 Beat Knechtle
Beat Knechtle Pantelis T. Nikolaidis
Pantelis T. Nikolaidis
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Physiol., 01 June 2018
Sec. Exercise Physiology
Volume 9 - 2018 | https://doi.org/10.3389/fphys.2018.00634
In this overview, we summarize the findings of the literature with regards to physiology and pathophysiology of ultra-marathon running. The number of ultra-marathon races and the number of official finishers considerably increased in the last decades especially due to the increased number of female and age-group runners. A typical ultra-marathoner is male, married, well-educated, and ~45 years old. Female ultra-marathoners account for ~20% of the total number of finishers. Ultra-marathoners are older and have a larger weekly training volume, but run more slowly during training compared to marathoners. Previous experience (e.g., number of finishes in ultra-marathon races and personal best marathon time) is the most important predictor variable for a successful ultra-marathon performance followed by specific anthropometric (e.g., low body mass index, BMI, and low body fat) and training (e.g., high volume and running speed during training) characteristics. Women are slower than men, but the sex difference in performance decreased in recent years to ~10–20% depending upon the length of the ultra-marathon. The fastest ultra-marathon race times are generally achieved at the age of 35–45 years or older for both women and men, and the age of peak performance increases with increasing race distance or duration. An ultra-marathon leads to an energy deficit resulting in a reduction of both body fat and skeletal muscle mass. An ultra-marathon in combination with other risk factors, such as extreme weather conditions (either heat or cold) or the country where the race is held, can lead to exercise-associated hyponatremia. An ultra-marathon can also lead to changes in biomarkers indicating a pathological process in specific organs or organ systems such as skeletal muscles, heart, liver, kidney, immune and endocrine system. These changes are usually temporary, depending on intensity and duration of the performance, and usually normalize after the race. In longer ultra-marathons, ~50–60% of the participants experience musculoskeletal problems. The most common injuries in ultra-marathoners involve the lower limb, such as the ankle and the knee. An ultra-marathon can lead to an increase in creatine-kinase to values of 100,000–200,000 U/l depending upon the fitness level of the athlete and the length of the race. Furthermore, an ultra-marathon can lead to changes in the heart as shown by changes in cardiac biomarkers, electro- and echocardiography. Ultra-marathoners often suffer from digestive problems and gastrointestinal bleeding after an ultra-marathon is not uncommon. Liver enzymes can also considerably increase during an ultra-marathon. An ultra-marathon often leads to a temporary reduction in renal function. Ultra-marathoners often suffer from upper respiratory infections after an ultra-marathon. Considering the increased number of participants in ultra-marathons, the findings of the present review would have practical applications for a large number of sports scientists and sports medicine practitioners working in this field.
In recent years and decades, races longer than the classical marathon distance (42.195 km) have experienced a boom. With the increase in the number of races and finishers (Nikolaidis and Knechtle, 2018a), ultra-marathons—defined as any running distance longer than the marathon distance—became more and more interesting for scientific research.
The aim of this narrative review is to present the current state of knowledge on the topic of physiology and pathophysiology of ultra-marathon running. For this purpose, we have searched all scientific papers on ultra-marathon in Scopus (www.scopus.com) until March 2018. The keywords were “ultra-marathon” and “ultra marathon.” This search resulted in more than 700 articles. All articles were then sorted so that only studies (i.e., case reports and original papers) on running were taken into consideration. Studies investigating swimmers, cyclists, triathletes or other sports were excluded. Specifically, studies with a practical relevance for the athlete, the coach and the physician were considered.
An ultra-marathon is any running event where the running distance is longer than the traditional race length of a marathon of 42.195 km. The shortest ultra-marathon is the 50-km run (Figure 1). An ultra-marathon can also be defined as a running competition lasting 6 h in duration or longer (Zaryski and Smith, 2005). Ultra-marathons are performed as distance-limited runs held in km or miles or as time-limited events held in hours or days (www.ultramarathonrunning.com). The most frequently performed ultra-marathons held as a distance-limited events are 50-km, 100-km, 50-miles, and 100-miles ultra-marathons (www.ultra-marathon.org). In addition, there are a variety of races of different distances, with the longest ultra-marathons up to 1,000 km for races held in km and 3,100 miles for races held in miles (www.ultra-marathon.org). In time-limited ultra-marathons, runners are competing mainly during 6, 12, 24, 48, 72 h, 6 and 10 days (www.ultra-marathon.org). Ultra-marathon running also includes multi-stage races, such as crossing countries or even continents (www.ultra-marathon.org). The longest official ultra-marathon in the world, which takes place regularly, is the “Self-Transcendence 3,100 Mile Race” covering the total distance of 3,100 miles (4,989 km) (www.3100.ws).
Figure 1. A 50-km ultra-marathon is the shortest ultra-marathon. Figure by Céline Dewas.
An analysis of all 100-miles runners from 1977 to 2008 showed that both the number of races offered and the number of official finishers increased exponentially (Hoffman et al., 2010a). Surprisingly, running performance has not improved over all these years (Hoffman, 2010), which should be attributed to the increased number of finishers. That is, more “recreational” runners participate nowadays compared to fewer and more “competitive” runners in the past.
With regards to their socio-demographic characteristics of US ultra-marathoners in particular (Tokudome et al., 2004; Hoffman and Krishnan, 2013), 100-mile ultra-marathoners were ~44.5 years old, usually men (80.2%), mostly married (70.1%) (Hoffman et al., 2014) and had a bachelor (43.6%) or higher (37.2%) university degree (Hoffman and Fogard, 2012). Ultra-marathoners have a stable body weight during their lifetime and gain less body weight with increasing age (Hoffman and Fogard, 2012; Hoffman et al., 2014) compared to the general population. The reason is likely to be the low BMI at a younger age (Hoffman et al., 2014).
The average age at the first participation in an ultra-marathon was ~36 years and before the first start in an ultra-marathoners had an experience of ~7 years of competition in shorter distances (Hoffman and Krishnan, 2013). The average age did not change at the first start in an ultra-marathon in recent decades, the ultra-marathoners completed more than 3,000 km in the year before an important competition and the training kilometers correlated with the length of the longest ultra-marathon that they completed (Hoffman and Krishnan, 2013). Ultra-marathoners were healthier compared to the general population and less often absent at school or at work. Serious diseases such as cancer (~4.5%), coronary heart disease (~0.7%), strokes (~0.7%), diabetes (~0.7%), and HIV (~0.2%) were very rare in ultra-marathoners, who, on the other hand, had more allergies (~25.1%) and exercise-induced asthma (~13.0%) than the general population (Hoffman and Krishnan, 2014).
In general, ultra-marathoners are highly intrinsically motivated people (Kruger and Saayman, 2013) and have a very healthy lifestyle (Tokudome et al., 2004). Ultra-marathoners do not seem to be motivated by the competition as such, but rather by the adventure ultra-marathon (Doppelmayr and Molkenthin, 2004). For an ultra-marathoner, the following five aspects are central for a successful race: the preparation and the strategy, the management of the race, the discovery of the performance, the personal performance and the shared experience with the opponents (Simpson et al., 2014).
Although it is well-known that ultra-marathon running can lead to adverse aspects regarding health, a large part of ultra-marathoners would not stop if they learned it was bad for their health. These ultra-marathoners were younger and less likely to be married runners with less children and a lower health orientation but with high personal goal achievement, psychological coping, and life meaning scores (Hoffman and Krouse, 2018).
When we consider the the winner list of the “Self-Transcendence 3,100 Mile Race” (Table 1) and world records in ultra-marathon running of elite and age group runners (Tables 2–6), we inevitably notice that there are “endurance talents” or “exceptional runners” in ultra-marathon running. It is striking that the Greek Yiannis Kouros has a large number of world records over different distances and in different age groups. His list of victories in ultra-marathons and world records is almost endless (www.yianniskouros.gr/index.php/en/kourosvictories). He is considered as one of the best runners in the world and the best ultra-marathoner of all time.

Table 1. Winners in the “Self-Transcendence 3100 Mile Race” in New York, USA, since1997, from https://3100.srichinmoyraces.org/.

Table 2. World records in female elite and age group athletes in distance-limited races, from http://www.iau-ultramarathon.org/.
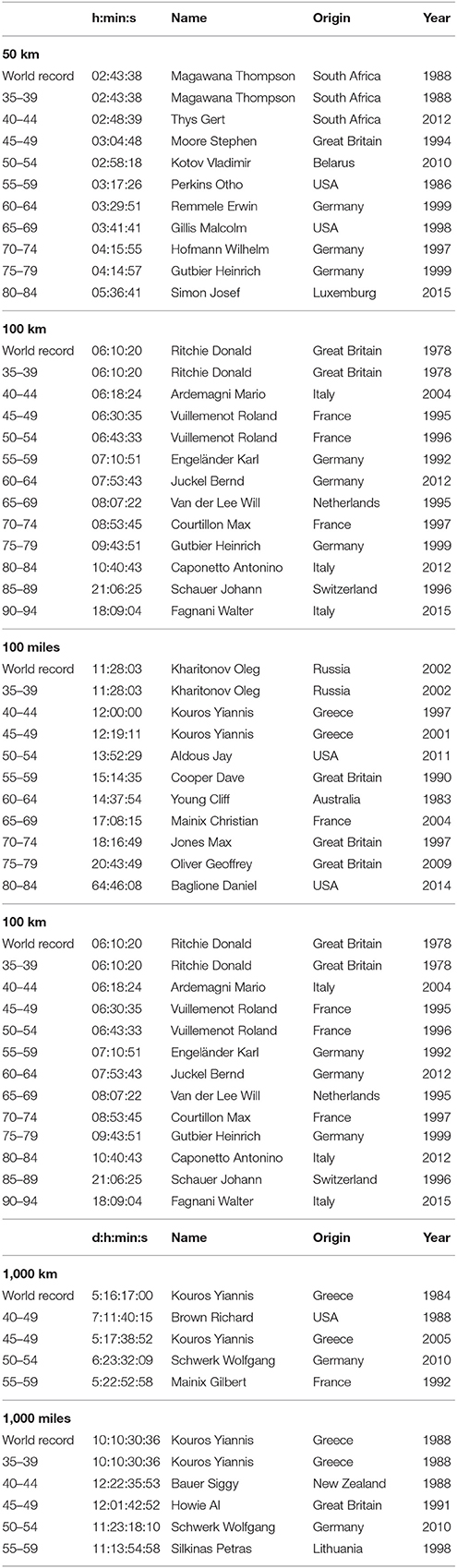
Table 3. World records in male elite and age group athletes in distance-limited races, from http://www.iau-ultramarathon.org/.

Table 4. World records in women in elite and age group athletes in time-limited races, from http://www.iau-ultramarathon.org/.
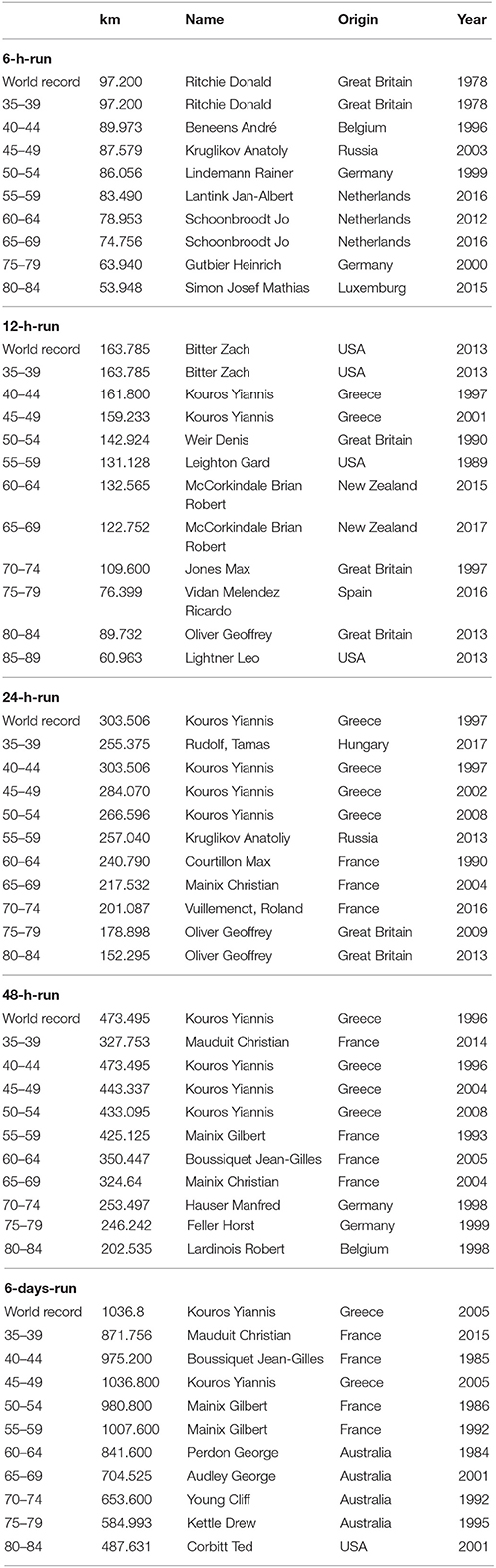
Table 5. World records in men in elite and age group athletes in time-limited races, from http://www.iau-ultramarathon.org/.
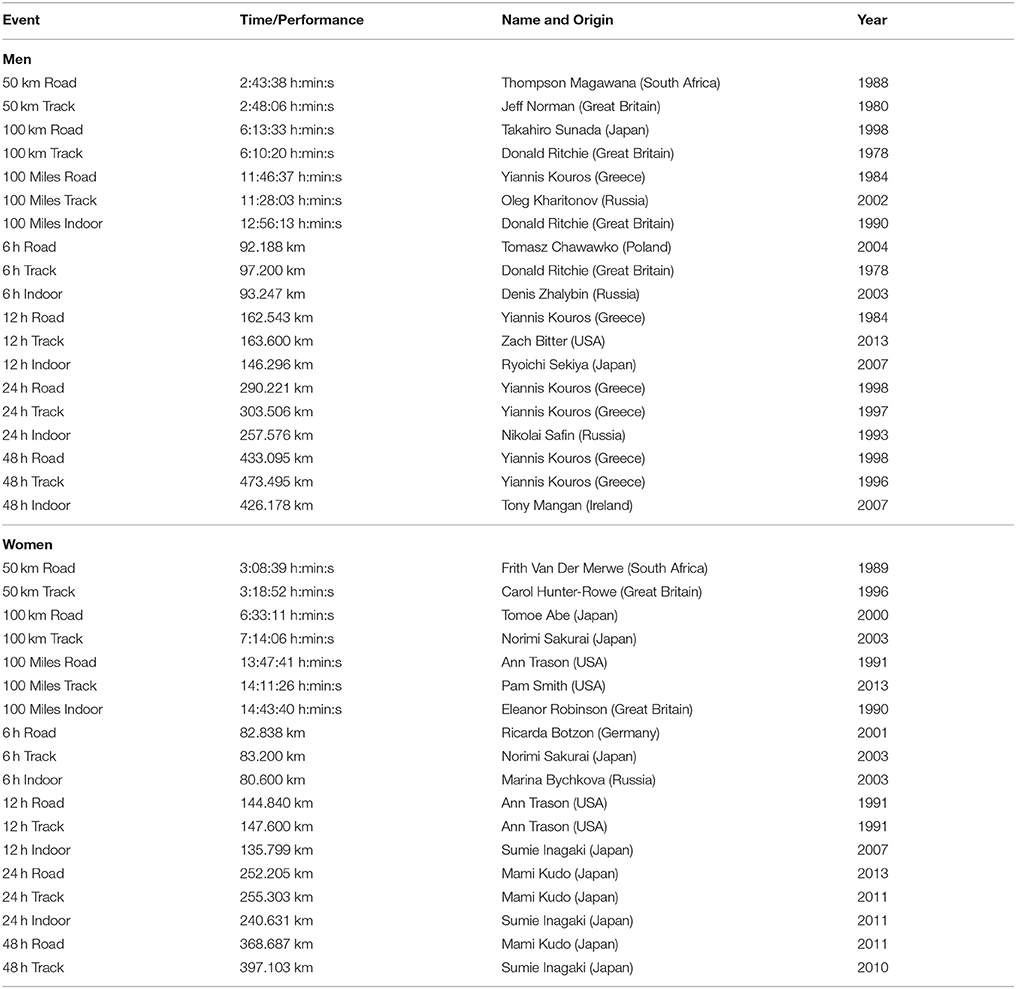
Table 6. World records in men and women in ultra-marathon running following IAU, from http://www.iau-ultramarathon.org/.
