 Isnaini Herawati
Isnaini Herawati Arimi Fitri Mat Ludin
Arimi Fitri Mat Ludin Mutalazimah M2
Mutalazimah M2 Nor M. F. Farah
Nor M. F. Farah- 1Biomedical Science Programme & Center for Healthy Ageing and Wellness (HCARE), Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, Malaysia
- 2Faculty of Health Sciences, Universitas Muhammadiyah Surakarta, J. A.Yani Tromol Pos 1 Pabelan Kartasura, Surakarta, Indonesia
- 3Biomedical Science Programme & Center for Toxicology and Health Risk (CORE), Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, Malaysia
- 4Occupational Therapy Programme & Center for Community Health Studies (REACH), Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, Malaysia
Background: Non-pharmacological management of hypertension includes weight loss, alcohol and sodium restriction, regular exercise, and relaxation. In people with overweight hypertension, systolic blood pressure (SBP) and diastolic blood pressure (DBP) can be decreased via exercise and weight loss together. Breathing exercises are one method of relaxing.
Objectives: The aim of this scoping review is to map the information that is currently available about the advantages of breathing exercises in decreasing blood pressure in hypertension patients.
Methods: This scoping review adheres to Arksey and O’Malley’s framework, which entails identifying review questions, seeking pertinent evidence, choosing pertinent studies, mapping data, and discussing, concluding, and reporting the findings. The PRISMA flowchart is used to show how the evidence search process works.
Results: As a result, 339 articles in total were retrieved from the three databases. 20 papers total were included in this review after screening. In 14 of the 20 investigations, participants with stage 1 and stage 2 essential hypertension, two with pre-hypertension, and four with Isolated Systolic Hypertension (ISH) were studied. The respondents’ ages ranged from 18 to 75. The systolic blood pressure declined by 4–54.22 mmHg, while the diastolic blood pressure dropped by 3–17 mmHg.
Conclusion: Slow breathing can be used as an alternate, non-pharmacological therapy for hypertension individuals to reduce blood pressure.
Systematic Review Registration: (https://osf.io/ta9u6/).
1 Introduction
High blood pressure, often known as hypertension, is a serious medical condition that increases the risk of heart disease, stroke, kidney failure, and other disorders. In the past 30 years, the number of adults aged 30–79 years with hypertension has risen from 650 million to 1.28 billion, with approximately half of these people unaware of their condition. According to WHO data from 2018, around 26.4 percent of the world’s population has hypertension, with a male-to-female ratio of 26.6 percent and 26.1 percent, and approximately 60 percent of those with hypertension live in developing countries, including Indonesia. In 2018, the National Institute of Basic Health Research (Riskesdas) reported an increase in the prevalence of hypertension in Indonesia’s 260 million population, which was 34.1 percent in 2018 compared to 27.8 percent in 2013 (Kementerian Kesehatan Republik Indonesia, 2019). Hypertension is also called the silent killer because it often occurs without significant complaints, so the patient does not know he has hypertension and is only known after complications occur. Symptoms usually appear after 20 years of being diagnosed with hypertension and are only known when it is affecting other organs such as the heart, kidneys, brain, and eyes. This leads to the delayed treatment and reduces life expectancy. Hypertension is frequently linked to other metabolic syndrome. In fact, one or more metabolic risk factors are present in more than 80% of hypertension patients. This clinical illness is becoming more common worldwide, and it is obviously linked to modern lifestyles marked by a lack of physical activity, resulting in overweight or obesity (Neves et al., 2013).
Pharmacological management of hypertension are often used to lower morbidity and mortality among adults with hypertension and prehypertension, by achieving and maintaining arterial blood pressure at or less than 140/90 mmHg. Keeping blood pressure under control can lower the chance of developing cardiovascular disease (Sierra & de la Sierra, 2008). Evidence suggests that pharmacological therapy for high blood pressure has limitations in regulating the condition and avoiding side effects (O’Brien, 2017). In lieu of this, individuals with hypertension should adopt a lifestyle or behavior modification strategy to lower blood pressure and prevent cardiovascular disease (Wang et al., 2010) (Wang et al., 2018) (Zhang and Moran, 2017) (Booth et al., 2017). Non-pharmacological management includes weight loss, alcohol and sodium restriction, regular exercise, and relaxation. Exercise and weight loss together have been demonstrated to reduce systolic blood pressure (SBP) and diastolic blood pressure (DBP) in overweight hypertension patients by 12.5 and 7.9 mmHg, respectively (Bacon et al., 2004).
Breathing exercise is a useful non-pharmacological interventions in controlling hypertension (Gavish, 2010). It is hypothesized that the stimulation of heart-lung mechanoreceptors during prolonged inhalation and exhalation can increase baroreflex sensitivity (BRS) and reduce sympathetic activity and chemoreflex activation (Joseph et al., 2005) (Forouzanfar et al., 2016). Deep breathing exercises at a respiratory rate of 6 or 10 breaths per minute prolongs the contraction of the diaphragm, minimize the frequency of respiration, and increase the volume of inspiration and expiration to maximize the amount of oxygen that enters the bloodstream, as well as resulting in arteriolar dilation (Ma et al., 2017). In people with hypertension, this breathing exercise can reduce SBP and DBP (Wang et al., 2010) (Chen et al., 2017). Diaphragmatic Deep Breathing has been shown to have a therapeutic effect on the physical and psychological health of people with hypertension (Ma et al., 2017) (Subbalakshmi et al., 2014) (Vasuki and Sweety, 2017) (Chen et al., 2017) (D’silva et al., 2014). Several studies have demonstrated the effect of slow breathing exercises on baroreflex sensitivity (BRS), BP, and Autonomic nervous system (ANS) function (Oneda et al., 2010) (Fonkoue et al., 2018).
Although there are available reviews on breathing exercise, however there is none specifically addressed the outcome of breathing exercise on hypertensive patients. This review would provide an overview on the effect of breathing exercise particularly on patients with hypertension. In this scoping review, we aim to map out the evidence from available studies and relevant literature regarding breathing exercises to support the management of hypertensive patients. The specific objectives of this scoping review are:
i) To summarize the research that has been done so far on the intervention method of breathing exercises for patients with hypertension.
ii) To visualize the reported outcomes (Blood pressure and heart rate) for hypertension patients who had breathing exercise intervention
iii) To determine the breathing exercise intervention’s gaps and restrictions for patients with hypertension.
