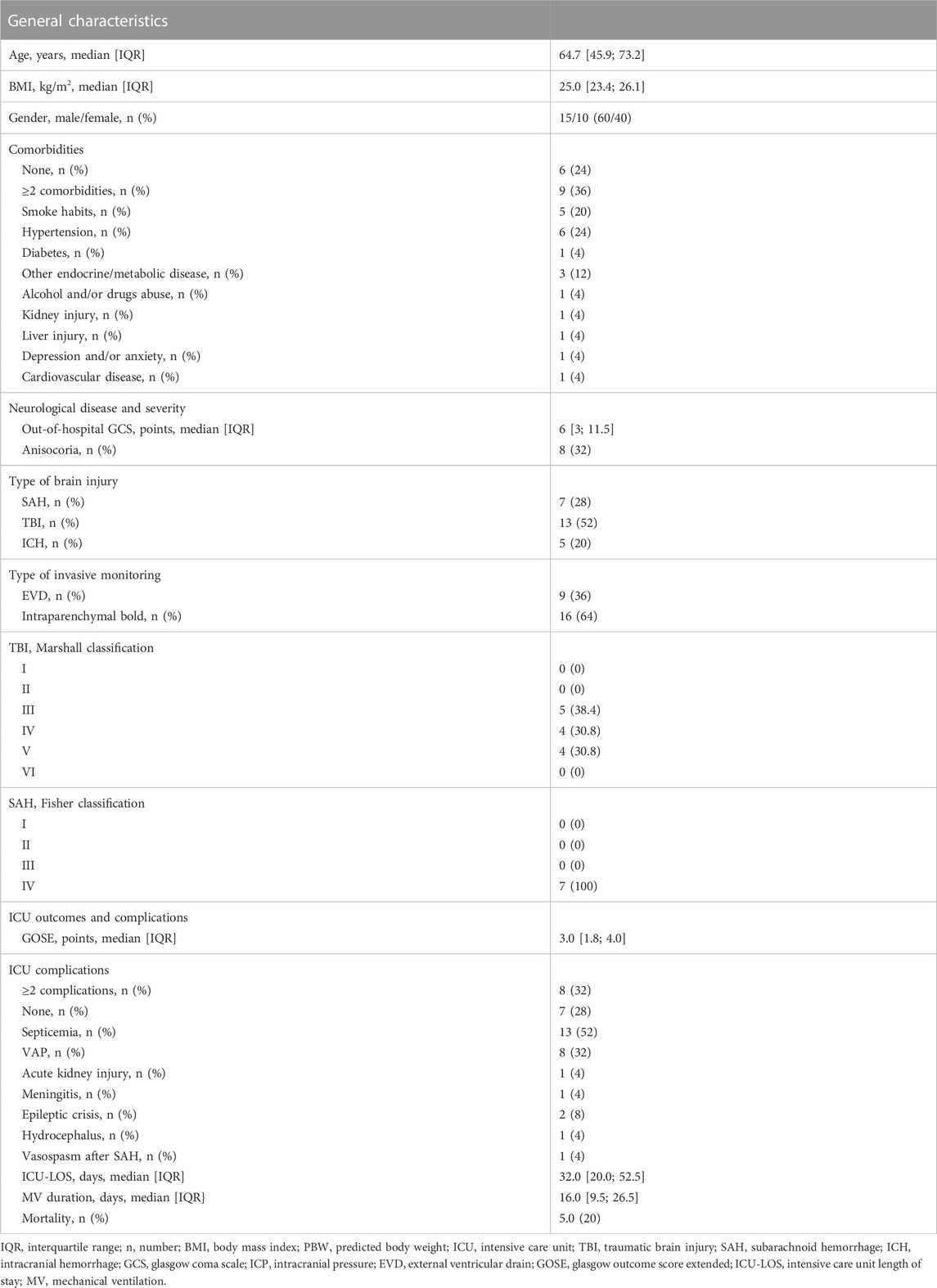
TABLE 1. Patients demographics, characteristics, intensive care unit (ICU) complications and patient outcomes.
