 Daniel G. Whitney
Daniel G. Whitney Mark D. Peterson
Mark D. Peterson
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol., 07 January 2019
Sec. Exercise Physiology
Volume 9 - 2018 | https://doi.org/10.3389/fphys.2018.01871
This article is part of the Research TopicPrecision Physical Activity and Exercise Prescriptions for Disease Prevention: The Effect of Interindividual Variability Under Different Training ApproachesView all 12 articles
The purpose of this study was to compare the predictive capacity of different post-processing methods of hand grip strength (GS) for mortality and incident cerebrovascular events in older adults. A sample of 4,143 participants aged 65 years and older was included from the National Health and Aging Trends Study (NHATS) and followed for 6 years. GS measures included baseline (i.e., round 1) (1) absolute GS, (2) GS divided by body mass (NGSmass), and (3) GS divided by body mass index (NGSBMI), as well as (4) change in absolute GS from round 1 to round 2 (GS1-2). Cox proportional hazards regression models were used to examine the association between sex- and age group-specific tertiles of GS measures (weak, moderate-strength, strong) with mortality (n = 641) and incident cerebrovascular events (n = 329). Absolute GS (hazard ratio [HR] = 1.83; 95% confidence interval [CI] = 1.51–2.22), NGSmass (HR = 1.46; 95% CI = 1.21–1.76), and NGSBMI (HR = 1.50; 95% CI = 1.24–1.82) were each associated with mortality among weak participants, but not GS1-2 (HR = 1.10; 95% CI = 0.99–1.46). NGSmass (HR = 1.54; 95% CI = 1.19–2.01) and NGSBMI (HR = 1.37; 95% CI = 1.06–1.79) were both associated with incident cerebrovascular event among weak participants, but not absolute GS (HR = 1.12; 95% CI = 0.86–1.47) or GS1-2 (HR = 1.11; 95% CI = 0.85–1.44). Absolute GS, NGSmass, and NGSBMI were each associated with mortality, whereas only NGSmass and NGSBMI were associated with cerebrovascular event. These findings suggest that different post-processing methods of GS may have differing predictive capacity in the elderly depending on the outcome of interest; however, since NGS measures were associated with both mortality and cerebrovascular events, they may be considered advantageous for screening in older adults.
Muscle strength capacity is a primary determinant of many functional aspects of daily living in older adults, including physical function, cardiometabolic health, and psychosocial wellbeing. The preservation of muscle strength with advancing age, through physical activity and exercise, is an important determinant of disease prevention and longevity (McGrath et al., 2018a). Hand grip strength (GS) is a reliable, inexpensive, and easily utilized surrogate of muscle strength (Peolsson et al., 2001; Savva et al., 2014), and has shown validity and reliability between different devices (Chkeir et al., 2012). Given that GS is highly associated with other measures of muscle strength (e.g., lower extremity strength capacity), it may be considered a valid proxy indicator of overall strength capacity (Cooper et al., 2013). Muscle weakness, as determined by GS assessment, is associated with increased risk of functional disabilities (McGrath et al., 2017b, 2018c), fracture (Dixon et al., 2005), cardiometabolic disease (Peterson et al., 2016a,b,d, 2017; McGrath et al., 2017c), musculoskeletal morbidities (Rikkonen et al., 2012; McGrath et al., 2017a), and early mortality (Leong et al., 2015; Peterson et al., 2016c; Oksuzyan et al., 2017; Celis-Morales et al., 2018). Moreover, statistical modeling of GS significantly improves prediction of morbidity and mortality beyond established office based risk scores (Celis-Morales et al., 2018), and is a stronger predictor of all-cause mortality than even systolic blood pressure (Leong et al., 2015).