2 Methods
This scoping review was conducted according to the PRISMA Extension for Scoping Reviews (Tricco et al., 2018), thus employing a systematic approach to mapping the evidence from available studies and relevant literature regarding breathing exercises to support the management of hypertensive patients (Figure 1). The detailed protocol for this scoping review has been registered on Open Science Foundation website (Herawati et al., 2021).
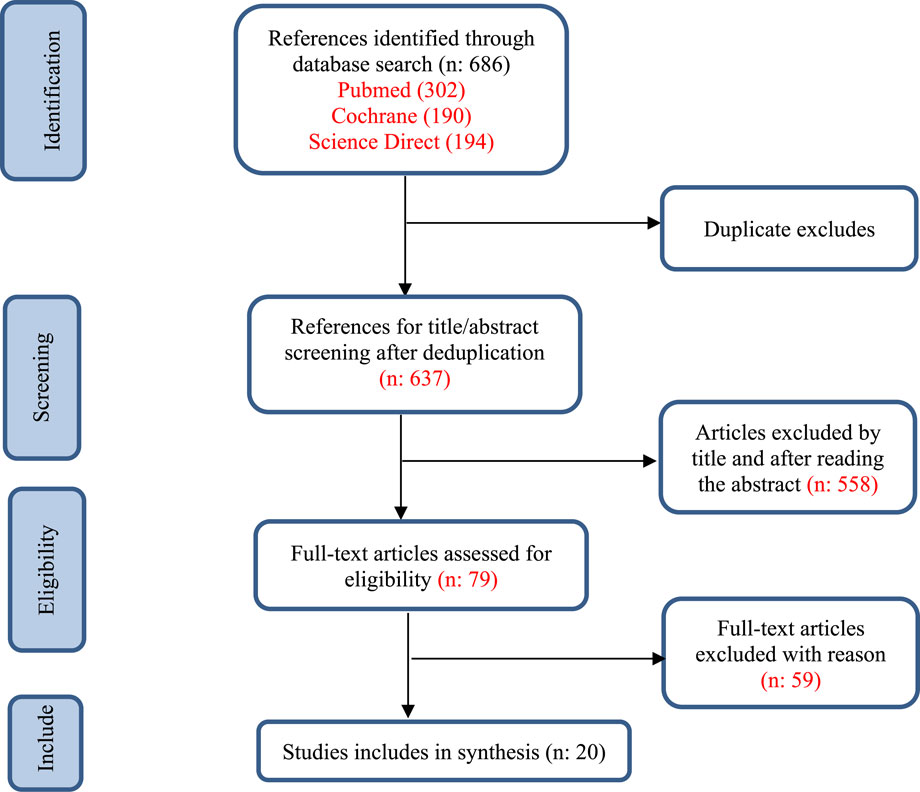
FIGURE 1. Flowchart of study selection.
2.1 Inclusion criteria
The inclusion criteria for the search will be empirical and theoretical studies related to breathing exercises for hypertensive patients aged 18 and above without any other uncontrolled cardiovascular or other diseases, with or without antihypertensive medications. For those on treatment, they should be stable on anti-hypertensive treatment for a minimum of 2 months prior to the study and no change in medications during participation in the trial, published in English, in the period from August 2010 to November 2022. Studies including multiple modalities of complementary and alternative medicine (CAM) techniques and research where breathing exercises are combined with other modalities will be excluded.
2.2 Literature search strategy
In brief, relevant studies were retrieved from electronic databases (i.e., PubMed, COCHRANE, and Science Direct). A list of references from reviews discovered through electronic searches was checked to ensure that pertinent papers were included in the scoping review. We also looked for several sources of gray literature, such as the websites of local, national, and worldwide organizations and related scientific or medical organizations, to ensure that all pertinent material is considered.
To build a search strategy, given the research questions mentioned above, literature searches from articles were guided by PCC: Population (hypertensive patients), Concept (breathing exercise), and Content (global- no geographic target). Search terms are generated by the research team member from keywords, subject headings and synonyms such as “breathing exercise”, “hypertension”, “heart rate”, and “quality of life”, to get an overview of all potential resources from the databases. The list of keywords is shown in Table 1. The search strings are generated using the Boolean operators “AND” and “OR”, as needed. Table 2 shows the search strings generated. Each search result will be documented, and selected articles will be exported to a separate folder using the Endnote 17 reference management software.
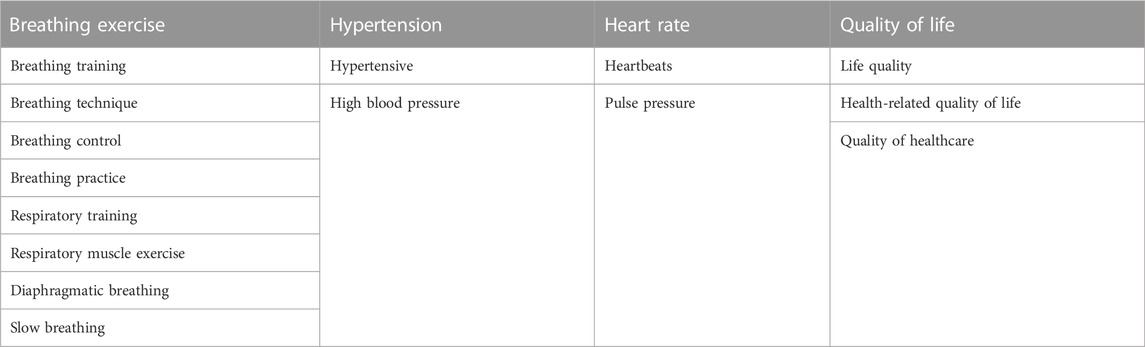
TABLE 1. List of keywords and synonyms generated as search terms.

TABLE 2. List of search strings.
2.3 Data extraction and charting
Screened articles that passed the initial selection process and were deemed suitable because they met the inclusion criteria—After the title and reading of the abstract were subjected to full-text analysis. From each study taken. First author’s name; Year of publication; Title; Population characteristics; Study design; The number of samples; Age and gender; and outcome. Two reviewers extracted the data, and disagreements were resolved by convention.
