
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Physiol., 02 May 2022
Sec. Clinical and Translational Physiology
Volume 13 - 2022 | https://doi.org/10.3389/fphys.2022.887734
This article is part of the Research TopicRole of Congestion in Heart Failure: from Bench to Clinical PracticeView all 10 articles
 Belén García-Magallón1
Belén García-Magallón1 Marta Cobo-Marcos1,2*
Marta Cobo-Marcos1,2* Aitor Dávila Martiarena3Esther Montero Hernández4
Aitor Dávila Martiarena3Esther Montero Hernández4 Maria Luisa Martín Jiménez3Aránzazu Martín García5Daniel De Castro Campos1Paula Vela Martín1Fernando Hernández Terciado1
Maria Luisa Martín Jiménez3Aránzazu Martín García5Daniel De Castro Campos1Paula Vela Martín1Fernando Hernández Terciado1 Ramón Garrido González1Andrea Matutano Muñoz1Daniel Escribano García1
Ramón Garrido González1Andrea Matutano Muñoz1Daniel Escribano García1 Fernando Domínguez1,2Ana Sainz Herrero3Camino Gómez Peñalba3Pablo Garcia-Pavia1,2,6
Fernando Domínguez1,2Ana Sainz Herrero3Camino Gómez Peñalba3Pablo Garcia-Pavia1,2,6 Javier Segovia1,2
Javier Segovia1,2Background and Purpose: European Guidelines recommend early evaluation of diuresis and natriuresis after the first administration of diuretic to identify patients with insufficient diuretic response during acute heart failure. The aim of this work is to evaluate the prevalence and characteristics of patients with insufficient diuretic response according to this new algorithm.
Methods: Prospective observational single centre study of consecutive patients with acute heart failure and congestive signs. Clinical evaluation, echocardiography and blood tests were performed. Diuretic naïve patients received 40 mg of intravenous furosemide. Patients on an oupatient diuretic regimen received 2 times the ambulatory dose. The diuresis volume was assessed 6 h after the first loop diuretic administration, and a spot urinary sample was taken after 2 h. Insufficient diuretic response was defined as natriuresis <70 mEq/L or diuresis volume <600 ml.
Results: From January 2020 to December 2021, 73 patients were included (59% males, median age 76 years). Of these, 21 patients (28.8%, 95%CI 18.4; 39.2) had an insufficient diuretic response. Diuresis volume was <600 ml in 13 patients (18.1%), and 12 patients (16.4%) had urinary sodium <70 mEq/L. These patients had lower systolic blood pressure, worse glomerular filtration rate, and higher aldosterone levels. Ambulatory furosemide dose was also higher. These patients required more frequently thiazides and inotropes during admission.
Conclusion: The diagnostic algorithm based on diuresis and natriuresis was able to detect up to 29% of patients with insufficient diuretic response, who showed some characteristics of more advanced disease.
Signs and symptoms of congestion are usually the most common manifestations among patients with acute heart failure (HF) (Adams et al., 2005), and intravenous loop diuretics remain the most widely used therapy to achieve euvolaemia (Fonarow et al., 2004). Diuretic response is defined as the capacity of diuretics to induce natriuresis and diuresis (ter Maaten et al., 2015a).
Identification of patients who may have a poor diuretic response is one of the most important challenges in the field of HF, since a poor diuretic response is associated with a higher risk of rehospitalization and increased mortality (Metra et al., 2012; Neuberg et al., 2002; Valente et al., 2014; ter Maaten et al., 2015b; Testani et al., 2014; Voors et al., 2014). To date, no uniform and standard definition was available to allow the early identification of patients at risk of developing resistance to diuretic treatment during HF hospitalization.
The Position Statement from the Heart Failure Association of the European Society of Cardiology about the use of diuretics in heart failure with congestion (Mullens et al., 2019), and more recently the European Guidelines for the diagnosis and treatment of acute and chronic heart failure (McDonagh et al., 2021), have proposed an algorithm that includes the early assessment of diuresis and natriuresis after the first administration of loop diuretics in patients with acute HF, in order to detect patients with insufficient diuretic response who might benefit from diuretic intensification.
To date, data on the prevalence of early diuretic resistance according to these parameters have not yet been described.
