 Yuanyuan Cao
Yuanyuan Cao Peijun Li
Peijun Li Yingqi Wang
Yingqi Wang Xiaodan Liu2*
Xiaodan Liu2* Weibing Wu
Weibing Wu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Physiol. , 02 May 2022
Sec. Striated Muscle Physiology
Volume 13 - 2022 | https://doi.org/10.3389/fphys.2022.872277
Chronic obstructive pulmonary disease (COPD) affects the whole body and causes many extrapulmonary adverse effects, amongst which diaphragm dysfunction is one of the prominent manifestations. Diaphragm dysfunction in patients with COPD is manifested as structural changes, such as diaphragm atrophy, single-fibre dysfunction, sarcomere injury and fibre type transformation, and functional changes such as muscle strength decline, endurance change, diaphragm fatigue, decreased diaphragm mobility, etc. Diaphragm dysfunction directly affects the respiratory efficiency of patients and is one of the important pathological mechanisms leading to progressive exacerbation of COPD and respiratory failure, which is closely related to disease mortality. At present, the possible mechanisms of diaphragm dysfunction in patients with COPD include systemic inflammation, oxidative stress, hyperinflation, chronic hypoxia and malnutrition. However, the specific mechanism of diaphragm dysfunction in COPD is still unclear, which, to some extent, increases the difficulty of treatment and rehabilitation. Therefore, on the basis of the review of changes in the structure and function of COPD diaphragm, the potential mechanism of diaphragm dysfunction in COPD was discussed, the current effective rehabilitation methods were also summarised in this paper. In order to provide direction reference and new ideas for the mechanism research and rehabilitation treatment of diaphragm dysfunction in COPD.
COPD is a common respiratory disease caused by exposure to harmful particles or gases, characterised by persistent respiratory symptoms and restricted airflow (Singh et al., 2019). According to the World Health Organization statistical report, COPD is the third leading cause of death in the world, causing 3.23 million deaths in 2019. The high incidence and mortality of COPD make it the fifth disease aggravating the global economic burden. In addition to damaging the airway, alveoli and pulmonary vessels, COPD also damages the circulatory system, nervous system, motor system and other systems, resulting in remarkable extrapulmonary adverse effects (Vanfleteren et al., 2016). Diaphragm dysfunction is present at all stages of COPD development (Donaldson et al., 2012). The diaphragm is the most important inspiratory muscle and the maximum inspiratory pressure is an independent determinant of survival in patients with severe COPD. Diaphragm dysfunction directly leads to dyspnoea and respiratory failure (Elsawy, 2017). It is also associated with increased risk of hospitalisation and increased disease mortality due to acute exacerbation of COPD (Vilaró et al., 2010). Diaphragm dysfunction in patients with COPD is mainly manifested in structural and functional changes, including negative changes and positive adaptive changes. The mechanism of diaphragm dysfunction may be related to systemic inflammation, oxidative stress, hyperinflation, chronic hypoxia, and malnutrition. These factors interact to affect the diaphragm function. Rehabilitation is an individualised and comprehensive treatment plan that is based on existing rehabilitation methods after the assessment of patients’ physique and disease progression. Pulmonary rehabilitation has been shown to be the most effective treatment strategy for improving health outcomes and exercise tolerance in patients with COPD according to the 2022 Global Initiative on Chronic Obstructive Pulmonary Disease guidelines. Studies have shown that rehabilitation could increase diaphragmatic endurance and strength, reduce airflow resistance and improve dyspnoea in patients with COPD, thereby reducing the incidence of diaphragm dysfunction (Gosselink et al., 2011). Therefore, in the present paper, the structural and functional changes and mechanisms of diaphragm dysfunction in COPD were discussed. The common rehabilitation treatment methods of diaphragm dysfunction in COPD, such as Inspiratory muscle training (IMT), exercise intervention and nutritional support, were also summarised to provide reference and new ideas for the rehabilitation and research direction of diaphragm dysfunction in COPD.
The function of diaphragm depends largely on its physiological characteristics at the structural level. Negative changes and positive adaptive changes exist at the same time in the structural changes of diaphragm in patients with COPD. The balance between negative changes and positive changes is closely related to the functional performance and changes of diaphragm in each stage of the disease, which has a profound impact on diaphragm dysfunction and disease progression.
Amongst the negative structural changes of diaphragm in patients with COPD, diaphragmatic atrophy is an important pathological basis of dysfunction (Ottenheijm et al., 2005). Studies have shown a 30% reduction in myosin heavy chain content in patients with mild to moderate COPD and a 30%–40% reduction in diaphragmatic muscle fibre cross-sectional area in patients with severe COPD (Levine et al., 2013). These findings suggested that diaphragmatic atrophy occurs early in the disease and may be present at all stages of the disease. In addition, reduced myosin content in the diaphragm induced changes in the contractile properties and passive properties of diaphragm single fibres in COPD patients. Levine and colleagues’ study showed a 35% reduction in the force generated by diaphragm fibres in patients with severe COPD, indicating a decrease in the contractile properties of diaphragm single fibres (Levine et al., 2003). Moore and colleagues’ data indicated that diaphragmatic fibres exhibit less passive tension during fibre stretching in patients with mild to moderate COPD than in patients without COPD, suggesting a reduction in the diaphragmatic single fibre elasticity (Moore et al., 2006). Sarcomere is the basic structure and function unit of muscle. Patients with COPD have a deletion of serial sarcomeres (Levine et al., 2013). Sarcomere disruption is more evident in patients with moderate and severe COPD(Orozco-Levi et al., 2001). With chronic hyperinflation, there is a 10%–15% loss of sarcomeres in the diaphragmatic muscle fibres (De Troyer, 1997). The biomechanical defects of diaphragm due to changes in diaphragm shape are the main negative factors for diaphragm dysfunction. Pulmonary hyperinflation and deformation of the thorax cause the diaphragm to drop in position, shorten and flatten the normal dome shape (Salito et al., 2015; Laghi et al., 2021). These changes put the diaphragm at a mechanical disadvantage, resulting in a reduced ability of the diaphragm to generate flow and pressure, increasing respiratory work, and causing diaphragmatic fatigue (Hellebrandová et al., 2016).
In addition to the negative changes, there are some positive adaptive structural changes in the diaphragm of patients with COPD. Due to pulmonary hyperinflation, the length of diaphragm muscle segments is shortened in patients with COPD and the greater the lung volume, the shorter the muscle segments are (Orozco-Levi et al., 1999). Muscle segments shortening may result in a partial reversal of the displacement of the diaphragm’s length-tension curve, increasing its ability to maintain tension (Gea et al., 2013), and enhance endurance. The transformation of diaphragm fibre type is the most remarkable structural and physiological characteristic of diaphragm in patients with COPD. The contraction rate and main metabolic types of muscle fibres determine its antifatigue ability. Studies have shown that the diaphragm type II fibres in patients with COPD are transformed into type I fibres with higher oxidation degree, resulting in an increase in the proportion of type I fibres (Nguyen et al., 2000; Levine et al., 2002). To some extent, this transformation is a positive adaptation of the diaphragm muscle. The peripheral vascular network of type I fibre is richer than that of type II fibre and it contains more myoglobin and mitochondria than that of type II fibre. The increase of capillary density, myoglobin content and mitochondrial density can improve the oxygen supply efficiency of diaphragm. Therefore, it compensatively increases the endurance and fatigue resistance of diaphragm (Levine et al., 2003). To some extent, they help the diaphragm adapt to the high load due to increased airway resistance that lowers airflow. However, beyond the compensatory range could cause a decrease in diaphragm endurance. The experimental data of rats show that type I fibres produced less force than type II fibres (Geiger et al., 2000), possibly leading to decreased diaphragm strength in patients with mild to severe COPD.
Therefore, in summary, although positive adaptive changes in diaphragm structure could be found in patients with COPD, negative structural changes still dominate (Levine et al., 2013). In the early and middle stages of the disease, a balance exists between positive and negative changes (Barreiro and Gea, 2015). However, this balance quickly shifts towards negative outcomes as the disease progresses (Gayan-Ramirez and Decramer, 2013).
Diaphragm dysfunction could be classified as partial or total loss of diaphragmatic function and it may involve one or both hemidiaphragms (McCool and Tzelepis, 2012). Diaphragm dysfunction in patients with COPD is mostly unilateral diaphragmatic paralysis, which is usually asymptomatic. However, dyspnoea may occur during exertion and supine. (Hart et al., 2002; Steier et al., 2008). From the specific function, patients with COPD with diaphragm dysfunction is mainly manifested as decreased diaphragm muscle strength, endurance changes, reduced mobility, and diaphragm fatigue.
Diaphragm muscle strength mainly depends on muscle fibre cross-sectional area, muscle fibre type and initial length (Mathur et al., 2014). The cross-sectional area of diaphragm muscle fibre in patients with COPD decreases, the muscle fibre type changes from fast twitch muscle to slow twitch muscle and the pulmonary hyperinflation shortens the length of diaphragm muscle (Finucane et al., 2005), resulting in the decline of diaphragm muscle strength in patients with COPD. Levine and colleagues found that although the type conversion of diaphragm fibres increased the ATP production capacity, the utilisation rate of ATP decreased, the specific force decreased, resulting in the weakening of the pressure-generating ability (Levine et al., 2003). Transdiaphragmatic pressure (Pdi) is a more direct indicator of diaphragm muscle strength. The maximum Pdi in patients with severe COPD is only 60% of that in healthy controls (McCool and Tzelepis, 2012). Increased lung volume and altered chest wall geometry led to diaphragm shortening (Silva et al., 2013). An early pioneering study found that the diaphragm of patients was on average 28% shorter than that of healthy subjects (Rochester and Braun, 1985). The diaphragm is shortened to the suboptimal length, which makes the conversion of diaphragm tension into trans-diaphragm pressure ineffective, so as to reduce the pressure-generating ability. Furthermore, pulmonary hyperinflation shortens the operation length of diaphragm and changes the mechanical linkage between its various parts, damaging the muscle strength of diaphragm (Nair et al., 2019).
Patients with COPD showed fragile positive fitness for diaphragm endurance (Papavramidis et al., 2011). The respiratory controller imposes a shorter duty cycle, and the transformation of diaphragm fibre to type II muscle fibre with higher oxidation degree is the main reason for the increase of endurance (Wijnhoven et al., 2006). However, studies have shown that patients with stable COPD have a lower mean diaphragm tension-time index (which indicates the ability of the inspiratory muscles to maintain sufficient pressure generation over time) than normal subjects (Ceriana et al., 2017), indicating decreased diaphragm endurance in patients with COPD. The enhanced endurance adaptations may only be maintained within a certain range. The reasons for this are the low ATP utilization in the diaphragm and the fact that the load on the diaphragm continues to rise with disease severity. Eventually, diaphragmatic endurance is further impaired due to increased muscle weakness and a series of factors that limit regeneration (Macgowan et al., 2001).
