 Maamer Slimani
Maamer Slimani Armin Paravlic
Armin Paravlic Ensar Abazovic
Ensar Abazovic Hela Znazen7
Hela Znazen7
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol. , 29 September 2022
Sec. Exercise Physiology
Volume 13 - 2022 | https://doi.org/10.3389/fphys.2022.912740
This article is part of the Research Topic Structural and Mechanistic Determinants of Endurance Performance View all 10 articles
Background: The aim of the present randomized, crossover study was to determine the physiological and cognitive function responses while wearing a facemask during a maximal running aerobic fitness test.
Methods: Fourteen healthy, nonsmoking physical education students (age = 17.5 years, height = 1.72 m, body mass = 70.4 kg) volunteered to participate in this study. They carried out a 20 m multistage fitness test (MSFT) while wearing or not a cloth facemask on two separate occasions performed in random order. The “Rating of Perceived Exertion” (RPE) and the d2 test for visual attention were administered and assessed before and immediately after the MSFT for both conditions (with or without a facemask).
Results: When wearing the facemask, the participants exhibited lower maximal aerobic speed (p = 0.039), VO2max (p = 0.039), distance covered during the MSFT (p = 0.057), and concentration performance (p < 0.001), when compared with the control situation (without facemask). Moreover, they made more errors compared with the control condition (p = 0.021). The use of a cloth facemask during maximal endurance running tests (such as the MSFT) reduced VO2max, and measures of cognitive performance as assessed by the test of focused visual attention (the d2 test). This data suggests avoiding using a cloth facemask during maximal aerobic fitness tests, and before any tasks that require a high level of visual attention.
Recently, the worldwide spread of the still ongoing “Coronavirus Disease 2019” (COVID-19) pandemic has profoundly disrupted the normality of daily life, forcing populations to practice social distancing and self-isolation. COVID-19 has directly impacted humans' health and affected their lifestyles, including physical activity, nutrition, and sleep behavior (Ammar et al., 2020; Znazen et al., 2021). The pandemic has had cascading and compound effects involving many domains and sectors of daily life, such as education, travel, and sport, globally, and resulted in canceling and/or postponing of many events, including major international sports events.
Given that the COVID-19 virus is primarily transmitted among people through respiratory droplets and contact routes, wearing a facemask was mandated in order to prevent the transmission and limit the spread of the virus, thus controlling and containing the infectious outbreak (Hopkins et al., 2021; Matuschek et al., 2020). At the same time, it has been reported that a prolonged use of facemasks may lead to physiological and psychological concerns (Li et al., 2005; Rosner, 2020; Epstein et al., 2021). Chronic use of facemasks may result in an increased hypoxia state, due to the decrease in blood oxygen saturation and increase in heart rate and transcutaneous CO2 (Li et al., 2005; Beder et al., 2008; Rebmann et al., 2013; Rosner, 2020; Scheid et al., 2020; Epstein et al., 2021). Moreover, it could consequently increase stress levels, mental fatigue, and reaction time, impairing responses to perceptual tasks (Modena et al., 2021; Grimm et al., 2022), resulting in headaches, and making communication more difficult and challenging (Rosner, 2020; Tornero-Aguilera and Clemente-Suárez, 2021; Lee et al., 2022).
