 Georges Jabbour
Georges Jabbour Rony Ibrahim
Rony Ibrahim Nicola Bragazzi
Nicola Bragazzi
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Physiol. , 06 July 2022
Sec. Exercise Physiology
Volume 13 - 2022 | https://doi.org/10.3389/fphys.2022.869998
This article is part of the Research Topic Improving Exercise Testing Methods and Interpretation in Human Health and Diseases View all 18 articles
This systematic review summarizes current evidence on the relation between preoperative physical activity (PA) levels with bariatric surgery (BS) outcomes and on the beneficial role of preoperative exercise/PA program among BS candidates. This systematic review suggests that candidate patients accumulating the preoperative PA level improved several BS outcomes. These improvements were reported mainly for anthropometric and cardiometabolic parameters and physical function. Observed improvements manifested during a distinct period of time in response to a wide variety of exercise programs. Evidence on the preoperative PA level as well as on preoperative exercise implementation on BS outcomes is advocated despite the small number of participants and lack of control. Thus, further studies are required to explore the most effective and suitable form of exercise prescription prior to BS while considering physical and psychological limitations of obese patients.
Since severe obesity is associated with several health, physical, and psychological impairments (WHO Consultation on Obesity, 2000; Flegal et al., 2007; Engin, 2017; Pan et al., 2017), bariatric surgery (BS) is widely accepted as a valuable strategy to improve these alterations (Jabbour and Salman, 2021) and related comorbidities (Brethauer et al., 2011; Schauer et al., 2012; Li et al., 2014; Ardestani et al., 2015; Sams et al., 2016) in both short and long term. Despite all of these promising attributes, the large intersubject variabilities in the number of intra- and postoperative complications, as well as the length of operating time and hospital stay, remain unexplained (Fernandez Jr et al., 2004; Steinbrook, 2004; Nguyen et al., 2013).
While the exact reason for this large intersubject variability of BS outcomes is unclear, it seems that a greater preoperative fitness level and an elevated insulin sensitivity are linked to better post-BS outcomes (Gilbertson et al., 2017), while a lower cardiorespiratory fitness (i.e., VO2max < 15.8 ml/kg/min) is associated with a longer operating time, intubation duration, estimated blood loss during surgery, and more frequent cardiovascular complications (Gilbertson et al., 2020).
In their pilot trial, Gilberston et al. (2020) reported that prescribing aerobic exercise at the preoperative stage in addition to standard medical care induced significant improvements in postoperative BS outcomes when compared to standard medical care alone. According to these authors, these improvements may be mediated by fitness-related adaptations, including a reduction in adipose tissue-derived hormones, preservation of lean mass, and enhanced metabolic flexibility. Additional studies are still necessary to better profile the potential benefit of adding aerobic exercise and/or other forms of exercise to improve health parameters in bariatric patients. Thus, enhancing fitness indicators and metabolic parameters, prior to surgery, may improve patient outcomes (McCullough et al., 2006; Gilbertson et al., 2017).
The purpose of the present systematic review was to review the available evidence for the beneficial health impact of adding exercise to SC preoperatively and to address metabolic health and surgical outcomes compared to SC alone in patients receiving BS. Moreover, this systematic review highlights the exercise form and modality being implemented in obese patients.
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009). The Population, Intervention, Comparator, Outcomes, and Study design (PICOS) approach was used to identify the inclusion criteria (Table 1). Studies that have examined the effects of implementing a structured exercise or a physical activity intervention before BS on postoperative outcomes “body composition, weight loss, physical activity level, performance, and metabolic parameters” were eligible for inclusion. The studies were included in the current systematic review if they met the following criteria: 1) published in peer-reviewed journals, 2) included adult participants, and 3) compared BS outcomes pre- and/or postoperatively. The studies were excluded if they 1) reported only subjective measures, 2) were not written in English, or 3) were retrospective. Moreover, review articles were not included in the current systematic review.
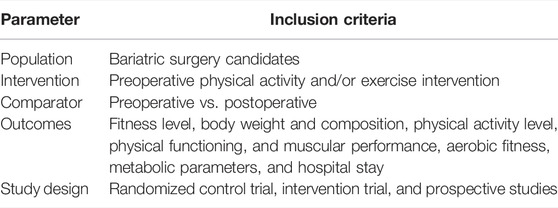
TABLE 1. PICOS criteria for inclusion of studies.
Literature searches were conducted in four electronic databases, including PubMed, Institute for Scientific Information (ISI) Web of Knowledge, Web of Science, and SPORTDiscus, to identify studies of preoperative exercise intervention or preoperative PA practices using the search terms “bariatric surgery” or “weight loss surgery” or “obesity surgery” or “weight reduction surgery” or “biliopancreatic diversion” or “laparoscopic band” or “lap and” or “gastric band” or “gastric bypass” or “gastroplasty” or “gastric sleeve” or “sleeve gastrectomy” and “preoperative exercise intervention” or “preoperative physical activity” or “preoperative lifestyle modification.”
The search was completed with a manual search of reference lists of key articles. Since the scope of this review is large in terms of outcome measures, a systematic review and not a meta-analysis was performed.
The final screening was performed by the principal investigator (GJ) based on the relevance of the inclusion and exclusion criteria and the identified items for assessing the effects of preoperative exercise intervention on anthropometric characteristics and body composition (e.g., body mass, body fat, and BMI), physical performances (e.g., muscular strength and physical capacity), cardiorespiratory fitness and function (e.g., oxygen uptake and heart rate), energy expenditure and metabolism parameters (e.g., resting metabolic rate, insulin resistance, and lipid profile), and hospital stay in obese adults of both genders undergoing BS using PICOS criteria. If the citation showed any potential relevance, the abstract was screened. When abstracts indicated potential inclusion, full-text articles were reviewed.
