 Rui Li
Rui Li Rui Qin1*
Rui Qin1* Yajun Tan
Yajun Tan Kun Wang
Kun Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol. , 29 March 2023
Sec. Skeletal Physiology
Volume 14 - 2023 | https://doi.org/10.3389/fphys.2023.1064625
This article is part of the Research Topic Biomechanical Performance and Relevant Mechanism of Physical Medicine and Rehabilitation for Neuromusculoskeletal Disorders View all 32 articles
Objective: The aim of this study was to investigate the effects of acute Kinesio Taping (KT) intervention on the muscle strength and balance ability of college basketball players with functional ankle instability (FAI).
Methods: Thirty college basketball players with FAI were treated with acute KT to test the changes in their muscle strength and balance ability.
Results: After acute KT intervention, the ankle dorsiflexion moment and the ankle plantar flexion moment increased by 34% and 19.9%, respectively. The stable plane test with the subjects’ eyes open decreased by 1%, whereas that with the subjects’ eyes closed decreased by 1.1%. The swaying environment test with the subjects’ eyes open increased by 2.4%. The swaying plane test with the subjects’ eyes open increased by 5.1%, whereas that with the subjects’ eyes closed increased by 16.2%. The swaying environment test with the subjects’ eyes open plus the use of a plane increased by 12.1%.
Conclusion: KT can increase the isokinetic strength of the ankle dorsum muscle and plantar flexion of college basketball players with FAI. The effect of KT in the static balance test was weaker than that in the dynamic balance test. The findings indicate that KT can significantly improve the balance ability of college basketball players with FAI during dynamic sports.
An ankle sprain is the main ankle injury in sports. The incidence of ankle injury is 76.7%, accounting for 10%–17% of all joint injuries in college athletes (Kim et al., 2022; Serra-Añó et al., 2021; D'Hooghe et al., 2020). Lateral ankle joint injury is one of the most common injuries (Doherty et al., 2017; Herzog et al., 2019; Alshahrani and Reddy, 2022). Studies have shown that functional ankle instability (FAI) is common in people who play jumping and turning sports, such as basketball, volleyball or soccer (Lin et al., 2021a). Approximately 70%–80% of basketball players develop FAI after their first ankle sprain (Santos and Liu, 2008). FAI leads to decreased postural control ability, which manifests as poor muscle strength (Mao et al., 2021), balance (Doherty et al., 2014), proprioception (Alghadir et al., 2020; Xu et al., 2022) and neuromuscular control (Huang et al., 2021). Falling may also increase the risk of a second sprain (Simpson et al., 2019).
Kinesio Taping (KT) was invented by Dr. Kenso Kase in Japan (Williams et al., 2012). The application of KT supports and relaxes muscles, ligaments and fascia, as well as other soft tissues. Tai Chi combined with KT significantly improves the dynamic and static balance ability of FAI football players (Li et al., 2022a). Furthermore, KT increases dynamic postural control in FAI patients after ankle muscle fatigue (Li et al., 2022b). KT application also improves the lower limb stability of patients with chronic ankle instability (CAI) (Yu et al., 2021). However, some studies suggest that KT has no positive effect on postural control and functional activities (Nunes et al., 2021).
Injuries to the ankles are usually caused by inversion (Woods et al., 2002; Doherty et al., 2014). Hence, increasing the strength around the ankle joint can improve the dynamic postural stability of the body during landing movement (Dewar et al., 2019). Increasing ankle muscle strength via KT intervention may reduce the recurrence of sprain in basketball (Shilun, 2011). KT application to college basketball players with FAI has recently been the focus of muscle strength and balance ability research, and the existing research on KT on muscle strength and balance ability is still controversial. The results of some studies indicate that KT does not seem to increase muscle strength or improve the balance ability of subjects (Shields et al., 2013; Bailey and Firth, 2017; Martonick et al., 2020). However, other studies have shown that KT plays a certain role in improving the muscle strength and proprioception of injured people (Williams S et al., 2012; Lin et al., 2021b; Mao et al., 2021; Biz et al., 2022). In this study, the aforementioned research scope is clarified by analysing the changes in muscle strength and balance ability through KT intervention and then evaluating its effect on the ankle of college student basketball players with FAI. The KT intervention was also conducted to improve muscle strength and balance ability and consequently derive the application’s theoretical basis. The research hypothesis is stated as follows: KT intervention can improve the ankle isokinetic muscle strength and balance ability of college basketball players with FAI.