The aim of this work is to evaluate the prevalence and features of acute HF patients who present an insufficient diuretic response according to this algorithm.
From January 2020 to December 2021, we conducted a prospective, observational and single centre study on a sample of consecutive patients aged ≥18 years whose primary admission diagnosis was acute HF and were admitted to the cardiology department. The diagnosis of acute HF was based on the current ESCF HF guidelines. In addition, NTproBNP >300 pg/dl and the presence of at least two of the following congestion criteria were required: jugular venous pressure >10 cm, lower limb edema, ascites, or pleural effusion determined by chest x-ray or pulmonary ultrasound.
Patients in cardiogenic shock and/or on dialysis were excluded. Patients in whom urine output or natriuresis could not be recorded or were missed were also excluded.
Complete clinical evaluation, echocardiogram and laboratory tests were performed. Diuretic naïve patients received 40 mg of intravenous furosemide. Patients on an outpatient diuretic regimen received 2 times the home dose. The diuresis volume was assessed 6 h after the first loop diuretic administration, and a spot urinary sample was taken after 2 h. Urinary sodium was measured using a Siemens Dimension EXL chemistry analyzer. Insufficient diuretic response was defined as natriuresis <70 mEq/L or diuresis volume <600 ml.
Values of continuous variables are given as the median and interquartile range (IQR). Categorical variables are described in absolute and relative frequencies. The associations between clinical characteristics and diuretic response were analyzed by univariate analysis using the Chi square test for categorical variables and the Mann-Whitney U test for contiuous variables. A p-value <0.05 was considered significant. All analyses were performed using STATA v.13 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX) and R software (R Foundation for Statistical Computing, version 3.6.0).
The present study conforms to the principles of the Declaration of Helsinki. Approval from the local ethics committee/internal review board was obtained at the participating centers and patients signed an informed consent.
From January 2020 to December 2021, 694 patients were admitted for acute HF. Nearly 50% of these patients did not meet the inclusion criteria as they presented predominant pulmonary congestion. About 30% could not be included as the treating physician didn’t follow the ESC protocol, in part due to Covid-19 pandemic.
A final sample of 73 patients were included (59% males, median age 76 years [IQR: 70–85]). Four initially included patients were not finally analysed as urinary output was not correctly collected. Of the remaining sample (73/78), 21 patients (28.8%) met the definition of early insufficient diuretic response.
The diuresis volume was <600 ml in 13 patients (18.1%), and 12 patients (16.4%) had urinary sodium <70 mEq/L. Only 4 patients (5.5%) had both low urinary sodium and decreased urine output.
Compared with patients with an adequate diuretic response, these patients had lower systolic blood pressure (133 mmHg [IQR: 116–148] vs. 148 [IQR: 124–175], p = 0.043), worse glomerular filtration rate (49 ml/min/1.73 m2 [IQR: 28–63] vs. 69 [44–86], p = 0.044), and showed greater neurohormonal activation (aldosterone levels: 19 ng/dl [IQR: 11–40] vs. 10 [IQR: 7–14], p = 0.005). This group of patients presented a higher percentage of previous admission due to HF (42.9 vs. 17.6%, p = 0.025), and their basal furosemide dose was also higher (80 mg [IQR: 5–88] vs. 40 [IQR: 0–60], p = 0.032) Table 1.