After PEEP test, changes in PRx were not statistically significant, from 0.17 (−0.003-0.28) to 0.18 (0.01–0.24), p = 0.83, Table 2; Figure 1).
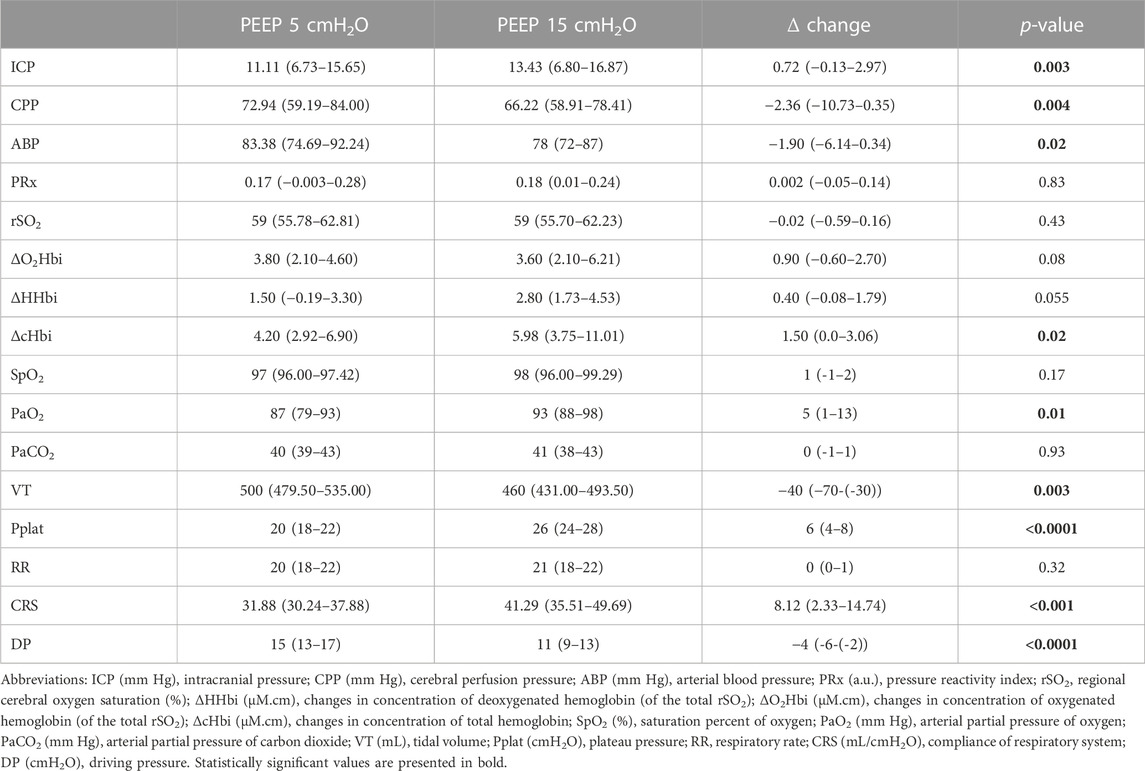
TABLE 2. Neuromonitoring and systemic parameters at baseline (PEEP 5 cmH2O) and post-PEEP test (PEEP 15 cmH2O) (median (interquartile range)).
