
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
EDITORIAL article
Front. Physiol., 06 February 2023
Sec. Redox Physiology
Volume 14 - 2023 | https://doi.org/10.3389/fphys.2023.1112860
This article is part of the Research TopicOzone in Medicine: Biochemical Background, Physiological Modulation and Clinical ApplicationsView all 5 articles
 Bernardino Clavo1,2,3*
Bernardino Clavo1,2,3* Emma Borrelli4,5*
Emma Borrelli4,5*Editorial on the Research Topic
Ozone in medicine: Biochemical background, physiological modulation and clinical applications
The triatomic allotrope of oxygen was described as “ozone” for the first time by Christian F. Schonbein in 1839, and it is the third most powerful oxidant agent after fluorine and persulfate (Bocci et al., 2009). On the basis of its strong oxidant capacity, the first use of ozone in medicine at the end of the XIX century was as large spectrum germicide, for example in the potabilization of drinking water (Tanner et al., 2004), and several potential clinical uses as widely described in the authoritative book by Bocci, (2011).
The goal of this Research Topic “Ozone in Medicine: Biochemical Background, Physiological Modulation, and Clinical Applications” is to offer a comprehensive picture of the new research evidence in ozone therapy from bench to bedside. In fact, the mini-review by Re, (2022), about the main action mechanisms of ozone, links the old knowledge about the role of ozone in modulation of oxidative stress with the recent findings about its modulation of the nuclear factor erythroid 2-related factor 2 (Nrf2). The review on pain management by Hidalgo-Tallón et al., based on the past, describes the clinical evidence about pain, one of the most evaluated symptoms treated with ozone. B Clavo et al. published a preliminary report where ozone is added in the management of painful chemotherapy-induced peripheral neuropathy (CIPN). This study confirms the efficacy of ozone therapy on pain relief and suggests a potential new indication for ozone application for a syndrome lacking successful therapies, thus opening a field for future research. The fourth article, by OS León Fernández et al., was focused on two different diseases in elderly patients mediated by oxidative stress, rheumatoid arthritis, and bronchial asthma.
Most of the potential clinical uses of ozone treatment are not based on the direct effect of the topical treatments. In fact, the majority of clinical studies with ozone treatment are carried out using systemic ozone treatment, principally by indirect venous administration or by rectal insufflations. Using these approaches, the effects of ozone are obtained in an “indirect way”, which resembles a concept described 2,000 years ago by Hippocrates, vis medicatrix naturae, which makes reference to the body’s own mechanisms that are within us, which try to restore our health and cure our diseases (Chu et al., 2022). By systemic treatment, ozone interacts with polyunsaturated fatty acids (PUFA), antioxidants, and other components of plasma (indirect venous administration) or glycocalyx and mucoproteins (rectal insufflation) to generate reactive species of oxygen (ROS) and lipid oxidation products (LPOs), which on turn interact with cell membranes (in blood cells or cells of the intestinal mucosa) and via the blood stream LOPs can reach distant tissues. These actions produce a controlled and transient oxidative stress that will induce an adaptive body response leading to an overall enhancement of antioxidant systems. The key role of this action of ozone depends on the regulation of Nrf2, a relationship described for the first time in the XXI century. Further details about the relationship of ozone with oxidative stress and its regulation of antioxidant mechanisms by the Nrf2 pathway were described in the review of Re, (2022). This way, the potential beneficial and deleterious effects of ozone should be similar to those described for Nrf2 activation (Milkovic et al., 2017; Rojo de la Vega et al., 2018; Borrelli, 2021).