Generally, a long-distance runner competes for first time in an ultra-marathon after having completed several marathons. Most ultra-marathoners have run at least one marathon before the first start in an ultra-marathon and continue to participate in marathon races during their career as marathon runners (Knechtle, 2012).
Several studies compared training and anthropometric characteristics of marathoners and ultra-marathoners (Knechtle, 2012; Knechtle et al., 2012c; Rüst et al., 2012a,b) showing quite characteristic differences between the two groups of runners (Table 7). Ultra-marathoners have a higher number of successfully completed marathons than marathoners, whereas marathoners have a faster personal marathon race time than ultra-marathoners (Knechtle, 2012). Successful and experienced ultra-marathoners usually have several years of experience in ultra-marathon running (Knechtle, 2012).
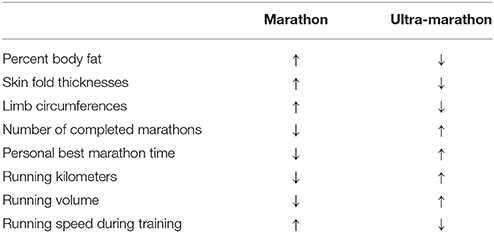
Table 7. Comparison between marathon and ultra-marathon runners regarding anthropometric and training characteristics.
There are also differences in anthropometric characteristics between marathoners and ultra-marathoners (Knechtle et al., 2012c). Generally, ultra-marathoners appear to be thinner than marathoners and have thinner skin folds. Marathoners have a significantly lower calf circumference than ultra-marathoners, but thicker skin folds on the upper body (Rüst et al., 2012b). Ultra-marathoners have a smaller circumference on the upper arms and thighs and thinner skin folds on the upper body than marathoners (Rüst et al., 2012a). Ultra-marathoners have thicker calves, but are thinner in the upper body than marathoners, probably due to adaptation due to the many training km and the many ultra-marathons.
Ultra-marathoners also show differences in training compared to marathoners. This is especially evident in the scope and intensity of running training. Ultra-marathoners run much slower in training than marathoners (Knechtle, 2012; Knechtle et al., 2012c), but complete more running kilometers and more running hours per week in training (Rüst et al., 2012b). One reason that ultra-marathoners train and compete longer distances than marathoners may be the fact that ultra-marathoners have a higher pain tolerance compared to other persons (Freund et al., 2013). Runners with increasing length in their race seem to invest more and more in training and are getting thinner and thinner.
Key predictors of a successful ultra-marathon finish were age (Knechtle et al., 2010b; Rüst et al., 2012b), specific aspects of anthropometry such as low body fat (Knechtle et al., 2012c), low BMI (Hoffman, 2008), and low limb circumferences (Knechtle et al., 2008b). Other aspects included fast personal best running times and extensive previous race experience (Knechtle et al., 2009, 2011d), and a high running speed and a high running volume during training (Knechtle et al., 2010a, 2012c; Rüst et al., 2012b).
Depending on the kind of the analysis (i.e., correlation of individual variables with running performance or inclusion of multiple variables in a regression model), results were different. For example, the thigh skinfold thickness as a highly predictive parameter for shorter running distance races (Arrese and Ostariz, 2006) is only significant in a single correlation for ultra-marathoners, but not in a multi-variate regression analysis involving multiple variables (Knechtle et al., 2009, 2011e). Analyzing the relationship between variables of anthropometric characteristics and race performance, the percentage of body fat and BMI appear to be the most important variables (Hoffman, 2008; Hoffman et al., 2010a). In 100-mile ultra-marathoners, a direct linear relationship between a low percentage of body fat and fast race times were found (Hoffman, 2008). In the same group of runners, faster ultra-marathoners and successful finishers had a lower body fat percentage than slower ultra-marathoners and non-finishers (Hoffman et al., 2010a).
When various anthropometric characteristics such as skeletal muscle mass, body fat and running training were examined in multi-variate analyses, only low body fat and fast running speed in training were correlated with fast race times (Knechtle et al., 2012c). In ultra-marathoners, weekly running kilometers and average running speed during training were negatively and the sum of the skin folds positively correlated with race times (Knechtle et al., 2010a).
Apart from aspects of anthropometry and training, age also seems to have a major impact on ultra-marathon performance. In 100-km ultra-marathoners, age, BMI and body fat were positively and the weekly running kilometers negatively correlated with race time (Rüst et al., 2012b). Low body fat and a fast running speed during training are the most important predictors for a fast ultra-marathon race time.
Besides these variables, experience seems to be the most important variable for a successful performance in an ultra-marathon (Knechtle et al., 2009, 2010a, 2011c). Ultra-marathoners need several years to reach their fastest running speed in a competition (Rae et al., 2005). The personal marathon best time was an important predictor variable for mountain ultra-marathoners (Knechtle et al., 2010a). In 24-h ultra-marathoners, aspects such as anthropometric characteristics and training running volume showed no correlation with race performance, and the personal marathon best time showed the highest impact on ultra-marathon race performance (Knechtle et al., 2009). To reach a maximum of km in a 24-h ultra-marathon, ultra-marathoners should have a personal best marathon time of 3:20 h:min and have completed a continuous training run of at least 60 km before the race, while anthropometric aspects such a low body fat or thin skin folds showed no relationship with race performance (Knechtle et al., 2011c). Therefore, apart from low body fat and fast running speed during training, previous experience such as a fast personal best marathon time seem to be the most important predictors for a fast ultra-marathon race time.
Other aspects were also investigated where cognitive functions should not be ignored. Faster ultra-marathoners seem to focus on the relevant, unlike slower ultra-marathoners (Cona et al., 2015). Also important are physiological variables such as maximal oxygen uptake (VO2max) (Davies and Thompson, 1979). In addition, faster runners experienced less pain in a 100-mile ultra-marathon, in the sense that these ultra-marathoners had a better exercise-induced analgesia (Hoffman et al., 2007). Another aspect is the pacing, or how ultra-marathoners distribute their energy across the race (Micklewright et al., 2015). In the 100-mile “Western States Endurance Run,” the winners initially ran behind the leaders during the race. In the middle of the race, they took over the lead themselves and the top ultra-marathoners were consistent over the entire race distance (Hoffman, 2014). In 24-h ultra-marathoners, the fastest runners start at lower relative intensities and display a more even pacing strategy than slower runners (Bossi et al., 2017). In 100-km ultra-marathon running, the strategy seems different. Fast 100-km ultra-marathoners tackle the race at a high pace, keeping the pace constant for a long time, and do not make any tempo changes (Lambert et al., 2004). Successful elite ultra-marathoners make little to no breaks during the race (Kerhervé et al., 2015) and often run in groups of runners of the same speed (Tan et al., 2016). Less experienced ultra-marathoners are advised to start at a rather low initial pace that they are most likely to endure during the full distance (Tan et al., 2016). Pacing has also been studied in a few studies for age group runners. It was shown the older runners during a 100-km ultra-marathon did not slow down as younger runners and that especially the young runners in the age group 18–24 years were slower than all other age group runners (Rüst et al., 2015). Taken together, pacing in an ultra-marathon is crucial to finish among the top.
There are also differences between finishers and non-finishers in strategy during the race. During an ultra-marathon many different problems occur, such as muscular spasms, overuse injuries, digestive problems, motivation problems and sleep deprivation (Hurdiel et al., 2015). Experienced ultra-marathoners also have less medical problems such as muscle cramps, digestive problems, etc. (Schwabe et al., 2014). Successful finishers tackle the competition in small stages, paying attention to running speed, nutrition, hydration and team support (Holt et al., 2014). A successful ultra-marathon finish is a good life experience while a non-finish is a big disappointment (Holt et al., 2014). Motivational self-talk seems to be an effective tool to cope with exertion, as well as other stressors such as blister discomfort and adverse conditions (McCormick et al., 2015).
The management of sleep deprivation seems to be central in long to very long ultra-marathons (Van Helder and Radoki, 1989). It has been shown in the “North-Face Ultra-Trail du Mont-Blanc” (UTMB) that ultra-marathoners who finished without sleep were faster than ultra-marathoners with sleep breaks. Runners who adopted a sleep management strategy based on increased sleep time before the race completed the race faster (Poussel et al., 2015).
The proportion of women in ultra-marathons was very low at the beginning of the ultra-running movement. In 100-mile ultra-marathons held in the United States, the proportion of women in the late 1970s increased from almost no participant to ~20% since 2004 (Hoffman et al., 2010b). This percentage has remained fairly stable at ~10–20% in recent years (Hoffman et al., 2010b; Eichenberger et al., 2012; Fonseca-Engelhardt et al., 2013). In most ultra-marathons, the proportion of women has increased in recent years such as in the “Badwater” to ~19.1% and in the “Spartathlon” to ~12.5% (Fonseca-Engelhardt et al., 2013), and in the “Swiss Alpine Marathon” held in Switzerland to ~16% (Eichenberger et al., 2012).
The rather low participation of women can have different reasons. One important reason is the different motivation of women toward men in ultra-marathon running. While female ultra-marathoners tend to be more intrinsically motivated (Krouse et al., 2011), less concerned with the competitive nature (Frick, 2011) and more attentive to health (Krouse et al., 2011), men have a competitive nature in which they want to compete with opponents and win a race (Doppelmayr and Molkenthin, 2004). Women also have a higher flow experience during an ultra-marathon than men (Wollseiffen et al., 2016).
An ealier assumption was that women become less tired than men during an ultra-marathon (Bam et al., 1997). Even though women run faster in exceptional cases than men, men are always faster than women in ultra-marathons (Coast et al., 2004; Eichenberger et al., 2012; Peter et al., 2014). Coast et al. (2004) compared the world's best performance for running distances from 100 m to 200 km, showing that men were on average ~12.4% faster than women.
It also known that the difference between the sexes increased with increasing race distance or race duration (Coast et al., 2004). An analysis of all 24-h ultra-marathons held worldwide between 1977 and 2012 showed that men were on average ~5% faster than women when all runners were considered (Peter et al., 2014). When the top 10 were evaluated, the difference was ~13%, for the top 100 the difference was on average ~12%, and when the fastest were taken per calendar year, the difference was again ~13% (Peter et al., 2014). Women seem to aim for a different running tactic than men in the ultra-marathon. In a 100-km ultra-marathon during the Masters World Championships, women were relatively slower than men at the start of the race, but at the end of the race they had a higher running speed than men (Renfree et al., 2016). However, in recent years women have been able to reduce the gap of men (Eichenberger et al., 2012; Rüst et al., 2013b; Peter et al., 2014). An analysis of 24 h ultra-marathoners showed that the gap fell to ~17% in the annual fastest, to ~11% for the annual 10 fastest, and to ~14% in the annual 100 fastest (Peter et al., 2014). An analysis of all 100-mile ultra-marathons in the world from 1998 to 2011 showed that women were able to close the gap to men to ~14% (Rüst et al., 2013b).
In recent decades, women have been able to reduce the gap to men, especially in the age group categories in which relatively many women were at the start (Knechtle et al., 2016b). The difference in performance between the sexes is influenced by several variables. Thus, the difference between the sexes is greatest when fewer women than men participate, especially on the shorter ultra-marathon distances (Senefeld et al., 2016). Considering the trend over different running distances in the last decades, it has been shown that over longer running distances such as 200 and 1,000 km the difference between the sexes remained the same. On the other hand, women approached to men over shorter running distances of 50 and 100 km. Since this trend is non-linear, it is absolutely unlikely that women will approach men in the near and far future even further and they will never beat the men (Zingg et al., 2014a). In rare cases, however, women may be able to beat all men in an ultra-marathon (www.runnersworld.com/trail-running-training/why-women-rule-ultrarunning). For example, the Japanese Hiroko Okiyama was able to beat all men in the “Germanyrun” 2007 (Knechtle et al., 2008a). Future studies need to investigate whether women were able to reduce the gap to men in older age groups.
The age of the best ultra-marathon performance has been analyzed in several studies in recent years (Eichenberger et al., 2012; Knechtle et al., 2012d; Fonseca-Engelhardt et al., 2013; Rüst et al., 2013b; Zingg et al., 2013b; Peter et al., 2014; Cejka et al., 2015; Nikolaidis and Knechtle, 2018b). In general, the best ultra-marathon performance is achieved at an older age than the best performance over half-marathon and marathon (Figure 2; Knechtle et al., 2012d, 2014b; Romer et al., 2014; Rüst et al., 2014; Zingg et al., 2014b; Nikolaidis and Knechtle, 2018a,b). The best marathon race time is achieved at the age of ~30 years, where performance level and nationality are important predictor variables of the age of peak performance (Hunter et al., 2011; Knechtle et al., 2014a, 2016a; Lara et al., 2014; Nikolaidis et al., 2016). In ultra-marathons, the age of best performance is often ~35 years or older (Knechtle et al., 2014b; Rüst et al., 2014; Knechtle and Nikolaidis, 2017; Nikolaidis and Knechtle, 2018a,b).
Figure 2. Ultra-marathoners are older than marathoners. Figure by Céline Dewas.
It seems that the age of peak ultra-marathon performance increases with increasing length of the race distance. In 50-km ultra-marathon running, the age of the best performance is at ~39–40 years (Nikolaidis and Knechtle, 2018a). In 100-km ultra-marathon running, the best race times are achieved at the age of 30–50 years for men and 30–55 years for women (Knechtle et al., 2012d). In 100-mile ultra-marathon running (161 km), the best race times were achieved at the age of 30–39 years for men and 40–49 years for women (Hoffman, 2010). The age of the best performance in ultra-marathons has increased in recent decades, with an increase especially in the long to very long ultra-marathons and in those runners who had finished many to very many ultra-marathons (Knechtle et al., 2014b). The older age of peak performance in the ultra-marathon comparted to marathon might be explained from the observation that ultra-marathon runners have finished many marathon races before finishing an ultra-marathon.