Information about the effects of facemask on physiological and cognitive functions during exercise is limited (Shaw et al., 2021a; Slimani et al., 2021). It seems that wearing a mask during exercise imposes extra pressure on ventilation (Hopkins et al., 2021), which may lead to small changes in physiological parameters, such as increased dyspnea, end-tidal CO2, heart rate and respiratory rate (Shaw et al., 2021b; Hopkins et al., 2021). In addition, contradictory results have been reported on its effect on physical performance. A recent randomized controlled trial of healthy adults aged 18–29 years showed that the use of cloth facemasks led to a 14% reduction in exercise time and 29% decrease in VO2max, attributed to perceived discomfort associated with mask-wearing (Driver et al., 2022). The same authors demonstrated that, when compared with the no-mask condition, participants reported feeling increasingly short of breath and claustrophobic at higher exercise intensities while wearing a cloth facemask. In contrast, a systematic review of the literature and meta-analysis showed that wearing a facemask while exercising had no impact on exercise performance (Shaw et al., 2021b). This contradiction may be due to the type of mask worn and the exercise practiced (do Prado et al., 2022; Fikenzer et al., 2020). In addition, considering that cardiovascular fitness is strongly correlated to cognition (Hötting and Röder, 2013) as well as exercise and physical activity in general (Mandolesi et al., 2018), it is important to evaluate the impact of exercising while wearing a facemask on cognitive functioning. Therefore, the aim of the present study was to determine the physiological and cognitive function responses while wearing a facemask during maximal exercise.
Fourteen healthy (9 males and 5 females), nonsmoking, physical education students (age = 17.5 years, height = 1.72 m, body mass = 70.4 kg) volunteered to participate in this study after being informed of the nature and of the possible risks associated with the experiment. We included only participants who 1) are active and healthy; 2) practice only physical education; 3) without co-morbidities like diabetes, hypertension, epilepsy, cardiac illness, asthma, and other respiratory illnesses; 4) have been inactive in the last 48 hhours before the physical activity session; and, 5) have accepted to be involved in the present study.
The cloth mask (Half and quarter masks, Tunisia) was a 3-layer comfortable elastic ear loop: extra-soft ear loops eliminate pressure on the ears with layers composed of non-woven fabric. It can be considered a facemask that is typically used by the general population (Matuschek et al., 2020). Due to its availability and usage frequency by the general population, this type of mask was used in this study. The ethical approval for this study was provided by local institutions and was conducted in accordance with the 1964 Declaration of Helsinki.
The study was carried out by implementing a randomized, crossover design during the COVID-19 pandemic, when the government adopted a package of protective and behavioral measures, such as the closing of universities and schools; avoidance of physical contact, handshakes, hugs, and kisses; wearing of facemasks; and, practicing of social/physical distancing. Each participant completed three 20 m multistage fitness tests (MSFT): one for familiarization with MSFT, one with and one without wearing a facemask. The last two MSFTs were conducted in random order. Each test took place at approximately the same time of the day (±1.5 h) and was separated by at least 3 days. During the first test, anthropometric data were collected. Furthermore, participants familiarized themselves with cognitive tests. During all sessions, no drug was administered. All participants gave maximum effort and were encouraged to do so.
Additionally, the d2 test and the “Rating of Perceived Exertion” (RPE) test were administered at the two-time points (15 min before the MSFT and immediately after the test) across the exercise tests (with and without wearing a facemask) in order to assess cognitive function and perceived exertion. After a 10 min warm-up, participants performed the MSFT and responded to the RPE scale immediately afterward. Participants were advised to avoid exercise, and restrain from caffeine, and alcohol consumption 48 h before each laboratory visit. Moreover, throughout the study, participants were instructed to maintain their regular dietary habits and exercise regimens.
The MSFT was carried out as outlined in Léger et al. (1988) study. It was previously validated as a predictor of VO2max (intra-class correlation coefficient = 0.90) in adult people (Chung et al., 2022). The participants ran backwards and forwards between two lines 20 m apart, in accordance with the recorded “beep” sound. Only completed shuttles were considered successful runs. The test commenced with an initial speed of 8 km/h, being gradually increased by 0.5 km/h every minute and was stopped if the participant did not reach the line (within 2 m) for two consecutive ends after being warned. Maximal aerobic speed (MAS) was computed as the velocity of the last successfully completed stage, associated with VO2max for the shuttle run test. VO2max was calculated using the Léger et al. (1988) equation.
