
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol. , 27 August 2020
Sec. Vascular Physiology
Volume 11 - 2020 | https://doi.org/10.3389/fphys.2020.00898
This article is part of the Research Topic Vascular Health: The Endothelial Perspective in Regulation of Inflammation and Injury View all 17 articles
 Cláudia Fetter1
Cláudia Fetter1 Juliana Romeu Marques1
Juliana Romeu Marques1 Liliane Appratto de Souza1
Liliane Appratto de Souza1 Daniela Ravizzoni Dartora1,2
Daniela Ravizzoni Dartora1,2 Bruna Eibel1
Bruna Eibel1 Liliana Fortini Cavalheiro Boll1
Liliana Fortini Cavalheiro Boll1 Sílvia Noll Goldmeier1Danielle Dias3,4
Sílvia Noll Goldmeier1Danielle Dias3,4 Katia De Angelis3,4
Katia De Angelis3,4 Maria Cláudia Irigoyen1,5*
Maria Cláudia Irigoyen1,5*Background: Hypertension remains highly prevalent in postmenopausal women, along with vascular dysfunction and increased oxidative stress. In such context, regular exercises, yoga practice, and slow breathing have been recommended to treat hypertension. However, the effects of the multiple components of yoga, including the respiratory techniques involved in the practice, on hypertension and on vascular and endothelial function have never been evaluated.
Objective: This study aimed to investigate the additional effects of respiratory technique on vascular function and oxidative stress profile in hypertensive postmenopausal women (HPMWs) following yoga or stretching video classes.
Study Design: Hypertensive postmenopausal women were recruited and randomized for 12 weeks, twice a week, of supervised yoga or stretching video classes of 75 min for 12 weeks associated or not with respiratory technique. Baseline and post-intervention measurements included pulse wave velocity (PWV), flow-mediated dilation (FMD), and oxidative stress parameters. Hypertensive postmenopausal women (59 ± 0.7 years) who ended the protocol were distributed into three groups: (1) control group (yoga or stretching, C, n = 14); (2) yoga + respiratory technique (Y+, n = 10); (3) stretching + respiratory technique (S+, n = 9).
Results: Diastolic blood pressure and FMD [baseline: C: 6.94 ± 1.97%, Y+: 7.05 ± 1.65%, and S+: 3.54 ± 2.01% vs. post: C: 16.59 ± 3.46% (p = 0.006), Y+: 13.72 ± 2.81% (p = 0.005), and S+: 11.79 ± 0.99% (p = 0.0001)] have significantly increased in all groups when baseline and post-practice values were compared. However, resting heart rate and PWV [baseline: Y+: 10.44 ± 3.69 and S+: 9.50 ± 0.53 m/s vs. post: Y+: 9.45 ± 0.39 (p = 0.003) and S+: 8.02 ± 0.47 m/s (p = 0.003)] decreased significantly only in the Y+ and S+ groups (baseline vs. post). Systemic antioxidant enzyme activities (superoxide dismutase and catalase) increased in all groups, and hydrogen peroxide and lipoperoxidation reduced in Y+ and S+ (baseline vs. post).
Conclusions: Twelve weeks of yoga or stretching video classes promoted positive changes in several outcomes generally regarded as cardiovascular risk factors in HPMWs, and these changes were even more pronounced by the association with respiratory technique.
There is a remarkable increased prevalence of hypertension in postmenopausal women (Yanes and Reckelhoff, 2011; Modena, 2014). Hypoestrogenism caused by menopause exerts deleterious effects on several tissues and organs, including vessels (Somani et al., 2019). This may lead to endothelial dysfunction (Sanchez-Barajas et al., 2018) arterial stiffness (Muka et al., 2016; Costa-Hong et al., 2018), and unfavorable oxidative stress profile (Dinh et al., 2014).
The mechanisms by which menopause leads to changes in vascular bed and impairment in endothelial function are complex and diverse, including decreasing vasodilation capacity and impairing the ability of signaling of blood flow, endothelium, and smooth muscle cells of the media layer (Somani et al., 2019). This process improperly generates reactive oxygen species (ROS), causing losses for vascular homeostasis (Hsieh et al., 2014). Along with this, increasing vascular resistance may represent a burden for hypertension and an overload for central arteries (Thijssen et al., 2016). Damage caused by mechanic stress of blood flow on walls of central arteries leads to lower compliance and arterial stiffness (Mitchell, 2009; Laurent, 2012). Arterial stiffness, in turn, increases with age, but the deleterious effects of menopause should not be seen as part of the natural aging process (Costa-Hong et al., 2018).
Taken together, these conditions demand appropriate clinical management, which should include non-pharmacological strategies in order to prevent their progression to cardiovascular diseases (Yanes and Reckelhoff, 2011). Among others, regular physical exercises and slow breathing are highly recommended to treat the effects of hypertension (Cornelissen and Smart, 2013), and in recent years, yoga also has been found to be an effective intervention (Hagins et al., 2013). Despite controversial results of yoga on arterial stiffness (Patil et al., 2015, 2017), an association between poor trunk flexibility and arterial stiffness has already been demonstrated (Yamamoto et al., 2009). Regarding endothelial function, several studies have demonstrated the effectiveness of yoga (Hunter et al., 2017, 2018). However, the impact of slow breathing on endothelial and vascular function has not yet been demonstrated (Limberg et al., 2013; DeLucia et al., 2018). Multiple components of yoga such as physical poses (asanas), respiratory exercises (pranayamas), meditation, and devotional and lifestyle aspects have never been analyzed separately in order to assess specific benefits (Hartley et al., 2014).
Pranayamas present different forms and speeds of inhalation, exhalation, and retentions (Jerath et al., 2006). Ujjayi is a slow-breathing pranayama, which narrows the glottis and extends respiratory phases. It decreases respiratory rate, and it is usually performed along with physical poses (Satin et al., 2014). Physical poses take limbs and spine to great range of motion, demanding mostly agonists' isometric contractions and antagonists' muscle group stretching (Jorge et al., 2016). In recent years, stretching has been regarded as an exercise able to promote changes on vascular function (Kato et al., 2017). Positive effects of single bouts of stretching have been reported, although mechanisms involved in such responses are not fully elucidated, and no studies have been carried out on chronic effects of this kind of exercise (Kruse et al., 2016; Kruse and Scheuermann, 2017).
As an innovative investigation, we may well hypothesize that in hypertensive postmenopausal women (HPMWs) additional improvements resulting from yoga poses and respiratory technique may be expected for blood pressure, vascular, and endothelial function, and oxidative stress profile after 12 weeks of video classes twice a week. Therefore, the aim of this study was to investigate the additional effect of respiratory techniques on vascular function and oxidative stress profile in HPMWs, following 12 weeks of yoga or stretching video classes.
The Ethical Committee of Instituto de Cardiologia do Rio Grande do Sul/Fundação Universitária de Cardiologia approved this study, which is in accordance with CONSORT statement. All participants signed an informed written consent form. Data have been collected between July 2018 and December 2019. The study was registered in the Clinical Trials Registry (NCT03137849). All data have been fed into the REDCap Platform (www.redcap.cardiology.org.br).