2.4 Collecting, summarizing, and reporting the result
Results from the data extraction table was collated and summarised according to our review objectives. Even though it is nota compulsory in a scoping review, we also included quality appraisal to strengthen our finding. Assessment of literature quality was conducted using PEDro quality scale, which is an 11-item scale assessing internal and external validity of clinical trials. The PEDro scale scores can range from 0 to 10, with a higher score indicating better methodological quality. Responses to items 2 to 11 are summed to create a total score, and item 1 relates to external validity Results ((Maher et al., 2003).
3 Results
3.1 Quality assessment
PEDro scores ranged from 5 to 10 points, with a mean score of 7.4 (Table 3). All of the selected studies but one (Adhana et al.) scored 6 or more, indicating the high quality of the selected trials. From the quality assessment using PEDro, we found that all study explicitly describe the eligibility criteria. Only two study [23, 38] did not employ random allocation and on top of that, [38] did not conceal participant allocation. In term of blinding, all participants and therapist were blinded only in three studies [26, 29, 33] and [18, 32, 33] accordingly. Whereby assessors were blinded in 5 of the included studies [18, 22, 26, 32, 33]. The rest of the PEDro criteria were abided by all of the included studies.
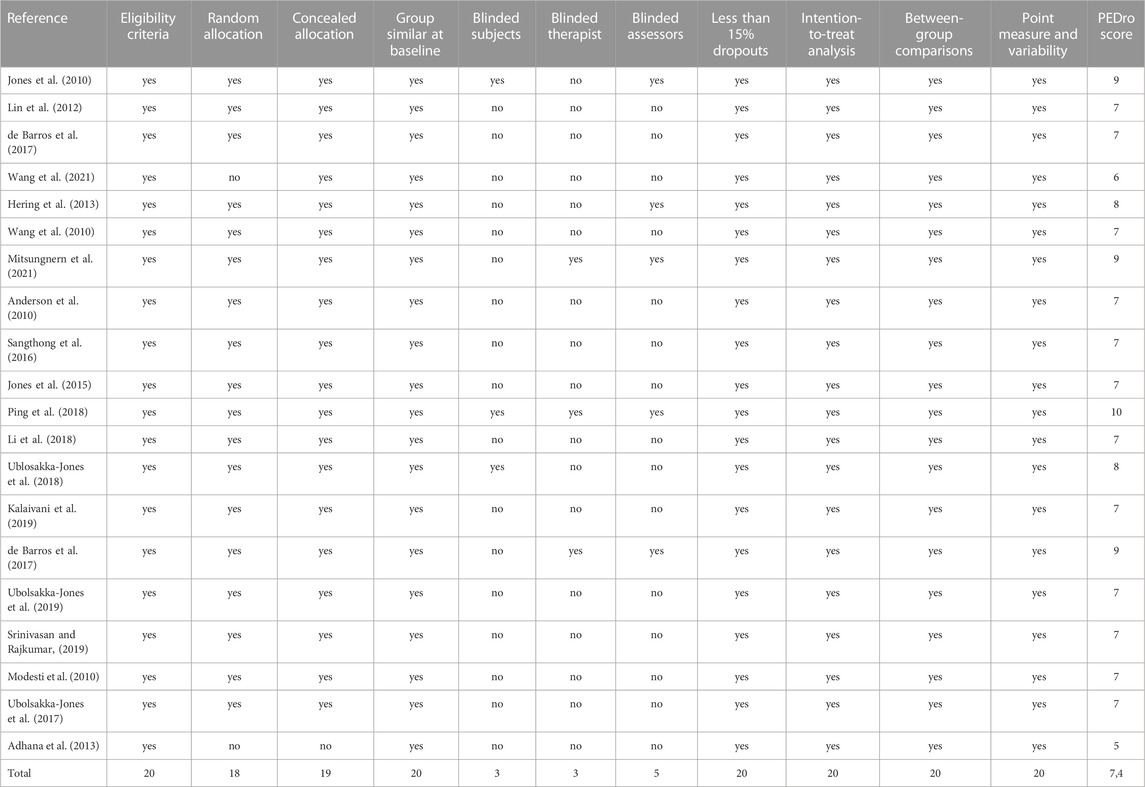
TABLE 3. PEDro scale quality assessment of the articles.
3.2 Study characteristic
A total of 686 articles were retrieved from the three selected databases. After all the screening, 20 articles were included in this review. Of the 20 selected studies, most were conducted in Thailand (n = 7), while others were published in China (n = 3), India (n = 3), Malaysia (n = 1), Brazil (n = 2), Italy (n = 1), Taiwan (n = 1), Poland (n = 1), and United States of America (n = 1). The 19 selected articles were randomized controlled trial (RCTs), while 1 article was considered prospective observational. A total of 940 respondents involved in this research. All studies aim to find out whether breathing exercises can be beneficial for lowering blood pressure in hypertensive patients. 14 of the 20 studies were conducted on respondents with stage 1 and 2 essential hypertension, two studies were conducted on respondents with pre-hypertension, and four studies were conducted on respondents with isolated systolic hypertension (ISH). The age range of the respondents was 18–75 years (Table 4).

TABLE 4. Characteristics and outcomes of included studies.
Resting blood pressure and heart rate was utilized as measures in almost all investigations. Blood pressure and heart rate responses to handgrip exercises were measured in two investigations, while ambulatory blood pressure was measured in two others. Autonomic nerve dysfunction is one of the causes of hypertension. There are five publications in this study that use MSNA (Muscle sympathetic nerve activity) (de Barros et al., 2017) (Hering et al., 2013) (Oneda et al., 2010), HRV (Heart Rate Variability) (Wang et al., 2010) (Wang et al., 2021), and three studies that use baroreflex sensitivity parameter to assess autonomic nerve status (Wang et al., 2021) (Lin et al., 2012) (Li et al., 2018). Blood inflammatory indicators, such as tumor necrosis factor-alpha (TNF-α), interleukin-6, interleukin-1 receptor agonist, and C-reactive protein (Wang et al., 2021), lung capacity, chest and abdominal expansion (Fonkoue et al., 2018), and plasma catecholamines, were also included in this review (de Barros et al., 2017).