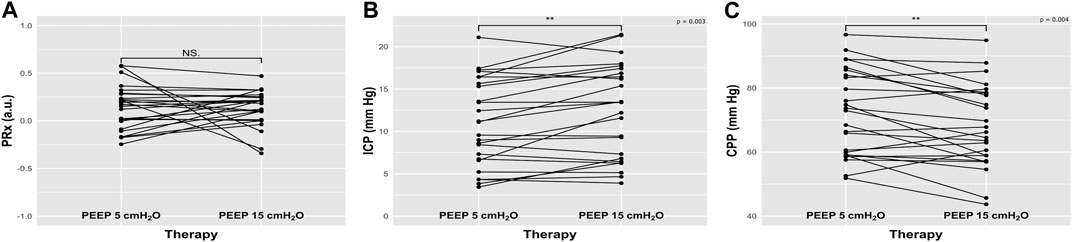
FIGURE 1. Plots representing the effect of increased positive end-expiratory pressure (PEEP) on cerebral autoregulation measured with pressure reactivity test (PRx), intracranial pressure (ICP), and cerebral perfusion pressure (CPP) from baseline. NS: not statistically significant; **: p < 0.01.
ICP significantly changed (from 11.11 (6.73–15.63) mm Hg to 13.43 (6.8–16.87) mm Hg, p = 0.003, as well as ABP and CPP (from 83.38 (74.69–92.24) to 78 (72–87) mm Hg, p = 0.02, and from 72.94 (59.19–84) mm Hg to 66.22 (58.91–78.41) mm Hg, p = 0.004, respectively) (Table 2; Figure 1). On the other hand, no changes in cerebral oxygenation parameters were observed from T0 to T1 (Table 2; Figure 2), apart from the changes in total hemoglobin content (ΔcHbi) (Table 2).
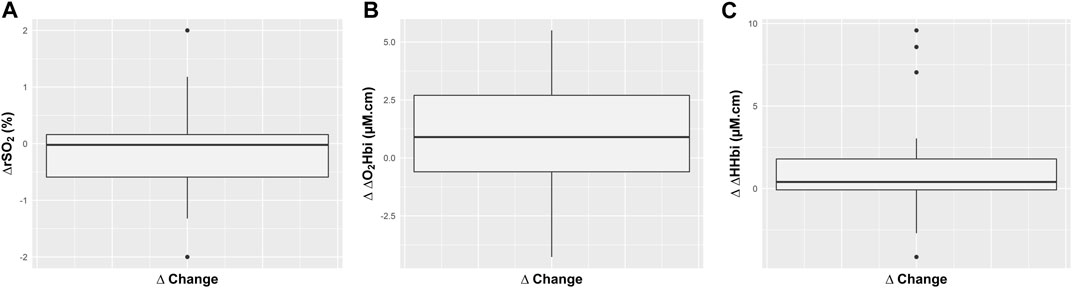
FIGURE 2. Boxplots representing the effect of increased positive end-expiratory pressure (PEEP) on absolute changes (∆) in regional cerebral oxygen saturation (rSO2), and in the arterial (ΔO2Hbi) and venous (ΔHHbi) components of cerebral oxygenation.
Systemic PaO2 also increased, from 87 (79–93) to 93 (88-98) mm Hg, p = 0.03), without causing changes in PaCO2 (from 40 (39-43) to 41 (38–43) mm Hg, p = 0.89) (Table 2).
Considering ventilatory settings, PEEP increase led to reduced tidal volume (500 (479–535) to 460 (431.00–493.50) mL, p = 0.003), increased plateau pressure (20 (18-22) to 26 (24-28) cmH2O, p < 0.0001), reduced driving pressure (15 (13–17) to 11 (9–13) cmH2O, p < 0.0001), and improvement of respiratory system compliance (from 31.88 (30.24–37.88) to 41.29 (35.51–49.69) mL/cmH2O, p < 0.001) (Table 2).
No significant correlations were observed between the changes in ICP and other parameters (Table 3), except with CPP and ABP (r = −0.71, p < 0.0001, and r = −0.48, p = 0.01) (Figure 3). Changes in compliance of respiratory system were correlated with ΔO2Hbi (r = 0.44, p = 0.03).