The d2 test was used to determine the level of concentrated visual attention of participants (Brickenkamp and Oosterveld, 2012). It consists of 14 rows with 47 characters per line. These characters are the letters d or p, with a total of one to four dashes above and below each letter. Participants were asked to scan each line and cross out only the characters containing the letter d with two dashes during 20 s. After completion of the d2 test, two variables were calculated: concentration performance (CP) and the total number of errors made by the participants (E). CP is calculated as the number of correctly marked d2-symbols minus the number of incorrectly marked symbols (symbols that are not d2-symbols). The total number of E is assessed as the number of errors made by failing to correctly identify a d2-symbol plus the number of errors made by incorrectly marking symbols that are not d2-symbols. We considered both CP and E in the current study.
RPE scale was used to estimate the participants’ perceived effort. It ranged between 0 “no perceived effort” (i.e., rest) and 10, which corresponded to “maximal perceived effort” (i.e., the most stressful exercise ever performed) (Borg, 1998).
Descriptive statistical analysis was carried out by computing the means and standard deviations for each of the variables under study. The normality of data distribution was verified by applying the Shapiro-Wilk test, which was preferred over other normality tests, given the sample size employed in the present investigation. Differences for performance-related measures between conditions (wearing a mask or not) were assessed by classical Average-Based Change statistics (ABC) (Estrada et al., 2019), more specifically the Student's t-test for dependent (paired) samples. MainThe main effects for cognitive response (CP, and E), and RPE were studied with repeated measure general linear models (GLM) with condition (wearing a mask or not) and time (PRE and POST) as within factors. Moreover, post hoc analyses were carried out, correcting for multiple comparisons.
Depending on the standard deviations, Glass's delta or Hedge's g was calculated as effect size. The former was computed for performance-related measures. For cognition- and perceived exertion-related measures, the magnitude of the difference between values was measured by using Hedge's g. The computed effect size was interpreted as follows: trivial: 0.0–0.2; small: 0.2–0.5; moderate: 0.5–0.8 and large: ≥ 0.8 (Lovakov and Agadullina, 2021). All statistical analyses were conducted utilizing the commercial software “Statistical Package for Social Sciences” (SPSS version 27.0, IBM, Armonk, NY, USA). Results with p-values less than or equal to 0.05 were considered statistically significant.
Regardless of condition they were allocated, significant alterations were observed for all measures of interest (all, p < 0.001) following MSFT.
During the experimental condition, the participants showed a 7%, 11% and 17% lower MAS (Glass’s delta = −0.85; p = 0.039), VO2max (Glass’s delta = −0.85; p = 0.039), and distance covered during the MSFT (Glass’s delta = −0.76; p = 0.057) when compared to the control condition, respectively (Table 1).
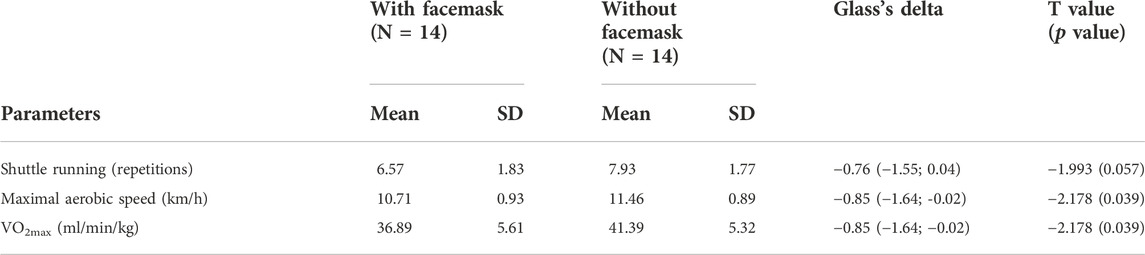
TABLE 1. Comparison of physical performance measures while wearing or not a facemask.