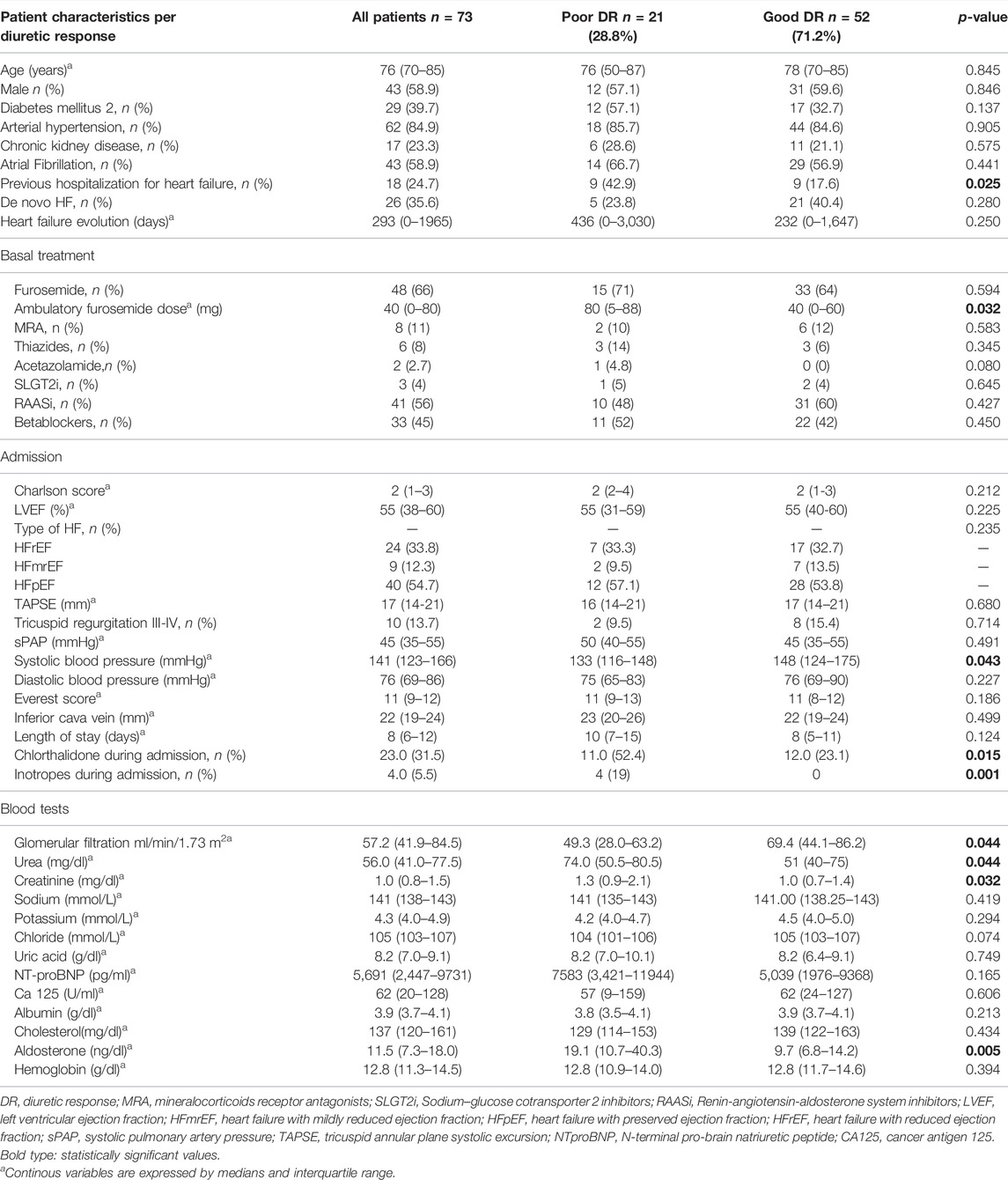
TABLE 1. Legend. Patient characteristics per diuretic response (n = 73).
During admission, patients with poor diuretic response required more frequently inotropes (19 vs. 0%, p = 0.001), and thiazides (52.4 vs. 23.1%, p = 0.015).
To date, this is the first study to show the performance of the algorithm proposed by the HF European guidelines for the early assessment of diuretic response in a cohort of patients with acute HF.
This algorithm based on diuresis volume and natriuresis was able to detect up to 29% of patients with insufficient diuretic response who might benefit from enhanced diuretic treatment.
These patients showed some characteristics traditionally described in patients with diuretic resistance in other settings.
Sodium and fluid retention is a hallmark of HF. As effective diuretic response is produced by natriuresis, urinary sodium has emerged as a useful parameter to predict natriuretic response in patients with HF soon after diuretic administration (Verbrugge et al., 2014), which can be measured from a urinary spot sample with good accuracy (Testani et al., 2016). In this line, several studies have reported the usefulness of natriuresis after the first dose of diuretic to predict long-term adverse events (Singh et al., 2014; Honda et al., 2018; Luk et al., 2018; Biegus et al., 2019; Hodson et al., 2019), and two studies have also suggested its usefulness in detecting the development of worsening HF during hospitalization (Collins et al., 2019; Cobo -Marcos et al., 2020).
