
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Physiol., 22 July 2022
Sec. Integrative Physiology
Volume 13 - 2022 | https://doi.org/10.3389/fphys.2022.941257
 A-ling Tang1,2
A-ling Tang1,2 Yu Peng1,2Mei-jia Shen2,3Xiao-yu Liu2,3Shan Li1,2Meng-chen Xiong1,2Nan Gao2,3Tian-peng Hu2,3
Yu Peng1,2Mei-jia Shen2,3Xiao-yu Liu2,3Shan Li1,2Meng-chen Xiong1,2Nan Gao2,3Tian-peng Hu2,3 Guo-qiang Zhang2*
Guo-qiang Zhang2*Background: The incidence and mortality of sepsis are increasing year by year, and there is still a lack of specific biomarkers to predict its prognosis. Prognostic value of vascular endothelial growth factor (VEGF) in predicting the severity and mortality of sepsis has been gradually discovered.
Methods: Literature was searched through Embase, PubMed, Web of Science, China National Knowledge Infrastructure(CNKI) and Cochrane Library databases in March 2022. Observational studies, evaluating the impact of VEGF in sepsis outcomes (mortality and severity) are included in this meta-analysis. Risk of bias was assessed with the Newcastle-Ottawa Scale (NOS). Sensitivity and publication bias analyses were also assessed. Meta-regression analysis were performed to identify the potential sources of heterogeneity.
Result: A total of 1,574 articles were retrieved from the systematic literature search. We included 20 studies for qualitative and quantitative analysis. Deceased and critically ill patients had higher baseline VEGF levels than survivors and non-severe patients. The pooled sensitivity and specificity for VEGF predicts sepsis mortality were 0.79and 0.76, respectively. the area under the SROC curve was 0.83.
Conclusion: High VEGF are associated with poor clinical outcomes for patients diagnosed with sepsis. This study was recorded on PROSPERO, under the registration ID: CRD42022323079.
Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection (Singer et al., 2016), which has the clinical characteristics of complex pathogenesis, rapid disease development and high mortality. Currently, there are no robust biomarkers that can effectively predict the prognosis of sepsis. There are no robust biomarkers that can stratify patients to the risk of sepsis complications (Alves et al., 2011), which brings great challenges to clinical work. In patients with sepsis, damage to microvascular endothelial cells can not only cause vascular leakage and edema but can also cause serious complications such as shock, microthrombosis, and multiple organ failure (MOF) (Lammers et al., 2008). Biomarkers related to sepsis prognosis include inflammation related (CRP, IL-6, IL-8, IL-18, PCT), organ dysfunction related (Lactate), vascular endothelial injury related (VEGF, Ang2/ANG-1, SFLT-1), and Oxidative Damage related (MDA, F2-ISOprostanes), etc (Vera et al., 2015). Endothelial dysfunction is associated with the pathogenesis and progression of systemic inflammatory responses (SIRS) (Shapiro et al., 2010). Several biomarkers related to vascular endothelial function have attracted the attention of researchers, such as Angiotensin 1 (Ang 1), Angiotensin 2 (Ang 2), VEGF, Soluble FMS-like tyrosine kinase 1(SFLT-1) (Pregernig et al., 2019), (Shapiro et al., 2020), (Russa et al., 2019). VEGF is an endothelial growth factor, which is involved in angiogenesis in various physiological and pathological states. Increased vascular permeability is an important pathophysiological mechanism of sepsis, and VEGF has a strong role in promoting vascular permeability (Senger et al., 1983). Compared with other biomarkers, it may better reflect the progression of sepsis from the pathophysiological mechanism. Blockade of VEGF-A reduces mortality in mice with sepsis, making it a potential target for the treatment of vascular barrier disruption in sepsis (Smadja et al., 2012). There was also a clinical study that found VEGF could distinguish between severe sepsis and non-infectious organ failure (Hauschildt et al., 2020). In several clinical studies, the impact of VEGF on the severity and mortality of sepsis patients has been confirmed. Therefore, this systematic review and meta-analysis evaluated the prognostic value of elevated VEGF in sepsis.
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement (Page et al., 2021).
Literature was searched through Embase, PubMed, Web of Science, China National Knowledge Infrastructure (CNKI) and Cochrane Library databases in March 2022, and no language or date restrictions were applied. Complete a systematic search on a combination of title, abstract and Medical Subject Headings (MeSH). The full search strategy is detailed in the Supplementary Table S1.