During both the experimental and the control conditions, the participants exhibited significantly lower CP following the MSFT, when compared with PRE (F1,26 = 393.558, p < 0.001, η2 = 0.938). There was a significant time × group interaction effect (F1,26 = 32.042, p < 0.001, η2 = 0.552). Post hoc analysis showed that, during the experimental condition, the participants experienced significantly greater decreases in CP compared with the control condition (−11% versus −5%, Hedges’ g = 2.08, p < 0.001) (Table 2).
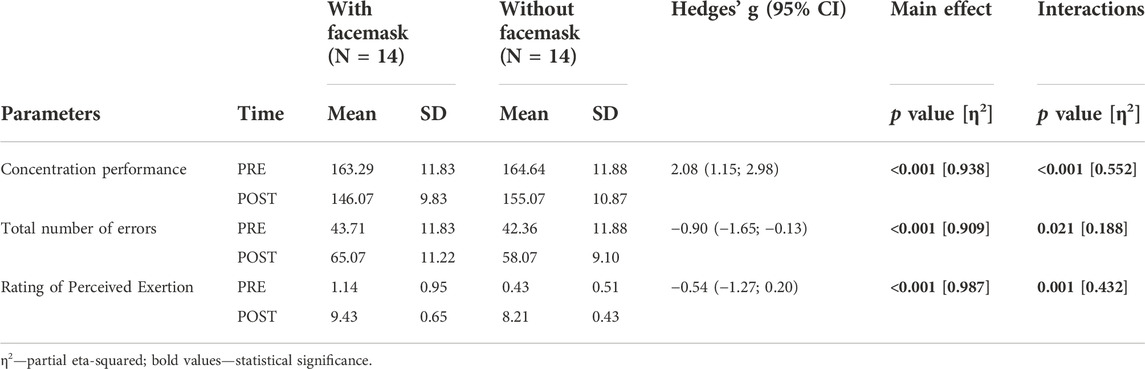
TABLE 2. Comparison of cognitive function following the MSFT, conducted while wearing or not a facemask.
During both the experimental and the control conditions, the participants had significantly higher number of errors following the MSFT, when compared with PRE (F1,26 = 260.523, p < 0.001, η2 = 0.909). There was a significant time × condition interaction effect (F1,26 = 6.036, p = 0.021, η2 = 0.188). Post hoc analysis showed that, during the experimental condition, the participants made more errors compared with the control condition (49% versus 37%, Hedges’s g = −0.90, p = 0.021) (Table 2).
During both the experimental and the control conditions, the participants had significantly higher RPE following the MSFT, when compared with PRE (F1,26 = 1931.651, p < 0.001, η2 = 0.987). There was a significant time × condition interaction effect (F1,26 = 9.520, p = 0.001, η2 = 0.432). Post hoc analysis showed that, during the experimental condition, the participants experienced a lower increase in RPE compared to the control condition, however, the observed difference was not significant (725% versus 1817%, Hedges’ g = −0.54, p = 0.155) (Table 2).
The current study investigated the effects of wearing the facemask during maximal-intensity aerobic endurance testing on physical performance and cognitive function parameters. The main findings were that wearing a facemask negatively affected MAS, predicted VO2max, and cognitive function. Briefly, both concentration performance and the number of errors made decreased and increased to a greater extent during the experimental condition after the MSFT than during the control condition, respectively. Although the difference was not statistically significant, an interesting finding was that, during the experimental condition, the participants experienced group experienced a smaller increase in RPE after the MSFT than during the control condition group. This could be primarily due to the overall exercise volume because MAS and the distance covered during the MSFT were 7% and 17% lower during the experimental condition than during the control condition, respectively.