This study was approved by the Human Testing Ethics Committee of Chengdu Sport University [2022] No. 3, and 30 college basketball players who met the standards were selected for this research. The age range of the subjects was 21.5 ± 1.2 years, their height range was 179.33 ± 7.56 cm, and their weight range was 78.9 ± 9.76 kg. Regarding the Cumberland CAI tool (CAIT), the left side was 24.07 ± 6.27, and the right side was. 22.4 ± 5.59), with 13 and 17 patients presenting left ankle points (≤24) and right ankle points (≤24), respectively.
The diagnostic criteria were as follows (Santos and Liu, 2008): 1) two or more unilateral varus sprains of the ankle joint; 2) subjective ankle instability that occurred twice or more in the past 6 months; and 3) negative anterior drawer test of the talus.
Included in the standard were the following items (Delahunt et al., 2010; Rein et al., 2020): 1) repeated ankle sprain more than twice; 2) aged 18 to 25; 3) most recent sprain was 30 days ago; 4) completed the ankle instability questionnaire by using CAIT (Wright et al., 2017), with a score of ≤24 points for the unilateral ankle joint; 5) a negative result in the anterior ankle drawer test; 6) no history of fracture or surgery of the lower limbs; and 7) informed that the study was based on the Declaration of Helsinki, with informed consent forms signed.
The exclusion criteria were as follows (Kunugi et al., 2018): 1) evident dislocation and fracture; 2) simultaneous severe sprain of both ankle joints; 3) other neurological diseases that may affect balance and muscle strength; and 4) skin allergy to KT.
Subjects were tested before and after the KT intervention. In the first experiment (i.e., before the KT intervention), the balance ability and lower limb muscle strength of all subjects were tested. In the second experiment (i.e., after KT intervention), the balance ability and lower limb muscle strength of all subjects were tested. The interval between the two experiments was 1 day, during which the subjects were required to maintain normal sleep and were not allowed to perform any muscle strength or balance training of the lower limbs (Figure 1).
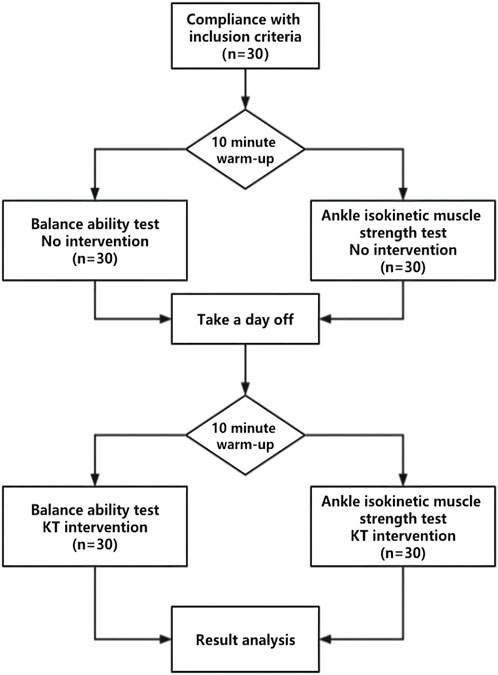
FIGURE 1. Experimental design flow chart.
According to John et al. (2018), for the first KT intervention, the anchor point should be set below the medial malleolus to prevent ankle sprain. In this method, an experimenter stretches the KT forward and pastes it along the position of the talus whilst simultaneously pressing the subject’s thigh against the ball of the foot (i.e., the subject’s foot is in a dorsiflexion position). Moderate stretching tension (approximately 30%) was applied to the KT through the lateral malleolus and terminated at the sole (Figure 2A). For the second kT intervention, the experimenter reversed pastes the KT along the first path with maximum tension (approximately 50%). The KT, passing from the outside of the foot, is stretched along the front of the ankle, and the pasting is terminated at the inside of the tibia (i.e., the KT should be one-third shorter than the original measurement length) (Figure 2B). If necessary, a third KT intervention may be adopted. The anchor point is set at the bottom of the foot. Without any tension to the KT, the experimenter, starting from the middle position, passing from the outside and front of the foot and bypassing the ankle joint, places the tail-end of the KT on the inside of the tibia. Then, the other end of the KT is placed by the experimenter on the inside of the foot, straining through the medial malleolus, then pulling back and terminating at the end of the first 2 KTs. The third KT intervention is usually conducted to allow the first and second kT interventions to fit well into the skin (Figure 2C). Figure 2D presents an image of a completed KT intervention.