Two authors independently selected studies. In case of disagreement, it was firstly resolved by discussion between the two authors. If there is still disagreement, a third author is consulted. The details of selection of articles in accordance with the PRISMA guidelines are shown in Figure 1.
The following inclusion criteria were used:1) Human subjects; 2) Clinical studies; 3) observational studies; 4) Research has a clear definition of sepsis (sepsis1-3) (Singer et al., 2016); 5) Prognostic information was associated with all-cause mortality and disease severity in patients with sepsis; The exclusion criteria were, as follows: 1) In vitro experiments, animal and interventional experiments; 2) Reviews, commentaries, letters, case reports, correspondences, conference abstracts, expert opinions; 3) Duplicate articles;
The internal quality of included studies was assessed using the NOS (Wells et al., 2014) by two independent reviewers. NOS includes the following components: selection of study groups; comparability of groups; evaluation of exposures or outcomes. These three parts include 4, 2, and three sub-aspects. For each item, if the answer is “yes”, you can give the study a star. According to the score, studies are divided into three qualities: high (7–9), medium (4–6) and low (0–3).
Information retrieved from all studies involved: 1) general study information: author, year, country, study design; 2) patient characteristics: sample size; 3) VEGF measurement: time point of measurement, assay method; 4) severity of sepsis: sepsis, septic shock, severe sepsis, sepsis with MOF; 5) mortality: follow-up duration; 6) outcome measures: VEGF concentration in survivors and nonsurvivors, VEGF concentration in sepsis and severe sepsis (septic shock, severe sepsis, sepsis with MOF), the area under the receiver operating characteristic (ROC) curve was used to calculate the sensitivity and specificity of VEGF in predicting mortality.Where possible, data is retrieved directly from publications. We will obtain the data indirectly through the pictures or computational data set provided by the author, if the data cannot be obtained directly (Wan et al., 2014). Data were independently extracted by two authors using a data extraction form containing patient characteristics and outcome data.
Data synthesis was performed using RevMan software 5.4 and Stata 12. For continuous variables, standardized mean difference (SMD) and 95% CI between two groups were calculated. To test heterogeneity, I2 statistics was computed, and a χ2 test was performed. When there is significant heterogeneity (I2 ≥ 50%), random effect model is used. Meta-regression analysis were performed to identify the potential sources of heterogeneity. When the heterogeneity was low (I2<50%), the fixed effect model was used. Sensitivity analyses were performed on all results to test the stability of the meta-analysis results. Funnel plot symmetry and Egger test was used to assess the risk of publication bias for each study. Significance level for all two-sided p values was set at less than 0.05.
A total of 1,574 articles were retrieved from the systematic literature search. We included 20 studies for qualitative and quantitative analysis., with a total of 2,242 participants. (Figure 1). A total of 16 prospective studies and four retrospective studies were included. All of the studies completed VEGF concentration testing within 3 days of admission or enrollment in the study. We summarize the general information of the study in Table 1: author, year, country, study design, sample size, assay used, mortality follow-up, and NOS scores. Thirteen high quality studies (Liu et al., 2009; Davis et al., 2010; Yang et al., 2011; Xu et al., 2013; Lin et al., 2015; Amalakuhan et al., 2016; Hou et al., 2017; Patry et al., 2018a; Patry et al., 2018b; Almasy et al., 2020; Li, 2020; Seol et al., 2020; Whitney et al., 2020) and seven medium quality studies (Karlsson et al., 2008; Zhang et al., 2012; Jiang et al., 2014; Tian et al., 2015; Akabawy et al., 2016; Koskela et al., 2017; Xu, 2021) were included, and the scoring details of NOS are shown in Table 2.
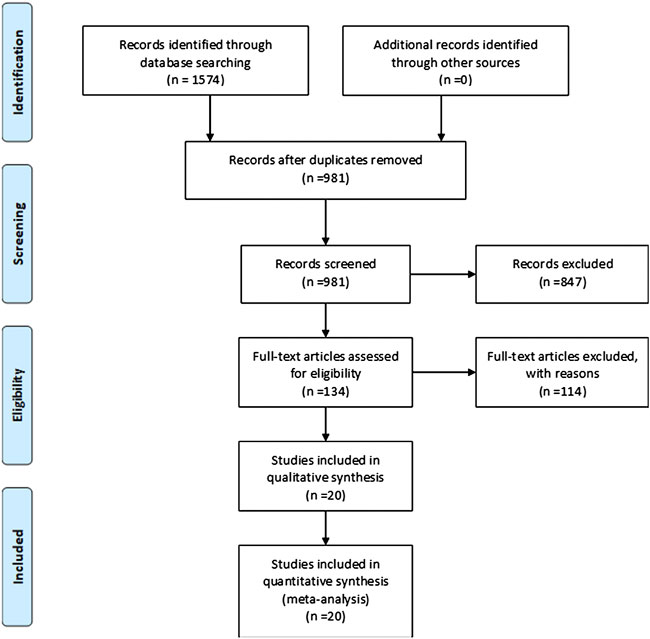
FIGURE 1. PRISMA flow diagram of study selection.
