
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Physiol., 23 October 2018
Sec. Exercise Physiology
Volume 9 - 2018 | https://doi.org/10.3389/fphys.2018.01443
This article is part of the Research TopicPrecision Physical Activity and Exercise Prescriptions for Disease Prevention: The Effect of Interindividual Variability Under Different Training ApproachesView all 12 articles
 Cristian Álvarez1†
Cristian Álvarez1† Rodrigo Ramírez-Campillo1†
Rodrigo Ramírez-Campillo1† Carlos Cristi-Montero2†
Carlos Cristi-Montero2† Robinson Ramírez-Vélez3†
Robinson Ramírez-Vélez3† Mikel Izquierdo4*†
Mikel Izquierdo4*†Background: Exercise is known to improve cardiometabolic outcomes; however, results are typically reported as mean values, and there is wide interindividual variability in terms of response that has not been explored in populations at risk for hypertension. Our aim was to investigate both the effects on and the prevalence of non-responders (NRs) for decreasing blood pressure (BP) and other risk factors among prehypertensive women after long-term high-intensity interval training (HIIT). A secondary aim was to report potential variables that can predict decreases in BP after HIIT.
Methods: Sedentary overweight/obese women (age 35.9 ± 5.4 year; body mass index [BMI] 30.9 ± 6.2 kg/m2) were assigned to a prehypertensive (PreHTN; N = 44) or normotensive (NT; N = 40) group according to their ambulatory BP at baseline. Subjects underwent a thrice-weekly 16-week HIIT program (7–10 × 1 min exercise with 2 min of rest). Training-induced changes in body composition and cardiovascular, metabolic, strength, and endurance performance markers were measured, and the prevalence of NRs was reported as a percentage. All outcomes were analyzed by multivariable regression.
Results: Statistically significant (P < 0.05) decreases in systolic BP (SBP) were detected in the PreHTN group (Δ −8 mmHg) compared with baseline, whereas the NT group (Δ + 3 mmHg) showed a non-significant increase in SBP. Diastolic BP (DBP) was significantly decreased in the PreHTN group (Δ −5.8 mmHg) and non-significantly decreased (Δ −2 mmHg) in the NT group. Also, there were significant differences (P < 0.0001) in the prevalence of NRs based on SBP between the PreHTN and NT groups (11.4 vs. 68.8%), but similar prevalence of NRs based on DBP. SBP alone was a powerful predictive factor for a beneficial SBP reduction, explaining 51.2% of the results, which was similar to other more complex models tested.
Conclusion: The prevalence of NRs based on SBP and DBP was different between prehypertensive and normotensive subjects after 16 weeks of HIIT. Other comorbidities such as body composition and metabolic outcomes showed almost similar modifications between prehypertensive and normotensive subjects, being the most basic predictive factor for BP reduction baseline SBP, which we refer to as ‘BP health status’ (51.2%). This improvement in BP was accompanied by other known improvements of HIIT on body composition, metabolic and endurance performance in both study cohorts.
Trial Registration: ClinicalTrials.gov ID: NCT03000140 (Register 20 December, 2016).
The prehypertensive state is generally associated with physical inactivity (not engaged in physical activity according to international physical activity guidelines) (O’Donovan et al., 2010) and other risk factors including diet, sodium intake, and smoking, which is the most important contributor to hypertension (HTN) development (Díaz-Martínez et al., 2017). HTN is also the most common primary diagnosis in Chile, and has increased in adult women from 25.0% in 2009–2010 to 27.7% in 2017 (Hawley, 2009). Because a single session of endurance exercise decreases 24-h blood pressure (BP) (Karoline de Morais et al., 2015), chronic exercise (i.e., regular exposure to exercise) provides powerful benefits for prehypertensive subjects (Park et al., 2006), where the changes (i.e., decreases) of blood pressure in normotensive subjects have been regularly reported. These effects have been corroborated by meta-analyses and, accordingly, prolonged endurance training has been recognized as a strategy to decrease BP and other comorbidities in prehypertensive and hypertensive populations (Montero et al., 2014).
Unfortunately, while there is ample evidence to support that exercise training (e.g., endurance exercise) decreases BP (Pescatello et al., 2015), ‘lack of time’ is frequently cited by the sedentary population as the main barrier to adherence to exercise guidelines (i.e., less than 150 min of low-moderate-intensity exercise/week or 75 min of vigorous-intensity exercise/week) (Trost et al., 2002). Therefore, more research in exercise science is needed for the prevention of HTN and the management of both early prehypertension and common comorbidities including obesity (e.g., waist circumference or fat mass) and dyslipidemia (i.e., to decrease low-density lipoprotein or triglycerides) (Russo et al., 2018). In this regard, high-intensity interval training (HIIT, defined as repeated bouts of high-intensity exercise interspersed with rest periods) has been reported to be a powerful regimen for improving body composition and cardiovascular, metabolic, and performance variables (Gibala et al., 2012). HIIT also reduces both arterial stiffness and microvascular dysfunction in hypertensive individuals (Shrout et al., 2017), and increases the expression of key proteins such as peroxisome proliferator-activated receptor-γ coactivator 1α and vascular endothelial growth factor, that play an important role in arterial remodeling, in trained/healthy subjects (Lim et al., 2012). Moreover, when compared with endurance exercise, HIIT has been shown to improve endothelial function in subjects at risk for HTN (Guimaraes et al., 2010) and also in patients with metabolic syndrome (Tjønna et al., 2008). Despite these beneficial effects from HIIT, it remains unknown whether HIIT impacts BP and comorbidities associated with the prehypertensive state more than normotensive subjects.
Most exercise intervention studies report mean data; however, there is usually wide interindividual variability (Bouchard and Rankinen, 2001). This implies that under the same stimulus, some subjects, referred to as responders (Rs), may achieve benefits, while others, referred to as non-responders (NRs), may exhibit a worsened or unchanged response (Bonafiglia et al., 2016). Although genetic [i.e., some polymorphisms (Yako et al., 2018)] and environmental (regular exercise, diet, and sleep) factors have been described to predictive Rs and NRs (Mann et al., 2014), not all of these factors have been explored in detail, such as the effects of a different ‘BP health status’ (e.g., prehypertension vs. HTN) on the prevalence of NRs after training. For example, it has been widely known that individuals with HTN show power and clinical decreases in blood pressure after traditional endurance exercise training (Cade et al., 1984). A recent report showed that after 6 weeks of HIIT ∼60% of participants were NRs for a decrease in diastolic BP (DBP) (Higgins et al., 2015). By contrast, after 20 weeks of endurance training a minority of subjects were NRs (12.2%), without any decreases in systolic BP (SBP) (Bouchard et al., 2012). Additionally, when prehypertensive individuals underwent 6 months of different training regimens [i.e., endurance, resistant, or concurrent training (i.e., endurance plus resistant training)], ∼60% were NRs for decreases in SBP or DBP (Moker et al., 2014).
Determining both the effects on and prevalence of NRs after HIIT is important for choosing the appropriate exercise regimen and optimizing responses in different cohorts (e.g., athletes or individuals with risk factors for HTN). Furthermore, knowing which variables can predict more changes after training could be useful to more efficiently determine the time to invest in a particular exercise modality. Along this line, some authors have shown that the magnitude of acute changes from chronic exercise is a good predictor of improvements in metabolism (Hecksteden et al., 2013a) and decreases in BP (Hecksteden et al., 2013b). However, neither of these studies simultaneously reported the effects on and the prevalence of NRs, nor determined the variables that can predict responses in populations at risk for HTN. Several studies have reported that certain factors such as exercise modality (Álvarez et al., 2017), acute exercise (Hecksteden et al., 2013b), baseline differences in aerobic fitness (Bouchard and Rankinen, 2001), or metabolic health status (i.e., healthy or diagnosed with a metabolic disease) (Alvarez et al., 2017) can influence the prevalence of NRs, but all have been conducted mainly with normotensive cohorts. Thus, due to the lack of evidence on the effects on and prevalence of NRs after HIIT among prehypertensive than normotensive subjects, and on the potential predictive factors for lowering BP, the aim of the present study was to investigate both the effects on and the prevalence of NRs for decreased BP and comorbidities among prehypertensive women after HIIT. A secondary aim was to report potential variables that predict decreases in BP. Based on previous genetic studies, where the training variation can be attributed to multiple factors, and considering a non-epidemiological sample size (Mann et al., 2014), we hypothesized that independent of training-induced changes there would be a similar effect from HIIT and a similar prevalence of NRs between prehypertensive and normotensive subjects after a 16-week HIIT intervention.