Although a high diuresis volume following a first intravenous loop diuretic administration is usually associated with good diuretic response and a high urinary sodium (Testani et al., 2016; Singh et al., 2014), some data indicate that in patients with low to medium volume output, spot urinary sodium content offers independent prognostic information (Brinkley et al., 2018). Indeed, in our cohort only 4 patients (5.5%) had both low urinary sodium and a decreased urine output.
Therefore, a spot urine sodium content of <50–70 mEq/L after 2 h, and/or an hourly urine output <100–150 ml during the first 6 h, provide additional information and could identify patients with an insufficient diuretic response.
The present study confirms findings from previous studies, that a poor response is associated with some features of more advanced disease (Metra et al., 2012; Neuberg et al., 2002; Valente et al., 2014; ter Maaten et al., 2015b; Testani et al., 2014; Voors et al., 2014; ter Maaten et al., 2015a). In our cohort 43% of the patients had a previous HF hospitalization, and the outpatient diuretic dose was high. Besides, compared with patients with an adequate diuretic response, these patients had lower systolic blood pressure at admission, worse glomerular filtration rate, and showed greater neurohormonal activation. It should be noted that variables such as age, left ventricular ejection fraction or natriuretic peptides are not usually associated with the diuretic response in different studies (Metra et al., 2012; Neuberg et al., 2002; Valente et al., 2014; ter Maaten et al., 2015b; Testani et al., 2014; Voors et al., 2014; ter Maaten et al., 2015a). Furthermore, in our cohort no other clinical (Charlson index, Everest score) or echocardiogram features (TAPSE, inferior cava vein) were different between both populations. These data highlight the role of this algorithm in the evaluation of diuretic response in this setting.
Finally, although this study didn’t assess long term events, we showed that patients with a worse diuretic response required diuretic association and inotropes more frequently during admission.
At this time, two other studies are evaluating the performance of this diagnostic strategy, the ENACT-HF trial (Rationale and Design of the Efficacy of a Standardized Diuretic Protocol in Acute Heart Failure Study) (Dauw et al., 2021), and the PUSH-HF trial (Natriuresis-guided therapy in acute heart failure: rationale and design of the Pragmatic Urinary Sodium-based treatment algoritHm in Acute Heart) (Maaten et al., 2022).
It should be noted that this novel algorithm involves a more proactive approach and closer monitoring of the diuretic response.
This requires specific training and coordinated and continuos collaboration between the professionals involved in the management of HF patients, especially with emergency department staff, in order to extend the implementation of this diuretic protocol.
Our cohort consisted of 73 patients from one academic institution so the findings may not be generalizable to the wider acute HF population.
In addition, there is a low percentage of patients included (11%) in terms of overall acute HF admissions. Patients with predominantly pulmonary congestion without other congestion signs were not included. Some patients didn’t follow the protocol by decision of the responsible staff. Recruitment was also affected by the COVID-19 pandemic.
The diagnostic algorithm based on diuresis and natriuresis provided complementary information and was capable of early detection of up to 29% of patients with acute HF from this cohort who presented an insufficient diuretic response.
This finding may help to stratify patients who may benefit from more intense treatment for decongestion during hospital admission.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Comité de Ética e Investigación con Medicamentos (CEIm) del Hospital Puerta de Hierro Majadahonda. The patients/participants provided their written informed consent to participate in this study.