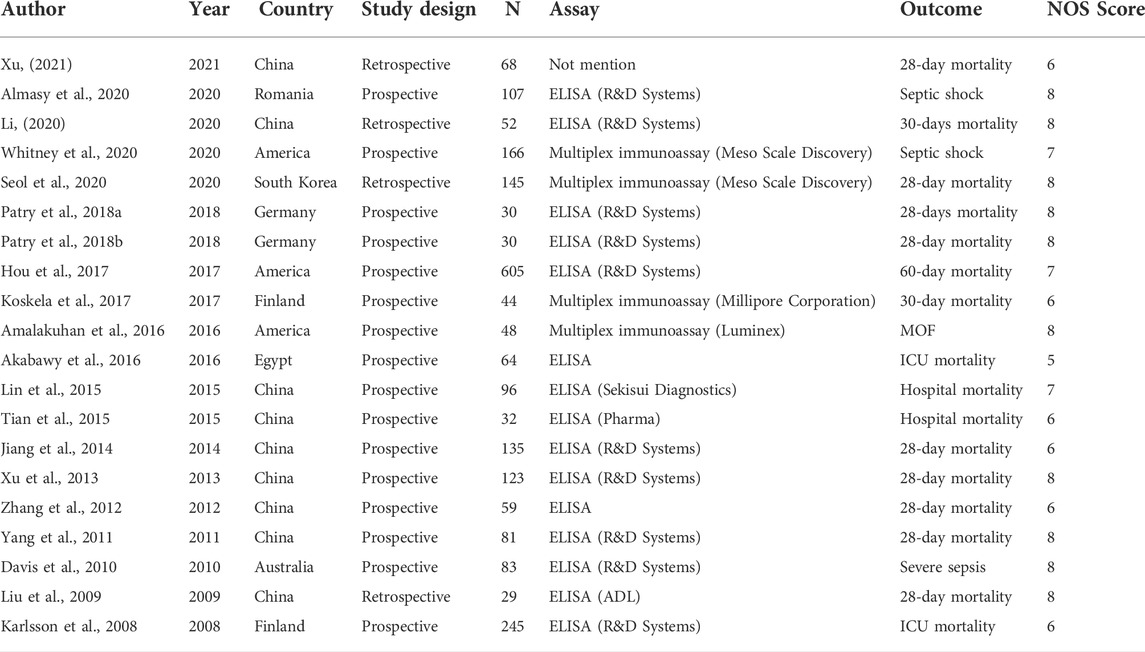
TABLE 1. Characteristics of all included studies.