With regards to sex differences in the age of peak performance, women achieve their best ultra-marathon race time at the same age as men (Knechtle et al., 2012d; Rüst et al., 2013a; Zingg et al., 2013b; Peter et al., 2014; Cejka et al., 2015). In 100-km ultra-marathon running, the age of the fastest annual female and male finishers was ~35 years for both sexes (Cejka et al., 2015). In 24-h ultra-marathon running (Zingg et al., 2013b) as well as in “Badwater” and “Spartathlon” (Zingg et al., 2013a), the best performance was achieved for both sexes at the age of ~40 years.
Considering newer studies with more runners and longer time frames, there seems to be a difference in the age of peak performance between women and men depending upon the length of the performance. In 50-km ultra-marathons, women seemed to achieve the best race time later in life compared to men (Nikolaidis and Knechtle, 2018a). In 100-km ultra-marathons, however, the age of peak performance was younger in women than in men (Nikolaidis and Knechtle, 2018b). These disparate findings were most likely explained by the different ages of women and men competing in these race distances. Furthermore, the approach of the analysis seems of importance. When the fastest runners in the “Comrades Marathon” were considered in 1-year intervals, the fastest running speed was achieved in men at the age of 36.38 years. For the fastest women, the age of the fastest running speed was at the age of 32.75 years. When all runners were considered, men achieved the best ultramarathon performance ~6 years earlier than women, whereas when the fastest runners were considered, men achieved the best performance ~4 years later than women (Knechtle and Nikolaidis, 2017).
It seems that the age of peak performance on the long running distances increases with increasing distance and/or race duration (Rüst et al., 2013b; Peter et al., 2014). In 100-miles ultra-marathons, the age of the fastest men was at ~37 years and the fastest women at ~39 years (Rüst et al., 2013b). In 24-h ultra-marathoners who reached 200 km and more, the fastest men are ~44 years and the fastest women ~43 years old (Peter et al., 2014). Table 8 summarizes the age of best performance in the time-limited ultra-marathons of 6 h to 10 days (Knechtle et al., 2014b). While the youngest age of ~37 years was found in women over 10 days, the age of best performance in men increases with increasing duration. Thus, the age of ~35 years in 6 h and ~37 years in 12 h increases to ~48 years in 72 h, 6 and 10 days (Rüst et al., 2014). However, future studies need to confirm these findings in distance-limited ultra-marathons such as races held in kilometers from 50 to 1,000 km and races held in miles from 50 to 3,100 miles.

Table 8. Increase in age of peak performance with increasing duration in ultra-marathon running.
When investigating the age of the best ultra-marathon performance over the years, in some cases the age of the year's fastest finishers increased (Eichenberger et al., 2012; Rüst et al., 2013b; Peter et al., 2014) or decreased (Fonseca-Engelhardt et al., 2013) over time. For example, the age of the fastest men in the 24-h ultra-marathons rose from 23 years in 1977 to 53 years in 2012 (Peter et al., 2014). These disparate findings are most likely due to the different length or durations of the races and the different time frames.
In addition to elite ultra-marathoners, the number of age-group runners has increased and their performance has improved (Jampen et al., 2013; Rüst et al., 2013a). In the “Swiss Alpine Marathon,” the number of runners older than 30 years increased significantly and the performance of women in age group 40–44 years significantly improved (Rüst et al., 2013a). In the “Marathon des Sables,” the number of finishers older than 40 years increased and the performance of men in the age groups 35–39 and 40–44 years improved (Jampen et al., 2013). The trend is different for the different age categories. Considering the best 100-km and 100-mile ultra-marathoners, younger runners (i.e., 25–35 years old) and older runners (i.e., 50–65 years old) can still improve their performance in the next years and decades (Rüst et al., 2014). A possible explanation for the relatively old age of ultra-marathoners could be the fact that the mean age at the first start of an ultra-marathon is quite high. Hoffman and Krishnan (Hoffman and Krishnan, 2013) showed that the age at the start of the first ultra-marathon was ~36 years.
The homeostatic control of energy balance, i.e., the optimization of the relationship between energy intake and expenditure, is a major concern in ultra-marathon due to its large energetic demands. Two important problems regarding energy and fluid metabolism in ultra-marathon running are the energy deficit and a potential fluid overload leading to exercise-associated hyponatremia.
An ultra-marathon leads to a great energetic demand (Thompson et al., 1982; Stuempfle et al., 2011). In a 24-h ultra-marathon, runners were only able to maintain their running speed for the first 6 h, after which they slowed continuously down (Gimenez et al., 2013). It could be shown that a runner consumed about 6,300 kcal per day during his “Run around Australia” (Hill and Davies, 2001). In order to cover the energy consumption, the runners have to consume high amounts of energy during an ultra-marathon. Successful ultra-marathon finishers are more likely to consume and deliver the required energy during performance than non-finishers (Glace et al., 2002).
In general, ultra-marathoners are unable to meet their energy demands during a race by feeding them (Machefer et al., 2007; Enqvist et al., 2010) and in some cases a considerable energy deficit arises (O'Hara et al., 1977; Hill and Davies, 2001; Enqvist et al., 2010). The energy deficit, i.e., negative energy balance, is due to insufficient energy intake, most likely due to suppression of appetite and digestive problems during the race (Enqvist et al., 2010). The negative energy balance reduces the concentration of leptin in the serum after a long endurance performance (Landt et al., 1997). In turn, decreased levels of leptin might be a concern for overtrained endurance runners (Bobbert et al., 2012). The abovementioned studies focused on the quantification of energy balance rather than to identify the energy sources for a race.
Nevertheless, knowledge about the main energy sources for an ultramarathon race—not only in terms of calories, but also in terms of choice of carbohydrates, lipids and protein—is necessary in order to develop optimal nutritional strategies. Carbohydrates are generally the most important source of energy during an ultra-marathon (Eden and Abernethy, 1994; Case et al., 1995; Fallon et al., 1998). A total of 88.6% of the energy in 100-km ultra-marathon comes from the intake of carbohydrates, only 6.7% from the intake of fat and 4.7% from the intake of protein (Fallon et al., 1998). However, ultra-marathoners generally do not meet the required intake of carbohydrates (Martinez et al., 2017). However, carbohydrate intake—regardless of type or amount—can not delay glycogen breakdown during performance (Noakes et al., 1988). In addition, top runners are able to maintain a high running speed—independent of the energy supply—without a decrease on plasma glucose concentration during performance (Sengoku et al., 2015). For longer ultra-marathons, the proportion of fat and protein to energy contribution seems to increase. In ultra-marathoners in a race over 1,005 km in 9 days, the average daily intake of carbohydrates dropped to 62%, while the proportion of fat increased to 27% and of protein to 11% (Eden and Abernethy, 1994). A recent study showed that the intake of fat increased with increasing race distance (Martinez et al., 2017). Thus, it was observed that the ratio among carbohydrates, lipids and protein follows the current nutritional recommendations for marathon runners (Stellingwerff, 2013) with the contribution of carbohydrates and lipids decreasing and increasing, respectively, as the distance of ultramarathon increases.
The result of the energy deficit is a decrease in body mass (Belli et al., 2016), where both fat-free body mass (i.e., muscle mass) and fat mass are reduced (Knechtle et al., 2011g; Schütz et al., 2013). The use of fat as an energy substrate is shown by the increase in free fatty acids during an ultra-marathon (Pestell et al., 1993; Fallon et al., 1999a). Another problem of the energy deficit is the insufficient intake of vitamins (Holtzhausen and Noakes, 1995; Machefer et al., 2007) which is preferably seen in the pre-race preparation. Overall, ultra-marathoners in very long races without brakes will face an energy deficit with a decrease in solid mass. To date, there is no obvious solution to solve this problem.
During an ultra-marathon, all runners experience dehydration with a decrease in body mass (Holtzhausen and Noakes, 1995). The greatest body weight loss occurrs in the first hours of an ultra-marathon (Kao et al., 2008). Therefore, ultra-marathoners have to consume large amounts of fluids during a race to avoid dehydration in terms of body weight loss (Newmark et al., 1991).
However, consumption of large amounts of fluid can lead to dilutional hyponatremia or exercise-associated hyponatremia hyponatraemia (Barr and Costill, 1989; Eijsvogels et al., 2008; Bürge et al., 2011; Knechtle et al., 2012b; Chlibkova et al., 2014). The association between excessive water intake and exercise-associated hyponatraemia was first recognized in 1981 in a runner competing in the “Comrades Marathon” (Noakes, 2008). Symptomatic exercise-associated hyponatraemia is described not only in ultra-marathoners (Hew-Butler et al., 2007) but also in marathoners (Spormann et al., 2012; Wellershoff, 2013).
Exercise-associated hyponatremia is defined as a plasma sodium level of 135 mmol/l or lower (McGreal et al., 2016). Fluid overload can be seen not only from the change in electrolytes, but also from changes in plasma volume (De Paz et al., 1995; Costa et al., 2014), total albumin, and albumin (Fallon et al., 1999a).
In ultra-marathon running, there is no need to drink more fluid than required, or to over-drink (Knechtle et al., 2012e). Even if ultra-marathoners lose more than 3% of their body weight, there is no reason to over-drink to prevent overheating (Valentino et al., 2016). In an ultra-marathon, a runner of ~70 kg body mass must lose ~1.9–5.0% of body mass to maintain the water supporting body water balance while also avoiding overhydration (Hoffman et al., 2017b). A recent study showed that water intake decreased with increasing race distance (Martinez et al., 2017).
In general, ultra-marathoners do not seem to consume excessive fluid (Knechtle et al., 2011b) and an ultra-marathoner should not experience any fluid overload (Knechtle et al., 2011f). In a 100-km ultra-marathon, faster ultra-marathoners drank more liquid than slower ultra-marathoners and faster ultra-marathoners lost more body weight than slower ultra-marathoners. The weight loss was greater with less fluid intake (Knechtle et al., 2012e). Due to the fact that faster ultra-marathoners lost more body weight, the weight loss can be ergogenic and the ultra-marathoners achieve a faster race time due to their lower body weight (Knechtle et al., 2012e). In a 100-mile ultra-marathon, increased body weight losses did not lead to a limited performance but were rather performance-enhancing (Landman et al., 2012). In a 100-km ultra-marathon, runners with a greater body weight loss were faster (Rüst et al., 2012c).
Ultra-marathoners also seem to be able to self-regulate their plasma sodium during an ultra-marathon. In an ultra-marathon, the prevalence of exercise-associated hyponatremia was considerably higher during the race than after the race (Cairns and Hew-Butler, 2015). It has also been reported that ultra-marathoners with the highest fluid intake had the least hemodilution without changes in plasma sodium and potassium (Kaminsky and Paul, 1991). Often, exercise-associated hyponatremia is clinically not perceivable, in very few cases; however, it can lead to major medical problems. Thus, a case of a 57-year-old man who developed exercise-associated hyponatremia during a 100-mile ultra-marathon is described. Hyponatraemia resulted in rapid neurological deterioration and cardiovascular instability (Surgenor and Uphold, 1994).
Exercise-associated hyponatraemia is a relatively frequently detectable electrolyte disorder in ultra-marathoners (Noakes and Carter, 1982; Knechtle et al., 2011b; Hoffman et al., 2012b; Costa et al., 2013), whereby high ambient temperatures must be given a great importance (Lebus et al., 2010; Costa et al., 2013). The prevalence of exercise-associated hyponatremia in a 225-km ultra-marathon over five stages was ~42% with ambient temperatures as high as ~40°C (Costa et al., 2013). In the “Rio de Lago 100-Mile Endurance Run,” held in 2008 in Granite Bay, California, USA, the prevalence of exercise-associated hyponatraemia was ~51.2% (Lebus et al., 2010). However, in 100-mile ultra-marathoners, the prevalence of exercise-associated hyponatraemia may be as low as ~30% (Hoffman et al., 2012b). A great cold seems also to be a major risk factor for exercise-associated hyponatremia. In a 100-mile ultra-marathon held in Alaska, 44% of runners had exercise-associated hyponatraemia (Stuempfle et al., 2002).
In ultra-marathons held in temperate climates, exercise-associated hyponatraemia is relatively uncommon (Cuthill et al., 2009; Bürge et al., 2011; Knechtle et al., 2011c,f, 2012b). In ultra-marathons held in Switzerland, Europe, a low prevalence of exercise-associated hyponatraemia was found. In the “Swiss Jura Marathon,” a mountain ultra-marathon over 350 km in 7 stages at medium to low temperatures held in the Swiss Jura region from Geneva to Basel, the prevalence of exercise-associated hyponatraemia was ~8% (Knechtle et al., 2012b). In the “100 km Lauf Biel” (Bürge et al., 2011; Knechtle et al., 2011f) and at the “24 h Run Basel” at medium to low temperatures, no case of exercise-associated hyponatraemia could even be detected (Knechtle et al., 2010a).
Also, the country in which the ultra-marathons take place seems to be of importance. The prevalence of exercise-associated hyponatraemia in ultra-marathons held in the USA is higher than in ultra-marathons held in Europe. While the prevalence of exercise-associated hyponatremia was ~30% in the “Western States Endurance Run” held in California (Hoffman et al., 2012b), it was no more than ~8% in ultra-marathons held in Switzerland (Knechtle et al., 2010a, 2012b; Bürge et al., 2011). Even in ultra-marathons held in the Czech Republic, the prevalence of exercise-associated hyponatraemia was very low (Chlibkova et al., 2014) as was the case in Asia, where the prevalence of exercise-associated hyponatremia was only ~3% in an 84-km ultra-marathon (Lee et al., 2011). In Australia, no case of exercise-associated hyponatremia could be detected in an ultra-marathon (Reid and King, 2007). The USA may be a special case, since a lot of drinking is promoted there and body weight loss can lead to disqualification. For example, in the “Vermont's 100-mile” race, athletes are required to: “Runners may be asked to weigh in or undergo further evaluation” and “7% of pre-race weight wants to be allowed to continue.”
The prevalence of exercise-associated hyponatraemia increased in a multi-stage ultra-marathon with increasing number of stages. In a 250-km multi-stage ultra-marathon, the prevalence of exercise-associated hyponatraemia per stage was 1.6% (S1), 4.8% (S3), and 10.1% (S5) with a cumulative incidence of 14.8% (Krabak et al., 2017).
It has already been investigated whether exercise-associated hyponatraemia can be prevented by means of education, drinking behavior or sodium intake. However, such efforts can not influence the onset of exercise-associated hyponatraemia (Winger et al., 2013). Several studies investigated whether the intake of sodium during an ultra-marathon is important (Hoffman and Stuempfle, 2014, 2016b). Considering 100-mile ultra-marathoners in the USA, up to 100% of runners consume supplements with sodium (Hoffman and Stuempfle, 2014). The benefits of this intake, however, seem to be very limited. Studies of 100-mile ultra-marathoners showed that supplemental intake of sodium during a heat-run did not affect the runners' state of hydration (Hoffman and Stuempfle, 2014, 2016b).