Patients have been recruited from the institution patient data, along with a social media network (i.e., Facebook). Inclusion criteria were as follows: age 45 to 68 years old, minimum of 12 months of amenorrhea, follicle-stimulating hormone >35 mUI/mL, blood pressure >140/90, or in continuous use of medication [diuretics, Ca+ channel inhibitors, angiotensin-converting enzyme (ACE) inhibitors, ARA2], not undergoing hormone replacement therapy, leading a sedentary lifestyle, and no previous yoga practice. Exclusion criteria were as follows: use of β-blockers and/or psychiatric medication, recent cardiovascular events or surgery, renal alterations, respiratory, and/or neuromotor pathologies, smoking, and body mass index >34.9 kg/m2.
After signing the informed consent form, participants were randomized and underwent baseline assessments at Clinical Investigation Laboratory and Ergometry Room of Institute of Cardiology of Rio Grande do Sul/Cardiology University Foundation by trained personnel blinded to the randomization. They were randomized into yoga, stretching, yoga + respiratory technique, and stretching + respiratory technique interventions. Given the dropout of subjects, and the lack of differences between yoga and stretching in baseline and post-interventions in the assessed parameters, participants were assigned into three groups: (1) control (yoga or stretching interventions alone, C, n = 14); (2) yoga + respiratory technique (Y+, n = 10), and (3) stretching + respiratory technique (S+, n = 9).
The participants were previously advised to fast overnight (12 h) and to refrain from alcohol, caffeine, and intensive exercise practice and were told to have proper night of sleep 24 h prior the examination day.
On the day of the evaluation, anthropometric measures, and body composition by bioimpedance were taken (BIODYNAMICS 310™). Systolic (SBP), diastolic blood pressure (DBP), and heart rate were assessed according to the American Health Association guideline recommendations. Blood sample were collected for biochemical analysis and systemic oxidative stress evaluations.
Arterial stiffness and endothelial function were assessed as described in the following section. Exercise electrocardiogram was performed to rule out any cardiac disease and to estimate maximal oxygen uptake (VO2max). Flexibility was evaluated with “Sit and Reach” test (Ayala et al., 2012).
After baseline assessments, participants attended 12 weeks (24 classes) of intervention and underwent final evaluations in the same baseline order. All participants have been told they were attending a yoga protocol. Blind investigators have taken all outcomes assessments to the interventions.
All evaluations have been repeated in the same order after completion of protocol, as follows:
Fasting blood samples were collected to analyze fasting glucose (automated enzymatic method). Total cholesterol, high-density lipoprotein cholesterol, and triglycerides were assessed by the enzymatic colorimetric method. Follicle-stimulating hormone was assessed by the electrochemiluminescence method.
Arterial stiffness was assessed by pulse wave velocity (PWV), which refers to the time a systolic wave travels in an arterial segment (Costa-Hong et al., 2018). Augmentation Index (Aix) refers to the sum of both anterograde systolic wave and the previously reflected systolic wave, and it is considered a reliable measure for vascular resistance along the arterial tree (Mitchell, 2009). Arterial stiffness was assessed by Complior Analyzer™ (ALAM Medical, France). Sensors were positioned upon the right carotid and femoral arteries. Distance between carotid and femoral pulse was provided by the investigator. Measures of blood pressure, height, and weight were fed into the software. Three consecutive measures were obtained from the equipment at a quality signal >90%. The mean of these three measures was considered for analysis of PWV, Aix, and central SBP and DBP (cSBP and cDBP, respectively) (Townsend et al., 2015).
A high-resolution ultrasonography equipment (Esaote My Lab 70X Vision) was used for the evaluation of endothelial function through a high-frequency transducer to obtain longitudinal images of the brachial artery. The transducer was positioned upon the brachial artery in the 1/3 arm size of superior antecubital fossa. Baseline images were recorded for 1 min, and this was immediately followed by a cuffing inflated up to 200 mmHg and kept for 5 min in order to characterize reactive hyperemia. Thirty seconds before the cuffing was released, new images started to be recorded for 3 min, considered endothelium-dependent dilation, and were analyzed by the Cardiovascular Suite™ software (Quipu, Italy). The software demands to specify the interest area of the arterial segment and flow using visual selection. Baseline and post-hyperemia diameter and flow were computed to obtain the percentage of dilation, volume, and shear stress (Thijssen et al., 2019).
Whole blood was sampled from the participants in EDTA tubes and then centrifuged at 2,000 rotations per minute (rpm) during 10 min at 4°C. Plasma was removed and kept aside for further analysis. Mononuclear cell fraction was removed, and the red blood cells were washed with phosphate-buffered saline and centrifuged three times, for 5 min each, at 2,000 rpm. Further, in 100 μL of washed red blood cells, 1 mL of acetic acid (1 mM) and MgSO4 (4 mM) was centrifuged at 3,000 rpm for 30 min at 4°C. The supernatant was stored at −80°C for subsequent assessments. Proteins were quantified by the method described by Lowry et al. (1951).
Catalase (CAT) activity was evaluated by spectrophotometry (240 nm), through the consumption of hydrogen peroxide (H2O2; Sigma–Aldrich Corporation, H3410) by measuring decreasing absorbance, whose rate of decomposition is straightly proportional to its activity. Superoxide dismutase (SOD) activity was determined through measures of oxidative pirogalol (Sigma–Aldrich Corporation, P0381). A colorful by-product based on oxidation of pirogalol was detected by spectrophotometry (420 nm, SP22, Bioespectro) (Fridovich, 1986).
Nicotinamide adenine dinucleotide phosphate oxidase (NADPH) oxidase was determined by the rate of NADPH consumption assessed by measuring the decline in absorbance (340 nm) every 10 min, using a plate reader spectrophotometer (Espectra Max 2, Molecular Devices) (Wei et al., 2006). For the assay, we used a 50 mM phosphate buffer containing EDTA (2 mM, Nuclear, 311737), sucrose (150 mM, Sigma–Aldrich Corporation, S7903), NADPH (1.3 mM, Sigma–Aldrich Corporation, N1630) and 10 μL of sample.
H2O2 was analyzed through measuring of oxidation of phenol red (Sigma–Aldrich Corporation, H3410) mediated by radish peroxidase (Sigma–Aldrich Corporation, P8250), using a plate reader spectrophotometer (610 nm, Espectra Max 2, Molecular Devices) (Pick and Keisari, 1980).
Plasma lipid peroxide levels were determined by measuring thiobarbituric acid reactive substances (TBARSs), a common method for measuring the concentration of malondialdehyde, the main breakdown product of oxidized lipids. For the TBARS assay, using 250 μL of sample, trichloroacetic acid (10%, wt/vol, Dinamica, 1072-1) was added to the homogenate to precipitate proteins and to acidify the samples. This mixture was then centrifuged (4,000 rpm, 10 min), the protein free sample was extracted, and thiobarbituric acid (0.67%, wt/vol, Sigma–Aldrich Corporation, T-550-0) was added to the reaction medium. The tubes were placed in a water bath (100°C) for 30 min. The absorbences were measured at 535 nm using a spectrophotometer (SP22, Bioespectro) (Buege and Aust, 1978).