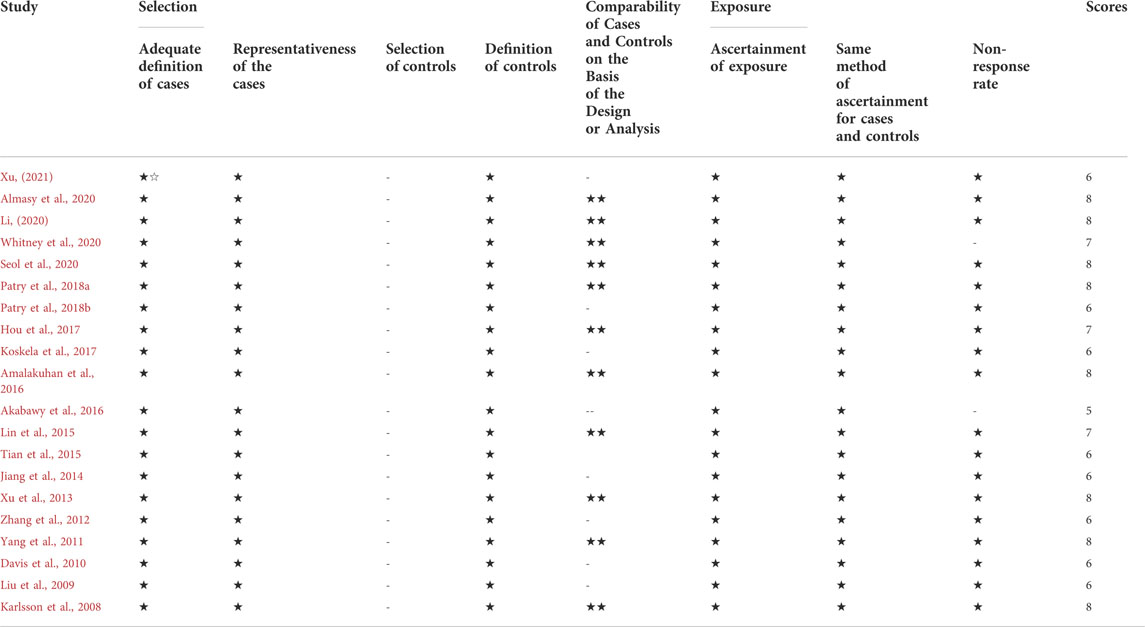
TABLE 2. NOS scores.
16 studies (Karlsson et al., 2008; Liu et al., 2009; Yang et al., 2011; Zhang et al., 2012; Xu et al., 2013; Jiang et al., 2014; Lin et al., 2015; Tian et al., 2015; Akabawy et al., 2016; Hou et al., 2017; Koskela et al., 2017; Patry et al., 2018a; Patry et al., 2018b; Li, 2020; Seol et al., 2020; Xu, 2021) reported baseline VEGF concentrations in sepsis survivors and non-survivor. Most studies confirmed that VEGF was significantly higher in the nonsurvivable group than in the survivable group. However, a number of studies have shown the opposite. Due to the high heterogeneity between studies (I2 = 91%, p < 0.00001), we used the random effects model. Meta-analysis showed significant differences in VEGF between the survival and non-survival groups (SMD = -0.77, 95%CI-1.17∼-0.37, p = 0.0002). (Figure 2). This suggests that high VEGF is associated with a high risk of mortality. Meta-regression analyses based on the confounding factors such as research starting year, nations, follow-up time of mortality, sample size, sampling time, severity of sepsis, and NOS scores were conducted. The results showed that sample size (>100 vs ≤ 100) may be the source of heterogeneity (p = 0.03). Other variables had no significant correlation with VEGF. (Supplementary Figure S1). Sensitivity analysis showed that the results remained stable after sequentially removing a single study. In addition, the funnel plot is asymmetric (Supplementary Figure S2), Egger test results show that p = 0.001, indicating that there may be publication bias between studies.
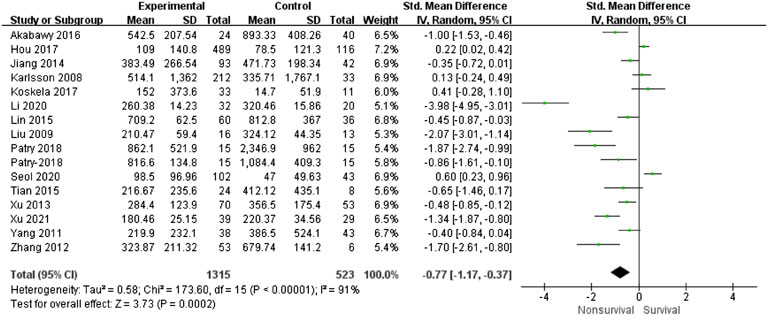
FIGURE 2. Forest plots of VEGF (nonsurvivors-survivors).
Six studies (Davis et al., 2010; Tian et al., 2015; Akabawy et al., 2016; Amalakuhan et al., 2016; Almasy et al., 2020; Whitney et al., 2020) reported a correlation between VEGF and the severity of sepsis. Due to the good homogeneity between studies (I2 = 22%, p = 0.26), we used the fixed effect model. Meta-analysis showed that VEGF was significantly higher in severe sepsis than in sepsis (SMD = -0.41, 95%CI-0.6∼-0.23, p = 0.0002) (Figure 3). Sensitivity analysis showed that the results remained stable after sequentially removing a single study. It confirmed that high VEGF was associated with more severe sepsis.