Compared with healthy individuals, patients with COPD had reduced diaphragmatic mobility (Gonçalves et al., 2018). Reduced diaphragmatic mobility has been found to be an important factor in decreased exercise tolerance and increased dyspnoea in patients with COPD(Paulin et al., 2007). The maximum level of diaphragm excursion (DEmax) can fully predict improvement in exercise tolerance in patients with COPD. Another study found a strong correlation between diaphragmatic mobility and maximal voluntary ventilation (MVV) in COPD patients, suggesting that greater diaphragmatic mobility was associated with better ventilatory capacity (Rocha et al., 2017). Increased airway resistance, pulmonary hyperinflation and air trapping are the main factors affecting diaphragm activity. Rocha et al. found that the decrease of diaphragm mobility in patients with COPD was related to airway obstruction (Rocha et al., 2017). Shiraishi et al. (2021). found that reduced diaphragmatic mobility may be associated with a range of symptoms associated with dynamic pulmonary hyperinflation. However, another study suggested that diaphragm mobility correlated strongly with pulmonary function parameters that quantify air trapping, moderately with airway resistance and weakly with pulmonary hyperinflation (Dos Santos Yamaguti et al., 2008).
Diaphragmatic fatigue in patients with COPD is characterized by reversible weakening of diaphragmatic contractility and decrease of contractile speed. From an overall point of view, it is the change of muscle output power. Due to hyperinflation and long-term unfavourable mechanical position, the diaphragm is forced to remain in a state of contraction, which is easy to cause the decline of diaphragm compliance and contraction force, leading to diaphragm fatigue (De Troyer, 1997). Additionally, muscle fibre atrophy and damage to the airway and lung parenchymal structure in patients with COPD lead to increased laborious respiratory movement, resulting in reduced fatigue resistance (McKenzie et al., 2009) (Figure 1).
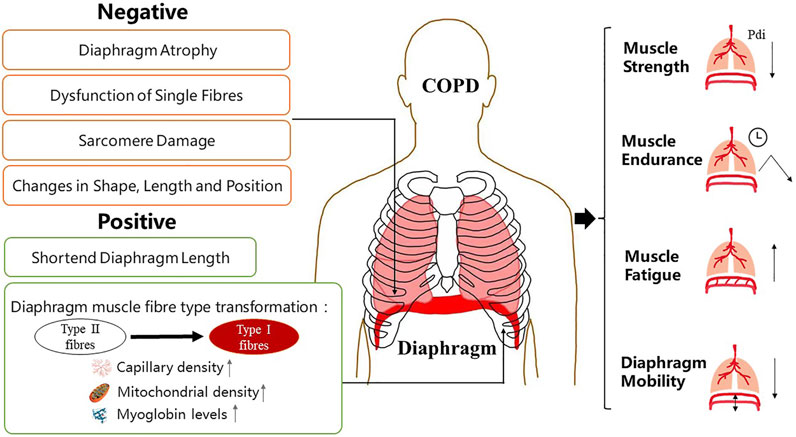
FIGURE 1. Manifestations of diaphragm dysfunction in COPD. Diaphragm dysfunction in patients with COPD is mainly manifested in structural and functional changes. Changes in diaphragm structure include both negative and positive changes. The function of diaphragm depends largely on its physiological characteristics at the structural level. COPD, chronic obstructive pulmonary disease.
According to recent studies, COPD is a systemic disease involving chronic low-grade inflammation and altered protein metabolism throughout the body (Mador and Sethi, 2013). Studies have shown that patients with COPD have a systemic inflammatory response, including the activation of inflammatory cells and increased levels of multiple circulating inflammatory factors, such as tumour necrosis factor-α (TNF-α), interleukin (IL)-1, IL-6, IL-8, and C-reactive protein (Huang et al., 2016). Elevated levels of inflammatory cytokines TNF-α and IL-6 were also found in the diaphragm in patients with severe COPD (Barreiro et al., 2011). Studies have shown that the levels of inflammatory factors are negatively correlated with diaphragm quality and muscle strength, suggesting that systemic inflammation is involved in the occurrence and development of diaphragm dysfunction in patients with COPD (Lin et al., 2010). Different studies have found that the negative effects of systemic inflammation on diaphragm dysfunction in COPD may be caused by multiple pathways.
TNF-α plays a major role in diaphragmatic catabolism and the levels of TNF-α in serum and diaphragm of COPD rats are higher than those of the normal control group, leading to diaphragmatic atrophy. TNF-α may directly stimulate total muscle protein, resulting in decreased protein content and loss of muscle-specific protein. It interacts with its receptor to activate caspase-8, thereby initiating the apoptosis pathway. It also activates the nuclear factor-κB (NF-κB) signalling pathway and induces apoptosis or muscle degradation.
NF-κB is an important signalling pathway involved in diaphragmatic mass depletion. Haegens and colleagues’ study reported that NF-κB activation and ubiquitin-proteasome system (UPS) mediated protein degradation are required for pulmonary inflammation-induced diaphragm atrophy (Haegens et al., 2012). Genetic studies have shown that inhibition of NF-κB activity promotes muscle regeneration (Mourkioti et al., 2006). Inflammatory factors may upregulate the expression of E3 ubiquitin ligase atrogin-1/MAFbx and muscle ring finger protein 1 (MURF-1) by influencing the NF-κB signalling pathway, so as to accelerate muscle protein decomposition (Attaix et al., 2005). Activation of NF-κB decreased the expression of MyoD mRNA, disrupted the stability of MyoD protein, and decreased the level of MyoD protein (Shirakawa et al., 2021). It could also inhibit muscle formation by suppressing the expression of growth-stimulating molecules, thus interfering with the regeneration of diaphragm and eventually leading to diaphragm dysfunction (Vogiatzis et al., 2007).
In addition, systemic inflammatory mediators indirectly contribute to muscle atrophy through dysregulation of tissue and organ systems, including GCs via the hypothalamic-pituitary-adrenal (HPA) axis, digestion leading to anorexia-cachexia, and altered liver and adipocyte behaviour, all of which subsequently lead to the development of diaphragmatic atrophy (Webster et al., 2020). The exact relationship between systemic inflammation and the process of diaphragmatic atrophy in COPD patients is currently unknown due to the lack of longitudinal data. The specific mechanisms of inflammatory response involved in diaphragm dysfunction have also not been fully elucidated and should be further investigated.
Oxidative stress refers to a state of imbalance between oxidation and antioxidant effects in the body. For the first time, Barreiro and colleagues detected higher levels of oxidative stress in the diaphragm of patients with severe COPD than in control muscles, resulting in increased diaphragmatic muscle depletion and diaphragm dysfunction (Barreiro et al., 2005). Reactive oxygen species (ROS) and reactive nitrogen species (RNS) are the triggering factors of diaphragm dysfunction. A certain amount of reactive oxides has a certain effect on muscle fibre adaptation to exercise or disuse state (Ábrigo et al., 2018). However, high levels of ROS and RNS over a long period of time could lead to proteolysis and potential apoptosis (Ji et al., 2006). Oxidative stress promotes muscle atrophy by activating various proteolytic pathways. UPS is the main pathway for intracellular protein degradation and oxidative stress increases protein degradation in the diaphragm by activating the UPS, resulting in diaphragmatic atrophy (Gomes-Marcondes and Tisdale, 2002; Pomiès et al., 2016). Calprotease is a Ca2+-dependent cysteine protease, which could catalyse the restricted hydrolysis of various substrates and plays an important role in the occurrence and development of muscular dystrophy. High ROS levels inhibit sarcoplasmic Ca2+-ATPase activity and prevent Ca2+ reabsorption into the sarcoplasmic reticulum, thus increasing intracellular free Ca2+ concentration and leading to calprotease activation, which promotes muscle degradation (Powers and Jackson, 2008; Whidden et al., 2010). Caspase is closely related to apoptosis and it participates in the apoptosis regulation of muscle cells (Kuwano and Hara, 2000). Oxidative stress can also activate caspase-3 in muscle cells and promote degradation of the complete actin-myosin complex and apoptosis of muscle nucleus cells, resulting in muscle atrophy and loss of muscle nucleus (Du et al., 2004). In addition to the activation of proteolytic enzymes, ROS and RNS modify the diaphragm with protein oxidation, which results in reduced protein activity and makes it more vulnerable to protease degradation. Oxidative damage to muscle proteins prior to characteristic respiratory changes may lead to muscle loss and dysfunction in patients with COPD (Barreiro et al., 2010). Additionally, muscle redox disorder caused by oxidative stress and altered expression of redox-sensitive genes may be responsible for increased susceptibility to diaphragm fatigue (Orozco-Levi, 2003). In conclusion, oxidative stress activates multiple proteolytic pathways, increases protein oxidation and results in altered expression of redox-sensitive genes, leading to diaphragm dysfunction.
Pulmonary hyperinflation can be due to loss of lung elastic recoil and airway closure at higher volumes, which significantly increases the mechanical load of the diaphragm (Krieger, 2009). The respiratory work of healthy individuals is relatively small and the diaphragm could easily maintain this level of power output. However, the increase of airway resistance places higher demands on diaphragm endurance, which could lead to dyspnoea and reduced exercise tolerance. Hyperinflation results in energy loss and breakdown of muscle proteins, leading to diaphragm atrophy, which makes it even less able to withstand increased stress. Increases in acute and chronic stresses lead to fibre damage and fibrosis of the diaphragm (Scott et al., 2006). During exacerbations of COPD, additional damage to sarcomere may occur when patients are faced with acute diaphragm load, which may further impair diaphragm function (Orozco-Levi et al., 2001), leading to respiratory failure. The increased workload on the diaphragm of patients with severe COPD may also induce oxidative stress and aggravate diaphragm wear by increasing the production of oxidants (Barreiro et al., 2005). Meanwhile, hyperinflation results in changes in diaphragm shape in patients with COPD. A normal diaphragm is located between the thoracoabdominal cavity and it closes the lower thoracic orifice. It is a thin fornix muscle with a flat central part and upward protruding on both sides. The fornix is low on the left and high on the right. By using chest radiographs and spiral CT, Sverzellati et al. found that excessive ventilation resulted in an increase in the radius of curvature of the diaphragm (Sverzellati et al., 2013). Thus, the shape of the diaphragm is nearly flat (Laghi et al., 2021). Normal dome shape plays an important role in diaphragm function. In patients with COPD, diaphragm shape changes and position downshifts away from the optimal mechanical position, resulting in increased respiratory work and diaphragm fatigue (Gayan-Ramirez and Decramer, 2013). In summary, pulmonary hyperinflation increases the dynamic load on the diaphragm, leading to varying degrees of damage and loss of function of the diaphragm cells and subcellular structures. Overloading increases diaphragmatic oxidative stress, leading to biomechanical defects in the diaphragm and ultimately to diaphragmatic dysfunction.