We studied overweight or obese sedentary women [body mass index (BMI) between 25 and 30 kg/m2; aged 30–40 years] who had been diagnosed with prehypertension for at least 1 month but no more than 3 months by our research team. The study inclusion criteria were as follows: (a) ambulatory SBP >120 and <140 mmHg and/or DBP ≥80 and <90 mmHg, according to standard classifications of blood pressure (Pescatello et al., 2015); (b) lack of drug therapy in the previous 3 months; (c) BMI >24 and <35 kg/m2; (d) physical inactivity (i.e., <150 min of low/moderate or <75 min of moderate/vigorous physical activity/week (O’Donovan et al., 2010), as assessed by the International Physical Activity Questionnaire previously validated in the Chilean population) (Seron et al., 2010); and (e) independent of commonly altered metabolic variables (normocholesterolemic/or slightly hypercholesterolemic) [total cholesterol (TC) <200/≥200 mg/dL, low-density lipoprotein cholesterol (LDL-C) <140/≥140 mg/dL, high-density lipoprotein cholesterol (HDL-C) ≤30/>30 mg/dL, and triglycerides (TG) ≤150/>150 mg/dL] following standard classifications (Turnbull et al., 2005). All subjects were not under pharmacological therapy. Subjects with (a) cardiovascular contraindications to exercise; (b) histories of stroke; (c) asthma or chronic obstructive pulmonary disease; (d) musculoskeletal disorders such as muscle or back pain; and (e) a history of smoking in the last 3 months were excluded. A minimum compliance to the exercise program of 70% was required for patients in the intervention group to be included in the final statistical analysis. The trial is registered on ClinicalTrials.gov; ID: NCT03000140 (registered 20 December 2016).
One hundred and ninety-nine healthy and prehypertensive subjects (aged 25 to 40 years) from the Family Healthcare Center Tomas Rojas of Los Lagos (Chile) were invited to participate by phone; these participants were provided with explanations about the study aims (first stage), informed about the study and invited to be formally screened. Subsequently, one hundred and eighty-five (N = 185) subjects agreed to participate in the second stage of screening, the first baseline measurements and the third stage of education regarding the experimental procedures for exercise training. The subjects underwent a structured medical history, medical record review, and physical examination by a physician to assess eligibility based on the criteria. All participants underwent 16 weeks of HIIT by cycling on ergometers and were statistically analyzed as two non-randomized groups: the prehypertensive (PreHTN) and normotensive (NTG) groups. After the intervention period, forty-four subjects were included in the final sample (PreHTN, aged 35.2 ± 5.1 years; BMI 31.9 ± 5.8 kg/m2; N = 44), and forty subjects were included in the normotensive group (NTG, aged 36.6 ± 5.8 years; BMI 30.0 ± 6.6 kg/m2; N = 40). The study design is shown in Figure 1, and the study protocol is shown in Figure 2.
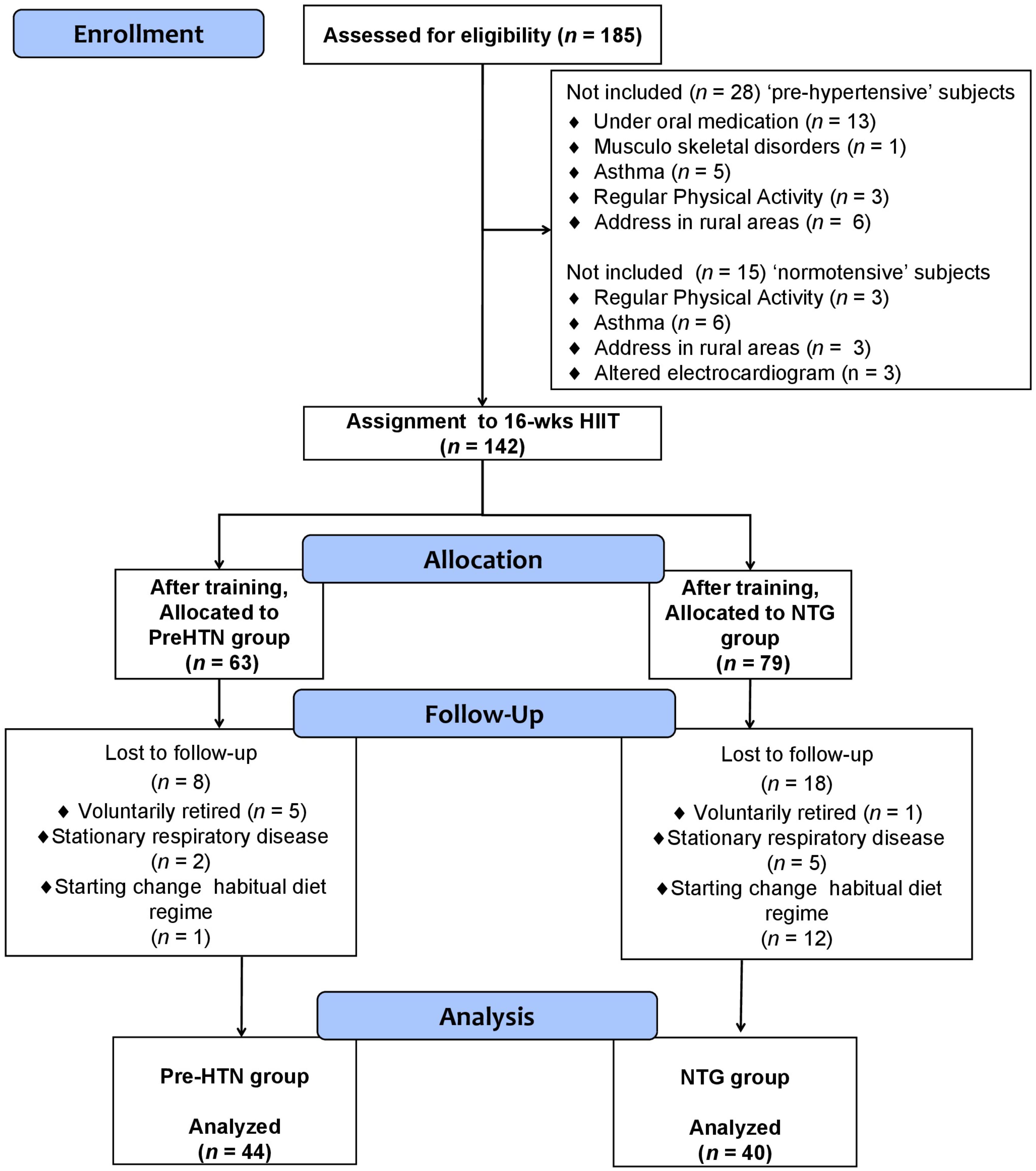
FIGURE 1. Study design.
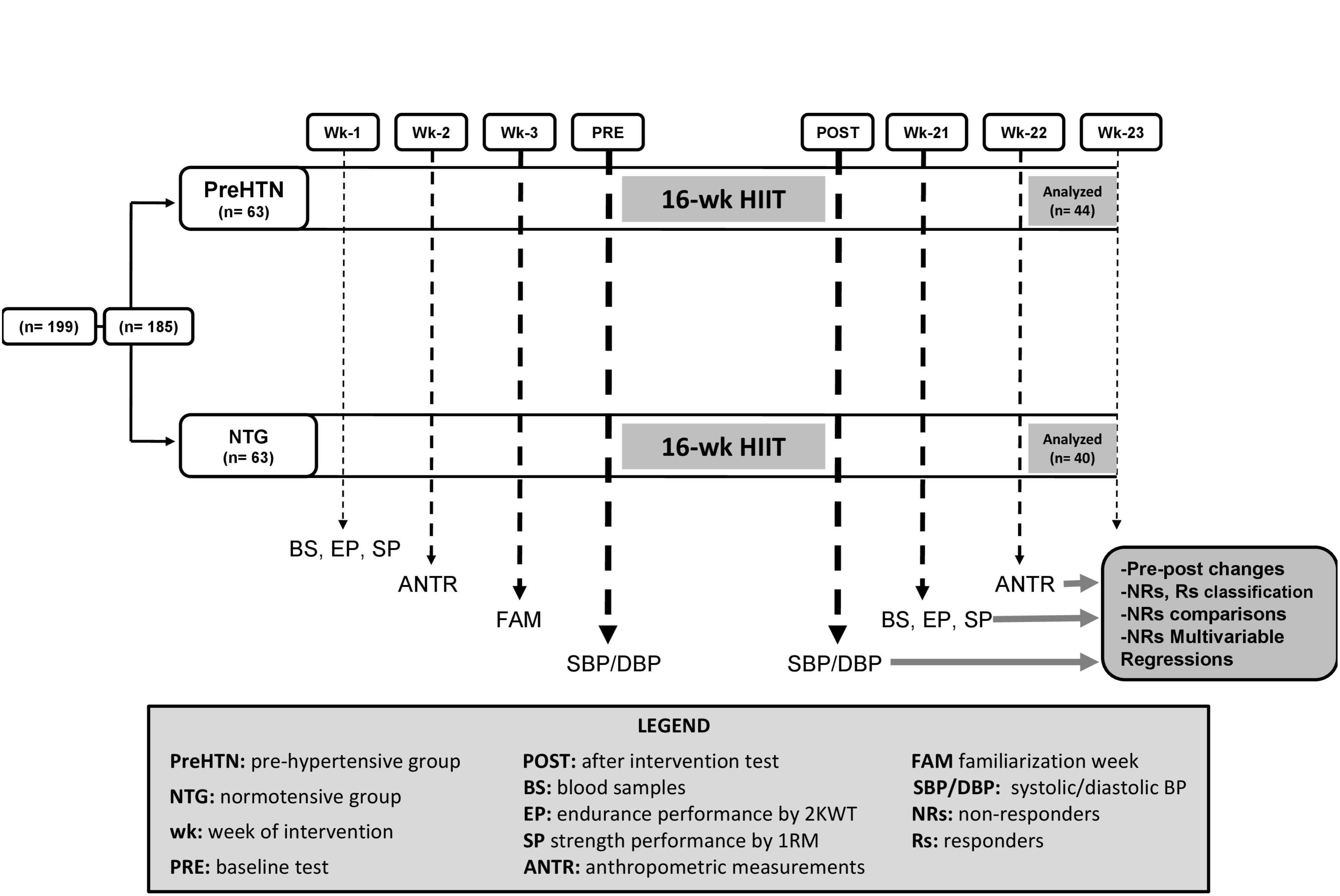
FIGURE 2. Study protocol.