The results showed significantly lower MAS, VO2max, and covered distance during the MSFT, while the participants wore the cloth facemask, thus indicating that wearing a mask reduces overall aerobic performance. We can assume that physical performance decrements were due to acute hypoxia, which can be explained by narrowing the arteriovenous oxygen difference and reduced maximal cardiac output (Peltonen et al., 2001; Lässing et al., 2020) but this claim needs further investigation. More likely, the primary reason for this could be attributed to perceived discomfort associated with mask-wearing. Namely, in a recent study by Driver et al. (2022), the participants reported feeling increasingly short of breath and claustrophobic at higher exercise intensities while wearing a cloth facemask. The ≈11% VO2max drop when wearing a mask compared to a mask-free environment emphasizes the concerns regarding facemask usage during high-intensity physical activity, but, still, these results are more mask-favorable than those by Driver et al. (2022), who observed a 29% decrease in VO2max. For instance, the higher decrease in VO2max in the study by Driver et al. (2022) compared with the present study may be due to the difference between exercise and environmental conditions (laboratory and field conditions). Furthermore, because the 20 m multistage fitness test was designed to determine the maximal aerobic power (Léger et al., 1988), these results further confirm the findings by Scott et al. (2018), who suggested that benefits from high-load exercise might not be augmented from additional hypoxia as for low- and moderate-load exercise.
There is strong evidence that regular physical activity and structured exercise interventions are associated with improvements in cognitive performance at both high and low intensity (Janssen et al., 2014). In the long-term view, these benefits are most likely related to improvements in cardiorespiratory fitness and consequently to cellular, molecular, and structural changes in brain regions involved in motor-cognitive function (Stillman et al., 2016). However, the benefits of short-term high-intensity exercise on cognitive function are inconclusive (Kao et al., 2017; Samuel et al., 2017), long with the mechanisms underlying those changes (Moreau and Chou, 2019). Our results complement previous findings (Alves et al., 2014; Samuel et al., 2017), showing the significant alteration in attention performance following maximal intensity exercise. Alves and colleagues (2014) showed that a single session of high-intensity interval training (HIIT) interval training reduced selective attention assessed using the Victoria Version of the Stroop test. We found that both groups experienced decrements in focused visual attention tasks whether or not the cloth mask was used, with the mask group showing significantly higher alterations than the no-mask group. The differences between the groups may be explained by various physiological factors, such as inhalation of exhaled CO2 that was mechanically trapped by the mask, which immediately triggers physiological adaptations to compensate for the lower O2 inhalation, similar to the condition during exercise in hypoxic environments (Peltonen et al., 2001; Lässing et al., 2020). In contrast, recent studies (Goh et al., 2019; Kim et al., 2016; Morris et al., 2020) showed that wearing a facemask during moderate, low and mild-intensity exercise had no effect on motor-cognitive performance. However, perceived dyspnea, manifested by 36% higher breathlessness, was observed when compared to the barefaced control group (Morris et al., 2020). In addition, another study investigated the effects of wearing a facemask during warm-up on attention (Slimani et al., 2021). Although positive changes in attention performance such as increased CP and decreased E were observed between wearing or not a cloth mask and no mask. Methodological differences between studies may have contributed to these discrepancies, as different types of facemasks (Modena et al., 2021) were used, eliciting lower or higher hypoxic environmental conditions. Also, different experimental conditions regarding the intensity of exercise, e.g., the maximum intensity of exercise until exhaustion was used in the present study versus moderate intensity of exercise involved in the study by Slimani et al. (2021) and/or prolonged sitting; and finally, different measures of interest were assessed in the studies by Samuel et al. (2017) and by Alves et al. (2014). These differences may account for some of the inconsistencies between studies that should be investigated in future experimental settings.
This study adds to the literature by providing new evidence about the effect of acute aerobic physical fitness tests with and without wearing a facemask on cognitive function. For example, a single bout of maximal aerobic exercise may have a negative effect on visual attention. Also, wearing a facemask during a physical fitness test can amplify this negative effect.