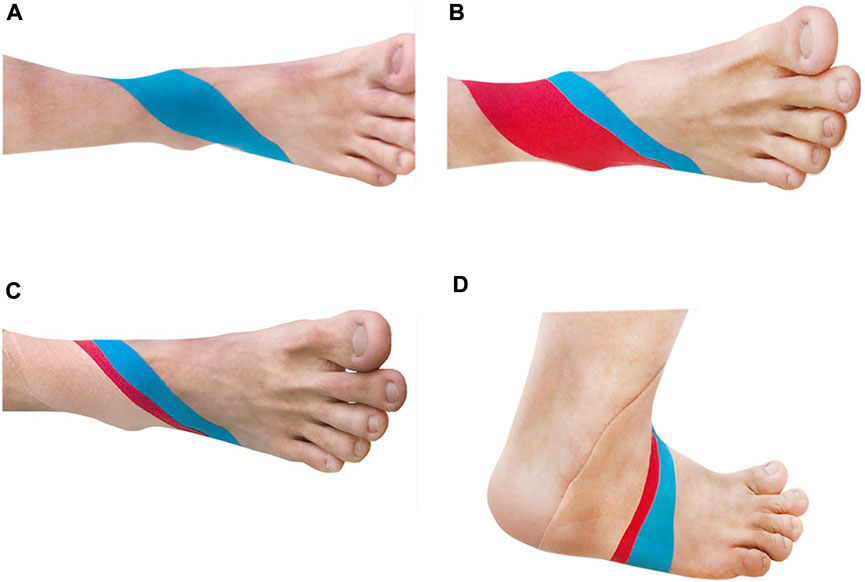
FIGURE 2. KT group (A) The first KT; (B) The second kT (C) The third KT; (D) Schematic diagram after completion.
The Smart Equi Test balance training tester developed in the United States was used, and the sensory integration experiment (SOT) was selected to perform six tests, which can be described as follows: 1) subjects with eyes open and floor and visual environment stable; 2) subjects with eyes closed and floor stable; 3) subjects with eyes open, floor stable and visual environment mobile; 4) subjects with eyes open, floor mobile and visual environment stable; 5) subjects with eyes closed and floor mobile; and 6) subjects with eyes open and floor and visual environment mobile. The tests were scored between 100 points (stable) and 0 points (fall). The balance ability index was taken as the test index; the higher the score is, the stronger the balance ability (Pickerill and Harter, 2011). Table 1 presents a detailed overview of the SOT (Delahunt et al., 2010).
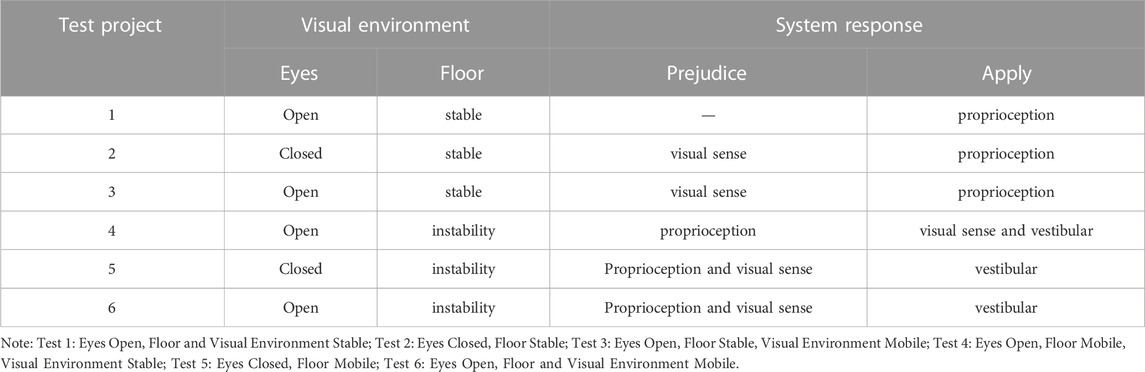
TABLE 1. Overview of the six SOT tests.
Flexion and extension tests (45°/s, 15 times) were performed on the affected ankle joints of 30 subjects by using the Swiss CONTRE isokinetic tester. The subjects were placed in the supine position during the test. Before the experiment, the subjects were allowed to warm up for 10 min. Then, the experimenter verbally stimulated the subjects to ensure that they could complete the whole experimental process as scheduled.
Peak torque was used as the test index. The maximum torque value of the joint muscle group, calculated during the ankle isokinetic test, was taken as the muscle strength level of the subject (Cheng et al., 2019; Cheng and Jiang, 2020).
The measurement data were processed as the mean ± standard deviation by using SPSS 20.0 statistical software. For measures conforming to normal distributions, the data of two measurements were tested by paired sample t-test, with the significance level set to α = 0.05.