Patients with COPD suffer from chronic hypoxia with varying degrees of hypoxemia and hypercapnia due to prolonged expiratory flow obstruction, dysfunction of ventilation and retention of sputum. Studies have shown that chronic hypoxia could reduce the aerobic capacity of the diaphragm, resulting in changes in the histological morphology, contractile properties, and metabolism of the diaphragm (Shiota et al., 2004), causing the diaphragm to be unable to cope with the increased load, which may cause diaphragm dysfunction. Histologically, a reduction in muscle fibre cross-sectional area has been observed in the diaphragm in animal models of chronic hypoxia (McMorrow et al., 2011; Gamboa and Andrade, 2012), decreased mitochondrial density and related protein loss in diaphragm muscle (Gamboa and Andrade, 2010). In terms of contractile properties, chronic hypoxia could reduce the rate of diaphragmatic contraction, inhibit the diaphragmatic isotonic properties and power output and reduce the endurance time during repeated isotonic contractions (Machiels et al., 2001). Metabolically, chronic hypoxia reduces diaphragmatic oxygen consumption and ATP production and it may increase dependence on fatty acid oxidation. Activation of hypoxia-inducible factor (HIF), activation of atrophy signal transduction and increased proteolysis due to chronic hypoxia are the main causes of diaphragm dysfunction (Lewis and O'Halloran, 2016). Hif-1 α, the subunit comprising HIF-1, is a major regulator of the adaptive response of cells to hypoxia stress and its increased expression limits muscle regeneration (Semenza, 2010). In addition, studies have shown that chronic hypoxia activates TNF-α, induces the formation of ROS, and induces high expression of myostatin. These factors can exacerbate systemic inflammation, oxidative stress, and inhibition of myogenesis, respectively (Remels et al., 2007; Gayan-Ramirez and Decramer, 2013), thereby aggravating the damage to diaphragm function. Archiza and colleagues found that female diaphragms were more prone to fatigue under acute hypoxia, which may be related to gender differences in diaphragm metabolism, such as fibre type composition, systolic properties, substrate utilisation and blood perfusion (Archiza et al., 2021). A notable detail that chronic hypoxia could lead to diaphragm dysfunction in patients with COPD, which in turn leads to further hypoxia in a vicious cycle (Bradford, 2004).
Patients with COPD often suffer from malnutrition due to inadequate energy and nutrient intake, gastrointestinal digestive and absorption dysfunction, increased energy expenditure and enhanced catabolism (Holst et al., 2019; Kaluźniak-Szymanowska et al., 2021). According to statistics, 25%–40% of patients with COPD are malnourished (Cano et al., 2004; Vermeeren et al., 2006). Malnutrition causes COPD patients to gradually develop a negative nitrogen balance. The massive consumption of fat and protein causes muscle atrophy and reduced muscle mass. The structural and functional changes of diaphragm caused by malnutrition may evolve into diaphragm dysfunction. At the structural level, malnutrition could directly lead to increased muscle consumption (Xie et al., 2021). Malnutrition is associated with increased diaphragmatic diastolic ratio, decreased muscle weight, decreased fibre size, decreased percentage of type II fibre, and consumption of energy-rich compounds (Orozco-Levi, 2003). At the functional level, malnutrition causes an imbalance in the energy supply and demand of the diaphragm, along with damage to the respiratory system and the body’s defense system. Malnutrition may lead to a reduction in the mass of the diaphragm, which reduces the power to maintain normal ventilation and decreases muscle strength and endurance (Sahebjami and Sathianpitayakul, 2000). In general, malnutrition mainly affects the activity of glycolytic enzymes but it does not impair the function of oxidative pathways. A notable detail that although malnutrition may be associated with diaphragm dysfunction, it is also associated with the severity of malnutrition and its effect is clinically relevant only in some patients. Hamnegard studied diaphragm strength in two groups of 10 patients with severe COPD and found that the levels of malnutrition did not cause diaphragm weakness (Hamnegard et al., 2002), possibly because these changes are related to changes in diaphragm structure without affecting the overall changes in diaphragm function. Structural damage does not necessarily lead to loss of function.
The mechanisms of diaphragm dysfunction in patients with COPD are correlated. For example, oxidative stress could serve as a signal for the expression of inflammatory mediators and inflammation could regulate ROS production and thus oxidative stress levels (Thoma and Lightfoot, 2018). The increased load caused by hyperinflation could induce oxidative stress and aggravate diaphragm wear (Barreiro et al., 2005). Inflammatory factors have been shown to be involved in the development of malnutrition through the fusion of multiple mechanisms (Laviano et al., 2003). Hyperinflation plays an important role in chronic hypoxia and hypercapnia (Zysman et al., 2021). Such interactions may further complicate the condition of diaphragmatic dysfunction. But it also means that partial improvement in each factor has the potential to improve the overall situation. Well-organized rehabilitation has been proven to have a positive effect on diaphragmatic dysfunction in COPD by eliminating adverse triggers and improving functional performance of the diaphragm.
To date, the clinical attention paid to the prevention and treatment of diaphragm dysfunction in patients with COPD is not sufficient. Certain clinical interventions could even aggravate diaphragm dysfunction. For instance, long-term mechanical ventilation could further aggravate diaphragm dysfunction and even makes it difficult to get off the ventilator (Marchioni et al., 2019). IMT, exercise intervention and nutritional support are the main rehabilitation treatment that have been proven to be effective in improving diaphragm function. They are expected to improve diaphragm strength and endurance, enhance the exercise tolerance of patient and improve symptoms such as dyspnoea, overall, improve health-related quality of life (HRQL).
IMT applies a load to the diaphragm and accessory inspiratory muscles to increase their strength and endurance. It has been proven to improve inspiratory muscle strength, relieve dyspnoea, and improve exercise capacity in COPD patients (Beckerman et al., 2005; Hill et al., 2006; Magadle et al., 2007). The American Thoracic Society/European Respiratory Society (ATS/ERS) guidelines for pulmonary rehabilitation recommend IMT as an effective adjunct to pulmonary rehabilitation. Breathing techniques and neuromuscular electrical stimulation can reinforce and complement the effects of diaphragmatic training. Strengthening of the intercostal muscle synergistically improves diaphragm function and increases the functional reserve of the inspiratory muscles.
Diaphragm training is performed via devices that impose resistive or threshold loads, including inspiratory resistive training and threshold pressure training. Inspiratory resistive training is a method of continuous resistance breathing on the resistive load device at a normal breathing rate. The amount of inspiratory resistance during training depends on the amount of air the patient is breathing. Studies have shown that inspiratory resistive training could combat diaphragm fatigue, increase diaphragm strength and endurance and relieve dyspnoea (Madariaga et al., 2007). In threshold pressure training, the threshold inspiratory muscle trainer is used to set the given domain pressure and the patient’s respiratory work could only reach a certain threshold to open the channel in the trainer and make air flow. Studies have shown that threshold pressure training could enhance the muscle strength and endurance of the diaphragm to relieve dyspnoea and improve lung function (Sturdy et al., 2003; Lee et al., 2021). The threshold pressure training has better effect than inspiratory resistive training (Wu et al., 2017). Notably, recent studies have shown that long-term diaphragm training with high resistance load could lead to diaphragmatic injury, especially in patients with advanced COPD(Bertoni et al., 2019). During diaphragmatic training, patients are usually unable to maintain a high constant load training for a long time due to factors, such as anaerobic respiration, lactic acid accumulation and inadequate perfusion adjustment (Louvaris et al., 2021). In view of this situation, low load should be selected for diaphragm training, which could usually be set to 15–50% of the maximum suction negative pressure, to achieve a relatively safe and efficient improvement of diaphragm function.
Breathing techniques include diaphragmatic breathing and pursed-lips breathing, which can be utilised as compensatory therapy for patients who are unable to exercise (Mendes et al., 2019). Diaphragmatic breathing minimises the respiratory demand of the disease, improving breathing patterns and ventilation efficiency without causing respiratory dyspnoea (Fernandes et al., 2011).Diaphragmatic breathing enables the diaphragm to be fully exercised, thus increasing muscle strength and endurance. Pursed-lips breathing could prevent premature closure of small airways, improve gas exchange and relieve hypoxia symptoms of patients. Studies have shown that pursed-lips breathing could effectively reduce the minute ventilation and respiratory rate during exercise in patients with COPD (Mayer et al., 2018). Pursed-lips breathing can reduce dynamic hyperinflation (de Araujo et al., 2015), thereby reducing the diaphragm load. It could also improve patients’ exercise tolerance (Cabral et al., 2015). Studies have shown that diaphragmatic breathing combined with pursed-lips breathing could increase tidal volume, improve chest wall volume by shortening breathing cycle and relieve diaphragm fatigue by reducing breathing rate (Mendes et al., 2019). Due to the simplicity of implementation and the low incidence of serious adverse effects during training, breathing techniques are suitable for patients with COPD at all stages.
Neuromuscular electrical stimulation trains muscle strength by stimulating the diaphragm and related nerves with a controllable current (Vieira et al., 2014). Studies have shown that neuromuscular electrical stimulation could promote muscle protein synthesis, increase muscle mass and improve diaphragm muscle strength and fatigue resistance (Maddocks et al., 2016), especially for patients with moderate and severe COPD with limited exercise capacity. However, because it is passive training, neuromuscular electrical stimulation should be combined with active exercise to achieve enhanced rehabilitation effect as an alternative to routine rehabilitation exercise.
The contraction of intercostal muscles causes the ribs to move outward and upward, assisting the diaphragm in the coordination of inspiratory completion (Rohrbach et al., 2003). Training the intercostal muscles could increase their strength, endurance and mobility, thereby improving their ability to resist high-load exercise and reducing the load on the diaphragm. Intercostal muscle training mostly adopts exercise that promote upper body activities, such as chest expansion, rotation, swimming and various ball games (Zhou and Sun, 2021). Intercostal muscle training has high compliance requirements for patients and it is suitable for patients with mild to moderate COPD.
Exercise is the core content of pulmonary rehabilitation treatment of COPD. Personalised strength and endurance training plan is the cornerstone of pulmonary rehabilitation. It could effectively improve the diaphragm dysfunction of patients with COPD. Studies have shown that exercise could improve local muscle inflammation and even systemic inflammation in patients with COPD by significantly reducing the levels of inflammatory factors, such as TNF-α, in muscle and increasing the levels of anti-inflammatory factors, such as IL-10 (Toledo-Arruda et al., 2017). Exercise also improves oxidative stress in patients with COPD by increasing antioxidant capacity (Vieira Ramos et al., 2018), reducing the activity of oxidase and improving mitochondrial function (Zhang et al., 2021). Long-term exercise could correct chronic hypoxia by improving the oxygen utilisation efficiency of the body. Nutritional status could be improved by increasing appetite and regulating intestinal flora (Donati Zeppa et al., 2021). Thus, exercise could improve diaphragm dysfunction by reducing adverse factors that lead to negative changes in diaphragmatic structure and function as a whole. In addition to the positive effects of direct action on the diaphragm, exercise interventions can train the supporting muscles of the abdomen, back and limbs. These muscles play a better supporting and supportive role during respiration, reducing the fatigue of the diaphragm and thus improving its function.