To classify the participants as Rs and NRs based on a decrease in SBP/DBP or the other dependent covariables, the typical error (TE) was calculated, similar to recent studies (Bonafiglia et al., 2016), using the following equation:
where SDdiff is the variance (standard deviation) of the different scores observed between the two repeats of each test. NRs were defined as an individual who failed to demonstrate a decrease or increase (in favor of beneficial changes) that was greater than two times the TE away from zero. A change beyond two times the TE indicates that there is a high probability (i.e., 12 to 1 odds) that this response is a true physiological adaptation beyond what might be expected to result from technical and/or biological variability (Hopkins, 2000). Thus, the cutoff values were the following for body mass, 2 × TE = 0.500 kg; BMI, 2 × TE = 0.21 kg/m2; waist circumference, 2 × TE = 1.1 cm; tricipital skinfold, 2 × TE = 1.3 mm; suprailiac skinfold, 2 × TE = 2.6 mm; abdominal skinfold, 2 × TE = 2.9 mm; fat mass, 2 × TE = 3.8%; muscle mass, 2 × TE = 0.3 kg; systolic BP, 2 × TE = 8.0 mmHg; diastolic BP, 4.9 mmHg; heart rate at rest, 2 × TE = 5.4 beats/min; fasting glucose, 2 × TE = 4.5 mg/dL; TC, 2 × TE = 7.1 mg/dL; LDL-C, 2 × TE = 5.2 mg/dL; HDL-C, 2 × TE = 3.9 mg/dL; TG, 2 × TE = 14.6 mg/dL; 1RMLE, 2 × TE = 5.0 kg; and 2KMWT, 2 × TE = 1.5 min/s.
Before the intervention, all subjects were familiarized with the HIIT program over three sessions. The participants underwent a thrice-weekly progressive program for 16 weeks. All exercise sessions were performed on cycle ergometers (OXFORDTM, model BE2601, OXFORD Inc., Santiago, Chile) and were supervised by an exercise physiologist. The HIIT program consisted of high-intensity intervals of work (cycling) for 1 min at a subjective intensity of 8–10 points on the modified Borg scale, which ranges from 1–10 points, similar to other reports (Álvarez et al., 2017) separated by an inactive (no movement on the bicycle) recovery period of 2 min. The training sessions were structured according to the following progression (presented in time cycling/rest/repetitions): weeks 1–4: 1/2/7; weeks 5–8: 1/2/8; weeks 9–12: 1/2/9; and weeks 13–16: 1/2/10. The total range of time investment was as follows: weeks 1–4, 21 min; and weeks 13–16, 30 min/session). Heart rate was continuously monitored among the subjects (ProTrainer 5, Polar Electro, Inc., Kempele, Finland), and their efforts were adjusted to maintain cycling at the subjective effort proposed. Thus, when a subject reported starting the first interval of cycling at 8–10 points on the Borg scale (corresponding to a 100-watt load, for example), this level was rechecked at each of the 3 sessions, and it was usually necessary to increase the load (watts) of cycling to maintain an initial intensity of cycling at 8–10 points, according to the normal exercise adaptations to a new threshold. This subjective intensity corresponded with all intervals of work to a range from 70–100% of the maximum heart rate based on age.
Compliance indices for attendance were calculated for the groups by dividing the total number of sessions attended by the number of training sessions prescribed in percentages. Intensity adherence was calculated from the mean 8 ± 2 points on the Borg modified scale (1–10) based on the cycling ratings across all exercises and sessions for weeks 2–16. The results showed that exercise compliance was 85.1% (41 sessions) in the PreHTN group and 93.7% (45 sessions) in the NTG, and there were no significant differences between groups.
For three sessions prior to the start of the pediment, participants were familiarized with the tests, and 1 week before and after the 16-week follow-up, anthropometric, cardiovascular, metabolic, and performance measurements were obtained. Body mass (kg) was measured (to the nearest 0.1 kg) using a professional scale (Health o MeterTM Professional, Sunbeam Products, Inc., Chicago, IL, United States). Height (m) was assessed using the same machine to the nearest 0.1 m of accuracy, similar to previous studies (Jebb et al., 2007). BMI was calculated as body mass divided by height squared (kg/m2). Waist circumference (cm) was measured to the nearest 0.1 cm using a flexible and unextendible measuring tape (HoechstmassTM, Sulzbach, Germany). Four skinfold thickness measurements were obtained (tricipital, suprailiac, subscapular, and abdominal) using a LangueTM caliper (Beta Technology, Inc., Santa Cruz, CA, United States) by a professional, and the same evaluator made the measurements in both the pre- and posttest stages following the standard protocols (Marfell-Jones et al., 2006). The percent (%) fat mass and % muscle mass were assessed by bioimpedance using a digital scale (Omron HBF-INTTM, Omron Healthcare, Inc., Lake Forest, IL, United States). This procedure was conducted without metal or watches on the body to increase precision, and the average of three measurements was used.
Ambulatory SBP and DBP were measured using an automatic monitor (OmronTM HEM 7114TM, Omron Healthcare, Inc., Lake Forest, IL, United States) in triplicate (2-min interval between measurements) with subjects in a seated position after they had rested for 15 min. The average data were recorded for each participant based on standard classification procedures (Mancia et al., 2013). Heart rate at rest was measured using a monitor (ProTrainer 5TM, Polar Electro Inc., Kempele, Finland) after at least 15 min of rest.
Strength performance was assessed 1 week before and after the intervention using the one-repetition maximum leg extension (1RMLE) test, which was implemented according to similar procedures previously described (Álvarez et al., 2017). The 1RMLE was performed using an exercise machine (OXFORDTM, model EE4002, Santiago, Chile) in the morning between 9 and 11 o’clock. The highest load of three attempts was reported as an average value.
On the third day, after 2 days of familiarization, the endurance performance test was conducted. The test involved a 2-km walking test (2KMWT) (Álvarez et al., 2017) in an indoor sports court (100-m track) after a 10-min warm-up of walking at low intensity and performing slow movements involving the knee and ankle joints. The subjects were instructed to walk as fast as possible with a steady pace and were warned not to run. Heart rate was continuously monitored (ProTrainer 5TM, Polar Electro Inc., Kempele, Finland) during the test. To ensure an accurate test, participants were encouraged to walk faster if their heart rate was lower than 70% of the maximum heart rate based on age. The time spent on the 2KMWT and the average heart rate during the 2KMWT were registered and used for the analysis.
Blood samples (4 ml) were collected before and after the 16-week follow-up in the morning and after a 10-h overnight fast. Posttraining blood sampling of the subjects was performed at least 48 h after the last exercise session to avoid any acute effects of exercise. The samples were placed on ice and centrifuged at 4000 rpm for 5 min at 4°C. Plasma samples were immediately transferred to prechilled microtubes and stored at −20°C for subsequent analysis. Plasma glucose was analyzed by enzymatic methods using standard kits (Wiener Lab, Inc., Rosario, Argentina) and an automatic analyzer (Metrolab 2300 PlusTM, Metrolab Biomed, Inc., Buenos Aires, Argentina). TC, HDL-C and TG were analyzed using an enzymatic calorimetric method (Diagnostica mbH, Alemania). LDL-C was calculated using the Friedewald equation (Friedewald et al., 1972).
Data are presented as the mean ± standard deviation (SD). Normality and homoscedasticity assumptions for all data were checked using the Shapiro-Wilk and Levene tests. Wilcoxon’s test was used for non-parametric data. Student’s t-test was performed to test for differences between groups at baseline and for each delta between groups. In addition, the non-parametric Wilcoxon test was applied for variables with non-normal distribution (TC and 2KMWT). To reduce within-group variability, a univariate test (ANCOVA) was performed for SBP and DBP as main variables using anthropometric covariables. Repeated-measures ANOVA was used to make comparisons based on group and time. After the intervention, delta values (Δ) were calculated in each dependent variable. Subjects were categorized as Rs and NRs according to the previously mentioned criteria (Hopkins, 2000). Bonferroni post hoc test was applied to determine the differences between groups. To test for differences between the prevalence of NRs in the PreHTN group and NTG, the Chi-Square test (X2) was used for categorical variables. The odds ratios (ORs) of NRs to HIIT were applied for both NR variables between groups, with an OR ≥2 indicating a high risk of being an NR. Finally, five different models (Model 1, based on only SBP at baseline; Model 2, based on SBP at baseline plus body composition changes; Model 3, based on SBP at baseline plus body composition and cardiovascular changes; Model 4, based on SBP at baseline plus body composition, cardiovascular, and metabolic changes; and Model 5, based on SBP at baseline plus body composition, cardiovascular, metabolic, and performance changes) were applied in order to predict the SBP changes. All statistical analyses were performed with SPSS software version 18 (SPSSTM Inc., Chicago, IL, United States). The alpha level was fixed at P < 0.05 for all tests of statistical significance.