MC-M, FD, PG-P and JS contributed to conception and design of the study. AiM, MM, AS, and CG, contributed to the patient inclusion. DD, PM, FT, RG, AnM, and DE contributed to the data inclusion on the database. AG organized the laboratory tests. MC-M organized the database. BG-M performed the statistical analysis. BG-M and EH wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
This work was partially supported by grants from the Instituto de Salud Carlos III (PI20/00689). (Co-funded by European Regional Development Fund/European Social Fund “A way to make Europe”/“Investing in your future”). We acknowledge funding from a grant from the Spanish Society of Cardiology (Heart Failure Section, 2019).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Adams K. F., Fonarow G. C., Emerman C. L., LeJemtel T. H., Costanzo M. R., Abraham W. T., et al. (2005). Characteristics and Outcomes of Patients Hospitalized for Heart Failure in the United States: Rationale, Design, and Preliminary Observations from the First 100,000 Cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am. Heart J. 149, 209–216. doi:10.1016/j.ahj.2004.08.005
Biegus J., Zymliński R., Sokolski M., Todd J., Cotter G., Metra M., et al. (2019). Serial Assessment of Spot Urine Sodium Predicts Effectiveness of Decongestion and Outcome in Patients with Acute Heart Failure. Eur. J. Heart Fail. 21, 624–633. doi:10.1002/ejhf.1428
Brinkley D. M., Burpee L. J., Chaudhry S.-P., Smallwood J. A., Lindenfeld J., Lakdawala N. K., et al. (2018). Spot Urine Sodium as Triage for Effective Diuretic Infusion in an Ambulatory Heart Failure Unit. J. Card. Fail. 24, 349–354. doi:10.1016/j.cardfail.2018.01.009
Cobo-Marcos M., Zegri-Reiriz I., Remior-Perez P., Garcia-Gomez S., Garcia-Rodriguez D., Dominguez-Rodriguez F., et al. (2020). Usefulness of Natriuresis to Predict In-Hospital Diuretic Resistance. Am. J. Cardiovasc. Dis. 10 (4), 350–355.
Collins S. P., Jenkins C. A., Baughman A., Miller K. F., Storrow A. B., Han J. H., et al. (2019). Early Urine Electrolyte Patterns in Patients with Acute Heart Failure. ESC Heart Fail. 6, 80–88. doi:10.1002/ehf2.12368
Dauw J., Lelonek M., Zegri‐Reiriz I., Paredes‐Paucar C. P., Zara C., George V., et al. (2021). Rationale and Design of the Efficacy of a Standardized Diuretic Protocol in Acute Heart Failure Study. ESC Heart Fail. 8 (6), 4685–4692. doi:10.1002/ehf2.13666
Fonarow G. C., Corday E. ADHERE Scientific Advisory Committee (2004). Overview of Acutely Decompensated Congestive Heart Failure (ADHF): a Report from the ADHERE Registry. Heart Fail. Rev. 9, 179–185. doi:10.1007/s10741-005-6127-6
Hodson D. Z., Griffin M., Mahoney D., Raghavendra P., Ahmad T., Turner J., et al. (2019). Natriuretic Response Is Highly Variable and Associated with 6-Month Survival. JACC: Heart Fail. 7, 383–391. doi:10.1016/j.jchf.2019.01.007
Honda S., Nagai T., Nishimura K., Nakai M., Honda Y., Nakano H., et al. (2018). Long-term Prognostic Significance of Urinary Sodium Concentration in Patients with Acute Heart Failure. Int. J. Cardiol. 254, 189–194. doi:10.1016/j.ijcard.2017.08.053
Luk A., Groarke J. D., Desai A. S., Mahmood S. S., Gopal D. M., Joyce E., et al. (2018). First Spot Urine Sodium after Initial Diuretic Identifies Patients at High Risk for Adverse Outcome after Heart Failure Hospitalization. Am. Heart J. 203, 95–100. doi:10.1016/j.ahj.2018.01.013
Maaten J. M., Beldhuis I. E., Meer P., Krikken J. A., Coster J. E., Nieuwland W., et al. (2022). Natriuresis‐guided Therapy in Acute Heart Failure: Rationale and Design of the Pragmatic Urinary Sodium‐based Treatment algorithm in Acute Heart Failure (PUSH‐AHF ) Trial. Eur. J Heart Fail 24 (2), 385–392. doi:10.1002/ejhf.2385
McDonagh T. A., Metra M., Adamo M., Gardner R. S., Baumbach A., Böhm M., et al. ESC Scientific Document Group (2021). 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 42 (36), 3599–3726. doi:10.1093/eurheartj/ehab368