Representatives from a variety of institutions participating in the Foundation for the National Institutes of Health (FNIH) Sarcopenia Project concluded that GS should be utilized to assess muscle weakness in the clinical setting (Studenski et al., 2014). There has been debate about the optimal methods for modeling GS in statistical prediction across health outcomes and populations. Most studies investigate absolute GS in an attempt to simplify the interpretation of findings in singular units; whereas we and others have preferred the use of normalizing GS (NGS) by incorporating body composition measures relative to GS (Lawman et al., 2016; Peterson et al., 2016a,b,c, 2017; McGrath et al., 2017a,b,c, 2018c). The FNIH Sarcopenia Project found that muscle weakness defined by GS normalized to body mass index was a stronger predictor of mobility impairment than absolute GS (McLean et al., 2014). Other post-processing techniques that are easily interpretable and computed in a clinical setting include normalizing GS to body mass (Peterson et al., 2016a,b) or assessing change in GS over time (Sirola et al., 2006; Karvonen-Gutierrez et al., 2018). Identifying which post-processing methods of GS is the strongest predictor of clinically important outcomes among older adults will provide clinicians better predictive options for evaluating muscle weakness in the elderly population. This has important implications for longitudinal monitoring or evaluating the efficacy of exercise interventions aimed at mitigating adverse health outcomes in the elderly. Accordingly, the purpose of this study was to determine which of the most common and easily utilized post-processing methods of GS (i.e., absolute GS, normalized GS, change in GS) was the strongest predictor of mortality and incident cerebrovascular events (myocardial infarction or stroke) in a sample of Medicare beneficiaries aged 65 and older.
Data were from the National Health and Aging Trends Study (NHATS). NHATS utilized a multistage survey design, sampling >8,000 Medicare beneficiaries aged 65+ with an annual face-to-face interview conducted by trained study personnel. Non-Hispanic Blacks and those aged 90+ were oversampled. NHATS started in 2011 and subjects were assessed each year for a total of six rounds. Response rates were 71% at baseline. Additional information pertaining to NHATS study design, methodology, and survey instruments is available from https://www.nhats.org/. The NHATS study protocol was approved by The Johns Hopkins University Institutional Review Board.
Of the 8,245 participants at baseline, 4,102 participants were excluded from the analyses because they dropped out of the study, were unable to answer survey questions on their own, had dementia, or had incomplete data for baseline GS, baseline body mass, baseline height, round 2 GS, or survival. Survey weights were not applied because the purpose of this study was to compare the different post-processing methods of GS for mortality and incident cerebrovascular events. Therefore, the sample is the same for each of the outcome variables.
The participant’s death was reported to the study personnel by informants during attempts to contact the participant for their annual interview. Since inclusion criteria required data for round 2 GS, survival time was computed as the annual rate for living and deceased participants from round 1 (alive) to rounds 3–6.
An incident cerebrovascular event was determined if participants reported myocardial infarction or stroke on the basis of an affirmative response to: “Please tell me if a doctor ever told you that you had [a heart attack or myocardial infarction/a stroke]?” Participants were excluded from analyses with cerebrovascular event as the outcome variable if they reported a cerebrovascular event at round 1. Myocardial infarction and stroke were combined into 1 category because of the low number of individuals who experienced either event that also met inclusion criteria.
The NHATS measured absolute GS (in kg) using a digital, adjustable hand dynamometer (Jamar Plus) in those that did not have surgery or flare up of pain in both hands or wrists, or have surgery in the arms or shoulders within the last 3 months. Participants were asked to squeeze the dynamometer as hard as they could with their arm at their side and elbow bent at 90 degrees. GS was measured twice and the highest value was used for this investigation. Height and body mass were self-reported. Body mass index (BMI) was calculated as follows: body mass (kg)/height (m)2. Four GS measures were computed: (1) baseline absolute GS; (2) baseline absolute GS divided by body mass (NGSmass); (3) baseline absolute GS divided by BMI (NGSBMI); and (4) percent change in GS from round 1 to round 2 (GS1-2).
Age and sex were available for all participants. Age was categorized into the following groups: 65–74, 75–84, and 85+ years. Weight status was determined by BMI and separated into the following categories: underweight (<18.5 kg/m2); normal weight (18.5–24.9 kg/m2); overweight (25.0–29.9 kg/m2); and obese (≥30.0 kg/m2).
Descriptive characteristics and GS measures were summarized as means ± SD or frequency (percentage). For each GS measure, sex- and age group-specific tertiles were created to categorize participants into the following muscle strength capacity groups: weak, moderate-strength, and strong. This method allowed for the comparative predictive assessment of GS for each of the outcomes of interest without introducing the confounding effects of age and sex. Unadjusted Cox proportional hazards regression models were used to examine the association between each transformed GS measure and mortality and incident cerebrovascular events. Participants were right censored at round 6 if they were alive (when modeling for mortality) or had no cerebrovascular events (when modeling for incident cerebrovascular events). Since GS measures were standardized using sex and age groups, the hazard ratios (HR) and 95% confidence intervals (CI) were examined to determine which sex- and age-adjusted GS measures were the strongest predictor of each outcome. All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, United States).