3.3 Type of breathing exercise
Breathing exercises are techniques that are easy to do and do not require a lot of muscle work, so all ages can do them. 16 of 20 studies used slow breathing to lower blood pressure with a frequency that varied between 4 and 10 breaths per minute. Six studies used slow-loaded breathing, and six studies used device-guided slow breathing. Loaded breathing is done using a Water Pressure Threshold Bottle by providing an inspiration load of 20 cm H2O (Jones et al., 2010) (Jones et al., 2015) or 18 cmH2O (Sangthong et al., 2016). Meanwhile, Chulee Ublosakka uses a BreatheMAX device with a 25% MIP load (Ublosakka-Jones et al., 2018) (Ubolsakka-Jones et al., 2019). To guide the respondent to do slow breathing, a guided slow breathing device is used. Wang used a wearable ECG wristband (MiCor A100, MiTAC Corp., Taiwan) (C. Wang et al., 2021), while Anderson used a device that included a microcomputer connected to a band worn around the torso and a set of earphones (Anderson et al., 2010) (de Barros et al., 2017). One study used pursed lip breathing (PLB) and the other used alternate nostril breathing, pranayama, and yoga (Table 5).
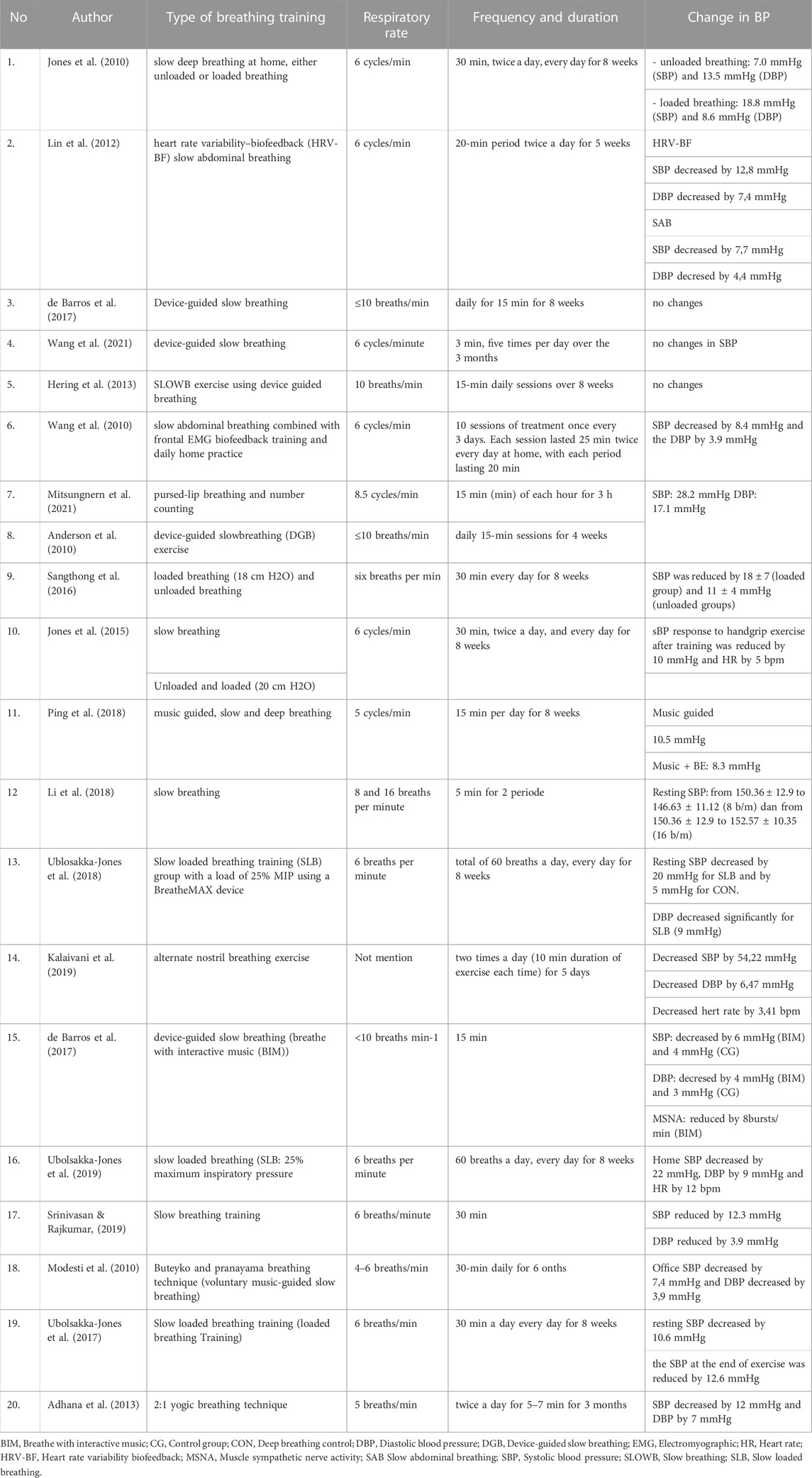
TABLE 5. Type, rate, dan frequency of breathing training.
3.4 Frequency and duration
Most of the studies selected in this scoping review applied daily breathing exercises, 10–60 min a day. Breathing exercises were used in some research for 15 min daily (7 studies), 30 min daily (4 studies), and 60 min daily (2 studies). Six studies were performed two times per day, the rest did the exercises once a day. There are 2 studies that have done breathing exercises 60 times a day with a frequency of 6 breaths per minute. The minimum duration was 3 min for 1 session, which is done 5 times a day so the total training time was 15 min per day. The effect of breathing exercises was seen in the duration of 12 weeks (2 studies), 8 weeks (12 studies), 6 months, 5 weeks, 4 weeks, and 5 days each in 1 study. There were 2 studies that looked at the direct effect of breathing exercises.
3.5 Effects of breathing exercises on blood pressure parameters
The effects of breathing exercise on cardiovascular condition, autonomic nerve activity, blood inflammatory biomarkers, and lung health were studied in this study. Only three research reported no change in blood pressure after receiving breathing training treatment, despite the fact that 17 studies reported a decrease in blood pressure, both systolic and diastolic. The systolic blood pressure declined by 4–54.22 mmHg, while the diastolic blood pressure dropped by 3–17 mmHg.