Our primary research identified 999 records, including 802 duplicates (Figure 1). After screening titles, abstracts, and full texts, 21 studies were included in our final analysis, and the characteristics of these studies are displayed in Table 2.

FIGURE 1. Flow diagram of included and excluded studies included in this systematic review using the recommendations in the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement.
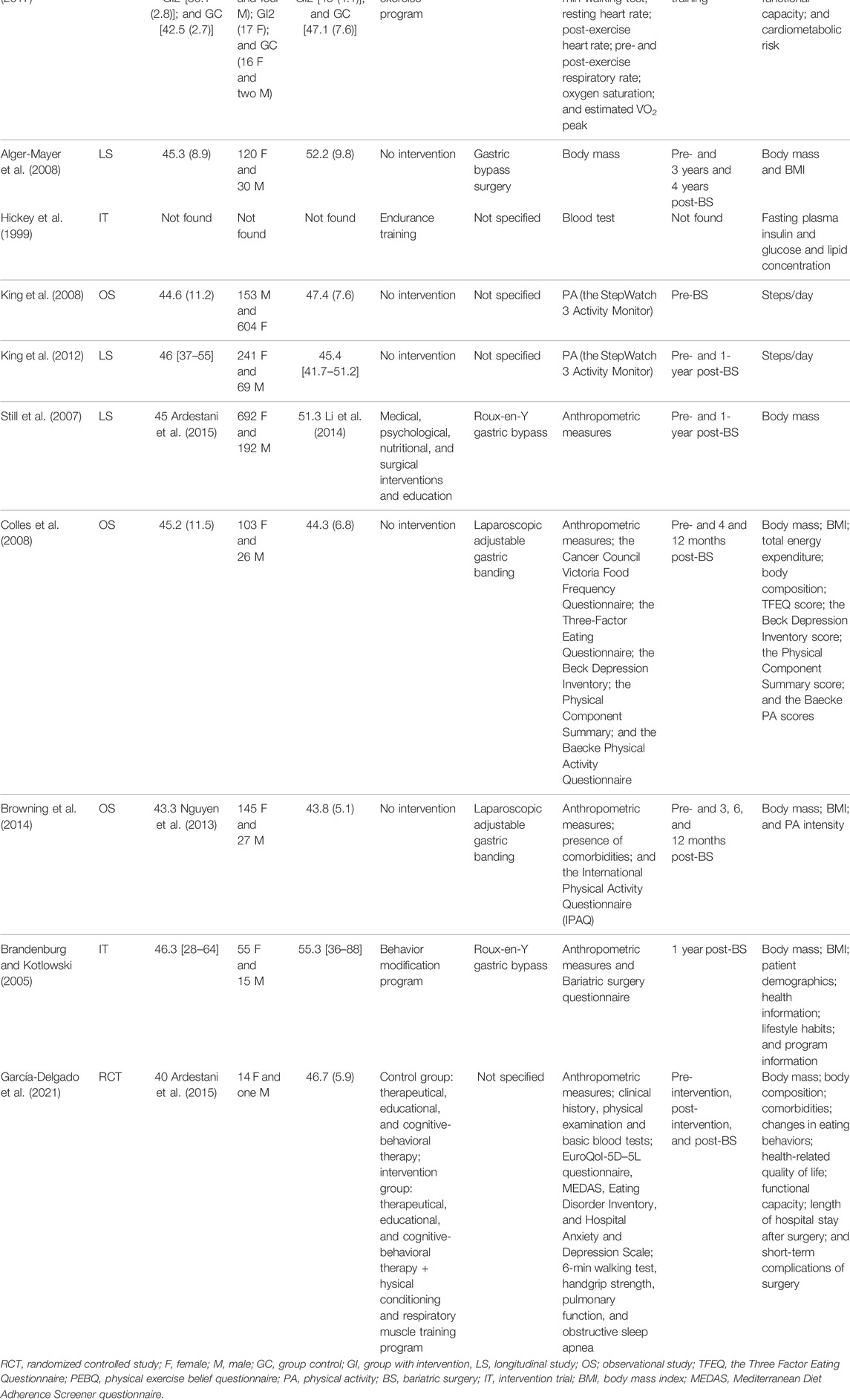
TABLE 2. Baseline characteristics of studies included in the review.
Out of 21 studies, 19 were prospective cohorts (Hickey et al., 1999; Still et al., 2007; Alger-Mayer et al., 2008; Colles et al., 2008; Funderburk and Callis, 2010; Marcon et al., 2011; King et al., 2012; Baillot et al., 2013; Browning et al., 2014; Bond et al., 2015a; Bond et al., 2015b; Baillot et al., 2016; Baillot et al., 2017; Bond et al., 2017; Marcon et al., 2017; Baillot et al., 2018; Daniels et al., 2018; Gilbertson et al., 2020; García-Delgado et al., 2021) and compared pre- to post-BS or pre- to postintervention outcomes in adult patients (Table 2). In total, 14 studies introduced an intervention pre-BS, of which 10 were randomized controlled trials that used a structured exercise program (Funderburk and Callis, 2010; Marcon et al., 2011; Baillot et al., 2013; Baillot et al., 2016; Baillot et al., 2017; Marcon et al., 2017; Baillot et al., 2018; Daniels et al., 2018; Gilbertson et al., 2020; García-Delgado et al., 2021), three studies used a physical activity program (Bond et al., 2015a; Bond et al., 2015b; Bond et al., 2017), and one study used a lifestyle modification program (Still et al., 2007) (Table 2). Among the 14 studies with an intervention, 11 studies performed a pre- to postintervention comparison, nine with exercise (Funderburk and Callis, 2010; Marcon et al., 2011; Baillot et al., 2013; Baillot et al., 2016; Baillot et al., 2017; Marcon et al., 2017; Daniels et al., 2018; Gilbertson et al., 2020), and two with PA intervention (Bond et al., 2015a; Bond et al., 2015b), while the remaining three studies performed a pre- to post-BS comparison (Still et al., 2007; Bond et al., 2017; Baillot et al., 2018) (Table 2).