Descriptive characteristics and GSs of study participants in the entire sample (n = 4,143) and by sex (45.1% male) are presented in Table 1. Over the 6 rounds, 641 participants were reported to be deceased (15.5%). Of those without a reported cerebrovascular event at round 1 (n = 3,309), 329 had acquired a cerebrovascular event (9.9%).
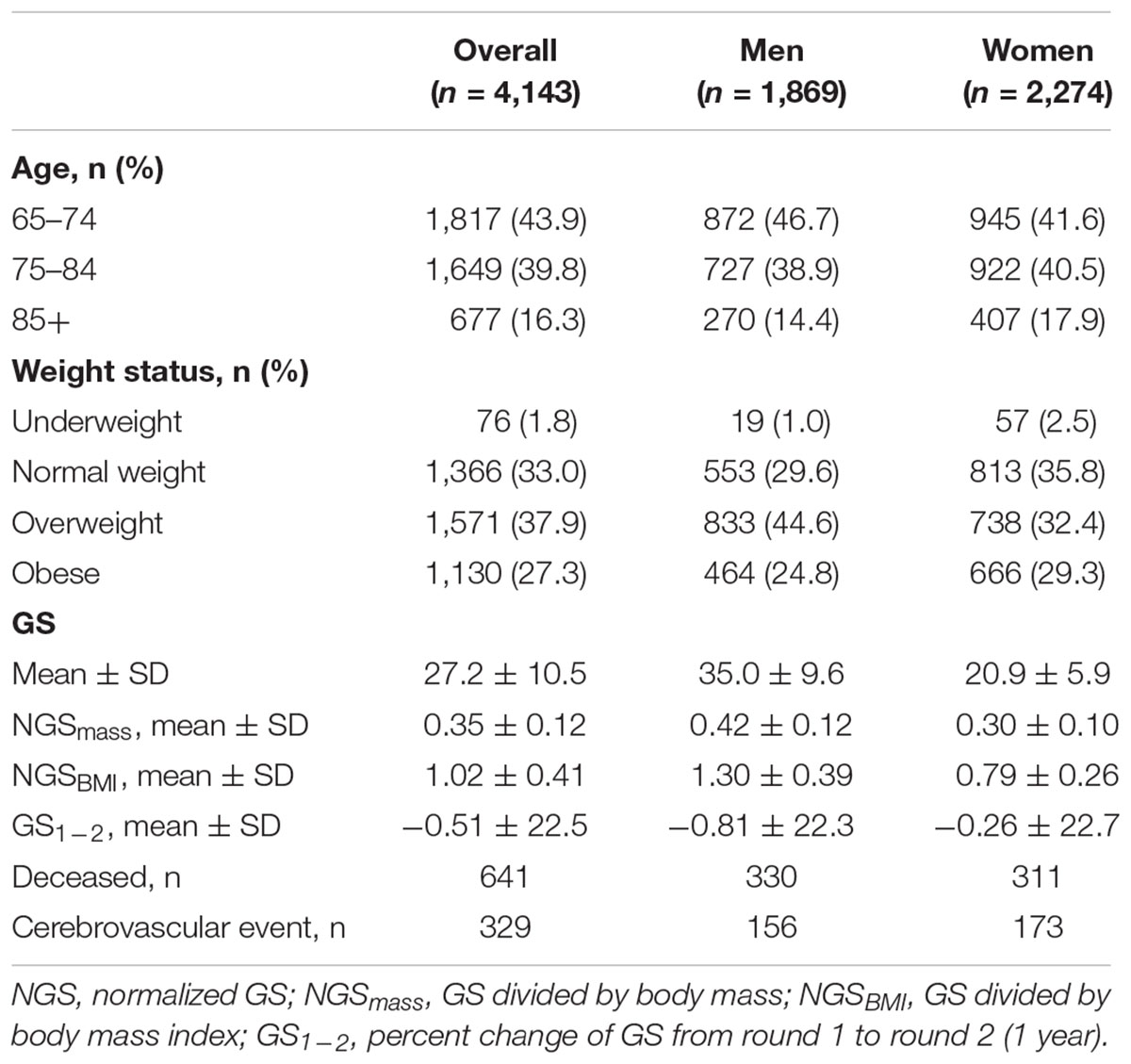
Table 1. Baseline descriptive characteristics and grip strength (GS) measures of the participants.
