
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Physiol. , 12 January 2022
Sec. Clinical and Translational Physiology
Volume 12 - 2021 | https://doi.org/10.3389/fphys.2021.815842
 Francesca Racca1,2*
Francesca Racca1,2* Gaia Pellegatta3
Gaia Pellegatta3 Giuseppe Cataldo1Edoardo Vespa2,3Elisa Carlani3
Giuseppe Cataldo1Edoardo Vespa2,3Elisa Carlani3 Corrado Pelaia4
Corrado Pelaia4 Giovanni Paoletti1,2Maria Rita Messina1,2Emanuele Nappi1,2Giorgio Walter Canonica1,2Alessandro Repici2,3
Giovanni Paoletti1,2Maria Rita Messina1,2Emanuele Nappi1,2Giorgio Walter Canonica1,2Alessandro Repici2,3 Enrico Heffler1,2
Enrico Heffler1,2
Eosinophilic esophagitis (EoE) is a chronic immune-mediated disease of the esophagus characterized clinically by symptoms related to esophageal dysfunction and histologically by eosinophil-predominant inflammation, whose incidence is rising. It significantly affects patients’ quality of life and, if left untreated, results in fibrotic complications. Although broad consensus has been achieved on first-line therapy, a subset of patients remains non-responder to standard therapy. The pathogenesis of EoE is multifactorial and results from the complex, still mostly undefined, interaction between genetics and intrinsic factors, environment, and antigenic stimuli. A deep understanding of the pathophysiology of this disease is pivotal for the development of new therapies. This review provides a comprehensive description of the pathophysiology of EoE, starting from major pathogenic mechanisms (genetics, type 2 inflammation, epithelial barrier dysfunction, gastroesophageal reflux, allergens, infections and microbiota) and subsequently focusing on the single protagonists of type 2 inflammation (involved cells, cytokines, soluble effectors, surface proteins and transcription factors) that could represent present and future therapeutic targets, while summarizing previous therapeutic approaches in literature.
Eosinophilic esophagitis (EoE) is a chronic immune-mediated disease of the esophagus characterized clinically by symptoms related to esophageal dysfunction and histologically by eosinophil-predominant inflammation (Dellon and Hirano, 2018).
Eosinophilic esophagitis can affect all age groups, with an incidence peak between the third and the fifth decade of life. Its estimated prevalence is 30–100/100.000 in the adult population and 29–42/100.000 in the pediatric population (Soon et al., 2013; Dellon et al., 2014a; Arias et al., 2016). EoE is most frequent in males, with a male-to-female ratio of about 3:1 (Hruz, 2014) and a predilection for Caucasian ethnicity (Arias et al., 2016).
Since its relatively new recognition in the ‘70s, EoE incidence has risen rapidly over the last 15 years both in the US (Prasad et al., 2009) and in Europe (Hruz et al., 2011; van Rhijn et al., 2013) and EoE is now recognized as the first cause of dysphagia in the adult population (Moawad et al., 2014). The reasons for this recent increase are still debated and, while increased recognition and raised awareness undoubtedly contributed, data are consistent with a true increase (Dellon, 2014; Dellon et al., 2015).
Up to 80% of patients have a personal history of atopic comorbidities, such as allergic rhinitis, asthma, food allergy and atopic dermatitis (AD) (Franciosi et al., 2009). Other associated diseases comprehend celiac disease, inherited connective tissue disorders (CTDs), type 1 diabetes, cystic fibrosis, autism, esophageal atresia and monogenic diseases (i.e., autosomal dominant hyper-IgE syndrome, Netherton syndrome, Severe atopic syndrome associated with metabolic wasting -SAM) (Abonia et al., 2013; Guarino et al., 2016; Votto et al., 2020).
The main clinical manifestations of EoE in adults are dysphagia and food impaction after ingestion of solid foods. Other less common symptoms are chest pain and refractory heartburn and regurgitation. In children and infants, symptoms might be more subtle with failure to thrive, vomiting, nausea, regurgitation, abdominal pain, food aversion, and feeding problems (Noel et al., 2004; Mukkada et al., 2010).
Compensation mechanisms, such as prolonged mastication and assumption of liquids during meals, frequently lead to diagnostic delay (Reed et al., 2018; Lenti et al., 2021). The endoscopic appearance of EoE can show mucosal edema, mucosal rings (trachealization), exudates, linear furrows, and strictures (Sherrill and Rothenberg, 2014). However, up to one-third of EoE patients have a macroscopically normal endoscopy (Liacouras et al., 2011; Figure 1).
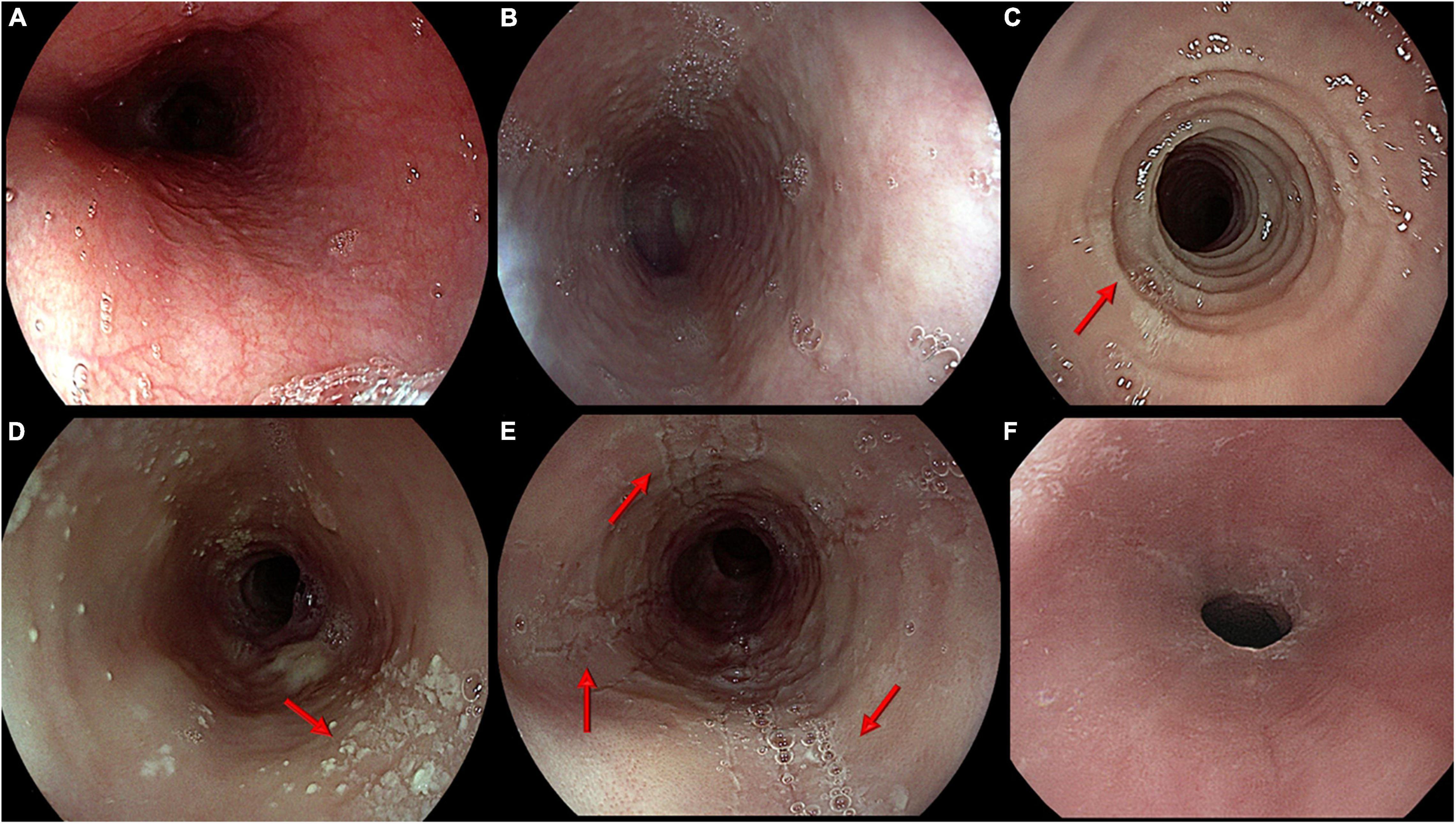
Figure 1. Main endoscopic features of eosinophilic esophagitis. From top left: (A) Normal appearance of esophageal mucosa; (B) Edema. Pale mucosa with attenuation of the normal vascular pattern; (C) Rings. Trachealized esophagus with multiple concentric rings (arrow); (D) Exudates. Whitish small plaques not washable through water jet (arrow); (E) Furrows. Typical longitudinal furrows (arrows); (F) Stricture. Narrowing of esophageal lumen not passable by a standard scope (diameter around 9 mm).
The current consensus criteria for EoE diagnosis include signs and symptoms of esophageal dysfunction and a eosinophil-predominant inflammation of the esophagus confirmed histologically by a peak count equal or higher than 15 eosinophils per high-power field, in the absence of other causes of esophageal eosinophilia (including eosinophilic gastritis -EG and enteritis – EGE, Leśniowski-Crohn disease, parasitic infection, achalasia, hypereosinophilic syndrome, hypersensitivity to medicines, CTD, vasculitis, graft-versus-host disease, pemphigus) (Lucendo et al., 2017). Natural history studies revealed that EoE is a chronic disease that significantly impacts on quality of life, including vitality and general health scores (van Rhijn et al., 2014a) and, if left untreated, results in continued inflammation (Dellon and Hirano, 2018) and complications such as strictures may develop (Schoepfer et al., 2013; Dellon et al., 2014b).
Although broad consensus has been achieved on first-line therapies (Dellon and Hirano, 2018), that involve proton pump inhibitors (PPIs), swallowed topical steroids and elimination diets (Figure 2), a subset of patients remains non-responder to standard therapy.
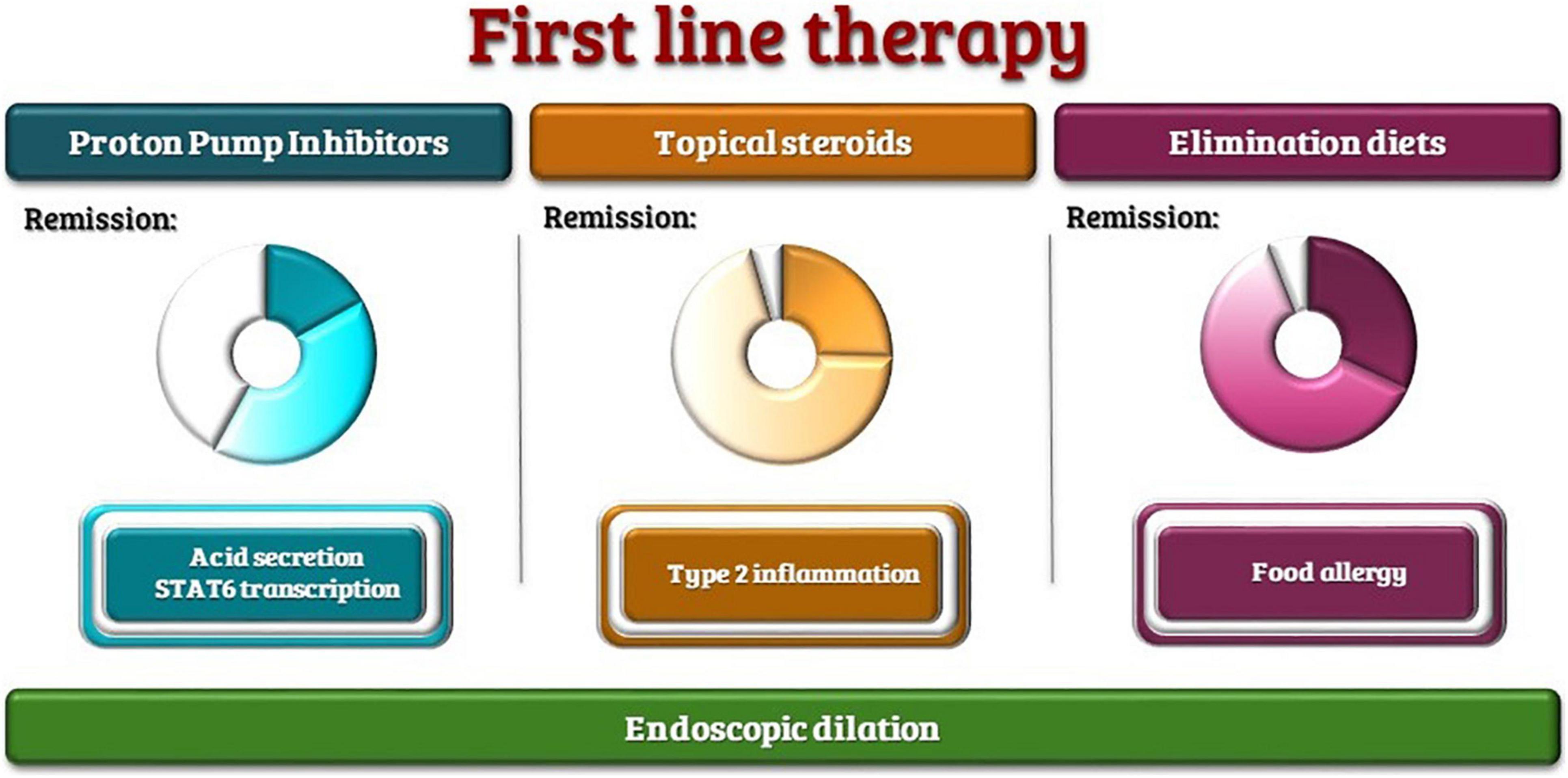
Figure 2. First-line therapies with the range of reported remission rates and therapeutic targets.
A deep understanding of the pathophysiology of this disease is pivotal for the development of new therapies.
The aim of this review is to provide a comprehensive description of the pathophysiology of EoE with a particular focus on therapeutic targets and results from previous therapeutic approaches in literature.
The pathogenesis of EoE is multifactorial and results from the complex, still mostly undefined, interaction between genetics and intrinsic factors, environment, and antigenic stimuli (Lim et al., 2011; Kottyan et al., 2014; Figure 3).
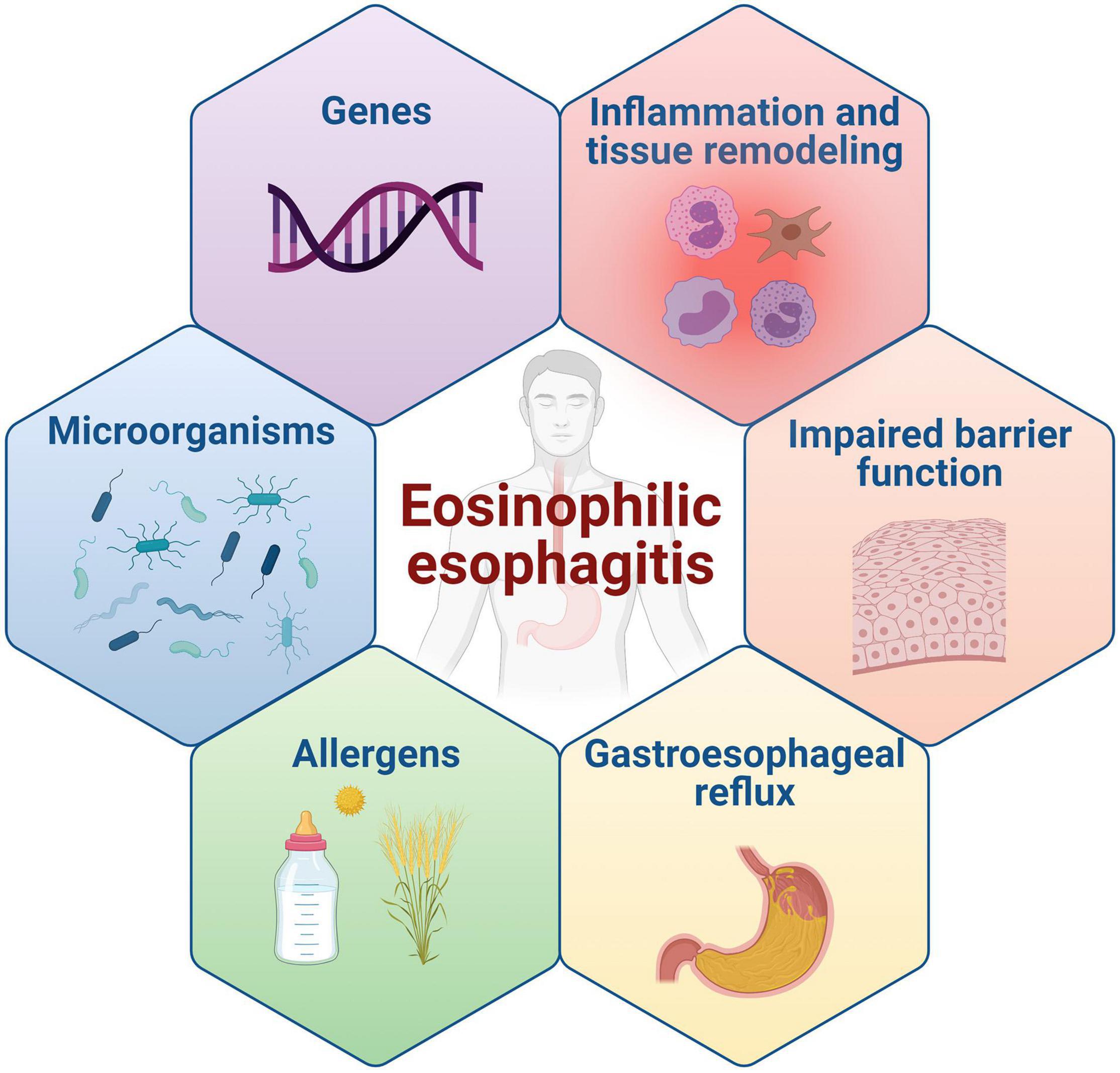
Figure 3. Main pathogenetic mechanisms of EoE.
Eosinophilic esophagitis occurs in family members in a non-Mendelian pattern, indicating a complex heritability (Straumann et al., 2016).
Male predominance, family history, twin concordance and genomewide association studies (GWAS) suggest that genetics contribute to the development of EoE (Alexander et al., 2014). Familial studies have identified a 44% concordance between monozygotic twins and 30% concordance in dizygotic twins, with familiarity proven in 7–10% of patients and a sibling recurrence ratio of 80/10.000 (Sherrill and Rothenberg, 2011; Guarino et al., 2016). The heritability risk is estimated to be 2% with a reported relative risk ratio for EoE in family members of 10–64, and is greater for male relatives (Alexander et al., 2014).
Candidate gene studies, GWAS and phenome-wide association studies (PheWas) identified multiple genes possibly contributing to the development; these include genes involved in the so-called “Type 2 (T2) inflammation” pathways, epidermal differentiation and barrier function. Interestingly, also some defects in mitochondrial function genes (dehydrogenase E1, and Dehydrogenase E1 and Transketolase Domain Containing 1 – DHTKD1) were associated with EoE (Henderson et al., 2014).
It should also be pointed out that many of these genetic loci were identified in other atopic diseases, including AD (c11orf30, filaggrin – FLG, desmoglein-1 – DSG-1, and serine peptidase inhibitor Kazal type 5 – SPINK5), asthma (Thymic stromal lymphopoietin – TSLP, c11orf30, C-C Motif Chemokine Ligand 26 – CCL26), allergic sensitization (TSLP, c11orf30, Signal Transducer and Activator Of Transcription 6 – STAT6) and allergic rhinitis (TSLP, c11orf30) (Doucet-Ladevèze et al., 2019; Lyles and Rothenberg, 2019).
Eosinophilic esophagitis inflammation presents all the hallmarks of a type 2 immunological response (Figure 4).
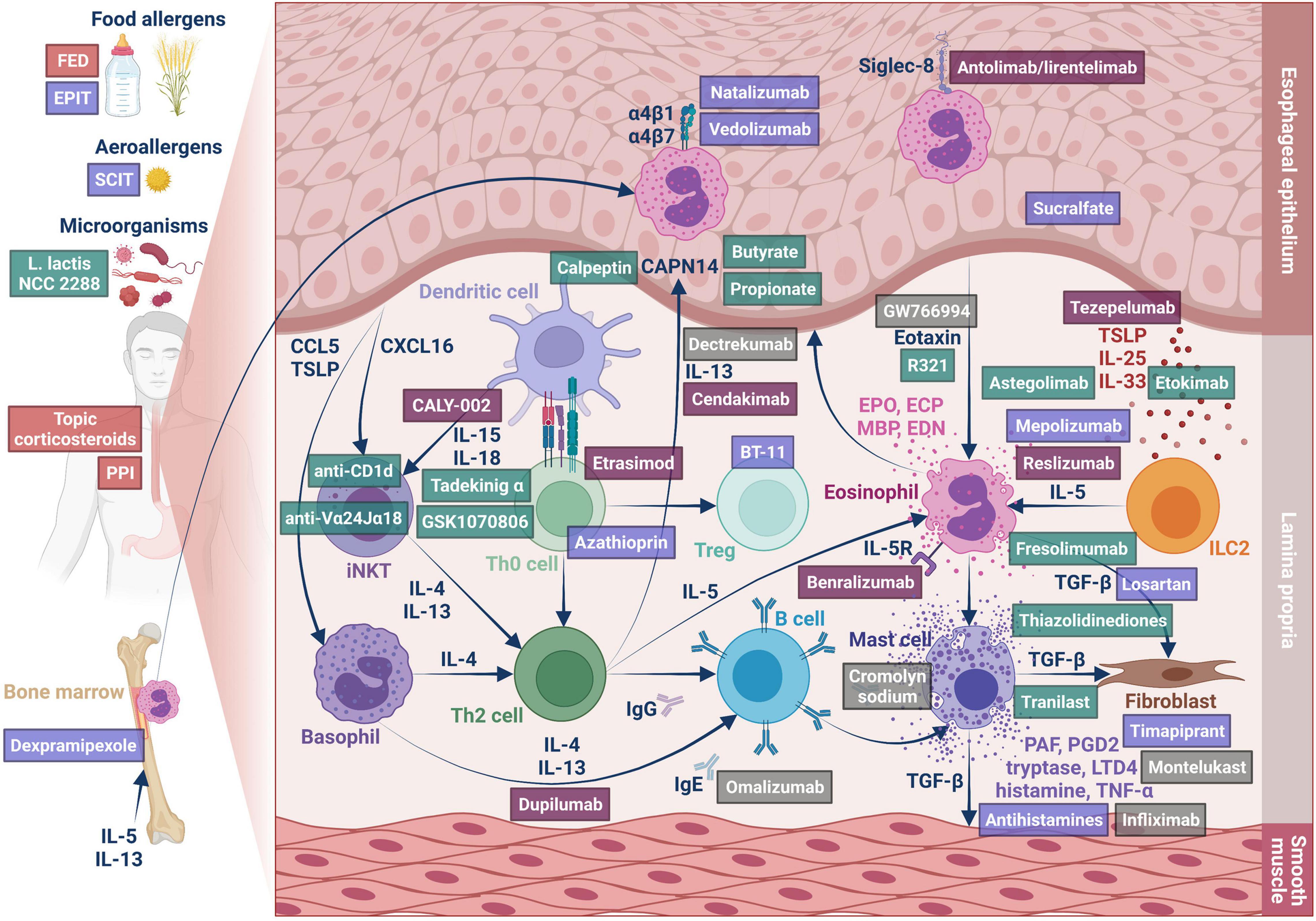
Figure 4. Type 2 inflammation in EoE. The figure represents the involved cells and mediators and the therapeutic approaches described in the review. The drugs are colored as follows: Red tag: first-line therapy, Plum tag: orphan drugs, Lilac tag: drugs with reported results on human patients, Green tag: drugs without reported results on human patients, Gray tag: drugs that failed to obtain significant results on human patients.
Following a still debated likely initial stimulus, epithelial and dendritic cells start to express epithelial-derived cytokines (the so-called “alarmins,” namely interleukin 25 – IL25, interleukin 33 – IL33, and TSLP), leading to homing and retention of immune cells, such as invariant natural killer T (iNKT) cells, adaptive CD4+ effector memory T-helper 2 (Th2) cells and innate lymphoid type 2 cells (ILC2) (Lexmond et al., 2014; Shukla et al., 2015).
Their activation, in turn, leads to the secretion of key cytokines, such as interleukins 13 (IL-13), 4 (IL-4), and 5 (IL-5), that ultimately lead to the migration of eosinophils to the esophagus and their degranulation with the release of many molecules responsible of tissue remodeling, as well as damage of the epithelial barrier.
Steroids represented the first treatment approach for EoE (Liacouras et al., 1998). Initially, systemic steroids were employed; however, topical steroids were subsequently proven equally effective, while sparing systemic adverse events (Faubion et al., 1998; Schaefer et al., 2008). Thus, systemic steroids are currently reserved for critical patients with severe dysphagia or significant weight loss (Gonzalez-Cervera and Lucendo, 2016; Lucendo et al., 2017). Swallowed topical corticosteroids, mainly fluticasone propionate and budesonide, currently represent one of the most effective first-line therapies for EoE in both children and adults (Navarro et al., 2021; Rokkas et al., 2021).
Glucocorticoid treatment reduces interleukin-13 transcription and the EoE transcriptome in vivo (Blanchard et al., 2007), reduces or even abolishes the eosinophilic infiltrate in 39–100% of patients (Hao et al., 2021), reduces T cell infiltration (Teitelbaum et al., 2002), downregulates mast cell associated genes (Hsu Blatman et al., 2011) and even decreases fibrosis (Aceves et al., 2010b) and restores esophageal motility (Nennstiel et al., 2016; Nakajima et al., 2017).
Swallowed topical steroids seem to be safe; the few adverse effects are superficial esophageal candidiasis (described in up to 10% of patients; it responds to specific treatment) and rarely adrenal axis suppression, bone demineralization, and diminished growth (Bagiella and Chehade, 2016).
Current research is focused on the development of formulations that enable optimal esophageal delivery (Racca et al., 2021).
Human esophageal mucosa consists of a multilayer squamous non-keratinized epithelium, which, together with the mucus layer, protects tissues from microorganisms and mechanical and chemical insults (Squier and Kremer, 2001).
Various assessments on esophageal tissues from patients with EoE have demonstrated the presence of an altered epithelial barrier function (van Rhijn et al., 2014c), with reduced transepithelial resistance and impedance (Katzka et al., 2015; Patel and Vaezi, 2017; Warners et al., 2017a,b). Histological characteristics comprehend dilated interepithelial spaces, basal cell hyperplasia (Mueller et al., 2006; Ravelli et al., 2006; Katzka et al., 2014), decreased desmosomes (Capocelli et al., 2015) and a profound loss of esophageal tissue differentiation (Rochman et al., 2017).
The principal factors involved in these alterations are the epidermal differentiation complex (EDC), FLG and Calpain (CAPN)14.
The EDC, on the 1q21 locus, is a cluster of genes involved in epithelial differentiation (South et al., 1999) and displays the most abundant dysregulation in the EoE transcriptome (Blanchard et al., 2010). EDC genes include FLG, involucrin, and many small proline-rich repeat (SPRR) family members (Blanchard et al., 2010).
Filaggrin encodes an intracellular protein involved in the aggregation of keratin filaments and interestingly, its dysfunction has been associated with AD (Fallon et al., 2009; O’Regan et al., 2009), a disease that frequently co-occurs with EoE.
Other downregulated junctional proteins in the esophageal mucosa of patients with EoE include E-cadherin, claudin-1 and 7 (Abdulnour-Nakhoul et al., 2013; Nguyen et al., 2018), zonulin-1 (Katzka et al., 2014), and desmoglein-1 (DSG1) (Sherrill et al., 2014a).
CAPN14 is an intracellular regulatory protease, member of the classical calpain subfamily, involved in the integrity of the esophageal epithelial barrier. This protease is exclusively expressed in the esophageal mucosa (Sleiman et al., 2014; Kottyan et al., 2021) and is dynamically regulated by IL-13 (Kottyan et al., 2014). Higher levels of CAPN14 expression, such as seen in active EoE (Sleiman et al., 2014; Kottyan et al., 2021), are associated with the downregulation of DSG1, FLG, and zonulin, all involved in epithelial barrier function (Sleiman et al., 2014). Proteases also seem to play a role in EoE. Serine protease inhibitors (SERPINs), serine protease inhibitors, Kazal type (SPINKs) and Kallikrein serine peptidases (LRRC31) have been shown to be dysregulated in EoE (D’Mello et al., 2016; Rochman et al., 2017; Azouz et al., 2018, 2020), potentially contributing to epithelial damage.