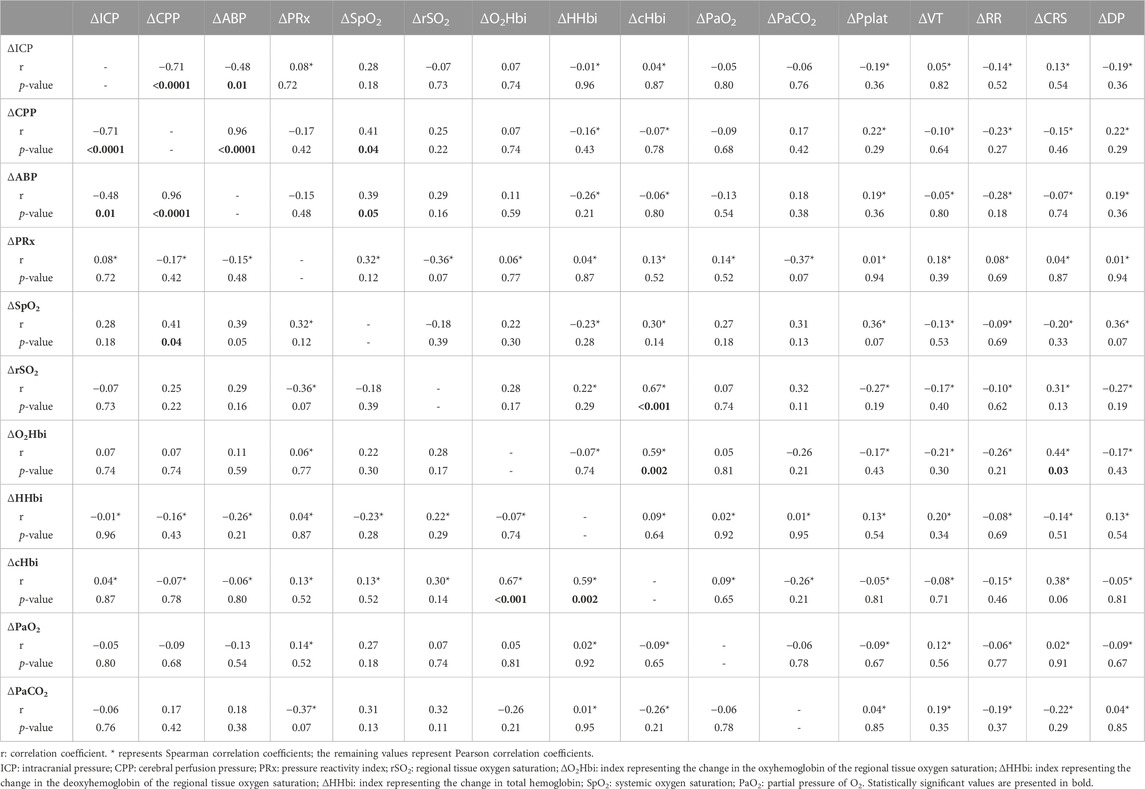
TABLE 3. Correlation matrix between changes (Δ) in systemic, ventilatory and neuromonitoring parameters.
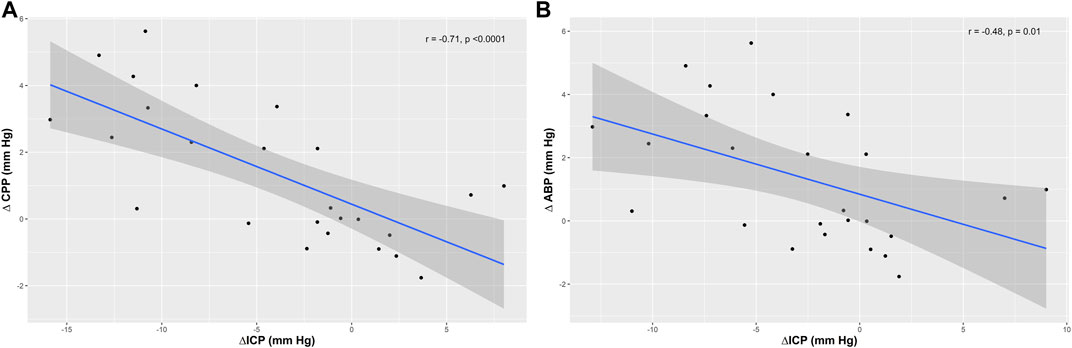
FIGURE 3. Scatter plots showing the correlation (r) between changes in intracranial pressure (ΔICP) and (A) cerebral perfusion pressure (ΔCPP), and (B) mean arterial blood pressure.