The autonomic nervous activity was determined in 5 of the 20 papers. MNSA was the subject of three studies, but only one of the recommended revisions. Sympathetic nerve activity reduces as people breathe slowly. Muscle sympathetic activity decreases during the fifth and 10th minutes of BIM use. At the time, the breathing frequency was already around ten breaths per minute, implying that sympathetic activity is linked to breathing frequency (Oneda et al., 2010).
In contrast to the Oneda study, de Barros et al. (2017) found that long-term device-guided slowbreathing (DGB) did not affect blood pressure, catecholamine levels, or MSNA in hypertensive individuals. Long-term slow breathing (SLOWB) training lowers office BP and HR, but not 24-h ambulatory BP and HR; SLOWB selectively attenuates cardiovascular effects of mental, but not physical stressors in this cohort of patients with untreated essential hypertension; and SLOWB reduces MSNA during acute device-guided lowering of breathing frequency, but not by long-term SLOWB home exercises (Hering et al., 2013).
According to a study, TNF alpha, IL 6, IL 1 receptor agonist, and C reactive protein levels are lower. TNF-α decreased significantly throughout the 3-month training period: the difference was significant after 1 month of DGB exercise training (p 0.05), and it continued to diminish after 3 months of training (p 0.05). TNF-α decrease levels did not change significantly between participants with and without comorbidities (all p > 0.05). Other biomarkers such as IL-6, IL-1ra, galectin-3, and CRP, on the other hand, did not demonstrate any significant alterations during the study period.
According to an article, the SLB group showed significant increases in chest and abdominal expansion, most likely due to their enhanced inspiratory muscle strength. With SLB, increased chest and abdominal expansion was linked to considerably bigger slow vital capacity (SVC) and inspiratory capacity (IC). The SLB has a higher tidal volume due to the lower breathing rate. Meanwhile, one study found that after being given Device-guided slow breathing, there was no change in plasma catecholamines (de Barros et al., 2017).
4 Discussion
An imbalance of the autonomic nervous system in the form of increased sympathetic activity and decreased parasympathetic activity has a major role in the etiology of hypertension (Howorka et al., 2013). Another factor that contributes to the incidence of hypertension is impaired baroreflex sensitivity.
According to research, slow breathing lowers sympathetic tone and raises parasympathetic tone. This could be partially mediated by alterations in intrathoracic pressure (Toska and Eriksen, 1993; Triedman and Saul, 1994), stimulation of arterial and cardiopulmonary baroreceptors and pulmonary afferent stretch receptors or by central interactions between respiratory and cardiovascular centers in brainstem modulation of vagal activity during breathing (Eckberg and Karemaker, 2009).
Slow breathing is defined as a respiratory rate of fewer than 10 breaths per minute with prolonged, rhythmic, slow, and deep expiratory periods. Slow and deep breathing can have a relaxing effect, through changes in the body’s biochemistry, such as increasing endorphins (substances that cause relaxation), lowering adrenaline, and lowering blood acidity (Pickering et al., 2005), increasing baroreflex sensitivity, and lowering blood pressure (Joseph et al., 2005) This breathing technique increases the length of the diaphragm contraction, minimizes the respiratory rate, and deepens the volume of inspiration and expiration, thus maximizing the amount of oxygen entering the bloodstream. Deep breathing exercises have been shown in numerous trials to be beneficial for hypertension patients (Joseph et al., 2005; Ma et al., 2017; Srinivasan and Rajkumar, 2019). In hypertensive patients, slow and deep breathing exercises over a period of weeks can significantly lower SBP and DBP (Elliot et al., 2004; Mourya et al., 2009), enhance baroreflex sensitivity, and significantly boost HRV in both prehypertensive and hypertensive people.
Reduced SBP and enhanced psychological well-being are linked to elevated HRV (Elliot et al., 2004; Wang et al., 2010). In hypertensive people, slow deep breathing for 2 minutes can lower SBP and DBP by 8.6 and 4.9 mmHg, respectively (Joseph et al., 2005). The lung stretch reflex, which prevents sympathetic outflow, can be activated during slow, deep breathing by having extended inspiratory phases (4 s) and high lung volumes (Seals et al., 1993). In addition, slow breathing also increases the interaction between respiratory neurons with the heart and autonomic centers in the brainstem. Respiratory sinus arrhythmias are much more pronounced during slow breathing at about six breaths per minute and are also greater with large lung volumes (Brown et al., 1993).
Additionally, there may be a close connection between the respiratory center, where voluntary control is present, and the autonomic nervous system, as evidenced by the fluctuating activity of the muscle sympathetic nerve and baroreceptor sensitivity during the respiratory cycle (Eckberg, 1980; St. Croix et al., 1999; Eckberg, 2003; Shantsila et al., 2015). Therefore, intentional slow breathing during exercise has the potential to change the neural pathways that control both resting blood pressure and how the body reacts to physical exertion. Numerous studies have demonstrated that six- to ten-breaths-per-minute deep diaphragmatic breathing exercises can increase arterial dilatation by stimulating heart-lung mechanoreceptors while reducing sympathetic nerve activity and chemoreflex activation. It raises parasympathetic activity and baroreflex sensitivity in hypertensive patients, lowering SBP and DBP (Elliot et al., 2004; Joseph et al., 2005; Mourya et al., 2009; Wang et al., 2010; Srinivasan and Rajkumar, 2019).
By stimulating stretch receptors in the aortic arch and carotid sinuses, the baroreflex is activated, which is one of the main mechanisms relating to the favorable cardiovascular effects of deep breathing (Heusser et al., 2010). By activating arterial baroreceptors, elevated afferent neural discharge to central-neural-autonomic areas causes increased parasympathetic efferent activity through the vagus nerve to the sinoatrial (SA) node, which in turn causes decreases in HR (Kougias et al., 2010). Then, it’s probable that changes in intrathoracic pressure brought on by the thorax expanding cause changes in the venous filling, stroke volume, cardiac output, and peripheral blood flow (the respiratory pump), which in turn causes a brief increase in blood pressure (Russo et al., 2017). The parasympathetic nervous system is then activated, which causes a drop in heart rate. Studying the impact of breathing patterns on baroreflex function is crucial because it reveals that slow breathing at 0.1 Hz (with an inspiration/expiration ratio of 1) enhances baroreflex gain (Wang et al., 2013).