Carbonyls represent a marker of the oxidative damage to proteins and were assessed by the reaction of oxidative proteins in plasma with 2,4-dinitrophenylhydrazine (DNPH, Sigma–Aldrich Corporation, D199303) in acid mean. This was followed by successive washings with acid and organic solvents in the final incubation with guanidine hydrochloride solution (6M, Sigma–Aldrich Corporation, G4505). Absorbance of carbonyls was measured by spectrophotometry (360 nm, SP22, Bioespectro) (Reznick and Packer, 1994).
The 12 week supervised video classes occurred twice a week between 2:00 and 6:00 P.M and have taken place in a room equipped with a 32-inch-screen television and yoga mats.
Four video classes have been created as intervention: yoga, stretching, yoga + respiratory technique, and stretching + respiratory technique. The respiratory technique employed as intervention was ujjayi pranayama (victorious breath), a nasal respiration that narrows the glottis in order to extend both inspiratory and expiratory phases, and was performed along with yoga or stretching poses. Yoga and stretching, as control intervention, took only “inhale/exhale” commands. After the 60 min of yoga or stretching, all groups underwent the same yoga-based relaxation technique in supine position (15 min). The protocols were developed by same experienced yoga and stretching licensed instructor.
Yoga included three full sequences of sun salutations, followed by traditional standing poses, balance poses, stabilizations (core positions) and retroversion poses, sit poses, and final poses in supine position.
Stretching was based on dynamic (warm-up) and static exercises excluding those similar to yoga poses, attaining great range of motion of the main body joints and muscle groups, and did not include any body weight bearing, thus avoiding isometric contractions.
Full video classes of yoga and stretching were compiled as yoga (Videos 1–6) and stretching (Videos 7–12) for electronic version (in Portuguese audio, associated with respiratory technique).
A comparative plot of interventions is displayed in Supplemental Table 1.
The study was not analyzed as “intention to treat.” A secondary analysis of those participants who ended the protocol was provided. Because of losses in the follow-up, yoga and stretching not associated with respiratory technique were considered as one active control group, so statistical analyses were performed for three intervention groups: (1) control group (yoga or stretching), (2) yoga + respiratory technique (Y+), (3) stretching + respiratory technique (S+). Power of study was calculated a posteriori considering PWV variance among groups for post-intervention values, which was determined as β = 0.83. Medication classes used by participants were divided into five categories: (1) none, (2), diuretics, (3) angiotensin-converting enzyme inhibitor, (4) angiotensin II receptor blockers (ARBs), (5) combination of any class. This classification was taken to determine any differences among groups concerning the use of drug classes.
Collected data were processed by SPSS Statistics for Windows, version 25.0. Differences between post-intervention and baseline measures and among groups were calculated to determine changes in the outcome measures by GEE (generalized estimating equation), in order to obtain population-averaged effects. Bonferroni post-hoc test was performed. Two factors have been considered for analysis: intervention group, named “group,” and moment of evaluation (baseline and post-intervention), named “moment,” as well as interaction between them, called “interaction.” Data are shown as mean (M) ± standard error (SE). Correlations of Pearson for parametric data and Spearman (non-parametric) have been taken. Significance considered a p ≤ 0.05.
The eligible study population consisted of 50 women, of which 33 completed the 12 week protocol (Figure 1). Participants' age and time of menopause were similar among groups (Table 1).
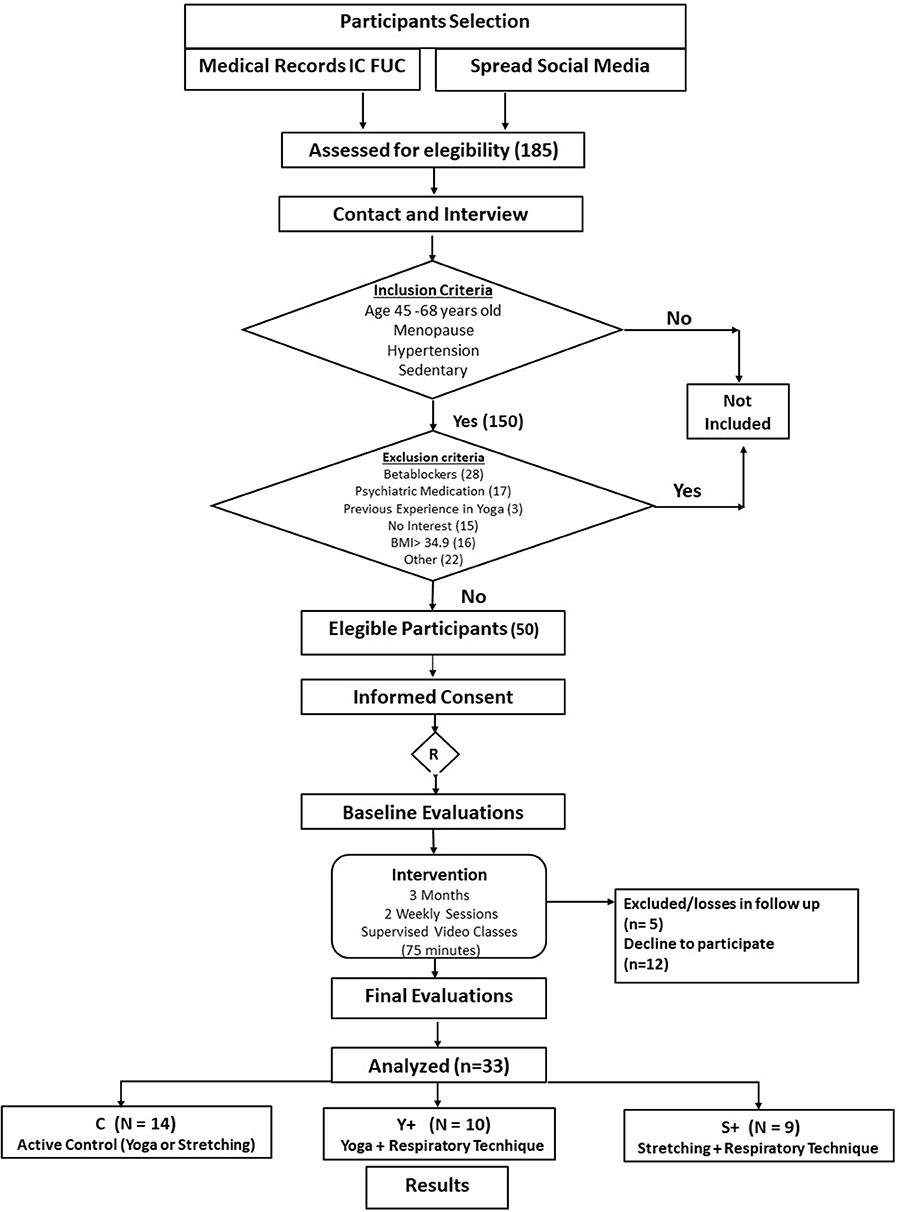
Figure 1. Flowchart of recruitment.