Table 2 shows the results of the Cox regression models for the association between sex- and age-specific GS tertiles (reference: strong participants [highest tertile]) and mortality. For weak participants (lowest tertile), GS had the largest HR with mortality (HR = 1.83; 95% CI = 1.51–2.22), followed by NGSBMI (HR = 1.50; 95% CI = 1.24–1.82) and NGSmass (HR = 1.46; 95% CI = 1.21–1.76). GS1-2 was not significantly associated with mortality for weak participants (HR = 1.20; 95% CI = 0.99–1.46). For moderate-strength participants (middle tertile), only GS was significantly associated with mortality (HR = 1.42; 95% CI = 1.16–1.73).
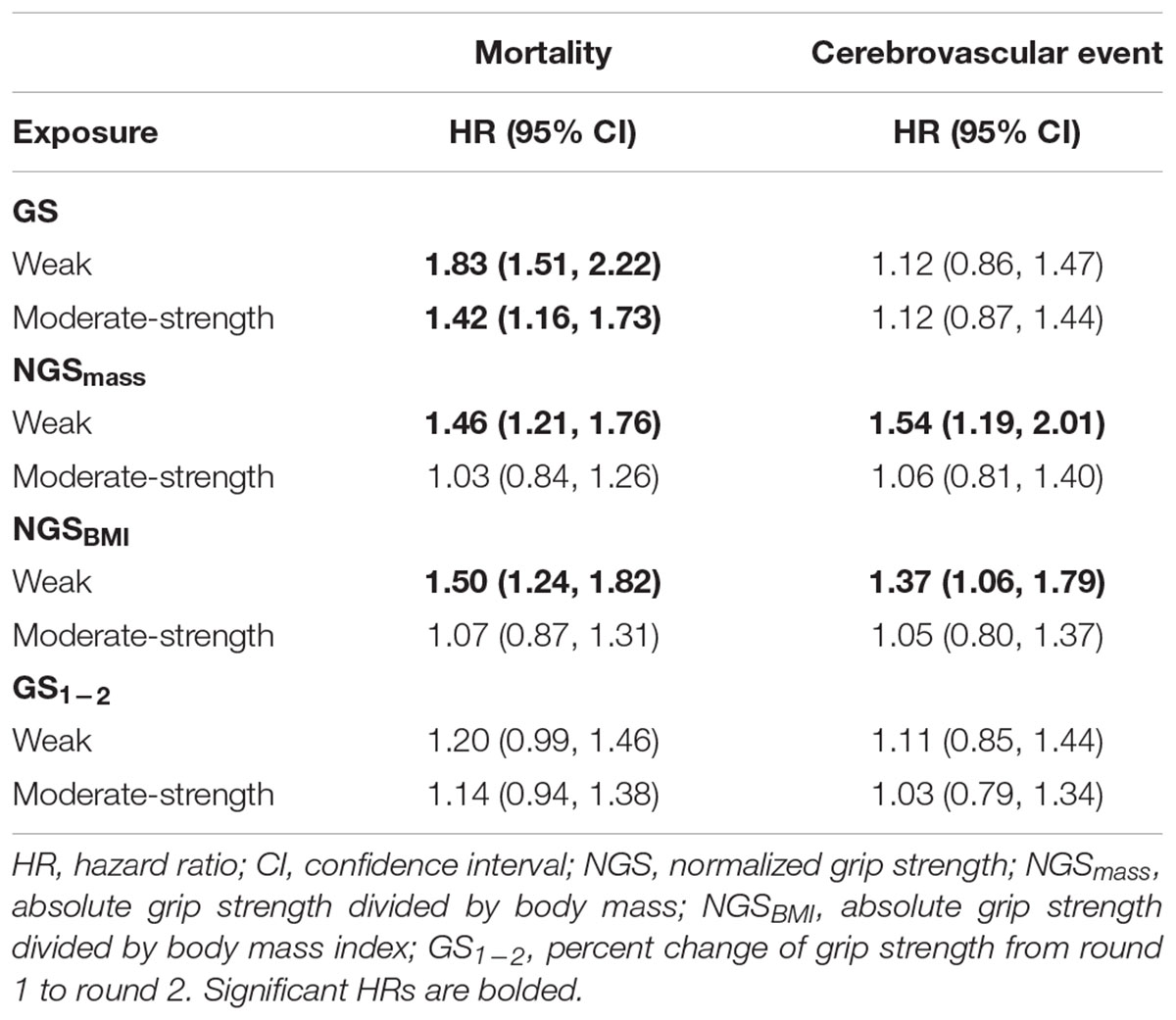
Table 2. Cox proportional hazards regression for the association between sex- and age group-specific tertiles for grip strength (GS) measures (reference group: strong tertile) with mortality (n = 4,143) and cerebrovascular event (n = 3,309).