Nine studies reported the effect of exercise training on anthropometric variables, among which five studies found no changes induced by the intervention (Table 3). Baillot et al. (2013) found a reduction in body mass, BMI, and fat mass after 12 weeks of supervised combined endurance and strength training (PreSET). In another study, Baillot et al. (2018) compared BMI between usual care and PreSET groups on seven different occasions (preintervention, 12 weeks postintervention, 2 weeks pre-BS, and 3, 6, 9, and 12 months post-BS). They found that the PreSET group experienced a greater decrease in BMI than the usual care group at 9 and 12 months post-BS. Furthermore, (Marcon et al. (2011 and 2017) reported larger decreases in body mass and BMI in the experimental groups than in the control group in two studies (Table 3). Funderburk and Callis (2010) reported a reduction in body mass after 12 weeks of supervised aquatic exercises, without a difference between the aquatic exercise and control groups. The rest of the studies did not find any anthropometric differences when comparing pre- to postintervention states or when comparing experimental (with exercise intervention) to control groups (without exercise intervention) (Hickey et al., 1999; Baillot et al., 2016; Baillot et al., 2017; Daniels et al., 2018; Gilbertson et al., 2020) (Table 3).
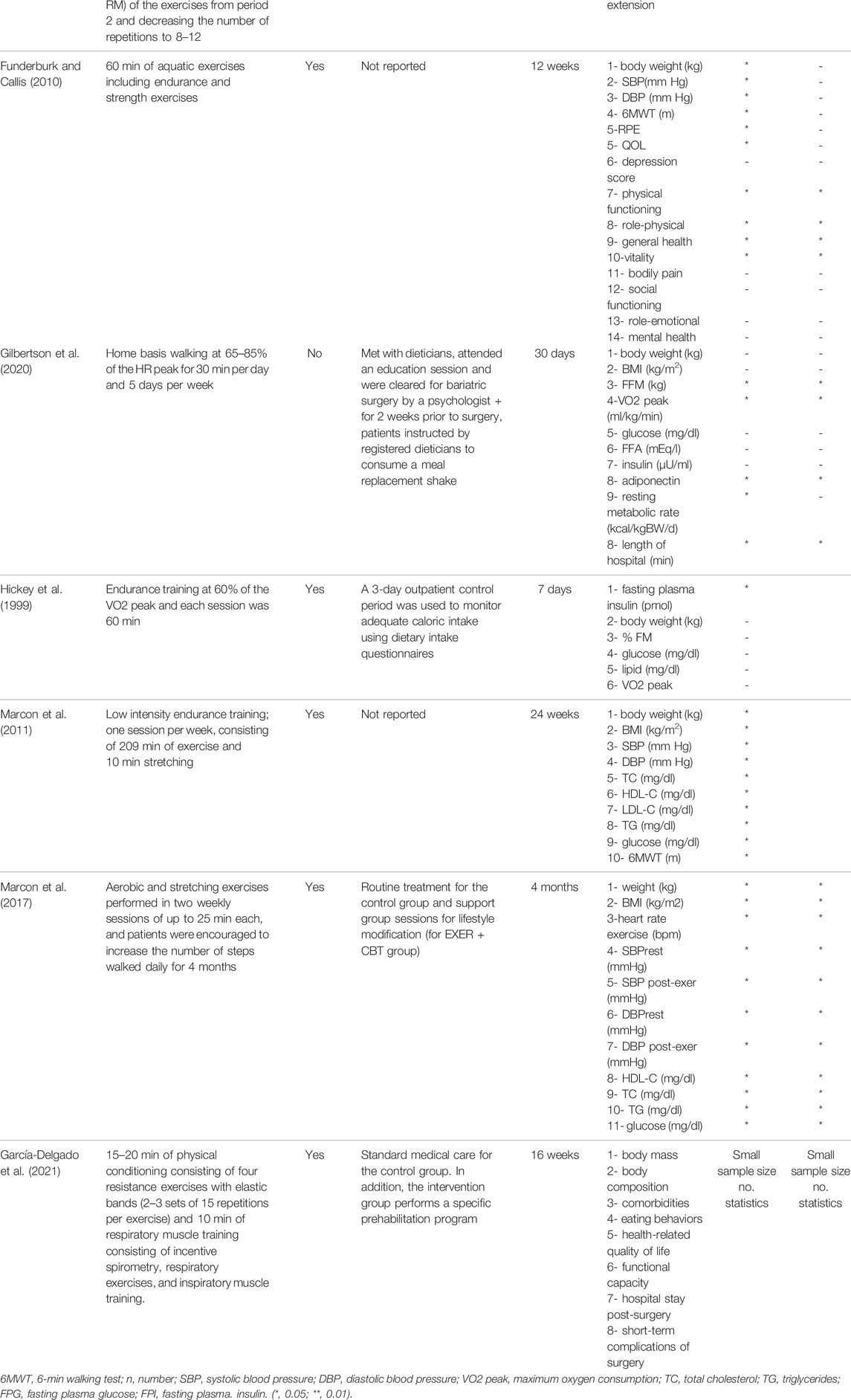
TABLE 3. Pre- vs. postoperative body composition, weight loss, physical activity level, performance, and metabolic parameters.