In our cohort of mechanically ventilated brain injured patients we found that: 1) ICP, CPP and ABP significantly changed after the PEEP test, however, PEEP increase did not worsen PRx; 2) No changes in cerebral oxygenation parameters related to arterial or venous components were observed; 3) There was an increase of systemic PaO2, without causing changes in PaCO2. Respiratory system compliance was improved.
The use of high PEEP has been challenged in the ABI population, as it can potentially increase intrathoracic pressure, reduce jugular vein outflow, decrease venous return, and lead to a drop in cardiac output and blood pressure. This may potentially cause hemodynamic instability with consequent detrimental effects on CPP and cerebral blood flow. When cerebral autoregulation is intact, extreme reduction of CPP can lead to cerebral vasodilation and an increase in cerebral blood volume that can potentially exacerbate ICP; on the other hand, when autoregulation is impaired, decreased CPP may lead to cerebral ischemia (Calviello et al., 2017). The transmission of PEEP into the thoracic cavity is variable and dependent on the properties of the chest wall and lungs. Some studies suggest that when the chest wall compliance is low, PEEP significantly increases intrathoracic pressure, and if PEEP does not lead to recruitment but causes alveolar hyperdistention, this can magnify the effect of PEEP and intrathoracic pressure on ICP (Burchiel et al., 1981; Robba et al., 2021a).
A multimodal approach for the assessment of cerebral hemodynamics, especially cerebral autoregulation, is therefore of great interest, and warrants clinical relevance in this context. We assessed a heterogeneous group of patients with ABI at fixed PEEP levels of 5 cmH2O and 15 cmH2O using hemodynamic parameters and recorded cerebral and respiratory function parameters. After the PEEP test, we observed an increase of PaO2 and improvement of CRS. PEEP increase in our cohort did not lead to increase of PaCO2 and the effect on cerebral physiological parameters was minimal, with no significative changes in autoregulation. These preliminary results suggest that an increase in PEEP within the proposed range might be a safe maneuver in patients with ABI, provided this improves respiratory mechanics and does not affect importantly hemodynamic status.
Survival after ABI is dependent on the control of intracranial hypertension and the provision of hemodynamic support to achieve an appropriate cerebral perfusion pressure (Robba et al., 2021b). The current Brain Trauma foundation Guidelines suggest targeting CPP between 60 and 70 mm Hg after TBI (Carney et al., 2017).
However, the idea of a single value or even a single range of CPP being suitable for the diverse group of ABI patients is an oversimplification. Age, comorbidities, and pre-injury arterial blood pressure are examples of factors likely to influence individual CPP targets, with elderly, hypertensive patients requiring a higher CPP compared with young, normotensive patients. In addition, in healthy, the ability to autoregulate occurs in a very wide CPP range, but after brain injury, this ability is impaired, and the risk of secondary damage increases dramatically (Menon, 1999).
The examination of continuous autoregulation and the definition of optimal CPP, which is the CPP at which each patient autoregulates at best, requires sophisticated signal analysis. ICM + bedside software and pressure reactivity index (PRx) have already been extensively validated in the literature and allow an individualized assessment of the effect of respiratory manipulations on the brain (Donnelly et al., 2015; Donnelly et al., 2018). PRx–which represents the between changes in arterial blood pressure and intracranial pressure offers a surrogate method for the continuous bedside estimation of global cerebral autoregulation, which has been suggested to be feasible and safe (Tas et al., 2021), and is considered at present the most accurate method for individualized autoregulation assessment (Needham et al., 2017; Depreitere et al., 2021).