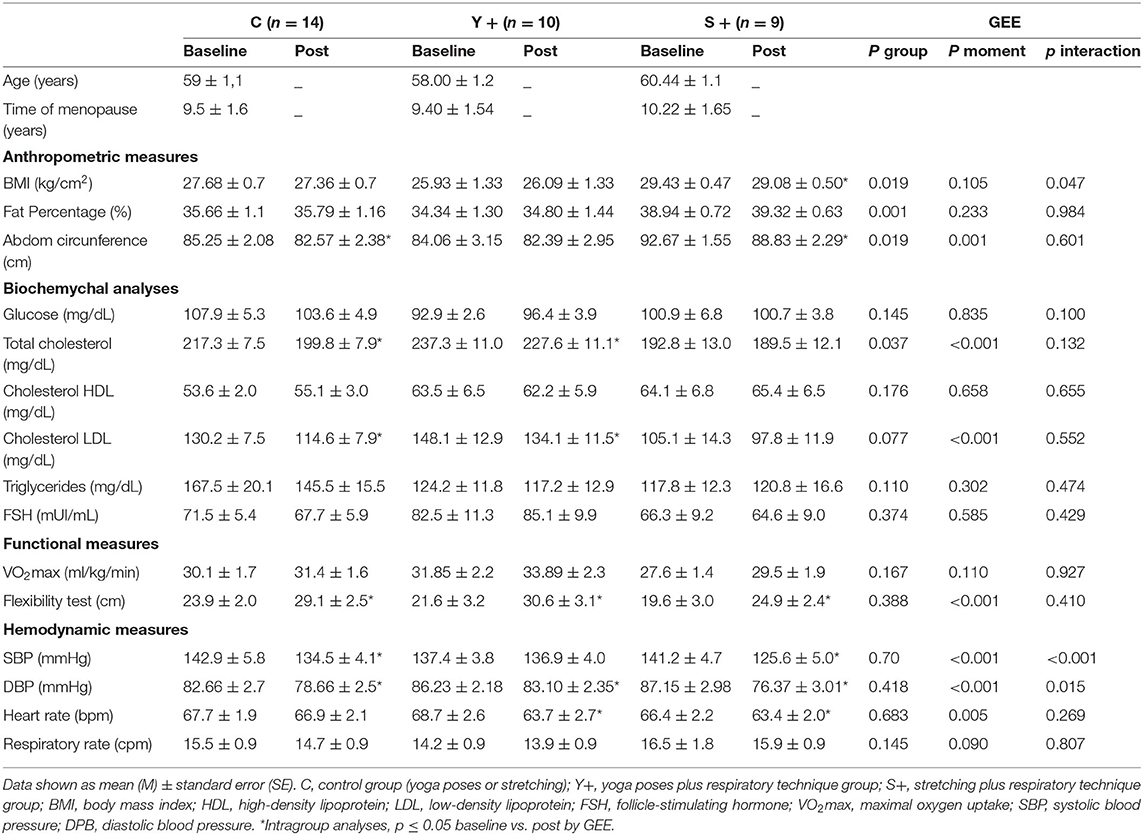
Table 1. Characterization of participants after randomization, at baseline, and post-intervention for 12 weeks of video classes two times a week.
Five participants were not taking any medication, three participants used only diuretics, 4 participants used ACE inhibitors, nine participants used ARBs, and 12 used a combination of drugs, including three who used of calcium-channel blockers. There were no differences between treated and untreated participants and the type of drugs used in all groups.
Body mass index was not changed significantly in any group from baseline to post-intervention moments. However, abdominal circumference was significantly decreased when baseline and post-intervention were compared. This is displayed in Table 1, which shows a significant decrease in the C (p = 0.031) and in S+ groups (p = 0.009), but not in the Y+ group (p = 0.294).
Total cholesterol levels and low-density lipoprotein (LDL) cholesterol decreased significantly in the C and Y+ groups when baseline and post-intervention were compared (p = 0.009, and p = 0.039). S+ did not present significant changes in these parameters. Other biochemical assessments were similar among groups and time of evaluation (Table 1).
Estimated maximal oxygen consumption was not changed in any group after intervention. Significantly increased flexibility was noticed in all groups through flexibility test (C: p = 0.034, Y+: p = 0.0001, and S+: p = 0.001; Table 1).
This study has demonstrated a significant improvement from baseline to post-intervention values concerning hemodynamic measures, as demonstrated in Table 1 (moment baseline vs. post by GEE). Systolic blood pressure was decreased significantly in both the C and S+ groups (Figure 2A), whereas DBP decreased significantly in all groups (Figure 2B). Heart rates at rest decreased significantly in the Y+ and S+ groups, whereas the C group has not changed significantly when baseline and post-intervention were compared (Figure 2C). Respiratory rate was not changed significantly in any group (Figure 2D).
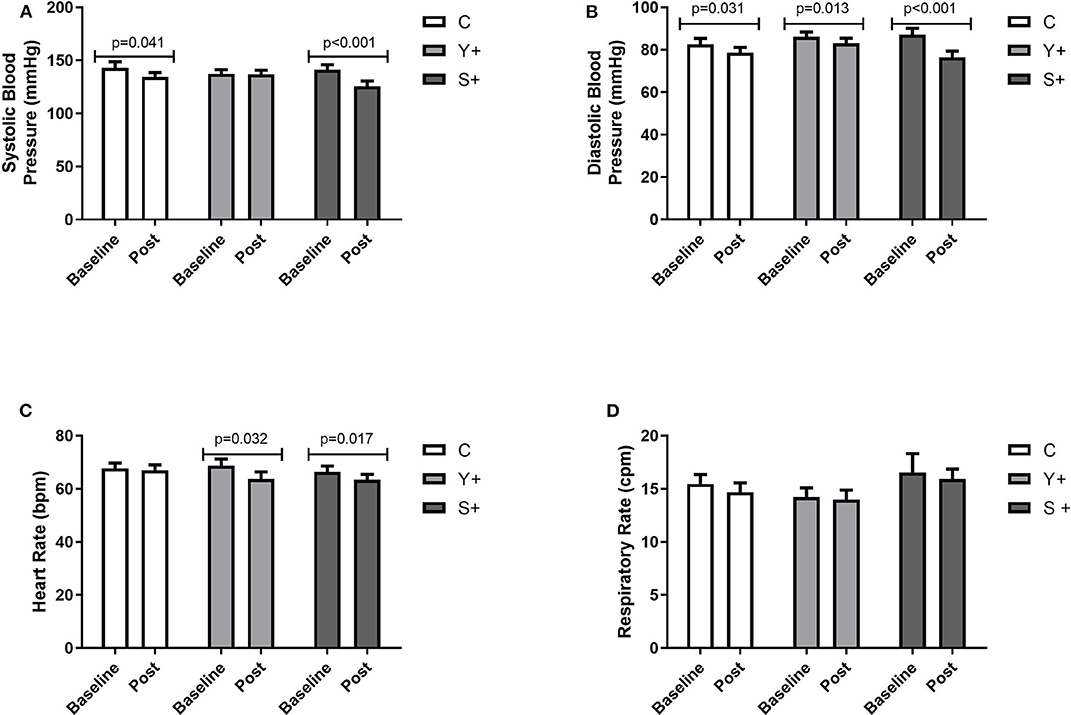
Figure 2. Hemodynamic and respiratory measures. (A) Systolic blood pressure expressed in mmHg. (B) Diastolic blood pressure expressed in mmHg. (C) Heart rate at rest expressed in beats per minute (bpm). (D) Respiratory rate expressed in cycles per minute (cpm). Baseline and post-intervention variations by generalized estimation equation (GEE) determined as Mean ± standard error. C, control group (yoga poses or stretching); Y+, yoga poses plus stretching technique group; S+, stretching plus control technique group.