The use of a cloth facemask during maximal endurance running tests (such as the MSFT) reduced MAS, predicted VO2max, and distance covered, as well as measures of cognitive performance assessed by the test of focused visual attention d2. These results suggest avoiding cloth mask use in a sports setting, such as in an open skills, scenario (i.e., team sports), particularly in exercise with high intensity, and before any tasks that require a high level of visual attention. Further studies in different sports, evaluating the effects of prolonged, continuous, and high-intensity interval training while wearing a cloth facemask on physical performance and cognitive function are warranted.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the ethical commitee of Postgraduate School of Public Health, Genoa, Italy. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Conceptualization, MS; methodology, MS and NLB; software, MS, AP, and NLB; validation, NLB; formal analysis, MS, AP, EA and NLB; investigation, MS; resources, MS and NLB; data curation, MS and NLB; writing—original draft preparation, MS, HZ, AP, EA, and NLB; writing—review and editing, MS, HZ, AP, EA, and NLB; project administration, MS and NLB; funding acquisition, NLB. All authors have read and agreed to the published version of the manuscript.
The authors would like to thank the participants and research support staff involved in this study for their input. Researchers Supporting Project number (TURSP-2020/170), Taif University, Taif, Saudi Arabia.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alves C. R., Tessaro V. H., Teixeira L. A., Murakava K., Roschel H., Gualano B., et al. (2014). Influence of acute high-intensity aerobic interval exercise bout on selective attention and short-term memory tasks. Percept. Mot. Ski. 118 (1), 63–72. doi:10.2466/22.06.PMS.118k10w4
Ammar A., Brach M., Trabelsi K., Chtourou H., Boukhris O., Masmoudi L., et al. (2020). Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 international online survey. Nutrients 12, 1583. doi:10.3390/nu12061583
Beder A., Büyükkoçak Ü., Sabuncuo ˘glu H., Keskil Z. A., Keskil S., Buyukkocak U. (2008). Preliminary report on surgical mask induced deoxygenation during major surgery. Neurocirugía 19, 121–126. doi:10.1016/s1130-1473(08)70235-5
Brickenkamp R., Oosterveld P. (2012). D2 aandachts-en concentratie test: Handleiding (d2 test of attention: User manual). Amsterdam, Netherlands: Hogrefe.
Chung J. W., Lee O., Lee K. H. (2022). Estimation of maximal oxygen consumption using the 20 m shuttle run test in Korean adults aged 19-64 years. Sci. Sports. doi:10.1016/j.scispo.2021.10.005
do Prado D. M. L., Silvino V. O., Motta-Santos D., Dos Santos M. A. P. (2022). The effect of the protective facemask on cardiorespiratory response during aerobic exercise. Clin. Exp. Pharmacol. Physiol. 49 (4), 453–461. doi:10.1111/1440-1681.13624
Driver S., Reynolds M., Brown K., Vingren J. L., Hill D. W., Bennett M., et al. (2022). Effects of wearing a cloth facemask on performance, physiological and perceptual responses during a graded treadmill running exercise test. Br. J. Sports Med. 56 (2), 107–113. doi:10.1136/bjsports-2020-103758
Estrada E., Ferrer E., Pardo A. (2019). Statistics for evaluating pre-post change: Relation between change in the distribution center and change in the individual scores. Front. Psychol. 9, 2696. doi:10.3389/fpsyg.2018.02696
Epstein D., Korytny A., Isenberg Y., Marcusohn E., Zukermann R., Bishop B., et al. (2021). Return to training in the COVID-19 era: The physiological effects of facemasks during exercise. Scand. J. Med. Sci. Sports 31 (1), 70–75. doi:10.1111/sms.13832