4.1 Research gaps and implications for future research
We found many actionable research needs as a result of our study. First, because hypertension is linked to stress and anxiety, more research is needed to determine the effects of breathing exercises in lowering stress and anxiety, which can lead to reduced blood pressure. Second, only one journal in this review measured plasma catecholamines, whereas an increase in blood pressure or hypertension is frequently accompanied by metabolic changes such as impaired glucose tolerance, hyperinsulinemia, hyperlipidemia, obesity, humeral changes such as increased renin activity, plasma, catecholamines, and aldosterone, and hemodynamic changes such as left ventricular hypertrophy and impaired diastolic function, as well as humeral changes such as increased renin activity, More research is needed to establish the impact of breathing exercises on metabolic parameters in the body.
Because the time spent conducting breathing exercises varied widely in this analysis, more research is needed to discover the minimal duration and intensity required to produce advantages for hypertension patients in decreasing blood pressure and many cardiovascular parameters. Finally, a study on how long breathing exercises can help hypertension patients should be conducted.
It is noteworthy that the included studies demonstrate a homogenous breathing exercise technique, which enables us to draw more conclusive findings. We also conducted quality appraisals on all included studies to improve the trustworthiness of our review. However, even though we did not limit the geographical region in our article search, the retrieved studies mainly originated from Asia countries. This might limit the generalization of the finding from this review.
5 Conclusion
Slow deep breathing can be a non-pharmacological alternative therapy for people with hypertension in addition to lifestyle modification. Slow deep breathing is easy for people of all ages and does not have to be expensive. This research gathered 20 studies on the benefits of breathing exercises in hypertension patients. Breathing exercise lowers blood pressure and pulse during and after exercise, as well as MSNA, but it has no effect on plasma catecholamines. In one trial, inflammatory biomarkers (TNF alpha, IL 6, IL 1 receptor agonist, and C reactive protein) decreased, but CRP remained unchanged. Enhanced chest and abdominal expansion, as well as increased inspiratory muscular strength, were also obtained. One There were no significant changes in plasma catecholamines, according to the study. There are still some questions to be answered about the frequency and intensity of breathing exercises that are useful for hypertension patients and how long the effects last.
This review mapped the outcomes of breathing exercises, one of the non-pharmacological approaches to managing hypertension. Almost all included studies demonstrate that this affordable approach leads to positive effects. This finding can be the basis of the breathing exercises implemented by healthcare providers for patients with hypertension.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
Conceptualization: AM, MM, II, and NF, Methodology: AM and IH, Investigation: All authors. Project administration: IH. Supervision: AM, MM, II, and NF. Writing—Original draft: IH. Writing—Review and editing: All authors. All authors approved the fnal version of the manuscript.
Funding
This study was supported by Universiti Kebangsaan Malaysia and Universitas Muhammadiyah Surakarta, Indonesia.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adhana R., Gupta R., Dvivedi J., Ahmad S. (2013). The influence of the 2:1 yogic breathing technique on essential hypertension. Indian J. Physiology Pharmacol. 57 (1), 38–44.
Anderson D. E., McNeely J. D., Windham B. G. (2010). Regular slow-breathing exercise effects on blood pressure and breathing patterns at rest. J. Hum. Hypertens. 24 (12), 807–813. doi:10.1038/jhh.2010.18
Bacon S. L., Sherwood A., Hinderliter A., Blumenthal J. A. (2004). Effects of exercise, diet and weight loss on high blood pressure. Sports Med. 34 (5), 307–316. doi:10.2165/00007256-200434050-00003
Booth J. N., Li J., Zhang L., Chen L., Muntner P., Egan B. (2017). Trends in prehypertension and hypertension risk factors in US adults 1999-2012. Hypertension 70 (2), 275–284. doi:10.1161/HYPERTENSIONAHA.116.09004
Brown T. E., Beightol L. A., Koh J., Eckberg D. L. (1993). Important influence of respiration on human R-R interval power spectra is largely ignored. J. Appl. Physiology 75 (5), 2310–2317. doi:10.1152/jappl.1993.75.5.2310
Chen Y. F., Huang X. Y., Chien C. H., Cheng J. F. (2017). The effectiveness of diaphragmatic breathing relaxation training for reducing anxiety. Perspect. Psychiatric Care 53 (4), 329–336. doi:10.1111/ppc.12184
de Barros S., da Silva G. V., de Gusmão J. L., de Araújo T. G., de Souza D. R., Cardoso C. G., et al. (2017). Effects of long term device-guided slow breathing on sympathetic nervous activity in hypertensive patients: A randomized open-label clinical trial. Blood Press. 26 (6), 359–365. doi:10.1080/08037051.2017.1357109
D’silva F., Vinay H., Muninarayanappa N. V. (2014). Effectiveness of deep breathing exercise (dbe) on the heart rate variability, bp, anxiety & depression of patients with coronary artery disease. J. Health Allied Sci. N. U. 04 (01), 035–041. doi:10.1055/s-0040-1703728
Eckberg D. L., Karemaker J. M. (2009). Point:Counterpoint: Respiratory sinus arrhythmia is due to a central mechanism vs. respiratory sinus arrhythmia is due to the baroreflex mechanism. J. Appl. Physiology 106 (5), 1740–1742. doi:10.1152/japplphysiol.91107.2008
Eckberg D. L. (1980). Nonlinearities of the human carotid baroreceptor-cardiac reflex. Circulation Res. 47 (2), 208–216. doi:10.1161/01.RES.47.2.208
Eckberg D. L. (2003). The human respiratory gate. J. Physiology 548 (2), 339–352. doi:10.1113/jphysiol.2002.037192
Elliot W. J., Izzo J. L., White W. B., Rosing D. R., Snyder C. S., Alter A., et al. (2004). Graded blood pressure reduction in hypertensive outpatients associated with use of a device to assist with slow breathing. J. Clin. Hypertens. (Greenwich, Conn.) 6 (10), 553–559. doi:10.1111/j.1524-6175.2004.03553.x
Fonkoue I. T., Marvar P. J., Norrholm S. D., Kankam M. L., Li Y., DaCosta D., et al. (2018). Acute effects of device-guided slow breathing on sympathetic nerve activity and baroreflex sensitivity in posttraumatic stress disorder. Am. J. Physiology - Heart Circulatory Physiology 315 (1), H141–H149. doi:10.1152/ajpheart.00098.2018
Forouzanfar M. H., Afshin A., Alexander L. T., Biryukov S., Brauer M., Cercy K., et al. (2016). Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the global burden of disease study 2015. Lancet 388 (10053), 1659–1724. doi:10.1016/S0140-6736(16)31679-8
Gavish B. (2010). Device-guided breathing in the home setting: Technology, performance and clinical outcomes. Biol. Psychol. 84 (1), 150–156. doi:10.1016/j.biopsycho.2010.02.013
Herawati I., Mat Ludin A. F., Ishak I., Fauzi M., Nor Farah M. (2021). Protocol for a scoping review of breathing exercise for Hypertensive Patients. Available at: https://osf.io/ta9u6/.