A multimodal approach of respiratory and cerebral parameters can therefore help with a better definition of the best individualized PEEP value to be applied in order to promote improvement of respiratory mechanics without altering cerebral dynamics.
This study has several limitations that need to be mentioned. Firstly, this is a single center study with a small sample, and heterogeneity of included patients, which limit the generalization of our results. The posteriori use of the data as presented in this study setting (e.g., the need to wait for the recording and calculation of different parameters) can potentially delay the modification of interventions in clinical practice. Only two arbitrary levels of PEEP were investigated for technical reasons and patient safety concerns, and as for our local protocols. The application of this protocol may cause physiological changes in CPP after an increase in PEEP due to a decrease in ABP or increase in right pressures above ICP. High levels of PEEP are useful in ARDS patients in whom pulmonary compliance is low; in such patients the PEEP effects on cerebral hemodynamics likely differ from the changes observed in most patients. Known limitations of NIRS, such as the potential influence of extracranial contamination (particularly in HHb and O2Hb signals), the nature of HHb and HbO2 dependent on the unknown scattering coefficient likely differing on an individual basis, and the unknown contribution of venous and arterial components to the measured signals, particularly O2Hb, are potential confounders in our study. Furthermore, we did not assess any direct measures of CBF in these patients. Finally, all patients had relatively low ICP at the moment of measurement; moreover, we cannot exclude that different ventilator settings or the addition of a recruitment maneuver may have led to different results.
In this study, PEEP increase led to improvement of respiratory system compliance, without affecting importantly systemic hemodynamics and PaCO2 values. This led to the absence of detrimental effects on cerebral autoregulation, cerebral oxygenation and intracranial pressure.
These results suggest that the use of augmented PEEP can be safe in acute brain injured patients. Our findings are in line with the current recommendations for this patient population, which suggests applying the same level of PEEP as in the general ICU population. This study also highlights the applicability and feasibility of a multimodal approach for the individualization of lung and cerebral management in future studies.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Liguria CER. The patients/participants provided their written informed consent to participate in this study.
AG, DC, MC, PS, CR, and PP planned the project. AG, PC, DB, and LB collected the data. DC and CR performed the statistical analysis. AG, DC, and CR wrote the first draft. All authors participated in the analysis and description of results, and on preparing the manuscript. All authors approved the final version.
The authors would like to thank the Italian Ministero della Salute for the support.
MC and PS are proprietary of ICMplus software. CR received fees for lectures from Masimo.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Aries, M. J., Czosnyka, M., Budohoski, K. P., Steiner, L. A., Lavinio, A., Kolias, A. G., et al. (2012). Continuous determination of optimal cerebral perfusion pressure in traumatic brain injury. Crit. Care Med. 40 (8), 2456–2463. doi:10.1097/CCM.0b013e3182514eb6
Borsellino, B., Schultz, M. J., Gama de Abreu, M., Robba, C., and Bilotta, F. (2016). Mechanical ventilation in neurocritical care patients: A systematic literature review. Expert Rev. Respir. Med. 10 (10), 1123–1132. doi:10.1080/17476348.2017.1235976