Table 2 shows the results of the Cox regression models for the association between sex- and age-specific GS tertiles (reference: strong participants) and incident cerebrovascular events. For weak participants, NGSmass had the largest HR with cerebrovascular event (HR = 1.54; 95% CI = 1.19–2.01), followed by NGSBMI (HR = 1.37; 95% CI = 1.06–1.79). GS (HR = 1.12; 95% CI = 0.86–1.47) and GS1-2 (HR = 1.11; 95% CI = 0.85–1.44) were not significantly associated with a cerebrovascular event. For moderate-strength participants, none of the predictors were significantly associated with a cerebrovascular event (HR = 1.03–1.12; all p > 0.05).
The primary findings of this study were that both GS and NGS measures were significant predictors of mortality in older adults, and that NGS measures were significant predictors of incident cerebrovascular events. For predicting mortality, GS had a higher HR than NGS or change in GS; whereas NGS measures were stronger predictors of cerebrovascular events than GS or changes in GS. These findings suggest that different post-processing methods of GS may have differing predictive capacities in the elderly depending on the outcome of interest; however, since NGS was robustly associated with both mortality and cerebrovascular events, it may be considered as a viable standalone tool for screening in older adults. Moreover, considering the well-established role of exercise and physical activity on muscle strength, body composition, and mitigating adverse health outcomes, NGS may serve as a better proxy than absolute GS for determining efficacy of exercise interventions because it encompasses both muscle strength and body composition.
The findings that absolute and NGS measures were associated with mortality and cerebrovascular event are consistent with previous reports (Leong et al., 2015; Peterson et al., 2016c; Oksuzyan et al., 2017; Celis-Morales et al., 2018). The finding that change in GS was not associated with adverse health outcomes is consistent with another report (Karvonen-Gutierrez et al., 2018). While it seems intuitive that a higher rate of strength decline would correspond to a higher rate of acquiring adverse health outcomes, our methodology was limited in adequately addressing this notion. In the current investigation, we used a time interval of 1 year to assess strength change, which may not have been long enough to capture greater strength declines across advancing age. Moreover, our sample included adults 65 years and older. The rate of strength decline from young- or middle-age may be more predictive of later functioning and health outcomes in the elder years.
The difference in associations between absolute GS versus NGS measures with mortality and cerebrovascular events may reflect the influence of body composition or the role of obesity. Myint et al. (2014) found that measures of body composition (BMI, body fat percent, and waist-to-hip ratio) were stronger predictors of incident cardiovascular disease than mortality in middle- and older-age adults. Therefore, by incorporating body mass or BMI, NGS may be a superior predictor for cerebrovascular events than for mortality, as it encompasses important constituents (i.e., body composition) for cerebrovascular function.
Another potential explanation for the unique associations found for absolute GS vs. NGS measures is the so-called “obesity paradox,” where there is lower mortality in those with cardiovascular disease who are obese compared to non-obese (Curtis et al., 2005; Angeras et al., 2013; Flegal et al., 2013), but not in those who are morbidly obese (Angeras et al., 2013). In the publically available NHATS dataset, mortality information is denoted as “deceased” or not, thus providing a “catch-all” cause of mortality. Further, in the current investigation, all participants who reported a cerebrovascular event were alive in the same round. Therefore, since absolute GS is a general measure of muscle strength capacity, it may capture the wider and non-specific construct of all-cause mortality and reflect the obesity paradox, i.e., those with greater BMIs may have greater absolute GSs (Lawman et al., 2016). On the other hand, GS normalized to body composition may be more specific to cardiometabolic-related morbidity and mortality, i.e., those with greater body masses or BMIs relative to GS may reflect poor cerebrovascular and metabolic health profiles (Lawman et al., 2016). Unfortunately, we were unable to determine how the different post-processing methods of GS were associated with specific causes of mortality.