Pulse wave velocity and years of menopause showed a moderate significant correlation at baseline (r = 0.613, p < 0.001), which was non-significant in the post-intervention assessment (r = 0.243, p = 0.187; Figure 3). Most outcomes of arterial stiffness demonstrated a significant improvement when baseline and post-intervention measurements were compared, as demonstrated in Table 2 (moment baseline vs. post by GEE). Augmentation Index was significantly decreased in the C group, and central DBP decreased in all groups when baseline and post-intervention were compared. The PWV decreased significantly only in both groups with respiratory technique post-intervention, but not in the control group (Figure 4).
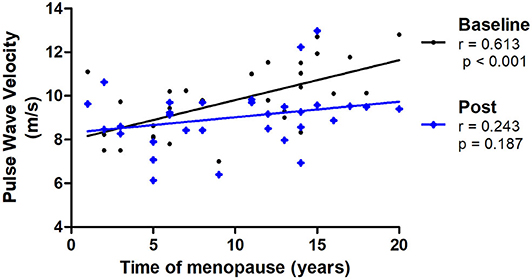
Figure 3. Correlations of PWV (pulse wave velocity) and time of menopause at baseline and post-intervention (N = 31).
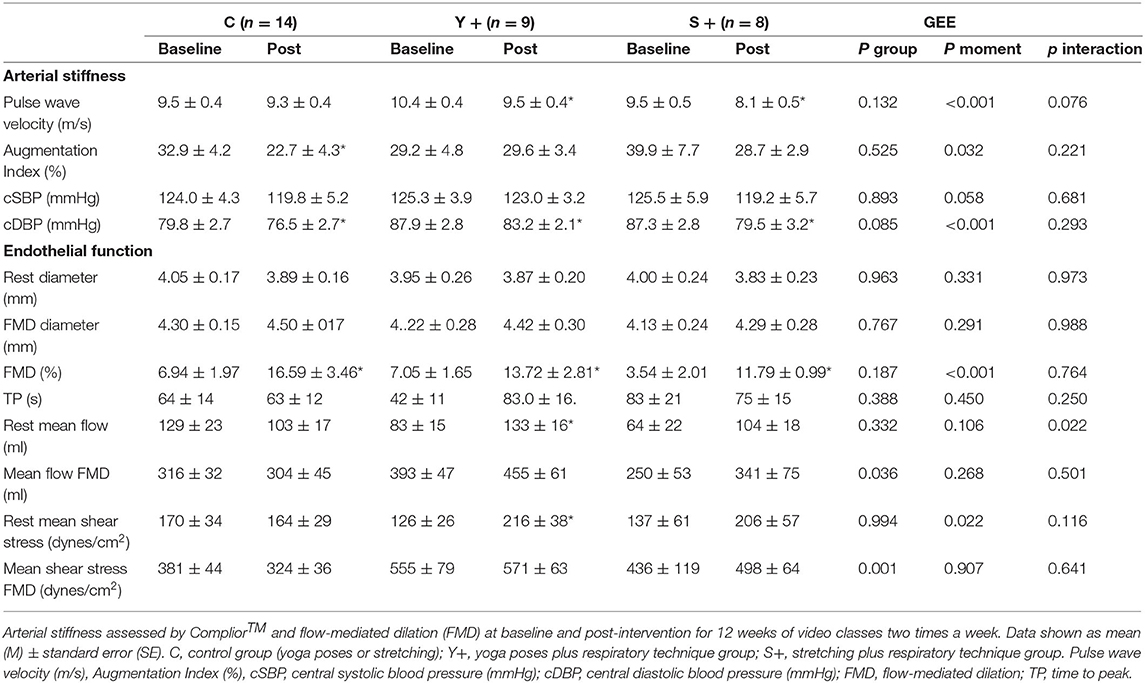
Table 2. Vascular function-arterial stiffness and endothelial function [flow-mediated dilation (FMD)].
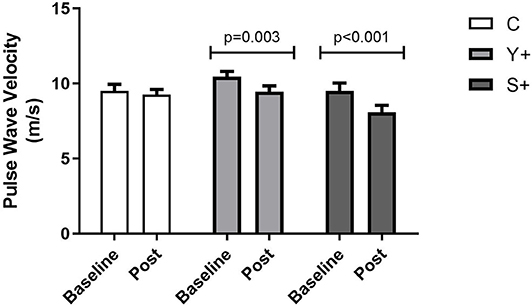
Figure 4. Arterial Stiffness assessed by pulse wave velocity (PWV) by Complior. Baseline and post-intervention variations determined by generalized estimation equation (GEE) determined as mean ± standard error. C, control group (yoga poses or stretching); Y+, yoga poses plus respiratory technique group; S+, stretching plus respiratory technique group.
Rest value diameters were no changed significantly, but flow-mediated dilation (FMD) (%) had a significant increase in all groups after interventions (Figure 5). Time to peak (TP), mean flow of FMD, and mean shear stress of FMD did not present any significant change. However, rest mean flow and mean shear stress were increased significantly only in the Y+ group. The data are shown in Table 2.
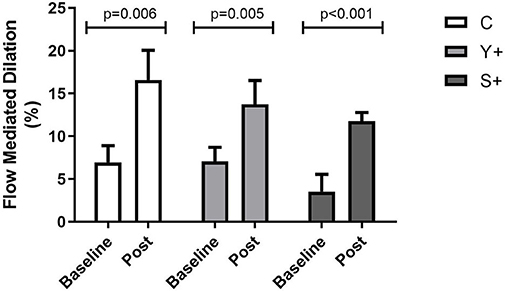
Figure 5. Endothelial function by flow-mediated dilation (FMD) at baseline and post-intervention variations determined by generalized estimation equation (GEE) determined as mean ± standard error. C, control group (Yoga poses or stretching); Y+, yoga poses plus respiratory technique group; S+, stretching plus respiratory technique group.
All systemic oxidative stress parameters demonstrated significant improvement when baseline and post-intervention measurements were compared (moment baseline vs. post by GEE), as demonstrated in Table 3. Regarding antioxidants, SOD, and CAT activities showed significant increases in all intervention groups when baseline and post-intervention values were compared. Although NADPH oxidase was not different, H2O2 concentration and lipoperoxidation (TBARS) decreased significantly in the Y+ and S+ groups after interventions. Protein oxidation (carbonyls) showed significant decrease in C and Y+ groups.
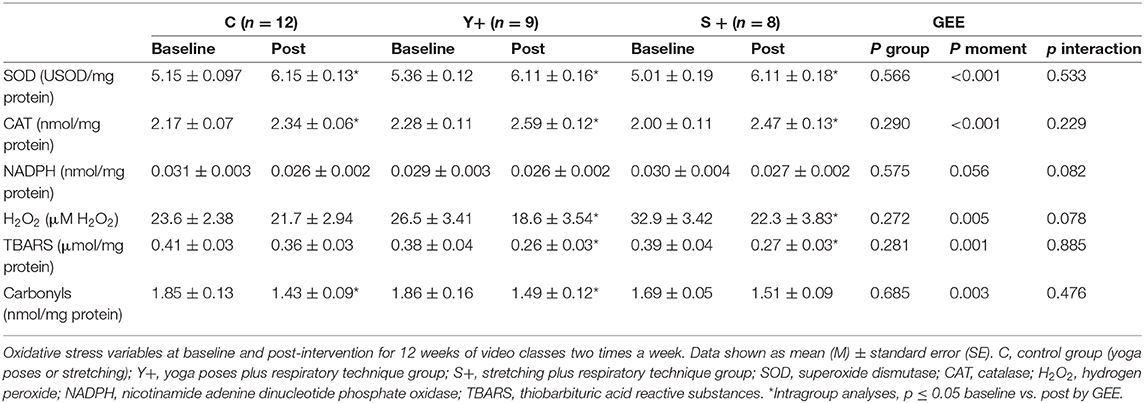
Table 3. Oxidative stress.