After KT intervention, the peak moment of ankle dorsiflexion increased by 34% from 45.0 ± 22.3 to 60.3 ± 21.9 (p = 0.045). The moment of ankle plantar flexion increased by 19.9% from 48.8 ± 23.9 to 58.5 ± 22.3 (p = 0.039). The test results suggest the ability of the KT intervention to improve the ankle plantar flexion and dorsi flexion muscle strength of college basketball players with FAI. The difference was statistically significant (Table 2).

TABLE 2. Changes in isokinetic muscle strength of the affected ankle joint before and after KT intervention.
According to the SOT test results, the equilibrium index of condition 1 decreased by 1% from 95.5 ± 1.2 to 94.5 ± 2.3 (p = 0.082), and the difference was statistically insignificant (Table 3). The balance index of condition 2 decreased by 1.1% from 93.3 ± 2.6 to 92.2 ± 3.0 (p = 0.208), and the difference was also statistically insignificant. The balance index of condition 3 increased by 2.4% from 92.3 ± 2.5 to 94.6 ± 2.3 (p = 0.002), with a statistically significant difference. These results indicate the ability of KT to improve the vestibular sensation of the ankle joint. In addition, the balance index of condition 4 increased from 85.6 ± 7.3 to 90.0 ± 4.9, which was 5.1% higher (p = 0.001), and the difference was statistically significant. Therefore, KT can improve the proprioception of the affected ankle joint. The balance index of condition 5 increased by 16.2% from 62.1 ± 17.9 to 72.2 ± 10.7 (p = 0.005), with a statistically significant difference. Hence, KT can significantly improve the proprioception of the affected ankle joint under visual deprivation conditions. The balance index of condition 6 increased by 12.1% from 73.1 ± 15.0 to 82.0 ± 5.5 (p = 0.006), and the difference was statistically significant. Thus, KT can improve balance ability even when both vestibular and proprioception are disturbed. In contrast, in conditions 1 and 2, the difference was statistically insignificant after intervention, as vision was not disturbed or only vision was shielded.
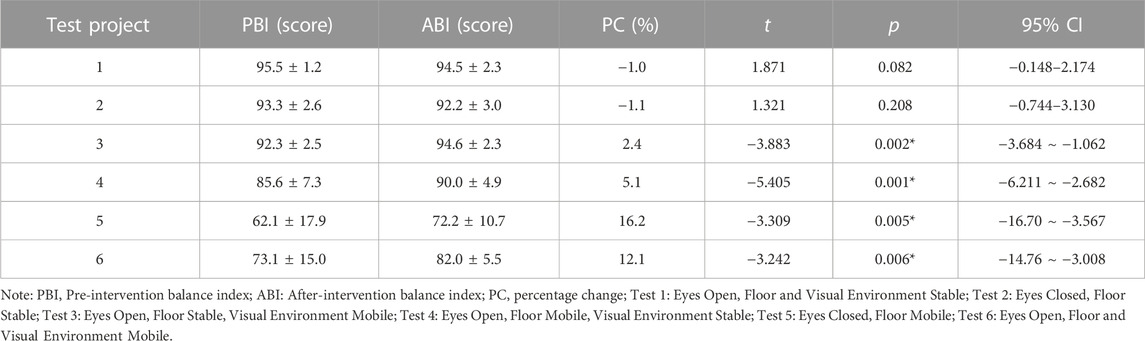
TABLE 3. Changes in balance ability before and after KT intervention.
The purpose of this study was to verify whether KT intervention can help improve the ankle isokinetic muscle strength and balance ability of college basketball players with FAI. After KT intervention, the performance of the subjects who participated in the ankle joint isokinetic muscle strength test significantly improved. In the static balance test, the difference in the results of the KT intervention was statistically insignificant. However, in the dynamic balance test, KT intervention significantly improved the balance ability of college basketball players with FAI.