It is still debated whether these alterations might be a cause or a consequence of EoE. Usually, food allergens are large molecules, with a molecular weight between 3 and 90 kDa, and are unable to cross the healthy esophageal epithelium. It has been postulated that altered epithelial permeability could lead to a permissive environment that facilitates contact between antigens and the immune system leading to the development of inflammation, but it can also be considered a consequence of esophageal inflammation.
On one side, eosinophil products have a known cytotoxic effect. Moreover, IL-13 and transforming growth factor β1 (TGF-β1), key cytokines in EoE, impact epithelial differentiation and cellular junction formation, downregulating EDC expression (Blanchard et al., 2010). Of note, treatment with FEDs or steroids has shown to reverse FLG downregulation (Politi et al., 2016).
Moreover, Major Basic Protein (MBP) and TGF, secreted by eosinophils (Gleich et al., 1979), promote extracellular matrix damage by increasing mast cells’ secretion of proteolytic enzymes, such as tryptase and chymase.
However, about 2% of EoE transcriptional alterations do not resolve upon disease remission (Blanchard et al., 2007) with persistence of dysregulations of cadherin-like 26 (CDH26), uroplakin 1B (UPK1B), periostin (POSTN), and DSG1, all involved in epithelial homeostasis (Blanchard et al., 2007).
Moreover, multiple genetic variants in epithelial barrier-related genes have been associated with an increased risk of developing EoE in life. These include two coding variants in FLG gene (R501X and 2282del4), associated with EoE irrespective of atopic status (Blanchard et al., 2010), a genetic risk locus located on chr19q13.11 that encodes several genes (ANKRD27, PDCD5) involved in apical transport in esophageal epithelial cells, wound healing (Tamura et al., 2011; Fukuda, 2016), transcriptional regulation, DNA damage response, and cell cycle control (Li et al., 2016), a variant in the 10p14 locus in an intron of Inter-α-trypsin inhibitor heavy chain 5 (ITIH5), a gene that encodes for a serine protease inhibitor and has been also linked to eosinophilic granulomatosis with polyangiitis (Kottyan et al., 2021), and a locus on chr2p23.1, involving the CAPN14 gene, was found to be highly associated with EoE in multiple studies (Kottyan et al., 2014, 2021; Sleiman et al., 2014).
Moreover, a Mendelian association was found between EoE and SAM syndrome, caused by homozygous mutations in DSG1 (Ryu et al., 2020), and Netherton syndrome, caused by autosomal dominant loss-of-function mutations in the protease inhibitor SPINK5 leading to unrestricted protease activity of KLK5 and KLK7 (Paluel-Marmont et al., 2017). Indeed, a murine model of EoE induced by epicutaneous ovalbumin (OVA) sensitization has pointed out that topical allergen application on unstripped skin induced experimental EoE in FLG-deficient mice but not in wild-type control mice (Venturelli et al., 2016).
There is scarce literature regarding epithelial barrier-targeted treatments in EoE.
Sucralfate, the aluminum salt of sucrose sulfate, is a known “cytoprotective” agent whose mechanism of action supposedly consists in the protection of eroded areas, induction of prostaglandin production and increase of growth factors bioavailability, leading to improved vascular flow and mucus production (Masuelli et al., 2010). This compound has also been shown to reduce the permeability of esophageal mucosa to hydrogen ions (Orlando and Powel, 1984), which elicited its proposal as a potential therapy for EoE. An early phase 1 clinical trial (NCT02353078) on the effect of sucralfate is listed as completed in 2016 on Clinicaltrials.gov1 but no result or publication is available so far.
Butyrate and propionate, short chain fatty acids (SCFAs) produced by microbial macronutrients fermentation, able to modulate host immune responses and human dendritic cell (DC) function, recently demonstrated in vitro capacity of reversing IL-13-driven impairment of esophageal epithelial barrier upregulating FLG and DSG1 expression and reducing CCL26 and CAPN14 expression (Kleuskens et al., 2021). However, no in vivo study is available.
Finally, in a recent study of an asthma mouse model, inhibition of CAPN by calpeptin was able to strongly reduce bronchial reactivity, bronchoalveolar lavage (BAL) fluid eosinophilia, subepithelial fibrosis and the expression of IL-4, IL-5, IL-13, TGF-β1, and ova-specific immunoglobulin E (Aich et al., 2012), suggesting its therapeutic potential in EoE.
The role of gastroesophageal reflux disease (GERD) in the pathogenesis of EoE is to date controversial. It is now universally accepted that the two diagnoses are not mutually exclusive and, despite their coexistence might be unrelated and due to the high prevalence of GERD in the general population, it has been suggested that the two diseases might have a more complex relationship (Spechler et al., 2007).
On one side, GERD can increase the permeability of the esophageal epithelium to food allergens (Votto et al., 2020) and promote inflammation and eosinophil recruitment (Tobey et al., 2004; Untersmayr and Jensen-Jarolim, 2006). On the other hand, the products of eosinophilic inflammation can reduce esophageal clearance by affecting smooth muscle contraction and esophageal compliance.
It is long known that GERD, both basic and acid, can stimulate squamous epithelial cells to produce eosinophil chemoattractants, such as IL-8 and RANTES (Regulated upon Activation Normal T cell Expressed and Secreted), leading to a mild esophageal eosinophilia (Winter et al., 1982; Isomoto et al., 2003). In vitro acid exposure upregulates eotaxins 1, 2, and 3 and macrophage inflammatory protein 1a (MIP-1a) (Ma et al., 2012) by esophageal squamous epithelial cells, promoting eosinophil recruitment (Luster and Rothenberg, 1997).
Eosinophils, on the other hand, produce vasoactive intestinal peptide (VIP) and IL-6 which reduce lower esophageal sphincter (LES) tone and weaken esophageal muscle contraction predisposing to reflux (Cao et al., 2004, 2006; Sarbinowska and Wasko-Czopnik, 2020). About 25–76% of EoE patients present esophageal motility abnormalities (van Rhijn et al., 2014b; Nennstiel et al., 2016; Spechler et al., 2018), mainly hypo-contractile abnormalities such as ineffective esophageal motility, absent contractility, hypotensive LES (van Rhijn et al., 2014b).
Post reflux swallow-induced peristaltic wave (PSPW), an index of esophageal chemical clearance, is reduced in EoE patients. Proton pump inhibitors (PPI) treatment improved all reflux parameters in PPI-responsive patients, including PSPW. In contrast, in PPI-unresponsive patients, PPI treatment improved all reflux parameters except for PSPW (Frazzoni et al., 2019).
Moreover, eosinophils secrete profibrotic products (such as MBP, TGF-β, IL-13, VEGF, and IL-8) that can induce tissue remodeling, interfering with lower esophageal sphincter function and peristalsis (Cheng et al., 2012).
Gastroesophageal reflux disease patients also display esophageal barrier alterations similar to EoE patients, such as dilated intercellular spaces (DISs), basal cell hyperplasia (Zentilin et al., 2005), and tight junction proteins alterations (e.g., claudin-1) (Vieth et al., 2016).
PPIs are an established first-line therapy for EoE, with a reported efficacy in 50% of pediatric and adult patients (Lucendo et al., 2016). However, beyond their blocking effect of gastric acid secretion, PPIs have demonstrated an anti-inflammatory effect on STAT6 (Molina-Infante et al., 2014) and will be therefore treated in the correspondent paragraph.
No other anti-reflux therapy has been tested on EoE to our knowledge.
Natural history studies revealed that, in line with other eosinophilic inflammatory conditions, patients whose inflammation is not controlled risk a gradual shift toward fibrosis (Schoepfer et al., 2013; Dellon, 2014).
Fibrotic remodeling occurs in both pediatric (Aceves et al., 2007; Chehade et al., 2007) and adult (Straumann et al., 2010a; Lucendo et al., 2011a) EoE patients. The persistence of activated fibroblasts was reported even after disease remission (Nhu et al., 2020).
IL-13, IL-4, IL-5, eotaxin-3, periostin, and TGFB1, together with eosinophils products like MBP, all have a role in tissue remodeling (Li-Kim-Moy et al., 2011; Schoepfer et al., 2013; Dellon et al., 2014b).
FGF9, CCL18, and Matrix metalloproteases (MMPs) are other important factors in fibroblast activation and extracellular matrix deposition (Lucendo et al., 2011a; Beppu et al., 2015).
Epithelial-mesenchymal transition (EMT), a process in which epithelial cells lose typical epithelial characteristics acquiring myofibroblasts’ functions, was suggested to play a major role in fibrosis (Kalluri and Weinberg, 2009). This process increases the number of activated fibroblasts and myofibroblasts involved in the extracellular matrix production (Kalluri and Weinberg, 2009; Roman et al., 2010; Kagalwalla et al., 2012; Muir et al., 2013) and can be induced by TGF-β, MMP-9, IL-13, and MBP released by eosinophils or damaged epithelium (Zeisberg, 2008; Kagalwalla et al., 2012).
Therapeutic approaches aimed at remodeling are targeted to the individual effectors and will be treated in individual paragraphs.
Several lines of evidence support the theory of EoE as an allergen-driven disease.
The concept of EoE as a food antigen-triggered disorder was initially based on the finding that, in children, feeding with elemental formula caused histologic remission (Kelly et al., 1995). This conception was then confirmed by the efficacy of FEDs, together with reports of onset of EoE in 2.7% of patients undergoing oral immunotherapy for food allergy desensitization (peanut, milk, egg) with subsequent resolution after suspension (Lucendo et al., 2014; Nilsson et al., 2021; Wright et al., 2021). Some other less repeated but interesting studies reported the presence of gluten deposits in esophageal surface of adult patients (Marietta et al., 2017), the presence of T killer cells able to recognize lipids and produce IL-4 and IL-13 after stimulation with cow milk lipids in patients with active EoE (Jyonouchi et al., 2013) and Th2 cells with CD154 + IL5 + phenotype in the peripheral blood of active EoE patients (but not in control atopic patients or inactive EoE patients) that can be stimulated by milk antigens in milk-induced EoE patients (Cianferoni et al., 2018).
Lately, a novel syndrome, referred to as “food-induced immediate response of the esophagus” (FIRE), consisting in an unpleasant or painful sensation, unrelated to dysphagia, occurring immediately after esophageal contact with specific foods, was observed in EoE patients and theorized to derive from a different, still undefined, physiopathological mechanism (Biedermann et al., 2021).
Food elimination diet (FED) therapy is today a recognized first-line therapy for EoE.
This approach’s efficacy depends on the extension of eliminated food antigens.
The elemental diet is now known to be efficacious in both children (Markowitz et al., 2003) and adults (Peterson et al., 2013; Warners et al., 2017c), leading to remission in around 70–90% of patients (Arias et al., 2014) and outperforms all other dietary-based strategies. However, its use in clinical practice is inhibited by the poor palatability (Liacouras et al., 2005), psycho-social impact (Franciosi et al., 2012; Slae et al., 2015), cost and developmental impact (Delaney and Arvedson, 2008) and is now used only in refractory patients or as a short-term approach to rapidly induce remission, especially in children (Arias and Lucendo, 2014; Mukkada and Furuta, 2014).
The empiric elimination of the six most common food allergens (cow’s milk proteins, wheat, egg, soy, peanut, fish/seafood) has a reported efficacy in around 70% of pediatric patients and 50% of adult patients (Kagalwalla et al., 2006; Arias et al., 2014; Philpott et al., 2016) but should be followed by sequential reintroduction of foods with repeated endoscopy and biopsies to identify the specific food or foods triggering EoE in each patient. Some reduced empiric diets eliminating 4 (milk, wheat, egg, and soy) (Kagalwalla et al., 2017), two foods (milk and gluten) or one food with a step-up approach in non-responders have been proposed (Molina-Infante et al., 2018a). FEDs based on skin prick test and atopy patch test were reported to lead to remission a high portion of patients in some studies (Spergel et al., 2012a; Terrados et al., 2020), but a sequent meta-analysis showed an overall efficacy of 45.5% and are not currently recommended, together with approaches based on basophil activation tests, serum food-specific IgG, component-resolved diagnosis and esophageal prick tests (van Rhijn et al., 2015; Philpott et al., 2016; Warners et al., 2018).
Recently, a combination of a peripheral blood CD4 + T-cell proliferation assay and food-specific tissue IgG4 levels was reported reduce median peak eosinophil counts but a low histologic remission rate (21%) (Dellon et al., 2019b).
Epicutaneous immunotherapy (EPIT) is an emerging treatment for food allergy (Bégin et al., 2021). A pilot study on pediatric patients with milk-induced EoE treated with EPIT found no significant difference between groups for the maximum eosinophil count at the end of the study. However, when only the subset of patients without major protocol deviations was selected, a significant reduction in eosinophil count was reported, with a 47% remission rate (<15 eosinophils/HPF) and a 36% deep remission rate (<5 eosinophils/HPF) (Spergel et al., 2020), that persisted after 2 years (Spergel et al., 2021).
The association of EoE with allergic rhinoconjunctivitis and asthma and especially the high prevalence of concurrent sensitization to aeroallergens (Capucilli et al., 2018), together with repeated reports of seasonal exacerbations of the disease (Fogg et al., 2003; Almansa et al., 2009; Ram et al., 2015; Reed et al., 2019), have raised the idea that aeroallergens could have a causative role in EoE.
Indeed, murine models using Aspergillus fumigatus, cockroach, or dust mite antigen demonstrate that aeroallergens can cause esophageal eosinophilia (Mishra et al., 2001; Rayapudi et al., 2010). Moreover, aeroallergens can induce EoE in humans when administered in the form of sublingual immunotherapy (Miehlke et al., 2013; Rokosz et al., 2017; Fujiwara et al., 2021) and house mites’ antigens have been found in the esophageal mucosa of EoE patients (Ravi et al., 2019), but the topic has not been further investigated.
Some case reports and small series report the efficacy of subcutaneous immunotherapy for aeroallergens in EoE resolution (De Swert et al., 2013; Iglesia et al., 2021) but no clinical trial has been reported.
The finding that premature delivery, cesarean birth, early antibiotic exposure, lack of breastfeeding and lack of early microbial exposure are risk factors for the development of EoE (Radano et al., 2014; Jensen and Dellon, 2018) has revived the idea of the Hygiene Hypothesis also in EoE (Mennini et al., 2021).
Indeed, Helicobacter pylori infection, known to increase Th1 and Th17 response, thus reducing Th2-skewing (Shi et al., 2010), has been linked to a reduction in the chance of developing EoE in many, mostly retrospective, studies (Furuta et al., 2013; Shah et al., 2019). However, the data has not been confirmed by a prospective study involving a large number of children (Molina-Infante et al., 2018b).
On the contrary, herpes simplex virus infection might trigger EoE in immunocompetent adults and children (Squires et al., 2009; Žaja Franulović et al., 2013; Fritz et al., 2018).
The oral and esophageal microbiota in patients with EoE has also been studied and results report a shift from a normally predominantly Gram-positive population (Streptococcus spp. and Atopobium spp.) to an increase in Gram-negative Haemophilus spp. and Proteobacteria (Neisseria spp. and Corynebacterium spp.) (Yang et al., 2009; Benitez et al., 2015; Hiremath et al., 2019). However, the difference was not significant between active and non-active EoE in most studies, and it is still unknown if the alteration could have a causative role or represent just a consequence of the altered microenvironment in this disease.
A single study on a murine model elicited by epicutaneous sensitization with Aspergillus fumigatus protein extract, reported a significant decrease of esophageal eosinophilia after supplementation with Lactococcus lactis NCC 2287, a strong inducer of the immunomodulatory cytokine IL-10 and an inhibitor of the eosinophil survival cytokine IL-5 (Holvoet et al., 2016). However, this effect was noticeable only when L. lactis was used after induction of the inflammation, and not when administered as a preventive strategy. No further studies were found on the subject.
Eosinophils are the hallmark of EoE.
They present receptors for eotaxin-1, -2, -3, RANTES, MIP-1α, MCP-2, -3, -4, and lipid mediators like Platelet Activating Factor (PAF), Leukotriene B4 (LTB4) and C4 (LTC4) (Shukla et al., 2015) and, upon activation, release cationic granule proteins, reactive oxygen species, lipid mediators, enzymes, growth factors and cytokines, largely responsible for the esophageal modifications seen in EoE.
Eosinophilic peroxidase (EPO), eosinophil cationic protein (ECP), and MBP have cytotoxic effects on the epithelium (Talley et al., 1992) and, together with EPO products (hydrogen peroxide and halide acids) and superoxide generated by the respiratory burst oxidase enzyme pathway (Talley et al., 1992; Reed et al., 2019), contribute to mucosal barrier impairment.
Eosinophils can alter esophageal motility through multiple mechanisms: MBP directly causes vagal muscarinic M2 receptor dysfunction, thus increasing smooth muscle reactivity (Lewis et al., 1990), and, together with TGF-β1, can lead to smooth muscle hyperplasia and hypercontractility; leukotriene D4, prostaglandin F2 alpha, and thromboxane B2 can cause contraction of esophageal muscle (Daniel et al., 1979; Kim et al., 1998; Rosenberg et al., 2013), while IL-6 and IL-13 reduce its amplitude (Rieder et al., 2014). Moreover, eosinophil-derived neurotoxin (EDN) and ECP have ribonuclease activity, toxic for neurons (Gleich et al., 1993).
MBP, TGF-β, IL-13, VEGF and IL-8 are also major factors contributing to EMT, remodeling and fibrosis (Zeisberg, 2008; Cheng et al., 2012; Kagalwalla et al., 2012).
Eosinophils stimulate inflammatory cell recruitment and activation of mast cells, basophils, T cells, fibroblasts, all involved in EoE pathophysiology, and can even act as antigen-presenting cells (Gleich et al., 1993; Mulder et al., 2008; Davis and Rothenberg, 2013).
They can produce IL-1, IL-3, IL-4, IL-5, IL-13; GM-CSF; TGF-β; tumor necrosis factor-α (TNF-α); RANTES (regulated on activation, normal T cells expressed and secreted); macrophage inflammatory protein 1 (MIP-1); and eotaxin (Klion et al., 2020), whose activity will be treated separately.
Benralizumab is a fully humanized afucosylated anti-human IL5-Rα antibody approved for severe asthma (Bleecker et al., 2016; FitzGerald et al., 2016). Its mechanism of action consists in recognition of the IL-5Rα subunit of the IL-5 receptor and activation of FcγRIIIa receptor on natural killer cells, thus rapidly depleting eosinophils (Kolbeck et al., 2010; Laviolette et al., 2013). A randomized, double-blind, placebo-controlled clinical trial (NCT03473977) to evaluate the efficacy of benralizumab in adults and adolescents with EG has recently been concluded,2 but the results have not yet been published. Results available in Clinicaltrials.gov report a significantly higher rate of histological remission (77%) vs. placebo (8%), and an improvement in the histologic score with non-significant improvement in endoscopic score and symptoms, in the absence of serious adverse events (SAE), while no statistical analysis is available on non-serious adverse events (AEs).
An ongoing phase 3 trial (NCT04543409) is currently assessing its efficacy in adult and adolescent EoE patients.3
Of note, in August 2019, the US Food and Drug Administration (FDA) has granted Orphan Drug Designation to benralizumab for the treatment of EoE.4
Dexpramipexole is the enantiomer of pramipexole, a dopamine agonist. During a clinical trial in amyotrophic lateral sclerosis patients, dexpramipexole unexpectedly reduced peripheral absolute eosinophil count (Dispenza and Bochner, 2018), most likely by induction of maturational arrest specific to the eosinophil lineage (Panch et al., 2018). A subsequent study to evaluate dexpramipexole as a steroid-sparing agent in hypereosinophilic syndrome showed efficacy in 40% of patients (Panch et al., 2018). Interestingly, two responders with gastrointestinal eosinophilia (a woman with esophageal and duodenal involvement and a man with gastric, duodenal and colonic involvement) showed complete resolution of tissue eosinophilia and symptom improvement at week 24 and 12, respectively. One SAE (a grade 1 squamous cell cancer of the skin in one subject) was reported, together with some minor AE in all patients, with central and/or peripheral nervous system–related symptoms such as insomnia (40%) and dizziness (30%) being the most common. Mood swings, palpitations, and skin rash were also noted in 20% of participants. No active trial is currently ongoing on EoE.
An increased mast cell number, infiltrating all layers of the esophagus, has been consistently observed in EoE (Nicholson et al., 1997; Straumann et al., 2001; Aceves et al., 2010a; Niranjan et al., 2013).
More recent microarray analysis of EoE tissues confirmed this finding, showing upregulation of many mast cell–associated genes, such as those that encode carboxypeptidase 3A (CPA3), FcεR-I, and tryptase (TPSAB1) (Mulder et al., 2012).
Moreover, mast cell number and the expression level of mast cell proteases in mucosal biopsies of EoE patients correlate with symptom score, contrarily to eosinophil number (Otani et al., 2013).
The tissue mast cell content usually lessens in response to FEDs, topical corticosteroids (Aceves et al., 2010a) and anti-IL-5 therapy (Otani et al., 2013). However, the persistence of an elevated mast cell number despite resolution of esophageal eosinophilia has been linked to persistence of endoscopic abnormalities and symptoms (Bolton et al., 2020).
Similarly to eosinophils, mast cells produce numerous pro-inflammatory cytokines and molecules showing activity on the epithelial barrier and esophageal motility. In fact, beyond their known role in the T2 cascade, mast cells are capable of causing smooth muscle hypertrophy (Elieh Ali Komi and Bjermer, 2019) and release mediators such as tryptase, leukotrienes, prostaglandins, platelet-activating factor, tumor necrosis factor (TNF)-α, 5- hydroxytryptamine and histamine that can induce smooth muscle contraction (Goyal and Rattan, 1978).
Cromolyn sodium or disodium cromoglicate is a mast cell stabilizer from the chromones class, able to suppress activation and degranulation by inhibiting calcium ion influx. Although animal model studies based on subcutaneous OVA sensitization followed by oral challenge showed some effects on eosinophilic and mast cell influx, collagen deposition, mast cell activation and Th2 immune response (Silva et al., 2020), a small randomized, double-blinded, placebo-controlled study of the use of viscous oral cromolyn sodium in children with EoE found no effect on eosinophilic infiltrate and symptoms (Lieberman et al., 2018).
Invariant natural killer T cells are a subset of lymphocytes that recognize lipid and glycolipid antigens presented on CD1d molecules, can produce type 2 cytokines and have been postulated to play a pathogenic role in EoE and some other atopic diseases (Bendelac et al., 2007).
In animal models, activation of iNKT by their specific agonist is sufficient to induce EoE (Rayapudi et al., 2014).
Indeed, increased esophageal iNKTs have been repeatedly reported in EoE pediatric and adult patients, especially in the active state of the disease (Jyonouchi et al., 2013; Rayapudi et al., 2014) and in early-onset patients (Lexmond et al., 2014). This esophageal increase is associated with a reduction of peripheral blood iNKTs (Upparahalli Venkateshaiah et al., 2021). This could be explained by iNKT cells homing in the tissue via receptor CXCR6 and esophageal epithelial cells have been described as the source of CXCL16 (Rayapudi et al., 2014).
Interestingly, iNKTs from patients with active EoE expand more readily and produce more IL-13 in response to cow milk-derived sphingomyelin (Jyonouchi et al., 2013), thus suggesting a possible role of iNKT in food allergen recognition.
Invariant Natural Killer T cells neutralization via anti-mCD1d or anti-hVα14Jα18 antibodies protected against the development of EoE in a murine model based on intranasal peanut and Aspergillus sensitization (Upparahalli Venkateshaiah et al., 2021). Consequently, iNKT cell neutralization by humanized anti-CD1d and anti-Vα24Jα18 antibodies has been suggested as a potential therapy for human EoE but no studies on humans been proposed yet.
T cells are an important constituent of EoE inflammatory milieu (Straumann et al., 2001; Teitelbaum et al., 2002; Blanchard, 2006; Lucendo et al., 2007). Studies on EoE biopsies describe an elevation in both CD4+ and CD8+ T cell numbers and an increase in the CD8+ T cell/CD4+ T cell ratio (Teitelbaum et al., 2002; Lucendo et al., 2007).
Th2 cells play an important role in the chemotaxis of eosinophils and initiation of the T2 cytokine cascade.
Th2 cells similar to those found in AD and EGE, producing IL-13- and IL-5 and expressing CD161 and hematopoietic prostaglandin D synthase, were detected in EoE patients (Mitson-Salazar et al., 2016).
Moreover, Th2 cells with CD154 + IL5 + phenotype were found in the peripheral blood of active EoE patients but not in the control atopic patients or inactive EoE patients. Further, these peripheral T cells could be stimulated by milk antigens in milk-induced EoE patients but not in control patients (Cianferoni et al., 2018).
In addition, a significantly higher number of stimulated CD3 + CD8 + T cells, able to produce TNF-α and interferon (IFN)-γ was described in active EoE (Sayej et al., 2016).
T cells in EoE patients are also able to express the TNF-related cytokine LIGHT (TNF superfamily member 14), which can induce an inflammatory phenotype in fibroblasts (Manresa et al., 2020).
Regulatory T cells (Tregs), another subset of T lymphocytes, are critical in preventing and controlling many autoimmune and allergic diseases. The esophageal tissue of adult EoE patients shows reduced Tregs and this finding is not modified by steroid therapy (Stuck et al., 2011). In contrast, pediatric patients display a relative increase of these cells (Tantibhaedhyangkul et al., 2009; Fuentebella et al., 2010).
Recently, two cellular CD4+ populations called T7 (likely deregulated Treg) and T8 (likely deregulated Th2 cells), not able to suppress the adaptive response and Th2 cytokine production, were described in EoE patient’s esophageal tissue (Wen et al., 2019).
Azathioprine or 6-mercaptopurine, a purine analog, has been reported to induce clinical and histological remission in steroid-refractory adult and pediatric EoE patients in some case reports (Netzer et al., 2007). Common side effects include allergic reactions, pancreatitis, bone marrow suppression, nausea and infections.
BT-11 (piperazine-1,4-diylbis((6-(1H-benzo[d]imidazol2-yl)pyridin-2-yl)methanone) dihydrochloride), an oral, gut-restricted, small molecule that activates lanthionine synthetase C-like 2 (LANCL2) (Leber et al., 2019), has demonstrated to be able to lead to an increase in number and function of regulatory CD4 + T cells (Tregs) in Inflammatory bowel disease (IBD) and is programmed to be tested in EoE patients in a phase Ib study (NCT04835168) planned to start in January 2022.5
The epithelium plays an important role in EoE inflammation.
Esophageal epithelial cells express toll-like receptors (Lim et al., 2009; Mulder et al., 2011) and produce pro-inflammatory cytokines and lipid mediators in response to both pathogen-associated and danger-associated molecular patterns (Straumann et al., 2001; Fillon et al., 2009; Lim et al., 2009).
Epithelial cells of EoE patients can also produce alarmins (TSLP, IL-25, and IL-33), RANTES (CCL5), a chemotactic factor for T cells, eosinophils, and basophils (Jyonouchi et al., 2013), and CXCL16 (Lexmond et al., 2014), a chemotactic factor for iNKT cells. Moreover, the esophageal epithelium is the main source of eotaxin-3 production following IL-13 stimulation (Blanchard, 2006). In addition, epithelial cells can act as non-professional antigen-presenting cells (APCs) (Mulder et al., 2011).
Therapeutic approaches are targeted at the individual cytokines and will be treated in the relative paragraphs.
Innate lymphoid cells (ILC2s) are tissue resident cells that express prostaglandin D2 receptor 2 (CRTH2) and, following IL-33 and TSLP signaling, can produce type 2 cytokines (Mjosberg et al., 2011; Christianson et al., 2015; Doherty et al., 2015).
A single study (Doherty et al., 2015) showed their presence in active EoE biopsies, especially in PPI unresponsive patients, as well as a correlation between ILC2 and eosinophil number.
No ILC2-targeted therapeutic approach has been found in literature.
Basophils can secrete various type 2 cytokines and act as APCs (Voehringer, 2013).
An increased number of basophils has been reported by multiple studies in EoE (Noti et al., 2013; Iwakura et al., 2015). In particular, this population develops in presence of TSLP (Siracusa et al., 2011) and expresses high levels of IL-4 (Noti et al., 2013) and the IL-33R (Siracusa et al., 2011).
No basophil-targeted therapeutic approach has been found in literature.