Metra M., Davison B., Bettari L., Sun H., Edwards C., Lazzarini V., et al. (2012). Is Worsening Renal Function an Ominous Prognostic Sign in Patients with Acute Heart Failure? Circ. Heart Fail. 5, 54–62. doi:10.1161/circheartfailure.111.963413
Mullens W., Damman K., Harjola V.-P., Mebazaa A., Brunner-La Rocca H.-P., Martens P., et al. (2019). The Use of Diuretics in Heart Failure with Congestion - a Position Statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 21, 137–155. doi:10.1002/ejhf.1369
Mullens W., Verbrugge F. H., Nijst P., Tang W. H. W. (2017). Renal Sodium Avidity in Heart Failure: from Pathophysiology to Treatment Strategies. Eur. Heart J. 38, 1872–1882. doi:10.1093/eurheartj/ehx035
Neuberg G. W., Miller A. B., O'Connor C. M., Belkin R. N., Carson P. E., Cropp A. B., et al. (2002). Diuretic Resistance Predicts Mortality in Patients with Advanced Heart Failure. Am. Heart J. 144, 31–38. doi:10.1067/mhj.2002.123144
Singh D., Shrestha K., Testani J. M., Verbrugge F. H., Dupont M., Mullens W., et al. (2014). Insufficient Natriuretic Response to Continuous Intravenous Furosemide Is Associated with Poor Long-Term Outcomes in Acute Decompensated Heart Failure. J. Card. Fail. 20, 392–399. doi:10.1016/j.cardfail.2014.03.006
ter Maaten J. M., Dunning A. M., Valente M. A. E., Damman K., Ezekowitz J. A., Califf R. M., et al. (2015). Diuretic Response in Acute Heart Failure-An Analysis from ASCEND-HF. Am. Heart J. 170, 313–321. doi:10.1016/j.ahj.2015.05.003
ter Maaten J. M., Valente M. A. E., Damman K., Hillege H. L., Navis G., Voors A. A. (2015). Diuretic Response in Acute Heart Failure-Pathophysiology, Evaluation, and Therapy. Nat. Rev. Cardiol. 12, 184–192. doi:10.1038/nrcardio.2014.215
Testani J. M., Hanberg J. S., Cheng S., Rao V., Onyebeke C., Laur O., et al. (2016). Rapid and Highly Accurate Prediction of Poor Loop Diuretic Natriuretic Response in Patients with Heart Failure. Circ. Heart Fail. 9 (1), e002370. doi:10.1161/CIRCHEARTFAILURE.115.002370
Testani J. M., Brisco M. A., Turner J. M., Spatz E. S., Bellumkonda L., Parikh C. R., et al. (2014). Loop Diuretic Efficiency. Circ. Heart Fail. 7, 261–270. doi:10.1161/circheartfailure.113.000895
Valente M. A. E., Voors A. A., Damman K., Van Veldhuisen D. J., Massie B. M., O'Connor C. M., et al. (2014). Diuretic Response in Acute Heart Failure: Clinical Characteristics and Prognostic Significance. Eur. Heart J. 35, 1284–1293. doi:10.1093/eurheartj/ehu065
Verbrugge F. H., Dupont M., Steels P., Grieten L., Swennen Q., Tang W. H. W., et al. (2014). The Kidney in Congestive Heart Failure: 'are Natriuresis, Sodium, and Diuretics Really the Good, the Bad and the Ugly?'. Eur. J. Heart Fail. 16, 133–142. doi:10.1002/ejhf.35
Keywords: diuretic, acute heart failure, natriuresis, diuretic response, diuretic resistance
Citation: García-Magallón B, Cobo-Marcos M, Martiarena AD, Hernández EM, Martín Jiménez ML, García AM, De Castro Campos D, Martín PV, Terciado FH, González RG, Matutano Muñoz A, Escribano García D, Domínguez F, Sainz Herrero A, Gómez Peñalba C, Garcia-Pavia P and Segovia J (2022) Role of Early Assesment of Diuresis and Natriuresis in Detecting In-Hospital Diuretic Resistance in Acute Heart Failure. Front. Physiol. 13:887734. doi: 10.3389/fphys.2022.887734
Received: 01 March 2022; Accepted: 14 April 2022;
Published: 02 May 2022.
Edited by:
Jesus Alvarez-Garcia, Ramón y Cajal University Hospital, SpainReviewed by:
Rafael De La Espriella, Hospital Clínico Universitario de Valencia, SpainCopyright © 2022 García-Magallón, Cobo-Marcos, Martiarena, Hernández, Martín Jiménez, García, De Castro Campos, Martín, Terciado, González, Matutano Muñoz, Escribano García, Domínguez, Sainz Herrero, Gómez Peñalba, Garcia-Pavia and Segovia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marta Cobo-Marcos, bWFydGFtYXJpYS5jb2JvQHNhbHVkLm1hZHJpZC5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.