This study verified the hypothesis that KT intervention can improve ankle isokinetic muscle strength in college basketball players with FAI. The obtained results showed a 34% and 19.9% increase in ankle extensor and flexor peak moments, respectively, which was similar to previous findings (Biz et al., 2022). Interestingly, although Muñoz-Barrenechea et al. (2019), reported that KT effectively improved the muscle strength of subjects with ankle instability, a few other researchers disagree. Nunes and de Noronha, 2019 applied KT to the calf triceps of 30 athletes and found no difference before and after the intervention. Ruoni (2021) found that KT could not significantly improve ankle dorsiflexion range of motion, lower limb muscle strength or subjective sensation in CAI patients within a short time. The conflicting results may be related to the different sticking methods and testing methods used by the researchers. In this study, the ability of KT to improve the isokinetic muscle strength of the subjects’ ankle joint may be explained by the elastic retraction force of the KT itself, producing traction on the subcutaneous tissue, thus causing neuromuscular stimulation and increasing muscle strength. On the basis of this analysed mechanism, KT may have enhanced the contraction ability of the damaged muscle, reduced the pain caused by muscle overextension, relieved the probability of spasm caused by muscle fatigue, improved the stability of the injured joint and surrounding soft tissue, prevented the abnormal work of the muscle from causing movement disorders of the normal joint and maintained the normal range of motion of the joint. These mechanisms can jointly reduce pain perception and increase muscle strength (Sarvestan and Svoboda, 2019). In addition, some researchers have reported the immediate effect of KT on muscle strength. For example, the tension of the pasting cloth can mechanically pull the muscle fascia, stimulate the contraction of weaker muscles and indirectly increase muscle strength (Merino-Marban et al., 2021; Li et al., 2022a).
This study verified the research hypothesis that KT intervention can improve the balance ability of college basketball players with FAI. The equilibrium indices of conditions 3, 4, 5, and 6 increased by 2.4%, 5.1%, 16.2% and 12.1%, respectively, which is consistent with the findings of previous research (Buchanan et al., 2008; Bicici et al., 2012). Ruoni (2021) also found that KT can improve ankle proprioception and lower limb dynamic balance ability in CAI patients in a short period. However, past findings were generally inconsistent. Yazici et al. (2015) found that KT intervention in the ankle joint of stroke patients could not change their static balance. Esposito et al. (2021) found that KT could not improve the static and dynamic balance of healthy semiprofessional football players. The varying results may be caused by different experimental subjects or intervention methods. In this study, the KT intervention was able to improve balance ability, which may be explained by the following: after KT is applied to the skin surface, sensory input information of the skin is generated, and proprioceptors may appear as collateral injury after ankle injury. Furthermore, the use of KT can stimulate skin effectors to enhance sensory afferent information; consequently, additional sensory and perceptual pathways are formed in the central nervous system, and the path of the reflex arc is increased, which improves the central nervous control of the periphery whilst enhancing stability (Cheng et al., 2017; Wang et al., 2018). Jackson et al. (2016) also proposed the application of KT to increase proprioceptive function and improve balance performance. The results of this research indicate that balance scores can be significantly improved compared with before intervention, especially when visual and vestibular perception is unfavourable, confirming the conclusions of Ruoni (2021) and Jackson et al. (2016).
This study, which entailed a small sample with a no-placebo control, encountered limitations. Future researchers may use more subjects to compare differences in age, sex and other factors. In addition, different taping methods have not yet been applied to patients to determine whether different taping methods have varying effects on college basketball players with FAI. Future studies may also consider adding other measures (i.e., neuromyography) and implementing longer follow-up investigations. Non-etheless, the mechanism related to KT’s improvement of muscle strength and the balance ability of FAI patients must be explored to generate more indicators.
KT can increase the isokinetic strength of the ankle dorsalis and plantaris flexion in college basketball players with FAI. The KT intervention presented a negligible effect on lower limb stability in patients with FAI during static balance tests, but it significantly improved the balance ability of FAI patients in the dynamic balance test.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by This study requested informed consent and was approved by the Ethics Committee of Chengdu Sport University [2022] No. 3. The patients/participants provided their written informed consent to participate in this study.
RL, RQ, YT, KW, HL, and LC contributed to conception and design of the study. RL and RQ organized the database. YT performed the statistical analysis. RL wrote the first draft of the manuscript. RQ, YT, KW, LC, and HL wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
This work was partially supported by the National Key R&D Program of China (No. 2020YFC2007200). It also was supported by Chengdu Sport University, Sichuan Provincial Key Laboratory, 2022–2023 Open Project: Biomechanical Mechanism of Muscle Strength Training Combined with Acupuncture and Moxibustion in Treating Chronic Ankle Instability (YY22KX01).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alghadir, A. H., Iqbal, Z. A., Iqbal, A., Ahmed, H., and Ramteke, S. U. (2020). Effect of chronic ankle sprain on pain, range of motion, proprioception, and balance among athletes. Int. J. Environ. Res. Public Health. 17 (15), 5318. doi:10.3390/ijerph17155318
Alshahrani, M. S., and Reddy, R. S. (2022). Relationship between kinesiophobia and ankle joint position sense and postural control in individuals with chronic ankle instability-A cross-sectional study. Int. J. Environ. Res. Public. Health. 19 (5), 2792. doi:10.3390/ijerph19052792
Bailey, D., and Firth, P. (2017). Does kinesiology taping of the ankles affect proprioceptive control in professional football (soccer) players? Phys. Ther. Sport 25, 94–98. doi:10.1016/j.ptsp.2016.09.001
Bicici, S., Karatas, N., and Baltaci, G. (2012). Effect of athletic taping and kinesiotaping® on measurements of functional performance in basketball players with chronic inversion ankle sprains. Int. J. Sports Phys. Ther. 7 (2), 154–166.