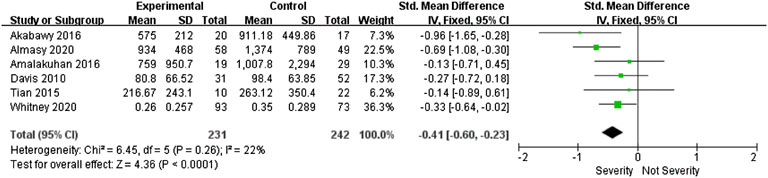
FIGURE 3. Forest plots of VEGF (sever sepsis-sepsis).
According to the data extracted from five reports (Liu et al., 2009; Yang et al., 2011; Zhang et al., 2012; Akabawy et al., 2016; Xu, 2021), the pooled sensitivity and specificity were 0.79 (95%CI 0.67–0.87) and 0.76 (95%CI 0.63–0.85). Figure 4. The area under the SROC curve is 0.84 (95%CI 0.81–0.87). (Supplementary Figure S3).
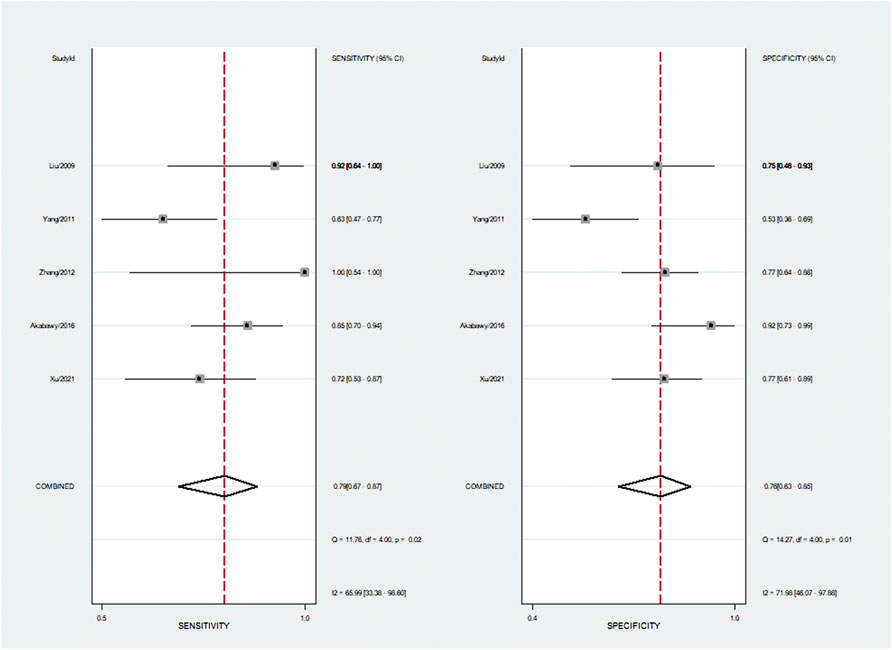
FIGURE 4. Summary of sensitivity and specificity.
Currently, the potential of inflammatory biomarkers to predict adverse outcomes in severe sepsis and septic shock patients remains uncertain (Dellinger et al., 20122013), (Reinhart et al., 2012). A study (Pregernig et al., 2019) evaluated the prognostic value of six biomarkers in sepsis patients and found that Ang-1, Ang-2, and suPAR had higher predictive value. The role of VEGF in this aspect has not been discussed by systematic review and meta-analysis. VEGF has important pro-angiogenic activity and participates in the regulation of normal and pathological angiogenesis (Melincovici et al., 2018). VEGF can induce leakage of blood vessels, and its increased expression can promote vascular hyperpermeability, edema and tissue damage (Wang et al., 2020). In sepsis, VEGF leads to vascular leakage and enhanced host response (Schuetz et al., 2011). At present, many studies have confirmed that VEGF can predict the prognosis of sepsis, but some studies believe that VEGF is not associated with the prognosis of sepsis (Koskela et al., 2017), (Karlsson et al., 2008).
Our meta-analysis results suggest that the encouraging prognostic value of VEGF in patients with sepsis. Higher VEGF is associated with higher mortality in sepsis. VEGF in the non-survival group of sepsis was significantly higher than that in the survival group, and in the severe sepsis group was significantly higher than that in the sepsis group. Sensitivity analysis suggested that our results were stable. VEGF has a high predictive accuracy in sepsis mortality, with AUC of 0.84, pooled sensitivity of 79%, and pooled specificity of 76%.