Very recent investigation showed an association between CK-values and exercise-associated hyponatremia. One study compared runners with and without exercise-associated hyponatremia on the same 100-mile ultra-marathon. Runners with exercise-associated hyponatraemia had less experience over 100 miles and a higher CK. In addition, there was an inverse relationship between plasma sodium levels and CK after arrival. On the other hand, there were no differences in age, sex, weekly training kilometers, use of sodium supplements during exercise, body weight loss, frequency of water intake, ingestion of pain killers, and symptoms during the race (Hoffman et al., 2013a). Whether there is really a correlation between CK-values after an ultra-marathon and exercise-associated hyponatraemia is still uncertain (Hoffman et al., 2012a).
Excessive fluid overload, in addition to biochemically detectable hyponatraemia, can lead to hyponatremic encephalopathy and swelling of the hands and feet (Figure 3). Fluid overload can lead to exercise-associated hyponatremic encephalopathy with severe consquences (Frizzell et al., 1986). Several cases of long-distance runners with symptomatic exercise-associated hyponatraemia with altered behavior, seizures and edema are known (Bruso et al., 2010; Hoffman and Myers, 2015; Pearce et al., 2015). Excessive hydration during exercise also has negative effects on the volume of the feet. Recent studies have shown an association between fluid intake during an ultra-marathon and feet swelling during running (Bracher et al., 2012; Cejka et al., 2012). Recent work also pointed to an association between exercise-associated hyponatraemia and skeletal muscle damage. A 24-h ultra-marathon revealed that hyponatremia preceded the increase in CK (Cairns and Hew-Butler, 2016).
Figure 3. Fluid overload can result in exercise-associated hyponatremia, limb swelling and exercise-associated hyponatremic encephalopathy. Figure by Céline Dewas.
Surprisingly, however, hypernatremia is much more common than hyponatraemia. In 133 collapsed runners in the “Comrades Marathon,” ~45% of runners had hypernatremia, ~2% hyponatremia and ~53% normonatremia (Hew-Butler et al., 2007). However, another study on the “Comrades Marathon” found hyponatremia in ~9% of the collapsed runners (Noakes et al., 1990). It must be noted that collapsed runners do not always have an electrolyte imbalance. In most cases, runners collapse to the target line and have an electrolyte imbalance in only ~16% of the cases, as opposed to ~19% for non-collapsed runners (Holtzhausen et al., 1994).
Some of these ultra-marathons take place in difficult external conditions such as extreme heat (Knoth et al., 2012). A problem of the heat is the fact that the performance is partly considerably impaired (Parise and Hoffman, 2011; Wegelin and Hoffman, 2011). A run in the heat like “Badwater” in Death Valley in the USA inevitably leads to a rise in body core temperature. However, the increase is dependent on running speed, with a slight increase in the fastest runners (Brown and Connolly, 2015). In addition, running in the sun seems to significantly increase the risk of malignant skin tumors (Ambros-Rudolph et al., 2006).
A sufficient adaptation to the heat can be achieved with adequate acclimatization (Sandström et al., 2008; Costa et al., 2013). Four days of short term heat acclimation facilitates effective perceptual adaptations (Willmott et al., 2017). The adaptation to the heat can also be achieved by pauses during heat or tropical runs (Joslin et al., 2015). It is also important that an appropriate cooling is initiated immediately in case of suspected overheating or heat stroke (Rae et al., 2008). High heat can also lead to a nutritional problem. For example, a study on the “Marathon des Sables” showed that runners had major nutritional problems due to the dry mouth and inability to consume highly sugared energy gels and sports drinks when the products were heated due to the ambient heat (McCubbin et al., 2016). Finally, ultra-marathoners will not develop exercise-associated hyponatremia when they drink ad libitum with no fluid overload. Athletes must be aware that extreme weather conditions such as extreme heat and extreme cold might lead to fluid overconsumption.
Ultra-marathon running leads to selective damages in different tissues and organs. The most apparent problem is muscular pain. However, a negative effect can be found for the heart, the liver, the kidneys, the bone, the digestive tract and both the immune and the hormone system.
Training for an ultra-marathon and ultra-marathons per se usually result in a damage to the musculo-skeletal system (Khodaee et al., 2015; Scheer and Murray, 2015), with the extent of damage depending on the length of the ultra-marathon (Kim et al., 2009). The damage is generally only of minor importance (Vernillo et al., 2016) and beginners are more often affected than experienced ultra-marathoners (Videbæk et al., 2015). Running over long to very long distances can cause minor damages such as muscle soreness on the musculature, but can also lead to substantial problems in the joints and tendons (Fallon, 1996; Freund et al., 2012; Lopes et al., 2012). In longer ultra-marathons, ~50–60% of participants experience musculoskeletal problems (Hutson, 1984). However, it is also possible in rare cases to cross a continent without any injury (Lathan and Cantwell, 1981). Various studies using Magnetic Resonance Imaging (MRI) have shown damages such as fluid retention around tendons, tissue edema, and damage to cartilage (Theysohn et al., 2013). Such overuse injuries are the most common reason that ultra-marathoners have to interrupt training, while other reasons such as work or family never lead to a training interruption (Hoffman and Krishnan, 2013).
The most common injuries in ultra-marathoners involve the lower limb, such as the ankle and the knee (Fallon, 1996; Scheer and Murray, 2011; Hetsroni and Mann, 2012), and are manifested as Achilles tendon inflammation and femoropatellar syndrome (Lopes et al., 2012). When a knee is already damaged, a further ultra-marathon has a further negative effect on the joint (Hagemann et al., 2008). At the lower leg, shin splints (i.e., medial tibial stress syndrome) occur frequently. In the ankle, inflammation of the extensor tendons is common. The pattern of overuse injuries depends on the kind of running. While ankle problems are more likely to occur in trail running, knee problems are more common in road running (Bishop and Fallon, 1999).
The symptoms are often relatively small, even in longer multi-stage ultra-marathons (Fallon, 1996; Krabak et al., 2011). During a multi-stage ultra-marathon of 5 days and covering 219 km, ~22% of the runners had lower limb problems, mainly affecting the knee (Scheer and Murray, 2011). In an ultra-marathon of 1,005 km from Sydney to Melbourne, 32 runners experienced a total of 64 different problems, of which the knee (~31.3%) and the ankle (~28.1%) were the most frequently affected joints (Fallon, 1996). Achilles tendonitis, femoropatellar pain, and inflammation of extensor tendons in the foot were the most common problems in a 6-day ultra-marathon (Bishop and Fallon, 1999).
For very long ultra-marathons, such as crossing a continent, adaptations of lower limb tissues occur. An increase in the diameter of the Achilles tendon was demonstrated during the “Trans Europe Footrace,” a multi-stage ultra-marathon covering 4,487 km from Bari in Italy to the North Cape. This thickening of the tendon was interpreted as an adaptation to the stress of the ultra-marathon (Freund et al., 2012). However, intraosseous changes and subcutaneous edema were also detected. Changes of this kind occurred rather in those runners who had to stop the race early (Freund et al., 2012).
Blisters on the feet are also quite common in ultra-marathon running (Scheer et al., 2014). However, it has been shown that the development of blisters is dependent on the experience of the ultra-marathoner. With increasing experience in ultra-marathon running, there are fewer blisters on the feet (Scheer et al., 2014).
Despite all problems with overuse injuries in ultra-marmathon running, a long run also seems to have a favorable influence on the cartilage (Mündermann et al., 2017). Runners in the “Trans Europe Footrace” initially showed a damage of the ankle cartilage which could regenerate during the the race (Schütz et al., 2014). MR-findings showed that elevated T2-values recovered during the second half of the “Trans Europe Footrace” supported the evidence that this response is a physiological adaptive mechanism of chondrocyte function via upregulation of de novo synthesis of proteoglycans and collagen (Schütz et al., 2014). In addition to MR-findings, changes in the concentrations of cartilage biomarkers in the serum showed that articular cartilage is able to adapt during a multi-stage ultra-marathon such as the “Trans Europe Footrace” (Mündermann et al., 2017). Although overuse injuries of the lower limbs may be frequent, not all ultra-marathoners must suffer from this problem. Most likely very experienced and highly trained athletes have an advantage to prevent overuse injuries.
An ultra-marathon can lead to further pathophysiological changes. Several studies revealed very different changes in laboratory values, with much of these changes being due to direct organ damage. Even a relatively short running distance can lead to considerable changes in biomarkers where the intensity or duration of the performance is proportional to the change in a specific marker (Bird et al., 2014). In other words, the body responds to the stress of an ultra-marathon with an “acute-phase reaction” (Fallon et al., 1999b; Fallon, 2001).
An ultra-marathon can lead to changes in biomarkers indicating a pathological process in specific organs or organ systems such as skeletal muscles, liver, kidney, etc. (Noakes and Carter, 1982; Nagel et al., 1990; Wu et al., 2004; Kim et al., 2007; Bürge et al., 2011; Shin et al., 2012; Bird et al., 2014; Jastrzebski et al., 2016); Table 9. These changes are usually temporary, depending on both the intensity and the duration of the performance and usually normalize after the race (Bird et al., 2014) mainly with a few days (Kłapcinska et al., 2013). When biomarkers change during an ultra-marathon, these changes are transient and there are no long-term or deleterious consequences (Wu et al., 2004; Bird et al., 2014). The changes affect both younger and older runners alike, regardless of their running experience (Jastrzebski et al., 2016). However, there are also biomarkers which remain unchanged despite high levels of physical stress (Fallon et al., 1999a).
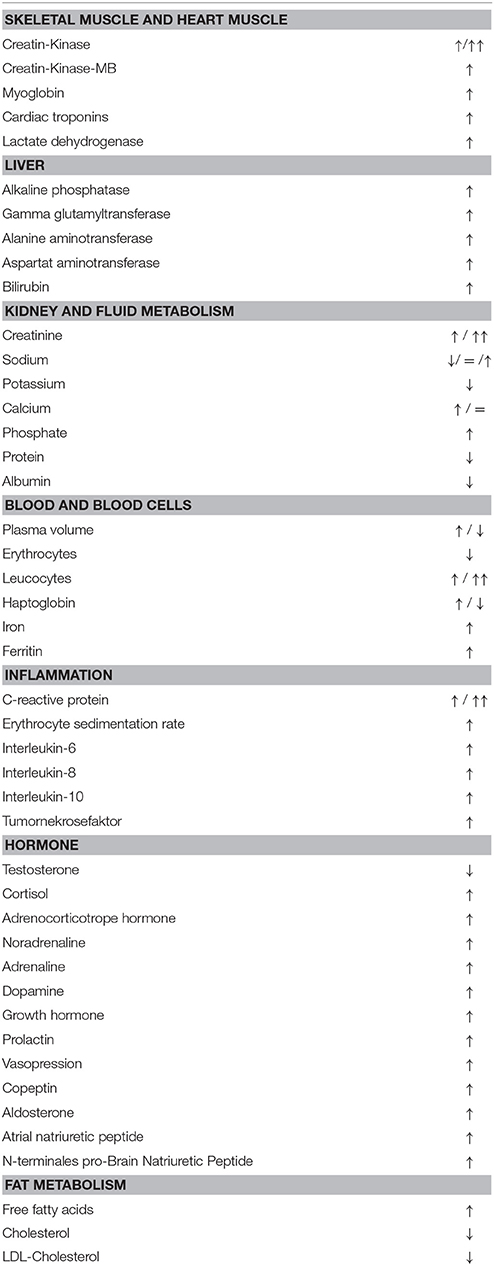
Table 9. Changes in metabolites and hormones during an ultra-marathon.
An ultra-marathon can lead to hemolysis (Chiu et al., 2015) and it is assumed that hemolysis leads to a significant loss of erythrocytes (Robach et al., 2014). Hematocrit has been shown to decrease after an ultra-marathon (Cejka et al., 2012) and haptoglobin increases (De Paz et al., 1995; Chiu et al., 2015). Haptoglobin does not always increase after an ultra-marathon, possibly the length of the race is crucial. At least, after a 60-km ultra-marathon (Lippi et al., 2012b) and a 24-h ultra-marathon (Liu et al., 2018), there was a decrease in haptoglobin. In a 166-km mountain ultra-marathon, it has been shown that “stress anemia” only occurs by causing anemia due to expansion of plasma volume (Fallon et al., 1999a) and not due to a reduction in the volume of erythrocytes (Robach et al., 2014). The extent of hemolysis can be significantly reduced by appropriate training (Casoni et al., 1985) and a corresponding diet with antioxidants (Aaseth and Birketvedt, 2012).
The phenomenon of hemolysis in runners and ultra-marathoners has been reported (Lippi et al., 2012b; Fazal et al., 2017). Repetitive forceful foot striking can lead to blood cell lysis in the feet, resulting in a mild macrocytic anemia and intravascular haemolysis (Fazal et al., 2017). The decrease of haptoglobin after an ultra-marathon reflects a certain degree of haemolysis, but since the changes in red blood cells is not relevant, the foot-strike haemolysis is very modest or even clinically negligible (Lippi et al., 2012b). Most probably there is no cellular damage to the red blood cells. A study with marathon and ultra-marathoners showed that hemoglobin, erythrocytes and erythrocyte indices did not change during the race (Banfi et al., 2004). In a 24-h ultra-marathon, red blood cells, hemoglobin, hematocrit, and mean cell hemoglobin decreased (Liu et al., 2018). Ultimately, the suspected anemia of the ultra-runner is just a “dilute anemia” (Dickson et al., 1982). The reticulocytes increase after a 6-day ultra-marathon (Fallon and Bishop, 2002), possibly as an indication that a longer ultra-marathon leads to some damage to the erythrocytes. As part of iron metabolism, ferritin increases (Liu et al., 2018) and transferrin saturation decreases (Kasprowicz et al., 2013). In the case of ferritin it could be shown that the value is increased due to the training and can remain elevated after an ultra-marathon up to 2 weeks (Dickson et al., 1982). Although hemolysis with a cellular damage of the red blood cells seems possible, it will not be of relevance. A decrease in hemoglobin is only due to plasma volume expansion.
During an ultra-marathon, some characteristic changes in specific hormones are evident (Pestell et al., 1989; Fournier et al., 1997), with the hypothalamic pituitary axis usually changing (Wittert et al., 1996; Table 9). An ultra-marathon leads to an increase in cortisol (Fournier et al., 1997), catecholamines (Pestell et al., 1993), and growth hormone (McKechnie et al., 1982) as well as a drop in testosterone (Fournier et al., 1997) where the decrease in testosterone is related with a decrease in libido (Longman et al., 2018).
The length of an ultra-marathon seems to have an influence on the change in hormones. In a run from Sydney to Melbourne over 1,000 km, an increase of norepinephrine, epinephrine, dopamine and adrenocorticotropic hormone was found. No changes were found for ß-endorphin, growth hormone, prolactin, testosterone, cortisol and cortisol-binding globulin. After the ultra-marathon, catecholamines increased and growth hormone, prolactin and cortisol increased (Pestell et al., 1989). Obvioulsy, the ultra-marathon leads to a chronic physical stress leading to an adjustment of stress hormones with a continuous increase (Pestell et al., 1989). The intensity is also crucial. Higher cortisol levels were found after an ultra-marathon when the athlete was competing at a high running speed (Tauler et al., 2014).