Burchiel, K. J., Steege, T. D., and Wyler, A. R. (1981). Intracranial pressure changes in brain-injured patients requiring positive end-expiratory pressure ventilation. Neurosurgery 8 (4), 443–449. doi:10.1227/00006123-198104000-00007
Calviello, L. A., Donnelly, J., Zeiler, F. A., Thelin, E. P., Smielewski, P., and Czosnyka, M. (2017). Cerebral autoregulation monitoring in acute traumatic brain injury: what's the evidence? Minerva Anestesiol. 83 (8), 844–857. doi:10.23736/s0375-9393.17.12043-2
Carney, N., Totten, A. M., O'Reilly, C., Ullman, J. S., Hawryluk, G. W. J., Bell, M. J., et al. (2017). Guidelines for the management of severe traumatic brain injury, fourth edition. Neurosurgery 80 (1), 6–15. Fourth Edition. doi:10.1227/neu.0000000000001432
Cressoni, M., Chiumello, D., Algieri, I., Brioni, M., Chiurazzi, C., Colombo, A., et al. (2017). Opening pressures and atelectrauma in acute respiratory distress syndrome. Intensive Care Med. 43 (5), 603–611. doi:10.1007/s00134-017-4754-8
Czosnyka, M., Smielewski, P., Kirkpatrick, P., Laing, R. J., Menon, D., and Pickard, J. D. (1997). Continuous assessment of the cerebral vasomotor reactivity in head injury. Neurosurgery 41 (1), 11–19. discussion 17-9. doi:10.1097/00006123-199707000-00005
Depreitere, B., Citerio, G., Smith, M., Adelson, P. D., Aries, M. J., Bleck, T. P., et al. (2021). Cerebrovascular autoregulation monitoring in the management of adult severe traumatic brain injury: A delphi consensus of clinicians. Neurocrit Care 34 (3), 731–738. doi:10.1007/s12028-020-01185-x
Donnelly, J., Aries, M. J., and Czosnyka, M. (2015). Further understanding of cerebral autoregulation at the bedside: Possible implications for future therapy. Expert Rev. Neurother. 15 (2), 169–185. doi:10.1586/14737175.2015.996552
Donnelly, J., Czosnyka, M., Adams, H., Robba, C., Steiner, L. A., Cardim, D., et al. (2018). Pressure reactivity-based optimal cerebral perfusion pressure in a traumatic brain injury cohort. Acta Neurochir. Suppl. 126, 209–212. doi:10.1007/978-3-319-65798-1_43
Frisvold, S. K., Robba, C., and Guérin, C. (2019). What respiratory targets should be recommended in patients with brain injury and respiratory failure? Intensive Care Med. 45 (5), 683–686. doi:10.1007/s00134-019-05556-7
Gattinoni, L., Caironi, P., Cressoni, M., Chiumello, D., Ranieri, V. M., Quintel, M., et al. (2006). Lung recruitment in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 354 (17), 1775–1786. doi:10.1056/NEJMoa052052
Menon, D. K. (1999). Cerebral protection in severe brain injury: Physiological determinants of outcome and their optimisation. Br. Med. Bull. 55 (1), 226–258. doi:10.1258/0007142991902231
Needham, E., McFadyen, C., Newcombe, V., Synnot, A. J., Czosnyka, M., and Menon, D. (2017). Cerebral perfusion pressure targets individualized to pressure-reactivity index in moderate to severe traumatic brain injury: A systematic review. J. Neurotrauma 34 (5), 963–970. doi:10.1089/neu.2016.4450
Nemer, S. N., Caldeira, J. B., Azeredo, L. M., Garcia, J. M., Silva, R. T., Prado, D., et al. (2011). Alveolar recruitment maneuver in patients with subarachnoid hemorrhage and acute respiratory distress syndrome: A comparison of 2 approaches. J. Crit. Care 26 (1), 22–27. doi:10.1016/j.jcrc.2010.04.015
Robba, C., Ball, L., Battaglini, D., Iannuzzi, F., Brunetti, I., Fiaschi, P., et al. (2022). Effects of positive end-expiratory pressure on lung ultrasound patterns and their correlation with intracranial pressure in mechanically ventilated brain injured patients. Crit. Care 26 (1), 31. doi:10.1186/s13054-022-03903-7