Nine studies reported the effect of exercise intervention on physical fitness parameters (Funderburk and Callis, 2010; Marcon et al., 2011; Baillot et al., 2013; Baillot et al., 2016; Baillot et al., 2017; Marcon et al., 2017; Baillot et al., 2018; Daniels et al., 2018; Gilbertson et al., 2020), of which two found no changes in measured parameters induced by the intervention (Marcon et al., 2017; Gilbertson et al., 2020) (Table 3). All four studies that used concurrent training (endurance and strength training) reported improvement in cardiovascular and/or muscular fitness parameters (Baillot et al., 2013; Baillot et al., 2016; Baillot et al., 2017; Baillot et al., 2018). Baillot et al. (2013 and 2016) compared patients’ baseline measures to 12 weeks post-training. They found an improvement in the 6-min walk test (6MWT) distance, percentage of theoretical 6MWT distance reached, 6MWT heart cost, half-squat test, and arm curl test. No differences were found in the sit-to-stand test or maximum aerobic capacity. In another study, Baillot et al. (2017) performed within (pre- and 12 weeks post-training) and between groups (training vs. conventional care group) comparisons. Compared to baseline measures, 6MWT distance, sit-to-stand repetitions, arm curl repetitions, and maximal aerobic capacity improved after 12 weeks of training. However, only the 6MWT distance, arm curl repetitions, and 6MWT heart cost improved in the training group compared to the conventional care group (Table 3). Another study between-group comparison revealed an improvement in 6MWT heart cost and the half-squat test for the training compared to the conventional care group (Baillot et al., 2018). Notably, the 6MWT distance was found to improve in two studies after aerobic training programs (Marcon et al., 2011) and aquatic exercise programs (Funderburk and Callis, 2010). Finally, only one study evaluated the effect of a 12-week resistance training program and found improvements in leg press strength, leg extension strength, and leg press muscle quality (Daniels et al., 2018) (Table 3).
Fourteen studies introduced an intervention, among which only four studies reported health-related parameters (Marcon et al., 2011; Baillot et al., 2016; Marcon et al., 2017; Gilbertson et al., 2020) (Table 3). Baillot et al. (2016) reported that BS candidates who were committed to a 12-week exercise intervention were protected from worsening of musculoskeletal pain. Gilbertson et al. (2020) tested the effect of a pre-BS aerobic exercise intervention on insulin sensitivity, metabolic flexibility, adipokines, and length of hospital stay. Marcon et al. (2011) evaluated the effect of an aerobic exercise program on the cardio-metabolic risk of BS candidates. A significant decrease in systolic and diastolic pressure and the Framingham risk score was found after 6 months of the supervised aerobic exercise program (Table 3).
In general, patients awaiting BS have a reduced physical fitness level and impairments in several metabolic variables and body composition before surgery. Although BS results in significant weight loss and body composition changes after surgery, it remains uncertain whether other health outcomes (e.g., fitness, metabolic, and cardiorespiratory parameters) are sufficiently improved and how long the improvements can be maintained. The present systematic review highlights the importance of implementing PA and/or exercise interventions close to the candidate’s date of surgery (Bond et al., 2006; Bond et al., 2015a; Bond et al., 2015b; Bond et al., 2017). Such interventions could procure many health benefits during the preoperative period (e.g., improved fitness level and PA levels) and in postoperative outcomes (e.g., reduced BS-related complications and reduced hospital length of stay) among BS candidates. Therefore, a preoperative PA/exercise intervention could be an ideal approach to maximize the BS benefits and to offer a successful transition toward improving postoperative lifestyle behaviors among BS candidates. Nevertheless, studies with larger cohorts are needed to confirm these results, and a longer follow-up period (>1 year) is required to understand more fully the impact of a preoperative intervention on postoperative outcomes.
Six studies examined the effect of PA and/or exercise intervention on body composition parameters pre- vs. postoperatively (Brandenburg and Kotlowski, 2005; Still et al., 2007; Alger-Mayer et al., 2008; Colles et al., 2008; Browning et al., 2014; Baillot et al., 2018), and five studies reported relevant data regarding body composition parameters before and after PA/exercise intervention in preoperative BS candidates (Baillot et al., 2013; Baillot et al., 2016; Baillot et al., 2017; Marcon et al., 2017; Baillot et al., 2018) (Table 4). Some studies showed a significant decrease in preoperative body mass (Still et al., 2007; Alger-Mayer et al., 2008; Bond et al., 2015a) or BMI (King et al., 2008) after an intervention. For these studies, the positive impact procured by a PA intervention prior to BS may be explained primarily by the improvement in PA and physical fitness levels among BS candidates, which is an important step toward improving their overall health parameters. Despite these promising results, it remains difficult to attribute all of these improvements solely to PA considering that many limitations have not been addressed, such as the lack of any control of PA (in the majority of cases, patients were only advised to practice PA) without excluding the interference of BS candidates’ existing conditions (such as BMI and comorbidities) as well as their diet and lifestyle prior to surgery.