Since not only men but also more and more women run ultra-marathons, the changes of the female hormones were also investigated. There was a marked increase in estradiol after an ultra-marathon (Copeland and Verzosa, 2014). There is also a change in neurotransmitters, such as an increase in serotonin, a drop in tryptophan and an increase in ß-endorphins (Agawa et al., 2008; Table 9). In summary, male ultra-marathoners must be aware that increased levels of cortisol and suppressed levels of testosterone might become counterproductive.
The term “skeletal muscle damage” applied to ultramarathon refers to the race-induced muscle pain that results not from fatigue but from muscle injury (Damas et al., 2018). An ultra-marathon has a considerable influence on the skeletal muscles (Kim et al., 2007), with the down passages causing the greatest muscle damage during the run (Koller et al., 1998) where a run of 330 km with an elevation gain of 24,000 m leads to a measurable inflammatory reaction and swelling of the thigh musculature (Andonian et al., 2016). Accordingly, skeletal muscle damage consists in a major concern for ultramarathon runners.
Studies in ultramarathon have used several blood markers to evaluate skeletal muscle damage. Skeletal muscle damage is well visible on specific myocellular metabolites increasing in blood, such as myoglobin (Bird et al., 2014; Jastrzebski et al., 2016), lactate dehydrogenase (Noakes and Carter, 1982; Kanter et al., 1986; Chiu et al., 2013; Bird et al., 2014; Shin et al., 2014; Jastrzębski et al., 2015a,b), and creatine kinase (Kanter et al., 1986; Suzuki, 2002; Chiu et al., 2013; Jee et al., 2013; Bird et al., 2014; Carmona et al., 2015; Jastrzębski et al., 2015b).
The creatine kinase as a muscular enzyme is very suitable to document muscular damage due to an ultra-marathon. The eccentric load, such as in a mountain ultra-marathon, can lead to a significant increase in creatine kinase (Noakes et al., 1983; Frey et al., 1994) and pronounced muscle soreness (Figure 4). The highest activity of creatine kinase is measured about 1 h after the completion of an ultra-marathon (Carmona et al., 2015) but may still be highest at ~36–72 h after the race (Bird et al., 2014). The increase in creatine kinase after an ultra-marathon can sometimes be grotesque (Noakes and Carter, 1982; Kim et al., 2007, 2009) and seems to increase with increasing race distance (Table 10). An ultra-marathon over 308 km leads to a significantly higher creatine kinase than an ultra-marathon over 100 km (Yoon et al., 2016). In a 200-km ultra-marathon, creatine kinase increased to 35 times the baseline and remained elevated until 5 days after the race (Kim et al., 2009). In another 200-km ultra-marathon, the creatine kinase even rose to 90 times the initial value (Kim et al., 2007). In the “Badwater,” creatine kinase can increase up to ~27,951 U/l (Roth et al., 2007). And in the “Western States Endurance Run,” 216 (66%) of 328 finishers had creatine kinase concentrations of 1,500 U/l to 264,300 U/l and 13 (6%) of the finishers had values of more than 100,000 U/l (Hoffman et al., 2012a).

Figure 4. Muscle pain can accompany muscle damage occurring during an ultra-marathon. Figure by Céline Dewas.
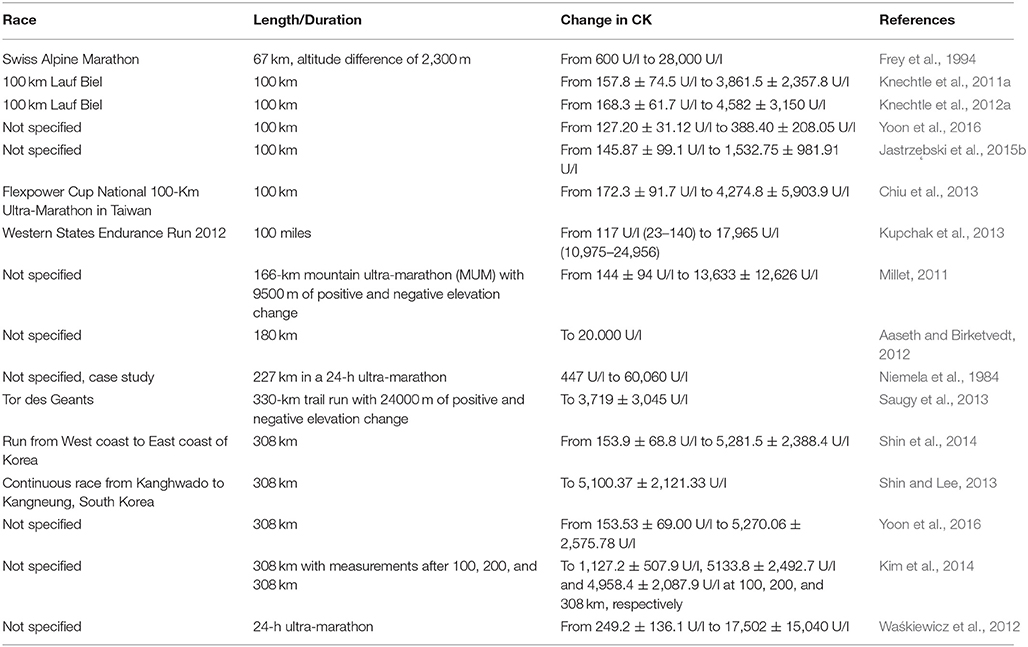
Table 10. Pre- and post-race CK-values from different races, sorted by the length of the races.
The increase in creatine kinase seems to be dependent on the fitness level of the runner (Noakes and Carter, 1982). Top ultra-marathoners have a lower creatine kinase before the start than slower runners, and after the run have significantly a lower creatine kinase than slower finishers (Suzuki, 2002). Ultra-marathoners with a creatine kinase higher than 500 mU/ml before the start felt tired and rather dropped out of the race (Suzuki, 2002). Important for athletes and coaches is the fact that the majority of athletes with significantly elevated creatine kinase levels are asymptomatic and do no require major medical attention (Magrini et al., 2017).
The extent of the skeletal muscle damage is clearly reflected in a severely limited muscular function after an ultra-marathon (Davies and Thompson, 1986) where standardized jumping exercises are restricted for ~18 days after an ultra-marathon (Chambers et al., 1998). The extensive muscle damage seems to lead to a decrease in muscle mass. Several studies have shown that an ultra-marathon leads to a significant reduction in skeletal muscle mass (Knechtle et al., 2011a, 2012a,e). Considering the relationship between skeletal muscle mass and muscle strength, it might be assumed that the post-race decrease in muscle strength would be partially attributed to the decrease of skeletal muscle mass.
Potential therapeutic options were investigated to reduce skeletal muscle damage during ultra-marathon running or to improve recovery after the race. An option was to reduce the decrease in skeletal muscle damage or to reduce the increase in metabolites of skeletal muscle damage by consumption amino acids during an ultra-marathon (Knechtle et al., 2012a). However, BCAA-supplementation before and during a 100-km ultra-marathon did not affect race performance and biomarkers of skeletal muscle damage (Knechtle et al., 2012a) and muscle pain (Knechtle et al., 2011a). It has also been investigated whether the use of a non-steroidal anti-inflammatory drug (NSAID) leads to reduced skeletal muscle damage. However, the use of diclofenac in a mountain ultra-marathon showed no effect on the increase in creatine kinase (Frey et al., 1994). The 100-mile “Western States Endurance Run” also showed that the intake of ibuprofen had no effect on skeletal muscle damage and pain sensation. Intake of ibuprofen leads to an increase in inflammatory markers such as C-reactive protein and interleukins (Nieman et al., 2006). The reason to consume NSAIDs in ultra-marathon running is explained by osteo-articular pain or to prevent pain. Ultra-marathoners consuming NSAIDS are predominantly motivated by their personal achievement (Didier et al., 2017). The intake of antioxidants does not seem to have any influence on skeletal muscle damage (Mastaloudis et al., 2004a, 2006). A diet with antioxidants leads to a significant reduction in skeletal muscle damage and increase in creatine kinase (Aaseth and Birketvedt, 2012).
The best option for a fast recovery after an ultra-marathon is appropriate training. In finishers in a 100-mile ultra-marathon, runners with lower post-race creatine kinase levels were better prepared for the race (Hoffman et al., 2017a). The extent of skeletal muscle damage can be significantly reduced by appropriate training with high training volumes (Hoffman et al., 2016) and long race experience (Noakes and Carter, 1982). It is well-known that the training for an ultra-marathon leads to characteristic changes and adaptations in the muscle fiber. As an adaptation to training, the mitochondria are very close to the capillaries, there is a proliferation of capillaries as well as an increase and enlargement of type I fibers (Crenshaw et al., 1991). Manual therapy and intermittent pneumatic compression are recovery methods used by endurance athletes with little evidence supporting effectiveness. In a controlled study with ultra-marathoners, both treatments reduced muscular fatigue scores acutely after treatment following the race and on post-race day 1. In addition, manual therapy improved muscle pain and soreness acutely following the race (Heapy et al., 2018). In summary, each ultra-marathon leads to skeletal muscle damage. Although levels of creatine-kinase can rise up to more than 100,000 U/l, this damage is reversible. The best prevention is appropriate training in the pre-race preparation.
Compared to other physiological systems and organs of human body, acute and chronic race-induced adaptations of bone in ultramarathon runners have been less studied. In addition to skeletal muscle, also bone appears to be damaged during an ultra-marathon (Kerschan-Schindl et al., 2009; Sansoni et al., 2017). During the “Spartathlon,” there is a direct influence on metabolites of bone metabolism leading to an increased bone resorption and a reduced bone formation (Kerschan-Schindl et al., 2009). In a mountain ultra-marathon, a correlation between the high energy consumption and bone damage with a decrease in osteocalcin was demonstrated (Sansoni et al., 2017). This could lead to a decrease in bone density leading to osteopenia and to osteoporosis after prolonged exposure. Furthermore, bone mineral density of women ultramarathoners has been related to menstrual function, where low lumbar spine bone mineral density has been observed in runners with history of oligo/amenorrhea (Micklesfield et al., 1995). Accordingly, it has been suggested that postmenopausal ultra-marathon runners were at high risk for large losses in bone mass (Folscher et al., 2015). Consequently, special attention is needed on the bone health of women ultramarathon runners.
As ultramarathon is a prolonged endurance exercise relying on aerobic energy transfer system, it is not surprising that a large body of the literature has focused on the exercise physiology of cardiovascular system. Due to the increase in creatine kinase, several studies investigated a potential heart damage through an ultra-marathon due to an increase in cardiac biomarkers such as creatine kinase, creatine kinase-MB, cardiac troponin I and N-terminal pro-brain natriuretic peptides after an ultra-marathon (Table 9; Roth et al., 2007; Kim et al., 2014; Christensen et al., 2017). A 90-km ultra-marathon also leads to a an increase in C-reactive protein as has been reported for heart attack patients (Strachan et al., 1984). However, the changes in these biomarkers are all transient (Christensen et al., 2017).
Running speed and the length of an ultra-marathon are important for potential changes of markers of cardiac damage. An ultra-marathon over 100 km leads to a significantly higher creatine kinase than an ultra-marathon over 308 km (Yoon et al., 2016). It is well-known that high-intensity endurance exercise leads to biochemical changes that may indicate heart damage (Salvagno et al., 2014). The highly sensitive cardiac troponin I increases after an ultra-marathon (Salvagno et al., 2014) where faster runners show a higher increase in cardiac troponin I than slower runners (Musha et al., 1997; Khodaee et al., 2015). The increase in cardiac troponin I can partially be dramatic. In the “Supermaratona dell'Etna” covering 43 km from sea level to 2850 m, mean cardiac troponin I increased by +900% (Da Ponte et al., 2018).
In men in a 308-km ultra-marathon, a normal creatine kinase-MB mass index (< 5.0 ng/ml) and no increase in cardiac troponin I could be detected and it was assumed that there had been no myocardial damage despite an increase in the creatine kinase-MB (Kim et al., 2014). Even in runners competing in “Badwater,” no structural damage to the myocardium could be demonstrated (Roth et al., 2007). In a 50- and 100-mile ultra-marathon, an increased activity of serum creatine kinase-MB could be detected in ~80% of the runners, with no evidence of myocardial damage in myocardial scintigraphy (Matin et al., 1983). Apart from creatine kinase, also specific cardiac hormones increase during an ultra-marathon. The hormones N-terminal brain natriuretic peptide (BNP) (Ohba et al., 2001; Hew-Butler et al., 2008a,b; Tchou et al., 2009) and atrial natriuretic peptide (ANP) (Ohba et al., 2001) were increased post-race.
It is very controversial whether an ultra-marathon leads to a damage of the heart. A study of 100-mile ultra-marathoners showed that the race induced changes in the heart. In the electrocardiogram, changes occurred in the right heart (Lord et al., 2015). The right heart leads showed a change in the electrocardiogram after the run compared to the electrocardiogram before the run for the P-wave, the ST-segment and the T-wave (Lord et al., 2016a).
A structural change of the heart muscle by an ultra-marathon could be detected by the use of echocardiography. Echocardiography can detect a reduction of the left (Niemela et al., 1984; Krzeminski et al., 2016; Maufrais et al., 2016) as well as the right ventricular (Oxborough et al., 2011; Lord et al., 2015, 2016b; Maufrais et al., 2016; Rothwell et al., 2018) function after an ultra-marathon. The changes in cardiac troponin I during an ultra-marathon are inversely associated with left ventriculare ejection fraction determined with echokardiography (Christensen et al., 2017).
The length of the ultra-marathon is important whether a change in the left and/or right ventricular function occurs. After the 2-day “Lowe Alpine Mountain Marathon,” both a systolic and diastolic dysfunction of the left ventricle could be detected. Humoral markers of myocardial damage were increased and the increase in cardiac troponin was considered to be associated with a minimal myocardial damage (Shave et al., 2002). After a 24-h ultra-marathon, two out of 20 runners showed a slight increase in cardiac troponins and echocardiography showed a decrease in left ventricular ejection fraction in one of the two runners (Passaglia et al., 2013). After an 89-km ultra-marathon, there was a reduced function of the left and right ventricles (Chan-Dewar et al., 2010). In a 4-h run, there was a decrease in the activity of the MIBG (131-J meta-iodo-benzylguanidine) in the myocardium, and the extent of activity decrease correlated with the distance covered during the run (Estorch et al., 1997). In a 160-km ultra-marathon, no correlation between the decrease in left ventricular function and the change in cardiac biomarkers could be demonstrated (Scott et al., 2009). During a 24-h ultra-marathon, the left ventricular function decreased during the last 6 h of the race where the function normalized within a few days after the race (Niemela et al., 1984). Another study showed that echocardiographic changes returned to normal within 1 day after the run (Dávila-Román et al., 1997). In some instances, an ultra-marathon leads to no echocardiographic changes. For runners in the “Western States Endurance Run,” echocardiographic findings were normal (George et al., 2011). Therefore, it is at the moment difficult to conclude that an ultra-marathon leads to substantial heart damage.
Although an ultra-marathon leads to a limitation of the left ventricular function and an increase in certain cardiac biomarkers, the mechanism behind these changes is unknown (Scott et al., 2009). An important aspect is also that the endurance training leads to an adjustment of the left ventricle in the sense of a left ventricular hypertrophy (Nagashima et al., 2003; Szauder et al., 2015). The size of the left ventricle is an important predictive variable for the performance of an ultramarathon (Nagashima et al., 2006). As women progressively compete in ultra-marathon, it has also been investigated whether a sex differences exist. In a 100-km and a 100-mile ultra-marathon, both men and women were examined and no difference was found in the echocardiographic changes between the sexes (Cote et al., 2015).