The association between muscle weakness and adverse health outcomes is likely driven in part by poor physical functioning (McGrath et al., 2018b). While muscle weakness is inversely associated with physical functioning (Henriksen et al., 2012; Ryder et al., 2013), normalized strength is more strongly associated with physical functioning than absolute strength (Schiller et al., 2000; Henriksen et al., 2012). The caveat in examining absolute GS is that individuals with a high body mass or BMI likely have a higher GS relative to their physical functioning ability. Therefore, normalized strength capacity may provide a better indicator of the ability for that individual to maneuver his/her body through space and perform physical activities. Interestingly, when we examined the strength profiles of the obese participants who were classified as “strong” according to absolute GS (upper GS tertile), nearly 80% were considered “moderate-strength” or “weak” according to NGS measures. These findings highlight the potential benefits of using NGS in evaluating muscle strength capacity in the elderly.
There are other limitations that need to be discussed. First, height and weight were self-reported, which may have influenced measures adjusting for body composition. Stommel and Schoenborn (2009) found that misclassification of weight status by self-report height and weight to determine BMI was more pronounced on the extreme ends, including underweight and obese. However, deviations of BMI values were modest, with the majority (56%) of misclassifications having self-reported BMI values within one-unit interval of their measured BMI. Second, we did not adjust models for sociodemographics, socioeconomics, or morbidities. Whether the difference in associations among the GSs with outcomes are mediated uniquely by confounding variables is unknown and requires future investigation.
In conclusion, NGS measures were significantly associated with both mortality and incident cerebrovascular event, whereas absolute GS was only significantly associated with mortality. Changes in GS were not significantly associated with mortality or incident cerebrovascular event; however, the lack of association may have been due to a short follow up period. These findings are important as they provide evidence of unique associations between clinically important aging outcomes with a variety of commonly used post-processing methods of GS that can be easily utilized in a clinical setting.
DW and MP designed the study and approved the final manuscript. DW contributed to data ascertainment, data analysis, and prepared the manuscript.
DW was supported by the University of Michigan Advanced Rehabilitation Research Training Program in Community Living and Participation from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) (90AR5020-0200). MP was supported in part by the Claude D. Pepper Center grant number AG024824 and Michigan Institute for Clinical and Health Research grant number UL1TR002240. The study sponsors had no role in the study design, collection, analysis, or interpretation of data, in writing the report, or in the decision to submit.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Angeras, O., Albertsson, P., Karason, K., Ramunddal, T., Matejka, G., James, S., et al. (2013). Evidence for obesity paradox in patients with acute coronary syndromes: a report from the Swedish Coronary Angiography and Angioplasty Registry. Eur. Heart J. 34, 345–353. doi: 10.1093/eurheartj/ehs217
Celis-Morales, C. A., Welsh, P., Lyall, D. M., Steell, L., Petermann, F., Anderson, J., et al. (2018). Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: prospective cohort study of half a million UK Biobank participants. BMJ 361:k1651. doi: 10.1136/bmj.k1651
Chkeir, A., Jaber, R., Hewson, D. J., and Duchene, J. (2012). Reliability and validity of the Grip-Ball dynamometer for grip-strength measurement. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2012, 1996–1999. doi: 10.1109/EMBC.2012.6346348
Cooper, C., Fielding, R., Visser, M., van Loon, L. J., Rolland, Y., Orwoll, E., et al. (2013). Tools in the assessment of sarcopenia. Calcif. Tissue Int. 93, 201–210. doi: 10.1007/s00223-013-9757-z
Curtis, J. P., Selter, J. G., Wang, Y., Rathore, S. S., Jovin, I. S., Jadbabaie, F., et al. (2005). The obesity paradox: body mass index and outcomes in patients with heart failure. Arch. Intern. Med. 165, 55–61. doi: 10.1001/archinte.165.1.55
Dixon, W. G., Lunt, M., Pye, S. R., Reeve, J., Felsenberg, D., Silman, A. J., et al. (2005). Low grip strength is associated with bone mineral density and vertebral fracture in women. Rheumatology 44, 642–646. doi: 10.1093/rheumatology/keh569