The constituent elements of the exercise prescription of the training plan include the form, intensity, frequency, and duration of exercise. Aerobic and resistance exercise are the most common forms of exercise used in the rehabilitation of COPD patients. Aerobic exercise is a periodic and dynamic activity involving the major muscle groups of the whole body. It is the basis of the standard training of pulmonary rehabilitation. Lower-extremity endurance training, such as cycling or walking, is the most commonly used aerobic exercise. Studies have shown that aerobic exercise enhances diaphragm endurance and the muscle strength of major muscle groups and relieve diaphragm fatigue (Wada et al., 2016; Burtch et al., 2017). Resistance exercise refers to the active movement of muscles to overcome external resistance, usually with the help of dumbbells, elastic bands and other impedance training equipment (Hoff et al., 2007). Spruit and colleagues reported that resistance exercise significantly improves respiratory muscle strength, exercise capacity and HRQL in patients (Spruit et al., 2002). Panton et al. found that resistance exercise can be a useful supplement to aerobic exercise, effectively improving muscle weakness and atrophy (Panton et al., 2004). The addition of resistance exercise improved functional outcomes in COPD patients currently participating in an aerobic exercise programme (Skumlien et al., 2007). In addition to the positive effect of direct action on the diaphragm, exercise could train the auxiliary muscles in the abdomen, back and limbs for these muscles to play a better auxiliary and supporting role in the breathing process, relieve diaphragm fatigue, and improve diaphragm dysfunction.
With regard to exercise intensity, studies have shown that patients with stable COPD have better clinical outcomes with high-intensity training than with low-intensity training. Higher intensity exercise significantly improves respiratory muscle strength (Gimenez et al., 2000), reduces minute ventilation (Ve), and reduces dyspnoea (Vallet et al., 1997). High intensity here refers to the exercise close to the individual’s peak level, which is operationally defined as reaching at least 60%–85% of the peak working speed during the incremental maximum exercise test, rather than training at high absolute work levels. Similarly, low intensity refers to 20%–40% of the peak working speed during the incremental maximum exercise test (Norton et al., 2010). A single bout of strenuous exercise may increase the level of oxidative stress in the diaphragm in patients with COPD, leading to diaphragm fatigue (Itoh et al., 2004). In addition to being based on objective data, exercise intensity can be developed by the degree of respiratory distress perceived by the patient during exercise. The recommended intensity for resistance training consists of performing one to four sets of 40%–50% resistance of one repetition maximum (RM) for 10 to 15 repetitions ≥2 days per week (Garvey et al., 2016).
Regarding exercise frequency, it is recommended that aerobic exercise is 3–5 times a week and resistance exercise is at least 2 times a week (Spruit et al., 2013). In terms of duration, a 6–12 weeks training program is recommended (Bolton et al., 2013). Some studies have shown that longer-term programs may provide more lasting benefits (du Moulin et al., 2009; Beauchamp et al., 2013).
Noninvasive positive-pressure ventilation (NPPV) includes continuous positive airway pressure, pressure support and proportional assist ventilation (PAV). NPPV is particularly suitable for COPD patients with hypercapnia and mild to moderate respiratory failure (Lightowler et al., 2003; Köhnlein et al., 2014), and can be an important adjunct to exercise training in COPD patients. Hawkins et al. found that compared to spontaneous breathing, the use of PAV in conjunction with exercise training significantly improved exercise capacity and reduced exercise fatigue (Hawkins et al., 2002). Garrod and colleagues report that the use of NPPV as an adjunct to exercise training in COPD patients can help improve exercise tolerance and health status (Garrod et al., 2000). Non-invasive ventilation can reduce hyperinflation (Dennis et al., 2021).The main objective of NPPV in patients with severe COPD is to improve gas exchange and to provide adequate rest for the respiratory muscles after periods of fatigue (García et al., 2011). NPPV assists the diaphragm in respiratory movements, which helps to relieve the burden on the diaphragm, reduce respiratory work and promote the recovery of diaphragmatic dysfunction (Duiverman et al., 2016). However, as it is passive ventilation, the effect of training the diaphragm to contract on its own is lost to a certain extent. It is recommended as an adjunct to exercise training and is not recommended for long-term use.
As mentioned above, chronic malnutrition is an important factor in diaphragm dysfunction, and even respiratory failure. Studies have shown that appropriate nutritional support can significantly improve calorie and protein intake, enhance inspiratory muscle function, improve exercise capacity and alleviate dyspnoea symptoms (Weekes et al., 2009; Collins et al., 2013). Nutritional support can improve diaphragm dysfunction in patients with COPD by regulating inflammation, improving oxidative stress and regulating carbon dioxide production (Broekhuizen et al., 2005; Marín-Hinojosa et al., 2021).The main forms of nutritional support include dietary strategy and oral nutritional supplement (ONS).
The dietary strategy is to adjust the daily dietary structure of patients, and provide personalized food fortification, food snacks and dietary suggestions according to the age, illness and nutritional status of patients. Patients with COPD are often complicated with protein-energy malnutrition, so the diet should be supplied with sufficient calories (Akner and Cederholm, 2001). The respiratory quotient (RQ) of carbohydrates is high, which will produce more CO2 after oxidation in the body, causing or aggravating CO2 retention, aggravating dyspnoea and the burden of diaphragm, so the diet of COPD patients should reduce the energy supply ratio of carbohydrates (Anker et al., 2006). The carbohydrate intake of patients with stable COPD should account for 50%–60% of the total energy, while the carbohydrate intake of patients with acute exacerbation should account for 35%–50%, but the whole day carbohydrate should not be less than 150 g. The RQ of fat is very low. The proportion of fat intake can be appropriately increased. The fat supply of COPD patients in stable stage can account for 20%–30% of the total energy. Patients with COPD suffer from hyperproteinysis, which is also an important factor in diaphragm atrophy. Therefore, a high protein diet should be provided to promote anabolism. Protein supply can be calculated as 1.2–1.5 g/kg body weight per day, accounting for 15%–20% of total energy (Schols et al., 2014). Moreover, adequate vitamins, minerals, and trace elements should also be supplied in the diet.
In order to increase oral nutritional intake, nutritional liquid, semi-solid or powder preparations rich in a variety of macronutrients and micronutrients are added to drinks and foods for oral administration. ONS is often used to supplement intake when food is insufficient to meet the body’s needs. Similarly, ONS can be used as a sole source of nutrition. Sugawara‘s study found that low-intensity exercise therapy with nutritional supplements containing whey peptide can inhibit systemic inflammation, increase muscle strength and improve exercise tolerance in elderly patients with stable COPD (Sugawara et al., 2012). Studies have shown that nutritional supplements such as polyunsaturated fatty acids (PUFAs) and respifor have anti-inflammatory effects and can improve muscle strength and exercise capacity in patients with COPD (Steiner et al., 2003; Broekhuizen et al., 2005). Another study found that L-carnitine could improve exercise tolerance and inspiratory muscle strength in patients with COPD(Borghi-Silva et al., 2006). However, due to the differences in nutritional supplement regimen and effect measurement, more evidence is still needed on the effect of nutritional support therapy in improving diaphragm dysfunction in patients with COPD (Table 1).
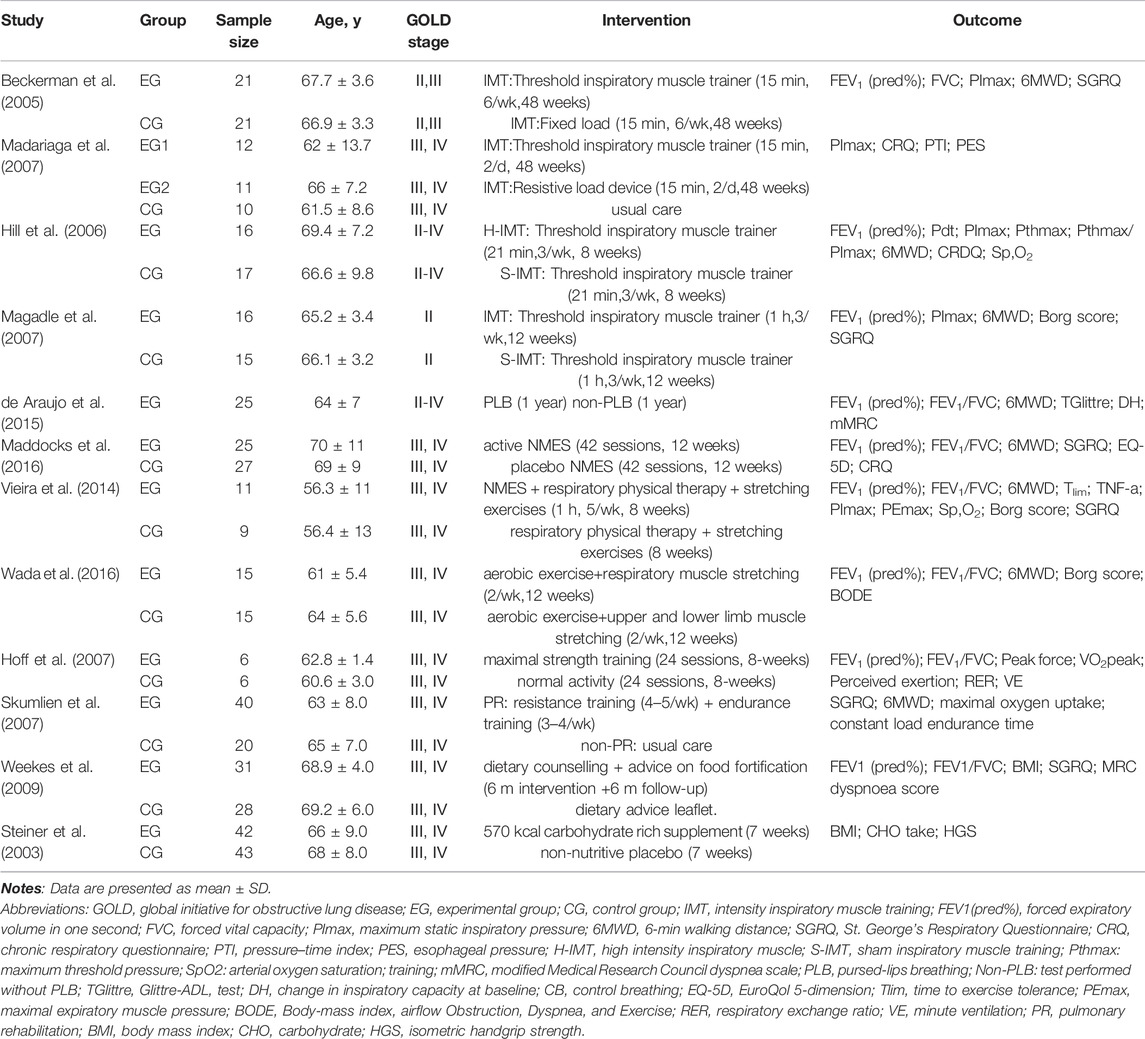
TABLE 1. Characteristics of included studies.