It is believed that elevated cholesterol is a cardiovascular risk factor with an increased morbidity and mortality. An ultra-marathon could be beneficial for reducing elevated cholesterol (Thompson et al., 1982; Kaminsky et al., 1988; Wu et al., 2004; Sapounakis et al., 2010). There has been shown a reduction in triglycerides and total cholesterol after a 24-h ultra-marathon, but no change in low density lipoprotein cholesterol and high density lipoprotein cholesterol (Emed et al., 2016). In another study, a reduction in total cholesterol, low density lipoprotein cholesterol and triglycerides was demonstrated after an ultra-marathon (Kaminsky et al., 1989). Only training lowers low density lipoprotein cholesterol in an ultra-marathon (Tomaszewski et al., 2004). Runners preparing for an ultra-marathon experience a decrease in total and low density lipoprotein cholesterol (Sapounakis et al., 2010). Obviously, training for and competing in an ultra-marathon might be considered as preventive for cardiovascular diseases.
The physiology and pathophysiology of digestive tract in ultramarathon runners attracts widespread interest due to the abovementioned large energetic demands of training and competititon. Digestive tract plays a critical role in delivering nutrients during endurance exercise; thus, the occurrence of digestive problems might limit performance (Jeukendrup, 2017). Ultra-marathoners often suffer from digestive problems (Rehrer et al., 1992) and gastrointestinal bleeding after an ultra-marathon is not uncommon (Baska et al., 1990) where often occult bleeding occurs (Chiu et al., 2015). Symptoms of the lower gastrointestinal tract correlate with gastrointestinal bleeding (Baska et al., 1990). In a 100-mile ultra-marathon, ~35% (Stuempfle and Hoffman, 2015) and in a mountain ultra-marathon ~43% of runners complained about digestive problems (Rehrer et al., 1992). In some cases as many as 80% and more of the finishers complain of digestive problems (Wardenaar et al., 2015; Stuempfle et al., 2016), with nausea being mentioned most frequently (Figure 5; Stuempfle et al., 2016). Digestive problems are one of the main reasons why ultra-runners have to give up an ultra-marathon (Hoffman and Fogard, 2011). Up to 90% of runners who give up an ultra-marathon complain of nausea (Stuempfle and Hoffman, 2015).

Figure 5. Nausea is the most frequently mentioned digestive problem in ultra-marathon runners. Figure by Céline Dewas.
A possible reason for these digestive problems could be that an ultra-marathon changes the motility of the esophagus (Simons and Kennedy, 2004). Endotoxemia seems to be a major cause of digestive problems, while factors such as hyperthermia, dehydration and nutrition are barely causative (Stuempfle et al., 2016). Experience seems to be important. Runners with digestive problems during an ultra-marathon have less training km and shorter training runs (Glace et al., 2002). From a pathomechanistic point of view, endotoxins and pro-inflammatory cytokines increased in a 24-h ultra-marathon and this increase led to a counter-regulatory anti-inflammatory reaction (Gill et al., 2015a,b).
From a therapeutic point of view, it seems very difficult to treat gastrointestinal problems. The intake of sodium during a 100-mile ultra-marathon definitely has no influence on nausea and vomiting (Hoffman and Stuempfle, 2016a). The best way to prevent digestive problems is to eat what you like most during an ultra-marathon (Moran et al., 2011). The high-fat foods and increased fat intake during an ultra-marathon seem to cause significantly less digestive problems (Stuempfle et al., 2013) and ingesting a proton pump inhibitor before an ultra-marathon significantly reduces the risk of gastrointestinal bleeding during the run (Thalmann et al., 2006). Regarding digestive problems in ultra-marathon running, the prevalence is very high and the only option is prevention by eating what you like most during an ultra-marathon.
Regular physical activity has a positive effect on liver function. On the other hand, a very long endurance exercise—especially under difficult climatic conditions (Carvalho et al., 2016)—can become a problem for the liver (Shephard and Johnson, 2015). Especially longer runs at low intensity seem to be more of a problem for the liver (Shin et al., 2016). There may be a detectable impairment in liver function during an ultra-marathon (De Paz et al., 1995; Chiu et al., 2013; Bird et al., 2014; Shin et al., 2014; Table 9).
An ultra-marathon can lead to an increase in gamma-glutamyltransferase (De Paz et al., 1995; Shin et al., 2014), alanine aminotransferase (De Paz et al., 1995; Chiu et al., 2013; Bird et al., 2014; Kupchak et al., 2014; Jastrzębski et al., 2015b), aspartate aminotransferase (De Paz et al., 1995; Chiu et al., 2013; Bird et al., 2014; Kupchak et al., 2014; Jastrzebski et al., 2015; Jastrzębski et al., 2015b), alkaline phosphatase (Noakes and Carter, 1982; Wu et al., 2004; Kupchak et al., 2014), and bilirubin (De Paz et al., 1995; Fallon et al., 1999a; Wu et al., 2004; Bird et al., 2014; Shin et al., 2014; Chou et al., 2016; Jastrzebski et al., 2016). These changes are dependent on the intensity and/or duration of the physical performance and generally normalize within a few days after the race (Wu et al., 2004; Bird et al., 2014).
However, it can happen in very rare cases that an ultra-marathon can lead to pronounced liver damage (Heneghan et al., 2014; Carvalho et al., 2016). In a young runner in a 62-km ultra-marathon a case was described with a heat stroke. As a result, pronounced rhabdomyolysis and hypoxic hepatitis with multiple organ failure, including fulminant liver failure, resulted in intensive care measures. Later, an emergency hepatectomy and orthotopic liver transplantation had to be performed (Heneghan et al., 2014). In another case, a 25-year-old man had hyperthermia with neurological restrictions during an ultra-marathon. In the further course, acute liver failure occurred and the patient had to be monitored intensively but recovered again (Carvalho et al., 2016). Regarding a potential liver damage, the increase in biomarkers of liver damage is reversible and a serious liver damage is very seldom to expect.
During ultra-marathon running, a damage to the kidney with an impaired renal function is quite often observed (Boulter et al., 2011). The prevalence of an acute kidney injury in ultra-marathon running is nearly 50% of all runners (Lipman et al., 2017).
From a pathophysiological point of view, the skeletal muscle damage leads to an influx of muscle proteins, such as myoglobin, into the bloodstream. In certain circumstances, such as pronounced dehydration or heat, there may be a marked accumulation in the kidney with consequent kidney damage (Schiff et al., 1978; Uberoi et al., 1991; Clarkson, 2007).
Regarding fluid and electrolyte metabolism, an ultra-marathon leads to quite characteristic changes. It seems that short and fast ultra-marathons are more likely to cause a kidney problem than longer ultra-marathons at lower speeds (Shin et al., 2016). An ultra-marathon leads to an increase in creatinine (Schiff et al., 1978; Uberoi et al., 1991; Clarkson, 2007; Lipman et al., 2017), urea (Shin et al., 2016), uric acid (Schiff et al., 1978; Uberoi et al., 1991), sodium (McKechnie et al., 1982; Bürge et al., 2011; Cejka et al., 2012), potassium (Uberoi et al., 1991; Kłapcinska et al., 2013; Jastrzebski et al., 2016), calcium (Fallon et al., 1999a; Kłapcinska et al., 2013) and phosphate (Fallon et al., 1999a). Furthermore, there is also a characteristic change in hormones of water and electrolyte metabolism such as vasopressin (Hew-Butler et al., 2008a, 2011; Rogers et al., 2011), copeptin (Hew-Butler et al., 2011; Lippi et al., 2015), oxytocin (Hew-Butler et al., 2008a) and aldosterone (Hew-Butler et al., 2011; Table 9).
An ultra-marathon often leads to a temporary reduction in renal function (Lippi et al., 2012a; Lipman et al., 2014, 2016; Hou et al., 2015; Mrakic-Sposta et al., 2015; Hoffman and Weiss, 2016), although in some cases all runners tested suffer from renal impairment (Kao et al., 2015). In rare cases, there is evidence of a considerably impaired renal function (Irving et al., 1990). Generally, the kidney function recovers within one (Kao et al., 2015) to a few days (Kallmeyer and Miller, 1993). In a multi-stage ultra-marathon, the kidney function often recovers until the next morning's start (Lipman et al., 2014). It can also happen that a dialysis-dependent renal insufficiency develops during an ultra-marathon (Uberoi et al., 1991). Even if a runner experiences a restriction of renal function during an ultra-marathon, another ultra-marathon does not necessarily lead to an additional restriction of kidney function (Irving et al., 1990; Hoffman and Weiss, 2016). It has been shown that certain people rather suffer a kidney problem and/or a certain behavior can preferably lead to a kidney problem.
Risk factors for kidney damage during an ultra-marathon are female sex, a low body weight and a significant body weight loss during the run (Lipman et al., 2016). Other risk factors include severe muscle damage with rhabdomyolysis, dehydration, hypotension, hyperuricemia, hyponatraemia, poor competition, and the use of NSAIDs (Seedat et al., 1989; Clarkson, 2007; Boulter et al., 2011). In ultra-marathoners, increased rates of acute kidney injury were found in those who took ibuprofen (Lipman et al., 2017).
From a diagnostic point of view, the test strip method under field conditions could serve well to detect kidney damage due to an ultra-marathon. In a certain percentage of finishers, microhematuria is a sign of kidney damage (Kallmeyer and Miller, 1993). In 100-mile ultra-marathoners, blood and urine levels were measured and compared upon arrival at the finish line. In ultra-marathoners with kidney damage detected by creatinine levels in the blood, the test strip showed very high specificity and sensitivity, protein, blood and increased urine specific gravity (Hoffman et al., 2013b). Damage to the kidneys occurs very often in ultra-marathon running; however, the kidney function recovers well within a few days. Similarly to the liver, serious kidney damage is very seldom to expect.
It is well-known that intense physical stress leads to tissue damage (McKune et al., 2005). Experienced ultra-marathoners experience also a change in the concentration of immunoglobulins after an ultra-marathon, which might have an impact on the health of finishers (McKune et al., 2005). An ultra-marathon seems to lead to an acute inflammatory reaction with classical laboratory chemical changes (Kasprowicz et al., 2013; Shin and Lee, 2013). The stress-related inflammation affects the bone marrow and leads to an increased leukocyte turnover (Spiropoulos et al., 2010). Markers of an inflammatory process include leucocytes (Jee et al., 2013; Bird et al., 2014; Chiu et al., 2015; Jastrzebski et al., 2016; Zakovska et al., 2017), C-reactive protein (Kim et al., 2009; Waśkiewicz et al., 2012; Kasprowicz et al., 2013), ferritin (Chiu et al., 2015), TNF-α (Nieman et al., 2000; Simons and Kennedy, 2004; Jee and Jin, 2012; Chiu et al., 2013, 2015), blood sedimentation reaction, iron (Fallon, 2001), y-interferon (Simons and Kennedy, 2004), Interleukin 1 receptor antagonist (Nieman et al., 2000), Interleukin-1b (Simons and Kennedy, 2004; Gill et al., 2015b), Interleukin-8 (Nieman et al., 2000; Gill et al., 2015b), Interleukin-10 (Nieman et al., 2000; Simons and Kennedy, 2004; Gill et al., 2015b) and Interleukin-6 (Fallon et al., 1999a; Waśkiewicz et al., 2012; Kasprowicz et al., 2013).
There seems to be an association between the stress on the immune system and skeletal muscle damage. In 100-km ultra-marathoners, an association between the markers of the acute inflammation of the organism (i.e., neutrophils, immature neutrophils, platelets, and monocytes) and the markers of muscle damage (i.e., CK, platelets, and LDH) could be demonstrated (Zakovska et al., 2017).
Ultra-marathoners often suffer from upper respiratory infections after a race (Peters and Bateman, 1983; Peters et al., 1993). It has been demonstrated that ultra-marathoners are more likely to suffer from an infection than runners over shorter distances (Castell, 1996). The infections can already occur 4 weeks before the start and 7–14 days after the end of the race (Peters et al., 2010). Regarding the frequency of infections, ~25–30% of runners are affected by an ultra-marathon (Peters and Bateman, 1983; Nieman et al., 2003). In the “Two Oceans Marathon” held in Cape Town, South Africa, more than 30% of runners suffered from upper respiratory tract infections, mainly affecting the faster runners (Peters and Bateman, 1983). Often, faster ultra-marathoners have more infections than slower ultra-marathoners (Peters et al., 2004) while slower ultra-marathoners have the frequency of infections in the range of persons in a control group (Peters and Bateman, 1983). It has been shown that a 24-h ultra-marathon leads to a decrease in salivary flow, a decrease in salivary IgA, and a decrease in the secretion of salivary lysozyme (Gill et al., 2013, 2014).
Both the frequency and the severity of an infection after an ultra-marathon can be favorably influenced. The concentration of glutamine in the blood is reduced by up to ~20% after an ultra-marathon (Castell and Newsholme, 1997). Intake of glutamine before and after an ultra-marathon reduces the frequency of infections (Castell, 1996; Castell and Newsholme, 1997, 1998). In addition to glutamine, vitamin C has beneficial effects on upper airway infections in ultra-marathoners (Peters, 1997). The regular intake of vitamin C can improve the resistance to the increased occurrence of upper respiratory tract infections and—if an infection nevertheless occurs—somewhat reduce the severity of the infection (Peters et al., 1993). Even if vitamin C has an influence on an infection, the intake of vitamin C does not lead to a change in various infection parameters such as immune cells, interleukins, or interferon (Nieman et al., 2002). The amount of vitamin C intake seems important. In runners who successfully completed the “Comrades Marathon,” the daily intake of 1,500 mg of vitamin C in the week before the competition resulted in a significantly lower increase in interleukins than the daily intake of 500 mg (Nieman et al., 2000). A higher amount of vitamin C also leads to low increases in cortisol and adrenaline during the race (Peters et al., 2001a,b).
In very rare cases, an infection after an ultra-marathon can lead to quite disastrous dimensions. In a 51-year-old runner, after a multi-stage ultra-marathon, a necrotizing soft tissue infection of both feet with septicemia occurred. A transmetatarsal amputation had to be performed on the left and a femoral amputation on the right side (Huang et al., 2014).
An ultra-marathon seems to have a positive influence on the immune system (Schobersberger et al., 2000). There is a correlation between regular endurance training and an increase in natural killer cells, a subset of lymphocytes and this increase leads to a favorable influence on the natural immune system (Francavilla et al., 2005). Even if it is clear that an ultra-marathon reduces the concentration of immunoglobulins, endurance exercise with moderate intensity will increase the concentration of immunoglobulins and reduce the risk of infection (Nieman and Nehlsen-Cannarella, 1991).
An ultra-marathon seems to lead to a depression of the immune function with an increased prevalence of infections of the upper respiratory tract. Most probably the intensity of running is crucial since running at moderate intensity seems to increase the concentration of immunoglobulins with a reduced risk of infections.