Robba, C., Ball, L., Nogas, S., Battaglini, D., Messina, A., Brunetti, I., et al. (2021). Effects of positive end-expiratory pressure on lung recruitment, respiratory mechanics, and intracranial pressure in mechanically ventilated brain-injured patients. Front. Physiol. 12, 711273. doi:10.3389/fphys.2021.711273
Robba, C., Graziano, F., Rebora, P., Elli, F., Giussani, C., Oddo, M., et al. (2021). Intracranial pressure monitoring in patients with acute brain injury in the intensive care unit (SYNAPSE-ICU): An international, prospective observational cohort study. Lancet Neurol. 20 (7), 548–558. doi:10.1016/s1474-4422(21)00138-1
Robba, C., Poole, D., McNett, M., Asehnoune, K., Bösel, J., Bruder, N., et al. (2020). Mechanical ventilation in patients with acute brain injury: Recommendations of the European society of intensive care medicine consensus. Intensive Care Med. 46 (12), 2397–2410. doi:10.1007/s00134-020-06283-0
Serpa Neto, A., Hemmes, S. N., Barbas, C. S., Beiderlinden, M., Biehl, M., Binnekade, J. M., et al. (2015). Protective versus conventional ventilation for surgery: A systematic review and individual patient data meta-analysis. Anesthesiology 123 (1), 66–78. doi:10.1097/aln.0000000000000706
Simonis, F. D., Serpa Neto, A., Binnekade, J. M., Braber, A., Bruin, K. C. M., et al. (2018). Effect of a low vs intermediate tidal volume strategy on ventilator-free days in intensive care unit patients without ARDS: A randomized clinical trial. Jama 320 (18), 1872–1880. doi:10.1001/jama.2018.14280
Smielewski, P., Czosnyka, M., Steiner, L., Belestri, M., Piechnik, S., and Pickard, J. D. (2005). ICM+: Software for on-line analysis of bedside monitoring data after severe head trauma. Acta Neurochir. Suppl. 95, 43–49. doi:10.1007/3-211-32318-x_10
Sorrentino, E., Diedler, J., Kasprowicz, M., Budohoski, K. P., Haubrich, C., Smielewski, P., et al. (2012). Critical thresholds for cerebrovascular reactivity after traumatic brain injury. Neurocrit Care 16 (2), 258–266. doi:10.1007/s12028-011-9630-8
Sutherasan, Y., Vargas, M., and Pelosi, P. (2014). Protective mechanical ventilation in the non-injured lung: Review and meta-analysis. Crit. Care 18 (2), 211. doi:10.1186/cc13778
Tas, J., Beqiri, E., van Kaam, R. C., Czosnyka, M., Donnelly, J., Haeren, R. H., et al. (2021). Targeting autoregulation-guided cerebral perfusion pressure after traumatic brain injury (COGiTATE): A feasibility randomized controlled clinical trial. J. Neurotrauma 38 (20), 2790–2800. doi:10.1089/neu.2021.0197
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., and Vandenbroucke, J. P. (2014). The strengthening the reporting of observational studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 12 (12), 1495–1499. doi:10.1016/j.ijsu.2014.07.013
Keywords: positive end-expiratory pressure, intracranial pressure, cerebral autoregulation, acute brain injury, mechanical ventilation
Citation: Giardina A, Cardim D, Ciliberti P, Battaglini D, Ball L, Kasprowicz M, Beqiri E, Smielewski P, Czosnyka M, Frisvold S, Groznik M, Pelosi P and Robba C (2023) Effects of positive end-expiratory pressure on cerebral hemodynamics in acute brain injury patients. Front. Physiol. 14:1139658. doi: 10.3389/fphys.2023.1139658
Received: 07 January 2023; Accepted: 14 April 2023;
Published: 02 May 2023.
Edited by:
Rajesh Kumar Tripathy, Birla Institute of Technology and Science, IndiaReviewed by:
Asher Mendelson, University of Manitoba, CanadaCopyright © 2023 Giardina, Cardim, Ciliberti, Battaglini, Ball, Kasprowicz, Beqiri, Smielewski, Czosnyka, Frisvold, Groznik, Pelosi and Robba. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chiara Robba, a2lhcm9iYmFAZ21haWwuY29t
†These authors have contributed equally to this work and share first authorship
‡Chiara Robba, orcid.org/0000-0003-1628-3845
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.