It is interesting to note that the potential beneficial effect at low-dose and detrimental effect at high-dose (hormetic effect mentioned by L Re, (2022) has been described for ozone (Bocci et al., 2011) and Nrf2 (Calabrese and Kozumbo, 2021), and they remind us the inverted U-shape response hypothesis described by Yerkes-Dodson at the beginning of the XX century for the relationship between psychological stress and productivity (Yerkes and Dodson, 1908). This would be similar to the relationship between physical exercise and cardio-respiratory or muscular adaptive response, or the relationship between oxidative stress induced by ozone and Nrf2/antioxidant adaptive response (Borrelli, 2021). In all these situations, it exists an appropriate range of stimulation/stress (psychological, physical, or oxidant) which is able to induce a beneficial adaptive response but only up to a threshold level. Above that level, the stimulus/stress overwhelms the adaptive capacity leading to detrimental effects. On the other hand, very small stimulus/stress will be managed by the basal capacity without any adaptive response. (Figure 1).
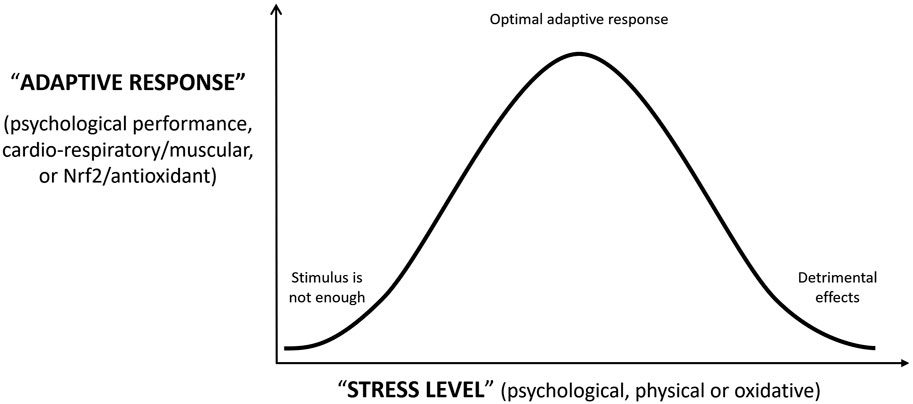
FIGURE 1. Adaptive response of the organism to psychological, physical or oxidative “stress level”.
Despite the well documented action mechanisms of ozone, well designed randomized controlled trials (RCT) are required. Although there are a limited number of RCT, fortunately, the number and clinical conditions evaluated are continuously growing.
Probably, the ozone-research field with wider and deeper clinical evidence is pain management. The article by Hidalgo-Tallón et al. describes RCTs, systematic reviews, and meta-analyses published about different pain syndromes treated by ozone as knee pathology (osteoarthritis, knee tendinopathies, patellofemoral chondromalacia), shoulder pathology (subacromial tendinopathy, calcifying tendinitis of the shoulder, and non-surgical lesions of the rotator cuff), disc herniation (and cervical and low back pain), rheumatoid arthritis among others. Overall, most studies described significant clinical improvement in treatment groups including ozone, alone or combined with conventional therapy. The most relevant clinical evidence is described for the treatment of knee osteoarthritis and lumbar disc herniation, although it is not accepted by many clinicians Hidalgo-Tallón et al. We hope that this will change soon in the interest of our patients.
A brief research report by B Clavo et al. extends the previous research field of ozone to a new painful clinical condition, the CIPN, which has been established as an urgent area of research by the American Society of Clinical Oncology (ASCO) (Markham et al., 2020). This is a very preliminary no-RCT study, with a very small sample size, and the encouraging results should be viewed with caution until larger RCTs have been conducted. However, the magnitude and length of the observed effects and the limited therapeutical approaches for CIPN (Zhang, 2021) support further research. Indeed, the authors have an ongoing RCT (NCT04299893).
The last research, by OS León Fernández et al., is a pilot study that integrates some characteristics of the three previous articles. On the one hand, this work is focused on the action mechanisms of ozone, with i) an assessment of nitric oxide (NO), prostacyclin, and thromboxane in elderly patients with bronchial asthma, ii) and an assessment of NO and several oxidative stress parameters in elderly patients with rheumatoid arthritis. On the other hand, patients with rheumatoid arthritis were studied inside a RCT, and it was also described the beneficial clinical effect of ozone in pain and in some scales of quality of life.