In summary, COPD combined with diaphragm dysfunction is a common phenomenon that directly affects patients’ respiratory status and quality of life and it is closely related to poor prognosis. In stable patients, diaphragmatic injury and adaptation achieved a special balance (Barreiro and Gea, 2015). However, these positive adaptations are not sufficient to restore normal muscle strength and endurance, resulting in increased susceptibility to fatigue and injury and leading to diaphragm dysfunction. No single factor could not fully explain its occurrence. The mechanism of diaphragmatic muscle dysfunction in patients with COPD is a pathway induced by various pathological factors and mechanisms involved in complex processes. Various factors induce protein breakdown, accelerate cell apoptosis, resulting in the loss of diaphragm muscle fibre, leading to diaphragm dysfunction. Rehabilitation methods, such as IMT, exercise intervention and nutritional support can eliminate the risk factors of diaphragm dysfunction to a certain extent, exercise the diaphragm and respiratory auxiliary muscle group locally and as a whole, improve the overall condition, and have a clear rehabilitation effect on COPD patients with diaphragm dysfunction, which can be used as a reference for clinical treatment of COPD patients with diaphragm dysfunction.
In the future, diaphragm dysfunction in patients with mild to moderate COPD should be the focus of research. In terms of the structure and function of diaphragm dysfunction, studies to determine the causal relationship between the presence and severity of COPD and changes in diaphragm structure and function are still lacking. On the one hand, the specific mechanism of inflammatory response, oxidative stress, chronic hypoxia and other factors playing a role in diaphragm dysfunction has not been fully clarified and each theory is not sufficient to fully explain the mechanism of diaphragm dysfunction. On the other hand, most of the current research is animal experimental research and clinical research and dynamic observation are lacking. In the study of rehabilitation treatment of diaphragm dysfunction, the rehabilitation treatment methods have not been unified and a complete and systematic pulmonary rehabilitation training prescription has not been formed. Large-scale clinical trials could be carried out in the future to explore the most suitable individualised rehabilitation programme for patients from clinical practice and to form standardised and unified operation and evaluation standards. A longitudinal dynamic follow-up study could be conducted to explore the correlation between the severity of diaphragm dysfunction and different stages of disease to provide a prospective basis for the early discovery of diaphragm dysfunction.
WW, XL, and YC contributed to the design of this review. YC, PL, and YW conducted the literature search selection and completed data extraction. YC completed data analysis and wrote the initial draft of the manuscript. PL and YW contributed important intellectual content and put forward suggestions for revision. YC and PL revised the article. WW, XL, and PL supervised the quality of articles. All authors have read and approved the submitted version.
This review was supported by the National Natural Science Foundation of China (No 82072551, 81902307).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ábrigo J., Elorza A. A., Riedel C. A., Vilos C., Simon F., Cabrera D., et al. (2018). Role of Oxidative Stress as Key Regulator of Muscle Wasting during Cachexia. Oxid. Med. Cell Longev. 2018, 1–17. doi:10.1155/2018/2063179
Akner G., Cederholm T. (2001). Treatment of Protein-Energy Malnutrition in Chronic Nonmalignant Disorders. Am. J. Clin. Nutr. 74, 6–24. doi:10.1093/ajcn/74.1.6
Anker S. D., John M., Pedersen P. U., Raguso C., Cicoira M., Dardai E., et al. (2006). ESPEN Guidelines on Enteral Nutrition: Cardiology and Pulmonology. Clin. Nutr. 25, 311–318. doi:10.1016/j.clnu.2006.01.017
Archiza B., Reinhard P. A., Welch J. F., Sheel A. W. (2021). Sex Differences in Diaphragmatic Fatigue: Effects of Hypoxia during Inspiratory Loading. J. Physiol. 599, 1319–1333. doi:10.1113/JP280704
Attaix D., Ventadour S., Codran A., Béchet D., Taillandier D., Combaret L. (2005). The Ubiquitin-Proteasome System and Skeletal Muscle Wasting. Essays Biochem. 41, 173–186. doi:10.1042/bse0410173
Barreiro E., Gea J. (2015). Respiratory and Limb Muscle Dysfunction in COPD. COPD J. Chronic Obstructive Pulm. Dis. 12, 413–426. doi:10.3109/15412555.2014.974737
Barreiro E., de la Puente B., Minguella J., Corominas J. M., Serrano S., Hussain S. N. A., et al. (2005). Oxidative Stress and Respiratory Muscle Dysfunction in Severe Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 171, 1116–1124. doi:10.1164/rccm.200407-887OC
Barreiro E., Peinado V. I., Galdiz J. B., Ferrer E., Marin-Corral J., Sánchez F., et al. (2010). Cigarette Smoke-Induced Oxidative Stress: A Role in Chronic Obstructive Pulmonary Disease Skeletal Muscle Dysfunction. Am. J. Respir. Crit. Care Med. 182, 477–488. doi:10.1164/rccm.200908-1220OC
Barreiro E., Ferrer D., Sanchez F., Minguella J., Marin-Corral J., Martinez-Llorens J., et al. (2011). Inflammatory Cells and Apoptosis in Respiratory and Limb Muscles of Patients with COPD. J. Appl. Physiol. 111, 808–817. doi:10.1152/japplphysiol.01017.2010
Beauchamp M. K., Evans R., Janaudis-Ferreira T., Goldstein R. S., Brooks D. (2013). Systematic Review of Supervised Exercise Programs after Pulmonary Rehabilitation in Individuals with COPD. Chest 144, 1124–1133. doi:10.1378/chest.12-2421
Beckerman M., Magadle R., Weiner M., Weiner P. (2005). The Effects of 1 Year of Specific Inspiratory Muscle Training in Patients with COPD. Chest 128, 3177–3182. doi:10.1378/chest.128.5.3177
Bertoni M., Telias I., Urner M., Long M., Del Sorbo L., Fan E., et al. (2019). A Novel Non-invasive Method to Detect Excessively High Respiratory Effort and Dynamic Transpulmonary Driving Pressure during Mechanical Ventilation. Crit. Care 23, 346. doi:10.1186/s13054-019-2617-0
Bolton C. E., Bevan-Smith E. F., Blakey J. D., Crowe P., Elkin S. L., Garrod R., et al. (2013). British Thoracic Society Guideline on Pulmonary Rehabilitation in Adults: Accredited by NICE. Thorax 68 (Suppl. 2), ii1–ii30. doi:10.1136/thoraxjnl-2013-203808
Borghi-Silva A., Baldissera V., Sampaio L. M. M., Pires-DiLorenzo V. A., Jamami M., Demonte A., et al. (2006). L-carnitine as an Ergogenic Aid for Patients with Chronic Obstructive Pulmonary Disease Submitted to Whole-Body and Respiratory Muscle Training Programs. Braz. J. Med. Biol. Res. 39, 465–474. doi:10.1590/s0100-879x2006000400006
Bradford A. (2004). Effects of Chronic Intermittent Asphyxia on Haematocrit, Pulmonary Arterial Pressure and Skeletal Muscle Structure in Rats. Exp. Physiol. 89, 44–52. doi:10.1113/expphysiol.2003.002656
Broekhuizen R., Wouters E. F., Creutzberg E. C., Weling-Scheepers C. A., Schols A. M. (2005). Polyunsaturated Fatty Acids Improve Exercise Capacity in Chronic Obstructive Pulmonary Disease. Thorax 60, 376–382. doi:10.1136/thx.2004.030858
Burtch A. R., Ogle B. T., Sims P. A., Harms C. A., Symons T. B., Folz R. J., et al. (2017). Controlled Frequency Breathing Reduces Inspiratory Muscle Fatigue. J. Strength Cond Res. 31, 1273–1281. doi:10.1519/JSC.0000000000001589
Cabral L. F., D'Elia T. C., Marins D. S., Zin W. A., Guimarães F. S. (2015). Pursed Lip Breathing Improves Exercise Tolerance in COPD: A Randomized Crossover Study. Eur. J. Phys. Rehabil. Med. 51, 79–88.