Fikenzer S., Lavall T. U. D., Falz U. R. R., Hepp M. B. P., Falz R., Busse M., et al. (2020). Effects of surgical and FFP2/N95 facemasks on cardiopulmonary exercise capacity. Clin. Res. Cardiol. 109, 1522–1530. doi:10.1007/s00392-020-01704-y
Grimm K., Niederer D., Nienhaus A., Groneberg D. A., Engeroff T. (2022). Blood gas levels, cardiovascular strain and cognitive performance during surgical mask and filtering face piece application. Sci. Rep. 12 (1), 9708. doi:10.1038/s41598-022-13711-2
Hopkins S. R., Dominelli P. B., Davis C. K., Guenette J. A., Luks A. M., Molgat-Seon Y., et al. (2021). Facemasks and the cardiorespiratory response to physical activity in health and disease. Ann. Am. Thorac. Soc. 18 (3), 399–407. doi:10.1513/AnnalsATS.202008-990CME
Hötting K., Röder B. (2013). Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci. Biobehav. Rev. 37 (9), 2243–2257. doi:10.1016/j.neubiorev.2013.04.005
Janssen M., Toussaint H. M., van Mechelen W., Verhagen E. A. (2014). Effects of acute bouts of physical activity on children's attention: A systematic review of the literature. Springerplus 3, 410. doi:10.1186/2193-1801-3-410
Kao S.-C., Westfall D. R., Soneson J., Gurd B., Hillman C. H. (2017). Comparison of the acute effects of highintensityinterval training and continuousaerobicwalking on inhibitory control. Psychophysiology 54, 1335–1345. doi:10.1111/psyp.12889
Lässing J., Falz R., Pökel C., Fikenzer S., Laufs U., Schulze A., et al. (2020). Effects of surgical facemasks on cardiopulmonary parameters during steady state exercise. Sci. Rep. 10 (1), 22363–22369. doi:10.1038/s41598-020-78643-1
Lee E., Cormier K., Sharma A. (2022). Facemask use in healthcare settings: Effects on communication, cognition, listening effort and strategies for amelioration. Cogn. Res. Princ. Implic. 7 (1), 2–9. doi:10.1186/s41235-021-00353-7
Léger L., Mercier D., Gadoury C., Lambert J. (1988). The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 6 (2), 93–101. doi:10.1080/02640418808729800
Li Y., Tokura H., Guo Y. P., Wong A. S. W., Wong T., Chung J., et al. (2005). Effects of wearing N95 and surgical facemasks on heart rate, thermal stress and subjective sensations. Int. Arch. Occup. Environ. Health 78 (6), 501–509. doi:10.1007/s00420-004-0584-4
Lovakov A., Agadullina E. R. (2021). Empirically derived guidelines for effect size interpretation in social psychology. Eur. J. Soc. Psychol. 51 (3), 485–504. doi:10.1002/ejsp.2752
Mandolesi L., Polverino A., Montuori S., Foti F., Ferraioli G., Sorrentino P., et al. (2018). Effects of physical exercise on cognitive functioning and wellbeing: Biological and psychological benefits. Front. Psychol. 5, 509. doi:10.3389/fpsyg.2018.00509
Matuschek C., Moll F., Fangerau H., Fischer J. C., Zanker K., Van Griensven M., et al. (2020). Facemasks: Benefits and risks during the COVID-19 crisis. Eur. J. Med. Res. 25 (1), 32. doi:10.1186/s40001-020-00430-5
Modena R., Fornasiero A., Callovini A., Savoldelli A., Pellegrini B., Schena F., et al. (2021). Exercising at the time of the COVID-19 pandemic: Acute physiological, perceptual and performance responses of wearing face masks during sports activity. J. Sports Med. Phys. Fitness Advance online publication. doi:10.23736/S0022-4707.21.12668-4
Moreau D., Chou E. (2019). The acute effect of high-intensity exercise on executive function: A meta-analysis. Perspect. Psychol. Sci. 14 (5), 734–764. doi:10.1177/1745691619850568
Morris N. B., Piil J. F., Christiansen L., Flouris A. D., Nybo L. (2020). Prolonged facemask use in the heat worsens dyspnea without compromising motor-cognitive performance. Temperature 8, 160–165. doi:10.1080/23328940.2020.1826840