The use of ozone in medicine is based on many years of old experiences and clinical reports and new scientific principles. However, only rigorous continuous evidence-based work will dispel misconceptions and skepticism about this therapy.
BC and EB have contributed equally to write and review this Editorial. All authors have read and agreed to the published version of the manuscript.
The randomized controlled trial NCT04299893 was partially supported by a grant (PI 19/00458) from the Instituto de Salud Carlos III (Spanish Ministry of Science and Innovation, Madrid, Spain and European Regional Development Fund-ERDF), a grant (016/2019) from the Fundación DISA (Las Palmas, Spain), and a grant (BF1-19-03) from the Fundación Española del Dolor (Spanish Pain Foundation, Madrid, Spain).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Bocci V. A., Zanardi I., Travagli V. (2011). Ozone acting on human blood yields a hormetic dose-response relationship. J. Transl. Med. 9, 66. doi:10.1186/1479-5876-9-66
Bocci V., Borrelli E., Travagli V., Zanardi I. (2009). The ozone paradox: Ozone is a strong oxidant as well as a medical drug. Med. Res. Rev. 29 (4), 646–682. doi:10.1002/med.20150
Borrelli E. (2021). The problem of chronic oxidative stress and the systemic indirect ozone therapy as a possible solution. Highlight Med. Med. Res. 4, 135–140. doi:10.9734/bpi/hmmr/v4/1739F
Calabrese E. J., Kozumbo W. J. (2021). The hormetic dose-response mechanism: Nrf2 activation. Pharmacol. Res. 167, 105526. doi:10.1016/j.phrs.2021.105526
Chu K.-H., Tung H.-H., Clinciu D. L., Hsu H.-I., Wu Y.-C., Hsu C.-I., et al. (2022). A preliminary study on self-healing and self-health management in older adults: Perspectives from healthcare professionals and older adults in Taiwan. Gerontology Geriatric Med. 8, 23337214221077788. doi:10.1177/23337214221077788
Markham M. J., Wachter K., Agarwal N., Bertagnolli M. M., Chang S. M., Dale W., et al. (2020). Clinical cancer advances 2020: Annual report on progress against cancer from the American society of clinical Oncology. J. Clin. Oncol. 38 (10), 1081. doi:10.1200/JCO.19.03141
Milkovic L., Zarkovic N., Saso L. (2017). Controversy about pharmacological modulation of Nrf2 for cancer therapy. Redox Biol. 12, 727–732. doi:10.1016/j.redox.2017.04.013
Rojo de la Vega M., Chapman E., Zhang D. D. (2018). NRF2 and the hallmarks of cancer. Cancer Cell 34 (1), 21–43. doi:10.1016/j.ccell.2018.03.022
Tanner B. D., Suwahara S., Gerba C. P., Reynolds K. A. (2004). Evaluation of electrochemically generated ozone for the disinfection of water and wastewater. Water Sci. Technol. 50 (1), 19–25. doi:10.2166/wst.2004.0007
Yerkes R., Dodson J. (1908). The relation of strength of stimulus to rapidity of habit-formation. J. Comp. Neurology Psychol. 18 (5), 459–482. doi:10.1002/cne.920180503
Keywords: ozone therapy, oxidative stress, Nrf2, pain, chemotherapy-induced peripheral neuropathy (CIPN), rheumathoid arthritis, bronchial asthma
Citation: Clavo B and Borrelli E (2023) Editorial: Ozone in medicine: Biochemical background, physiological modulation and clinical applications. Front. Physiol. 14:1112860. doi: 10.3389/fphys.2023.1112860
Received: 30 November 2022; Accepted: 27 January 2023;
Published: 06 February 2023.
Edited and reviewed by:
Miriam M. Cortese-Krott, Heinrich Heine University of Düsseldorf, GermanyCopyright © 2023 Clavo and Borrelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bernardino Clavo, YmVybmFyZGlub2NsYXZvQGdtYWlsLmNvbQ==; Emma Borrelli, ZWJvcnJlbGxpMTRAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.