As expected based on the study design, there were significant differences in SBP (128 ± 6 vs. 108 ± 5 mmHg, P = 0.003) and DBP (85 ± 8 vs. 75 ± 10 mmHg, P = 0.007) at baseline between the PreHTN group and NTG (Table 1). There were no baseline differences in the other dependent anthropometric, cardiovascular, metabolic and performance covariables between groups (Table 1).
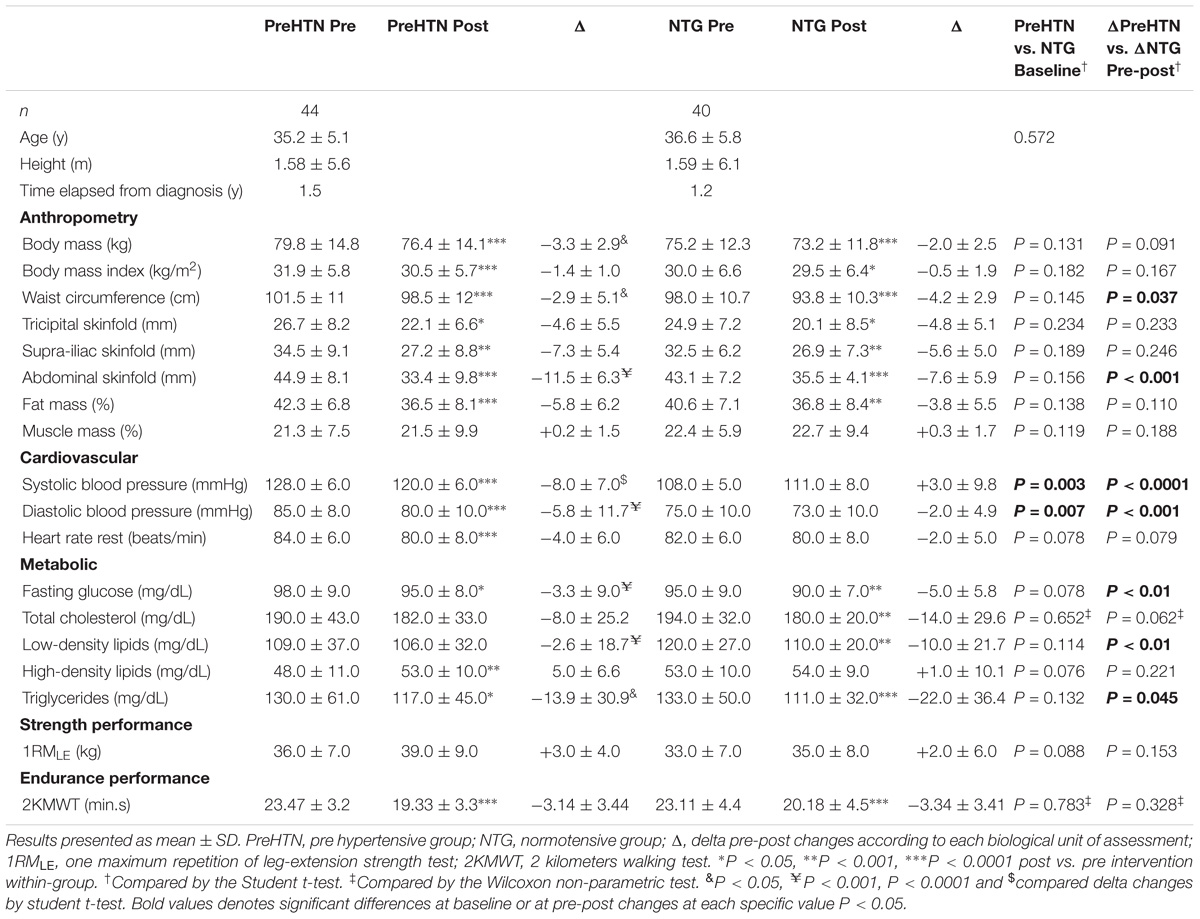
TABLE 1. Characteristics of the sample before and after the 16-weeks follow-up.
After training, in the PreHTN group, there was a significant decrease in body mass (Δ −3.3 kg, P < 0.0001), BMI (Δ −1.4 kg/m2, P < 0.0001), and waist circumference (Δ −2.9 cm, P < 0.0001); the NTG also showed similar decreases in body mass (Δ −2.0 kg, P < 0.0001), BMI (Δ −0.5 kg/m2, P < 0.05), and waist circumference (Δ −4.2 cm, P < 0.0001). Significant differences in waist circumference (Δ −1.3 cm, P = 0.037) were observed between groups (Table 1). Subcutaneous skinfold measurements, including tricipital (Δ −4.6 mm, P < 0.05 and Δ −4.8 mm, P < 0.05), suprailiac (Δ −7.3 mm, P < 0.001 and Δ −5.6 mm, P < 0.001), and abdominal (Δ −11.5 mm, P < 0.0001 and Δ −7.6 mm, P < 0.0001) skinfold measurements, were similarly decreased in the PreHTN group and NTG. Significant differences between groups were detected only in abdominal skinfold thickness (Δ −3.9 mm, P < 0.001) (Table 1). The % fat mass was reduced in both the PreHTN group and NTG (Δ −5.8%, P < 0.0001; and Δ −3.8%, P < 0.001) (Table 1). The % muscle mass was not different between groups (Table 1).
SBP was significantly decreased in the PreHTN group (Δ −8 mmHg, P < 0.0001) (Table 1); in contrast, the NTG showed no changes in SBP (Table 1). There was a significant difference between groups in the change in SBP (Δ −8 vs. + 3.0 mmHg, P < 0.003) (Table 1). DBP was significantly decreased in the PreHTN group (Δ −5.8 mmHg, P < 0.0001) compared to the NTG, and there was a significant difference in the change in DBP (−5.8 vs. −2.0 mmHg, P = 0.007) between groups (Table 1). A significant reduction in heart rate at rest was detected in the PreHTN group (Δ −4 beats/min, P < 0.0001) but not in the NTG (Table 1).
Fasting glucose was significantly decreased in both the PreHTN group and NTG (Δ −3.3 mg/dL, P < 0.05 and Δ −5 mg/dL, P < 0.001), with significant differences between groups (Δ 1.7 mg/dL, P < 0.01) (Table 1). TC and LDL-C were significantly decreased in the NTG (Δ −14 mg/dL and Δ −10 mg/dL, P < 0.001) (Table 1). There were significant differences in the changes in LDL-C (Δ + 7.4 mg/dL P = 0.01) between groups (Table 1). HDL-C was significantly increased (Δ + 5.0 mg/dL, P < 0.001) in the PreHTN group, while the NTG showed no significant changes in HDL-C (Table 1). TG levels were significantly reduced in both the PreHTN group and NTG (Δ −13.9 mg/dL, P < 0.05 and Δ −22 mg/dL, P < 0.0001), with significant differences between groups (Δ 8.1 mg/dL, P = 0.045) (Table 1).
There were no changes in the 1RMLE strength test in either group (Table 1). However, there were significant improvements in endurance performance, with decreases in the time spent on the 2KMWT in both the PreHTN group and NTG (Δ −3.14 min and Δ −3.34 min, P < 0.0001) (Table 1).
There were significant differences in the prevalence of NRs in the PreHTN group vs. the NTG based on the following variables: BMI (13.6 vs. 40.0%, P = 0.006), abdominal skinfold (6.8 vs. 15.0%, P < 0.0001), LDL-C (72.7 vs. 50.0%, P = 0.032), HDL-C (56.8 vs. 77.5%, P = 0.045), and TG (70.5 vs. 35.0%, P < 0.001) (Table 2). The risk (based on OR: 95% CI) of no response was high (≥2-fold) in the PreHTN group for LDL-C (OR 2.6: 1.0 to 6.6) and TG (OR 4.4: 1.7 to 11) (Table 2).