Interleukin (IL)-4 and IL-13 share their alpha-chain and their receptor, but also activate specific receptors. They are known to initiate T2 immune response by inducing skewing of naive Th cells into Th2 cells, class switching to IgE production in B cells and macrophage maturation toward the M2 subpopulation, increasing dendritic cells activity, and activating and recruiting eosinophils (Blanchard et al., 2007).
These two cytokines can be produced in EoE patients by TSLP-elicited basophils, Th2 cells, Tc2 cells, iNKT, eosinophils, mast cells, activated fibroblasts and epithelial cells (Straumann et al., 2001; Lucendo et al., 2008; Zhu et al., 2010).
IL-13 and IL-4 signaling utilizes the JAK-STAT pathway, in particular STAT6 (Shukla et al., 2015), leading to eosinophilic recruitment (CCL26/eotaxin-3 gene) and downregulation of the EDC (cAPN-14 and SPINK7 genes) (Zeisberg, 2008; Kagalwalla et al., 2012).
IL-13 is currently recognized as a major effector cytokine in EoE, while IL-4 is less abundant (Blanchard et al., 2007). In a murine model, intratracheal IL-13 administration was able to induce EoE in a STAT6-dependent way, with a contribution of IL-5 and eotaxin (Mishra and Rothenberg, 2003). As a confirmation, PheWas studies have described that IL-13 polymorphisms are common in EoE (Blanchard et al., 2007, 2010). IL-13 is overexpressed in the esophageal mucosa of EoE patients (Blanchard et al., 2010), induces a gene transcript profile similar to the EoE-specific esophageal transcriptome (Kc et al., 2015), and has effects on eosinophil recruitment, esophageal barrier function, and tissue remodeling (Blanchard et al., 2007; Brightling et al., 2010; Zuo et al., 2010; Sherrill et al., 2014a).
In particular, IL-13, by inducing the expression of adhesion molecules such as VCAM-1 and ICAM-1 on blood vessels, facilitates the release of eosinophils from the bone marrow and induces the production of IL-5 by T and B cells, thus contributing to eosinophils homing and survival (Klion et al., 2020).
IL-13 also has a role in tissue remodeling: it promotes epithelial hyperplasia, collagen deposition and angiogenesis (Zuo et al., 2010) and, together with TGF-β1, activates quiescent fibroblasts to transdifferentiate into myofibroblasts and reduce the amplitude of esophageal muscle contraction (Rieder et al., 2014).
Interleukin-4 and Interleukin-13 as Therapeutic Targets. Two monoclonal antibodies targeting circulating IL-13 (dectrekumab and cendakimab) and a monoclonal antibody targeting the IL4/IL13 receptor (dupilumab) have been tested in patients with EoE.
Dectrekumab (QAX576), a fully human anti-IL-13 mAb, was the first anti-IL-13 therapy used on EoE patients. It received Orphan Drug Designation status from the FDA6 and EMA7 in 2013. A double-blind, placebo-controlled study on 23 adults showed improvement in symptoms, esophageal eosinophilia (60% improvement in treated patients versus 23% improvement in the placebo group), and disease-related transcripts. In particular, the expression of eotaxin-3, periostin and markers of mast cells and barrier function were reduced (Rothenberg et al., 2015). However, no patient achieved histological remission. Importantly, the effects of this drug (including the number of intraepithelial eosinophils and gene expression profiles) persisted for 6 months after treatment discontinuation, suggesting a potential role of this medication in combination therapies. No significant AE was reported. Nevertheless, the study of this drug in EoE has since then been discontinued.
Cendakimab RPC4046/CC-93538 is a recombinant, humanized, monoclonal antibody that inhibits binding of IL-13 to both IL-13Rα1 and IL-13Rα2 receptors (Tripp et al., 2017; Muir et al., 2019). Cendakimab received Orphan Drug Designation status from the FDA in 2015.8 A 16-week, double-blind, placebo-controlled, phase 2, multicenter study in adults with active EoE showed the ability of this drug to significantly reduce eosinophil counts, with a partial remission rate of 50% and a deep remission rate of 25% (Hirano et al., 2019). Macroscopic esophageal appearance improved as well; however symptomatic improvement was not significant. Of note, symptomatic improvement was best achieved in patients with steroid-refractory disease. AE rates were not different from the placebo group. However, four patients discontinued the drug due to dizziness, influenza-like illness, pruritus and rash, and worsening of EoE symptoms.
In a longer (52-week) open label study a prolonged symptomatic and histological improvement was initially briefly described (Dellon et al., 2019a). The recent publication (Dellon et al., 2021) reports that most patients maintained responses through week 52, with an improved symptom remission rate and an induction of remission in 36% of previously non-responding patients. The tolerability of the drug was confirmed, the most commonly reported AEs being upper respiratory tract infections, nasopharyngitis, sinusitis and headache, mainly in the induction period.
A phase 3, placebo-controlled induction and long-term study (NCT04753697) in adult and adolescent subjects is currently ongoing.9
Dupilumab is a IL4/IL13 receptor antagonist, at present approved for the treatment of severe forms of AD, asthma and nasal polyposis (Blauvelt et al., 2017). Dupixent received Orphan Drug Designation from the FDA in 2017 for the potential treatment of EoE.10
A recently published phase 2, double-blind, placebo-controlled RCT showed that dupilumab (600-mg loading dose followed by 300 mg weekly) induced a significant improvement in the Dysphagia Symptoms Score, an 82.6% remission rate and a 65.2% deep remission rate. Endoscopic and histological involvement, as well as esophageal compliance (measured with endoFLIP) significantly improved (Hirano et al., 2020). The most common AEs reported were injection-site reactions and nasopharyngitis. The long-term effects of dupilumab (in terms of tolerability and efficacy) are currently being studied by two phase 3 RCTs (one in adults and adolescents – NCT03633617, and one in pediatric patients – NCT04394351).11,12 A phase 2 trial (NCT03678545) is evaluating its applicability in EG and EGE13.
IL-5 is produced by Th2 cells, mast cells, eosinophils, natural killer cells, ILC2 cells and basophils. It regulates eosinophil maturation, survival and activation (O’Byrne et al., 2001) through multiple signal transduction pathways including nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) and Janus kinase (JAK)/STAT5 modules (Roufosse, 2018).
IL-5 is overexpressed in the esophagus of patients with EoE (Straumann et al., 2001; Bullock et al., 2007; Molina-Infante et al., 2014) and correlates with esophageal eosinophilia and disease activity (Namjou et al., 2014). Blood-circulating lymphocytes producing high amounts of IL-5 and correlating with the severity of esophageal tissue eosinophilia have also been described (Bullock et al., 2007).
Finally, an association between polymorphisms in the IL5–IL13 region was also reported in a PheWAS study (Namjou et al., 2014).
Interleukin-5 as a Therapeutic Target. In murine models, mucosal IL-5 overexpression is able to induce EoE and IL-5 neutralization can nearly completely avoid intratracheal IL-13-induced EoE (Mishra and Rothenberg, 2003).
Mepolizumab, a fully humanized monoclonal IgG1 kappa anti-IL-5 antibody approved for severe asthma and hypereosinophilic syndrome, has been studied in both adult and pediatric EoE.
A first case report on three adults (Rothenberg et al., 2008) reported an improvement of symptoms, endoscopic features and esophageal eosinophil counts but absence of histologic remission.
A little and very short double blind, placebo-controlled trial in 11 adults (Stein et al., 2006) receiving two weekly intravenous infusions of 750 mg of mepolizumab and evaluated 2 weeks later, showed a reduction in esophageal infiltrate but absence of histologic remission and endoscopic or symptomatic improvement. The most common AE were headache and upper respiratory tract infection symptoms. Other reported AE were hypotension, nausea, fatigue, non-specific chest pain, and cough during infusions. No further improvements were reported after two additional infusions of 1500 mg of mepolizumab at 4-week intervals (Straumann et al., 2010b).
A subsequent non-placebo-controlled trial involving 3 different doses on 59 pediatric patients (Assa’ad et al., 2011) reported, after 12 weeks, a significant reduction in epithelial eosinophil counts, with 31.6% of children reaching remission, and only 8.8% achieving deep remission. There was no symptoms improvement and at week 24, with no additional mepolizumab doses, eosinophilia increased in all arms. The most common AEs were vomiting, diarrhea and upper abdominal pain.
A new multi-center, randomized, double-blind, parallel-arm, placebo-controlled trial (NCT03656380) in adults and adolescents with mepolizumab 300 mg subcutaneously monthly for 3 months or mepolizumab 100 mg SQ monthly is currently ongoing.14
Reslizumab is a humanized IgG4 kappa monoclonal antibody that binds to human IL-5, approved for severe eosinophilic asthma (Castro et al., 2015). It received Orphan Drug Designation status from the FDA in 2007.15 A double blind, placebo-controlled trial on 227 patients receiving four intravenous infusions of 1, 2, or 3 mg/kg of reslizumab every 4 weeks showed a reduction of the eosinophilic infiltrate but a disease remission in only 4.4% of patients (Spergel et al., 2012b). No reported AE resulted significantly different from the placebo group. However, a subsequent study reporting the follow-up data of 12 patients undergoing the open-label extension of this trial or receiving reslizumab as a compassionate use for up to 9 years, reported that 92% of the children showed a reduction in eosinophil count to less than 5/hpf and a significant symptomatic improvement (Markowitz et al., 2018).
IL-15, produced predominantly by monocytes, macrophages, and dendritic cells, has a structural similarity to IL-2, with which it shares the ability to stimulate the proliferation and differentiation of activated T cells (Anderson et al., 1995). In addition, IL-15 is required for NK cells and some T cells survival and activation (Kennedy and Park, 1996). IL-15 has also been shown to support type 2 allergic inflammatory responses: it can induce murine mast cells to produce IL-4 through the STAT6 pathway and esophageal epithelial cells to increase the expression of eotaxin (Tagaya et al., 1996; Masuda et al., 2000). Moreover, IL-15 can induce skewing of CD4 + T and iNKT cells (Lucendo et al., 2008) and induce the synthesis of IL-5 and IL-13 (Mishra et al., 2008; Blanchard et al., 2010).
IL-15 and its receptor IL-15Ra are elevated in esophageal tissue samples of patients with EoE, as well as in an intranasal Aspergillus-induced murine model of EoE, and correlate with esophageal eosinophilia (Zhu et al., 2010). Interestingly, peripheral blood IL-15Ra mRNA levels are reduced, seemingly indicating that most of the cells expressing IL-15Rα moved to the tissue (Upparahalli Venkateshaiah et al., 2021).
Interleukin-15 as a Therapeutic Target. IL-15-deficient mice show a significantly reduced esophageal eosinophilia when challenged with intranasal Aspergillus fumigatus (Zhu et al., 2010; Venkateshaiah et al., 2019).
CALY-002 is a first-in-class humanized monoclonal antibody inhibiting IL-15. It received Orphan Drug Designation from EMA in 201616 and from the FDA in 201817 for the potential treatment of EoE. A multi-site, randomized, placebo-controlled study (NCT04593251) in celiac patients that includes an open label multiple dose expansion cohort in participants with EoE is currently ongoing.18
IL-18 shares structural similarities with IL-1 (Nakanishi et al., 2001). Myeloid cells constitutively produce the inactivated version of this cytokine (proIL-18), and the conversion into its bioactive form (IL-18) occurs only upon inflammasome activation, through the enzymatic activity of caspase-1. In the extracellular space, IL-18 exerts its inflammatory activity via binding to its receptors, IL-18Rα and IL-18Rβ (Van Gorp et al., 2019). Initially it was thought that this cytokine mainly played a role in inducing Th1 differentiation, however it is also known to mediate T2 responses as well. Some IL-18 polymorphisms have been linked to a decreased risk of atopy, and IL-18 was shown to induce T2 inflammation in animal models (Tsutsui et al., 2004; Cheng et al., 2014). This cytokine is indeed able to induce iNKT cell production of the key T2 cytokines IL-5 and IL-13 (Niranjan et al., 2015).
It appears that the esophageal mucosa of EoE patients is characterized by a high expression of the IL-18 mRNA, as well as higher distribution of IL-18Rα (Niranjan et al., 2015).
These findings were confirmed in a murine model of Aspergillus and peanut-induced EoE (Dutt et al., 2015), where high levels of circulating IL-18 and esophageal IL-18Rα mRNA were detected. Moreover, this study confirmed that IL-18Rα was expressed by esophageal iNKT cells and that intranasal administration of IL-18 resulted in a time- and dose-dependent esophageal mast cell and eosinophilic inflammation. IL-18 overexpression was also able to induce eosinophilic and mast cell infiltration of the esophagus and increased collagen deposition in the epithelial mucosa, lamina propria, and muscularis mucosa.
Interleukin-18 as a Therapeutic Target. Based on the previously cited findings, IL-18 or IL8Rα have been proposed as therapeutic targets for EoE by many authors (Dutt et al., 2015; Niranjan et al., 2015; Shukla et al., 2015).
Indeed, tadekinig alfa, a human recombinant IL-18 binding protein (IL-18BP) (Gabay et al., 2018) is being actively studied in Still Disease and other autoinflammatory diseases (NCT03113760) and GSK1070806, a humanized IgG1/kappa antibody directed against the soluble cytokine interleukin-18 (IL-18), is starting to be employed in type 2 Diabetes Mellitus (McKie et al., 2016), renal transplant recipient (Wlodek et al., 2021) and Crohn’s disease.19 However, their use in EoE patients has not yet been studied.
IL-33 is an alarmin cytokine of the IL-1 family, released in response to injury. IL-33 binds to a receptor complex of IL-1 receptor-like 1 (IL1RL1, also known as ST2) and IL-1 receptor accessory protein (IL1RAcP). It is constitutively produced by endothelial cells, epithelial cells, keratinocytes and dendritic cells (Geering et al., 2013) and can also be expressed by other immune cells upon activation, including eosinophils, mast cells, macrophages, dendritic cells (DCs), B cells and monocytes (Johnston and Bryce, 2017). IL-33 can activate the STAT6 pathway, increases IL-5 production and is required for eosinophil survival (Johnston et al., 1950). Additionally, it induces cytokines release from mast cells and Th2 cells and induces the production of IL-1 beta, IL-4, IL-5, IL-6, IL-8, IL-13 and GM-CSF from basophils (He et al., 2013).
IL-33 expression is increased in pediatric EoE (Judd et al., 2016) and appears to be expressed by both the endothelium and the basal layer of the epithelium by an undifferentiated, non-dividing esophageal epithelial cell population (Judd et al., 2016; Travers et al., 2016). Moreover, an increased expression of ST2 (IL-33R) has been described in other studies, especially in basophils (Siracusa et al., 2011; Venturelli et al., 2016).
IL-33 is able to promote EoE development in mice (Judd et al., 2016) and a murine model of EoE based on epicutaneous OVA sensitization followed by intranasal OVA challenge, revealed that the IL-33–ST2 axis, together with the expression of ST2 on basophils, were required to induce EoE (Venturelli et al., 2016).
Interleukin-33 as a Therapeutic Target. ST2-deficient mice do not develop EoE (Venturelli et al., 2016), thus suggesting that drugs acting on the IL-33-ST2 axis might be efficacious in EoE.
Currently, two drugs are being investigated in other T2- inflammation-related conditions.
Etokimab (ANB020), an IgG1 anti-IL-33 monoclonal antibody is being investigated in severe eosinophilic asthma,20 food allergy (Chinthrajah et al., 2019), and AD (Chen et al., 2019) with promising results.
Astegolimab (MSTT1041A/AMG 282), a human IgG2 monoclonal antibody that selectively inhibits ST2, reduced asthmatic exacerbation rate in a broad population of patients (Kelsen et al., 2021). However, no study has been announced in EoE.
Transforming growth factor beta regulates epithelial growth and tissue remodeling and has complex roles in cell differentiation, proliferation, apoptosis and in immune regulation. It is produced by various cells, including mast cells, eosinophils, fibroblasts and epithelial cells.
An elevated TGF-β expression has repeatedly been found in esophageal biopsy samples of patients with active EoE (Aceves et al., 2007; Mishra et al., 2008; Straumann et al., 2010a), especially in mast cells (Aceves et al., 2010a). Also other TGF-beta-induced factors, such as plasminogen activator inhibitor-1 (PAI-1) (Rawson et al., 2016) and Thrombospondin-1 (TSP-1) (Hsieh et al., 2021) are significantly increased in the EoE esophageal epithelium and are associated with fibrosis and collagen deposition.
Indeed, multiple studies have shown a major role of TGF-β1 in esophageal remodeling through stimulation of fibroblast secretion of extracellular matrix and expression of periostin and smooth muscle actin (Muir et al., 2016; Rawson et al., 2016; Hsieh et al., 2021), activation of transdifferentiation into myofibroblasts (Aceves et al., 2010a) and EMTs (Kagalwalla et al., 2012; Rieder et al., 2014).
Moreover, TGF-β1 can increase esophageal smooth muscle contractility (Aceves et al., 2010a) by preventing the uptake of cytosolic calcium through the action of phospholamban (PLN) (Beppu et al., 2014).
TGF-β1 exposure also leads to decreased epithelial barrier function. TGF-β can induce epithelial cells apoptosis through p38 mitogen–activated protein kinase (MAPK)– signaling pathway, reduce the expression of the tight-junction molecule claudin-7 (CLDN7) (Nguyen et al., 2018) and induce matrix metalloproteinase expression in esophageal epithelial cells.
A relationship between TGF-β and EoE pathogenesis was also suggested by some inconstant genetic associations: a polymorphism (SNP C509T) in the TGFβ1 promoter on chromosome 19q13 was associated with an increase of TGFβ1 and tryptase and with increased remodeling, especially in the presence of concurrent food sensitization and steroid unresponsiveness (Aceves et al., 2010b; Rawson et al., 2015; Duong et al., 2020). Moreover, the repeatedly reported association between EoE and polymorphisms in locus 11q13, attributed to EMSY by most authors [see section “Tumor necrosis factor-α and Interferon-γ”], was recently attributed by Kottyan et al. (2021) to the near encoded protein LRRC32 (leucine-rich repeat-containing protein 32; also known as GARP), a TGF-β binding protein with a role in latent surface expression and signaling of TGF-β and highly expressed in activated forkhead box P3 (FOXP3) + T regulatory cells (D’Mello et al., 2016). Interestingly, there is also a high rate association of EoE with Loeys-Dietz syndrome, caused by gain-of-function mutations in the TGF-β receptors (Frischmeyer-Guerrerio et al., 2013).
Transforming Growth Factor Beta as a Therapeutic Target. The evidence that Smad3 (TGF-β signaling pathway), -deficient EoE mice show reduced esophageal fibrosis and angiogenesis (Cho et al., 2014) has induced the theory that anti-TGF-β therapy could be used to prevent fibrosis and remodeling in EoE patients.
Indeed, the use of neutralizing antibodies to TGF-β has shown to prevent organ fibrosis in murine models of different diseases (McCormick et al., 1994, 1999; Ziyadeh et al., 2000; Fukasawa et al., 2004) and in vitro (McMillan et al., 2005). However, in different murine models of allergic airways disease, treatment with anti–TGF-b led to contrasting results (McMillan et al., 2005; Fattouh et al., 2008).
In humans, Fresolimumab, a monoclonal anti–TGF-β antibody, decreased biomarkers and reversed skin fibrosis in systemic sclerosis patients (Rice et al., 2015), however no studies have been carried out in EoE patients.
In addition to targeted therapy, several commonly used drugs have demonstrated anti-TGF-β activity and thus constitute a possible anti-fibrotic therapeutic strategy.
Losartan, an angiotensin II receptor blocker, has shown anti-fibrotic activity by blocking angiotensin II induction of TGF-β in numerous animal models and in some inconstant and small human trials of organ fibrosis (Couluris et al., 2012; Salama et al., 2016). A preliminary, open-label trial (NCT01808196) of losartan potassium in pediatric EoE patients with or without a CTD21 and a phase 2 trial (NCT03029091) with losartan assessing this drug’s potential to achieve endoscopic, histological, and symptomatic improvement in 14 pediatric and adult EoE patients with or without CTDs at 16 weeks22 have been completed respectively in February 2015 and in September 2020 but the results have not been published. The results available on Clinicaltrials.gov, however, show very modest effects on eosinophilic infiltrate, remission, histologic and endoscopic scores and symptoms. No data is available on fibrosis or esophageal compliance.
Thiazolidinediones rosiglitazone and pioglitazone, two PPARγ agonists, significantly inhibited TGF-β1-induced mRNA expression of several remodeling-related genes in vitro in EoE esophageal fibroblasts with a dose-dependent effect, disrupting TGF-ß-Smad signal transduction (Nhu et al., 2020).
Tranilast is an anthranilic acid derivative that prevents mast cell degranulation, in use in Japan for the treatment of allergic rhinitis, asthma and AD. In an in vitro study, tranilast prevented the secretion of TGF-ß, and blocked TGF-ß-induced Smad2 and ERK1 activation (Platten et al., 2001).
Thymic stromal lymphopoietin and its receptor promote Th2 differentiation and dendritic cells activation (Ziegler, 2010).
It is produced by epithelial cells, macrophages, mast cells and dendritic cells (Geering et al., 2013) in response to cytokines (Bogiatzi et al., 2007), noxious substances (Smelter et al., 2010), and mechanical stress (Oyoshi et al., 2010).
It also has a broad variety of cell targets, including eosinophils (Wong et al., 2010), mast cells (Allakhverdi et al., 2007), and basophils (Siracusa et al., 2011).
An increased TSLP expression has been repeatedly reported in the esophageal tissue of patients with EoE (Blanchard, 2006; Rothenberg et al., 2010).
As a confirmation of the major role of this cytokine in EoE, the TSLP locus (5q22) is highly associated with EoE in multiple GWAS studies (Sherrill et al., 2010; Kottyan et al., 2014, 2021; Namjou et al., 2014; Sleiman et al., 2014). In particular, a TSLP single nucleotide polymorphism (SNP), that results in increased TSLP expression, correlates with EoE risk and increased basophil numbers (Rothenberg et al., 2010; Noti et al., 2013).
Moreover, a single nucleotide variation (rs36133495) in the cytokine receptor-like factor 2 (CRLF2) gene, that codes for the receptor of TSLP and is located on the pseudoautosomal region of the sex chromosomes, was found to be associated to EoE in males and is thus the first molecular mechanism that associate EoE to its male predominance (Sherrill and Rothenberg, 2011; Holvoet et al., 2016).
Thymic Stromal Lymphopoietin as Therapeutic Target. Targeting TSLP decreased eosinophilia and total immune cell infiltration in a murine model of EoE induced by epicutaneous OVA or peanut sensitization followed by oral challenge (Noti et al., 2013).
Tezepelumab (AMG 157) is a fully human anti-TSLP antibody with potential use in uncontrolled asthma (Corren et al., 2017). On October 8th, 2021 Tezepelumab was granted Orphan Drug Designation (ODD) in the US by the FDA for the treatment of EoE.23
Eotaxins, a subfamily of chemokines, are critical for the chemotaxis of eosinophils into tissues. They are mainly produced by epithelial cells, but can also be produced by activated eosinophils, mast cells and fibroblasts (Forssmann et al., 1997). The eotaxin subfamily consists of three different molecules. Eotaxin-1 attracts eosinophils in the gastrointestinal tract (except for the esophagus), eotaxin-2 is mostly expressed in the lung, while eotaxin-3 is found in lungs and gastrointestinal tract (Forssmann et al., 1997).
They are upregulated by IL-4 and IL-13 via STAT6 and signal exclusively through receptor CCR3, which is expressed predominantly on eosinophils and mast cells, but is also found on basophils Th2 cells (Rothenberg et al., 1995; Forssmann et al., 1997; Kitaura et al., 1999). Its activation causes an increase of cell adhesion molecules and the production of T2 cytokines such as IL-13.
Eotaxin-3 seems to be less potent and to be expressed later than eotaxin 1 and 2 and is seems to be involved in prolonged eosinophil recruitment (Ravensberg et al., 2005).
Eotaxin-3 is the most expressed cytokine in all EoE patients (Blanchard et al., 2006; Sherrill et al., 2014b). In particular, it had the highest differential value between patients and controls and its expression strongly correlates with eosinophil and mast cell infiltrate (Blanchard et al., 2006).
Additionally, an increased expression of PARP14, a transcriptional cofactor that facilitates CCL26 transcription, was also described in EoE pediatric patients. CCL26 expression strongly correlates with PARP14 expression (Krishnamurthy et al., 2014).
Finally, a single-nucleotide polymorphism on the eotaxin-3 gene (chromosome 7q11) has been associated with increased eotaxin-3 levels and an increased EoE risk, possibly through an enhancement of the stability of the eotaxin-3 mRNA (Blanchard et al., 2006; Romano et al., 2014; Moawad et al., 2015).
Eotaxin as a Therapeutic Target. CCL26 expression is downregulated upon treatment with topical steroids (Blanchard, 2006) and PPIs (Zhang et al., 2012).
Also CCR3 has been identified as a promising target for novel therapies directed to eosinophilic diseases, and thus, to have a possible role in EoE therapy.
GW766994, an oral small-molecule selective competitive antagonist of CCR3, has been investigated in asthma with no significant results (Neighbour et al., 2014).
More recently, R321, a peptide-based CCR3 antagonist with a different mechanism of action was described (Grozdanovic et al., 2019). In mouse models of acute allergic airways disease R321 blocked eosinophil recruitment into the blood, lungs, and airways and prevented airway hyperresponsiveness. No further studies on this molecule are currently available in literature.
At present, no studies in EoE with these drugs have been proposed.
Even if it is widely recognized that EoE pathogenesis is mainly orchestrated by T2 responses, Th1-related cytokines, including TNF–α and IFN-γ are found to be increased in EoE tissue specimens (Straumann et al., 2001; Gupta et al., 2006; Ruffner et al., 2021).
It was described that CD8 + T cells are a source of these cytokines in active disease settings, but not during remission or in control groups (Sayej et al., 2016). Moreover, circulating CD4 + T cells from pediatric EoE patients were able to produce interferon upon stimulation with EoE-causal allergens (Ruffner et al., 2021).
TNF-α derived from dendritic cells, eosinophils, mast cells and T cells is able to induce epithelial cell contraction, migration, and collagen secretion, as well as the expression of adhesion molecules on endothelial cells (Straumann et al., 2001; Rieder et al., 2014; Upparahalli Venkateshaiah et al., 2021). These aspects may link this cytokine to tissue remodeling and angiogenesis in EoE patients. Moreover, fibroblast-derived TNF-α can stimulate epithelial expression of lysyl oxidase (LOX), a collagen cross-linking enzyme, through activation of nuclear factor κB and TGF-β–mediated signaling. LOX upregulation has been linked to EoE complications, including fibrostenotic alterations (Kasagi et al., 2019).
Genetically, an association between EoE risk and polymorphisms in gene c11orf30 has been described (Sleiman et al., 2014). This gene encodes for EMSY, a transcriptional regulator recently found to be involved as a critical mediator of a novel Akt-dependent mechanism exploited by IFN and other growth factors to regulate interferon-stimulated genes (Ezell et al., 2012). EMSY expression was also found to be significantly enhanced in active EoE compared to controls (Kottyan et al., 2021). Variants at the c11orf30 locus have also been associated with seasonal allergic rhinitis (Ramasamy et al., 2011), ulcerative colitis (Anderson et al., 2011), Crohn’s disease (Barrett et al., 2008), AD (Esparza-Gordillo et al., 2009; Hirota et al., 2012), asthma (Ferreira et al., 2011), and allergic sensitization (Bønnelykke et al., 2013; Amaral et al., 2015).
Tumor Necrosis Factor-α and Interferon-γ as a Therapeutic Target. Infliximab, a chimeric IgG1 monoclonal antibody that inhibits TNF-α, was studied in a short pilot study on three adult patients refractory to standard treatments (Straumann et al., 2008). An infliximab dose of 5 mg/kg at weeks 0 and 2 failed to cause a significant decrease in esophageal eosinophil counts nor in symptoms. However, the short treatment period did not consent to assess efficacy on remodeling.
No therapeutic approaches involving IFN-γ are available in literature.
Prostaglandin D2 (PGD2) has an established role in allergic diseases such as asthma. It is produced by mast cells (He et al., 2013) and recruits Th2 cells, eosinophils, and basophils through receptor CRTH2 (Pettipher et al., 2007). Moreover, it mediates vasodilatation and the increase of vascular permeability (He et al., 2013). PGD2 injection in the esophagus leads to an increase of eosinophil infiltration in esophageal epithelium at the injection site (Zhang et al., 2014), and prostaglandin D synthase is expressed in adaptive CD4+ effector memory Th2 cells in EoE (Mitson-Salazar et al., 2016).