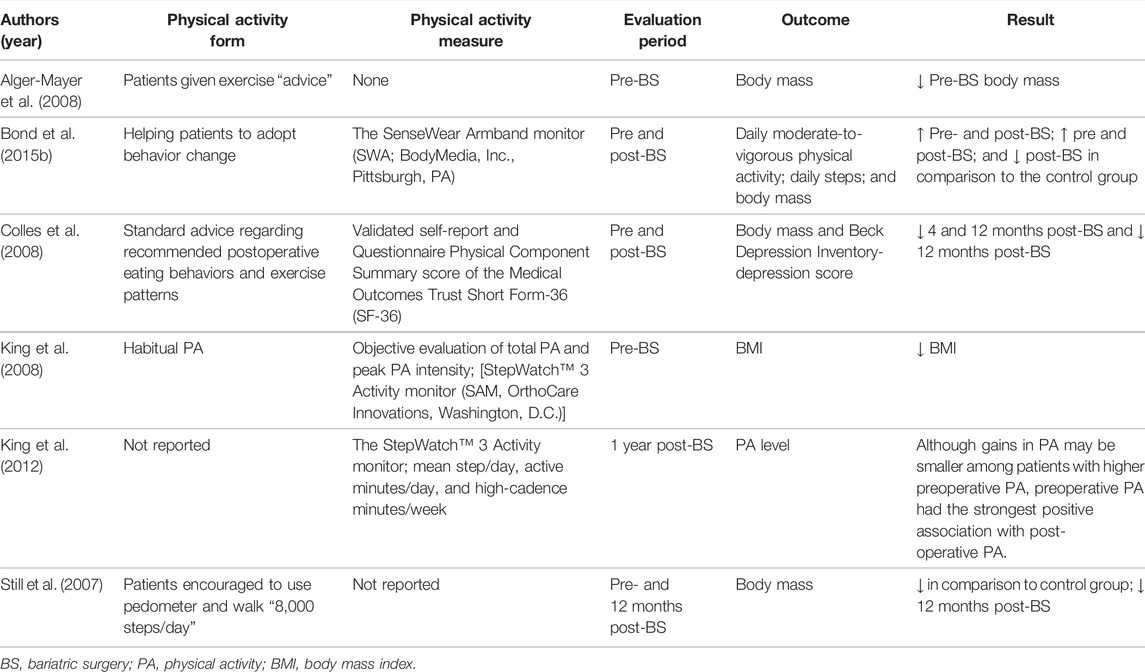
TABLE 4. Preoperative physical activity and its effects on candidates’ outcomes.
Nonetheless, the effect of PA and exercise interventions on postoperative anthropometric parameters has been considered an interesting topic. Studies using interdisciplinary individual lifestyle counseling and helping BS patients adopt behavioral changes (e.g., to be active) (Still et al., 2007; Colles et al., 2008; Bond et al., 2015b) reported significant decreases in body mass during the post-BS period (Table 4). However, the lack of a control group, the small sample size, and the specificity of the sample may limit the generalizability of these results.
Other studies (Funderburk and Callis, 2010; Baillot et al., 2016; Baillot et al., 2017; Daniels et al., 2018; Gilbertson et al., 2020) applying supervised exercise training during the preoperative period found no significant pre- to postoperative changes in any body composition parameters between the intervention and usual care groups. It seems that BS induces a strong influence on weight loss and therefore can mask any eventual effect of preoperative intervention. In a study by Baillot et al. (2016), participants received lifestyle counseling for an average of 10.4 ± 4.0 months (5.8 ± 1.8 dietician and 5.6 ± 1.8 PA specialist visits) before inclusion in the study. Thus, significant changes might have occurred before inclusion in the surgical treatment option. In contrast, Baillot et al. (2018) reported a larger BMI decrease in the BS group undergoing preoperative exercise intervention (PreSET) compared to that in the usual care group and attributed this improvement to the higher loss of fat-free mass (FFM) in the PreSET group. Moreover, Gilbertson et al. (2020) reported a significant decrease in FFM in participants undergoing preoperative home-based walking for 30 min per day. In addition, Marcon et al. (2017) reported similar results after 4 months of aerobic and stretching exercises. These discrepancies among results might be primarily attributed to the duration and form of intervention. Moreover, the characteristics of patients prior to the PA and exercise intervention must be considered. In fact, many BS candidates encounter remarkable difficulties (e.g., musculoskeletal problems, preoperative fitness level) that might affect their exercise tolerance and adherence, consequently limiting or reducing the PA/exercise intervention benefits. Therefore, more support in selecting an appropriate activity along with a feasible monitoring technique is highly required in such a context.
Reduced physical fitness, reported mostly in BS candidates, may affect the BS results. Current evidence supporting the importance of increasing the physical fitness level in BS candidates is not abundant but is promising. In fact, several studies found that a preoperative intervention based on exercise or Pa that aimed at improving physical fitness and performance indicators (e.g., strength, 6MWT distance, and maximal aerobic capacity) among individuals awaiting BS may be an effective strategy to improve the BS candidates’ overall health parameters and their BS outcomes (Funderburk and Callis, 2010; Baillot et al., 2013; Baillot et al., 2016; Baillot et al., 2017; Marcon et al., 2017; Baillot et al., 2018; Daniels et al., 2018). In this regard, Baillot et al. (2013 and 2016), in their randomized controlled trial, reported a significant increase in some physical function parameters assessed with a test battery (6MWT, sit-to-stand, half-squat, and arm curl test) after 12 weeks of supervised exercise training either with or without an individual lifestyle counseling intervention. One study by Gilbertson et al. (2020) reported significant increases in the VO2 peak among BS candidates after adding preoperative aerobic exercise to standard medical care. To the best of our knowledge, this is the only study to investigate the effect of a preoperative PA intervention on aerobic performance. The increase in the VO2 peak may be associated with a shorter operation time and length of hospital stay and with prevention of muscle loss along with a concomitant increase in the PA level among BS candidates. However, the mechanism underlying these improvements remains to be studied.