Peltonen J. E., Tikkanen H. O., Rusko H. K. (2001). Cardiorespiratory responses to exercise in acute hypoxia, hyperoxia and normoxia. Eur. J. Appl. Physiol. 85 (1), 82–88. doi:10.1007/s004210100411
Rebmann T., Carrico R., Wang J. (2013). Physiologic and other effects and compliance with long-term respirator use among medical intensive care unit nurses. Am. J. Infect. Control 41, 1218–1223. doi:10.1016/j.ajic.2013.02.017
Rosner E. (2020). Adverse effects of prolonged mask use among healthcare professionals during COVID-19. J. Infect. Dis. Epidemiol. 6 (3), 130. doi:10.23937/2474-3658/1510130
Samuel R. D., Zavdy O., Levav M., Reuveny R., Katz U., Dubnov-Raz G. (2017). The effects of maximal intensity exercise on cognitive performance in children. J. Hum. Kinet. 57, 85–96. doi:10.1515/hukin-2017-0050
Scheid J. L., Lupien S. P., Ford G. S., West S. L. (2020). Commentary: Physiological and psychological impact of facemask usage during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 17 (18), 6655. doi:10.3390/ijerph17186655
Scott B. R., Slattery K. M., Sculley D. V., Smith S. M., Peiffer J. J., Dascombe B. J. (2018). Acute physiological and perceptual responses to high-load resistance exercise in hypoxia. Clin. Physiol. Funct. Imaging 38 (4), 595–602. doi:10.1111/cpf.12451
Shaw K. A., Butcher S., Ko J. B., Absher A., Gordon J., Tkachuk C., et al. (2021a). Wearing a surgical facemask has minimal effect on performance and physiological measures during high-intensity exercise in youth ice-hockey players: A randomized cross-over trial. Int. J. Environ. Res. Public Health 18, 10766. doi:10.3390/ijerph182010766
Shaw K. A., Zello G. A., Butcher S. J., Ko J. B., Bertrand L., Chilibeck P. D. (2021b). The impact of facemasks on performance and physiological outcomes during exercise: A systematic review and meta-analysis. Appl. Physiol. Nutr. Metab. 46 (7), 693–703. doi:10.1139/apnm-2021-0143
Slimani M., Miarka B., Znazen H., Moalla W., Hammami A., Paravlic A., et al. (2021). Effect of a warm-up protocol with and without facemask-use against covid-19 on cognitive function: A pilot, randomized counterbalanced, cross-sectional study. Int. J. Environ. Res. Public Health 18, 5885.
Stillman C. M., Cohen J., Lehman M. E., Erickson K. I. (2016). Mediators of physicalactivity on neurocognitive function:areview at multiple levels of analysis. Front. Hum. Neurosci. 10, 626. doi:10.3389/fnhum.2016.00626
Tornero-Aguilera J. F., Clemente-Suárez V. J. (2021). Cognitive and psychophysiological impact of surgical mask use during university lessons. Physiol. Behav. 234, 113342. doi:10.1016/j.physbeh.2021.113342
Znazen H., Slimani M., Bragazzi N. L., Tod D. (2021). The relationship between cognitive function, lifestyle behaviours and perception of stress during the covid-19 induced confinement: Insights from correlational and mediation analyses. Int. J. Environ. Res. Public Health 18 (6), 3194. doi:10.3390/ijerph18063194
Keywords: COVID-19, facemask, exercice, neuropsychological Tests, coronavirus
Citation: Slimani M, Paravlic A, Abazovic E, Znazen H and Bragazzi NL (2022) Effect of facemask use on cognitive function during a maximal running aerobic fitness test. Front. Physiol. 13:912740. doi: 10.3389/fphys.2022.912740
Received: 26 May 2022; Accepted: 15 August 2022;
Published: 29 September 2022.
Edited by:
Leonardo Alexandre Peyré-Tartaruga, Federal University of Rio Grande do Sul, BrazilReviewed by:
Rodrigo Gomes Da Rosa, Federal University of Rio Grande do Sul, BrazilCopyright © 2022 Slimani, Paravlic, Abazovic, Znazen and Bragazzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maamer Slimani, bWFhbWVyMjAxMUBob3RtYWlsLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.