Other eicosanoids, such as leukotriene D4, prostaglandin F2 alpha and thromboxane B2 appear to have a role in contraction of esophageal muscle (Daniel et al., 1979; Kim et al., 1998; Rosenberg et al., 2013).
Eicosanoids as a Therapeutic Target. Prostaglandin inhibition was able to protect against EoE-like inflammation in an animal model (guinea pig) based on intraperitoneal OVA sensitization followed by aerosol challenge (Zhang et al., 2014).
Timapiprant (OC000459/CHF 6532), a CRTH2 inhibitor, was studied in a double-blind, placebo-controlled RCT of 26 adults with refractory EoE for 8 weeks (Straumann et al., 2013). The study reported a significant decrease in eosinophilic infiltrate and symptoms with a trend toward normalization of endoscopic features, but absence of remission. No significant AEs were reported.
Montelukast, a competitive, selective leukotriene D4 receptor antagonist that has been used since long time in asthma treatment, was evaluated as a possible adjunctive treatment to maintain remission in EoE patients after steroid therapy with no significant results and no significant AEs (Lucendo et al., 2011b; Alexander et al., 2017).
The histamine receptors HR1, HR2, and HR4 have been reported to be highly expressed the esophagus of patients with active EoE, in particular by epithelial eosinophils (Merves et al., 2015).
Histamine is produced by mast cells and induces vasodilation, microvascular leakage, dendritic cells polarization toward T2, eosinophilic homing, production of IL-6 in mast cells and fibroblast and endothelial proliferation (He et al., 2013). Moreover, histamine could also play a role in smooth muscle contraction (Goyal and Rattan, 1978). However, no further studies have assessed histamine role in EoE.
Histamine as a Therapeutic Target. Up to date, no clinical trial or case report was published on the use of antihistamines in EoE.
A phase II, randomized, placebo-controlled study (NCT04248712) evaluating the efficacy of antihistamines (the anti-H2 famotidine and anti H1 loratadine) in the treatment of EoE (the ATEE Study) is currently ongoing.24
Local IgE production by B cells (Vicario et al., 2009) and an increase of FcεRI-positive cells (namely Langherans cells) (Yen et al., 2010) have been described in EoE.
Also, an increased level of IgG4 in homogenates of esophageal tissues, granular extracellular IgG4 deposits in lamina propria in biopsy specimens and an increased total serum level of IgG4 with increased serum levels of IgG4 that reacted with milk, wheat, egg, and nuts have been reported (Clayton et al., 2014; Zukerberg et al., 2016; Schuyler et al., 2017, 2018; Wilson et al., 2017; Rosenberg et al., 2018; Weidlich et al., 2020).
However, other studies collecting IgG4 directly from the esophageal mucosa showed no differences in the levels of food-specific IgG4 between patients and controls (Ramaswamy et al., 2019) and studies evaluating the efficacy of serum or mucosal IgE or IgG-directed tests in the identification of causal food allergens yielded disappointing results.
Moreover, B cell-deficient mice are still able to develop EoE (Mishra et al., 2007), thus indicating a non-crucial role of humoral immunity in EoE pathogenesis.
IgE and IgG as a Therapeutic Target. Omalizumab, a monoclonal antibody that binds to free serum IgE and prevents it from binding to high-affinity receptor Fche identification of causal food allergens yielded disappointibronchial asthma and chronic urticaria, has been investigated in EoE with scarce results. In particular, some case reports (Rocha et al., 2011; Arasi et al., 2016) and a randomized double-blind placebo-controlled study on adults and children (Clayton et al., 2014) showed no significant histological and clinical improvements, while an open-label single-arm trial demonstrated endoscopic and histological remission in 33% of the subjects (Loizou et al., 2015).
No other therapy approach directed to humoral immunity has been found in literature.
Periostin is an extracellular matrix (ECM) protein produced by esophageal fibroblasts and epithelial cells in response to TGF-β and IL-13 (Nguyen et al., 2016), that supports adhesion and migration eosinophils and regulates extracellular matrix deposition (Conway and Molkentin, 2008; Snider et al., 2008). Its expression has been reported to be highly upregulated (approximately 52-fold) in biopsies from patients with EoE (Politi et al., 2016) but not in serum (Dellon et al., 2016).
Periostin as a Therapeutic Target. Periostin has been shown to be reduced by diet and steroid therapy in EoE (Politi et al., 2016). Up to date, no periostin-specific therapy has been proposed for EoE. Recently, a new peptide antagonist has been developed and tested in vitro in the oncologic field (Oo et al., 2021).
Sphingosine-1-phosphate is a blood borne lipid mediator derived from sphingosine which regulates eosinophils recruitment, migration of natural killer cells, mast cells activation, lymphocyte trafficking, Th17 cell polarization and dendritic cell differentiation (Sugita et al., 2010; Cohen et al., 2019). A dysregulation of S1PRs has been found in some immunological diseases, including asthma (Sun et al., 2010), but the role of S1P in EoE has not yet been studied.
Sphingosine-1-Phosphate as a Therapeutic Target. Several selective sphingosine-1-phosphate receptor (SP1R) modulators have yielded promising results in other immune-mediated diseases like multiple sclerosis, psoriasis, and IBD (Vaclavkova et al., 2014; Sandborn et al., 2016, 2020; Pérez-Jeldres et al., 2019).
Etrasimod (APD334), a SP1R modulator, has received Orphan Drug Designation status from the FDA in June 202125 and is currently being evaluated in EoE in a phase 2b, randomized, double-blind, placebo-controlled trial (NCT04682639).26
α4β7 integrin is expressed on T lymphocytes, eosinophils, and natural killer cells surface (Soler et al., 2009; Wyant et al., 2016) and is gut-specific (Cherry et al., 2015).
Expression of both α4β7 and α4β1 by eosinophils has been described (Berlin et al., 1993; Cook et al., 1995), but β7 seems to be more important homing eosinophils into the GI tract] through its receptor, MAdCAM-1, expressed in high endothelial venules of lymph nodes and in the lamina propria of intestine. In murine IBD models, blockade of α4β7 prevents GI eosinophilic recruitment (Picker and Butcher, 1992; Berlin et al., 1993; Gonzalo et al., 1998; Brandt et al., 2006).
This integrin appears to be also expressed on EoE Th2 cells (Wen et al., 2019). Moreover, studies suggest that Cadherin 26 promotes α4β7-mediated cell adhesion via direct interactions with α4 and β7 subunits (Caldwell et al., 2017).
α4β7 as a Therapeutic Target. Integrins represent a therapeutic target in some inflammatory conditions as IBDs and rheumatoid arthritis. No clinical trial has been conducted in EoE patients, but some case reports have been published.
Natalizumab, a humanized monoclonal antibody that binds to the α4 integrin in both α4β1 and α4β7 integrins and has demonstrated efficacy in multiple sclerosis (Tramacere et al., 2015) and Crohn’s disease (MacDonald and McDonald, 2007), has been reported to lead to complete resolution of EoE not responsive to PPIs, swallowed corticosteroids and 6FED in a woman treated for multiple sclerosis, with persistence of clinical and histological remission after 3 years of treatment (Beales, 2019).
Vedolizumab, an antibody that specifically blocks α4β7, has led to complete resolution of EoE in 2 patients receiving treatment for Crohn disease (Nhu et al., 2018; Taft and Mutlu, 2018).
This finding is associated with the description of vedolizumab as an effective rescue therapy for eosinophilic gastroenteritis in small case series (Kim H. P. et al., 2018; Grandinetti et al., 2019).
Sialic acid-binding Ig-like lectins (Siglecs) are found on the membrane of many immune cells. They are involved in cell signaling. Siglec 8, expressed on eosinophils, mast cells, and basophils, controls eosinophil apoptosis, inhibits mast cell degranulation, and reverses tissue remodeling (Kiwamoto et al., 2012).
Siglec-8 as a Therapeutic Target. In a murine model of EoE based on OVA intraperitoneal sensitization and subsequent intraesophageal challenge, the administration of anti-Siglec monoclonal antibodies has significantly reduced esophageal, circulating and bone marrow eosinophils and decreased remodeling processes (Rubinstein et al., 2011). Similar results have been obtained on eosinophilic and mast cells infiltrate and on inflammatory mediators in a murine model of EGE (Youngblood et al., 2019).
Antolimab/lirentelimab (AK002), a humanized non-fucosylated IgG1 monoclonal antibody directed against Siglec-8, was recently evaluated in a randomized, phase 2, placebo-controlled study in adult patients with EG and/or EGE (Dellon et al., 2020), showing a 95% mean reduction of tissue eosinophilia and a clinic-histological response in 69% of patients. Of note, a subanalysis on 23 patients presenting with an associated esophageal eosinophilia reported a significant reduction of the esophageal eosinophilic infiltrate with a high esophageal remission rate and a dysphagia score reduction. The most significant AEs reported were infusion-related reactions, of which one severe, and lymphopenia with no clinical consequences. Antolimab received Orphan Drug Designation status from the FDA in 2019.27 A phase 2/3, multicenter, randomized, double-blind, placebo-controlled study (NCT04322708) to evaluate the efficacy and safety in adult and adolescent EoE patients28 is currently ongoing.
The Signal Transducer and Activator of Transcription 6 (STAT6) pathway is pivotal in the development of EoE in intranasal Aspergillus-based murine models (Mishra and Rothenberg, 2003).
IL-4 and IL-13, together with IL-3, IL-15, IL-33, IFNα and platelet-derived growth factor-PDGF, can activate STAT6 through the action of Janus family (JAKs) tyrosine kinases (Huang et al., 2020). It acts as a Th2-inducing transcriptional activator (Goenka and Kaplan, 2011) and is implicated in the immunity to helminths and in the pathophysiology of various allergic conditions (Karpathiou et al., 2021).
Its effects are varied. In T cells, it decreases the expression of CDKN1B reducing proliferation; it induces Th2 differentiation and is needed for IL-9 secretion. In B cells, STAT6 induces IgE and IgG1 immunoglobulin class switching. In macrophages, it promotes differentiation to M2 and the expression of the major histocompatibility complex (MHC) class II (Goenka and Kaplan, 2011). In esophageal epithelial cells, the activation of STAT6 results in eotaxin-3 expression. In fibroblasts, it induces periostin expression (Blanchard et al., 2005).
Additionally, STAT6-mediated (Miller et al., 2019) activation of CAPN14 and SPIK7 genes (Pesek and Gupta, 2019) has been identified as the mechanism by which IL-13 downregulates the EDC and thus its effects on barrier function (Blanchard et al., 2010; Sherrill et al., 2014a; Kleuskens et al., 2021).
STAT6 polymorphisms on locus 12q13, previously associated with serum IgE levels (Granada et al., 2012), allergic sensitization (Bønnelykke et al., 2013), and asthma (Qian et al., 2014), have also been reported to have a major genetic association in EoE independent of sensitization (Sleiman et al., 2014) but a subsequent meta-analysis did not confirm the finding (Kottyan et al., 2021).
Recently, STAT6 variants were associated with relapse of EoE in pediatric patients receiving long-term PPI therapy (Mougey et al., 2021).
The STAT6 Pathway as a Therapeutic Target. STAT6-deficient mice do not develop EoE (Blanchard et al., 2007).
PPIs are an established first-line therapy for EoE, with a reported efficacy in 50% of pediatric and adult patients (Lucendo et al., 2016; Laserna-Mendieta et al., 2020; Navarro et al., 2021). Beyond their blocking effect of gastric acid secretion, PPIs have been demonstrated to be able to downregulate the esophageal gene expression of eotaxin-3, IL-5, and IL-13 similarly to topical steroids (Molina-Infante et al., 2014) and to inhibit ICAM-1 and VCAM-1 expression and enhance barrier function (Spergel et al., 2018). Indeed, in vitro omeprazole appears to block the chromatin remodeling that is necessary for STAT6 -mediated transcription of the eotaxin-3 gene (Zhang et al., 2012; Cheng et al., 2013). Common AEs, mainly derived from prolonged use, comprehend gastrointestinal infections, decreased vitamin B12 absorption, hypomagnesemia and increased risk for bone fractures.
JAKSTAT6 pathway inhibitors (ruxolitinib, AS1517499, leflunomide) have demonstrated in vitro ability to inhibit IL-13 induced eotaxin-3 expression in esophageal epithelial cells similar to PPIs (Cheng et al., 2013). Moreover, this effect was confirmed in esophageal fibroblasts, suggesting a role for JAK inhibitors in EoE treatment (Cheng et al., 2016).
Tofacitinib, a JAK inhibitor that showed some preliminary results in other eosinophilic diseases, as hypereosinophilic syndrome (King et al., 2017), bronchial asthma (Younis et al., 2019), and eosinophilic fasciitis (Kim S. R. et al., 2018; Cao et al., 2019), has recently been reported to induce clinical and endoscopic remission in a patient with refractory EoE (Mendoza Alvarez et al., 2019).
Peroxisome Proliferator-Activated Receptor γ (PPARγ) is a nuclear receptor that plays a crucial role in adipocyte physiology. Emerging evidence suggests that this molecule also play a role in macrophage and dendritic cells differentiation and polarization to M2 phenotype, lipid metabolism control in multiple immune cells and has an immune-modulatory role consisting in inhibition of Th1 and Th17 type inflammation, while its role on Th2 inflammation is still contradictory (Hernandez-Quiles et al., 2021). The IL4/STAT6 pathway stimulates PPARγ expression, and both IL-13 and STAT6 facilitate signaling through PPARγ (Huang et al., 1999). This nuclear receptor is able to regulate genes involved in lipid transport and metabolism (including the class B scavenger receptor CD36, FABP4, LXRA, and PGAR) in monocytes, macrophages and dendritic cells. Moreover, PPARγ may also play a role in lipid antigen presentation to T cells, by increasing CD1d expression in dendritic cells, making these cells more prone to activate iNKT cells (Szatmari et al., 2004). On the other side of the coin, PPARγ also appears to be linked in the downregulation of T2 cytokines in T cells, interacting with NFAT (Chung et al., 2003) and in the inhibition of mast cell maturation and activation (Zhang et al., 2017) showing a protective role in murine models of asthma and allergic rhinitis (Hammad et al., 2004; Wang et al., 2011).
In EoE, PPAR-γ-positive CD4± T cells were recently identified (Wen et al., 2019) and a study (Nhu et al., 2020) demonstrated a higher expression of PPAR-γ mRNA in EoE-derived fibroblasts, upregulated by IL-4 stimulation, and that expression of PPAR-γ was detectable in the epithelium and subepithelial lamina propria of active EoE but not in the normal esophagus.
Peroxisome Proliferator-Activated Receptor γ as a Therapeutic Target. Thiazolidinediones (TZDs), a class of antihyperglycemic drugs able to activate PPAR-γ, that include rosiglitazone and pioglitazone (Lehmann et al., 1995) have been proposed as potential drugs to target fibrosis in EoE, also for the ability to act mainly at the level of damaged tissue, sparing healthy areas. The TZDs preferentially exert antifibrotic effects in TGF-β1-activated EoE fibroblasts. In an in vitro study (Nhu et al., 2020) rosiglitazone and pioglitazone strongly inhibited TGF-β1-mediated synthesis of α-sma, collagen-1α1, and ctgf in EoE fibroblasts, in a dose-dependent fashion, while failing to do so in fibroblasts from healthy controls.
Eosinophilic esophagitis pathophysiology is complex and involves a still poorly understood net of genetic predisposition, mainly involving epithelial barrier and T2-related genes, and external factors that initiate a type 2 inflammatory cascade in which both innate and adaptive immunity play an important role. Deepening our understanding of the underlying mechanisms is crucial to the identification of new therapeutic targets to allow the development of a precision medicine in a debilitating condition whose incidence is rapidly rising. Some promising results have been reached with drugs targeting the IL-4/13 pathway, eosinophils recruitment and apoptosis, but it is still unknown whether these drugs also have the ability to prevent the remodeling processes or even revert it.
Finally, the identification of the mechanisms involved in the recognition of external antigens and the subsequent development of diagnostic tests directed to the identification of external triggers is a pivotal, yet still unanswered, goal in the management of these patients.
FR proposed the review and the layout, contributed to all sections and was in charge of the assembly of the individual paragraphs and final corrections. EH, GWC, and AR were in charge of the project and the layout, directed the aims and bibliography, distributed roles and supervised and corrected the final work. GaP, GC, EV, EC, GiP, MM, EN, and CP contributed to individual paragraphs and associated bibliography and revised the final work. All authors agreed to be accountable for the content of the work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor declared a past collaboration with several of the authors GWC and EH.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Figures 3, 4 created with BioRender.com.
Abdulnour-Nakhoul, S. M., Al-Tawil, Y., Gyftopoulos, A. A., Brown, K. L., Hansen, M., Butcher, K. F., et al. (2013). Alterations in junctional proteins, inflammatory mediators and extracellular matrix molecules in eosinophilic esophagitis. Clin. Immunol. 148, 265–278. doi: 10.1016/j.clim.2013.05.004
Abonia, J. P., Wen, T., Stucke, E. M., Grotjan, T., Griffith, M. S., Kemme, K. A., et al. (2013). High prevalence of eosinophilic esophagitis in patients with inherited connective tissue disorders. J. Allergy Clin. Immunol. 132, 378–386. doi: 10.1016/j.jaci.2013.02.030
Aceves, S. S., Chen, D., Newbury, R. O., Dohil, R., Bastian, J. F., and Broide, D. H. (2010a). Mast cells infiltrate the esophageal smooth muscle in patients with eosinophilic esophagitis, express TGF-β1, and increase esophageal smooth muscle contraction. J. Allergy Clin. Immunol. 126, 1198–1204.e4. doi: 10.1016/j.jaci.2010.08.050
Aceves, S. S., Newbury, R. O., Chen, D., Mueller, J., Dohil, R., Hoffman, H., et al. (2010b). Resolution of remodeling in eosinophilic esophagitis correlates with epithelial response to topical corticosteroids. Allergy 65, 109–116. doi: 10.1111/j.1398-9995.2009.02142.x
Aceves, S. S., Newbury, R. O., Dohil, R., Bastian, J. F., and Broide, D. H. (2007). Esophageal remodeling in pediatric eosinophilic esophagitis. J. Allergy Clin. Immunol. 119, 206–212. doi: 10.1016/j.jaci.2006.10.016
Aich, J., Mabalirajan, U., Ahmad, T., Agrawal, A., and Ghosh, B. (2012). Loss-of-function of inositol polyphosphate-4-phosphatase reversibly increases the severity of allergic airway inflammation. Nat. Commun. 3:877. doi: 10.1038/ncomms1880
Alexander, E. S., Martin, L. J., Collins, M. H., Kottyan, L. C., Sucharew, H., He, H., et al. (2014). Twin and family studies reveal strong environmental and weaker genetic cues explaining heritability of eosinophilic esophagitis. J. Allergy Clin. Immunol. 134, 1084–1092.e1. doi: 10.1016/j.jaci.2014.07.021
Alexander, J. A., Ravi, K., Enders, F. T., Geno, D. M., Kryzer, L. A., Mara, K. C., et al. (2017). Montelukast Does not Maintain Symptom Remission After Topical Steroid Therapy for Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 15, 214–221.e2. doi: 10.1016/j.cgh.2016.09.013
Allakhverdi, Z., Comeau, M. R., Jessup, H. K., Yoon, B.-R. P., Brewer, A., Chartier, S., et al. (2007). Thymic stromal lymphopoietin is released by human epithelial cells in response to microbes, trauma, or inflammation and potently activates mast cells. J. Exp. Med. 204, 253–258. doi: 10.1084/jem.20062211
Almansa, C., Krishna, M., Buchner, A. M., Ghabril, M. S., Talley, N., DeVault, K. R., et al. (2009). Seasonal distribution in newly diagnosed cases of eosinophilic esophagitis in adults. Am. J. Gastroenterol. 104, 828–833. doi: 10.1038/ajg.2008.169
Amaral, A. F., Minelli, C., Guerra, S., Wjst, M., Probst-Hensch, N., Pin, I., et al. (2015). The locus C11orf30 increases susceptibility to poly-sensitization. Allergy 70, 328–333. doi: 10.1111/all.12557
Anderson, C. A., Boucher, G., Lees, C. W., Franke, A., D’Amato, M., Taylor, K. D., et al. (2011). Meta-analysis identifies 29 additional ulcerative colitis risk loci, increasing the number of confirmed associations to 47. Nat. Genet. 43, 246–252. doi: 10.1038/ng.764
Anderson, D. M., Kumaki, S., Ahdieh, M., Bertles, J., Tometsko, M., Loomis, A., et al. (1995). Functional characterization of the human interleukin-15 receptor alpha chain and close linkage of IL15RA and IL2RA genes. J. Biol. Chem. 270, 29862–29869. doi: 10.1074/jbc.270.50.29862
Arasi, S., Costa, S., Magazzù, G., Ieni, A., Crisafulli, G., Caminiti, L., et al. (2016). Omalizumab therapy in a 13-year-old boy with severe persistent asthma and concomitant eosinophilic esophagitis. Ital. J. Pediatr. 42:32. doi: 10.1186/s13052-016-0243-x
Arias, A., and Lucendo, A. J. (2014). Dietary therapies for eosinophilic esophagitis. Expert Rev. Clin. Immunol. 10, 133–142. doi: 10.1586/1744666X.2014.856263
Arias, A., González-Cervera, J., Tenias, J. M., and Lucendo, A. J. (2014). Efficacy of dietary interventions for inducing histologic remission in patients with eosinophilic esophagitis: a systematic review and meta-analysis. Gastroenterology 146, 1639–1648. doi: 10.1053/j.gastro.2014.02.006
Arias, A., Pérez-Martínez, I., Tenías, J. M., and Lucendo, A. J. (2016). Systematic review with meta-analysis: the incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies. Aliment. Pharmacol. Ther. 43, 3–15. doi: 10.1111/apt.13441
Assa’ad, A. H., Gupta, S. K., Collins, M. H., Thomson, M., Heath, A. T., Smith, D. A., et al. (2011). An antibody against IL-5 reduces numbers of esophageal intraepithelial eosinophils in children with eosinophilic esophagitis. Gastroenterology 141, 1593–1604. doi: 10.1053/j.gastro.2011.07.044
Azouz, N. P., Klingler, A. M., Pathre, P., Besse, J. A., Baruch-Morgenstern, N. B., Ballaban, A. Y., et al. (2020). Functional role of kallikrein 5 and proteinase-activated receptor 2 in eosinophilic esophagitis. Sci. Transl. Med. 12:eaaz7773. doi: 10.1126/scitranslmed.aaz7773
Azouz, N. P., Ynga-Durand, M. A., Caldwell, J. M., Jain, A., Rochman, M., Fischesser, D. M., et al. (2018). The antiprotease SPINK7 serves as an inhibitory checkpoint for esophageal epithelial inflammatory responses. Sci. Transl. Med. 10:eaa9736. doi: 10.1126/scitranslmed.aap9736
Bagiella, E., and Chehade, M. (2016). Swallowed fluticasone propinate is an effective long-term maintenance therapy for children with eosinophilic esophagitis. Am. J. Gastroenterol. 111, 1187–1197. doi: 10.1038/ajg.2016.238
Barrett, J. C., Hansoul, S., Nicolae, D. L., Cho, J. H., Duerr, R. H., Rioux, J. D., et al. (2008). Genome-wide association defines more than 30 distinct susceptibility loci for Crohn’s disease. Nat. Genet. 40, 955–962. doi: 10.1038/ng.175
Beales, I. L. P. (2019). Resolution of Refractory Eosinophilic Esophagitis with the Leukocyte-Trafficking Inhibitor Natalizumab. Dig. Dis. Sci. 64, 2688–2689. doi: 10.1007/s10620-019-05704-5
Bégin, P., Bird, J. A., Spergel, J. M., Campbell, D. E., Green, T. D., Bee, K. J., et al. (2021). Reduction in peanut reaction severity during oral challenge after 12 months of epicutaneous immunotherapy. Allergy 76, 3835–3838. doi: 10.1111/all.15083
Bendelac, A., Savage, P. B., and Teyton, L. (2007). The biology of NKT cells. Annu. Rev. Immunol. 25, 297–336.
Benitez, A. J., Hoffmann, C., Muir, A. B., Dods, K. K., Spergel, J. M., Bushman, F. D., et al. (2015). Inflammation-associated microbiota in pediatric eosinophilic esophagitis. Microbiome 3:23. doi: 10.1186/s40168-015-0085-6
Beppu, L. Y., Anilkumar, A. A., Newbury, R. O., Dohil, R., Broide, D. H., and Aceves, S. S. (2014). TGF-β1-induced phospholamban expression alters esophageal smooth muscle cell contraction in patients with eosinophilic esophagitis. J. Allergy Clin. Immunol. 134, 1100–1107.e4. doi: 10.1016/j.jaci.2014.04.004
Beppu, L., Yang, T., Luk, M., Newbury, R. O., Palmquist, J., Dohil, R., et al. (2015). MMPs-2 and -14 are elevated in eosinophilic esophagitis and reduced following topical corticosteroid therapy. J. Pediatr. Gastroenterol. Nutr. 61, 194–199. doi: 10.1097/mpg.0000000000000668
Berlin, C., Berg, E. L., Briskin, M. J., Andrew, D. P., Kilshaw, P. J., Holzmann, B., et al. (1993). Alpha 4 beta 7 integrin mediates lymphocyte binding to the mucosal vascular addressin MAdCAM-1. Cell 74, 185–195. doi: 10.1016/0092-867490305-a
Biedermann, L., Holbreich, M., Atkins, D., Chehade, M., Dellon, E. S., Furuta, G. T., et al. (2021). Food-induced immediate response of the esophagus-A newly identified syndrome in patients with eosinophilic esophagitis. Allergy 76, 339–347. doi: 10.1111/all.14495
Blanchard, C. (2006). Eotaxin-3 and a uniquely conserved gene expression profile in eosinophilic esophagitis. J. Clin. Investig. 116, 536–547. doi: 10.1172/jci26679
Blanchard, C., Mingler, M. K., Vicario, M., Abonia, J. P., Wu, Y. Y., Lu, T. X., et al. (2007). IL-13 involvement in eosinophilic esophagitis: transcriptome analysis and reversibility with glucocorticoids. J. Allergy Clin. Immunol. 120, 1292–1300. doi: 10.1016/j.jaci.2007.10.024
Blanchard, C., Mishra, A., Saito-Akei, H., Monk, P., Anderson, I., and Rothenberg, M. E. (2005). Inhibition of human interleukin-13-induced respiratory and oesophageal inflammation by anti-human-interleukin-13 antibody (CAT-354). Clin. Exp. Allergy 35, 1096–1103. doi: 10.1111/j.1365-2222.2005
Blanchard, C., Stucke, E. M., Burwinkel, K., Caldwell, J. M., Collins, M. H., Ahrens, A., et al. (2010). Coordinate interaction between IL-13 and epithelial differentiation cluster genes in eosinophilic esophagitis. J. Immunol. 184, 4033–4041. doi: 10.4049/jimmunol.0903069
Blanchard, C., Wang, N., Stringer, K. F., Mishra, A., Fulkerson, P. C., Abonia, J. P., et al. (2006). Eotaxin-3 and a uniquely conserved gene-expression profile in eosinophilic esophagitis. J. Clin. Invest. 116, 536–547. doi: 10.1172/JCI26679
Blauvelt, A., de Bruin-Weller, M., Gooderham, M., Cather, J. C., Weisman, J., Pariser, D., et al. (2017). Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): a 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet 389, 2287–2303. doi: 10.1016/S0140-673631191-1
Bleecker, E. R., FitzGerald, J. M., Chanez, P., Papi, A., Weinstein, S. F., Barker, P., et al. (2016). Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β2-agonists (SIROCCO): a randomised, multicentre, placebo-controlled phase 3 trial. Lancet 388, 2115–2127. doi: 10.1016/S0140-673631324-1
Bogiatzi, S. I., Fernandez, I., Bichet, J. C., Marloie-Provost, M. A., Volpe, E., Sastre, X., et al. (2007). Cutting edge: proinflammatory and Th2 cytokines synergize to induce thymic stromal lymphopoietin production by human skin keratinocytes. J. Immunol. 178, 3373–3377. doi: 10.4049/jimmunol.178.6.3373
Bolton, S. M., Kagalwalla, A. F., Arva, N. C., Wang, M. Y., Amsden, K., Melin-Aldana, H., et al. (2020). Mast Cell Infiltration Is Associated With Persistent Symptoms and Endoscopic Abnormalities Despite Resolution of Eosinophilia in 382 Pediatric Eosinophilic Esophagitis. Am. J. Gastroenterol. 115, 224–233. doi: 10.14309/ajg.0000000000000474
Bønnelykke, K., Matheson, M. C., Pers, T. H., Granell, R., Strachan, D. P., Alves, A. C., et al. (2013). Meta-analysis of genome-wide association studies identifies ten loci influencing allergic sensitization. Nat. Genet. 45, 902–906. doi: 10.1038/ng.2694
Brandt, E. B., Zimmermann, N., Muntel, E. E., Yamada, Y., Pope, S. M., Mishra, A., et al. (2006). The alpha4bbeta7-integrin is dynamically expressed on murine eosinophils and involved in eosinophil trafficking to the intestine. Clin. Exp. Allergy 36, 543–553. doi: 10.1111/j.1365-2222.2006.02456.x
Brightling, C. E., Saha, S., and Hollins, F. (2010). Interleukin-13: prospects for new treatments. Clin. Exp. Allergy 40, 42–49. doi: 10.1111/j.1365-2222.2009.03383.x
Bullock, J. Z., Villanueva, J. M., Blanchard, C., Filipovich, A. H., Putnam, P. E., Collins, M. H., et al. (2007). Interplay of adaptive th2 immunity with eotaxin-3/c-C chemokine receptor 3 in eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 45, 22–31. doi: 10.1097/MPG.0b013e318043c097
Caldwell, J. M., Collins, M. H., Kemme, K. A., Sherrill, J. D., Wen, T., Rochman, M., et al. (2017). Cadherin 26 is an alpha integrin-binding epithelial receptor regulated during allergic inflammation. Mucosal Immunol. 10, 1190–1201. doi: 10.1038/mi.2016.120
Cao, W., Cheng, L., Behar, J., Biancani, P., and Harnett, K. M. (2006). IL-1beta signaling in cat lower esophageal sphincter circular muscle. Am. J. Physiol. Gastrointest. Liver Physiol. 291, G672–G680. doi: 10.1152/ajpgi.00110.2006
Cao, W., Cheng, L., Behar, J., Fiocchi, C., Biancani, P., and Harnett, K. M. (2004). Proinflammatory cytokines alter/reduce esophageal circular muscle contraction in experimental cat esophagitis. Am. J. Physiol. Gastrointest. Liver Physiol. 287, G1131–G1139. doi: 10.1152/ajpgi.00216.2004
Cao, X.-Y., Zhao, J.-L., Hou, Y., Wang, F.-D., and Lu, Z.-H. (2019). Janus kinase inhibitor tofacitinib is a potential therapeutic option for refractory eosinophilic fasciitis. Clin. Exp. Rheumatol. 38, 567–568.