Biz, C., Nicoletti, P., Tomasin, M., Bragazzi, N. L., Di Rubbo, G., and Ruggieri, P. (2022). Is kinesio taping effective for sport performance and ankle function of athletes with chronic ankle instability (CAI)? A systematic review and meta-analysis. Med. Kaunas. 58 (5), 620. doi:10.3390/medicina58050620
Buchanan, A. S., Docherty, C. L., and Schrader, J. (2008). Functional performance testing in participants with functional ankle instability and in a healthy control group. J. Athl. Train. 43 (4), 342–346. doi:10.4085/1062-6050-43.4.342
Cheng, L., Chang, S., Li, J., and Hong, Y. (2017). Effects of different periods of Tai Chi exercise on the kinesthesia of the lower limb joints of elderly women. Res Sports Med 25 (4), 462–469. doi:10.1080/15438627.2017.1365300
Cheng, L., Chang, S., Qian, L., Wang, Y., and Yang, M. (2019). Extracorporeal shock wave therapy for isokinetic muscle strength around the knee joint in athletes with patellar tendinopathy. J. Sports. Med. Phys. Fit. 59 (5), 822–827. doi:10.23736/S0022-4707.18.09023-0
Cheng, L., and Jiang, Y. (2020). Effect of extracorporeal shock wave therapy on pain and forearm rotating muscle strength in patients with tennis elbow. Med. Sport. 73 (4), 661–672. doi:10.23736/S0025-7826.20.03685-6
D'Hooghe, P., Cruz, F., and Alkhelaifi, K. (2020). Return to play after a lateral ligament ankle sprain. Curr. Rev. Musculoskelet. Med. 13 (3), 281–288. doi:10.1007/s12178-020-09631-1
Delahunt, E., Coughlan, G. F., Caulfield, B., Nightingale, E. J., Lin, C. W., and Hiller, C. E. (2010). Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med. Sci. Sports Exerc. 42 (11), 2106–2121. doi:10.1249/MSS.0b013e3181de7a8a
Dewar, R. A., Arnold, G. P., Wang, W., Drew, T. S., and Abboud, R. J. (2019). The effects of wearing an Ankle Stabilizing Orthosis (ASO) Ankle Brace on ankle joints kinetics and kinematics during a basketball rebounding task. Foot. (Edinb). 40, 34–38. doi:10.1016/j.foot.2019.05.003
Doherty, C., Bleakley, C., Delahunt, E., and Holden, S. (2017). Treatment and prevention of acute and recurrent ankle sprain: An overview of systematic reviews with meta-analysis. Br. J. Sports Med. 51 (2), 113–125. doi:10.1136/bjsports-2016-096178
Doherty, C., Delahunt, E., Caulfield, B., Hertel, J., Ryan, J., and Bleakley, C. (2014). The incidence and prevalence of ankle sprain injury: A systematic review and meta-analysis of prospective epidemiological studies. Sports Med. Auckl. N.Z.) 44 (1), 123–140. doi:10.1007/s40279-013-0102-5
Esposito, F., Barni, L., Manzi, F., Braccio, P., Latella, L., Corvi, A., et al. (2021). Does ankle kinesio taping application improve static and dynamic balance in healthy trained semi-professional soccer male players? A single blinded randomized placebo controlled crossover study. Sci. Sports 36 (5), 167–174. doi:10.1016/j.scispo.2021.02.002
Herzog, M. M., Kerr, Z. Y., Marshall, S. W., and Wikstrom, E. A. (2019). Epidemiology of ankle sprains and chronic ankle instability. J. Athl. Train. 54, 603–610. doi:10.4085/1062-6050-447-17
Huang, P. Y., Jankaew, A., and Lin, C. F. (2021). Effects of plyometric and balance training on neuromuscular control of recreational athletes with functional ankle instability: A randomized controlled laboratory study. Int. J. Environ. Res. Public Health. 18 (10), 5269. doi:10.3390/ijerph18105269
Jackson, K., Simon, J. E., and Docherty, C. L. (2016). Extended use of kinesiology tape and balance in participants with chronic ankle instability. J. Athl. Train. 51 (1), 16–21. doi:10.4085/1062-6050-51.2.03
John, L., Jianwu, X., Yang, G., and Guohui, L. (2018). Bonding technique in exercise Emergency management of sports injury and pain. Shenyang: Liaoning Science and Technology Press.