The PA level is an interesting parameter that has been evaluated. In a long-term study (1 year after surgery), Baillot et al. (2018) reported that the addition of preoperative supervised exercise training to individual lifestyle counseling improved PA levels and submaximal physical fitness 1 year post-BS. Similarly, King et al. (2012) reported a gain in the PA level 1 year after surgery among patients with higher preoperative PA levels. Other short-term studies (Bond et al., 2015a; Baillot et al., 2016; Bond et al., 2017) reported similar results regarding PA levels in response to preoperative intervention. A small amount of evidence suggests that improvements in PA in response to a preoperative PA/exercise intervention may mainly be attributed to improvements in PA barriers, social interactions, and feelings of embarrassment (Bond et al., 2015a; Baillot et al., 2016). In addition, the impact of the overall improvement in the fitness level following a PA/exercise intervention aimed at improving the physical fitness of preoperative BS candidates cannot be overlooked. However, the small sample size and exclusion criteria applied in the aforementioned studies prevent their generalization to all subjects awaiting BS. Moreover, the study recruitment process was limited to volunteers who were able to frequently visit the facility and were without major functional limitations.
Only four studies have explored a limited number of health parameters (Marcon et al., 2011; Baillot et al., 2016; Marcon et al., 2017; Gilbertson et al., 2020). Baillot et al. (2016) looked at the effect of a 12-week exercise program on musculoskeletal pain and found that BS candidates can be protected from worsening of pain associated with daily life activities. Additional studies are required to confirm the impact of PA on musculoskeletal pain before and after BS. In a study by Gilbertson et al. (2020), patients undergoing preoperative EX + SC prior to bariatric surgery had a shorter length of hospital stay than patients undergoing preoperative SC. Two studies by Marcon et al. (2011 and 2017) reported a significant decrease in systolic and diastolic blood pressure and the Framingham risk score after 6 months of a supervised aerobic exercise program.
To date, the mechanisms responsible for such improvement have not been explored, although current evidence clearly favors a preoperative PA/exercise intervention for facilitating better postoperative outcomes. Few studies have investigated the role of preoperative interventions on BS outcomes. The differences in study design and the lack of randomized controlled trials decrease the evidence level of the results. Moreover, the heterogeneity of activities performed (with or without supervision), the inclusion criteria, and the interference of covariates (e.g., participant characteristics) were not well controlled. Finally, it is important to mention that the included studies were very small and had a short follow-up time, thus making the results less convincing. The data provided by this review did not consider BS procedures (i.e., type of surgery), making the results difficult to interpret.
In conclusion, this review summarizes the benefits of a preoperative PA/exercise intervention among BS candidates and highlights the importance of such strategies as a component of medical therapy. A good understanding of the beneficial effect of improving the preoperative physical condition on postoperative outcomes is highly recommended for future interventional studies to potentiate the beneficial effect of BS among obese candidates. Based on significant evidence, including optimized weight loss post BS, reduced cardiovascular risk, and increases in patients’ regular PA and fitness levels, there is a need to implement a PA/exercise program before BS to promote and optimize BS outcomes. Nevertheless, there is a need for future investigations in this field to determine the most appropriate form(s) of PA/exercise intervention according to the patient profile.
GJ and RI were involved in the conceptualization of the study, data analysis, and the writing of the manuscript. NB was involved in data assessment, data analysis, and the writing of the manuscript. All authors approved the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
BMI, body mass index; BS, bariatric surgery; BW, body weight; C, abdominal circumference; F, female; FFM, fat-free mass; FM, fat mass; GC, group control; GI, group with intervention; HbA1c, glycated hemoglobin; HOMA-IR, homeostatic model assessment for insulin resistance; HR, heart rate; IT, intervention trial; LS, longitudinal study; M, male; OS, observational study; PA, physical activity; PEBQ, physical exercise belief questionnaire; REE, resting energy expenditure; TEE, total energy expenditure; W/H, waist-to-hip ratio; WC, waist circumference; RCT, randomized controlled study; and TFEQ, three-factor eating questionnaire.