Capocelli, K. E., Fernando, S. D., Menard-Katcher, C., Furuta, G. T., Masterson, J. C., and Wartchow, E. P. (2015). Ultrastructural features of eosinophilic oesophagitis: impact of treatment on desmosomes. J. Clin. Pathol. 68, 51–56. doi: 10.1136/jclinpath-2014-202586
Capucilli, P., Cianferoni, A., Grundmeier, R. W., and Spergel, J. M. (2018). Comparison of comorbid diagnoses in children with and without eosinophilic esophagitis in a large population. Ann. Allergy Asthma Immunol. 121, 711–716. doi: 10.1016/j.anai.2018.08.022
Castro, M., Zangrilli, J., Wechsler, M. E., Bateman, Brusselle, G. G., Bardin, P., et al. (2015). Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet Respir. Med. 3, 355–366. doi: 10.1016/S2213-260000042-9
Chehade, M., Sampson, H. A., Morotti, R. A., and Magid, M. S. (2007). Esophageal subepithelial fibrosis in children with eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 45, 319–328. doi: 10.1097/mpg.0b013e31806ab384
Chen, Y. L., Gutowska-Owsiak, D., Hardman, C. S., Westmoreland, M., MacKenzie, T., Cifuentes, L., et al. (2019). Proof-of-concept clinical trial of etokimab shows a key role for IL-33 in atopic dermatitis pathogenesis. Sci. Transl. Med. 11:eaax2945. doi: 10.1126/scitranslmed.aax2945
Cheng, D., Hao, Y., Zhou, W., and Ma, Y. (2014). The relationship between interleukin-18 polymorphisms and allergic disease: a meta-analysis. Biomed. Res. Int. 2014:290687. doi: 10.1155/2014/290687
Cheng, E., Souza, R. F., and Spechler, S. J. (2012). Tissue remodeling in eosinophilic es- ophagitis. Am. J. Physiol. Gastrointest. Liver Physiol. 303, G1175–G1187.
Cheng, E., Zhang, X., Huo, X., Yu, C., Zhang, Q., Wang, D. H., et al. (2013). Omeprazole blocks eotaxin-3 expression by oesophageal squamous cells from patients with eosinophilic oesophagitis and GORD. Gut 62, 824–832. doi: 10.1136/gutjnl-2012-302250
Cheng, E., Zhang, X., Wilson, K. S., Wang, D. H., Park, J. Y., Huo, X., et al. (2016). JAK-STAT6 pathway inhibitors block eotaxin-3 secretion by epithelial cells and fibroblasts from esophageal eosinophilia patients: promising agents to improve inflammation and prevent fibrosis in EoE. PLoS One 11:e0157376. doi: 10.1371/journal.pone.0157376
Cherry, L. N., Yunker, N. S., Lambert, E. R., Vaughan, D., and Lowe, D. K. (2015). Vedolizumab: an alpha4beta7 integrin antagonist for ulcerative colitis and Crohn’s disease. Ther. Adv. Chronic. Dis. 6, 224–233. doi: 10.1177/2040622315586970
Chinthrajah, S., Cao, S., Liu, C., Lyu, S. C., Sindher, S. B., Long, A., et al. (2019). Phase 2a randomized, placebo-controlled study of anti-IL-33 in peanut allergy. JCI Insight 4:e131347. doi: 10.1172/jci.insight.131347
Cho, J. Y., Doshi, A., Rosenthal, P., Beppu, A., Miller, M., Aceves, S., et al. (2014). Smad3-deficient mice have reduced esophageal fibrosis and angiogenesis in a model of egg-induced eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 59, 10–16. doi: 10.1097/MPG.0000000000000343
Christianson, C. A., Goplen, N. P., Zafar, I., Irvin, C., Good, J. T. Jr., Rollins, D. R., et al. (2015). Persistence of asthma requires multiple feedback circuits involving type 2 innate lymphoid cells and IL-33. J. Allergy Clin. Immunol. 136, 59.e–68.e. doi: 10.1016/j.jaci.2014.11.037
Chung, S. W., Kang, B. Y., and Kim, T. S. (2003). Inhibition of interleukin-4 production in CD4+ T cells by peroxisome proliferator-activated receptor-gamma (PPAR-gamma) ligands: involvement of physical association between PPAR-gamma and the nuclear factor of activated T cells transcription factor. Mol. Pharmacol. 64, 1169–1179. doi: 10.1124/mol.64.5.1169
Cianferoni, A., Ruffner, M. A., Guzek, R., Guan, S., Brown-Whitehorn, T., Muir, A., et al. (2018). Elevated expression of activated TH2 cells and milk-specific TH2 cells in milk-induced eosinophilic esophagitis. Ann. Allergy Asthma Immunol. 120, 177–183.e2. doi: 10.1016/j.anai.2017.11.006
Clayton, F., Fang, J. C., Gleich, G. J., Lucendo, A. J., Olalla, J. M., Vinson, L. A., et al. (2014). Eosinophilic esophagitis in adults is associated with IgG4 and not mediated by IgE. Gastroenterology 147, 602–609. doi: 10.1053/j.gastro.2014.05.036
Cohen, J. A., Comi, G., Selmaj, K. W., Bar-Or, A., Arnold, D. L., Steinman, L., et al. (2019). Safety and efficacy of ozanimod versus interferon beta-1a in relapsing multiple sclerosis (RADIANCE): a multicentre, randomised, 24-month, phase 3 trial. Lancet Neurol. 18, 1021–1033. doi: 10.1016/S1474-442230238-8
Conway, S., and Molkentin, J. (2008). Periostin as a heterofunctional regulator of cardiac development and disease. Curr. Genomics 9, 548–555. doi: 10.2174/138920208786847917
Cook, D. N., Beck, M. A., Coffman, T. M., Kirby, S. L., Sheridan, J. F., Pragnell, I. B., et al. (1995). Requirement of MIP-1 alpha for an inflammatory response to viral infection. Science 269, 1583–1585. doi: 10.1126/science.7667639
Corren, J., Parnes, J. R., Wang, L., Mo, M., Roseti, S. L., Griffiths, J. M., et al. (2017). Tezepelumab in Adults with Uncontrolled Asthma. N. Engl. J. Med. 377, 936–946. doi: 10.1056/NEJMoa1704064
Couluris, M., Kinder, B. W., Xu, P., Gross-King, M., Krischer, J., and Panos, R. J. (2012). Treatment of idiopathic pulmonary fibrosis with losartan: a pilot project. Lung 190, 523–527. doi: 10.1007/s00408-012-9410-z
Daniel, E. E., Crankshaw, J., and Sarna, S. (1979). Prostaglandins and myogenic control of tension in lower esophageal sphincter in vitro. Prostaglandins 17, 629–639. doi: 10.1016/0090-6980(79)90014-5
Davis, B. P., and Rothenberg, M. E. (2013). Antigen presentation by eosinophils in eosinophilic esophagitis? J. Pediatr. Gastroenterol. Nutr. 56:242. doi: 10.1097/MPG.0b013e31827ab8d3
De Swert, L., Veereman, G., Bublin, M., Breiteneder, H., Dilissen, E., Bosmans, E., et al. (2013). Eosinophilic gastrointestinal disease suggestive of pathogenesis-related class 10 (PR-10) protein allergy resolved after immunotherapy. J. Allergy Clin. Immunol. 131, 600–2.e1–3. doi: 10.1016/j.jaci.2012.10.057
Delaney, A. L., and Arvedson, J. C. (2008). Development of swallowing and feeding: prenatal through first year of life. Dev. Disabil. Res. Rev. 14, 105–117. doi: 10.1002/ddrr.16
Dellon, E. S. (2014). Epidemiology of eosinophilic esophagitis. Gastroenterol. Clin. North Am. 43, 201–218.
Dellon, E. S., and Hirano, I. (2018). Epidemiology and natural history of eosinophilic esophagitis. Gastroenterology 154, 319–332. doi: 10.1053/j.gastro.2017.06.067
Dellon, E. S., Collins, M. H., Assouline-Dayan, Y., Evans, L., Gupta, S., Schoepfer, A., et al. (2019a). Long-term efficacy and safety of RPC4046, an anti-Interleukin-13 monoclonal antibody, in patients with eosinophilic esophagitis: results from the openlabel extension of the HEROES Study. J. Allergy Clin. Immunol. 143:AB08.
Dellon, E. S., Collins, M. H., Rothenberg, M. E., Assouline-Dayan, Y., Evans, L., Gupta, S., et al. (2021). Long-term Efficacy and Tolerability of RPC4046 in an Open-Label Extension Trial of Patients With Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 19, 473–483.e17. doi: 10.1016/j.cgh.2020.03.036
Dellon, E. S., Erichsen, R., Baron, J. A., Shaheen, N. J., Vyberg, M., Sorensen, H. T., et al. (2015). The increasing incidence and prevalence of eosinophilic oesophagitis outpaces changes in endoscopic and biopsy practice: national population-based estimates from Denmark. Aliment. Pharmacol. Ther. 41, 662–670. doi: 10.1111/apt.13129
Dellon, E. S., Guo, R., McGee, S. J., Hamilton, D. K., Nicolai, E., Covington, J., et al. (2019b). Novel Allergen-Specific Immune Signature-Directed Approach to Dietary Elimination in Eosinophilic Esophagitis. Clin. Transl. Gastroenterol. 10:e00099. doi: 10.14309/ctg.0000000000000099
Dellon, E. S., Higgins, L. L., Beitia, R., Rusin, S., Woosley, J. T., Veerappan, R., et al. (2016). Prospective assessment of serum periostin as a biomarker for diagnosis and monitoring of eosinophilic oesophagitis. Aliment. Pharmacol. Ther. 44, 189–197. doi: 10.1111/apt.13672
Dellon, E. S., Jensen, E. T., Martin, C. F., Shaheen, N. J., and Kappelman, M. D. (2014a). Prevalence of eosinophilic esophagitis in the United States. Clin. Gastroenterol. Hepatol. 12, 589–596.e1.
Dellon, E. S., Kim, H. P., Sperry, S. L. W., Rybnicek, D. A., Woosley, J. T., and Shaheen, N. J. (2014b). A phenotypic analysis shows that eosinophilic esophagitis is a progressive fibrostenotic disease. Gastrointest. Endosc. 79, 577–585.e4. doi: 10.1016/j.gie.2013.10.027
Dellon, E. S., Peterson, K. A., Murray, J. A., Falk, G. W., Gonsalves, N., Chehade, M., et al. (2020). Anti-Siglec-8 Antibody for Eosinophilic Gastritis and Duodenitis. N. Engl. J. Med. 383, 1624–1634. doi: 10.1056/NEJMoa2012047
Dispenza, M. C., and Bochner, B. S. (2018). Diagnosis and novel approaches to the treatment of hypereosinophilic syndromes. Curr. Hematol. Malig. Rep. 13, 191–201. doi: 10.1007/s11899-018-0448-8
D’Mello, R. J., Caldwell, J. M., Azouz, N. P., Wen, T., Sherrill, J. D., Hogan, S. P., et al. (2016). LRRC31 is induced by IL-13 and regulates kallikrein expression and barrier function in the esophageal epithelium. Mucosal Immunol. 9, 744–756. doi: 10.1038/mi.2015.98
Doherty, T. A., Baum, R., Newbury, R. O., Yang, T., Dohil, R., Aquino, M., et al. (2015). Group 2 innate lymphocytes (ILC2) are enriched in active eosinophilic esophagitis. J. Allergy Clin. Immunol. 136, 792–794.e3. doi: 10.1016/j.jaci.2015.05.048
Doucet-Ladevèze, R., Holvoet, S., Raymond, F., Foata, F., Hershey, G. K. K., Sherrill, J. D., et al. (2019). Transcriptomic Analysis Links Eosinophilic Esophagitis and Atopic Dermatitis. Front. Pediatr. 7:467. doi: 10.3389/fped.2019.00467
Duong, L. D., Rawson, R., Bezryadina, A., Manresa, M. C., Newbury, R. O., Dohil, R., et al. (2020). β1 single-nucleotide polymorphism C-509T alters mucosal cell function in pediatric eosinophilic esophagitis. Mucosal Immunol. 13, 110–117. doi: 10.1038/s41385-019-0214-9
Dutt, P., Shukla, J. S., Ventateshaiah, S. U., Mariswamy, S. J., Mattner, J., Shukla, A., et al. (2015). Allergen-induced interleukin-18 promotes experimental eosinophilic oesophagitis in mice. Immunol. Cell Biol. 93:914. doi: 10.1038/icb.2015.84
Elieh Ali Komi, D., and Bjermer, L. (2019). Mast Cell-Mediated Orchestration of the Immune Responses in Human Allergic Asthma: current Insights. Clin. Rev. Allergy Immunol. 56, 234–247. doi: 10.1007/s12016-018-8720-1
Esparza-Gordillo, J., Weidinger, S., Fölster-Holst, R., Bauerfeind, A., Ruschendorf, F., Patone, G., et al. (2009). A common variant on chromosome 11q13 is associated with atopic dermatitis. Nat. Genet. 41, 596–601. doi: 10.1038/ng.347
Ezell, S. A., Polytarchou, C., Hatziapostolou, M., Guo, A., Sanidas, I., Bihani, T., et al. (2012). The protein kinase Akt1 regulates the interferon response through phosphorylation of the transcriptional repressor EMSY. Proc. Natl. Acad. Sci. U. S. A. 109, E613–E621. doi: 10.1073/pnas.1115029109
Fallon, P. G., Sasaki, T., Sandilands, A., Campbell, L. E., Saunders, S. P., Mangan, N. E., et al. (2009). A homozygous frameshift mutation in the mouse Flg gene facilitates enhanced percutaneous allergen priming. Nat. Genet. 41, 602–608. doi: 10.1038/ng.358
Fattouh, R., Midence, N. G., Arias, K., Johnson, J. R., Walker, T. D., Goncharova, S., et al. (2008). Transforming growth factor-beta regulates house dust mite-induced allergic airway inflammation but not airway remodeling. Am. J. Respir. Crit. Care Med. 177, 593–603. doi: 10.1164/rccm.200706-958OC
Faubion, W. A., Perrault, J., Burgart, L. J., Zein, N. N., Clawson, M., and Freese, D. K. (1998). Treatment of eosinophilic esophagitis with inhaled corticosteroids. J. Pediatr. Gastroenterol. Nutr. 27, 90–93. doi: 10.1097/00005176-199807000-00016
Ferreira, M. A., Matheson, M. C., Duffy, D. L., Marks, G. B., Hui, J., Le Souëf, P., et al. (2011). Identification of IL6R and chromosome 11q13.5 as risk loci for asthma. Lancet 378, 1006–1014. doi: 10.1016/S0140-6736(11)60874-X
Fillon, S., Robinson, Z. D., Colgan, S. P., and Furuta, G. T. (2009). Epithelial function in eosinophilic gastrointestinal diseases. Immunol. Allergy Clin. N. Am. 29, 171–178. doi: 10.1016/j.iac.2008.09.003
FitzGerald, J. M., Bleecker, E. R., Nair, P., Korn, S., Ohta, K., Lommatzsch, M., et al. (2016). Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet 388, 2128–2141. doi: 10.1016/S0140-673631322-8
Fogg, M. I., Ruchelli, E., and Spergel, J. M. (2003). Pollen and eosinophilic esophagitis. J. Allergy Clin. Immunol. 112, 796–797. doi: 10.1016/s0091-6749(03)01715-9
Forssmann, U., Uguccioni, M., Loetscher, P., Dahinden, C. A., Langen, H., Thelen, M., et al. (1997). Eotaxin-2, a novel CC chemokine that is selective for the chemokine receptor CCR3, and acts like eotaxin on human eosinophil and basophil leukocytes. J. Exp. Med. 185, 2171–2176. doi: 10.1084/jem.185.12.2171
Franciosi, J. P., Hommel, K. A., DeBrosse, C. W., Greenberg, A. B., Greenler, A. J., Abonia, J. P., et al. (2012). Quality of life in paediatric eosinophilic oesophagitis: what is important to patients? Child Care Health Dev. 38, 477–483. doi: 10.1111/j.1365-2214.2011.01265.x
Franciosi, J. P., Tam, V., Liacouras, C. A., and Spergel, J. M. (2009). A case-control study of sociodemographic and geographic characteristics of 335 children with eosinophilic esophagitis. Clin. Gastroenterol. Hepatol. 7, 415–419. doi: 10.1016/j.cgh.2008.10.006
Frazzoni, M., Penagini, R., Frazzoni, L., de Bortoli, N., Mauro, A., Tolone, S., et al. (2019). Role of Reflux in the Pathogenesis of Eosinophilic Esophagitis: comprehensive Appraisal With Off- and On PPI Impedance-pH Monitoring. Am. J. Gastroenterol. 114, 1606–1613. doi: 10.14309/ajg.0000000000000379
Frischmeyer-Guerrerio, P. A., Guerrerio, A. L., Oswald, G., Chichester, K., Myers, L., Halushka, M. K., et al. (2013). TGF receptor mutations impose a strong predisposition for human allergic disease. Sci. Transl. Med. 5, ra194–ra195. doi: 10.1126/scitranslmed.3006448
Fritz, J., Lerner, D., and Suchi, M. (2018). Herpes Simplex Virus Esophagitis in Immunocompetent Children: a Harbinger of Eosinophilic Esophagitis? J. Pediatr. Gastroenterol. Nutr. 66, 609–613. doi: 10.1097/MPG.0000000000001748
Fuentebella, J., Patel, A., Nguyen, T., Sanjanwala, B., Berquist, W., Kerner, J. A., et al. (2010). Increased number of regulatory T cells in children with eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 51, 283–289. doi: 10.1097/MPG.0b013e3181e0817b
Fujiwara, Y., Tanaka, F., Sawada, A., Nadatani, Y., Nagami, Y., Taira, K., et al. (2021). A case series of sublingual immunotherapy-induced eosinophilic esophagitis: stop or spit. Clin. J. Gastroenterol. 14, 1607–1611. doi: 10.1007/s12328-021-01520-5
Fukasawa, H., Yamamoto, T., Suzuki, H., Togawa, A., Ohashi, N., Fujigaki, Y., et al. (2004). Treatment with anti-TGF-beta antibody ameliorates chronic progressive nephritis by inhibiting Smad/TGF-beta signaling. Kidney Int. 65, 63–74. doi: 10.1111/j.1523-1755.2004.00393.x
Fukuda, M. (2016). Multiple Roles of VARP in Endosomal Trafficking: rabs, Retromer Components and R-SNARE VAMP7 Meet on VARP. Traffic 17, 709–719. doi: 10.1111/tra.12406
Furuta, K., Adachi, K., Aimi, M., Ishimura, N., Sato, S., Ishihara, S., et al. (2013). Case-control study of association of eosinophilic gastrointestinal disorders with Helicobacter pylori infection in Japan. J. Clin. Biochem. Nutr. 53, 60–62. doi: 10.3164/jcbn.13-15
Gabay, C., Fautrel, B., Rech, J., Spertini, F., Feist, E., Kötter, I., et al. (2018). Open-label, multicentre, dose-escalating phase II clinical trial on the safety and efficacy of tadekinig alfa (IL-18BP) in adult-onset Still’s disease. Ann. Rheum. Dis. 77, 840–847. doi: 10.1136/annrheumdis-2017-212608
Geering, B., Stoeckle, C., Conus, S., and Simon, H. U. (2013). Living and dying for inflammation: neutrophils, eosinophils, basophils. Trends Immunol. 34, 398–409. doi: 10.1016/j.it.2013.04.002
Gleich, G. J., Adolphson, C. R., and Leiferman, K. M. (1993). The biology of the eosinophilic leukocyte. Annu. Rev. Med. 44, 85–101.
Gleich, G. J., Frigas, E., Loegering, D. A., Wassom, D. L., and Steinmuller, D. (1979). Cytotoxic properties of the eosinophil major basic protein. J. Immunol. 123, 2925–2927.
Gonzalez-Cervera, J., and Lucendo, A. J. (2016). Eosinophilic esophagitis: an evidence-based approach to therapy. J. Investig. Allergol. Clin. Immunol. 26, 8–18. doi: 10.18176/jiaci.0002
Gonzalo, J. A., Lloyd, C. M., Wen, D., Albar, J. P., Wells, T. N., Proudfoot, A., et al. (1998). The coordinated action of CC chemokines in the lung orchestrates allergic inflammation and airway hyperresponsiveness. J. Exp. Med. 188, 157–167. doi: 10.1084/jem.188.1.157
Goyal, R. K., and Rattan, S. (1978). Neurohumoral, hormonal, and drug receptors for the lower esophageal sphincter. Gastroenterology 74, 598–619. doi: 10.1016/0016-5085(78)90304-9
Granada, M., Wilk, J. B., Tuzova, M., Strachan, D. P., Weidinger, S., Albrecht, E., et al. (2012). A genome-wide association study of plasma total IgE concentrations in the Framingham Heart Study. J. Allergy Clin. Immunol. 129, 840–845.e21. doi: 10.1016/j.jaci.2011.09.029
Grandinetti, T., Biedermann, L., Bussmann, C., Straumann, A., and Hruz, P. (2019). Eosinophilic Gastroenteritis: clinical Manifestation, Natural Course, and Evaluation of Treatment with Corticosteroids and Vedolizumab. Dig. Dis. Sci. 64, 2231–2241. doi: 10.1007/s10620-019-05617-3
Grozdanovic, M., Laffey, K. G., Abdelkarim, H., Hitchinson, B., Harijith, A., Moon, H. G., et al. (2019). Novel peptide nanoparticle-biased antagonist of CCR3 blocks eosinophil recruitment and airway hyperresponsiveness. J. Allergy Clin. Immunol. 143, 669–680.e12. doi: 10.1016/j.jaci.2018.05.003
Guarino, M. P. L., Cicala, M., and Behar, J. (2016). Eosinophilic esophagitis: new insights in pathogenesis and therapy. World J. Gastrointest. Pharmacol. Ther. 7, 66–77. doi: 10.4292/wjgpt.v7.i1.66
Gupta, S. K., Fitzgerald, J. F., Kondratyuk, T., and Hogen Esch, H. (2006). Cytokine expression in normal and inflamed oesophageal mucosa: a study into the pathogenesis of allergic eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 42, 22–26. doi: 10.1097/01.mpg.0000188740.38757.d2
Hammad, H., de Heer, H. J., Soullié, T., Angeli, V., Trottein, F., Hoogsteden, H. C., et al. (2004). Activation of peroxisome proliferator-activated receptor-gamma in dendritic cells inhibits the development of eosinophilic airway inflammation in a mouse model of asthma. Am. J. Pathol. 164, 263–271. doi: 10.1016/s0002-944063116-1
Hao, L. X., Lu, Y., Li, T., and Gong, B. (2021). A meta-analysis of efficacy of topical steroids in eosinophilic esophagitis: from the perspective of histologic, clinical, and endoscopic outcome. Gastroenterol. Hepatol. 44, 251–260. doi: 10.1016/j.gastrohep.2020.07.010
He, S. H., Zhang, H. Y., Zeng, X. N., Chen, D., and Yang, P. C. (2013). Mast cells and basophils are essential for allergies: mechanisms of allergic inflammation and a proposed procedure for diagnosis. Acta Pharmacol. Sin. 34, 1270–1283. doi: 10.1038/aps.2013.88
Henderson, C. J., Ngeow, J., Collins, M. H., Martin, L. J., Putnam, P. E., Abonia, J. P., et al. (2014). Increased prevalence of eosinophilic gastrointestinal disorders in pediatric PTEN hamartoma tumor syndromes. J. Pediatr. Gastroenterol. Nutr. 58, 553–560. doi: 10.1097/MPG.0000000000000253
Hernandez-Quiles, M., Broekema, M. F., and Kalkhoven, E. (2021). PPARgamma in Metabolism, Immunity, and Cancer: unified and Diverse Mechanisms of Action. Front. Endocrinol. 12:624112. doi: 10.3389/fendo.2021.624112
Hirano, I., Collins, M. H., Assouline-Dayan, Y., Evans, L., Gupta, S., Schoepfer, A. M., et al. (2019). RPC4046, a Monoclonal Antibody Against IL13, Reduces Histologic and Endoscopic Activity in Patients With Eosinophilic Esophagitis. Gastroenterology 156, 592–603.e10. doi: 10.1053/j.gastro.2018.10.051
Hirano, I., Dellon, E. S., Hamilton, J. D., Collins, M. H., Peterson, K., Chehade, M., et al. (2020). Efficacy of Dupilumab in a Phase 2 Randomized Trial of Adults With Active Eosinophilic Esophagitis. Gastroenterology 158, 111–122.e10. doi: 10.1053/j.gastro.2019.09.042
Hiremath, G., Shilts, M. H., Boone, H. H., Correa, H., Acra, S., Tovchigrechko, A., et al. (2019). The Salivary Microbiome Is Altered in Children With Eosinophilic Esophagitis and Correlates With Disease Activity. Clin. Transl. Gastroenterol. 10:e00039. doi: 10.14309/ctg.0000000000000039
Hirota, T., Takahashi, A., Kubo, M., Tsunoda, T., Tomita, K., Sakashita, M., et al. (2012). Genome-wide association study identifies eight new susceptibility loci for atopic dermatitis in the Japanese population. Nat. Genet. 44, 1222–1226. doi: 10.1038/ng.2438
Holvoet, S., Doucet-Ladevèze, R., Perrot, M., Barretto, C., Nutten, S., and Blanchard, C. (2016). Beneficial effect of Lactococcus lactis NCC 2287 in a murine model of eosinophilic esophagitis. Allergy 71, 1753–1761. doi: 10.1111/all.12951
Hruz, P. (2014). Epidemiology of eosinophilic esophagitis. Dig. Dis. 32, 40–47. doi: 10.1159/000357008
Hruz, P., Straumann, A., Bussmann, C., Heer, P., Simon, H. U., Zwahlen, M., et al. (2011). Escalating incidence of eosinophilic esophagitis: a 20-year prospective, population-based study in Olten County, Switzerland. J. Allergy Clin. Immunol. 128, 1349–1350.e5. doi: 10.1016/j.jaci.2011.09.013
Hsieh, L. Y., Chiang, A. W. T., Duong, L. D., Kuo, C. C., Dong, S. X., Dohil, R., et al. (2021). unique esophageal extracellular matrix proteome alters normal fibroblast function in severe eosinophilic esophagitis. J. Allergy Clin. Immunol. 148, 486–494. doi: 10.1016/j.jaci.2021.01.023
Hsu Blatman, K. S., Gonsalves, N., Hirano, I., and Bryce, P. J. (2011). Expression of mast cell-associated genes is upregulated in adult eosinophilic esophagitis and responds to steroid or dietary therapy. J. Allergy Clin. Immunol. 127, 1307–1308.e3. doi: 10.1016/j.jaci.2010.12.1118
Huang, H., Zheng, Y., Li, L., Shi, W., Zhang, R., Liu, H., et al. (2020). The roles of post-translational modifications and coactivators of STAT6 signaling in tumor growth and progression. Future Med. Chem. 12, 1945–1960. doi: 10.4155/fmc-2020-0224
Huang, J. T., Welch, J. S., Ricote, M., Binder, C. J., Willson, T. M., Kelly, C., et al. (1999). Interleukin-4-dependent production of PPAR-gamma ligands in macrophages by 12/15-lipoxygenase. Nature 400, 378–382. doi: 10.1038/22572
Iglesia, E. G. A., Commins, S. P., and Dellon, E. S. (2021). Complete remission of eosinophilic esophagitis with multi-aeroallergen subcutaneous immunotherapy: a case report. J. Allergy Clin. Immunol. Pract. 9, 2517–2519.e2. doi: 10.1016/j.jaip.2021.01.045
Isomoto, H., Wang, A., Mizuta, Y., Akazawa, Y., Ohba, K., Omagari, K., et al. (2003). Elevated levels of chemokines in esophageal mucosa of patients with reflux esophagitis. Am. J. Gastroenterol. 98, 551–556. doi: 10.1111/j.1572-0241.2003.07303.x
Iwakura, N., Fujiwara, Y., Tanaka, F., Tanigawa, T., Yamagami, H., Shiba, M., et al. (2015). Basophil infiltration in eosinophilic oesophagitis and proton pump inhibitor-responsive oesophageal eosinophilia. Aliment. Pharmacol. Ther. 41, 776–784. doi: 10.1111/apt.13141
Jensen, E. T., and Dellon, E. S. (2018). Environmental factors and eosinophilic esophagitis. J. Allergy Clin. Immunol. 142, 32–40. doi: 10.1016/j.jaci.2018.04.015
Johnston, L. K., and Bryce, P. J. (2017). Understanding Interleukin 33 and Its Roles in Eosinophil Development. Front. Med. 4:51. doi: 10.3389/fmed.2017.00051
Johnston, L. K., Hsu, C. L., Krier-Burris, R. A., Chhiba, K. D., Chien, K. B., McKenzie, A., et al. (1950). (2016) IL-33 precedes IL-5 in regulating eosinophil commitment and is required for eosinophil homeostasis. J. Immunol. 197, 3445–3453. doi: 10.4049/jimmunol.1600611
Judd, L. M., Heine, R. G., Menheniott, T. R., Buzzelli, J., O’Brien-Simpson, N., Pavlic, D., et al. (2016). Elevated IL-33 expression is associated with pediatric eosinophilic esophagitis, and exogenous IL-33 promotes eosinophilic esophagitis development in mice. Am. J. Physiol. Gastrointest. Liver Physiol. 310, G13–G25. doi: 10.1152/ajpgi.00290.2015
Jyonouchi, S., Smith, C. L., Saretta, F., Abraham, V., Ruymann, K. R., Modayur-Chandramouleeswaran, P., et al. (2013). Invariant natural killer T cells in children with eosinophilic esophagitis. Clin. Exp. Allergy 44, 58–68. doi: 10.1111/cea.12201
Kagalwalla, A. F., Akhtar, N., Woodruff, S. A., Rea, B. A., Masterson, J. C., Mukkada, V., et al. (2012). Eosinophilic esophagitis: epithelial mesenchymal transition contributes to esophageal remodeling and reverses with treatment. J. Allergy Clin. Immunol. 129, 1387–1396.e7. doi: 10.1016/j.jaci.2012.03.005
Kagalwalla, A. F., Sentongo, T. A., Ritz, S., Hess, T., Nelson, S. P., Emerick, K. M., et al. (2006). Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis. Clin. Gastroenterol. Hepatol. 4, 1097–1102. doi: 10.1016/j.cgh.2006.05.026
Kagalwalla, A. F., Wechsler, J. B., Amsden, K., Schwartz, S., Makhija, M., Olive, A., et al. (2017). Efficacy of a 4-Food Elimination Diet for Children With Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 15, 1698–1707.e7. doi: 10.1016/j.cgh.2017.05.048
Kalluri, R., and Weinberg, R. A. (2009). The basics of epithelial-mesenchymal transition. J. Clin. Invest. 119, 1420–1428.