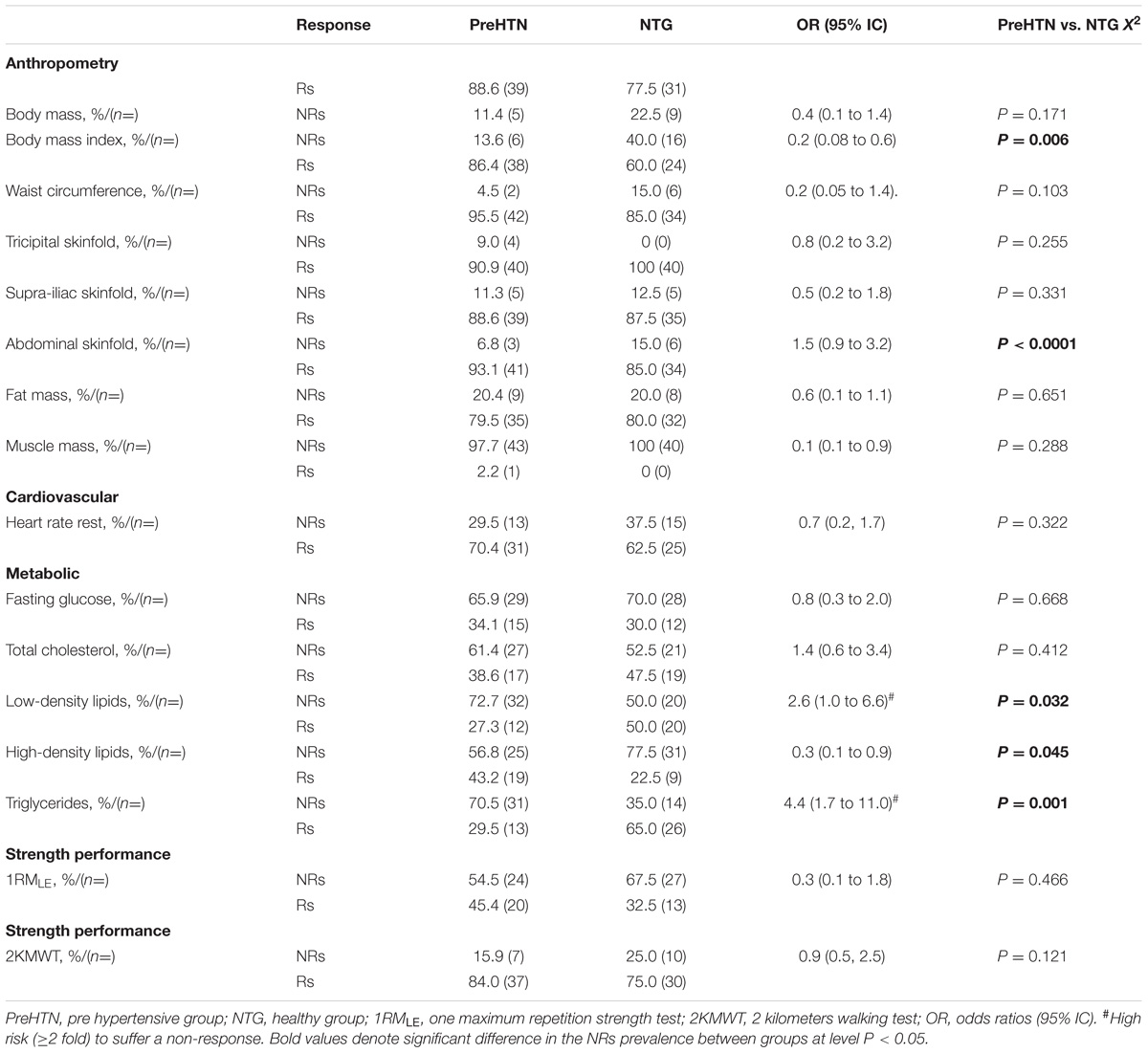
TABLE 2. Prevalence of non-responders by health status (i.e., prehypertensive and normotensive subjects) after intervention.
Figure 3A shows the delta values for individual changes in SBP (ΔSBP in mmHg) in the PreHTN group, in which the prevalence of NRs was 54.5% (24 patients). Figure 3B shows the delta values for individual changes (ΔSBP in mmHg) in the NTG, in which the prevalence of NRs was 92.5% (37 patients). There was a significant difference in the prevalence of NRs based on SBP between the PreHTN group and NTG (54.5 vs. 92.5%, P < 0.0001) (Figures 3A,B).
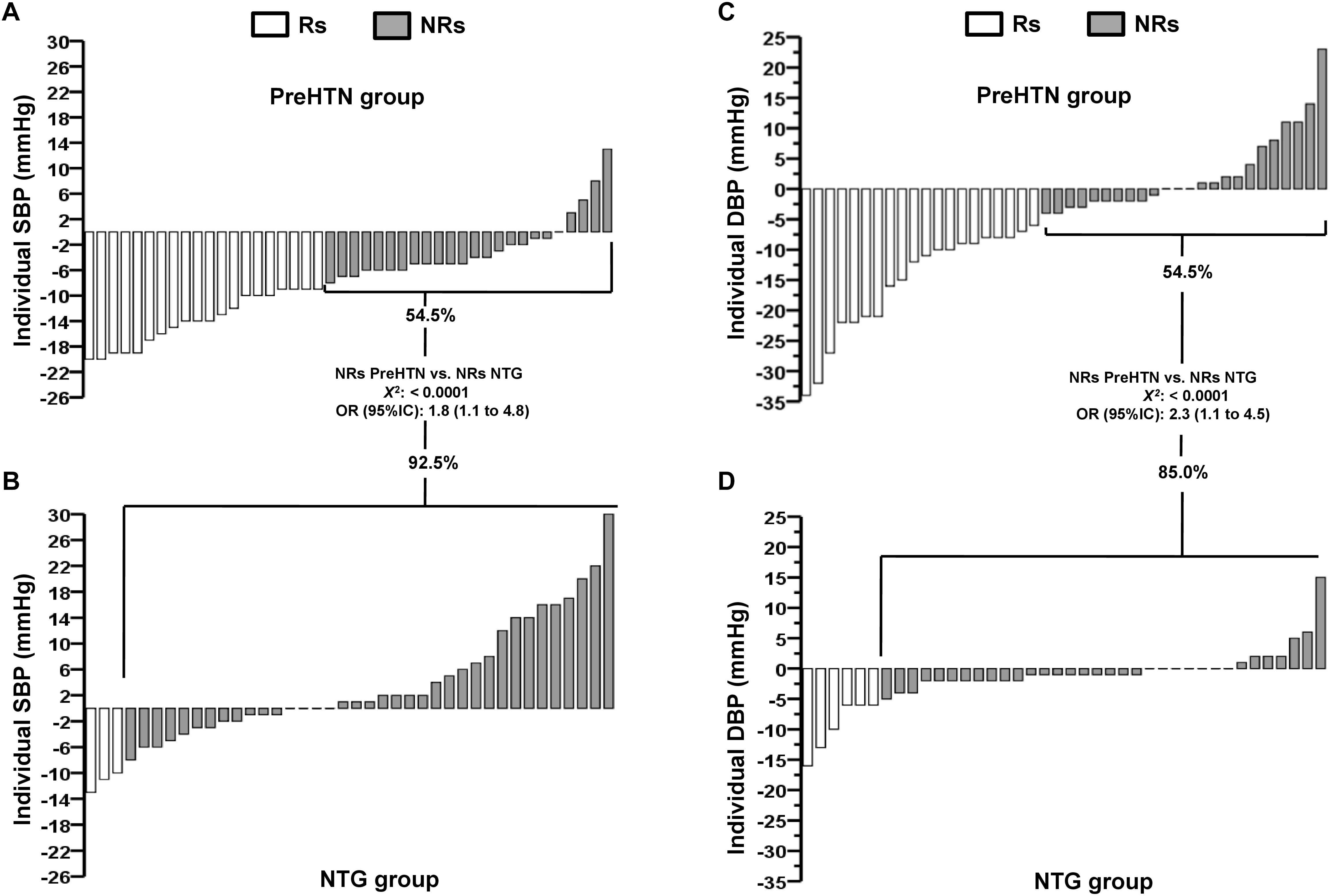
FIGURE 3. Individual changes for systolic blood pressure in (A) prehypertensive and (B) normotensive, and individual changes for diastolic blood pressure in (C) prehypertensive and (D) normotensive subjects after 16-weeks of HIIT. PreHTN, prehypertensive group; NTG, normotensive subjects; SBP, systolic blood pressure; DBP, diastolic blood pressure; Rs, responders; NRs, non-responders; OR, odds ratios.
Figure 3C shows the delta of individual changes in DBP (ΔDBP in mmHg) in the PreHTN group, in which the prevalence of NRs was 54.5% (24 patients). Figure 3D shows the delta of individual changes in DBP (ΔDBP in mmHg) in the NTG, in which the prevalence of NRs was 85.0% (34 patients). There was a significant difference in the prevalence of NRs based on DBP between the PreHTN group and NTG (54.5 vs. 85.0%, P < 0.0001) (Figures 3A,D).
Table 3 shows the five models used to predict a response in SBP, where model 3 (based on baseline SBP + body composition and cardiovascular measurements), model 2 (based on baseline SBP + body composition measurements), and model 1 (based on only baseline SBP), which we named previously as ‘health status,’ could explain, respectively, 53.8, 52.3, and 51.2% of the total variance in SBP changes after training. Model 5, in which performance variables were added, explained a significant 25.5% of the total variance in SBP changes (Table 3).