This innovative investigative study was able to demonstrate multiple significant improvements in HPMWs after 12 weeks of yoga or stretching video classes, with additional effects of respiratory technique. General decreases in blood pressure concur to beneficial effects of these practices and are in accordance with previous findings for yoga (Hagins et al., 2014) and respiratory techniques (Pinheiro et al., 2007).
Along with decreased heart rate at rest, both groups with respiratory technique were able to significantly decrease PWV. Previous findings for yoga have demonstrated decreased PWV (Patil et al., 2015), but to our knowledge, this is the first study to demonstrate that protocols including respiratory technique may influence PWV in HPMWs.
Respiration and heart rhythms respond to their interrelated changes (Dick et al., 2014) and heart rate may modulate vascular endothelium, acting on mechanical pulsatile stress (Laosiripisan et al., 2017). Changes in intrathoracic and transmural pressure during inspiration influences cardiac filling and stroke volume, generating stroke volume variability (Shibata et al., 2006). Thus, changes in pattern of respiration such as expansibility of rib cage may influence hemodynamics. Responses of venous return and atrial filling to respiration may be associated to the pattern of respiration, instead of rate (Byeon et al., 2012). Increasing venous return due to diaphragmatic breathing has been demonstrated in healthy individuals (Miller et al., 2005; Balzan et al., 2014). We may speculate that the decreased PWV and rest heart rate in both groups with respiratory technique in the present study are, at least in part, mediated by these mechanisms.
A moderate significant correlation between PWV and years of menopause at baseline was noticed, as expected (Thijssen et al., 2016). At the end of interventions, this correlation disappeared, showing an attenuation of the effects of menopause on PWV, possibly caused by these non-pharmacological interventions.
Moreover, the prevention of losses in nitric oxide bioavailability should be a goal in HPMWs because estrogen deprivation reduces it and increases ROS (Green et al., 2014) thus increasing risk for atherosclerosis (Witkowski and Serviente, 2018). The increase in FMD in all intervention groups found in this study corroborates previous findings of increased FMD after Bikram yoga (hot yoga) (Hunter et al., 2018) and strengthens the potential role of this practice to prevent deleterious effects of menopause. Increased FMD has also been found after some types of exercise training (Early et al., 2017) including isometric exercises (Badrov et al., 2016) which are present in many yoga poses of this study protocol.
Accordingly, increased systemic antioxidant defenses were noticed in this study, once SOD and CAT, as a frontline expression of it, were increased in all groups. As a unique complex producing only ROS, the tendency to decrease (p = 0.056, moment baseline vs. post by GEE) in NADPH oxidase (an important source of superoxide anion) and the reduction in systemic hydrogen peroxide (H2O2) concentration in the Y+ and S+ groups indicate an overall decrease of pro oxidants. Regarding oxidative stress damage, lipoperoxidation (TBARS) was reduced when baseline and post-intervention values were compared in the Y+ and S+ groups. Moreover, carbonyls, as markers of oxidative damage to proteins were significantly decreased in groups undergoing yoga intervention (C and Y+, baseline vs. post). Taken together, our findings demonstrate markedly improvements in antioxidant, pro-oxidants, and biomolecule damage after interventions, suggesting additional effects in yoga groups and in the groups undergoing respiratory technique. In fact, beneficial effects of yoga on oxidative stress in elderly hypertensive subjects have been previously demonstrated (Patil et al., 2014) along with the beneficial effects of stretching on oxidative stress profile of heart failure patients (Sankaralingam et al., 2011; Kato et al., 2017).
Perhaps increasing fascicle length and local shear stress by ischemia during stretching, present in both yoga poses and stretching, may provide an overall reduction in peripheral resistance through reducing smooth muscle cells tone, besides other adaptations that may induce changes in endothelial function and oxidative stress profile (Wong and Figueroa, 2014; Kruse and Scheuermann, 2017).
Increased flexibility might be considered a functional achievement, once losses in flexibility are expected in postmenopausal women. Although there were no significant increases in estimated VO2max, decreases in total cholesterol and LDL in C and S+ point to a possible metabolic improvement.
The main limitation of this study lies in the relatively high number of dropouts−17 out of 50 recruited HPMWs—higher than other yoga studies (most carried out in developed countries), which reduced the number of subjects in each group. However, despite that, the power of study calculated a posteriori—considering PWV variance among groups for post-intervention—was β = 0.83.
In summary, our findings demonstrated that yoga poses and stretching supervised video classes for 12 weeks improved blood pressure, arterial stiffness, endothelial function, and oxidative stress profile in HPMWs. Effects of respiratory technique along with yoga poses or stretching point to possible improvement in arterial stiffness. Therefore, yoga or stretching, even when administered through video classes seems to have a positive impact on several outcomes regarded as cardiovascular risk factors, and these benefits are extended by the association of respiratory technique. Nevertheless, more research based on more robust yoga and stretching interventions and a larger sample are needed to lend further support to our findings.
All data supporting the conclusions of this study will be fully provided on request by authors.