Karpathiou, G., Papoudou-Bai, A., Ferrand, E., Dumollard, J. M., and Peoc’h, M. (2021). STAT6: a review of a signaling pathway implicated in various diseases with a special emphasis in its usefulness in pathology. Pathol. Res. Pract. 223:153477. doi: 10.1016/j.prp.2021.153477
Kasagi, Y., Dods, K., Wang, J. X., Chandramouleeswaran, P. M., Benitez, A. J., Gambanga, F., et al. (2019). Fibrostenotic eosinophilic esophagitis might reflect epithelial lysyl oxidase induction by fibroblast-derived TNF-α. J. Allergy Clin. Immunol. 144, 171–182. doi: 10.1016/j.jaci.2018.10.067
Katzka, D. A., Ravi, K., Geno, D. M., Smyrk, T. C., Iyer, P. G., Alexander, J. A., et al. (2015). Endoscopic Mucosal Impedance Measurements Correlate With Eosinophilia and Dilation of Intercellular Spaces in Patients With Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 13, 1242–1248.e1. doi: 10.1016/j.cgh.2014.12.032
Katzka, D. A., Tadi, R., Smyrk, T. C., Katarya, E., Sharma, A., Geno, D. M., et al. (2014). Effects of topical steroids on tight junction proteins and spongiosis in esophageal epithelia of patients with eosinophilic esophagitis. Clin. Gastroenterol. Hepatol. 12, 1824–1829.e1. doi: 10.1016/j.cgh.2014.02.039
Kc, K., Rothenberg, M. E., and Sherrill, J. D. (2015). In vitro model for studying esophageal epithelial differentiation and allergic inflammatory responses identifies keratin involvement in eosinophilic esophagitis. PLoS One 10:e0127755. doi: 10.1371/journal.pone.0127755
Kelly, K. J., Lazenby, A. J., Rowe, P. C., Yardley, J. H., Perman, J. A., and Sampson, H. A. (1995). Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology 109, 1503–1512. doi: 10.1016/0016-5085(95)90637-1
Kelsen, S. G., Agache, I. O., Soong, W., Israel, E., Chupp, G. L., Cheung, D. S., et al. (2021). Astegolimab (anti-ST2) efficacy and safety in adults with severe asthma: a randomized clinical trial. J. Allergy Clin. Immunol. 148, 790–798. doi: 10.1016/j.jaci.2021.03.044
Kennedy, M. K., and Park, L. S. (1996). Characterization of interleukin-15 (IL-15) and the IL-15 receptor complex. J. Clin. Immunol. 16, 134–143. doi: 10.1007/BF01540911
Kim, H. P., Reed, C. C., Herfarth, H. H., and Dellon, E. S. (2018). Vedolizumab treatment may reduce steroid burden and improve histology in patients with eosinophilic gastroenteritis. Clin. Gastroenterol. Hepatol. 16, 1992–1994. doi: 10.1016/j.cgh.2018.03.024
Kim, N., Cao, W., Song, I. S., Kim, C. Y., Sohn, U. D., Harnett, K. M., et al. (1998). Leukotriene D4-induced contraction of cat esophageal and lower esophageal sphincter circular smooth muscle. Gastroenterology 115, 919–928. doi: 10.1016/s0016-508570264-1
Kim, S. R., Charos, A., Damsky, W., Heald, P., Girardi, M., and King, B. A. (2018). Treatment of generalized deep morphea and eosinophilic fasciitis with the Janus kinase inhibitor tofacitinib. JAAD Case Rep. 4, 443–445. doi: 10.1016/j.jdcr.2017.12.003
King, B., Lee, A. I., and Choi, J. (2017). Treatment of hypereosinophilic syndrome with cutaneous involvement with the JAK inhibitors tofacitinib and ruxolitinib. J. Invest. Dermatol. 137, 951–954. doi: 10.1016/j.jid.2016.10.044
Kitaura, M., Suzuki, N., Imai, T., Takagi, S., Suzuki, R., Nakajima, T., et al. (1999). Molecular cloning of a novel human CC chemokine (Eotaxin-3) that is a functional ligand of CC chemokine receptor 3. J. Biol. Chem. 274, 27975–27980. doi: 10.1074/jbc.274.39.27975
Kiwamoto, T., Kawasaki, N., Paulson, J. C., and Bochner, B. S. (2012). Siglec-8 as a drugable target to treat eosinophil and mast cell-associated conditions. Pharmacol. Ther. 135, 327–336. doi: 10.1016/j.pharmthera.2012.06.005
Kleuskens, M. T. A., Haasnoot, M. L., Herpers, B. M., van Ampting, M. T. J., Bredenoord, A. J., Garssen, J., et al. (2021). Butyrate and propionate restore interleukin 13-compromised esophageal epithelial barrier function. Allergy [Online ahead of print] doi: 10.1111/all.15069
Klion, A. D., Ackerman, S. J., and Bochner, B. S. (2020). Contributions of Eosinophils to Human Health and Disease. Annu. Rev. Pathol. 15, 179–209. doi: 10.1146/annurev-pathmechdis-012419-032756
Kolbeck, R., Kozhich, A., Koike, M., Peng, L., Andersson, C. K., Damschroder, M. M., et al. (2010). MEDI-563, a humanized anti-IL-5 receptor alpha mAb with enhanced antibody-dependent cell-mediated cytotoxicity function. J. Allergy Clin. Immunol. 125, 1344–1353.e2. doi: 10.1016/j.jaci.2010.04.004
Kottyan, L. C., Davis, B. P., Sherrill, J. D., Liu, K., Rochman, M., Kaufman, K., et al. (2014). Genome-wide association analysis of eosinophilic esophagitis provides insight into the tissue specificity of this allergic disease. Nat. Genet. 46, 895–900. doi: 10.1038/ng.3033
Kottyan, L. C., Trimarchi, M. P., Lu, X., Caldwell, J. M., Maddox, A., Parameswaran, S., et al. (2021). Replication and meta-analyses nominate numerous eosinophilic esophagitis risk genes. J. Allergy Clin. Immunol. 147, 255–266. doi: 10.1016/j.jaci.2020.10.018
Krishnamurthy, P., Sherrill, J. D., Parashette, K., Goenka, S., Rothenberg, M. E., Gupta, S., et al. (2014). Correlation of increased PARP14 and CCL26 expression in biopsies from children with eosinophilic esophagitis. J. Allergy Clin. Immunol. 133, 577–580. doi: 10.1016/j.jaci.2013.09.031
Laserna-Mendieta, E. J., Casabona, S., Savarino, E., Perelló, A., Pérez-Martínez, I., Guagnozzi, D., et al. (2020). Efficacy of Therapy for Eosinophilic Esophagitis in Real-World Practice. Clin. Gastroenterol. Hepatol. 18, 2903–2911.e4. doi: 10.1016/j.cgh.2020.01.024
Laviolette, M., Gossage, D. L., Gauvreau, G., Leigh, R., Olivenstein, R., Katial, R., et al. (2013). Effects of benralizumab on airway eosinophils in asthmatic patients with sputum eosinophilia. J Allergy Clin. Immunol. 132, 1086–1096.e5. doi: 10.1016/j.jaci.2013.05.020
Leber, A., Hontecillas, R., Zoccoli-Rodriguez, V., Ehrich, M., Davis, J., Chauhan, J., et al. (2019). Nonclinical Toxicology and Toxicokinetic Profile of an Oral Lanthionine Synthetase C-Like 2 (LANCL2) Agonist, BT-11. Int. J. Toxicol. 38, 96–109. doi: 10.1177/1091581819827509
Lehmann, J. M., Moore, L. B., Smith-Oliver, T. A., Wilkison, W. O., Willson, T. M., and Kliewer, S. A. (1995). An antidiabetic thiazolidinedione is a high affinity ligand for peroxisome proliferator-activated receptor gamma (PPAR gamma). J. Biol. Chem. 270, 12953–12956. doi: 10.1074/jbc.270.22.12953
Lenti, M. V., Savarino, E., Mauro, A., Penagini, R., Racca, F., Ghisa, M., et al. (2021). Diagnostic delay and misdiagnosis in eosinophilic oesophagitis. Dig. Liver Dis. 53, 1632–1639. doi: 10.1016/j.dld.2021.05.017
Lewis, R. A., Austen, K. F., and Soberman, R. J. (1990). Leukotrienes and other products of the 5-lipoxygenase pathway. Biochemistry and relation to pathobiology in human diseases. N. Engl. J. Med. 323, 645–655. doi: 10.1056/NEJM199009063231006
Lexmond, W. S., Neves, J. F., Nurko, S., Olszak, T., Exley, M. A., Blumberg, R. S., et al. (2014). Involvement of the iNKT cell pathway is associated with early-onset eosinophilic esophagitis and response to allergen avoidance therapy. Am. J. Gastroenterol. 109, 646–657. doi: 10.1038/ajg.2014.12
Li, G., Ma, D., and Chen, Y. (2016). Cellular functions of programmed cell death 5. Biochim. Biophys. Acta 1863, 572–580. doi: 10.1016/j.bbamcr.2015.12.021
Liacouras, C. A., Furuta, G. T., Hirano, I., Atkins, D., Attwood, S. E., Bonis, P. A., et al. (2011). Eosinophilic esophagitis: updated consensus recommendations for children and adults. J. Allergy Clin. Immunol. 128, 3–20.e6. doi: 10.1016/j.jaci.2011.02.040
Liacouras, C. A., Spergel, J. M., Ruchelli, E., Verma, R., Mascarenhas, M., Semeao, E., et al. (2005). Eosinophilic esophagitis: a 10-year experience in 381 children. Clin. Gastroenterol. Hepatol. 3, 1198–1206. doi: 10.1016/s1542-356500885-2
Liacouras, C. A., Wenner, W. J., Brown, K., and Ruchelli, E. (1998). Primary eosinophilic esophagitis in children: successful treatment with oral corticosteroids. J. Pediatr. Gastroenterol. Nutr. 26, 380–385. doi: 10.1097/00005176-199804000-00004
Lieberman, J. A., Zhang, J., Whitworth, J., and Cavender, C. (2018). A randomized, double-blinded, placebo-controlled study of the use of viscous oral cromolyn sodium for the treatment of eosinophilic esophagitis. Ann. Allergy Asthma Immunol. 120, 527–531. doi: 10.1016/j.anai.2018.03.006
Li-Kim-Moy, J. P., Tobias, V., Day, A. S., Leach, S., and Lemberg, D. A. (2011). Esophageal subepithelial fibrosis and hyalinization are features of eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 52, 147–153. doi: 10.1097/MPG.0b013e3181ef37a1
Lim, D. M., Narasimhan, S., Michaylira, C. Z., and Wang, M. L. (2009). TLR3-mediated NF- B signaling in human esophageal epithelial cells. Am. J. Physiol. Gastrointest. Liver Physiol. 297, G1172–G1180. doi: 10.1152/ajpgi.00065.2009
Lim, E. J., Lu, T. X., Blanchard, C., and Rothenberg, M. E. (2011). Epigenetic regulation of the IL-13-induced human eotaxin-3 gene by CREB-binding protein-mediated histone 3 acetylation. J. Biol. Chem. 286, 13193–13204. doi: 10.1074/jbc.M110.210724
Loizou, D., Enav, B., Komlodi-Pasztor, E., Hider, P., Kim-Chang, J., Noonan, L., et al. (2015). A pilot study of omalizumab in eosinophilic esophagitis. PLoS One 10:e0113483. doi: 10.1371/journal.pone.0113483
Lucendo, A. J., Arias, Á, De Rezende, L. C., Yagüe-Compadre, J. L., Mota-Huertas, T., González-Castillo, S., et al. (2011a). Subepithelial collagen deposition, profibrogenic cytokine gene expression, and changes after prolonged fluticasone propionate treatment in adult eosinophilic esophagitis: a prospective study. J. Allergy Clin. Immunol. 128, 1037–1046. doi: 10.1016/j.jaci.2011.08.007
Lucendo, A. J., Arias, A., and Molina-Infante, J. (2016). Efficacy of proton pump inhibitor drugs for inducing clinical and histologic remission in patients with symptomatic esophageal eosinophilia: a systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 14, 13–22. doi: 10.1016/j.cgh.2015.07.041
Lucendo, A. J., Arias, A., and Tenias, J. M. (2014). Relation between eosinophilic esophagitis and oral immunotherapy for food allergy: a systematic review with meta-analysis. Ann. Allergy Asthma Immunol. 113, 624–629. doi: 10.1016/j.anai.2014.08.004
Lucendo, A. J., De Rezende, L. C., Jiménez-Contreras, S., Yagüe-Compadre, J. L., González-Cervera, J., Mota-Huertas, T., et al. (2011b). Montelukast was inefficient in maintaining steroid-induced remission in adult eosinophilic esophagitis. Dig. Dis. Sci. 56, 3551–3558. doi: 10.1007/s10620-011-1775-y
Lucendo, A. J., De Rezende, L., Comas, C., Caballero, T., and Bellón, T. (2008). Treatment with topical steroids downregulates IL-5, Eotaxin-1/CCL11, and eotaxin-3/CCL26 gene expression in eosinophilic esophagitis. Am. J. Gastroenterol. 103, 2184–2193. doi: 10.1111/j.1572-0241.2008.01937.x
Lucendo, A. J., Molina-Infante, J., Arias, Á, von Arnim, U., Bredenoord, A. J., Bussmann, C., et al. (2017). Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol. J. 5, 335–358. doi: 10.1177/2050640616689525
Lucendo, A. J., Navarro, M., Comas, C., Pascual, J. M., Burgos, E., Santamaria, L., et al. (2007). Immunophenotypic characterization and quantification of the epithelial inflammatory infiltrate in eosinophilic esophagitis through stereology. Am. J. Surg. Pathol. 31, 598–606. doi: 10.1097/01.pas.0000213392.49698.8c
Luster, A. D., and Rothenberg, M. E. (1997). Role of the monocyte chemoattractant protein and eotaxin subfamily of chemokines in allergic inflammation. J. Leukoc. Biol. 62, 620–633. doi: 10.1002/jlb.62.5.620
Lyles, J., and Rothenberg, M. (2019). Role of genetics, environment, and their interactions in the pathogenesis of eosinophilic esophagitis. Curr. Opin. Immunol. 60, 46–53. doi: 10.1016/j.coi.2019.04.004
Ma, J., Altomare, A., Guarino, M., Cicala, M., Rieder, F., Fiocchi, C., et al. (2012). HCl-induced and ATP-dependent upregulation of TRPV1 receptor expression and cytokine production by human esophageal epithelial cells. Am. J. Physiol. Gastrointest. Liver Physiol. 303, G635–G645. doi: 10.1152/ajpgi.00097.2012
MacDonald, J. K., and McDonald, J. W. (2007). Natalizumab for induction of remission in Crohn’s disease. Cochrane Database Syst. Rev. 1:CD006097.
Manresa, M. C., Chiang, A. W. T., Kurten, R. C., Dohil, R., Brickner, H., Dohil, L., et al. (2020). Increased Production of LIGHT by T Cells in Eosinophilic Esophagitis Promotes Differentiation of Esophageal Fibroblasts Toward an Inflammatory Phenotype. Gastroenterology 159, 1778–1792.e13. doi: 10.1053/j.gastro.2020.07.035
Marietta, E. V., Geno, D. M., Smyrk, T. C., Becker, A., Alexander, J. A., Camilleri, M., et al. (2017). Presence of intraepithelial food antigen in patients with active eosinophilic oesophagitis. Aliment Pharmacol. Ther. 45, 427–433. doi: 10.1111/apt.13877
Markowitz, J. E., Jobe, L., Miller, M., Frost, C., Laney, Z., and Eke, R. (2018). Safety and efcacy of Reslizumab for children and adolescents with eosinophilic esophagitis treated for 9 Years. J. Pediatr. Gastroenterol. Nutr. 66, 893–897. doi: 10.1097/MPG.0000000000001840
Markowitz, J. E., Spergel, J. M., Ruchelli, E., and Liacouras, C. A. (2003). Elemental diet is an effective treatment for eosinophilic esophagitis in children and adolescents. Am. J. Gastroenterol. 98, 777–782. doi: 10.1111/j.1572-0241.2003.07390.x
Masuda, A., Matsuguchi, T., Yamaki, K., Hayakawa, T., Kubo, M., LaRochelle, W. J., et al. (2000). Interleukin-15 induces rapid tyrosine phosphorylation of STAT6 and the expression of interleukin-4 in mouse mast cells. J. Biol. Chem. 275, 29331–29337. doi: 10.1074/jbc.M910290199
Masuelli, L., Tumino, G., Turriziani, M., Modesti, A., and Bei, R. (2010). Topical use of sucralfate in epithelial wound healing: clinical evidences and molecular mechanisms of action. Recent Pat. Inflamm. Allergy Drug Discov. 4, 25–36. doi: 10.2174/187221310789895649
McCormick, L. L., Zhang, Y., Tootell, E., and Gilliam, A. C. (1999). Anti–TGF-beta treatment prevents skin and lung fibrosis in murine sclerodermatous graft-versus-host disease: a model for human scleroderma. J. Immunol. 163, 5693–5699.