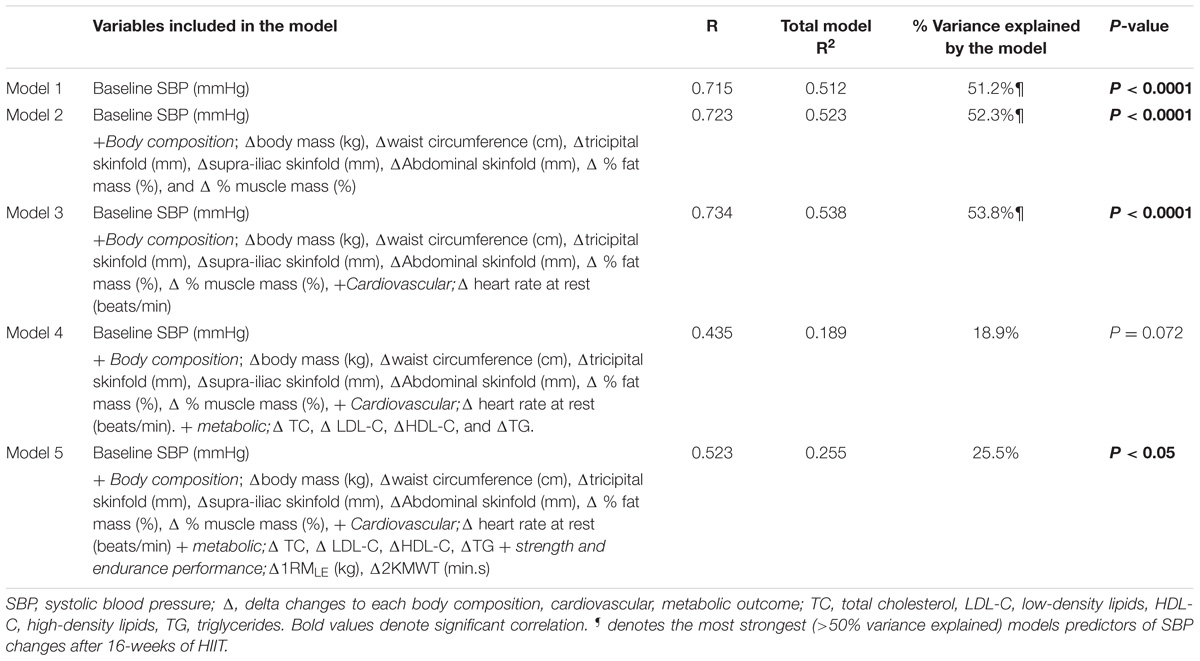
TABLE 3. Percentage of total variance explained by 5 models of factors predictive SBP decreases.
This study has two main findings: (i) the prevalence of NRs based on SBP, DBP, and other comorbidities is different between groups; and (ii) between the 5 tested models (from the most basic to the most complex) for BP reduction, baseline SBP alone (model 1), referred to as ‘BP-health status’ by us, is the simplest model with similar (e.g., model 2; 52.3%, model 3; 53.8%, both P < 0.0001) efficacy for predicting Rs with a predictive capacity in SBP (51.2%) after 16 weeks of HIIT, when compared with other more complex models that included added outcomes. Decreases in SBP were accompanied by other known effects of exercise, but not in both cohorts. Accordingly, HIIT decreased both SBP (Δ −8 mmHg) and DBP (Δ −5.8 mmHg) only in prehypertensive subjects, whereas improvements in anthropometric/body composition, metabolic and endurance performance were observed in both groups.
Contrary to our hypothesis, the prevalence of NRs between prehypertensive and normotensive subjects after HIIT was different, whereas changes in anthropometric, metabolic, and endurance performance were almost similar. However, there is little evidence at present regarding the prevalence of NRs in terms of changes in SBP/DBP after HIIT (Higgins et al., 2015; Alvarez et al., 2017). Including other training methods, such as endurance or resistance training (Bouchard et al., 2012; Moker et al., 2014), would help confirm which training modality is more appropriate for decreasing BP with fewer NRs. For example, in ∼1600 subjects after 20 weeks of endurance training (30–50 min/session, 3 days/week, 55–75% of the maximum oxygen uptake), 12.2% of subjects were considered NRs based on decreased SBP (Bouchard et al., 2012). After 6 months of endurance (65–80% peak of oxygen uptake, walking/jogging), resistance (8–12 repetitions, 8 exercises, 70–85% of one-maximum repetition, 3 days/week) or combined training, ∼60.9% of subjects were NRs based on decreased SBP and ∼59.1% of subjects were NRs based on decreased DBP (Moker et al., 2014). Furthermore, 6 weeks of HIIT in adults (3 × 1 min maximum intensity with 2 min recovery, 3 days/week) resulted in ∼61.5% NRs in terms of decreased DBP (Higgins et al., 2015). We found that among prehypertensive subjects, 11.4% were NRs for decreased SBP and 31.8% were NRs for decreased DBP. By contrast, the prevalence of NRs based on decreased SBP and DBP in the NT group was greater at 68.8 and 35.0%, respectively. Additionally, among 23 healthy adults who underwent 6 weeks of HIIT (Higgins et al., 2015) a wide interindividual variability was reported, in which Rs showed a decrease in SBP of ∼10 mmHg, and NRs showed an increase in SBP of 10 mmHg.
Interestingly, in terms of BP effects, 30 min of moderate-intensity exercise/day in combination with resistance training for a cumulative 150 min/week decreased BP by 5–7 mmHg in individuals with HTN (Pescatello et al., 2015). Here we report that 16 weeks of HIIT at a low volume of exercise/week (∼21–30 min/week) is able to decrease BP (SBP −8 mmHg and DBP −5.8 mmHg) in a prehypertensive cohort to similar values as for endurance or resistance training, but with less time investment. The evidence supporting endurance exercise for normalizing BP is not novel (Cade et al., 1984); however, to the best of our knowledge, the evidence for HIIT in decreasing BP has been little explored at all in prehypertensive or hypertensive populations. After 12 weeks of HIIT and endurance training, HIIT decreased the average 24-h ambulatory SBP of hypertensive subjects by 12 mmHg, whereas endurance training decreased it by only 4.5 mmHg (Molmen-Hansen et al., 2012). Similarly, the ambulatory 24-h DBP was decreased by 8 mmHg after HIIT and by 3.5 mmHg after endurance training, leading the authors to conclude that the decrease in BP among patients with HTN is intensity-dependent. In another study, after 16 weeks of HIIT, SBP and DBP were decreased in hypertensive patients by 6 and 4 mmHg, respectively, but these measures were not markedly changed in normotensive patients, with decreases of ∼1 mmHg for both variables (Guimaraes et al., 2010), which is similar to our findings. Moreover, after 12 weeks of HIIT in healthy men, SBP decreased by 18 mmHg (Nybo et al., 2010). Thus, it is not surprising that short HIIT programs (Whyte et al., 2010) lasting only 2 weeks showed decreases in SBP of 6 mmHg and in DBP of 9 mmHg among prehypertensive individuals. The mechanisms by which HIIT leads to decreases in BP have not been fully elucidated, but it has been reported that a combination of factors could be involved, including increasing shear stress, decreasing sympathetic nervous activity, reducing vascular peripheral resistance, and increasing nitric oxide-mediated vasodilatation (Halliwill, 2001). In our study, although the BP increases at the individual level were high in both groups, they were higher in the NT group than in the PreHTN group (Figure 2). A report from an epidemiological study has shown increases in SBP of ∼10 mmHg as an adverse response to exercise (Bouchard et al., 2012). Here, we report, using an experimental approach, increases in SBP by ∼30 to 15 mmHg in the normotensive group and by 14 to 20 mmHg in the HTN group, indicating the relevance of reporting data not only as the ‘mean,’ but also at the interindividual level using a typical sample size (∼20–40 subjects) for experimental studies.
In our study, other anthropometric/body composition effects from HIIT included body mass decreases (−3.3 and −2.0 kg), BMI (−1.4 and −0.5% kg/m2), tricipital (−4.6 and −4.8 mm), and suprailiac (−7.3 and −5.6 mm) skinfold thickness, and fat mass (−5.8 and −3.8%), which were similar in both the prehypertensive and hypertensive groups. Other authors have reported similar results after 2 weeks of HIIT (Whyte et al., 2010; Boutcher, 2011), and these findings were corroborated with molecular changes after HIIT (Little et al., 2011). For example, in the study of Whyte et al. (2010), 6 sessions of 30 s of ‘all out’ exercise were shown to decrease body mass by 1 kg and waist circumference by 2.4 cm. In our previous study using 16 weeks of HIIT, we found a 1.6 kg decrease in body mass, 4.1 cm decrease in waist circumference, and ∼20% decrease in subcutaneous fat in patients with type 2 diabetes (T2DM) (Alvarez et al., 2016). Other authors, however, have not observed decreases in body mass after 12 months of HIIT in adolescents (Tjønna et al., 2009). Additionally, in the present study, for some variables we found significant differences between groups in the magnitude of change, including waist circumference (∼1 cm, P = 0.037) and abdominal skinfolds (∼4 mm, P < 0.0001). We presume that these effects would be in addition to a similar general effect of HIIT. Fat mass, for example, was decreased similarly between groups; thus, we speculate that the same specific (not measured) molecular mechanisms accrued as a result of the HIIT protocol, and that any small differences in the magnitude of changes between groups may have been influenced by the anthropometric and/or the BP differences between groups at baseline (pre-HIIT). The weight loss, and other fat markers such as waist circumference and subcutaneous skinfold thickness, as well as postexercise adrenergic mechanisms, are relatively well known and described (Boutcher, 2011).