The studies involving human participants were reviewed and approved by Comitê de Ética do Instituto de Cardiologia - 5273/16 - 03/11/2016. The patients/participants provided their written informed consent to participate in this study.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
This work was supported by CNPQ (Conselho Nacional de Desenvolvimento Científico e Tecnológico) and CAPES (Comissão de Aperfeiçoamento de Pessoal do Nível Superior). KD and MI are recipients of CNPQ-BPQ.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors express deep gratitude to all participants of the research, as well as the valuable help of the institutional coworkers that made it possible.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2020.00898/full#supplementary-material
Ayala, F., Sainz de Baranda, P., De Ste Croix, M., and Santonja, F. (2012). Reproducibility and criterion-related validity of the sit and reach test and toe touch test for estimating hamstring flexibility in recreationally active young adults. Phys. Ther. Sport 13, 219–226. doi: 10.1016/j.ptsp.2011.11.001
Badrov, M. B., Freeman, S. R., Zokvic, M. A., Millar, P. J., and McGowan, C. L. (2016). Isometric exercise training lowers resting blood pressure and improves local brachial artery flow-mediated dilation equally in men and women. Eur. J. Appl. Physiol. 116, 1289–1296. doi: 10.1007/s00421-016-3366-2
Balzan, F. M., da Silva, R. C., da Silva, D. P., Sanches, P. R., Tavares, A. M., Ribeiro, J. P., et al. (2014). Effects of diaphragmatic contraction on lower limb venous return and central hemodynamic parameters contrasting healthy subjects versus heart failure patients at rest and during exercise. Physiol. Rep. 2:e12216. doi: 10.14814/phy2.12216
Buege, J., and Aust, S. (1978). Microsomal lipid peroxidation. Meth. Enzymol 52, 302–310. doi: 10.1016/S0076-6879(78)52032-6
Byeon, K., Choi, J. O., Yang, J. H., Sung, J., Park, S. W., Oh, J. K., et al. (2012). The response of the vena cava to abdominal breathing. J. Altern. Complement Med. 18, 153–157. doi: 10.1089/acm.2010.0656
Cornelissen, V. A., and Smart, N. A. (2013). Exercise training for blood pressure: a systematic review and meta-analysis. J. Am. Heart Assoc. 2:e004473. doi: 10.1161/JAHA.112.004473
Costa-Hong, V. A., Muela, H. C. S., Macedo, T. A., Sales, A. R. K., and Bortolotto, L. A. (2018). Gender differences of aortic wave reflection and influence of menopause on central blood pressure in patients with arterial hypertension. BMC Cardiovasc. Disord. 18:123. doi: 10.1186/s12872-018-0855-8
DeLucia, C. M., De Asis, R. M., and Bailey, E. F. (2018). Daily inspiratory muscle training lowers blood pressure and vascular resistance in healthy men and women. Exp. Physiol. 103, 201–211. doi: 10.1113/EP086641
Dick, T. E., Hsieh, Y. H., Dhingra, R. R., Baekey, D. M., Galan, R. F., Wehrwein, E., et al. (2014). Cardiorespiratory coupling: common rhythms in cardiac, sympathetic, and respiratory activities. Prog. Brain Res. 209, 191–205. doi: 10.1016/B978-0-444-63274-6.00010-2
Dinh, Q. N., Drummond, G. R., Sobey, C. G., and Chrissobolis, S. (2014). Roles of inflammation, oxidative stress, and vascular dysfunction in hypertension. Biomed. Res. Int. 2014:406960. doi: 10.1155/2014/406960
Early, K. S., Stewart, A., Johannsen, N., Lavie, C. J., Thomas, J. R., and Welsch, M. (2017). The effects of exercise training on brachial artery flow-mediated dilation: a meta-analysis. J. Cardiopulm. Rehabil. Prev. 37, 77–89. doi: 10.1097/HCR.0000000000000206
Fridovich, I. (1986). Superoxide dismutases. Adv. Enzymol Relat. Areas Mol. Biol. 58, 61–97. doi: 10.1002/9780470123041.ch2
Green, D. J., Dawson, E. A., Groenewoud, H. M., Jones, H., and Thijssen, D. H. (2014). Is flow-mediated dilation nitric oxide mediated?: a meta-analysis. Hypertension 63, 376–382. doi: 10.1161/HYPERTENSIONAHA.113.02044
Hagins, M., Rundle, A., Consedine, N. S., and Khalsa, S. B. S. (2014). A randomized controlled trial comparing the effects of yoga with an active control on ambulatory blood pressure in individuals with prehypertension and stage 1 hypertension. J. Clin. Hypertens. 16, 54–62. doi: 10.1111/jch.12244
Hagins, M., States, R., Selfe, T., and Innes, K. (2013). Effectiveness of yoga for hypertension: systematic review and meta-analysis. Evid. Based Complement Alternat. Med. 2013:649836. doi: 10.1155/2013/649836
Hartley, L., Dyakova, M., Holmes, J., Clarke, A., Lee, M. S., Ernst, E., et al. (2014). Yoga for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 5:Cd010072. doi: 10.1002/14651858.CD010072.pub2
Hsieh, H. J., Liu, C. A., Huang, B., Tseng, A. H., and Wang, D. L. (2014). Shear-induced endothelial mechanotransduction: the interplay between reactive oxygen species (ROS) and nitric oxide (NO) and the pathophysiological implications. J. Biomed. Sci. 21:3. doi: 10.1186/1423-0127-21-3
Hunter, S. D., Dhindsa, M. S., Cunningham, E., Tarumi, T., Alkatan, M., Nualnim, N., et al. (2017). The effect of bikram yoga on endothelial function in young and middle-aged and older adults. J. Bodyw. Mov. Ther. 21, 30–34. doi: 10.1016/j.jbmt.2016.06.004
Hunter, S. D., Laosiripisan, J., Elmenshawy, A., and Tanaka, H. (2018). Effects of yoga interventions practised in heated and thermoneutral conditions on endothelium-dependent vasodilatation: the bikram yoga heart study. Exp. Physiol. 103, 391–396. doi: 10.1113/EP086725
Jerath, R., Edry, J. W., Barnes, V. A., and Jerath, V. (2006). Physiology of long pranayamic breathing: neural respiratory elements may provide a mechanism that explains how slow deep breathing shifts the autonomic nervous system. Med. Hypotheses 67, 566–571. doi: 10.1016/j.mehy.2006.02.042
Jorge, M. P., Santaella, D. F., Pontes, I. M., Shiramizu, V. K., Nascimento, E. B., Cabral, A., et al. (2016). Hatha yoga practice decreases menopause symptoms and improves quality of life: a randomized controlled trial. Complement Ther. Med. 26, 128–135. doi: 10.1016/j.ctim.2016.03.014
Kato, M., Masuda, T., Ogano, M., Hotta, K., Takagi, H., Tanaka, S., et al. (2017). Stretching exercises improve vascular endothelial dysfunction through attenuation of oxidative stress in chronic heart failure patients with an implantable cardioverter defibrillator. J. Cardiopulm. Rehabil. Prev. 37, 130–138. doi: 10.1097/HCR.0000000000000229
Kruse, N. T., and Scheuermann, B. W. (2017). Cardiovascular responses to skeletal muscle stretching: “stretching” the truth or a new exercise paradigm for cardiovascular medicine? Sports Med. 47, 2507–2520. doi: 10.1007/s40279-017-0768-1
Kruse, N. T., Silette, C. R., and Scheuermann, B. W. (2016). Influence of passive stretch on muscle blood flow, oxygenation and central cardiovascular responses in healthy young males. Am. J. Physiol. Heart Circ. Physiol. 310, H1210–H1221. doi: 10.1152/ajpheart.00732.2015
Laosiripisan, J., Parkhurst, K. L., and Tanaka, H. (2017). Associations of resting heart rate with endothelium-dependent vasodilation and shear rate. Clin Exp Hypertens. 39, 150–154. doi: 10.1080/10641963.2016.1226890
Laurent, S. (2012). Defining vascular aging and cardiovascular risk. J. Hypertens. 30, S3–S8. doi: 10.1097/HJH.0b013e328353e501
Limberg, J. K., Morgan, B. J., Schrage, W. G., and Dempsey, J. A. (2013). Respiratory influences on muscle sympathetic nerve activity and vascular conductance in the steady state. Am. J. Physiol. Heart Circ. Physiol. 304, H1615–H1623. doi: 10.1152/ajpheart.00112.2013
Lowry, O. H., Rosebrough, N. J., Farr, A. L., and Randall, R. J. (1951). Protein measurement with the folin phenol reagent. J. Biol. Chem. 193, 265–275.