McCormick, M. L., Roeder, T. L., Railsback, M. A., and Britigan, B. E. (1994). Eosinophil peroxidase-dependent hydroxyl radical generation by human eosinophils. J. Biol. Chem. 269, 27914–27919. doi: 10.1016/s0021-9258(18)46874-3
McKie, E. A., Reid, J. L., Mistry, P. C., DeWall, S. L., Abberley, L., Ambery, P. D., et al. (2016). Study to Investigate the Efficacy and Safety of an Anti-Interleukin-18 Monoclonal Antibody in the Treatment of Type 2 Diabetes Mellitus. PLoS One 11:e0150018. doi: 10.1371/journal.pone.0150018
McMillan, S. J., Xanthou, G., and Lloyd, C. M. (2005). Manipulation of allergen-induced airway remodeling by treatment with anti–TGF-beta antibody: effect on the Smad signaling pathway. J. Immunol. 174, 5774–5780. doi: 10.4049/jimmunol.174.9.5774
Mendoza Alvarez, L. B., Liu, X., and Glover, S. (2019). Treatment-resistant eosinophilic oesophagitis successfully managed with tofacitinib. BMJ Case Rep. 12:1. doi: 10.1136/bcr-2019-232558
Mennini, M., Tambucci, R., Riccardi, C., Rea, F., De Angelis, P., Fiocchi, A., et al. (2021). Eosinophilic Esophagitis and Microbiota: state of the Art. Front. Immunol. 12:595762. doi: 10.3389/fimmu.2021.595762
Merves, J., Chandramouleeswaran, P. M., Benitez, A. J., Muir, A. B., Lee, A. J., Lim, D. M., et al. (2015). Altered esophageal histamine receptor expression in Eosinophilic Esophagitis (EoE): implications on disease pathogenesis. PLoS One 10:e0114831. doi: 10.1371/journal.pone.0114831
Miehlke, S., Alpan, O., Schröder, S., and Straumann, A. (2013). Induction of eosinophilic esophagitis by sublingual pollen immunotherapy. Case Rep. Gastroenterol. 7, 363–368. doi: 10.1159/000355161
Miller, D. E., Forney, C., Rochman, M., Cranert, S., Habel, J., Rymer, J., et al. (2019). Genetic, Inflammatory, and Epithelial Cell Differentiation Factors Control Expression of Human Calpain-14. G3 9, 729–736. doi: 10.1534/g3.118.200901
Mishra, A., and Rothenberg, M. E. (2003). Intratracheal IL-13 induces eosinophilic esophagitis by an IL-5, eotaxin-1, and STAT6-dependent mechanism. Gastroenterology 125, 1419–1427. doi: 10.1016/j.gastro.2003.07.007
Mishra, A., Hogan, S. P., Brandt, E. B., and Rothenberg, M. E. (2001). An etiological role for aeroallergens and eosinophils in experimental esophagitis. J. Clin. Invest. 107, 83–90. doi: 10.1172/JCI10224
Mishra, A., Schlotman, J., Wang, M., and Rothenberg, M. E. (2007). Critical role for adaptive T cell immunity in experimental eosinophilic esophagitis in mice. J. Leukoc. Biol. 81, 916–924. doi: 10.1189/jlb.1106653
Mishra, A., Wang, M., Pemmaraju, V. R., Collins, M. H., Fulkerson, P. C., Abonia, J. P., et al. (2008). Esophageal remodeling develops as a consequence of tissue specific IL-5-induced eosinophilia. Gastroenterology 134, 204–214. doi: 10.1053/j.gastro.2007.10.002
Mitson-Salazar, A., Yin, Y., Wansley, D. L., Young, M., Bolan, H., Arceo, S., et al. (2016). Hematopoietic prostaglandin D synthase defines a proeosinophilic pathogenic effector human T(H)2 cell subpopulation with enhanced function. J. Allergy Clin. Immunol. 137, 907–918.e9. doi: 10.1016/j.jaci.2015.08.007
Mjosberg, J. M., Trifari, S., Crellin, N. K., Peters, C. P., van Drunen, C. M., Piet, B., et al. (2011). Human IL-25- and IL-33-responsive type 2 innate lymphoid cells are defined by expression of CRTH2 and CD161. Nat. Immunol. 12, 1055–1062. doi: 10.1038/ni.2104
Moawad, F. J., Schoepfer, A. M., Safroneeva, E., Ally, M. R., Chen, Y. J., Maydonovitch, C. L., et al. (2014). Eosinophilic oesophagitis and proton pump inhibitor-responsive oesophageal eosinophilia have similar clinical, endoscopic and histological findings. Aliment. Pharmacol. Ther. 39, 603–608. doi: 10.1111/apt.12636
Moawad, F. J., Wells, J. M., Johnson, R. L., Reinhardt, B. J., Maydonovitch, C. L., and Baker, T. P. (2015). Comparison of eotaxin-3 biomarker in patients with eosinophilic oesophagitis, proton pump inhibitor-responsive oesophageal eosinophilia and gastro-oesophageal reflux disease. Aliment. Pharmacol. Ther. 42, 231–238. doi: 10.1111/apt.13258
Molina-Infante, J., Arias, Á, Alcedo, J., Garcia-Romero, R., Casabona-Frances, S., Prieto-Garcia, A., et al. (2018a). Step-up empiric elimination diet for pediatric and adult eosinophilic esophagitis: the 2-4-6 study. J. Allergy Clin. Immunol. 141, 1365–1372. doi: 10.1016/j.jaci.2017.08.038
Molina-Infante, J., Gutierrez-Junquera, C., Savarino, E., Penagini, R., Modolell, I., Bartolo, O., et al. (2018b). Helicobacter pylori infection does not protect against eosinophilic esophagitis: results from a large multicenter case-control study. Am. J. Gastroenterol. 113, 972–979. doi: 10.1038/s41395-018-0035-6
Molina-Infante, J., Rivas, M. D., Hernandez-Alonso, M., Vinagre-Rodríguez, G., Mateos-Rodríguez, J. M., Dueñas-Sadornil, C., et al. (2014). Proton pump inhibitor-responsive oesophageal eosinophilia correlates with downregulation of eotaxin-3 and Th2 cytokines overexpression. Aliment. Pharmacol. Ther. 40, 955–965. doi: 10.1111/apt.12914
Mougey, E. B., Nguyen, V., Gutiérrez-Junquera, C., Fernández-Fernández, S., Cilleruelo, M. L., Rayo, A., et al. (2021). STAT6 Variants Associate With Relapse of Eosinophilic Esophagitis in Patients Receiving Long-term Proton Pump Inhibitor Therapy. Clin. Gastroenterol. Hepatol. 19, 2046–2053.e2. doi: 10.1016/j.cgh.2020.08.020
Mueller, S., Aigner, T., Neureiter, D., and Stolte, M. (2006). Eosinophil infiltration and degranulation in oesophageal mucosa from adult patients with eosinophilic oesophagitis: a retrospective and comparative study on pathological biopsy. J. Clin. Pathol. 59, 1175–1180. doi: 10.1136/jcp.2005.031922
Muir, A. B., Dods, K., Henry, S. J., Benitez, A. J., Lee, D., Whelan, K. A., et al. (2016). Eosinophilic Esophagitis-Associated Chemical and Mechanical Microenvironment Shapes Esophageal Fibroblast Behavior. J. Pediatr. Gastroenterol. Nutr. 63, 200–209. doi: 10.1097/MPG.0000000000001100
Muir, A. B., Lim, D. M., Benitez, A. J., Modayur Chandramouleeswaran, P., Lee, A. J., Ruchelli, E. D., et al. (2013). Esophageal epithelial and mesenchymal cross-talk leads to features of epithelial to mesenchymal transition in vitro. Exp. Cell Res. 319, 850–859. doi: 10.1016/j.yexcr.2012.12.002
Muir, A. B., Wang, J. X., and Nakagawa, H. (2019). Epithelial-stromal crosstalk and fibrosis in eosinophilic esophagitis. J. Gastroenterol. 54, 10–18. doi: 10.1007/s00535-018-1498-3
Mukkada, V. A., and Furuta, G. T. (2014). Management of refractory eosinophilic esophagitis. Dig. Dis. 32, 134–138. doi: 10.1159/000357296
Mukkada, V. A., Haas, A., Maune, N. C., Capocelli, K. E., Henry, M., Gilman, N., et al. (2010). Feeding dysfunction in children with eosinophilic gastrointestinal diseases. Pediatrics 126, e672–e677. doi: 10.1542/peds.2009-2227
Mulder, D. J., Mak, N., Hurlbut, D. J., and Justinich, C. J. (2012). Atopic and non-atopic eosinophilic oesophagitis are distinguished by immunoglobulin E-bearing intraepithelial mast cells. Histopathology 61, 810–822. doi: 10.1111/j.1365-2559.2012.4303.x
Mulder, D. J., Pacheco, I., Hurlbut, D. J., Mak, N., Furuta, G. T., MacLeod, R. J., et al. (2008). FGF9-induced proliferative response to eosinophilic inflammation in oesophagitis. Gut 58, 166–173. doi: 10.1136/gut.2008.157628
Mulder, D. J., Pooni, A., Mak, N., Hurlbut, D. J., Basta, S., and Justinich, C. J. (2011). Antigen presentation and MHC class II expression by human esophageal epithelial cells. Am. J. Pathol. 178, 744–753. doi: 10.1016/j.ajpath.2010.10.027
Nakajima, N., Sato, H., Takahashi, K., Hasegawa, G., Mizuno, K., Hashimoto, S., et al. (2017). Muscle layer histopathology and manometry pattern of primary esophageal motility disorders including achalasia. Neurogastroenterol. Motil. 29:e12968. doi: 10.1111/nmo.12968
Nakanishi, K., Yoshimoto, T., Tsutsui, H., and Okamura, H. (2001). Interleukin-18 regulates both Th1 and Th2 responses. Annu. Rev. Immunol. 19, 423–474. doi: 10.1146/annurev.immunol.19.1.423
Namjou, B., Marsolo, K., Caroll, R. J., Denny, J. C., Ritchie, M. D., Verma, S. S., et al. (2014). Phenome-wide association study (PheWAS) in EMR-linked pediatric cohorts, genetically links PLCL1 to speech language development and IL5-IL13 to Eosinophilic Esophagitis. Front. Genet. 5:401. doi: 10.3389/fgene.2014.00401
Navarro, P., Laserna-Mendieta, E. J., Guagnozzi, D., Casabona, S., Perelló, A., Savarino, E., et al. (2021). Proton pump inhibitor therapy reverses endoscopic features of fibrosis in eosinophilic esophagitis. Dig. Liver Dis. 53, 1479–1485. doi: 10.1016/j.dld.2021.05.025
Neighbour, H., Boulet, L. P., Lemiere, C., Sehmi, R., Leigh, R., Sousa, A. R., et al. (2014). Safety and efficacy of an oral CCR3 antagonist in patients with asthma and eosinophilic bronchitis: a randomized, placebo-controlled clinical trial. Clin. Exp. Allergy 44, 508–516. doi: 10.1111/cea.12244
Nennstiel, S., Bajbouj, M., Becker, V., Slotta-Huspenina, J., Wagenpfeil, S., Schmid, R. M., et al. (2016). High-resolution manometry in patients with eosinophilic esophagitis under topical steroid therapy-a prospective observational study (HIMEOS-study). Neurogastroenterol. Motil. 28, 599–607. doi: 10.1111/nmo.12753
Netzer, P., Gschossmann, J. M., Straumann, A., Sendensky, A., Weimann, R., and Schoepfer, A. M. (2007). Corticosteroid-dependent eosinophilic oesophagitis: azathioprine and 6-mercaptopurine can induce and maintain long-term remission. Eur. J. Gastroenterol. Hepatol. 19, 865–869. doi: 10.1097/MEG.0b013e32825a6ab4
Nguyen, N., Fernando, S. D., Biette, K. A., Hammer, J. A., Capocelli, K. E., Kitzenberg, D. A., et al. (2018). TGF-β1 alters esophageal epithelial barrier function by attenuation of claudin-7 in eosinophilic esophagitis. Mucosal Immunol. 11, 415–426. doi: 10.1038/mi.2017.72
Nguyen, N., Furuta, G. T., and Masterson, J. C. (2016). Deeper than the epithelium: role of matrix and fibroblasts in pediatric and adult eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 63, 168–169. doi: 10.1097/MPG.0000000000001183
Nhu, Q. M., Chiao, H., Moawad, F. J., Bao, F., and Konijeti, G. G. (2018). The Anti-α4β7 Integrin Therapeutic Antibody for Inflammatory Bowel Disease, Vedolizumab, Ameliorates Eosinophilic Esophagitis: a Novel Clinical Observation. Am. J. Gastroenterol. 113, 1261–1263. doi: 10.1038/s41395-018-0145-1
Nhu, Q. M., Hsieh, L., Dohil, L., Dohil, R., Newbury, R. O., Kurten, R., et al. (2020). Antifibrotic Effects of the Thiazolidinediones in Eosinophilic Esophagitis Pathologic Remodeling: a Preclinical Evaluation. Clin. Transl. Gastroenterol. 11:e00164. doi: 10.14309/ctg.0000000000000164
Nicholson, A. G., Li, D., Pastorino, U., Goldstraw, P., and Jeffery, P. K. (1997). Full thickness eosinophilia in oesophageal leiomyomatosis and idiopathic eosinophilic oesophagitis. A common allergic inflammatory profile? J. Pathol. 183, 233–236. doi: 10.1002/(SICI)1096-9896(199710)183:2<233::AID-PATH936>3.0.CO;2-Z
Nilsson, C., Scurlock, A. M., Dellon, E. S., Brostoff, J. M., Pham, T., Ryan, R., et al. (2021). Onset of eosinophilic esophagitis during a clinical trial program of oral immunotherapy for peanut allergy. J. Allergy Clin. Immunol. Pract. 9, 4496–4501. doi: 10.1016/j.jaip.2021.07.048
Niranjan, R., Mavi, P., Rayapudi, M., Dynda, S., and Mishra, A. (2013). Pathogenic role of mast cells in experimental eosinophilic esophagitis. Am. J. Physiol. Gastrointest. Liver Physiol. 304, G1087–G1094. doi: 10.1152/ajpgi.00070.2013
Niranjan, R., Rajavelu, P., Ventateshaiah, S. U., Shukla, J. S., Zaidi, A., Mariswamy, S. J., et al. (2015). Involvement of interleukin-18 in the pathogenesis of human eosinophilic esophagitis. Clin. Immunol. 157, 103–113. doi: 10.1016/j.clim.2015.01.007
Noel, R. J., Putnam, P. E., and Rothenberg, M. E. (2004). Eosinophilic esophagitis. N. Engl. J. Med. 351, 940–941.
Noti, M., Wojno, E. D., Kim, B. S., Siracusa, M. C., Giacomin, P. R., Nair, M. G., et al. (2013). Thymic stromal lymphopoietin-elicited basophil responses promote eosinophilic esophagitis. Nat. Med. 19, 1005–1013. doi: 10.1038/nm.3281
O’Byrne, P. M., Inman, M. D., and Parameswaran, K. (2001). The trials and tribulations of IL-5, eosinophils, and allergic asthma. J. Allergy Clin. Immunol. 108, 503–508. doi: 10.1067/mai.2001.119149
Oo, K. K., Kamolhan, T., Soni, A., Thongchot, S., Mitrpant, C., O-Charoenrat, P., et al. (2021). Development of an engineered peptide antagonist against periostin to overcome doxorubicin resistance in breast cancer. BMC Cancer 21:65. doi: 10.1186/s12885-020-07761-w
O’Regan, G. M., Sandilands, A., McLean, W. H. I., and Irvine, A. D. (2009). Filaggrin in atopic dermatitis. J. Allergy Clin. Immunol. 124, R2–R6. doi: 10.1016/j.jaci.2009.07.013
Orlando, R. C., and Powel, D. W. (1984). Effect of sucralfate on esophageal epithelial resistance to acid in the rabbit. Gastroenterology 86:1201A.
Otani, I. M., Anilkumar, A. A., Newbury, R. O., Bhagat, M., Beppu, L. Y., Dohil, R., et al. (2013). Anti–IL-5 therapy reduces mast cell and IL-9 cell numbers in pediatric patients with eosinophilic esophagitis. J. Allergy Clin. Immunol. 131, 1576–1582. doi: 10.1016/j.jaci.2013.02.042
Oyoshi, M. K., Larson, R. P., Ziegler, S. F., and Geha, R. S. (2010). Mechanical injury polarizes skin dendritic cells to elicit a TH2 response by inducing cutaneous thymic stromal lymphopoietin expression. J. Allergy Clin. Immunol. 126, 976–984.e1–5. doi: 10.1016/j.jaci.2010.08.041
Paluel-Marmont, C., Bellon, N., Barbet, P., Leclerc-Mercier, S., Hadj-Rabia, S., Dupont, C., et al. (2017). Eosinophilic esophagitis and colonic mucosal eosinophilia in Netherton syndrome. J. Allergy Clin. Immunol. 139, 2003–2005.e1. doi: 10.1016/j.jaci.2016.10.045
Panch, S. R., Bozik, M. E., Brown, T., Makiya, M., Prussin, C., Archibald, D. G., et al. (2018). Dexpramipexole as an oral steroid-sparing agent in hypereosinophilic syndromes. Blood 132, 501–509. doi: 10.1182/blood-2018-02-835330
Patel, D. A., and Vaezi, M. F. (2017). Utility of esophageal mucosal impedance as a diagnostic test for esophageal disease. Curr. Opin. Gastroenterol. 33, 277–284. doi: 10.1097/MOG.0000000000000367
Pérez-Jeldres, T., Tyler, C. J., Boyer, J. D., Karuppuchamy, T., Yarur, A., Giles, D. A., et al. (2019). Targeting Cytokine Signaling and Lymphocyte Traffic via Small Molecules in Inflammatory Bowel Disease: JAK Inhibitors and S1PR Agonists. Front. Pharmacol. 10:212. doi: 10.3389/fphar.2019.00212
Pesek, R. D., and Gupta, S. K. (2019). Future Therapies for Eosinophilic Gastrointestinal Disorders. Ann. Allergy Asthma Immunol. 124, 219–226. doi: 10.1016/j.anai.2019.11.018
Peterson, K. A., Byrne, K. R., Vinson, L. A., Ying, J., Boynton, K. K., Fang, J. C., et al. (2013). Elemental diet induces histologic response in adult eosinophilic esophagitis. Am. J. Gastroenterol. 108, 759–766. doi: 10.1038/ajg.2012.468
Pettipher, R., Hansel, T. T., and Armer, R. (2007). Antagonism of the prostaglandin D2 receptors DP1 and CRTH2 as an approach to treat allergic diseases. Nat. Rev. Drug Discov. 6, 313–325. doi: 10.1038/nrd2266
Philpott, H., Nandurkar, S., Royce, S. G., Thien, F., and Gibson, P. R. (2016). Allergy tests do not predict food triggers in adult patients with eosinophilic oesophagitis. A comprehensive prospective study using five modalities. Aliment Pharmacol. Ther. 44, 223–233. doi: 10.1111/apt.13676
Picker, L. J., and Butcher, E. C. (1992). Physiological and molecular mechanisms of lymphocyte homing. Annu. Rev. Immunol. 10, 561–591. doi: 10.1146/annurev.iy.10.040192.003021
Platten, M., Wild-Bode, C., Wick, W., Leitlein, J., Dichgans, J., and Weller, M. (2001). N-[3,4-dimethoxycinnamoyl]-anthranilic acid (tranilast) inhibits transforming growth factor-beta relesase and reduces migration and invasiveness of human malignant glioma cells. Int. J. Cancer 93, 53–61. doi: 10.1002/ijc.1289
Politi, E., Angelakopoulou, A., Grapsa, D., Zande, M., Stefanaki, K., Panagiotou, I., et al. (2016). Filaggrin and periostin expression is altered in eosinophilic esophagitis and normalized with treatment. J. Pediatr. Gastroenterol. Nutr. 65, 47–52. doi: 10.1097/mpg.0000000000001419
Prasad, G. A., Alexander, J. A., Schleck, C. D., Zinsmeister, A. R., Smyrk, T. C., Elias, R. M., et al. (2009). Epidemiology of eosinophilic esophagitis over three decades in Olmsted County, Minnesota. Clin. Gastroenterol. Hepatol. 7, 1055–1061. doi: 10.1016/j.cgh.2009.06.023
Qian, X., Gao, Y., Ye, X., and Lu, M. (2014). Association of STAT6 variants with asthma risk: a systematic review and meta-analysis. Hum. Immunol. 75, 847–853. doi: 10.1016/j.humimm.2014.06.007
Racca, F., Pellegatta, G., Heffler, E., Repici, A., and Canonica, G. W. (2021). Viscous Fluticasone in Eosinophilic Esophagitis: a Suitable Step Forward. Am. J. Biomed. Sci. Res. 13:AJBSR.MS.ID.001827. doi: 10.34297/AJBSR.2021.13.001827
Radano, M. C., Yuan, Q., Katz, A., Fleming, J. T., Kubala, S., Shreffler, W., et al. (2014). Cesarean section and antibiotic use found to be associated with eosinophilic esophagitis. J. Allergy Clin. Immunol. Pract. 2, 475–477.e1. doi: 10.1016/j.jaip.2014.02.018
Ram, G., Lee, J., Ott, M., Brown-Whitehorn, T. F., Cianferoni, A., Shuker, M., et al. (2015). Seasonal exacerbation of esophageal eosinophilia in children with eosinophilic esophagitis and allergic rhinitis. Ann. Allergy Asthma Immunol. 115, 224–228.e1. doi: 10.1016/j.anai.2015.07.004
Ramasamy, A., Curjuric, I., Coin, L. J., Kumar, A., McArdle, W. L., Imboden, M., et al. (2011). A genome-wide meta-analysis of genetic variants associated with allergic rhinitis and grass sensitization and their interaction with birth order. J. Allergy Clin. Immunol. 128, 996–1005. doi: 10.1016/j.jaci.2011.08.030
Ramaswamy, A. T., No, J. S., Anderson, L., Solomon, A., Ciecierega, T., Barfield, E., et al. (2019). Esophageal IgE, IgG4, and mucosal eosinophilia in individuals with dysphagia. Int. Forum Allergy Rhinol. 9, 870–875. doi: 10.1002/alr.22339
Ravelli, A. M., Villanacci, V., Ruzzenenti, N., Grigolato, P., Tobanelli, P., Klersy, C., et al. (2006). Dilated intercellular spaces. J. Pediatr. Gastroenterol. Nutr. 42, 510–515. doi: 10.1097/01.mpg.0000215312.78664.b9
Ravensberg, A. J., Ricciardolo, F. L., van Schadewijk, A., Rabe, K. F., Sterk, P. J., Hiemstra, P. S., et al. (2005). Eotaxin-2 and eotaxin-3 expression is associated with persistent eosinophilic bronchial inflammation in patients with asthma after allergen challenge. J. Allergy Clin. Immunol. 115, 779–785. doi: 10.1016/j.jaci.2004.11.045
Ravi, A., Marietta, E. V., Geno, D. M., Alexander, J. A., Murray, J. A., and Katzka, D. A. (2019). Penetration of the Esophageal Epithelium by Dust Mite Antigen in Patients With Eosinophilic Esophagitis. Gastroenterology 157, 255–256. doi: 10.1053/j.gastro.2019.02.042
Rawson, R., Anilkumar, A., Newbury, R. O., Bafna, V., Aquino, M., Palmquist, J., et al. (2015). The TGFbeta1 promoter SNP C-509T and food sensitization promote esophageal remodeling in pediatric eosinophilic esophagitis. PLoS One 10:e0144651. doi: 10.1371/journal.pone.0144651
Rawson, R., Yang, T., Newbury, R. O., Aquino, M., Doshi, A., Bell, B., et al. (2016). TGF-beta1-induced PAI-1 contributes to a profibrotic network in patients with eosinophilic esophagitis. J. Allergy Clin. Immunol. 138, 791–800.e4. doi: 10.1016/j.jaci.2016.02.028
Rayapudi, M., Mavi, P., Zhu, X., Pandey, A. K., Abonia, J. P., Rothenberg, M. E., et al. (2010). Indoor insect allergens are potent inducers of experimental eosinophilic esophagitis in mice. J. Leukoc. Biol. 88, 337–346. doi: 10.1189/jlb.0110025
Rayapudi, M., Rajavelu, P., Zhu, X., Kaul, A., Niranjan, R., Dynda, S., et al. (2014). Invariant natural killer T-cell neutralization is a possible novel therapy for human eosinophilic esophagitis. Clin. Transl. Immunol. 3:e9. doi: 10.1038/cti.2013.13
Reed, C. C., Iglesia, E. G. A., Commins, S. P., and Dellon, E. S. (2019). Seasonal exacerbation of eosinophilic esophagitis histologic activity in adults and children implicates role of aeroallergens. Ann. Allergy Asthma Immunol. 122, 296–301. doi: 10.1016/j.anai.2018.12.013
Reed, C. C., Koutlas, N. T., Robey, B. S., Hansen, J., and Dellon, E. S. (2018). Prolonged Time to Diagnosis of Eosinophilic Esophagitis Despite Increasing Knowledge of the Disease. Clin. Gastroenterol. Hepatol. 16, 1667–1669. doi: 10.1016/j.cgh.2018.01.028
Rice, L. M., Padilla, C. M., McLaughlin, S. R., Mathes, A., Ziemek, J., Goummih, S., et al. (2015). Fresolimumab treatment decreases biomarkers and improves clinical symptoms in systemic sclerosis patients. J. Clin. Invest. 125, 2795–2807. doi: 10.1172/JCI77958
Rieder, F., Nonevski, I., Ma, J., Ouyang, Z., West, G., Protheroe, C., et al. (2014). T-helper 2 cytokines, transforming growth factor β1, and eosinophil products induce fibrogenesis and alter muscle motility in patients with eosinophilic esophagitis. Gastroenterology 146, 1266–77.e1–e9. doi: 10.1053/j.gastro.2014.01.051
Rocha, R., Vitor, A. B., Trindade, E., Lima, R., Tavares, M., Lopes, J., et al. (2011). Omalizumab in the treatment of eosinophilic esophagitis and food allergy. Eur. J. Pediatr. 170, 1471–1474. doi: 10.1007/s00431-011-1540-4
Rochman, M., Travers, J., Miracle, C. E., Bedard, M. C., Wen, T., Azouz, N. P., et al. (2017). Profound loss of esophageal tissue differentiation in patients with eosinophilic esophagitis. J. Allergy Clin. Immunol. 140, 738–749.e3. doi: 10.1016/j.jaci.2016.11.042
Rokkas, T., Niv, Y., and Malfertheiner, P. (2021). A Network Meta-Analysis of Randomized Controlled Trials on the Treatment of Eosinophilic Esophagitis in Adults and Children. J. Clin. Gastroenterol. 55, 400–410. doi: 10.1097/MCG.0000000000001356
Rokosz, M., Bauer, C., and Schroeder, S. (2017). Eosinophilic esophagitis induced by aeroallergen sublingual immunotherapy in an enteral feeding tube-dependent pediatric patient. Ann. Allergy Asthma Immunol. 119, 88–89. doi: 10.1016/j.anai.2017.05.004
Roman, S., Hirano, I., Kwiatek, M. A., Gonsalves, N., Chen, J., Kahrilas, P. J., et al. (2010). Manometric features of eosinophilic esophagitis in esophageal pressure topography. Neurogastroenterol. Motil. 23, 208–e111. doi: 10.1111/j.1365-2982.2010.01633.x
Romano, C., Chiaro, A., Lucarelli, S., Santarelli, C., Cucchiara, S., Guadagnini, T., et al. (2014). Mucosal cytokine profiles in paediatric eosinophilic oesophagitis: a case-control study. Dig. Liver Dis. 46, 590–595. doi: 10.1016/j.dld.2014.03.003
Rosenberg, C. E., Mingler, M. K., Caldwell, J. M., Collins, M. H., Fulkerson, P. C., Morris, D. W., et al. (2018). Esophageal IgG4 levels correlate with histopathologic and transcriptomic features in eosinophilic esophagitis. Allergy 73, 1892–1901. doi: 10.1111/all.13486
Rosenberg, H. F., Dyer, K. D., and Foster, P. S. (2013). Eosinophils: changing perspectives in health and disease. Nat. Rev. Immunol. 13, 9–22. doi: 10.1038/nri3341
Rothenberg, M. E., Klion, A. D., Roufosse, F. E., Kahn, J. E., Weller, P. F., Simon, H. U., et al. (2008). Treatment of patients with the hypereosinophilic syndrome with mepolizumab. N. Engl. J. Med. 358, 1215–1228. doi: 10.1056/NEJMoa070812
Rothenberg, M. E., Luster, A. D., and Leder, P. (1995). Murine eotaxin: an eosinophil chemo attractant inducible in endothelial cells and in interleukin 4-induced tumor suppression. Proc. Natl. Acad. Sci. U. S. A. 92, 8960–8964. doi: 10.1073/pnas.92.19.8960
Rothenberg, M. E., Spergel, J. M., Sherrill, J. D., Annaiah, K., Martin, L. J., Cianferoni, A., et al. (2010). Common variants at 5q22 associate with pediatric eosinophilic esophagitis. Nat. Genet. 42, 289–291. doi: 10.1038/ng.547
Rothenberg, M. E., Wen, T., Greenberg, A., Alpan, O., Enav, B., Hirano, I., et al. (2015). Intravenous anti-IL-13 mAb QAX576 for the treatment of eosinophilic esophagitis. J. Allergy Clin. Immunol. 135, 500–507. doi: 10.1016/j.jaci.2014.07.049
Roufosse, F. (2018). Targeting the interleukin-5 pathway for treatment of eosinophilic conditions other than asthma. Front. Med. 5:49. doi: 10.3389/fmed.2018.00049
Rubinstein, E., Cho, J. Y., Rosenthal, P., Chao, J., Miller, M., Pham, A., et al. (2011). Siglec-F inhibition reduces esophageal eosinophilia and angiogenesis in a mouse model of eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 53, 409–416. doi: 10.1097/MPG.0b013e3182182ff8
Ruffner, M. A., Hu, A., Dilollo, J., Benocek, K., Shows, D., Gluck, M., et al. (2021). Conserved IFN Signature between Adult and Pediatric Eosinophilic Esophagitis. J. Immunol. 206, 1361–1371. doi: 10.4049/jimmunol.2000973
Ryu, S., Lee, K. H., Tizaoui, K., Terrazzino, S., Cargnin, S., Effenberger, M., et al. (2020). Pathogenesis of Eosinophilic Esophagitis: a Comprehensive Review of the Genetic and Molecular Aspects. Int. J. Mol. Sci. 21:7253. doi: 10.3390/ijms21197253
Salama, Z. A., Sadek, A., Abdelhady, A. M., Darweesh, S. K., Morsy, S. A., and Esmat, G. (2016). Losartan may inhibit the progression of liver fibrosis in chronic HCV patients. Hepatobiliary Surg. Nutr. 5, 249–255. doi: 10.21037/hbsn.2016.02.06
Sandborn, W. J., Feagan, B. G., Wolf, D. C., D’Haens, G., Vermeire, S., Hanauer, S. B., et al. (2016). Ozanimod Induction and Maintenance Treatment for Ulcerative Colitis. N. Engl. J. Med. 374, 1754–1762. doi: 10.1056/NEJMoa1513248
Sandborn, W. J., Peyrin-Biroulet, L., Zhang, J., Chiorean, M., Vermeire, S., Lee, S. D., et al. (2020). Efficacy and Safety of Etrasimod in a Phase 2 Randomized Trial of Patients With Ulcerative Colitis. Gastroenterology 158, 550–561. doi: 10.1053/j.gastro.2019.10.035
Sarbinowska, J. A., and Waśko-Czopnik, D. (2020). High-resolution manometry in diagnostics and evaluation of therapy effectiveness in patients with eosinophilic esophagitis – underestimated breakthrough or dead end? Gastroenterol. Rev. 15, 22–26. doi: 10.5114/pg.2019.83793