Kim, K. M., Estepa-Gallego, A., Estudillo-Martínez, M. D., Castellote-Caballero, Y., and Cruz-Díaz, D. (2022). Comparative effects of neuromuscular- and strength-training protocols on pathomechanical, sensory-perceptual, and motor-behavioral impairments in patients with chronic ankle instability: Randomized controlled trial. Healthc. (Basel) 10 (8), 1364. doi:10.3390/healthcare10081364
Kunugi, S., Masunari, A., Yoshida, N., and Miyakawa, S. (2018). Association between Cumberland Ankle Instability Tool score and postural stability in collegiate soccer players with and without functional ankle instability. Phys. Ther. Sport. 32, 29–33. doi:10.1016/j.ptsp.2018.03.002
Li, P., Liu, X., Luo, X., and Guo, C. (2022b). Effect of tai chi combined with kinesio taping on posture control of football players with FAI: Protocol for a randomized controlled trial. Trials 23 (1), 162. doi:10.1186/s13063-022-06083-5
Li, P., Wei, Z., Zeng, Z., and Wang, L. (2022a). Acute effect of kinesio tape on postural control in individuals with functional ankle instability following ankle muscle fatigue. Front. Physiol. 13, 980438. doi:10.3389/fphys.2022.980438
Lin, C. C., Guo, M. L., Wang, H., Lin, C., Xu, G., Chen, A., et al. (2021b). Effects of kinesio tape on delayed onset muscle soreness: A systematic review and meta-analysis. Biomed. Res. Int. 2021, 6692828. doi:10.1155/2021/6692828
Lin, C. C., Lee, W. C., Chen, J. C., Chen, S. J., and Lin, C. F. (2021a). The influence of kinesio tape and an ankle brace on the lower extremity joint motion in fatigued, unstable ankles during a lateral drop landing. Int. J. Environ. Res. Public Health. 18 (11), 6081. doi:10.3390/ijerph18116081
Mao, H. Y., Hu, M. T., Yen, Y. Y., Lan, S. J., and Lee, S. D. (2021). Kinesio taping relieves pain and improves isokinetic not isometric muscle strength in patients with knee osteoarthritis-A systematic review and meta-analysis. Int. J. Environ. Res. Publi. Health. 18 (19), 10440. doi:10.3390/ijerph181910440
Martonick, N., Kober, K., Watkins, A., DiEnno, A., Perez, C., Renfro, A., et al. (2020). The effect of kinesio tape on factors for neuromuscular control of the lower-extremity: A critically appraised topic. J. Sport Rehabil. 29 (6), 841–846. doi:10.1123/jsr.2019-0339
Merino-Marban, R., Smuka, I., Romero-Ramos, O., Fernandez-Rodriguez, E., and Mayorga-Vega, D. (2021). Acute and 24 h effect of kinesio taping on lower back muscle soreness during continued practice of cross-country skiing among collegiate students. A double-blind, randomized, placebo-controlled trial. J. Sports. Sci. 39 (21), 2427–2433. doi:10.1080/02640414.2021.1936958
Muñoz-Barrenechea, I. A., Garrido-Beroíza, M. A., Achiardi, O., Serón, P., and Marzuca-Nassr, G. N. (2019). Revisión sistemática de la efectividad funcional del vendaje neuromuscular en sujetos con inestabilidad de tobillo A systematic review of the functional effectiveness of kinesiotaping in individuals with ankle instability. Medwave 19 (4), e7635. doi:10.5867/medwave.2019.04.7635
Nunes, G. S., and de Noronha, M. (2019). Do we really have evidence that Kinesio taping improves ankle functional performance? Clin. Rehabil. 33 (3), 584–586. doi:10.1177/0269215518824683
Nunes, G. S., Feldkircher, J. M., Tessarin, B. M., Bender, P. U., da Luz, C. M., and de Noronha, M. (2021). Kinesio taping does not improve ankle functional or performance in people with or without ankle injuries: Systematic review and meta-analysis. Clin. Rehabil. 35 (2), 182–199. doi:10.1177/0269215520963846
Pickerill, M. L., and Harter, R. A. (2011). Validity and reliability of limits-of-stability testing: A comparison of 2 postural stability evaluation devices. J. Athl. Train. 46 (6), 600–606. doi:10.4085/1062-6050-46.6.600
Rein, S., Houschyar, K. S., and Sterling-Hauf, T. (2020). Ultrasound analysis of lateral ankle ligaments in functional ankle instability. Med. Biol. 46 (12), 3228–3238. doi:10.1016/j.ultrasmedbio.2020.08.018
Ruoni, Y. (2021). Study on the effect of different lengths of kinesio taping effect patches on ankle joint function in patients with chronic ankle instability. Shanghai: Shanghai university of sport.