Hering D., Kucharska W., Kara T., Somers V. K., Parati G., Narkiewicz K. (2013). Effects of acute and long-term slow breathing exercise on muscle sympathetic nerve activity in untreated male patients with hypertension. J. Hypertens. 31 (4), 739–746. doi:10.1097/HJH.0b013e32835eb2cf
Heusser K., Tank J., Engeli S., Diedrich A., Menne J., Eckert S., et al. (2010). Carotid baroreceptor stimulation, sympathetic activity, baroreflex function, and blood pressure in hypertensive patients. Hypertension 55 (3), 619–626. doi:10.1161/HYPERTENSIONAHA.109.140665
Howorka K., Pumprla J., Tamm J., Schabmann A., Klomfar S., Kostineak E., et al. (2013). Effects of guided breathing on blood pressure and heart rate variability in hypertensive diabetic patients. Aut. Neurosci. Basic Clin. 179 (1–2), 131–137. doi:10.1016/j.autneu.2013.08.065
Jones C. U., Sangthong B., Pachirat O. (2010). An inspiratory load enhances the antihypertensive effects of home-based training with slow deep breathing: A randomised trial. J. Physiother. 56 (3), 179–186. doi:10.1016/S1836-9553(10)70023-0
Jones C. U., Sangthong B., Pachirat O., Jones D. A. (2015). Slow breathing training reduces resting blood pressure and the pressure responses to exercise. Physiological Res. 64 (5), 673–682. doi:10.33549/physiolres.932950
Joseph C. N., Porta C., Casucci G., Casiraghi N., Maffeis M., Rossi M., et al. (2005). Slow breathing improves arterial baroreflex sensitivity and decreases blood pressure in essential hypertension. Hypertension 46 (4), 714–718. doi:10.1161/01.HYP.0000179581.68566.7d
Kalaivani S., Kumari M., Pal G. (2019). Effect of alternate nostril breathing exercise on blood pressure, heart rate, and rate pressure product among patients with hypertension in JIPMER, Puducherry. J. Educ. Health Promot 8, 145. doi:10.4103/jehp.jehp
Kementerian Kesehatan Republik Indonesia (2019). “Laporan nasional rislesdas 2018,” in F1000Research. Badan penelitian dan pengembangan kesehatan. Available at: http://labdata.litbang.kemkes.go.id/images/download/laporan/RKD/2018/Laporan_Nasional_RKD2018_FINAL.pdf.
Kougias P., Weakley S. M., Yao Q., Lin P. H., Chen C. (2010). Arterial baroreceptors in the management of systemic hypertension. Med. Sci. Monit. 16 (1), 1–RA8.
Li C., Chang Q., Zhang J., Chai W. (2018). Effects of slow breathing rate on heart rate variability and arterial baroreflex sensitivity in essential hypertension. Med. (United States) 97 (18), 06399–e645. doi:10.1097/MD.0000000000010639
Lin G., Xiang Q., Fu X., Wang S., Wang S., Chen S., et al. (2012). Heart rate variability biofeedback decreases blood pressure in prehypertensive subjects by improving autonomic function and baroreflex. J. Altern. Complementary Med. 18 (2), 143–152. doi:10.1089/acm.2010.0607
Ma X., Yue Z. Q., Gong Z. Q., Zhang H., Duan N. Y., Shi Y. T., et al. (2017). The effect of diaphragmatic breathing on attention, negative affect and stress in healthy adults. Front. Psychol. 8, 874–912. doi:10.3389/fpsyg.2017.00874
Maher C. G., Sherrington C., Herbert R. D., Moseley A. M., Elkins M. (2003). Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 83 (8), 713–721. doi:10.1093/ptj/83.8.713
Mitsungnern T., Srimookda N., Imoun S., Wansupong S., Kotruchin P. (2021). The effect of pursed-lip breathing combined with number counting on blood pressure and heart rate in hypertensive urgency patients: A randomized controlled trial. J. Clin. Hypertens. 23 (3), 672–679. doi:10.1111/jch.14168
Modesti P. A., Ferrari A., Bazzini C., Costanzo G., Simonetti I., Taddei S., et al. (2010). Psychological predictors of the antihypertensive effects of music-guided slow breathing. J. Hypertens. 28 (5), 1097–1103. doi:10.1097/HJH.0b013e3283362762
Mourya M., Mahajan A. S., Singh N. P., Jain A. K. (2009). Effect of slow- and fast-breathing exercises on autonomic functions in patients with essential hypertension. J. Altern. Complementary Med. 15 (7), 711–717. doi:10.1089/acm.2008.0609
Neves M. F., Virdis A., Sanjuliani A. F., Tibiriçá E. V. (2013). Hypertension and cardiometabolic risk factors. Int. J. Hypertens. 2013, 634798–634804. doi:10.1155/2013/634798
O’Brien E. (2017). The Lancet Commission on hypertension: Addressing the global burden of raised blood pressure on current and future generations. J. Clin. Hypertens. 19 (6), 564–568. doi:10.1111/jch.12998
Oneda B., Ortega K. C., Gusmão J. L., Araújo T. G., Mion D. (2010). Sympathetic nerve activity is decreased during device-guided slow breathing. Hypertens. Res. 33 (7), 708–712. doi:10.1038/hr.2010.74
Pickering T. G., Hall J. E., Appel L. J., Falkner B. E., Graves J., Hill M. N., et al. (2005). Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans: A statement for professionals from the subcommittee of professional and public education of the American heart association council on high blood pressure research. Hypertension 45 (1), 142–161. doi:10.1161/01.HYP.0000150859.47929.8e
Ping K. F., Bakar A., Subramaniam S., Narayanan P., Keong N. K., Heong A. A., et al. (2018). The impact of music guided deep breathing exercise on blood pressure control - a participant blinded randomised controlled study. Med. J. Malays. 73 (4), 233–238.