Cano N. J. M., Pichard C., Roth H., Court-Fortuné I., Cynober L., Gérard-Boncompain M., et al. (2004). C-reactive Protein and Body Mass index Predict Outcome in End-Stage Respiratory Failure. Chest 126, 540–546. doi:10.1378/chest.126.2.540
Ceriana P., Vitacca M., Carlucci A., Paneroni M., Pisani L., Nava S. (2017). Changes of Respiratory Mechanics in COPD Patients from Stable State to Acute Exacerbations with Respiratory Failure. COPD: J. Chronic Obstruct. Pulm. Dis. 14, 150–155. doi:10.1080/15412555.2016.1254173
Collins P. F., Elia M., Stratton R. J. (2013). Nutritional Support and Functional Capacity in Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Respirology 18, 616–629. doi:10.1111/resp.12070
de Araujo C., Karloh M., Reis C., PalÃ˚ M., Mayer A. (2015). Pursed-lips Breathing Reduces Dynamic Hyperinflation Induced by Activities of Daily Living Test in Patients with Chronic Obstructive Pulmonary Disease: A Randomized Cross-Over Study. J. Rehabil. Med. 47, 957–962. doi:10.2340/16501977-2008
Dennis C. J., Menadue C., Schneeberger T., Leitl D., Schoenheit-Kenn U., Hoyos C. M., et al. (2021). Bilevel Noninvasive Ventilation during Exercise Reduces Dynamic Hyperinflation and Improves Cycle Endurance Time in Severe to Very Severe COPD. Chest 160, 2066–2079. doi:10.1016/j.chest.2021.06.050
Donati Zeppa S., Amatori S., Sisti D., Gervasi M., Agostini D., Piccoli G., et al. (2021). Nine Weeks of High-Intensity Indoor Cycling Training Induced Changes in the Microbiota Composition in Non-athlete Healthy Male College Students. J. Int. Soc. Sports Nutr. 18, 74. doi:10.1186/s12970-021-00471-z
Dos Santos Yamaguti W. P., Paulin E., Shibao S., Chammas M. C., Salge J. M., Ribeiro M., et al. (2008). Air Trapping: The Major Factor Limiting Diaphragm Mobility in Chronic Obstructive Pulmonary Disease Patients. Respirology 13, 138–144. doi:10.1111/j.1440-1843.2007.01194.x
Du J., Wang X., Miereles C., Bailey J. L., Debigare R., Zheng B., et al. (2004). Activation of Caspase-3 Is an Initial Step Triggering Accelerated Muscle Proteolysis in Catabolic Conditions. J. Clin. Invest. 113, 115–123. doi:10.1172/JCI18330
du Moulin M., Taube K., Wegscheider K., Behnke M., van den Bussche H. (2009). Home-Based Exercise Training as Maintenance after Outpatient Pulmonary Rehabilitation. Respiration 77, 139–145. doi:10.1159/000150315
Duiverman M. L., Arellano-Maric M. P., Windisch W. (2016). Long-Term Noninvasive Ventilation in Patients with Chronic Hypercapnic Respiratory Failure. Curr. Opin. Pulm. Med. 22, 130–137. doi:10.1097/MCP.0000000000000239
Elsawy S. B. (2017). Impact of Chronic Obstructive Pulmonary Disease Severity on Diaphragm Muscle Thickness. Egypt. J. Chest Dis. Tuberc. 66, 587–592. doi:10.1016/j.ejcdt.2017.08.002
Fernandes M., Cukier A., Feltrim M. I. Z. (2011). Efficacy of Diaphragmatic Breathing in Patients with Chronic Obstructive Pulmonary Disease. Chron. Respir. Dis. 8, 237–244. doi:10.1177/1479972311424296
Finucane K. E., Panizza J. A., Singh B. (2005). Efficiency of the normal Human Diaphragm with Hyperinflation. J. Appl. Physiol. 99, 1402–1411. doi:10.1152/japplphysiol.01165.2004
Gamboa J. L., Andrade F. H. (2010). Mitochondrial Content and Distribution Changes Specific to Mouse Diaphragm after Chronic Normobaric Hypoxia. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 298, R575–R583. doi:10.1152/ajpregu.00320.2009
Gamboa J. L., Andrade F. H. (2012). Muscle Endurance and Mitochondrial Function after Chronic Normobaric Hypoxia: Contrast of Respiratory and Limb Muscles. Pflugers Arch. - Eur. J. Physiol. 463, 327–338. doi:10.1007/s00424-011-1057-8
García V. E., Sandoval A. J., Díaz C. L., Salgado C. J. (2011). Invasive Mechanical Ventilation in COPD and Asthma. Med. Intensiva 35, 288–298. doi:10.1016/j.medin.2010.11.004
Garrod R., Mikelsons C., Paul E. A., Wedzicha J. A. (2000). Randomized Controlled Trial of Domiciliary Noninvasive Positive Pressure Ventilation and Physical Training in Severe Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 162, 1335–1341. doi:10.1164/ajrccm.162.4.9912029
Garvey C., Bayles M. P., Hamm L. F., Hill K., Holland A., Limberg T. M., et al. (2016). Pulmonary Rehabilitation Exercise Prescription in Chronic Obstructive Pulmonary Disease: Review of Selected Guidelines: An OFFICIAL STATEMENT FROM the AMERICAN ASSOCIATION of CARDIOVASCULAR and PULMONARY REHABILITATION. J. Cardiopulm. Rehabil. Prev. 36, 75–83. doi:10.1097/HCR.0000000000000171
Gayan-Ramirez G., Decramer M. (2013). Mechanisms of Striated Muscle Dysfunction during Acute Exacerbations of COPD. J. Appl. Physiol. 114, 1291–1299. doi:10.1152/japplphysiol.00847.2012
Gea J., Agustí A., Roca J. (2013). Pathophysiology of Muscle Dysfunction in COPD. J. Appl. Physiol. 114, 1222–1234. doi:10.1152/japplphysiol.00981.2012
Geiger P. C., Cody M. J., Macken R. L., Sieck G. C. (2000). Maximum Specific Force Depends on Myosin Heavy Chain Content in Rat Diaphragm Muscle Fibers. J. Appl. Physiol. 89, 695–703. doi:10.1152/jappl.2000.89.2.695
Gimenez M., Servera E., Vergara P., Bach J. R., Polu J.-M. (2000). Endurance Training in Patients with Chronic Obstructive Pulmonary Disease: A Comparison of High versus Moderate Intensity. Arch. Phys. Med. Rehabil. 81, 102–109. doi:10.1053/apmr.2000.0810102
Gomes-Marcondes M. C. C., Tisdale M. J. (2002). Induction of Protein Catabolism and the Ubiquitin-Proteasome Pathway by Mild Oxidative Stress. Cancer Lett. 180, 69–74. doi:10.1016/s0304-3835(02)00006-x
Gonçalves M. A., Leal B. E., Lisboa L. G., Tavares M. G. d. S., Yamaguti W. P., Paulin E. (2018). Comparison of Diaphragmatic Mobility between COPD Patients with and without Thoracic Hyperkyphosis: A Cross-Sectional Study. J. Bras. Pneumol. 44, 5–11. doi:10.1590/S1806-37562016000000248
Gosselink R., De Vos J., van den Heuvel S. P., Segers J., Decramer M., Kwakkel G. (2011). Impact of Inspiratory Muscle Training in Patients with COPD: What Is the Evidence? Eur. Respir. J. 37, 416–425. doi:10.1183/09031936.00031810
Haegens A., Schols A. M., Gorissen S. H., van Essen A. L., Snepvangers F., Gray D. A., et al. (2012). NF-κB Activation and Polyubiquitin Conjugation Are Required for Pulmonary Inflammation-Induced Diaphragm Atrophy. Am. J. Physiol.-Lung Cell Mol. Physiol. 302, L103–L110. doi:10.1152/ajplung.00084.2011
Hamnegård C.-H., Bake B., Moxham J., Polkey M. I. (2002). Does Undernutrition Contribute to Diaphragm Weakness in Patients with Severe COPD? Clin. Nutr. 21, 239–243. doi:10.1054/clnu.2002.0538
Hart N., Nickol A. H., Cramer D., Ward S. P., Lofaso F., Pride N. B., et al. (2002). Effect of Severe Isolated Unilateral and Bilateral Diaphragm Weakness on Exercise Performance. Am. J. Respir. Crit. Care Med. 165, 1265–1270. doi:10.1164/rccm.2110016
Hawkins P., Johnson L. C., Nikoletou D., Hamnegård C. H., Sherwood R., Polkey M. I., et al. (2002). Proportional Assist Ventilation as an Aid to Exercise Training in Severe Chronic Obstructive Pulmonary Disease. Thorax 57, 853–859. doi:10.1136/thorax.57.10.853
Hellebrandová L., Chlumský J., Vostatek P., Novák D., Rýznarová Z., Bunc V. (2016). Airflow Limitation Is Accompanied by Diaphragm Dysfunction. Physiol. Res. 65, 469–479. doi:10.33549/physiolres.933064
Hill K., Jenkins S. C., Philippe D. L., Cecins N., Shepherd K. L., Green D. J., et al. (2006). High-intensity Inspiratory Muscle Training in COPD. Eur. Respir. J. 27, 1119–1128. doi:10.1183/09031936.06.00105205
Hoff J., Tjønna A. E., Steinshamn S., Høydal M., Richardson R. S. (2007). Maximal Strength Training of the Legs in COPD: A Therapy for Mechanical Inefficiency. Med. Sci. Sports Exerc. 39, 220–226. doi:10.1249/01.mss.0000246989.48729.39
Holst M., Beck A. M., Rasmussen H. H., Lange P. (2019). Insufficient Intake of Energy and Protein Is Related to Physical Functional Capacity Among COPD Patients Referred to Municipality Based Pulmonary Rehabilitation. Clin. Nutr. ESPEN 30, 35–41. doi:10.1016/j.clnesp.2019.02.009
Huang A.-X., Lu L.-W., Liu W.-J., Huang M. (2016). Plasma Inflammatory Cytokine IL-4, IL-8, IL-10, and TNF-α Levels Correlate with Pulmonary Function in Patients with Asthma-Chronic Obstructive Pulmonary Disease (COPD) Overlap Syndrome. Med. Sci. Monit. 22, 2800–2808. doi:10.12659/msm.896458
Itoh M., Oh-Ishi S., Hatao H., Leeuwenburgh C., Selman C., Ohno H., et al. (2004). Effects of Dietary Calcium Restriction and Acute Exercise on the Antioxidant Enzyme System and Oxidative Stress in Rat Diaphragm. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 287, R33–R38. doi:10.1152/ajpregu.00598.2003
Ji L. L., Gomez-Cabrera M. C., Vina J. (2006). Exercise and Hormesis: Activation of Cellular Antioxidant Signaling Pathway. Ann. N.Y Acad. Sci. 1067, 425–435. doi:10.1196/annals.1354.061
Kaluźniak-Szymanowska A., Krzymińska-Siemaszko R., Deskur-Śmielecka E., Lewandowicz M., Kaczmarek B., Wieczorowska-Tobis K. (2021). Malnutrition, Sarcopenia, and Malnutrition-Sarcopenia Syndrome in Older Adults with COPD. Nutrients 14, 44. doi:10.3390/nu14010044
Köhnlein T., Windisch W., Köhler D., Drabik A., Geiseler J., Hartl S., et al. (2014). Non-invasive Positive Pressure Ventilation for the Treatment of Severe Stable Chronic Obstructive Pulmonary Disease: A Prospective, Multicentre, Randomised, Controlled Clinical Trial. Lancet Respir. Med. 2, 698–705. doi:10.1016/S2213-2600(14)70153-5
Krieger B. P. (2009). Hyperinflation and Intrinsic Positive End-Expiratory Pressure: Less Room to Breathe. Respiration 77, 344–350. doi:10.1159/000192790
Kuwano K., Hara N. (2000). Signal Transduction Pathways of Apoptosis and Inflammation Induced by the Tumor Necrosis Factor Receptor Family. Am. J. Respir. Cel Mol Biol. 22, 147–149. doi:10.1165/ajrcmb.22.2.f178
Laghi F. A., Saad M., Shaikh H. (2021). Ultrasound and Non-ultrasound Imaging Techniques in the Assessment of Diaphragmatic Dysfunction. BMC Pulm. Med. 21, 85. doi:10.1186/s12890-021-01441-6
Laviano A., Meguid M. M., Rossi-Fanelli F. (2003). Cancer Anorexia: Clinical Implications, Pathogenesis, and Therapeutic Strategies. Lancet Oncol. 4, 686–694. doi:10.1016/s1470-2045(03)01247-6
Lee C.-T., Chien J.-Y., Hsu M.-J., Wu H.-D., Wang L.-Y. (2021). Inspiratory Muscle Activation during Inspiratory Muscle Training in Patients with COPD. Respir. Med. 190, 106676. doi:10.1016/j.rmed.2021.106676
Levine S., Gregory C., Nguyen T., Shrager J., Kaiser L., Rubinstein N., et al. (2002). Bioenergetic Adaptation of Individual Human Diaphragmatic Myofibers to Severe COPD. J. Appl. Physiol. 92, 1205–1213. doi:10.1152/japplphysiol.00116.2001
Levine S., Nguyen T., Kaiser L. R., Rubinstein N. A., Maislin G., Gregory C., et al. (2003). Human Diaphragm Remodeling Associated with Chronic Obstructive Pulmonary Disease: Clinical Implications. Am. J. Respir. Crit. Care Med. 168, 706–713. doi:10.1164/rccm.200209-1070OC
Levine S., Bashir M. H., Clanton T. L., Powers S. K., Singhal S. (2013). COPD Elicits Remodeling of the Diaphragm and Vastus Lateralis Muscles in Humans. J. Appl. Physiol. 114, 1235–1245. doi:10.1152/japplphysiol.01121.2012
Lewis P., O'Halloran K. D. (2016). Diaphragm Muscle Adaptation to Sustained Hypoxia: Lessons from Animal Models with Relevance to High Altitude and Chronic Respiratory Diseases. Front. Physiol. 7, 623. doi:10.3389/fphys.2016.00623
Lightowler J. V., Wedzicha J. A., Elliott M. W., Ram F. S. (2003). Non-invasive Positive Pressure Ventilation to Treat Respiratory Failure Resulting from Exacerbations of Chronic Obstructive Pulmonary Disease: Cochrane Systematic Review and Meta-Analysis. Bmj 326, 185. doi:10.1136/bmj.326.7382.185
Lin H., Sun S. H., Gao J., Liu C., Zhan J. (2010). The Influence of Indomethacin on TNFα and Skeletal Muscle Protein Catabolism in Chronic Obstructive Pulmonary Disease Rat Model. Zhonghua Nei Ke Za Zhi 49, 776–780.