Considering the increased exercise-induced stress for most physiological systems of human body as demonstrated in the previous sections of this review, one might assume that the completion of ultra-marathons must be very health-damaging. Undoubtedly, the completion of an ultra-marathon has no immediate health benefits. However, with regards to the length of the telomeres, training for ultra-marathons seems to have a certain positive effect in endurance athletes (Borghini et al., 2015). Particularly, regular endurance training seems to have a protective effect on telomere length and should slow down the aging process (Denham et al., 2013). On the other hand, an extreme ultra-marathon such as “Tor des Géants” (330 km, 24,000 m vertically) leads to shortening of telomeres, probably due to oxidative damage to the DNA (Borghini et al., 2015). However, it does not necessarily take such a tremendous run as the “Tor des Géants”; even a 50-km run might provoke DNA damage (Mastaloudis et al., 2004b). The production of serum reactive oxygen species increases during an ultra-marathon indicating that the antioxidant system restricts the production of serum reactive oxygen species (Hattori et al., 2009). Thus, it might be supported that the overall effect of ultra-marathon on health is positive due to the beneficial role of endurance exercise.
In summary, considering the increased number of participants in ultra-marathons, the findings of the present review would have practical applications for a large number of sports scientists and sports medicine practitioners working in this field. Ultra-marathoners seem to be aware of the potential harmful influence on health, but also know that the side effects of ultra-marathon running are reversible within a few days. It should be highlighted that only one review had been conducted previously concerning only ultra-marathoners which focused on a very specific topic (neuromuscular fatigue) (Millet, 2011). Other reviews examined musculoskeletal injuries of both ultra-marathoners and other distance runners (e.g., marathon and shorter distances) (Kluitenberg et al., 2015; Videbæk et al., 2015). Thus, the present review is the most comprehensive review ever conducted on physiology and pathophysiology in ultra-marathon.
BK and PN collected the studies for the review and drafted the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The figures are credited to Dr. Céline Dewas, specialist in medical images.
Aaseth, J., and Birketvedt, G. S. (2012). Hemolysis and rhabdomyolysis after marathon and long distance running. Immunol. Endocr. Metab. Agents Med. Chem. 12, 8–13. doi: 10.2174/187152212799857655
Agawa, H., Yamada, N., Enomoto, Y., Suzuki, H., Hosono, A., Arakawa, K., et al. (2008). Changes of mental stress biomarkers in ultramarathon. Int. J. Sports Med. 29, 867–871. doi: 10.1055/s-2008-ssss490
Ambros-Rudolph, C. M., Hofmann-Wellenhof, R., Richtig, E., Müller-Fürstner, M., Soyer, H. P., and Kerl, H. (2006). Malignant melanoma in marathon runners. Arch. Dermatol. 142, 1471–1474. doi: 10.1001/archderm.142.11.1471
Andonian, P., Viallon, M., Le Goff, C., De Bourguignon, C., Tourel, C., Morel, J., et al. (2016). Shear-wave elastography assessments of quadriceps stiffness changes prior to, during and after prolonged exercise: a longitudinal study during an extreme mountain ultra-marathon. PLoS ONE 11:e0161855. doi: 10.1371/journal.pone.0161855
Arrese, A. L., and Ostariz, E. S. (2006). Skinfold thicknesses associated with distance running performance in highly trained runners. J. Sports Sci. 24, 69–76. doi: 10.1080/02640410500127751
Bam, J., Noakes, T. D., Juritz, J., and Dennis, S. C. (1997). Could women outrun men in ultramarathon races? Med. Sci. Sports Exerc. 29, 244–247. doi: 10.1097/00005768-199702000-00013
Banfi, G., Roi, G. S., Dolci, A., and Susta, D. (2004). Behaviour of haematological parameters in athletes performing marathons and ultramarathons in altitude (‘skyrunners’). Clin. Lab. Haematol. 26, 373–377. doi: 10.1111/j.1365-2257.2004.00642.x
Barr, S. I., and Costill, D. L. (1989). Water: can the endurance athlete get too much of a good thing? J. Am. Diet. Assoc. 89, 1629-1632, 1635.
Baska, R. S., Moses, F. M., Graeber, G., and Kearney, G. (1990). Gastrointestinal bleeding during an ultramarathon. Dig. Dis. Sci. 35, 276–279. doi: 10.1007/bf01536777
Belli, T., Meireles, C. L. S., Costa, M. O., Ackermann, M. A., and Gobatto, C. A. (2016). Somatotype, body composition and performance in ultramarathon. Rev. Bras. Cineantropom. Desempenho Hum. 18, 127–135. doi: 10.5007/1980-0037.2016v18n2p127
Bird, S. R., Linden, M., and Hawley, J. A. (2014). Acute changes to biomarkers as a consequence of prolonged strenuous running. Ann. Clin. Biochem. 51, 137–150. doi: 10.1177/0004563213492147
Bishop, G. W., and Fallon, K. E. (1999). Musculoskeletal injuries in a six-day track race: ultramarathoner's ankle. Clin. J. Sport Med. 9, 216–220.
Bobbert, T., Mai, K., Brechtel, L., Schulte, H. M., Weger, B., Pfeiffer, A. F., et al. (2012). Leptin and endocrine parameters in marathon runners. Int. J. Sports Med. 33, 244–248. doi: 10.1055/s-0031-1291251
Borghini, A., Giardini, G., Tonacci, A., Mastorci, F., Mercuri, A., Mrakic-Sposta, S., et al. (2015). Chronic and acute effects of endurance training on telomere length. Mutagenesis 30, 711–716. doi: 10.1093/mutage/gev038
Bossi, A. H., Matta, G. G., Millet, G. Y., Lima, P., Pertence, L. C., De Lima, J. P., et al. (2017). Pacing strategy during 24-hour ultramarathon-distance running. Int. J. Sports Physiol. Perform. 12, 590–596. doi: 10.1123/ijspp.2016-0237
Boulter, J., Noakes, T. D., and Hew-Butler, T. (2011). Acute renal failure in four Comrades Marathon runners ingesting the same electrolyte supplement: coincidence or causation? S. Afr. Med. J. 101, 876–878.
Bracher, A., Knechtle, B., Gnadinger, M., Burge, J., Rust, C. A., Knechtle, P., et al. (2012). Fluid intake and changes in limb volumes in male ultra-marathoners: does fluid overload lead to peripheral oedema? Eur. J. Appl. Physiol. 112, 991–1003. doi: 10.1007/s00421-011-2056-3
Brown, J. S., and Connolly, D. A. (2015). Selected human physiological responses during extreme heat: the badwater ultramarathon. J. Strength Cond. Res. 29, 1729–1736. doi: 10.1519/JSC.0000000000000787
Bruso, J. R., Hoffman, M. D., Rogers, I. R., Lee, L., Towle, G., and Hew-Butler, T. (2010). Rhabdomyolysis and hyponatremia: a cluster of five cases at the 161-km 2009 Western States Endurance Run. Wilderness Environ. Med. 21, 303–308. doi: 10.1016/j.wem.2010.06.012
Bürge, J., Knechtle, B., Knechtle, P., Gnadinger, M., Rust, C. A., and Rosemann, T. (2011). Maintained serum sodium in male ultra-marathoners-the role of fluid intake, vasopressin, and aldosterone in fluid and electrolyte regulation. Horm. Metab. Res. 43, 646–652. doi: 10.1055/s-0031-1284352
Cairns, R. S., and Hew-Butler, T. (2015). Incidence of exercise-associated hyponatremia and its association with nonosmotic stimuli of arginine vasopressin in the GNW100s ultra-endurance marathon. Clin. J. Sport Med. 25, 347–354. doi: 10.1097/JSM.0000000000000144
Cairns, R. S., and Hew-Butler, T. (2016). Proof of concept: hypovolemic hyponatremia may precede and augment creatine kinase elevations during an ultramarathon. Eur. J. Appl. Physiol. 116, 647–655. doi: 10.1007/s00421-015-3324-4
Carmona, G., Roca, E., Guerrero, M., Cussó, R., Irurtia, A., Nescolarde, L., et al. (2015). Sarcomere disruptions of slow fiber resulting from mountain ultramarathon. Int. J. Sports Physiol. Perform. 10, 1041–1047. doi: 10.1123/ijspp.2014-0267
Carvalho, A. S., Rodeia, S. C., Silvestre, J., and Povoa, P. (2016). Exertional heat stroke and acute liver failure: a late dysfunction. BMJ Case Rep. 2016:214434. doi: 10.1136/bcr-2016-214434
Case, S., Evans, D., Tibbets, G., Case, S., and Miller, D. (1995). Dietary intakes of participants in the IditaSport Human Powered Ultra-marathon. Alaska Med. 37, 20–24.
Casoni, I., Borsetto, C., Cavicchi, A., Martinelli, S., and Conconi, F. (1985). Reduced hemoglobin concentration and red cell hemoglobinization in Italian marathon and ultramarathon runners. Int. J. Sports Med. 6, 176–179.
Castell, L. M. (1996). Does glutamine have a role in reducing infections in athletes? Eur. J. Appl. Physiol. Occup. Physiol. 73, 488–490. doi: 10.1007/BF00334429
Castell, L. M., and Newsholme, E. A. (1997). The effects of oral glutamine supplementation on athletes after prolonged, exhaustive exercise. Nutrition 13, 738–742.
Castell, L. M., and Newsholme, E. A. (1998). Glutamine and the effects of exhaustive exercise upon the immune response. Can. J. Physiol. Pharmacol. 76, 524–532.
Cejka, C., Knechtle, B., Knechtle, P., Rüst, C. A., and Rosemann, T. (2012). An increased fluid intake leads to feet swelling in 100-km ultra-marathoners-an observational field study. J. Int. Soc. Sports Nutr. 9:11. doi: 10.1186/1550-2783-9-11
Cejka, N., Knechtle, B., Rust, C. A., Rosemann, T., and Lepers, R. (2015). Performance and age of the fastest female and male 100-KM ultramarathoners worldwide from 1960 to 2012. J. Strength Cond. Res. 29, 1180–1190. doi: 10.1519/jsc.0000000000000370
Chambers, C., Noakes, T. D., Lambert, E. V., and Lambert, M. I. (1998). Time course of recovery of vertical jump height and heart rate versus running speed after a 90-km foot race. J. Sports Sci. 16, 645–651. doi: 10.1080/026404198366452
Chan-Dewar, F., Oxborough, D., Shave, R., Gregson, W., Whyte, G., Noakes, T., et al. (2010). Evidence of increased electro-mechanical delay in the left and right ventricle after prolonged exercise. Eur. J. Appl. Physiol. 108, 581–587. doi: 10.1007/s00421-009-1264-6
Chiu, Y. H., Hou, S. K., How, C. K., Li, L. H., Kao, W. F., Yang, C. C., et al. (2013). Influence of a 100-km ultra-marathon on hepatitis B carrier runners. Int. J. Sports Med. 34, 841–845. doi: 10.1055/s-0032-1331769
Chiu, Y. H., Lai, J. I., Wang, S. H., How, C. K., Li, L. H., Kao, W. F., et al. (2015). Early changes of the anemia phenomenon in male 100-km ultramarathoners. J. Chin. Med. Assoc. 78, 108–113. doi: 10.1016/j.jcma.2014.09.004
Chlibkova, D., Knechtle, B., Rosemann, T., Zakovska, A., and Tomaskova, I. (2014). The prevalence of exercise-associated hyponatremia in 24-hour ultra-mountain bikers, 24-hour ultra-runners and multi-stage ultra-mountain bikers in the Czech Republic. J. Int. Soc. Sports Nutr. 11:3. doi: 10.1186/1550-2783-11-3
Chou, S. L., Chou, M. Y., Wang, Y. H., Kuo, F. C., and Kao, W. F. (2016). The impact of chronic carrier of hepatitis B virus on liver function in a 7-day ultramarathon race. J. Chin. Med. Assoc. 79, 179–184. doi: 10.1016/j.jcma.2015.10.006
Christensen, D. L., Espino, D., Infante-Ramirez, R., Cervantes-Borunda, M. S., Hernandez-Torres, R. P., Rivera-Cisneros, A. E., et al. (2017). Transient cardiac dysfunction but elevated cardiac and kidney biomarkers 24 h following an ultra-distance running event in Mexican Tarahumara. Extr. Physiol. Med. 6, 3. doi: 10.1186/s13728-017-0057-5
Clarkson, P. M. (2007). Exertional rhabdomyolysis and acute renal failure in marathon runners. Sports Med. 37, 361–363.
Coast, J. R., Blevins, J. S., and Wilson, B. A. (2004). Do gender differences in running performance disappear with distance? Can. J. Appl. Physiol. 29, 139–145. doi: 10.1139/h04-010
Cona, G., Cavazzana, A., Paoli, A., Marcolin, G., Grainer, A., Bisiacchi, P. S., et al. (2015). It's a matter of mind! Cognitive functioning predicts the athletic performance in ultra-marathon runners. PLoS ONE, 10:e0132943. doi: 10.1371/journal.pone.0132943
Copeland, J. L., and Verzosa, M. L. S. (2014). Endocrine response to an ultra-marathon in pre- and post-menopausal women. Biol. Sport 31, 125–131. doi: 10.5604/20831862.1097480
Costa, R. J. S., Gill, S. K., Hankey, J., Wright, A., and Marczak, S. (2014). Perturbed energy balance and hydration status in ultra-endurance runners during a 24 h ultra-marathon. Br. J. Nutr. 112, 428–437. doi: 10.1017/S0007114514000907
Costa, R. J. S., Teixeira, A., Rama, L., Swancott, A. J. M., Hardy, L. D., Lee, B., et al. (2013). Water and sodium intake habits and status of ultra-endurance runners during a multi-stage ultra-marathon conducted in a hot ambient environment: an observational field based study. Nutr. J. 12:13. doi: 10.1186/1475-2891-12-13
Cote, A. T., Phillips, A. A., Foulds, H. J., Charlesworth, S. A., Bredin, S. S. D., Burr, J. F., et al. (2015). Sex differences in cardiac function after prolonged strenuous exercise. Clin. J. Sport Med. 25, 276–283. doi: 10.1097/JSM.0000000000000130
Crenshaw, A. G., Fridén, J., Thornell, L. E., and Hargens, A. R. (1991). Extreme endurance training evidence of capillary and mitochondria compartmentalization in human skeletal muscle. Eur. J. Appl. Physiol. Occup. Physiol. 63, 173–178. doi: 10.1007/BF00233843
Cuthill, J. A., Ellis, C., and Inglis, A. (2009). Hazards of ultra-marathon running in the Scottish highlands: exercise-associated hyponatraemia. Emerg. Med. J. 26, 906–907. doi: 10.1136/emj.2008.065524
Da Ponte, A., Giovanelli, N., Antonutto, G., Nigris, D., Curcio, F., Cortese, P., et al. (2018). Changes in cardiac and muscle biomarkers following an uphill-only marathon. Res. Sports Med. 26, 100–111. doi: 10.1080/15438627.2017.1393750
Damas, F., Libardi, C. A., and Ugrinowitsch, C. (2018). The development of skeletal muscle hypertrophy through resistance training: the role of muscle damage and muscle protein synthesis. Eur. J. Appl. Physiol. 118, 485–500. doi: 10.1007/s00421-017-3792-9
Davies, C. T. M., and Thompson, M. W. (1979). Aerobic performance of female marathon and male ultramarathon athletes. Eur. J. Appl. Physiol. Occup. Physiol. 41, 233–245. doi: 10.1007/BF00429740
Davies, C. T. M., and Thompson, M. W. (1986). Physiological responses to prolonged exercise in ultramarathon athletes. J. Appl. Physiol. 61, 611–617.