Sayej, W. N., Ménoret, A., Maharjan, A. S., Fernandez, M., Wang, Z., Balarezo, F., et al. (2016). Characterizing the inflammatory response in esophageal mucosal biopsies in children with eosinophilic esophagitis. Clin. Transl. Immunol. 5:e88. doi: 10.1038/cti.2016.30
Schaefer, E. T., Fitzgerald, J. F., Molleston, J. P., Croffie, J. M., Pfefferkorn, M. D., Corkins, M. R., et al. (2008). Comparison of oral prednisone and topical fluticasone in the treatment of eosinophilic esophagitis: a randomized trial in children. Clin. Gastroenterol. Hepatol. 6, 165–173. doi: 10.1016/j.cgh.2007.11.008
Schoepfer, A. M., Safroneeva, E., Bussmann, C., Kuchen, T., Portmann, S., Simon, H. U., et al. (2013). Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner. Gastroenterology 145, 1230–6.e1–2. doi: 10.1053/j.gastro.2013.08.015
Schuyler, A. J., Erwin, E. A., Oken, E., Rifas-Shiman, S., Lidholm, J., Wilson, J., et al. (2017). The diagnostic utility of serum assays for total IgG4 and specific IgG4 antibodies to cow’s milk proteins in children with eosinophilic esophagitis: comparison with an unselected birth cohort. J. Allergy Clin. Immunol. 139:AB48. doi: 10.1016/j.jaci.2016.12.108
Schuyler, A. J., Wilson, J. M., Tripathi, A., Commins, S. P., Ogbogu, P. U., Kruzsewski, P. G., et al. (2018). Specific IgG4 antibodies to cow’s milk proteins in pediatric patients with eosinophilic esophagitis. J. Allergy Clin. Immunol. 142, 139–148.e12. doi: 10.1016/j.jaci.2018.02.049
Shah, S. C., Tepler, A., Peek, R. M. Jr., Colombel, J. F., Hirano, I., and Narula, N. (2019). Association Between Helicobacter pylori Exposure and Decreased Odds of Eosinophilic Esophagitis-A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 17, 2185–2198.e3. doi: 10.1016/j.cgh.2019.01.013
Sherrill, J. D., and Rothenberg, M. E. (2011). Genetic dissection of eosinophilic esophagitis provides insight into disease pathogenesis and treatment strategies. J. Allergy Clin. Immunol. 128, 23–32. doi: 10.1016/j.jaci.2011.03.046
Sherrill, J. D., and Rothenberg, M. E. (2014). Genetic and epigenetic underpinnings of eosinophilic esophagitis. Gastroenterol. Clin. North Am. 43, 269–280. doi: 10.1016/j.gtc.2014.02.003
Sherrill, J. D., Gao, P. S., Stucke, E. M., Blanchard, C., Collins, M. H., Putnam, P. E., et al. (2010). Variants of thymic stromal lymphopoietin and its receptor associate with eosinophilic esophagitis. J. Allergy Clin. Immunol. 126, 160–165.e3. doi: 10.1016/j.jaci.2010.04.037
Sherrill, J. D., Kc, K., Wu, D., Djukic, Z., Caldwell, J. M., Stucke, E. M., et al. (2014a). Desmoglein-1 regulates esophageal epithelial barrier function and immune responses in eosinophilic esophagitis. Mucosal Immunol. 7, 718–729. doi: 10.1038/mi.2013.90
Sherrill, J. D., Kiran, K. C., Blanchard, C., Stucke, E. M., Kemme, K. A., Collins, M. H., et al. (2014b). Analysis and expansion of the eosinophilic esophagitis transcriptome by RNA sequencing. Genes Immun. 15, 361–369. doi: 10.1038/gene.2014.27
Shi, Y., Liu, X. F., Zhuang, Y., Zhang, J. Y., Liu, T., Yin, Z., et al. (2010). Helicobacter pylori-induced Th17 responses modulate Th1 cell responses, benefit bacterial growth, and contribute to pathology in mice. J. Immunol. 184, 5121–5129. doi: 10.4049/jimmunol.0901115
Shukla, A., Mishra, A., Venkateshaiah, S. U., Manohar, M., Mahadevappa, C. P., and Mishra, A. (2015). Elements involved in promoting eosinophilic gastrointestinal disorders. J. Genet. Syndr. Gene Ther. 6:2. doi: 10.4172/2157-7412.1000265
Silva, F. M. C. E., de Oliveira, E. E., Ambrósio, M. G. E., Ayupe, M. C., de Souza, V. P., Menegati, L. M., et al. (2020). Disodium cromoglycate treatment reduces TH2 immune response and immunohistopathological features in a murine model of Eosinophilic Esophagitis. Int. Immunopharmacol. 83:106422. doi: 10.1016/j.intimp.2020.106422
Siracusa, M. C., Saenz, S. A., Hill, D. A., Kim, B. S., Headley, M. B., Doering, T. A., et al. (2011). TSLP promotes interleukin-3-independent basophil haematopoiesis and type 2 inflammation. Nature 477, 229–233. doi: 10.1038/nature10329
Slae, M., Persad, R., Leung, A. J.-T., Gabr, R., Brocks, D., and Huynh, H. Q. (2015). Role of environmental factors in the development of pediatric eosinophilic esophagitis. Dig. Dis. Sci. 60, 3364–3372. doi: 10.1007/s10620-015-3740-7
Sleiman, P. M., Wang, M. L., Cianferoni, A., Aceves, S., Gonsalves, N., Nadeau, K., et al. (2014). GWAS identifies four novel eosinophilic esophagitis loci. Nat. Commun. 5:5593. doi: 10.1038/ncomms6593
Smelter, D. F., Sathish, V., Thompson, M. A., Pabelick, C. M., Vassallo, R., and Prakash, Y. S. (2010). Thymic stromal lymphopoietin in cigarette smoke-exposed human airway smooth muscle. J. Immunol. 185, 3035–3040. doi: 10.4049/jimmunol.1000252
Snider, P., Hinton, R. B., Moreno-Rodriguez, R. A., Wang, J., Rogers, R., Lindsley, A., et al. (2008). Periostin is required for maturation and extracellular matrix stabilization of noncardiomyocyte lineages of the heart. Circ. Res. 102, 752–760. doi: 10.1161/circresaha.107.159517
Soler, D., Chapman, T., Yang, L. L., Wyant, T., Egan, R., and Fedyk, E. R. (2009). The binding specificity and selective antagonism of vedolizumab, an anti-alpha4beta7 integrin therapeutic antibody in development for inflammatory bowel diseases. J. Pharmacol. Exp. Ther. 330, 864–875. doi: 10.1124/jpet.109.153973
Soon, I. S., Butzner, J. D., Kaplan, G. G., and deBruyn, J. C. (2013). Incidence and prevalence of eosinophilic esophagitis in children. J. Pediatr. Gastroenterol. Nutr. 57, 72–80. doi: 10.1097/MPG.0b013e318291fee2
South, A. P., Ives, J. H., James, C. H., Nizetic, D., Cabral, A., Mirza, G., et al. (1999). Human epidermal differentiation complex in a single 2.5 Mbp long continuum of overlapping DNA cloned in bacteria integrating physical and transcript maps. J. Investig. Dermatol. 112, 910–918. doi: 10.1046/j.1523-1747.1999.00613.x
Spechler, S. J., Genta, R. M., and Souza, R. F. (2007). Thoughts on the complex relationship between gastroesophageal reflux disease and eosinophilic esophagitis. Am. J. Gastroenterol. 102, 1301–1306. doi: 10.1111/j.1572-0241.2007.01179.x
Spechler, S., Konda, V., and Souza, R. (2018). Can eosinophilic esophagitis cause Achalasia and other esophageal Motility disorders? Am. J. Gastroenterol. 113, 1594–1599. doi: 10.1038/s41395-018-0240-3
Spergel, J. M., Brown-Whitehorn, T. F., Cianferoni, A., Shuker, M., Wang, M. L., Verma, R., et al. (2012a). Identification of causative foods in children with eosinophilic esophagitis treated with an elimination diet. J. Allergy Clin. Immunol. 130, 461–467. doi: 10.1016/j.jaci.2012.05.021
Spergel, J. M., Dellon, E. S., Liacouras, C. A., Hirano, I., Molina-Infante, J., Bredenoord, A. J., et al. (2018). Summary of the updated international consensus diagnostic criteria for eosinophilic esophagitis: AGREE conference. Ann. Allergy Asthma Immunol. 121, 281–284. doi: 10.1016/j.anai.2018.05.035
Spergel, J. M., Elci, O. U., Muir, A. B., Liacouras, C. A., Wilkins, B. J., Burke, D., et al. (2020). Efficacy of Epicutaneous Immunotherapy in Children With Milk-Induced Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 18, 328–336.e7. doi: 10.1016/j.cgh.2019.05.014
Spergel, J. M., Muir, A. B., Liacouras, C. A., Burke, D., Lewis, M. O., Brown-Whitehorn, T., et al. (2021). Sustained milk consumption after 2 years post-milk epicutaneous immunotherapy for eosinophilic esophagitis. Allergy 76, 1573–1576. doi: 10.1111/all.14659
Spergel, J. M., Rothenberg, M. E., Collins, M. H., Furuta, G. T., Markowitz, J. E., and Fuchs, G. III, et al. (2012b). Reslizumab in children and adolescents with eosinophilic esophagitis: results of a double-blind, randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 129, 456–63.e1–3. doi: 10.1016/j.jaci.2011.11.044
Squier, C. A., and Kremer, M. J. (2001). Biology of oral mucosa and esophagus. J. Natl. Cancer Inst. Monogr. 29, 7–15. doi: 10.1093/oxfordjournals.jncimonographs.a003443
Squires, K. A., Cameron, D. J., Oliver, M., and da Fonseca Junqueira, J. C. (2009). Herpes simplex and eosinophilic oesophagitis: the chicken or the egg? J. Pediatr. Gastroenterol. Nutr. 49, 246–250. doi: 10.1097/MPG.0b013e31817b5b73
Stein, M. L., Collins, M. H., Villanueva, J. M., Kushner, J. P., Putnam, P. E., Buckmeier, B. K., et al. (2006). Anti-IL-5 (mepolizumab) therapy for eosinophilic esophagitis. J. Allergy Clin. Immunol. 118, 1312–1319. doi: 10.1016/j.jaci.2006.09.007
Straumann, A., Bauer, M., Fischer, B., Blaser, K., and Simon, H. U. (2001). Idiopathic eosinophilic esophagitis is associated with a T(H)2-type allergic inflammatory response. J. Allergy Clin. Immunol. 108, 954–961. doi: 10.1067/mai.2001.119917
Straumann, A., Blanchard, C., Radonjic-Hoesli, S., Bussmann, C., Hruz, P., Safroneeva, E., et al. (2016). A new eosinophilic esophagitis (EoE)-like disease without tissue eosinophilia found in EoE families. Allergy 71, 889–900. doi: 10.1111/all.12879
Straumann, A., Bussmann, C., Conus, S., Beglinger, C., and Simon, H. U. (2008). Anti-TNF-alpha (infliximab) therapy for severe adult eosinophilic esophagitis. J. Allergy Clin. Immunol. 122, 425–427. doi: 10.1016/j.jaci.2008.06.012
Straumann, A., Conus, S., Degen, L., Felder, S., Kummer, M., Engel, H., et al. (2010a). Budesonide is effective in adolescent and adult patients with active eosinophilic esophagitis. Gastroenterology 139, 1526–1537.e1. doi: 10.1053/j.gastro.2010.07.048
Straumann, A., Conus, S., Grzonka, P., Kita, H., Kephart, G., Bussmann, C., et al. (2010b). Anti-interleukin-5 antibody treatment (mepolizumab) in active eosinophilic oesophagitis: a randomised, placebo-controlled, double-blind trial. Gut 59, 21–30. doi: 10.1136/gut.2009.178558
Straumann, A., Hoesli, S., Bussmann, C. H., Stuck, M., Perkins, M., Collins, L. P., et al. (2013). Anti-eosinophil activity and clinical efficacy of the CRTH2 antagonist OC000459 in eosinophilic esophagitis. Allergy 68, 375–385. doi: 10.1111/all.12096
Stuck, M. C., Straumann, A., and Simon, H. U. (2011). Relative lack of T regulatory cells in adult eosinophilic esophagitis: no normalization after corticosteroid therapy. Allergy 66, 705–707. doi: 10.1111/j.1398-9995.2010.02525.x
Sugita, K., Kabashima, K., Sakabe, J., Yoshiki, R., Tanizaki, H., and Tokura, Y. (2010). FTY720 regulates bone marrow egress of eosinophils and modulates late-phase skin reaction in mice. Am. J. Pathol. 177, 1881–1887. doi: 10.2353/ajpath.2010.100119
Sun, X., Ma, S. F., Wade, M. S., Flores, C., Pino-Yanes, M., Moitra, J., et al. (2010). Functional variants of the sphingosine-1-phosphate receptor 1 gene associate with asthma susceptibility. J. Allergy Clin. Immunol. 126, 241–249.e1–e3. doi: 10.1016/j.jaci.2010.04.036
Szatmari, I., Gogolak, P., Im, J. S., Dezso, B., Rajnavolgyi, E., and Nagy, L. (2004). Activation of PPARgamma specifies a dendritic cell subtype capable of enhanced induction of iNKT cell expansion. Immunity 21, 95–106. doi: 10.1016/j.immuni.2004.06.003
Taft, T. H., and Mutlu, E. A. (2018). The potential role of vedolizumab in concomitant eosinophilic esophagitis and Crohn’s disease. Clin. Gastroenterol. Hepatol. 16, 1840–1841. doi: 10.1016/j.cgh.2018.06.022
Tagaya, Y., Burton, J. D., Miyamoto, Y., and Waldmann, T. A. (1996). Identification of a novel receptor/signal transduction pathway for IL-15/T in mast cells. EMBO J. 15, 4928–4939. doi: 10.1002/j.1460-2075.1996.tb00873.x
Talley, N. J., Kephart, G. M., McGovern, T. W., Carpenter, H. A., and Gleich, G. J. (1992). Deposition of eosinophil granule major basic protein in eosinophilic gastroenteritis and celiac disease. Gastroenterology 103, 137–145. doi: 10.1016/0016-5085(92)91106-e
Tamura, K., Ohbayashi, N., Ishibashi, K., and Fukuda, M. (2011). Structure-function analysis of VPS9-ankyrin-repeat protein (Varp) in the trafficking of tyrosinase-related protein 1 in melanocytes. J. Biol. Chem. 286, 7507–7521. doi: 10.1074/jbc.M110.191205
Tantibhaedhyangkul, U., Tatevian, N., Gilger, M. A., Major, A. M., and Davis, C. M. (2009). Increased esophageal regulatory T cells and eosinophil characteristics in children with eosinophilic esophagitis and gastroesophageal reflux disease. Ann. Clin. Lab Sci. 39, 99–107.
Teitelbaum, J. E., Fox, V. L., Twarog, F. J., Nurko, S., Antonioli, D., Gleich, G., et al. (2002). Eosinophilic esophagitis in children: immunopathological analysis and response to fluticasone propionate. Gastroenterology 122, 1216–1225. doi: 10.1053/gast.2002.32998
Terrados, S., Villafana, L., Antolín-Amérigo, D., Camarero, C., Martínez-Botas, J., Sánchez-Ruano, L., et al. (2020). Effectiveness of allergy testing in milk induced eosinophilic esophagitis. Description and follow-up of patients. Allergol. Immunopathol. 48, 576–581. doi: 10.1016/j.aller.2020.05.006
Tobey, N. A., Hosseini, S. S., Argote, C. M., Dobrucali, A. M., Awayda, M. S., and Orlando, R. C. (2004). Dilated intercellular spaces and shunt permeability in nonerosive acid-damaged esophageal epithelium. Am. J. Gastroenterol. 99, 13–22. doi: 10.1046/j.1572-0241.2003.04018.x
Tramacere, I., Del Giovane, C., Salanti, G., D’Amico, R., and Filippini, G. (2015). Immunomodulators and immunosuppressants for relapsingremitting multiple sclerosis: a network meta-analysis. Cochrane Database Syst. Rev. 9:CD011381.
Travers, J., Rochman, M., Wen, T., and Rothenberg, M. E. (2016). IL-33 is selectively expressed by esophageal basal layer epithelial cells during allergic inflammation. J. Allergy Clin. Immunol. 137:AB228. doi: 10.1016/j.jaci.2015.12.879
Tripp, C. S., Cuff, C., Campbell, A. L., Hendrickson, B. A., Voss, J., Melim, T., et al. (2017). RPC4046, A Novel Anti-interleukin-13 Antibody, Blocks IL-13 Binding to IL-13 α1 and α2 Receptors: a Randomized, Double-Blind, Placebo-Controlled, Dose-Escalation First-in-Human Study. Adv. Ther. 34, 1364–1381. doi: 10.1007/s12325-017-0525-8
Tsutsui, H., Yoshimoto, T., Hayashi, N., Mizutani, H., and Nakanishi, K. (2004). Induction of allergic inflammation by interleukin-18 in experimental animal models. Immunol. Rev. 202, 115–138. doi: 10.1111/j.0105-2896.2004.00205.x
Untersmayr, E., and Jensen-Jarolim, E. (2006). The effect of gastric digestion on food allergy. Curr. Opin. Allergy Clin. Immunol. 6, 214–219. doi: 10.1097/01.all.0000225163.06016.93
Upparahalli Venkateshaiah, S., Rayapudi, M., Kandikattu, H. K., Yadavalli, C. S., and Mishra, A. (2021). Blood mRNA levels of T cells and IgE receptors are novel non-invasive biomarkers for eosinophilic esophagitis (EoE). Clin. Immunol. 227:108752. doi: 10.1016/j.clim.2021.108752
Vaclavkova, A., Chimenti, S., Arenberger, P., Holló, P., Sator, P. G., Burcklen, M., et al. (2014). Oral ponesimod in patients with chronic plaque psoriasis: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet 384, 2036–2045. doi: 10.1016/S0140-673660803-5
Van Gorp, H., Van Opdenbosch, N., and Lamkanfi, M. (2019). Inflammasome-Dependent Cytokines at the Crossroads of Health and Autoinflammatory Disease. Cold Spring Harb. Perspect. Biol. 11:a028563. doi: 10.1101/cshperspect.a028563
van Rhijn, B. D., Oors, J. M., Smout, A. J., and Bredenoord, A. J. (2014b). Prevalence of esophageal motility abnormalities increases with longer disease duration in adult patients with eosinophilic esophagitis. Neurogastroenterol. Motil. 26, 1349–1355. doi: 10.1111/nmo.12400
van Rhijn, B. D., Smout, A. J. P. M., and Bredenoord, A. J. (2014a). Disease duration determines health-related quality of life in adult eosinophilic esophagitis patients. Neurogastroenterol. Motil. 26, 772–778. doi: 10.1111/nmo.12323
van Rhijn, B. D., Verheij, J., Smout, A. J., and Bredenoord, A. J. (2013). Rapidly increasing incidence of eosinophilic esophagitis in a large cohort. Neurogastroenterol. Motil. 25, 47–52.e5. doi: 10.1111/nmo.12009
van Rhijn, B. D., Vlieg-Boerstra, B. J., Versteeg, S. A., Akkerdaas, J. H., van Ree, R., Terreehorst, I., et al. (2015). Evaluation of allergen-microarray-guided dietary intervention as treatment of eosinophilic esophagitis. J. Allergy Clin. Immunol. 136, 1095–1097.e3. doi: 10.1016/j.jaci.2015.02.038
van Rhijn, B. D., Weijenborg, P. W., Verheij, J., van den Bergh Weerman, M. A., Verseijden, C., and van denWijngaard, R. M, et al. (2014c). Proton pump inhibitors partially restore mucosal integrity in patients with proton pump inhibitor-responsive esophageal eosinophilia but not eosinophilic esophagitis. Clin. Gastroenterol. Hepatol. 12, 1815–1823.e2. doi: 10.1016/j.cgh.2014.02.037
Venkateshaiah, S. U., Kandikattu, H. K., and Mishra, A. (2019). Significance of Interleukin (IL)-15 in IgE associated eosinophilic Esophagitis (EoE). Int. J. Basic Clin. Immunol. 2, 1–12.
Venturelli, N., Lexmond, W. S., Ohsaki, A., Nurko, S., Karasuyama, H., Fiebiger, E., et al. (2016). Allergic skin sensitization promotes eosinophilic esophagitis through the IL-33-basophil axis in mice. J. Allergy Clin. Immunol. 138, 1367–1380.e5. doi: 10.1016/j.jaci.2016.02.034
Vicario, M., Blanchard, C., Stringer, K. F., Collins, M. H., Mingler, M. K., Ahrens, A., et al. (2009). Local B cells and IgE production in the oesophageal mucosa in eosinophilic oesophagitis. Gut 59, 12–20. doi: 10.1136/gut.2009.178020
Vieth, M., Mastracci, L., Vakil, N., Dent, J., Wer- nersson, B., Baldycheva, I., et al. (2016). Epithelial thickness is a marker of gastroesophageal reflux disease. Clin. Gastroenterol. Hepatol. 14, 1544–1551. doi: 10.1016/j.cgh.2016.06.018
Voehringer, D. (2013). Protective and pathological roles of mast cells and basophils. Nat. Rev. Immunol. 13, 362–375. doi: 10.1038/nri3427
Votto, M., Marseglia, G. L., De Filippo, M., Brambilla, I., Caimmi, S. M. E., and Licari, A. (2020). Early Life Risk Factors in Pediatric EoE: could We Prevent This Modern Disease? Front. Pediatr. 8:263. doi: 10.3389/fped.2020.00263
Wang, W., Zhu, Z., Zhu, B., and Ma, Z. (2011). Peroxisome proliferator-activated receptor-gamma agonist induces regulatory T cells in a murine model of allergic rhinitis. Otolaryngol. Head Neck Surg. 144, 506–513. doi: 10.1177/0194599810396133
Warners, M. J., Terreehorst, I., van den Wijngaard, R. M., Akkerdaas, J., van Esch, B. C. A. M., van Ree, R., et al. (2018). Abnormal Responses to Local Esophageal Food Allergen Injections in Adult Patients With Eosinophilic Esophagitis. Gastroenterology 154, 57–60.e2. doi: 10.1053/j.gastro.2017.08.062
Warners, M. J., van Rhijn, B. D., Verheij, J., Smout, A. J. P. M., and Bredenoord, A. J. (2017a). Disease activity in eosinophilic esophagitis is associated with impaired esophageal barrier integrity. Am. J. Physiol. Gastrointest. Liver Physiol. 313, G230–G238. doi: 10.1152/ajpgi.00058.2017
Warners, M. J., Vlieg-Boerstra, B. J., Verheij, J., van Hamersveld, P. H. P., van Rhijn, B. D., Van Ampting, M. T. J., et al. (2017b). Esophageal and Small Intestinal Mucosal Integrity in Eosinophilic Esophagitis and Response to an Elemental Diet. Am. J. Gastroenterol. 112, 1061–1071. doi: 10.1038/ajg.2017.107
Warners, M. J., Vlieg-Boerstra, B. J., Verheij, J., van Rhijn, B. D., Van Ampting, M. T., Harthoorn, L. F., et al. (2017c). Elemental diet decreases inflammation and improves symptoms in adult eosinophilic oesophagitis patients. Aliment Pharmacol. Ther. 45, 777–787. doi: 10.1111/apt.13953
Weidlich, S., Nennstiel, S., Jesinghaus, M., Brockow, K., Slotta-Huspenina, J., Bajbouj, M., et al. (2020). IgG4 is Elevated in Eosinophilic Esophagitis but Not in Gastroesophageal Reflux Disease Patients. J. Clin. Gastroenterol. 54, 43–49. doi: 10.1097/MCG.0000000000001154
Wen, T., Aronow, B. J., Rochman, Y., Rochman, M., Kc, K., Dexheimer, P. J., et al. (2019). Single-cell RNA sequencing identifies inflammatory tissue T cells in eosinophilic esophagitis. J. Clin. Invest. 129, 2014–2028. doi: 10.1172/JCI125917
Wilson, J., Schuyler, A. J., Tripathi, A., Commins, S. P., Erwin, E. A., and Platts-Mills, T. A. E. (2017). Serum IgG4 to food proteins, but not to the barrier function proteins desmoglein 1 or 3, are increased in eosinophilic esophagitis. J. Allergy Clin. Immunol. 139:AB50. doi: 10.1016/j.jaci.2016.12.114
Winter, H. S., Madara, J. L., Stafford, R. J., Grand, R. J., Quinlan, J. E., and Goldman, H. (1982). Intraepithelial eosinophils: a new diagnostic criterion for reflux esophagitis. Gastroenterology 83, 818–823. doi: 10.1016/s0016-5085(82)80011-5
Wlodek, E., Kirkpatrick, R. B., Andrews, S., Noble, R., Schroyer, R., Scott, J., et al. (2021). pilot study evaluating GSK1070806 inhibition of interleukin-18 in renal transplant delayed graft function. PLoS One 16:e0247972. doi: 10.1371/journal.pone.0247972
Wong, C. K., Hu, S., Cheung, P. F. Y., and Lam, C. W. K. (2010). Thymic stromal lymphopoietin induces chemotactic and prosurvival effects in eosinophils. Am. J. Respir. Cell Mol. Biol. 43, 305–315. doi: 10.1165/rcmb.2009-0168oc
Wright, B. L., Fernandez-Becker, N. Q., Kambham, N., Purington, N., Cao, S., Tupa, D., et al. (2021). Gastrointestinal Eosinophil Responses in a Longitudinal, Randomized Trial of Peanut Oral Immunotherapy. Clin. Gastroenterol. Hepatol. 19, 1151–1159.e14. doi: 10.1016/j.cgh.2020.05.019
Wyant, T., Fedyk, E., and Abhyankar, B. (2016). An Overview of the mechanism of action of the monoclonal antibody vedolizumab. J. Crohns Colitis 10, 1437–1444. doi: 10.1093/ecco-jcc/jjw092
Yang, L., Lu, X., Nossa, C. W., Francois, F., Peek, R. M., and Pei, Z. (2009). Inflammation and intestinal metaplasia of the distal esophagus are associated with alterations in the microbiome. Gastroenterology 137, 588–597. doi: 10.1053/j.gastro.2009.04.046
Yen, E. H., Hornick, J. L., Dehlink, E., Dokter, M., Baker, A., Fiebiger, E., et al. (2010). Comparative analysis of FcεRI expression patterns in patients with eosinophilic and reflux esophagitis. J. Pediatr. Gastroenterol. Nutr. 51, 584–592. doi: 10.1097/MPG.0b013e3181de7685
Youngblood, B. A., Brock, E. C., Leung, J., Falahati, R., Bochner, B. S., Rasmussen, H. S., et al. (2019). Siglec-8 antibody reduces eosinophils and mast cells in a transgenic mouse model of eosinophilic gastroenteritis. JCI Insight 4:e126219. doi: 10.1172/jci.insight.126219
Younis, U. S., Vallorz, E., Addison, K. J., Ledford, J. G., and Myrdal, P. B. (2019). Preformulation and evaluation of tofacitinib as a therapeutic treatment for asthma. AAPS PharmSciTech 20:167. doi: 10.1208/s12249-019-1377-0
Žaja Franulović, O., Lesar, T., Busic, N., and Tešović, G. (2013). Herpes simplex primoinfection in an immunocompetent host with eosinophilic esophagitis. Pediatr. Int. 55, 38–41. doi: 10.1111/ped.12027
Zeisberg, M. (2008). Fibroblasts emerge via epithelial-mesenchymal transition in chronic kidney fibrosis. Front. Biosci. 13:6991. doi: 10.2741/3204
Zentilin, P., Savarino, V., Mastracci, L., Spaggiari, P., Dulbecco, P., Ceppa, P., et al. (2005). Reassessment of the diag- nostic value of histology in patients with GERD, using multiple biopsy sites and an ap- propriate control group. Am. J. Gastroenterol. 100, 2299–2306. doi: 10.1111/j.1572-0241.2005.50209.x
Zhang, S., Wu, X., and Yu, S. (2014). Prostaglandin D2 receptor D-type prostanoid receptor 2 mediates eosinophil trafficking into the esophagus. Dis. Esophagus. 27, 601–606. doi: 10.1111/dote.12118
Zhang, X., Cheng, E., Huo, X., Yu, C., Zhang, Q., Pham, T. H., et al. (2012). Omeprazole blocks STAT6 binding to the eotaxin-3 promoter in eosinophilic esophagitis cells. PLoS One 7:e50037. doi: 10.1371/journal.pone.0050037
Zhang, Y., Li, X., Fang, S., Zhu, Z., Yao, M., Ying, L., et al. (2017). Peroxisome proliferator-activated receptor γ agonist suppresses mast cell maturation and induces apoptosis. Mol. Med. Rep. 16, 1793–1800. doi: 10.3892/mmr.2017.6802
Zhu, X., Wang, M., Mavi, P., Rayapudi, M., Pandey, A. K., Kaul, A., et al. (2010). Interleukin-15 expression is increased in human eosinophilic esophagitis and mediates pathogenesis in mice. Gastroenterology 139, 182–193.e7. doi: 10.1053/j.gastro.2010.03.057
Ziegler, S. F. (2010). The role of thymic stromal lymphopoietin (TSLP) in allergic disorders. Curr. Opin. Immunol. 22, 795–799. doi: 10.1016/j.coi.2010.10.020
Ziyadeh, F. N., Hoffman, B. B., Han, D. C., Iglesias-De La Cruz, M. C., Hong, S. W., Isono, M., et al. (2000). Long-term prevention of renal insufficiency, excess matrix gene expression, and glomerular mesangial matrix expansion by treatment with monoclonal antitransforming growth factor–beta antibody in DB/DB diabetic mice. Proc. Natl. Acad. Sci. U. S. A. 97, 8015–8020. doi: 10.1073/pnas.120055097
Zukerberg, L., Mahadevan, K., Selig, M., and Deshpande, V. (2016). Oesophageal intrasquamous IgG4 deposits: an adjunctive marker to distinguish eosinophilic oesophagitis from reflux oesophagitis. Histopathology 68, 968–976. doi: 10.1111/his.12892
Keywords: eosinophilic esophagitis, type 2 inflammation, therapeutic targets, precision medicine, pathophysiology
Citation: Racca F, Pellegatta G, Cataldo G, Vespa E, Carlani E, Pelaia C, Paoletti G, Messina MR, Nappi E, Canonica GW, Repici A and Heffler E (2022) Type 2 Inflammation in Eosinophilic Esophagitis: From Pathophysiology to Therapeutic Targets. Front. Physiol. 12:815842. doi: 10.3389/fphys.2021.815842
Received: 15 November 2021; Accepted: 09 December 2021;
Published: 12 January 2022.
Edited by:
Gilda Varricchi, University of Naples Federico II, ItalyReviewed by:
Darío Antolín-Amérigo, Ramón y Cajal University Hospital, SpainCopyright © 2022 Racca, Pellegatta, Cataldo, Vespa, Carlani, Pelaia, Paoletti, Messina, Nappi, Canonica, Repici and Heffler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesca Racca, ZnJhbmNlc2NhLnJhY2NhQGh1bWFuaXRhcy5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.