Flegal, K. M., Kit, B. K., Orpana, H., and Graubard, B. I. (2013). Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA 309, 71–82. doi: 10.1001/jama.2012.113905
Henriksen, M., Christensen, R., Danneskiold-Samsoe, B., and Bliddal, H. (2012). Changes in lower extremity muscle mass and muscle strength after weight loss in obese patients with knee osteoarthritis: a prospective cohort study. Arthritis Rheum. 64, 438–442. doi: 10.1002/art.33394
Karvonen-Gutierrez, C. A., Peng, Q., Peterson, M., Duchowny, K., Nan, B., and Harlow, S. (2018). Low grip strength predicts incident diabetes among mid-life women: the Michigan Study of Women’s Health Across the Nation. Age Ageing 47, 685–691. doi: 10.1093/ageing/afy067
Lawman, H. G., Troiano, R. P., Perna, F. M., Wang, C. Y., Fryar, C. D., and Ogden, C. L. (2016). Associations of relative handgrip strength and cardiovascular disease biomarkers in U.Adults, 2011-2012. Am. J. Prev. Med. 50, 677–683. doi: 10.1016/j.amepre.2015.10.022
Leong, D. P., Teo, K. K., Rangarajan, S., Lopez-Jaramillo, P., Avezum, A. Jr., Orlandini, A., et al. (2015). Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 386, 266–273. doi: 10.1016/S0140-6736(14)62000-6
McGrath, R. P., Kraemer, W. J., Snih, S. A., and Peterson, M. D. (2018a). Handgrip strength and health in aging adults. Sports Med. 48, 1993–2000. doi: 10.1007/s40279-018-0952-y
McGrath, R. P., Vincent, B. M., Lee, I. M., Kraemer, W. J., and Peterson, M. D. (2018b). Handgrip strength, function, and mortality in older adults: a time-varying approach. Med. Sci. Sports Exerc. 50, 2259–2266. doi: 10.1249/MSS.0000000000001683
McGrath, R., Robinson-Lane, S. G., Peterson, M. D., Bailey, R. R., and Vincent, B. M. (2018c). Muscle strength and functional limitations: preserving function in older mexican americans. J. Am. Med. Dir. Assoc. 19, 391–398. doi: 10.1016/j.jamda.2017.12.011
McGrath, R. P., Kraemer, W. J., Vincent, B. M., Hall, O. T., and Peterson, M. D. (2017a). Muscle strength is protective against osteoporosis in an ethnically diverse sample of adults. J. Strength Cond. Res. 31, 2586–2589. doi: 10.1519/JSC.0000000000002080
McGrath, R. P., Ottenbacher, K. J., Vincent, B. M., Kraemer, W. J., and Peterson, M. D. (2017b). Muscle weakness and functional limitations in an ethnically diverse sample of older adults. Ethn. Health doi: 10.1080/13557858.2017.1418301 [Epub ahead of print].
McGrath, R., Vincent, B. M., Al, S., Snih Markides, K. S., and Peterson, M. D. (2017c). The association between muscle weakness and incident diabetes in older Mexican Americans. J. Am. Med. Dir. Assoc. 18:e457-52. doi: 10.1016/j.jamda.2017.01.017
McLean, R. R., Shardell, M. D., Alley, D. E., Cawthon, P. M., Fragala, M. S., Harris, T. B., et al. (2014). Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: the foundation for the National Institutes of Health (FNIH) sarcopenia project. J. Gerontol. A Biol. Sci. Med. Sci. 69, 576–583. doi: 10.1093/gerona/glu012
Myint, P. K., Kwok, C. S., Luben, R. N., Wareham, N. J., and Khaw, K. T. (2014). Body fat percentage, body mass index and waist-to-hip ratio as predictors of mortality and cardiovascular disease. Heart 100, 1613–1619. doi: 10.1136/heartjnl-2014-305816
Oksuzyan, A., Demakakos, P., Shkolnikova, M., Thinggaard, M., Vaupel, J. W., Christensen, K., et al. (2017). Handgrip strength and its prognostic value for mortality in Moscow, Denmark, and England. PLoS One 12:e0182684. doi: 10.1371/journal.pone.0182684
Peolsson, A., Hedlund, R., and Oberg, B. (2001). Intra- and inter-tester reliability and reference values for hand strength. J. Rehabil. Med. 33, 36–41. doi: 10.1080/165019701300006524
Peterson, M. D., Duchowny, K., Meng, Q., Wang, Y., Chen, X., and Zhao, Y. (2017). Low normalized grip strength is a biomarker for cardiometabolic disease and physical disabilities among U. S. and Chinese Adults. J. Gerontol. A Biol. Sci. Med. Sci. 72, 1525–1531. doi: 10.1093/gerona/glx031
Peterson, M. D., McGrath, R., Zhang, P., Markides, K. S., Al, Snih S, and Wong, R. (2016a). Muscle weakness is associated with diabetes in older mexicans: the Mexican health and aging study. J. Am. Med. Dir. Assoc. 17, 933–938. doi: 10.1016/j.jamda.2016.06.007
Peterson, M. D., Zhang, P., Choksi, P., Markides, K. S., and Al Snih, S. (2016b). Muscle weakness thresholds for prediction of diabetes in adults. Sports Med. 46, 619–628. doi: 10.1007/s40279-015-0463-z
Peterson, M. D., Zhang, P., Duchowny, K. A., Markides, K. S., Ottenbacher, K. J., and Snih, S. A. (2016c). Declines in strength and mortality risk among older mexican americans: joint modeling of survival and longitudinal data. J. Gerontol. A Biol. Sci. Med. Sci. 71, 1646–1652.