Louvaris Z., Rodrigues A., Dacha S., Gojevic T., Janssens W., Vogiatzis I., et al. (2021). High-intensity Exercise Impairs Extradiaphragmatic Respiratory Muscle Perfusion in Patients with COPD. J. Appl. Physiol. 130, 325–341. doi:10.1152/japplphysiol.00659.2020
Macgowan N. A., Evans K. G., Road J. D., Reid W. D. (2001). Diaphragm Injury in Individuals with Airflow Obstruction. Am. J. Respir. Crit. Care Med. 163, 1654–1659. doi:10.1164/ajrccm.163.7.2001042
Machiels H. A., van der Heijden H. F. M., Heunks L. M. A., Dekhuijzen P. N. R. (2001). The Effect of Hypoxia on Shortening Contractions in Rat Diaphragm Muscle. Acta Physiol. Scand. 173, 313–321. doi:10.1046/j.1365-201X.2001.00895.x10.1046/j.1365-201x.2001.00895.x
Madariaga V. B., Iturri J. B. G., Manterola A. G., Buey J. C., Sebastián N. T., Peña V. S. (2007). Comparison of 2 Methods for Inspiratory Muscle Training in Patients with Chronic Obstructive Pulmonary Disease. Archivos de Bronconeumol. ((Eng. Ed.)) 43, 431–438. doi:10.1016/s1579-2129(07)60099-8
Maddocks M., Nolan C. M., Man W. D.-C., Polkey M. I., Hart N., Gao W., et al. (2016). Neuromuscular Electrical Stimulation to Improve Exercise Capacity in Patients with Severe COPD: A Randomised Double-Blind, Placebo-Controlled Trial. Lancet Respir. Med. 4, 27–36. doi:10.1016/S2213-2600(15)00503-2
Mador M. J., Sethi S. (2013). Systemic Inflammation in Predicting COPD Exacerbations. Jama 309, 2390–2391. doi:10.1001/jama.2013.5733
Magadle R., McConnell A. K., Beckerman M., Weiner P. (2007). Inspiratory Muscle Training in Pulmonary Rehabilitation Program in COPD Patients. Respir. Med. 101, 1500–1505. doi:10.1016/j.rmed.2007.01.010
Man W., Donaldson M., Maddocks D., Martolini M. I., Polkey M. (2012). Muscle Function in COPD: A Complex Interplay. Copd 7, 523–535. doi:10.2147/COPD.S28247
Marchioni A., Tonelli R., Fantini R., Tabbì L., Castaniere I., Livrieri F., et al. (2019). Respiratory Mechanics and Diaphragmatic Dysfunction in COPD Patients Who Failed Non-invasive Mechanical Ventilation. Copd 14, 2575–2585. doi:10.2147/COPD.S219125
Marín-Hinojosa C., Eraso C. C., Sanchez-Lopez V., Hernández L. C., Otero-Candelera R., Lopez-Campos J. L. (2021). Nutriepigenomics and Chronic Obstructive Pulmonary Disease: Potential Role of Dietary and Epigenetics Factors in Disease Development and Management. Am. J. Clin. Nutr. 114, 1894–1906. doi:10.1093/ajcn/nqab267
Mathur S., Brooks D., Carvalho C. R. F. (2014). Structural Alterations of Skeletal Muscle in Copd. Front. Physiol. 5, 104. doi:10.3389/fphys.2014.00104
Mayer A. F., Karloh M., dos Santos K., de Araujo C. L. P., Gulart A. A. (2018). Effects of Acute Use of Pursed-Lips Breathing during Exercise in Patients with COPD: A Systematic Review and Meta-Analysis. Physiotherapy 104, 9–17. doi:10.1016/j.physio.2017.08.007
McCool F. D., Tzelepis G. E. (2012). Dysfunction of the Diaphragm. N. Engl. J. Med. 366, 932–942. doi:10.1056/NEJMra1007236
McKenzie D. K., Butler J. E., Gandevia S. C. (2009). Respiratory Muscle Function and Activation in Chronic Obstructive Pulmonary Disease. J. Appl. Physiol. 107, 621–629. doi:10.1152/japplphysiol.00163.2009
McMorrow C., Fredsted A., Carberry J., O'Connell R. A., Bradford A., Jones J. F. X., et al. (2011). Chronic Hypoxia Increases Rat Diaphragm Muscle Endurance and Sodium-Potassium ATPase Pump Content. Eur. Respir. J. 37, 1474–1481. doi:10.1183/09031936.00079810
Mendes L. P., Moraes K. S., Hoffman M., Vieira D. S., Ribeiro-Samora G. A., Lage S. M., et al. (2019). Effects of Diaphragmatic Breathing with and without Pursed-Lips Breathing in Subjects with COPD. Respir. Care 64, 136–144. doi:10.4187/respcare.06319
Moore A. J., Stubbings A., Swallow E. B., Dusmet M., Goldstraw P., Porcher R., et al. (2006). Passive Properties of the Diaphragm in COPD. J. Appl. Physiol. 101, 1400–1405. doi:10.1152/japplphysiol.01614.2005
Mourkioti F., Kratsios P., Luedde T., Song Y.-H., Delafontaine P., Adami R., et al. (2006). Targeted Ablation of IKK2 Improves Skeletal Muscle Strength, Maintains Mass, and Promotes Regeneration. J. Clin. Invest. 116, 2945–2954. doi:10.1172/JCI28721
Nair A., Alaparthi G. K., Krishnan S., Rai S., Anand R., Acharya V., et al. (2019). Comparison of Diaphragmatic Stretch Technique and Manual Diaphragm Release Technique on Diaphragmatic Excursion in Chronic Obstructive Pulmonary Disease: A Randomized Crossover Trial. Pulm. Med. 2019, 1–7. doi:10.1155/2019/6364376
Nguyen T., Shrager J., Kaiser L., Mei L., Daood M., Watchko J., et al. (2000). Developmental Myosin Heavy Chains in the Adult Human Diaphragm: Coexpression Patterns and Effect of COPD. J. Appl. Physiol. 88, 1446–1456. doi:10.1152/jappl.2000.88.4.1446
Norton K., Norton L., Sadgrove D. (2010). Position Statement on Physical Activity and Exercise Intensity Terminology. J. Sci. Med. Sport 13, 496–502. doi:10.1016/j.jsams.2009.09.008
Orozco-Levi M., Gea J., Lloreta J. L., Félez M., Minguella J., Serrano S., et al. (1999). Subcellular Adaptation of the Human Diaphragm in Chronic Obstructive Pulmonary Disease. Eur. Respir. J. 13, 371–378. doi:10.1183/09031936.99.13237199
Orozco-Levi M., Lloreta J., Minguella J., Serrano S., Broquetas J. M., Gea J. (2001). Injury of the Human Diaphragm Associated with Exertion and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 164, 1734–1739. doi:10.1164/ajrccm.164.9.2011150
Orozco-Levi M. (2003). Structure and Function of the Respiratory Muscles in Patients with COPD: Impairment or Adaptation? Eur. Respir. J. 22, 41s–51s. doi:10.1183/09031936.03.00004607
Ottenheijm C. A. C., Heunks L. M. A., Sieck G. C., Zhan W.-Z., Jansen S. M., Degens H., et al. (2005). Diaphragm Dysfunction in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 172, 200–205. doi:10.1164/rccm.200502-262OC
Panton L. B., Golden J., Broeder C. E., Browder K. D., Cestaro-Seifer D. J., Seifer F. D. (2004). The Effects of Resistance Training on Functional Outcomes in Patients with Chronic Obstructive Pulmonary Disease. Eur. J. Appl. Physiol. 91, 443–449. doi:10.1007/s00421-003-1008-y
Papavramidis T. S., Kotidis E., Ioannidis K., Cheva A., Lazou T., Koliakos G., et al. (2011). Diaphragmatic Adaptation Following Intra-abdominal Weight Charging. Obes. Surg. 21, 1612–1616. doi:10.1007/s11695-010-0334-5
Paulin E., Yamaguti W. P. S., Chammas M. C., Shibao S., Stelmach R., Cukier A., et al. (2007). Influence of Diaphragmatic Mobility on Exercise Tolerance and Dyspnea in Patients with COPD. Respir. Med. 101, 2113–2118. doi:10.1016/j.rmed.2007.05.024
Pomiès P., Blaquière M., Maury J., Mercier J., Gouzi F., Hayot M. (2016). Involvement of the FoxO1/MuRF1/Atrogin-1 Signaling Pathway in the Oxidative Stress-Induced Atrophy of Cultured Chronic Obstructive Pulmonary Disease Myotubes. PLoS One 11, e0160092. doi:10.1371/journal.pone.0160092
Powers S. K., Jackson M. J. (2008). Exercise-induced Oxidative Stress: Cellular Mechanisms and Impact on Muscle Force Production. Physiol. Rev. 88, 1243–1276. doi:10.1152/physrev.00031.2007
Remels A. H., Gosker H. R., van der Velden J., Langen R. C., Schols A. M. (2007). Systemic Inflammation and Skeletal Muscle Dysfunction in Chronic Obstructive Pulmonary Disease: State of the Art and Novel Insights in Regulation of Muscle Plasticity. Clin. Chest Med. 28, 537–552. doi:10.1016/j.ccm.2007.06.003
Rocha F. R., Brüggemann A. K. V., Francisco D. d. S., Medeiros C. S. d., Rosal D., Paulin E. (2017). Diaphragmatic Mobility: Relationship with Lung Function, Respiratory Muscle Strength, Dyspnea, and Physical Activity in Daily Life in Patients with COPD. J. Bras. Pneumol. 43, 32–37. doi:10.1590/S1806-37562016000000097
Rochester D. F., Braun N. M. (1985). Determinants of Maximal Inspiratory Pressure in Chronic Obstructive Pulmonary Disease. Am. Rev. Respir. Dis. 132, 42–47. doi:10.1164/arrd.1985.132.1.42
Rohrbach M., Perret C., Kayser B., Boutellier U., Spengler C. M. (2003). Task Failure from Inspiratory Resistive Loaded Breathing: A Role for Inspiratory Muscle Fatigue? Eur. J. Appl. Physiol. 90, 405–410. doi:10.1007/s00421-003-0871-x
Sahebjami H., Sathianpitayakul E. (2000). Influence of Body Weight on the Severity of Dyspnea in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 161, 886–890. doi:10.1164/ajrccm.161.3.9905023
Salito C., Luoni E., Aliverti A. (2015). Alterations of Diaphragm and Rib Cage Morphometry in Severe COPD Patients by CT Analysis. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2015, 6390–6393. doi:10.1109/EMBC.2015.7319855