Alger-Mayer S., Polimeni J. M., Malone M. (2008). Preoperative Weight Loss as a Predictor of Long-Term Success Following Roux-En-Y Gastric Bypass. Obes. Surg. 18 (7), 772–775. doi:10.1007/s11695-008-9482-2
Ardestani A., Rhoads D., Tavakkoli A. (2015). Insulin Cessation and Diabetes Remission after Bariatric Surgery in Adults with Insulin-Treated Type 2 Diabetes. Diabetes Care 38 (4), 659–664. doi:10.2337/dc14-1751
Baillot A., Boissy P., Tousignant M., Langlois M.-F. (2017). Feasibility and Effect of In-Home Physical Exercise Training Delivered via Telehealth before Bariatric Surgery. J. Telemed. Telecare 23 (5), 529–535. doi:10.1177/1357633x16653511
Baillot A., Mampuya W. M., Comeau E., Méziat-Burdin A., Langlois M. F. (2013). Feasibility and Impacts of Supervised Exercise Training in Subjects with Obesity Awaiting Bariatric Surgery: a Pilot Study. Obes. Surg. 23 (7), 882–891. doi:10.1007/s11695-013-0875-5
Baillot A., Mampuya W. M., Dionne I. J., Comeau E., Méziat-Burdin A., Langlois M.-F. (2016). Impacts of Supervised Exercise Training in Addition to Interdisciplinary Lifestyle Management in Subjects Awaiting Bariatric Surgery: a Randomized Controlled Study. Obes. Surg. 26 (11), 2602–2610. doi:10.1007/s11695-016-2153-9
Baillot A., Vallée C.-A., Mampuya W. M., Dionne I. J., Comeau E., Méziat-Burdin A., et al. (2018). Effects of a Pre-surgery Supervised Exercise Training 1 Year after Bariatric Surgery: a Randomized Controlled Study. Obes. Surg. 28 (4), 955–962. doi:10.1007/s11695-017-2943-8
Bond D. S., Evans R. K., DeMaria E., Wolfe L., Meador J., Kellum J., et al. (2006). Physical Activity and Quality of Life Improvements before Obesity Surgery. Am. J. Health Behav. 30 (4), 422–434. doi:10.5993/ajhb.30.4.8
Bond D. S., Thomas J. G., King W. C., Vithiananthan S., Trautvetter J., Unick J. L., et al. (2015). Exercise Improves Quality of Life in Bariatric Surgery Candidates: Results from theBari-Activetrial. Obesity 23 (3), 536–542. doi:10.1002/oby.20988
Bond D. S., Thomas J. G., Vithiananthan S., Unick J., Webster J., Roye G. D., et al. (2017). Intervention-related Increases in Preoperative Physical Activity Are Maintained 6-months after Bariatric Surgery: Results from the Bari-Active Trial. Int. J. Obes. 41 (3), 467–470. doi:10.1038/ijo.2016.237
Bond D. S., Vithiananthan S., Thomas J. G., Trautvetter J., Unick J. L., Jakicic J. M., et al. (2015). Bari-Active: a Randomized Controlled Trial of a Preoperative Intervention to Increase Physical Activity in Bariatric Surgery Patients. Surg. Obes. Relat. Dis. 11 (1), 169–177. doi:10.1016/j.soard.2014.07.010
Brandenburg D., Kotlowski R. (2005). Practice Makes Perfect? Patient Response to a Prebariatric Surgery Behavior Modification Program. Obes. Surg. 15 (1), 125–132. doi:10.1381/0960892052993594
Brethauer S. A., Heneghan H. M., Eldar S., Gatmaitan P., Huang H., Kashyap S., et al. (2011). Early Effects of Gastric Bypass on Endothelial Function, Inflammation, and Cardiovascular Risk in Obese Patients. Surg. Endosc. 25 (8), 2650–2659. doi:10.1007/s00464-011-1620-6
Browning M. G., Baugh N. G., Wolfe L. G., Kellum J. K., Maher J. W., Evans R. K. (2014). Evaluation of Pre- and Postoperative Physical Activity Participation in Laparoscopic Gastric Banding Patients. Obes. Surg. 24 (11), 1981–1986. doi:10.1007/s11695-014-1283-1
Colles S. L., Dixon J. B., O’Brien P. E. (2008). Hunger Control and Regular Physical Activity Facilitate Weight Loss after Laparoscopic Adjustable Gastric Banding. Obes. Surg. 18 (7), 833–840. doi:10.1007/s11695-007-9409-3
Daniels P., Burns R. D., Brusseau T. A., Hall M. S., Davidson L., Adams T. D., et al. (2018). Effect of a Randomised 12-week Resistance Training Programme on Muscular Strength, Cross-Sectional Area and Muscle Quality in Women Having Undergone Roux-En-Y Gastric Bypass. J. Sports Sci. 36 (5), 529–535. doi:10.1080/02640414.2017.1322217
Engin A. (2017). The Definition and Prevalence of Obesity and Metabolic Syndrome. Adv. Exp. Med. Biol. 960, 1–17. doi:10.1007/978-3-319-48382-5_1
Fernandez Jr A. Z., DeMaria E. J., Tichansky D. S., Kellum J. M., Wolfe L. G., Meador J., et al. (2004). Experience with over 3,000 Open and Laparoscopic Bariatric Procedures: Multivariate Analysis of Factors Related to Leak and Resultant Mortality. Surg. Endosc. 18 (2), 193–197. doi:10.1007/s00464-003-8926-y
Flegal K. M., Graubard B. I., Williamson D. F., Gail M. H. (2007). Cause-specific Excess Deaths Associated with Underweight, Overweight, and Obesity. JAMA 298 (17), 2028–2037. doi:10.1001/jama.298.17.2028
Funderburk J., Callis S. (2010). Aquatic Intervention Effect on Quality of Life Prior to Obesity Surgery: a Pilot Study. Annu. Ther. Recreat. 18, 66–78.
García-Delgado Y., López-Madrazo-Hernández M. J., Alvarado-Martel D., Miranda-Calderín G., Ugarte-Lopetegui A., González-Medina R. A., et al. (2021). Prehabilitation for Bariatric Surgery: A Randomized, Controlled Trial Protocol and Pilot Study. Nutrients 13 (9). doi:10.3390/nu13092903
Gilbertson N. M., Gaitán J. M., Osinski V., Rexrode E. A., Garmey J. C., Mehaffey J. H., et al. (2020). Pre-operative Aerobic Exercise on Metabolic Health and Surgical Outcomes in Patients Receiving Bariatric Surgery: A Pilot Trial. PLoS One 15 (10), e0239130. doi:10.1371/journal.pone.0239130
Gilbertson N. M., Paisley A. S., Kranz S., Weltman A., Kirby J. L., Hallowell P. T., et al. (2017). Bariatric Surgery Resistance: Using Preoperative Lifestyle Medicine And/or Pharmacology for Metabolic Responsiveness. Obes. Surg. 27 (12), 3281–3291. doi:10.1007/s11695-017-2966-1
Hickey M., Gavigan K., McCammon M., Tyndall G., Pories W., Israel R., et al. (1999). Effects of 7 Days of Exercise Training on Insulin Action in Morbidly Obese Men. Clin. Exerc Physiol. 1, 24–28.