Peterson, M. D., Zhang, P., Saltarelli, W. A., Visich, P. S., and Gordon, P. M. (2016d). Low muscle strength thresholds for the detection of cardiometabolic risk in adolescents. Am. J. Prev. Med. 50, 593–599. doi: 10.1016/j.amepre.2015.09.019
Rikkonen, T., Sirola, J., Salovaara, K., Tuppurainen, M., Jurvelin, J. S., Honkanen, R., et al. (2012). Muscle strength and body composition are clinical indicators of osteoporosis. Calcif. Tissue Int. 91, 131–138. doi: 10.1007/s00223-012-9618-1
Ryder, J. W., Buxton, R. E., Goetchius, E., Scott-Pandorf, M., Hackney, K. J., Fiedler, J., et al. (2013). Influence of muscle strength to weight ratio on functional task performance. Eur. J. Appl. Physiol. 113, 911–921. doi: 10.1007/s00421-012-2500-z
Savva, C., Giakas, G., Efstathiou, M., and Karagiannis, C. (2014). Test-retest reliability of handgrip strength measurement using a hydraulic hand dynamometer in patients with cervical radiculopathy. J. Manip. Physiol. Ther. 37, 206–210. doi: 10.1016/j.jmpt.2014.02.001
Schiller, B. C., Casas, Y. G., Tracy, B. L., DeSouza, C. A., and Seals, D. R. (2000). Age-related declines in knee extensor strength and physical performance in healthy Hispanic and Caucasian women. J. Gerontol. A Biol. Sci. Med. Sci. 55, B563–B569. doi: 10.1093/gerona/55.12.B563
Sirola, J., Rikkonen, T., Tuppurainen, M., Honkanen, R., Jurvelin, J. S., and Kröger, H. (2006). Maintenance of muscle strength may counteract weight-loss-related postmenopausal bone loss–a population-based approach. Osteoporos. Int. 17, 775–782. doi: 10.1007/s00198-005-0054-1
Stommel, M., and Schoenborn, C. A. (2009). Accuracy and usefulness of BMI measures based on self-reported weight and height: findings from the NHANES & NHIS 2001-2006. BMC Public Health 9:421. doi: 10.1186/1471-2458-9-421
Keywords: grip strength, normalized grip strength, mortality, cerebrovascular event, elderly, National Health and Aging Trends Study
Citation: Whitney DG and Peterson MD (2019) The Association Between Differing Grip Strength Measures and Mortality and Cerebrovascular Event in Older Adults: National Health and Aging Trends Study. Front. Physiol. 9:1871. doi: 10.3389/fphys.2018.01871
Received: 05 July 2018; Accepted: 11 December 2018;
Published: 07 January 2019.
Edited by:
Robinson Ramírez-Vélez, Universidad del Rosario, ColombiaReviewed by:
Carlos Celis-Morales, University of Glasgow, United KingdomCopyright © 2019 Whitney and Peterson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel G. Whitney, ZGd3aGl0QG1lZC51bWljaC5lZHU= Mark D. Peterson, bWRwZXRlcnpAbWVkLnVtaWNoLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.