Miller, J. D., Pegelow, D. F., Jacques, A. J., and Dempsey, J. A. (2005). Skeletal muscle pump versus respiratory muscle pump: modulation of venous return from the locomotor limb in humans. J Physiol. 563, 925–943. doi: 10.1113/jphysiol.2004.076422
Mitchell, G. F. (2009). Arterial stiffness and wave reflection: biomarkers of cardiovascular risk. Artery Res. 3, 56–64. doi: 10.1016/j.artres.2009.02.002
Modena, M. G. (2014). Hypertension in postmenopausal women: how to approach hypertension in menopause. High Blood Press Cardiovasc. Prev. 21, 201–204. doi: 10.1007/s40292-014-0057-0
Muka, T., Oliver-Williams, C., Colpani, V., Kunutsor, S., Chowdhury, S., Chowdhury, R., et al. (2016). Association of vasomotor and other menopausal symptoms with risk of cardiovascular disease: a systematic review and meta-analysis. PLoS ONE 11:e0157417. doi: 10.1371/journal.pone.0157417
Patil, S. G., Aithala, M. R., and Das, K. K. (2015). Effect of yoga on arterial stiffness in elderly subjects with increased pulse pressure: a randomized controlled study. Complement Ther. Med. 23, 562–569. doi: 10.1016/j.ctim.2015.06.002
Patil, S. G., Dhanakshirur, G. B., Aithala, M. R., Naregal, G., and Das, K. K. (2014). Effect of yoga on oxidative stress in elderly with grade-I hypertension: a randomized controlled study. J. Clin. Diagn. Res. 8, BC04–BC07. doi: 10.7860/JCDR/2014/9498.4586
Patil, S. G., Patil, S. S., Aithala, M. R., and Das, K. K. (2017). Comparison of yoga and walking-exercise on cardiac time intervals as a measure of cardiac function in elderly with increased pulse pressure. Indian Heart J. 69, 485–490. doi: 10.1016/j.ihj.2017.02.006
Pick, E., and Keisari, Y. (1980). A simple colorimetric method for the measurement of hydrogen peroxide produced by cells in culture. J. Immunol. Methods 38, 161–170. doi: 10.1016/0022-1759(80)90340-3
Pinheiro, C. H., Medeiros, R. A., Pinheiro, D. G., and Marinho M. D. E. J. (2007). Spontaneous respiratory modulation improves cardiovascular control in essential hypertension. Arq. Bras. Cardiol. 88, 651–659. doi: 10.1590/S0066-782X2007000600005
Reznick, A. Z., and Packer, L. (1994). Oxidative damage to proteins: spectrophotometric method for carbonyl assay. Meth. Enzymol 233, 357–363. doi: 10.1016/S0076-6879(94)33041-7
Sanchez-Barajas, M., Ibarra-Reynoso, L. D. R., Ayala-Garcia, M. A., and Malacara, J. M. (2018). Flow mediated vasodilation compared with carotid intima media thickness in the evaluation of early cardiovascular damage in menopausal women and the influence of biological and psychosocial factors. BMC Womens Health 18:153. doi: 10.1186/s12905-018-0648-3
Sankaralingam, S., Jiang, Y., Davidge, S. T., and Yeo, S. (2011). Effect of exercise on vascular superoxide dismutase expression in high-risk pregnancy. Am. J. Perinatol. 28, 803–810. doi: 10.1055/s-0031-1284230
Satin, J. R., Linden, W., and Millman, R. D. (2014). Yoga and psychophysiological determinants of cardiovascular health: comparing yoga practitioners, runners, and sedentary individuals. Ann. Behav. Med. 47, 231–241. doi: 10.1007/s12160-013-9542-2
Shibata, S., Zhang, R., Hastings, J., Fu, Q., Okazaki, K., Iwasaki, K., et al. (2006). Cascade model of ventricular-arterial coupling and arterial-cardiac baroreflex function for cardiovascular variability in humans. Am. J. Physiol. Heart Circ. Physiol. 291, H2142–H2151. doi: 10.1152/ajpheart.00157.2006
Somani, Y. B., Pawelczyk, J. A., De Souza, M. J., Kris-Etherton, P. M., and Proctor, D. N. (2019). Aging women and their endothelium: probing the relative role of estrogen on vasodilator function. Am. J. Physiol. Heart Circ. Physiol. 317, H395–H404. doi: 10.1152/ajpheart.00430.2018
Thijssen, D. H., Carter, S. E., and Green, D. J. (2016). Arterial structure and function in vascular ageing: are you as old as your arteries? J. Physiol. 594, 2275–2284. doi: 10.1113/JP270597
Thijssen, D. H. J., Bruno, R. M., van Mil, A., Holder, S. M., Faita, F., Greyling, A., et al. (2019). Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Heart J. 40, 2534–2547. doi: 10.1093/eurheartj/ehz350
Townsend, R. R., Wilkinson, I. B., Schiffrin, E. L., Avolio, A. P., Chirinos, J. A., Cockcroft, J. R., et al. (2015). Recommendations for improving and standardizing vascular research on arterial stiffness: a scientific statement from the american heart association. Hypertension 66, 698–722. doi: 10.1161/HYP.0000000000000033
Wei, Y., Sowers, J. R., Nistala, R., Gong, H., Uptergrove, G. M., Clark, S. E., et al. (2006). Angiotensin II-induced NADPH oxidase activation impairs insulin signaling in skeletal muscle cells. J. Biol. Chem. 281, 35137–35146. doi: 10.1074/jbc.M601320200
Witkowski, S., and Serviente, C. (2018). Endothelial dysfunction and menopause: is exercise an effective countermeasure? Climacteric 21, 267–275. doi: 10.1080/13697137.2018.1441822
Wong, A., and Figueroa, A. (2014). Eight weeks of stretching training reduces aortic wave reflection magnitude and blood pressure in obese postmenopausal women. J. Hum. Hypertens. 28, 246–250. doi: 10.1038/jhh.2013.98
Yamamoto, K., Kawano, H., Gando, Y., Iemitsu, M., Murakami, H., Sanada, K., et al. (2009). Poor trunk flexibility is associated with arterial stiffening. Am. J. Physiol. Heart Circ. Physiol. 297, H1314–H1318. doi: 10.1152/ajpheart.00061.2009
Keywords: hypertension, arterial stiffness, endothelial function, yoga, breathing, oxidative stress
Citation: Fetter C, Marques JR, de Souza LA, Dartora DR, Eibel B, Boll LFC, Goldmeier SN, Dias D, De Angelis K and Irigoyen MC (2020) Additional Improvement of Respiratory Technique on Vascular Function in Hypertensive Postmenopausal Women Following Yoga or Stretching Video Classes: The YOGINI Study. Front. Physiol. 11:898. doi: 10.3389/fphys.2020.00898
Received: 09 December 2019; Accepted: 06 July 2020;
Published: 27 August 2020.
Edited by:
Felix W. Wehrli, University of Pennsylvania, United StatesReviewed by:
Barbara Ruszkowska-Ciastek, Nicolaus Copernicus University in Torun, PolandCopyright © 2020 Fetter, Marques, de Souza, Dartora, Eibel, Boll, Goldmeier, Dias, De Angelis and Irigoyen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Cláudia Irigoyen, aGlwaXJpZ295ZW5AaW5jb3IudXNwLmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.