Our study has the following advantages: This study is the first meta-analysis of the prognostic value of VEGF in sepsis. To avoid the impact of other interventions on results, only observational studies were included. Most of the studies were prospective and the quality of the included studies was high. There were a large number of included studies and a large sample size. Sepsis was clearly defined in the included studies. Eligible languages include English and Chinese, which makes the included studies more comprehensive.
This study had some limitations. We detected substantial heterogeneity between studies. Meta-regression found that the sample size of the study might be the source of some heterogeneity, which could not fully explain the source of heterogeneity. Funnel plot indicates that publication bias may exist. We are still unable to explain some studies (Xu et al., 2013) suggesting that VEGF in the non-survival group of sepsis patients is lower than that in the survival group, which is contrary to the results of our meta-analysis.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
A-LT: Propose study concepts and designs; Drafting of the manuscript; YP: Acquisition of the data; Analysis and interpretation of the data; M-JS: Acquisition of the data; Analysis and interpretation of the data; X-YL: Statistical expertise; SL: Drafting of the manuscript; M-CX: Statistical expertise; NG: Analysis and interpretation of the data; T-PH: Drafting of the manuscript; G-QZ: Critical revision of the manuscript for important intellectual content; Acquisition of funding.
This study was supported by grants from the project of National Natural Science Foundation of China (grant number: 81871600).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2022.941257/full#supplementary-material
Akabawy H. E., Abo M., Ayman H., Abozekry G. A. (2016). Prognostic value of vascular endothelial growth factor in sepsis syndrome. Egypt. J. Crit. Care Med. 4 (3), 119–126. doi:10.1016/j.ejccm.2016.10.002
Almasy E., Szederjesi J., Grigorescu B. L., Badea I., Petrisor M., Manasturean C., et al. (2020). The diagnostic and prognostic role of vascular endothelial growth factor C in sepsis and septic shock. J. Crit. Care Med. 6 (3), 152–158. doi:10.2478/jccm-2020-0020
Alves B. E., Montalvao S. A. L., Aranha S. J. P., Metze I. L., Souza C. A. D., Bizzacchi J. M. A., et al. (2011). Time-course of sFlt-1 and VEGF-A release in neutropenic patients with sepsis and septic shock: a prospective study. J. Transl. Med. 9, 23. doi:10.1186/1479-5876-9-23
Amalakuhan B., Habib S. A., Mangat M., Reyes L. F., Rodriguez A. H., Hinojosa C. A., et al. (2016). Endothelial adhesion molecules and multiple organ failure in patients with severe sepsis. Cytokine 88, 267–273. doi:10.1016/j.cyto.2016.08.028
Davis J. S., Yeo T. W., Piera K. A., Woodberry T., Celermajer D. S., Stephens D. P., et al. (2010). Angiopoietin-2 is increased in sepsis and inversely associated with nitric oxide-dependent microvascular reactivity. Crit. Care 14 (3), R89. doi:10.1186/cc9020
Dellinger R. P., Levy M. M., Rhodes A., Annane D., Gerlach H., Opal S. M., et al. (20122013). Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 41, 580–637. doi:10.1097/CCM.0b013e31827e83af
Hauschildt J., Schrimpf C., Thamm K., Retzlaff J., Idowu T. O., von Kaisenberg C., et al. (2020). Dual pharmacological inhibition of angiopoietin-2 and VEGF-A in murine experimental sepsis. J. Vasc. Res. 57 (1), 34–45. doi:10.1159/000503787
Hou P. C., Filbin M. R., Wang H., Ngo L., Huang D. T., Aird W. C., et al. (2017). Endothelial permeability and hemostasis in septic shock: results from the process trial. Chest 152 (1), 22–31. doi:10.1016/j.chest.2017.01.010
Jiang W. Q., Ouyang W. F., Chen C. B., Zhu G. F., Huang L. Q., Zeng H. K., et al. (2014). Significance of the ratio of plasma vascular endothelial growth factor level to platelet count in the prognosis of patients with sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 26 (7), 484–488. doi:10.3760/cma.j.issn.2095-4352.2014.07.008