Russo M. A., Santarelli D. M., O’Rourke D. (2017). The physiological effects of slow breathing in the healthy human. Breathe 13 (4), 298–309. doi:10.1183/20734735.009817
Sangthong B., Ubolsakka-Jones C., Pachirat O., Jones D. A. (2016). Breathing training for older patients with controlled isolated systolic hypertension. Med. Sci. Sports Exerc. 48 (9), 1641–1647. doi:10.1249/MSS.0000000000000967
Seals D. R., Suwarno N. O., Joyner M. J., Iber C., Copeland J. G., Dempsey J. A. (1993). Respiratory modulation of muscle sympathetic nerve activity in intact and lung denervated humans. Circulation Res. 72 (2), 440–454. doi:10.1161/01.res.72.2.440
Shantsila A., Mcintyre D. B., Lip G. Y. H., Fadel P. J., Paton J. F. R., Pickering A. E., et al. (2015). Influence of age on respiratory modulation of muscle sympathetic nerve activity, blood pressure and baroreflex function in humans. Exp. Physiol. 100 (9), 1039–1051. doi:10.1113/EP085071
Sierra C., de la Sierra A. (2008). Early detection and management of the high-risk patient with elevated blood pressure. Vasc. Health Risk Manag. 4 (2), 289–296. doi:10.2147/vhrm.s930
Srinivasan B., Rajkumar D. (2019). Effects of slow breathing on blood pressure and end tidal carbon dioxide in hypertension: Randomised controlled trial. J. Clin. Diagnostic Res. 7, 10–12. doi:10.7860/jcdr/2019/42327.13121
St. Croix C. M., Satoh M., Morgan B. J., Skatrud J. B., Dempsey J. A. (1999). Role of respiratory motor output in within-breath modulation of muscle sympathetic nerve activity in humans. Circulation Res. 85 (5), 457–469. doi:10.1161/01.RES.85.5.457
Subbalakshmi N. K., Adhikari P., Shanmugavel Jeganathan P. (2014). Comparative study on cardiac autonomic modulation during deep breathing test and diaphragmatic breathing in type 2 diabetes and healthy subjects. J. Diabetes Investigation 5 (4), 456–463. doi:10.1111/jdi.12163
Toska K., Eriksen M. (1993). Respiration-synchronous fluctuations in stroke volume, heart rate and arterial pressure in humans. J. Physiology 472 (1), 501–512. doi:10.1113/jphysiol.1993.sp019958
Tricco A. C., Lillie E., Zarin W., O’Brien K. K., Colquhoun H., Levac D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 169 (7), 467–473. doi:10.7326/M18-0850
Triedman J. K., Saul J. P. (1994). Blood pressure modulation by central venous pressure and respiration: Buffering effects of the heart rate reflexes. Circulation 89 (1), 169–179. doi:10.1161/01.CIR.89.1.169
Ublosakka-Jones C., Tongdee P., Pachirat O., Jones D. A. (2018). Slow loaded breathing training improves blood pressure, lung capacity and arm exercise endurance for older people with treated and stable isolated systolic hypertension. Exp. Gerontol. 108, 48–53. doi:10.1016/j.exger.2018.03.023
Ubolsakka-Jones C., Sangthong B., Khrisanapant W., Jones D. A. (2017). The effect of slow-loaded breathing training on the blood pressure response to handgrip exercise in patients with isolated systolic hypertension. Hypertens. Res. 40 (10), 885–891. doi:10.1038/hr.2017.54
Ubolsakka-Jones C., Tongdee P., Jones D. A. (2019). The effects of slow loaded breathing training on exercise blood pressure in isolated systolic hypertension. Physiother. Res. Int. 24 (4), 17855–e1810. doi:10.1002/pri.1785
Vasuki G., Sweety L. M. (2017). The study of usefulness of deep breathing exercise (non pharmacological adjunct) on blood pressure in hypertensive patients. IOSR J. Dent. Med. Sci. 16 (02), 59–62. doi:10.9790/0853-1602045962
Wang C., Yang H. W., Huang H. L., Hsiao C. Y., Jiu B. K., Lin C., et al. (2021). Long-term effect of device-guided slow breathing on blood pressure regulation and chronic inflammation in patients with essential hypertension using a wearable ECG device. Acta Cardiol. Sin. 37 (2), 195–203. doi:10.6515/ACS.202103_37(2).20200907A
Wang S. Z., Li S., Xu X. Y., Lin G. P., Shao L., Zhao Y., et al. (2010). Effect of slow abdominal breathing combined with biofeedback on blood pressure and heart rate variability in prehypertension. J. Altern. Complementary Med. 16 (10), 1039–1045. doi:10.1089/acm.2009.0577
Wang Y. P., Kuo T. B. J., Lai C. T., Chu J. W., Yang C. C. H. (2013). Effects of respiratory time ratio on heart rate variability and spontaneous baroreflex sensitivity. J. Appl. Physiology 115 (11), 1648–1655. doi:10.1152/japplphysiol.00163.2013
Wang Z., Chen Z., Zhang L., Wang X., Hao G., Zhang Z., et al. (2018). Status of hypertension in China: Results from the China hypertension survey, 2012-2015. Circulation 137 (22), 2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
Keywords: breathing exercise, slow breathing, blood pressure, hypertension, heart rate
Citation: Herawati I, Mat Ludin AF, M M, Ishak I and Farah NMF (2023) Breathing exercise for hypertensive patients: A scoping review. Front. Physiol. 14:1048338. doi: 10.3389/fphys.2023.1048338
Received: 19 September 2022; Accepted: 11 January 2023;
Published: 25 January 2023.
Edited by:
Raphael Ritti-Dias, Universidade Nove de Julho, BrazilReviewed by:
Diego Christofaro, São Paulo State University, BrazilLuciana Maria Malosá Sampaio, Universidade Nove de Julho, Brazil
Copyright © 2023 Herawati, Mat Ludin, M, Ishak and Farah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Arimi Fitri Mat Ludin, arimifitri@ukm.edu.my