Schols A. M., Ferreira I. M., Franssen F. M., Gosker H. R., Janssens W., Muscaritoli M., et al. (2014). Nutritional Assessment and Therapy in COPD: A European Respiratory Society Statement. Eur. Respir. J. 44, 1504–1520. doi:10.1183/09031936.00070914
Scott A., Wang X., Road J. D., Reid W. D. (2006). Increased Injury and Intramuscular Collagen of the Diaphragm in COPD: Autopsy Observations. Eur. Respir. J. 27, 51–59. doi:10.1183/09031936.06.00143004
Shiota S., Okada T., Naitoh H., Ochi R., Fukuchi Y. (2004). Hypoxia and Hypercapnia Affect Contractile and Histological Properties of Rat Diaphragm and Hind Limb Muscles. Pathophysiology 11, 23–30. doi:10.1016/j.pathophys.2003.09.003
Shiraishi M., Higashimoto Y., Sugiya R., Mizusawa H., Takeda Y., Fujita S., et al. (2021). Diaphragmatic Excursion Is Correlated with the Improvement in Exercise Tolerance after Pulmonary Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease. Respir. Res. 22, 271. doi:10.1186/s12931-021-01870-1
Shirakawa T., Rojasawasthien T., Inoue A., Matsubara T., Kawamoto T., Kokabu S. (2021). Tumor Necrosis Factor Alpha Regulates Myogenesis to Inhibit Differentiation and Promote Proliferation in Satellite Cells. Biochem. Biophys. Res. Commun. 580, 35–40. doi:10.1016/j.bbrc.2021.09.067
Silva I. S., Fregonezi G. A., Dias F. A., Ribeiro C. T., Guerra R. O., Ferreira G. M. (2013). Inspiratory Muscle Training for Asthma. Cochrane Database Syst. Rev. 2013, D3792. doi:10.1002/14651858.CD003792.pub2
Singh D., Agusti A., Anzueto A., Barnes P. J., Bourbeau J., Celli B. R., et al. (2019). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: The GOLD Science Committee Report 2019. Eur. Respir. J. 53, 1900164. doi:10.1183/13993003.00164-2019
Skumlien S., Skogedal E. A., Bjørtuft O., Ryg M. S. (2007). Four Weeks’ Intensive Rehabilitation Generates Significant Health Effects in COPD Patients. Chron. Respir. Dis. 4, 5–13. doi:10.1177/1479972306070374
Spruit M. A., Gosselink R., Troosters T., De Paepe K., Decramer M. (2002). Resistance versus Endurance Training in Patients with COPD and Peripheral Muscle Weakness. Eur. Respir. J. 19, 1072–1078. doi:10.1183/09031936.02.00287102
Spruit M. A., Singh S. J., Garvey C., ZuWallack R., Nici L., Rochester C., et al. (2013). An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 188, e13–e64. doi:10.1164/rccm.201309-1634ST
Steier J., Jolley C. J., Seymour J., Kaul S., Luo Y. M., Rafferty G. F., et al. (2008). Sleep-disordered Breathing in Unilateral Diaphragm Paralysis or Severe Weakness. Eur. Respir. J. 32, 1479–1487. doi:10.1183/09031936.00018808
Steiner M. C., Barton R. L., Singh S. J., Morgan M. D. (2003). Nutritional Enhancement of Exercise Performance in Chronic Obstructive Pulmonary Disease: A Randomised Controlled Trial. Thorax 58, 745–751. doi:10.1136/thorax.58.9.745
Sturdy G., Hillman D., Green D., Jenkins S., Cecins N., Eastwood P. (2003). Feasibility of High-Intensity, Interval-Based Respiratory Muscle Training in COPD. Chest 123, 142–150. doi:10.1378/chest.123.1.142
Sugawara K., Takahashi H., Kashiwagura T., Yamada K., Yanagida S., Homma M., et al. (2012). Effect of Anti-inflammatory Supplementation with Whey Peptide and Exercise Therapy in Patients with COPD. Respir. Med. 106, 1526–1534. doi:10.1016/j.rmed.2012.07.001
Sverzellati N., Colombi D., Randi G., Pavarani A., Silva M., Walsh S. L., et al. (2013). Computed Tomography Measurement of Rib Cage Morphometry in Emphysema. PLoS One 8, e68546. doi:10.1371/journal.pone.0068546
Thoma A., Lightfoot A. P. (2018). NF-kB and Inflammatory Cytokine Signalling: Role in Skeletal Muscle Atrophy. Adv. Exp. Med. Biol. 1088, 267–279. doi:10.1007/978-981-13-1435-3_12
Toledo-Arruda A. C., Vieira R. P., Guarnier F. A., Suehiro C. L., Caleman-Neto A., Olivo C. R., et al. (2017). Time-course Effects of Aerobic Physical Training in the Prevention of Cigarette Smoke-Induced COPD. J. Appl. Physiol. 123, 674–683. doi:10.1152/japplphysiol.00819.2016
Vallet G., Ahmaïdi S., Serres I., Fabre C., Bourgouin D., Desplan J., et al. (1997). Comparison of Two Training Programmes in Chronic Airway Limitation Patients: Standardized versus Individualized Protocols. Eur. Respir. J. 10, 114–122. doi:10.1183/09031936.97.10010114
Vanfleteren L. E. G. W., Spruit M. A., Wouters E. F. M., Franssen F. M. E. (2016). Management of Chronic Obstructive Pulmonary Disease beyond the Lungs. Lancet Respir. Med. 4, 911–924. doi:10.1016/S2213-2600(16)00097-7
Vermeeren M. A. P., Creutzberg E. C., Schols A. M. W. J., Postma D. S., Pieters W. R., Roldaan A. C., et al. (2006). Prevalence of Nutritional Depletion in a Large Out-Patient Population of Patients with COPD. Respir. Med. 100, 1349–1355. doi:10.1016/j.rmed.2005.11.023
Vieira P. J. C., Güntzel Chiappa A. M., Cipriano G., Umpierre D., Arena R., Chiappa G. R. (2014). Neuromuscular Electrical Stimulation Improves Clinical and Physiological Function in COPD Patients. Respir. Med. 108, 609–620. doi:10.1016/j.rmed.2013.12.013
Vieira Ramos G., Choqueta de Toledo-Arruda A., Maria Pinheiro-Dardis C., Liyoko Suehiro C., Luiz de Russo T., Vieira R. P., et al. (2018). Exercise Prevents Diaphragm Wasting Induced by Cigarette Smoke through Modulation of Antioxidant Genes and Metalloproteinases. Biomed. Res. Int. 2018, 1–8. doi:10.1155/2018/5909053
Vilaró J., Ramirez-Sarmiento A., Martínez-Llorens J. M., Mendoza T., Alvarez M., Sánchez-Cayado N., et al. (2010). Global Muscle Dysfunction as a Risk Factor of Readmission to Hospital Due to COPD Exacerbations. Respir. Med. 104, 1896–1902. doi:10.1016/j.rmed.2010.05.001
Vogiatzis I., Stratakos G., Simoes D. C. M., Terzis G., Georgiadou O., Roussos C., et al. (2007). Effects of Rehabilitative Exercise on Peripheral Muscle TNF , IL-6, IGF-I and MyoD Expression in Patients with COPD. Thorax 62, 950–956. doi:10.1136/thx.2006.069310
Wada J., Borges-Santos E., Porras D., Paisani D., Cukier A., Lunardi A., et al. (2016). Effects of Aerobic Training Combined with Respiratory Muscle Stretching on the Functional Exercise Capacity and Thoracoabdominal Kinematics in Patients with COPD: A Randomized and Controlled Trial. Copd Vol. 11, 2691–2700. doi:10.2147/COPD.S114548
Webster J. M., Kempen L. J. A. P., Hardy R. S., Langen R. C. J. (2020). Inflammation and Skeletal Muscle Wasting during Cachexia. Front. Physiol. 11, 597675. doi:10.3389/fphys.2020.597675
Weekes C. E., Emery P. W., Elia M. (2009). Dietary Counselling and Food Fortification in Stable COPD: A Randomised Trial. Thorax 64, 326–331. doi:10.1136/thx.2008.097352
Whidden M. A., Smuder A. J., Wu M., Hudson M. B., Nelson W. B., Powers S. K. (2010). Oxidative Stress Is Required for Mechanical Ventilation-Induced Protease Activation in the Diaphragm. J. Appl. Physiol. 108, 1376–1382. doi:10.1152/japplphysiol.00098.2010
Wijnhoven J. H., Janssen A. J. M., van Kuppevelt T. H., Rodenburg R. J. T., Dekhuijzen P. N. R. (2006). Metabolic Capacity of the Diaphragm in Patients with COPD. Respir. Med. 100, 1064–1071. doi:10.1016/j.rmed.2005.09.029
Wu W., Zhang X., Lin L., Ou Y., Li X., Guan L., et al. (2017). Transdiaphragmatic Pressure and Neural Respiratory Drive Measured during Inspiratory Muscle Training in Stable Patients with Chronic Obstructive Pulmonary Disease. Copd Vol. 12, 773–781. doi:10.2147/COPD.S126354
Xie L., Jiang J., Fu H., Zhang W., Yang L., Yang M. (2021). Malnutrition in Relation to Muscle Mass, Muscle Quality, and Muscle Strength in Hospitalized Older Adults. J. Am. Med. Directors Assoc. doi:10.1016/j.jamda.2021.11.025
Zhang B., Li P., Li J., Liu X., Wu W. (2021). Effect of Oxidative Stress on Diaphragm Dysfunction and Exercise Intervention in Chronic Obstructive Pulmonary Disease. Front. Physiol. 12, 684453. doi:10.3389/fphys.2021.684453
Zhou T., Sun C. (2021). Effect of Physical Manipulation Pulmonary Rehabilitation on Lung Cancer Patients after Thoracoscopic Lobectomy. Thorac. Cancer 13, 308–315. doi:10.1111/1759-7714.14225
Keywords: COPD, diaphragm dysfunction, structural change, systemic inflammation, inspiratory muscle training, exercise rehabilitation
Citation: Cao Y, Li P, Wang Y, Liu X and Wu W (2022) Diaphragm Dysfunction and Rehabilitation Strategy in Patients With Chronic Obstructive Pulmonary Disease. Front. Physiol. 13:872277. doi: 10.3389/fphys.2022.872277
Received: 10 February 2022; Accepted: 18 April 2022;
Published: 02 May 2022.
Edited by:
Hua Linda Cai, University of California, Los Angeles, United StatesReviewed by:
Feng He, California State University, United StatesCopyright © 2022 Cao, Li, Wang, Liu and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaodan Liu, aHpocDQwM0AxMjYuY29t; Weibing Wu, d3diNzVAMTI2LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.