Karlsson S., Pettilä V., Tenhunen J., Lund V., Hovilehto S., Ruokonen E., et al. (2008). Vascular endothelial growth factor in severe sepsis and septic shock. Anesth. Analg. 106 (6), 1820–1826. doi:10.1213/ane.0b013e31816a643f
Koskela M., Kokko T. A., Gäddnäs F., Herzig K. H., Karhu T., Oikarinen A., et al. (2017). Blister fluid and serum cytokine levels in severe sepsis in humans reflect skin dysfunction. Acta Anaesthesiol. Scand. 61 (1), 53–61. doi:10.1111/aas.12771
Lammers K. M., Lu R., Brownley J., Lu B., Gerard C., Thomas K., et al. (2008). Gliadin induces an increase in intestinal permeability and zonulin release by binding to the chemokine receptor CXCR3. Gastroenterology 135 (3), 194–204. doi:10.1053/j.gastro.2008.03.023
Li X. J. (2020). Relationship between serum vascular endothelial cadherin levels and prognosis in patients with septic shock. Henan Med. Res. 29 (1), 43–44. doi:10.3969/j.issn.1004-437X.2020.01.015
Lin S. M., Chung F. T., Kuo C. H., Chou P. C., Wang T. Y., Chang P. J., et al. (2015). Circulating angiopopietin-1 correlates with the clinical course of multiple organ dysfunction syndrome and mortality in patients with severe sepsis. Med. Baltim. 94 (20), e878. doi:10.1097/MD.0000000000000878
Liu Y., Song S. D., Wang H. X. (2009). Levels of vascular endothelial growth factor in severe sepsis patients and its relation to prognosis. Chin. J. Emerg. Med. 18 (2), 132–135. doi:10.3760/cma.j.issn.1671-0282.2009.02.004
Melincovici C. S., Boşca A. B., Şuşman S., Marginean M., Mihu C., Istrate M., et al. (2018). Vascular endothelial growth factor (VEGF) - key factor in normal and pathological angiogenesis. Rom. J. Morphol. Embryol. 59 (2), 455–467.
Page M. J., McKenzie J. E., Bossuyt P. M., Boutron I., Hoffmann T. C., Mulrow C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 29 (372), n71. doi:10.1136/bmj.n71
Patry C., Remmé C., Betzen C., Tönshoff B., Yard B. A., Beck G., et al. (2018). VCAM-1 expression is upregulated by CD34+/CD133+-stem cells derived from septic patients. PLoS One 13 (3), e0195064. doi:10.1371/journal.pone.0195064
Patry C., Stamm D., Betzen C., Tönshoff B., Yard B. A., Beck G. C., et al. (2018). CXCR-4 expression by circulating endothelial progenitor cells and SDF-1 serum levels are elevated in septic patients. J. Inflamm. 15, 10. doi:10.1186/s12950-018-0186-7
Pregernig A., Müller M., Held U., Schimmer B. B. (2019). Prediction of mortality in adult patients with sepsis using six biomarkers: a systematic review and meta-analysis. Ann. Intensive Care 8;9 (1), 125. doi:10.1186/s13613-019-0600-1
Reinhart K., Bauer M., Riedemann N. C., Hartog C. S. (2012). New approaches to sepsis: molecular diagnostics and biomarkers. Clin. Microbiol. Rev. 25 (4), 609–634. doi:10.1128/CMR.00016-12
Russa R. L., Maiese A., Viola R. V., Matteis A. D., Pinchi E., Frati P., et al. (2019). Searching for highly sensitive and specific biomarkers for sepsis: State-of-the-art in post-mortem diagnosis of sepsis through immunohistochemical analysis. Int. J. Immunopathol. Pharmacol. 33, 2058738419855226. doi:10.1177/2058738419855226
Schuetz P., Jones A. E., Aird W. C., Shapiro N. I. (2011). Endothelial cell activation in emergency department patients with sepsis-related and non-sepsis-related hypotension. Shock 36, 104–108. doi:10.1097/SHK.0b013e31821e4e04
Senger D. R., Galli S. J., Dvorak A. M., Perruzzi C. A., Harvey V. S., Dvorak H. F., et al. (1983). Tumor cells secrete a vascular permeability factor that promotes accumulation of ascites fluid. Science 219, 983–985. doi:10.1126/science.6823562
Seol C. H., Yong S. H., Shin J. H., Lee S. H., Leem A. Y., Park M. S., et al. (2020). The ratio of plasma angiopoietin-2 to angiopoietin-1 as a prognostic biomarker in patients with sepsis. Cytokine 129, 155029. doi:10.1016/j.cyto.2020.155029