Fasting glucose was decreased after HIIT in both groups, with a more pronounced decrease in the NT group (∼5 mg/dL) over the PreHTN group (∼3.3 mg/dL). Our previous study reported that 16 weeks of HIIT resulted in a decrease in fasting glucose of ∼15% in T2DM patients (Alvarez et al., 2016), showing more pronounced benefits in the same time period than in our present non-diabetic sample. However, we also reported in this study that there were decreases in TG in both groups, as well as TC and LDL-C in the NT group, and increases in HDL-C in the prehypertensive cohort. Interestingly, TC, LDL-C, and TG were decreased by a greater magnitude in the NT group than in the PreHTN group. The additional metabolic benefits of HIIT, including improving dyslipidemia, alongside the benefits on BP are considered relevant for decreasing/preventing comorbidities in prehypertensive populations. Reduced risk of HTN in populations with dyslipidemia is related to higher physical activity levels than the minimal recommended activity level in current guidelines (Williams and Franklin, 2015). In the present study, the HIIT program had a weekly time commitment of ∼60 to ∼90 min divided into three exercise sessions (∼21–30 min/session), which was lower than the minimum 150 min/week of activity recommended in current guidelines (O’Donovan et al., 2010). For example, in T2DM patients, decreases of 2.1/0.9 mmHg in BP reduced the risk of major cardiovascular events by 10% (Turnbull et al., 2005), whereas the risk of developing coronary artery disease was reduced by 2–3% for each 1 mg/dL increase in HDL-C (Maron, 2000). Thus, the 8 mmHg reduction in systolic BP and the ∼5 mg/dL increase in HDL-C observed in prehypertensive women in the present study may have clinical implications. The mechanisms by which HIIT decreases plasmatic lipoprotein levels are unclear, but we presume that a decrease in the intramyocellular fat in the liver could play a role (Heijden et al., 2010).
A similar 16-week HIIT program was shown to improve endurance performance, similarly decreasing the time needed to complete the 2KMWT in T2DM patients by 2 min (Alvarez et al., 2016). There is strong evidence that HIIT increases endurance performance (Gibala et al., 2012), which is corroborated by the findings in our prehypertensive cohort. Twelve weeks of HIIT have been reported to increase the maximum oxygen uptake ∼13%, similar/or more than traditional endurance training of ∼7%, with this outcome considered as a performance marker frequently related with health and disease (Nybo et al., 2010).
Multiple regressions analyses of baseline SBP (model 1) and baseline SBP associated with one (anthropometric, model 2), two (cardiovascular, model 3), three (metabolic, model 4), and four (performance, model 5) additional parameters showed that baseline SBP (model 1) explained a similar percentage of variance (51.2%) to that of the more complex models tested (model 2: 52.3%; model 3: 53.8%; and model 5: 25.5%). Thus, our findings confirm that baseline measurements can be useful for predicting responses to HIIT. More recently, the ‘magnitude’ of the hypotensive effect has been reported as a predictive factor for decreasing BP after chronic exercise (Hecksteden et al., 2013b). Unfortunately, the authors referred to 4 weeks of training as ‘chronic’ exercise, and these results are limited to the specific endurance protocol used, showing the importance of effects, the prevalence of NRs, and predictive factors of a response to long-term HIIT.
The strengths of the present study include our data on the effects, prevalence of NRs and predictive factors for decreasing BP in prehypertensive subjects. One limitation was the lack of a true no-exercise control group. Another limitation was that we used BIA to assess body composition variables; however, BIA is not considered the ‘gold standard’ method. We also did not implement dietary control during the intervention. Nonetheless, we continually reminded subjects to maintain their baseline dietary habits. Finally, as heart rate at rest, fasting glucose, HDL-C, and 1RMLE were almost significantly different at baseline, the significant differences in each group pre- and post-intervention (Table 1) must be interpreted with caution.
In conclusion, the prevalence of NRs based on SBP and DBP was different between prehypertensive and normotensive subjects after 16 weeks of HIIT. Other comorbidities such as body composition and metabolic outcomes showed almost similar modifications between prehypertensive and normotensive subjects, being the most basic predictive factor for BP reduction baseline SBP, which we refer to as ‘BP health status’ (51.2%). This improvement in BP was accompanied by other known improvements of HIIT on body composition, metabolic, and endurance performance in both study cohorts.
Although both prehypertensive and normotensive groups showed improvements in fat markers, metabolic risk factors (fasting glucose, lipid profile), and endurance performance, and thus a decrease in comorbidities, there was a different prevalence of non-responders based on decreased systolic and diastolic BP among prehypertensive individuals compared to normotensive individuals.
To normalize high blood pressure and improve lipid profiles, an appropriate type of exercise training must be chosen. In addition, other non-pharmacological strategies are required to prevent hypertension.
Among participants in a prehypertensive state, altered blood pressure alone (health status) is a powerful predictive factor for the normalization of blood pressure, an increase in endurance performance and improvements in other metabolic risk factors after exercise.
The datasets during and/or analyzed during the current study available from the corresponding author on reasonable request.
Prior to providing written informed consent, the clinical records of all participants were reviewed to ensure that they met all of the inclusion criteria. Additionally, all subjects were personally informed about the study procedures that would occur before, during and after the intervention. All procedures were approved by the local Ethics Committee of the Family Healthcare Center Tomás Rojas in the city of Los Lagos, Chile.
CÁ and RR-V conceived and designed the project. CÁ and RR-C reviewed the literature studies and conducted the data extraction. CÁ conducted the data analyses. CÁ, RR-C, and MI were responsible for the data interpretation. CÁ, RRC, and CC-M drafted the manuscript. RR-V and MI revised it critically for the intellectual contributions. CÁ and RR-C coordinated the study development. All authors reviewed, edited, read, and approved the final manuscript.
The present research project was funded by grants from the Family Healthcare Center Tomás Rojas and with public funding from the Health Service of Los Ríos by the Health promotion program of the 2014. MI was funded by research grants RD12/043/0002 [Spanish Net on Aging and frailty; (RETICEF)] (ISCIII and fondos FEDER), PI17/01814 and CIBER de Fragilidad y Envejecimiento Saludable (CIBERFES).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This study was carried out with participants from the Family Healthcare Center Tomás Rojas, of Los Lagos, Chile. We thank all the patients for their commitment with the program, as well as to Mr. Farid Sade, physician, and to Miss Paulina Carrasco from the Family Healthcare Center Tomás Rojas for the recruitment of patients. The results of the study are presented clearly, honestly, without fabrication, falsification, or inappropriate data manipulation.
1RMLE, one-maximum repetition test of leg extension; 2KMWT, 2 kilometer walking test; BMI, body mass index; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein; HIIT, high-intensity interval training; LDL-C, low-density lipoproteins; NRs, non-responders; NTG, normotensive group; OR, odds ratios; PreHTN, prehypertensive group; Rs, responders; SBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides.
Alvarez, C., Ramirez-Campillo, R., Martinez-Salazar, C., Mancilla, R., Flores-Opazo, M., Cano-Montoya, J., et al. (2016). Low-volume high-intensity interval training as a therapy for type 2 diabetes. Int. J. Sports Med. 37, 723–729. doi: 10.1055/s-0042-104935
Alvarez, C., Ramirez-Campillo, R., Ramírez-Velez, R., and Izquierdo, M. (2017). Prevalence of non-responders in glucose control markers after 10-weeks of high-intensity interval training in higher and lower insulin resistant adult women. Front. Physiol. 8:479. doi: 10.3389/fphys.2017.00479
Álvarez, C., Ramírez-Campillo, R., Ramírez-Vélez, R., and Izquierdo, M. (2017). Effects and prevalence of nonresponders after 12 weeks of high-intensity interval or resistance training in women with insulin resistance: a randomized trial. J. Appl. Physiol. 122, 985–996. doi: 10.1152/japplphysiol.01037.2016
Bonafiglia, J. T., Rotundo, M. P., Whittall, J. P., Scribbans, T. D., Graham, R. B., and Gurd, B. J. (2016). Inter-individual variability in the adaptive responses to endurance and sprint interval training: a randomized crossover study. PLoS One 11:e0167790. doi: 10.1371/journal.pone.0167790
Bouchard, C., Blair, S. N., Church, T. S., Earnest, C. P., Hagberg, J. M., Häkkinen, K., et al. (2012). Adverse metabolic response to regular exercise: is it a rare or common occurrence? PLoS One 7:e37887. doi: 10.1371/journal.pone.0037887
Bouchard, C., and Rankinen, T. (2001). Individual differences in response to regular physical activity. Med. Sci. Sports Exerc. 33, S446–S451. doi: 10.1097/00005768-200106001-00013
Boutcher, S. H. (2011). High-intensity intermittent exercise and fat loss. J. Obes. 2011:868305. doi: 10.1155/2011/868305
Cade, R., Mars, D., Wagemaker, H., Zauner, C., Packer, D., Privette, M., et al. (1984). Effect of aerobic exercise training on patients with systemic arterial hypertension. Am. J. Med. 77, 785–790. doi: 10.1016/0002-9343(84)90513-8
Díaz-Martínez, X., Steell, L., Martinez, M. A., Leiva, A. M., Salas-Bravo, C., Labraña, A. M., et al. (2017). Higher levels of self-reported sitting time is associated with higher risk of type 2 diabetes independent of physical activity in Chile. J. Public Health doi: 10.1093/pubmed/fdx091 [Epub ahead of print].
Friedewald, W. T., Levy, R. I., and Fredrickson, D. S. (1972). Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 18, 499–502.
Gibala, M. J., Little, J. P., Macdonald, M. J., and Hawley, J. A. (2012). Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 590, 1077–1084. doi: 10.1113/jphysiol.2011.224725
Guimaraes, G. V., Ciolac, E. G., Carvalho, V. O., D’avila, V. M., Bortolotto, L. A., and Bocchi, E. A. (2010). Effects of continuous vs. interval exercise training on blood pressure and arterial stiffness in treated hypertension. Hypertens. Res. 33, 627–632. doi: 10.1038/hr.2010.42
Halliwill, J. R. (2001). Mechanisms and clinical implications of post-exercise hypotension in humans. Exerc. Sport Sci. Rev. 29, 65–70.