Jabbour G., Salman A. (2021). Bariatric Surgery in Adults with Obesity: the Impact on Performance, Metabolism, and Health Indices. Obes. Surg. 31 (4), 1767–1789. doi:10.1007/s11695-020-05182-z
King W. C., Belle S. H., Eid G. M., Dakin G. F., Inabnet W. B., Mitchell J. E., et al. (2008). Physical Activity Levels of Patients Undergoing Bariatric Surgery in the Longitudinal Assessment of Bariatric Surgery Study. Surg. Obes. Relat. Dis. 4 (6), 721–728. doi:10.1016/j.soard.2008.08.022
King W. C., Hsu J. Y., Belle S. H., Courcoulas A. P., Eid G. M., Flum D. R., et al. (2012). Pre- to Postoperative Changes in Physical Activity: Report from the Longitudinal Assessment of Bariatric Surgery-2 (LABS-2). Surg. Obes. Relat. Dis. 8 (5), 522–532. doi:10.1016/j.soard.2011.07.018
Li J.-F., Lai D.-D., Lin Z.-H., Jiang T.-Y., Zhang A.-M., Dai J.-F. (2014). Comparison of the Long-Term Results of Roux-En-Y Gastric Bypass and Sleeve Gastrectomy for Morbid Obesity. Surg. Laparosc. Endosc. Percutan Tech. 24 (1), 1–11. doi:10.1097/sle.0000000000000041
Marcon E. R., Baglioni S., Bittencourt L., Lopes C. L. N., Neumann C. R., Trindade M. R. M. (2017). What Is the Best Treatment before Bariatric Surgery? Exercise, Exercise and Group Therapy, or Conventional Waiting: a Randomized Controlled Trial. Obes. Surg. 27 (3), 763–773. doi:10.1007/s11695-016-2365-z
Marcon E. R., Gus I., Neumann C. R. (2011). Impacto de um programa mínimo de exercícios físicos supervisionados no risco cardiometabólico de pacientes com obesidade mórbida. Arq. Bras. Endocrinol. Metab. 55 (5), 331–338. doi:10.1590/s0004-27302011000500006
McCullough P. A., Gallagher M. J., Dejong A. T., Sandberg K. R., Trivax J. E., Alexander D., et al. (2006). Cardiorespiratory Fitness and Short-Term Complications after Bariatric Surgery. Chest 130 (2), 517–525. doi:10.1378/chest.130.2.517
Moher D., Liberati A., Tetzlaff J., Altman D. G., Group P. (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA Statement. Ann. Intern Med. 151 (4), 264W64–9. doi:10.7326/0003-4819-151-4-200908180-00135
Nguyen N. Q., Game P., Bessell J., Debreceni T. L., Neo M., Burgstad C. M., et al. (2013). Outcomes of Roux-En-Y Gastric Bypass and Laparoscopic Adjustable Gastric Banding. Wjg 19 (36), 6035–6043. doi:10.3748/wjg.v19.i36.6035
Pan F., Laslett L., Blizzard L., Cicuttini F., Winzenberg T., Ding C., et al. (2017). Associations between Fat Mass and Multisite Pain: A Five‐Year Longitudinal Study. Arthritis Care & Res. 69 (4), 509–516. doi:10.1002/acr.22963
Sams V. G., Blackledge C., Wijayatunga N., Barlow P., Mancini M., Mancini G., et al. (2016). Effect of Bariatric Surgery on Systemic and Adipose Tissue Inflammation. Surg. Endosc. 30 (8), 3499–3504. doi:10.1007/s00464-015-4638-3
Schauer P. R., Kashyap S. R., Wolski K., Brethauer S. A., Kirwan J. P., Pothier C. E., et al. (2012). Bariatric Surgery versus Intensive Medical Therapy in Obese Patients with Diabetes. N. Engl. J. Med. 366 (17), 1567–1576. doi:10.1056/nejmoa1200225
Steinbrook R. (2004). Surgery for Severe Obesity. N. Engl. J. Med. 350 (11), 1075–1079. doi:10.1056/nejmp048029
Still C. D., Benotti P., Wood G. C., Gerhard G. S., Petrick A., Reed M., et al. (2007). Outcomes of Preoperative Weight Loss in High-Risk Patients Undergoing Gastric Bypass Surgery. Arch. Surg. 142 (10), 994–998. discussion 9. doi:10.1001/archsurg.142.10.994
Keywords: bariatric surgery, physical activity, exercise intervention, pre-operative, health outcomes
Citation: Jabbour G, Ibrahim R and Bragazzi N (2022) Preoperative Physical Activity Level and Exercise Prescription in Adults With Obesity: The Effect on Post-Bariatric Surgery Outcomes. Front. Physiol. 13:869998. doi: 10.3389/fphys.2022.869998
Received: 05 February 2022; Accepted: 16 May 2022;
Published: 06 July 2022.
Edited by:
Mathieu Gruet, Université de Toulon, FranceReviewed by:
Nicole Gilbertson, The Pennsylvania State University (PSU), United StatesCopyright © 2022 Jabbour, Ibrahim and Bragazzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Georges Jabbour, Z2phYmJvdXJAcXUuZWR1LnFh, Z2Vvcmdlc2phYmJvdXIxOTgwQGhvdG1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.