Shapiro N., Schuetz P., Yano K., Sorasaki M., Parikh S. M., Jones A. E., et al. (2010). The association of endothelial cell signaling, severity of illness, and organ dysfunction in sepsis. Crit. Care 14 (5), R182. doi:10.1186/cc9290
Shapiro N. I., Schuetz P., Yano K., Sorasaki M., Parikh S. M., Jones A. E., et al. (2020). The association of endothelial cell signaling, severity of illness, and organ dysfunction in sepsis. Crit. Care 14, 182. doi:10.1186/cc9290
Singer M., Deutschman C. S., Seymour C. W., Hari M. S., Annane D., Bauer M., et al. (2016). The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 315 (8), 801–810. doi:10.1001/jama.2016.0287
Smadja D. M., Borgel D., Diehl J. L., Gaussem P. (2012). Vascular endothelial growth factor, as compared with placental growth factor, is increased in severe sepsis but not in organ failure. J. Thromb. Haemost. 10 (5), 974–976. doi:10.1111/j.1538-7836.2012.04680.x
Tian Y., Zhu C. Y., Hong J., Huang Y. L., Wu X. H. (2015). The variation and significance of interleukin-6 and E-selectin, intercellular adhesion molecule-1 in children with sepsis. Chin. Pediatr. Emerg. Med. 9, 595–598. doi:10.3760/cma.j.issn.1673-4912.2015.09.001
Vera S., Martínez R., Gormaz J. G., Gajardo A., Galleguillos F., Rodrigo R., et al. (2015). Novel relationships between oxidative stress and angiogenesis-related factors in sepsis: New biomarkers and therapies. Ann. Med. 47 (4), 289–300. doi:10.3109/07853890.2015.1029967
Wan X., Wang W., Liu J., Tong T. (2014). Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 14, 135. doi:10.1186/1471-2288-14-135
Wang L., Astone M., Alam S. K., et al. (2020). Suppressing STAT3 activity protects the endothelial barrier from VEGF-mediated vascular permeability. J. Crit. Care Med. (Targu Mures. 6 (3), 152–158. doi:10.1101/2020.10.27.358374
Wells G. A., Shea B., O'Connell D., Peterson J., Welch V., Losos M., et al. (2014). “The newcastle–ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analysis,” Symposium on systematic reviews: Beyond the basics, Environmental Science, 2014.
Whitney J. E., Silverman M., Norton J. S., Bachur R. G., Melendez E. (2020). Vascular endothelial growth factor and soluble vascular endothelial growth factor receptor as novel biomarkers for poor outcomes in children with severe sepsis and septic shock. Pediatr. Emerg. Care 36 (12), e715–e719. doi:10.1097/PEC.0000000000001638
Xu B. (2021). Investigation of the relationship between the early lactate acid area, the primary lactate acid level, serum procalcitonin level, Apache scores and vascular endothelial growth factor and prognosis in patients with sepsis. J. Qiqihar Univ. Med. 42 (11), 1002–1256. doi:10.3969/j.issn.1002-1256.2021.11.004
Xu Q. H., Wang X. T., Li L., Chen J., Hu C. B., Cai G. L., et al. (2013). Effects of changes of endothelial function on prognosis in patients with severe sepsis. Zhonghua Yi Xue Za Zhi 93 (13), 1003–1007. doi:10.3969/j.issn.1002-1256.2021.11.004
Yang K. Y., Liu K. T., Chen Y. C., Chen C. S., Lee Y. C., Perng R. P. (2011). Plasma soluble vascular endothelial growth factor receptor-1 levels predict outcomes of pneumonia-related septic shock patients: a prospective observational study. Crit. Care 15 (1), R11. doi:10.1186/cc9412
Keywords: sepsis, VEGF, meta-analysis, systematic review, prognostic
Citation: Tang A-l, Peng Y, Shen M-j, Liu X-y, Li S, Xiong M-c, Gao N, Hu T-p and Zhang G-q (2022) Prognostic role of elevated VEGF in sepsis: A systematic review and meta-analysis. Front. Physiol. 13:941257. doi: 10.3389/fphys.2022.941257
Received: 07 June 2022; Accepted: 30 June 2022;
Published: 22 July 2022.
Edited by:
Elizabeth S. Fernandes, Pelé Pequeno Príncipe Research Institute, BrazilReviewed by:
Nefsu Awoke, Wolaita Sodo University, EthiopiaCopyright © 2022 Tang, Peng, Shen, Liu, Li, Xiong, Gao, Hu and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guo-qiang Zhang, emhhbmdjaG9uZzIwMDNAdmlwLnNpbmEuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.