Hawley, J. A. (2009). Molecular responses to strength and endurance training: are they incompatible? Appl. Physiol. Nutr. Metab. 34, 355–361. doi: 10.1139/H09-023
Hecksteden, A., Grütters, T., and Meyer, T. (2013a). Associations between acute and chronic effects of exercise on indicators of metabolic health: a pilot training trial. PLoS One 8:e81181. doi: 10.1371/journal.pone.0081181
Hecksteden, A., Grütters, T., and Meyer, T. (2013b). Association between postexercise hypotension and long-term training-induced blood pressure reduction: a pilot study. Clin. J. Sport Med. 23, 58–63. doi: 10.1097/JSM.0b013e31825b6974
Heijden, G. J., Wang, Z. J., Chu, Z. D., Sauer, P. J., Haymond, M. W., Rodriguez, L. M., et al. (2010). A 12-week aerobic exercise program reduces hepatic fat accumulation and insulin resistance in obese, hispanic adolescents. Obesity 18, 384–390. doi: 10.1038/oby.2009.274
Higgins, T. P., Baker, M. D., Evans, S.-A., Adams, R. A., and Cobbold, C. (2015). Heterogeneous responses of personalised high intensity interval training on type 2 diabetes mellitus and cardiovascular disease risk in young healthy adults. Clin. Hemorheol. Microcirc. 59, 365–377. doi: 10.3233/CH-141857
Hopkins, W. G. (2000). Measures of reliability in sports medicine and science. Sports Med. 30, 1–15. doi: 10.2165/00007256-200030010-00001
Jebb, S., Siervo, M., Murgatroyd, P., Evans, S., Frühbeck, G., and Prentice, A. (2007). Validity of the leg-to-leg bioimpedance to estimate changes in body fat during weight loss and regain in overweight women: a comparison with multi-compartment models. Int. J. Obes. 31, 756–762. doi: 10.1038/sj.ijo.0803475
Karoline de Morais, P., Sales, M. M., Alves De Almeida, J., Motta-Santos, D., Victor De Sousa, C., and Simões, H. G. (2015). Effects of aerobic exercise intensity on 24-h ambulatory blood pressure in individuals with type 2 diabetes and prehypertension. J. Phys. Ther. Sci. 27, 51–56. doi: 10.1589/jpts.27.51
Lim, S. S., Vos, T., Flaxman, A. D., Danaei, G., Shibuya, K., Adair-Rohani, H., et al. (2012). A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet 380, 2224–2260. doi: 10.1016/S0140-6736(12)61766-8
Little, J. P., Gillen, J. B., Percival, M. E., Safdar, A., Tarnopolsky, M. A., Punthakee, Z., et al. (2011). Low-volume high-intensity interval training reduces hyperglycemia and increases muscle mitochondrial capacity in patients with type 2 diabetes. J. Appl. Physiol. 111, 1554–1560. doi: 10.1152/japplphysiol.00921.2011
Mancia, G., Fagard, R., Narkiewicz, K., Redon, J., Zanchetti, A., Böhm, M., et al. (2013). 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC). Blood Press. 22, 193–278. doi: 10.3109/08037051.2013.812549
Mann, T. N., Lamberts, R. P., and Lambert, M. I. (2014). High responders and low responders: factors associated with individual variation in response to standardized training. Sports Med. 44, 1113–1124. doi: 10.1007/s40279-014-0197-3
Marfell-Jones, M., Olds, T., and Stewart, A. And Carter, L. (2006). International Standards for Anthropometric Assessment. Potchefstroom: The International Society for the Advancement of Kinanthropometry (ISAK).
Maron, D. J. (2000). The epidemiology of low levels of high-density lipoprotein cholesterol in patients with and without coronary artery disease. Am. J. Cardiol. 86, 11–14. doi: 10.1016/S0002-9149(00)01462-4
Moker, E. A., Bateman, L. A., Kraus, W. E., and Pescatello, L. S. (2014). The relationship between the blood pressure responses to exercise following training and detraining periods. PLoS One 9:e105755. doi: 10.1371/journal.pone.0105755
Molmen-Hansen, H. E., Stolen, T., Tjonna, A. E., Aamot, I. L., Ekeberg, I. S., Tyldum, G. A., et al. (2012). Aerobic interval training reduces blood pressure and improves myocardial function in hypertensive patients. Eur. J. Prev. Cardiol. 19, 151–160. doi: 10.1177/1741826711400512
Montero, D., Roche, E., and Martinez-Rodriguez, A. (2014). The impact of aerobic exercise training on arterial stiffness in pre-and hypertensive subjects: a systematic review and meta-analysis. Int. J. Cardiol. 173, 361–368. doi: 10.1016/j.ijcard.2014.03.072
Nybo, L., Sundstrup, E., Jakobsen, M. D., Mohr, M., Hornstrup, T., Simonsen, L., et al. (2010). High-intensity training versus traditional exercise interventions for promoting health. Med. Sci. Sports Exerc. 42, 1951–1958. doi: 10.1249/MSS.0b013e3181d99203
O’Donovan, G., Blazevich, A. J., Boreham, C., Cooper, A. R., Crank, H., Ekelund, U., et al. (2010). The abc of physical activity for health: a consensus statement from the British association of sport and exercise sciences. J. Sports Sci. 28, 573–591. doi: 10.1080/02640411003671212
Park, S., Rink, L. D., and Wallace, J. P. (2006). Accumulation of physical activity leads to a greater blood pressure reduction than a single continuous session, in prehypertension. J. Hypertens. 24, 1761–1770.NODOI doi: 10.1097/01.hjh.0000242400.37967.54
Pescatello, L. S., Macdonald, H. V., Lamberti, L., and Johnson, B. T. (2015). Exercise for hypertension: a prescription update integrating existing recommendations with emerging research. Curr. Hypertens. Rep. 17:87. doi: 10.1007/s11906-015-0600-y
Russo, A., Di Gaetano, C., Cugliari, G., and Matullo, G. (2018). Advances in the genetics of hypertension: the effect of rare variants. Int. J. Mol. Sci. 19:E688. doi: 10.3390/ijms19030688
Seron, P., Munoz, S., and Lanas, F. (2010). Levels of physical activity in an urban population from temuco, chile. Rev. Med. Chil. 138, 1232–1239.
Shrout, T., Rudy, D. W., and Piascik, M. T. (2017). Hypertension update, JNC8 and beyond. Curr. Opin. Pharmacol. 33, 41–46. doi: 10.1016/j.coph.2017.03.004
Tjønna, A. E., Lee, S. J., Rognmo, Ø., Stølen, T. O., Bye, A., Haram, P. M., et al. (2008). Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome. Circulation 118, 346–354. doi: 10.1161/CIRCULATIONAHA.108.772822
Tjønna, A. E., Stølen, T. O., Bye, A., Volden, M., Slørdahl, S. A., Odegård, R., et al. (2009). Aerobic interval training reduces cardiovascular risk factors more than a multitreatment approach in overweight adolescents. Clin. Sci. 116, 317–326. doi: 10.1042/CS20080249
Trost, S. G., Owen, N., Bauman, A. E., Sallis, J. F., and Brown, W. (2002). Correlates of adults’ participation in physical activity: review and update. Med. Sci. Sports Exerc. 34, 1996–2001. doi: 10.1097/00005768-200212000-00020
Turnbull, F., Neal, B., Algert, C., Chalmers, J., Chapman, N., Cutler, J., et al. (2005). Effects of different blood pressure-lowering regimens on major cardiovascular events in individuals with and without diabetes mellitus: results of prospectively designed overviews of randomized trials. Arch. Intern. Med. 14, 1410–1419.
Whyte, L. J., Gill, J. M. R., and Cathcart, A. J. (2010). Effect of 2 weeks of sprint interval training on health-related outcomes in sedentary overweight/obese men. Metabolism 59, 1421–1428. doi: 10.1016/j.metabol.2010.01.002
Williams, P. T., and Franklin, B. A. (2015). Incident diabetes mellitus, hypertension, and cardiovascular disease risk in exercising hypercholesterolemic patients. Am. J. Cardiol. 116, 1516–1520. doi: 10.1016/j.amjcard.2015.08.011
Keywords: high-intensity interval training, prehypertension, responders, non-responders, women, risk factors, systolic blood pressure
Citation: Álvarez C, Ramírez-Campillo R, Cristi-Montero C, Ramírez-Vélez R and Izquierdo M (2018) Prevalence of Non-responders for Blood Pressure and Cardiometabolic Risk Factors Among Prehypertensive Women After Long-Term High-Intensity Interval Training. Front. Physiol. 9:1443. doi: 10.3389/fphys.2018.01443
Received: 03 January 2018; Accepted: 21 September 2018;
Published: 23 October 2018.
Edited by:
Billy Sperlich, Universität Würzburg, GermanyReviewed by:
David Andrew Low, Liverpool John Moores University, United KingdomCopyright © 2018 Álvarez, Ramírez-Campillo, Cristi-Montero, Ramírez-Vélez and Izquierdo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mikel Izquierdo, bWlrZWwuaXpxdWllcmRvQGdtYWlsLmNvbQ==
†All authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.