Santos, M. J., and Liu, W. (2008). Possible factors related to functional ankle instability. J. Orthop. Sports Phys. Ther. 38 (3), 150–157. doi:10.2519/jospt.2008.2524
Sarvestan, J., and Svoboda, Z. (2019). Acute effect of ankle kinesio and athletic taping on ankle range of motion during various agility tests in athletes with chronic ankle sprain. J. Sport Rehabil. 29 (5), 527–532. doi:10.1123/jsr.2018-0398
Serra-Añó, P., Inglés, M., Espí-López, G. V., Sempere-Rubio, N., and Aguilar-Rodríguez, M. (2021). Biomechanical and viscoelastic properties of the ankle muscles in men with previous history of ankle sprain. J. Biomech. 115, 110191. doi:10.1016/j.jbiomech.2020.110191
Shields, C. A., Needle, A. R., Rose, W. C., Swanik, C. B., and Kaminski, T. W. (2013). Effect of elastic taping on postural control deficits in subjects with healthy ankles, copers, and individuals with functional ankle instability. Foot Ankle Int. 34 (10), 1427–1435. doi:10.1177/1071100713491076
Shilun, H. (2011). Research on the Influence of ankle joint Insertion on the Athletic ability of male basketball players and its timeliness. Beijing: Beijing Sport University.
Simpson, J. D., Stewart, E. M., Macias, D. M., Chander, H., and Knight, A. C. (2019). Individuals with chronic ankle instability exhibit dynamic postural stability deficits and altered unilateral landing biomechanics: A systematic review. Phys. Ther. Sport. 37, 210–219. doi:10.1016/j.ptsp.2018.06.003
Wang, Y., Gu, Y., Chen, J., Luo, W., He, W., Han, Z., et al. (2018). Kinesio taping is superior to other taping methods in ankle functional performance improvement: A systematic review and meta-analysis. Clin. Rehabil. 32 (11), 1472–1481. doi:10.1177/0269215518780443
Williams, S., Whatman, C., Hume, P. A., and Sheerin, K. (2012). Kinesio taping in treatment and prevention of sports injuries: A meta-analysis of the evidence for its effectiveness. Sports. Med. 42 (2), 153–164. doi:10.2165/11594960-000000000-00000
Woods, C., Hawkins, R., Hulse, M., and Hodson, A. (2002). The football association medical research programme: An audit of injuries in professional football-analysis of preseason injuries. Br. J. Sports Med. 36 (6), 436–441. doi:10.1136/bjsm.36.6.436
Wright, C. J., Linens, S. W., and Cain, M. S. (2017). A randomized controlled trial comparing rehabilitation efficacy in chronic ankle instability. J. Sport Rehabil. 26 (4), 238–249. doi:10.1123/jsr.2015-0189
Xu, Y., Song, B., Ming, A., Zhang, C., and Ni, G. (2022). Chronic ankle instability modifies proximal lower extremity biomechanics during sports maneuvers that may increase the risk of acl injury: A systematic review. Front. Physiol. 13, 1036267. doi:10.3389/fphys.2022.1036267
Yazici, G., Guclu-Gunduz, A., Bayraktar, D., Aksoy, S., Nazliel, B., Kilinc, M., et al. (2015). Does correcting position and increasing sensorial input of the foot and ankle with Kinesio Taping improve balance in stroke patients? NeuroRehabilitation 36 (3), 345–353. doi:10.3233/NRE-151223
Keywords: functional ankle instability, college basketball player, kinesio taping, isokinetic muscle strength, balance
Citation: Li R, Qin R, Tan Y, Liu H, Wang K and Cheng L (2023) Effect of kinesio taping intervention on the muscle strength and balance of college basketball players with functional ankle instability. Front. Physiol. 14:1064625. doi: 10.3389/fphys.2023.1064625
Received: 08 October 2022; Accepted: 14 March 2023;
Published: 29 March 2023.
Edited by:
Feng Wei, Michigan State University, United StatesReviewed by:
Andressa Germann Avila, Federal University of Santa Maria, BrazilCopyright © 2023 Li, Qin, Tan, Liu, Wang and Cheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rui Qin, NzcyOTMxOTU1QHFxLmNvbQ==; Yajun Tan, MTEzMTM4OTc5OUBxcS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.