Dávila-Román, V. G., Guest, T. M., Tuteur, P. G., Rowe, W. J., Ladenson, J. H., and Jaffe, A. S. (1997). Transient right but not left ventricular dysfunction after strenuous exercise at high altitude. J. Am. Coll. Cardiol. 30, 468–473. doi: 10.1016/S0735-1097(97)00179-4
De Paz, J. A., Villa, J. G., Lopez, P., and Gonzalez-Gallego, J. (1995). Effects of long-distance running on serum bilirubin. Med. Sci. Sports Exerc. 27, 1590–1594.
Denham, J., Nelson, C. P., O'Brien, B. J., Nankervis, S. A., Denniff, M., Harvey, J. T., et al. (2013). Longer leukocyte telomeres are associated with ultra-endurance exercise independent of cardiovascular risk factors. PLoS ONE 8:e0069377. doi: 10.1371/journal.pone.0069377
Dickson, D. N., Wilkinson, R. L., and Noakes, T. D. (1982). Effects of ultra-marathon training and racing on hematologic parameters and serum ferritin levels in well-trained athletes. Int. J. Sports Med. 3, 111–117.
Didier, S., Vauthier, J. C., Gambier, N., Renaud, P., Chenuel, B., and Poussel, M. (2017). Substance use and misuse in a mountain ultramarathon: new insight into ultrarunners population? Res. Sports Med. 25, 244–251. doi: 10.1080/15438627.2017.1282356
Doppelmayr, M., and Molkenthin, A. (2004). Motivation of participants in adventure ultramarathons compared to other foot races. Biol. Sport 21, 319–323.
Eden, B. D., and Abernethy, P. J. (1994). Nutritional intake during an ultraendurance running race. Int. J. Sport Nutr. 4, 166–174.
Eichenberger, E., Knechtle, B., Rüst, C. A., Lepers, R., Rosemann, T., and Onywera, V. O. (2012). The aspect of nationality and performance in a mountain ultra-maratho-the ‘Swiss Alpine Marathon’. J. Hum. Sport Exerc. 7, 748–762. doi: 10.4100/jhse.2012.74.03
Eijsvogels, T. M., Thijssen, D. H., Poelkens, F., Binkhorst, M., Wouters, C. W., Schouwenberg, B. J., et al. (2008). [Physical risks whilst walking the Nijmegen Four Days Marches in 2007: electrolyte imbalance in 1 in 5 walkers]. Ned. Tijdschr. Geneeskd. 152, 1571–1578.
Emed, L. G. M., Passaglia, D. G., Guerios, S. T., João, P. G. D., Moser, A. I. S., Abdalla, D. S. P., et al. (2016). Acute modification in plasma lipid levels in ultramarathon runners. J. Sports Sci. 34, 1657–1661. doi: 10.1080/02640414.2015.1130237
Enqvist, J. K., Mattsson, C. M., Johansson, P. H., Brink-Elfegoun, T., Bakkman, L., and Ekblom, B. T. (2010). Energy turnover during 24 hours and 6 days of adventure racing. J. Sports Sci. 28, 947–955. doi: 10.1080/02640411003734069
Estorch, M., Serra-Grima, R., Carrió, I., Flotats, A., Lizárraga, A., Bernà, L. L., et al. (1997). Influence of prolonged exercise on myocardial distribution of 123I-MIBG in long-distance runners. J. Nucl. Cardiol. 4, 396–402. doi: 10.1016/s1071-3581(97)90031-3
Fallon, K. E. (1996). Musculoskeletal injuries in the ultramarathon: the 1990 westfield Sydney to Melbourne run. Br. J. Sports Med. 30, 319–323.
Fallon, K. E. (2001). The acute phase response and exercise: the ultramarathon as prototype exercise. Clin. J. Sport Med. 11, 38–43. doi: 10.1097/00042752-200101000-00007
Fallon, K. E., and Bishop, G. (2002). Changes in erythropoiesis assessed by reticulocyte parameters during ultralong distance running. Clin. J. Sport Med. 12, 172–178. doi: 10.1097/00042752-200205000-00005
Fallon, K. E., Broad, E., Thompson, M. W., and Reull, P. A. (1998). Nutritional and fluid intake in a 100-km ultramarathon. Int. J. Sport Nutr. Exerc. Metab. 8, 24–35.
Fallon, K. E., Sivyer, G., Sivyer, K., and Dare, A. (1999a). The biochemistry of runners in a 1600 km ultramarathon. Br. J. Sports Med. 33, 264–269.
Fallon, K. E., Sivyer, G., Sivyer, K., Dare, A., and Watts, E. J. (1999b). Changes in haematological parameters and iron metabolism associated with a 1600 kilometre ultramarathon. Br. J. Sports Med. 33, 27–32.
Fazal, A. A., Whittemore, M. S., and DeGeorge, K. C. (2017). Foot-strike haemolysis in an ultramarathon runner. BMJ Case Rep. 2017:220661. doi: 10.1136/bcr-2017-220661
Folscher, L. L., Grant, C. C., Fletcher, L., and Janse van Rensberg, D. C. (2015). Ultra-marathon athletes at risk for the female athlete triad. Sports Med. Open 1, 29. doi: 10.1186/s40798-015-0027-7
Fonseca-Engelhardt, K., Knechtle, B., Rüst, C. A., Knechtle, P., Lepers, R., and Rosemann, T. (2013). Participation and performance trends in ultra-endurance running races under extreme conditions - ‘Spartathlon’ versus ‘Badwater’. Extr. Physiol. Med. 2:15. doi: 10.1186/2046-7648-2-15
Fournier, P. E., Stalder, J., Mermillod, B., and Chantraine, A. (1997). Effects of a 110 kilometers ultra-marathon race on plasma hormone levels. Int. J. Sports Med. 18, 252–256. doi: 10.1055/s-2007-972629
Francavilla, G., Tripoli, S., Amato, S., Tolomeo, M., and Francavilla, V. C. (2005). Modifications of some immune parameters in a group of amateur athletes playing marathon and ultra-marathon. Med. Dello Sport 58, 203–206.
Freund, W., Weber, F., Billich, C., and Schuetz, U. H. (2012). The foot in multistage ultra-marathon runners: experience in a cohort study of 22 participants of the Trans Europe Footrace Project with mobile MRI. BMJ Open 2:e001118. doi: 10.1136/bmjopen-2012-001118
Freund, W., Weber, F., Billich, C., Birklein, F., Breimhorst, M., and Schuetz, U. H. (2013). Ultra-marathon runners are different: investigations into pain tolerance and personality traits of participants of the TransEurope footrace 2009. Pain Pract. 13, 524–532. doi: 10.1111/papr.12039
Frey, W., Wassmer, P., Frey-Rindova, P., Braun, D., Schwarz, F., Arnold, M., et al. (1994). Muscle pain and biochemical changes after an ultramarathon in cold weather condition-Influence of diclofenac treatment. SPORT Schweiz. Z. Med. Traumatol. 2, 30–36.
Frick, B. (2011). Gender differences in competitive orientations: empirical evidence from ultramarathon running. J. Sports Econom. 12, 317–340. doi: 10.1177/1527002511404784
Frizzell, R. T., Lang, G. H., Lowance, D. C., and Lathan, S. R. (1986). Hyponatremia and ultramarathon running. JAMA J. Am. Med. Assoc. 255, 772–774. doi: 10.1001/jama.1986.03370060086025
George, K. P., Warburton, D. E. R., Oxborough, D., Scott, J. M., Esch, B. T. A., Williams, K., et al. (2011). Upper limits of physiological cardiac adaptation in ultramarathon runners. J. Am. Coll. Cardiol. 57, 754–755. doi: 10.1016/j.jacc.2010.05.070
Gill, S. K., Ana, T., Rama, L., Rosado, F., Hankey, J., Scheer, V., et al. (2015a). Circulatory endotoxin concentration and cytokine profile in response to exertional-heat stress during a multi-stage ultra-marathon competition. Exerc. Immunol. Rev. 21, 114–128.
Gill, S. K., Hankey, J., Wright, A., Marczak, S., Hemming, K., Allerton, D. M., et al. (2015b). The impact of a 24-h ultra-marathon on circulatory endotoxin and cytokine profile. Int. J. Sports Med. 36, 688–695. doi: 10.1055/s-0034-1398535
Gill, S. K., Teixeira, A. M., Rama, L., Rosado, F., Hankey, J., Scheer, V., et al. (2013). Salivary antimicrobial protein responses during multistage ultramarathon competition conducted in hot environmental conditions. Appl. Physiol. Nutr. Metab. 38, 977–987. doi: 10.1139/apnm-2013-0005
Gill, S. K., Teixeira, A. M., Rosado, F., Hankey, J., Wright, A., Marczak, S., et al. (2014). The impact of a 24-H ultra-marathon on salivary antimicrobial protein responses. Int. J. Sports Med. 35, 966–971. doi: 10.1055/s-0033-1358479
Gimenez, P., Kerhervé, H., Messonnier, L. A., Féasson, L., and Millet, G. Y. (2013). Changes in the energy cost of running during a 24-h treadmill exercise. Med. Sci. Sports Exerc. 45, 1807–1813. doi: 10.1249/MSS.0b013e318292c0ec
Glace, B., Murphy, C., and McHugh, M. (2002). Food and fluid intake and disturbances in gastrointestinal and mental function during an ultramarathon. Int. J. Sport Nutr. Exerc. Metab. 12, 414–427.
Hagemann, G. J., Rijke, A. M., and Corr, P. D. (2008). Do knees survive the comrades marathon? South Afr. Med. J. 98, 873–876.
Hattori, N., Hayashi, T., Nakachi, K., Ichikawa, H., Gotoau, C., Tokudome, Y., et al. (2009). Changes of ROS during a two-day ultra-marathon race. Int. J. Sports Med. 30, 426–429. doi: 10.1055/s-0028-1112144
Heapy, A. M., Hoffman, M. D., Verhagen, H. H., Thompson, S. W., Dhamija, P., Sandford, F. J., et al. (2018). A randomized controlled trial of manual therapy and pneumatic compression for recovery from prolonged running-an extended study. Res. Sports Med. 7, 1–11. doi: 10.1080/15438627.2018.1447469
Heneghan, H. M., Nazirawan, F., Dorcaratto, D., Fiore, B., Boylan, J. F., Maguire, D., et al. (2014). Extreme heatstroke causing fulminant hepatic failure requiring liver transplantation: a case report. Transplant. Proc. 46, 2430–2432. doi: 10.1016/j.transproceed.2013.12.055
Hetsroni, I., and Mann, G. (2012). “Ultra-marathon lower limb injuries,” in Sports Injuries: Prevention, Diagnosis, Treatment, and Rehabilitation, ed M. Doral (Berlin; Heidelberg: Springer), 1109–1111.
Hew-Butler, T., Hoffman, M. D., Stuempfle, K. J., Rogers, I. R., Morgenthaler, N. G., and Verbalis, J. G. (2011). Changes in copeptin and bioactive vasopressin in runners with and without hyponatremia. Clin. J. Sport Med. 21, 211–217. doi: 10.1097/JSM.0b013e31821a62c2
Hew-Butler, T., Jordaan, E., Stuempfle, K. J., Speedy, D. B., Siegel, A. J., Noakes, T. D., et al. (2008a). Osmotic and nonosmotic regulation of arginine vasopressin during prolonged endurance exercise. J. Clin. Endocrinol. Metab. 93, 2072–2078. doi: 10.1210/jc.2007-2336
Hew-Butler, T., Noakes, T. D., Soldin, S. J., and Verbalis, J. G. (2008b). Acute changes in endocrine and fluid balance markers during high-intensity, steady-state, and prolonged endurance running: unexpected increases in oxytocin and brain natriuretic peptide during exercise. Eur. J. Endocrinol. 159, 729–737. doi: 10.1530/EJE-08-0064
Hew-Butler, T., Sharwood, K., Boulter, J., Collins, M., Tucker, R., Dugas, J., et al. (2007). Dysnatremia predicts a delayed recovery in collapsed ultramarathon runners. Clin. J. Sport Med. 17, 289–296. doi: 10.1097/JSM.0b013e31804c779b
Hill, R. J., and Davies, P. S. (2001). Energy expenditure during 2 wk of an ultraendurance run around Australia. Med. Sci. Sports Exerc. 33, 148–151.
Hoffman, M. D. (2008). Anthropometric characteristics of ultramarathoners. Int. J. Sports Med. 29, 808–811. doi: 10.1055/s-2008-1038434
Hoffman, M. D. (2010). Performance trends in 161-km ultramarathons. Int. J. Sports Med. 31, 31–37. doi: 10.1055/s-0029-1239561
Hoffman, M. D. (2014). Pacing by winners of a 161-km mountain ultramarathon. Int. J. Sports Physiol. Perform. 9, 1054–1056. doi: 10.1123/ijspp.2013-0556
Hoffman, M. D., and Fogard, K. (2011). Factors related to successful completion of a 161-km ultramarathon. Int. J. Sports Physiol. Perform. 6, 25–37. doi: 10.1123/ijspp.6.1.25
Hoffman, M. D., and Fogard, K. (2012). Demographic characteristics of 161-km ultramarathon runners. Res. Sports Med. 20, 59–69. doi: 10.1080/15438627.2012.634707
Hoffman, M. D., and Krishnan, E. (2013). Exercise behavior of ultramarathon runners: baseline findings from the ultra study. J. Strength Cond. Res. 27, 2939–2945. doi: 10.1519/JSC.0b013e3182a1f261
Hoffman, M. D., and Krishnan, E. (2014). Health and exercise-related medical issues among 1,212 ultramarathon runners: baseline findings from the Ultrarunners Longitudinal TRAcking (ULTRA) Study. PLoS ONE 9:e0083867. doi: 10.1371/journal.pone.0083867
Hoffman, M. D., and Krouse, R. (2018). Ultra-obligatory running among ultramarathon runners. Res. Sports Med. 26, 211–221. doi: 10.1080/15438627.2018.1431533
Hoffman, M. D., and Myers, T. M. (2015). Case study: symptomatic exercise-associated hyponatremia in an endurance runner despite sodium supplementation. Int. J. Sport Nutr. Exerc. Metab. 25, 603–606. doi: 10.1123/ijsnem.2014-0241
Hoffman, M. D., and Stuempfle, K. J. (2014). Hydration strategies, weight change and performance in a 161 km ultramarathon. Res. Sports Med. 22, 213–225. doi: 10.1080/15438627.2014.915838
Hoffman, M. D., and Stuempfle, K. J. (2016a). Does oral buffered sodium supplementation reduce nausea and vomiting during an ultramarathon? Res. Sports Med. 24, 94–103. doi: 10.1080/15438627.2015.1126278
Hoffman, M. D., and Stuempfle, K. J. (2016b). Is sodium supplementation necessary to avoid dehydration during prolonged exercise in the heat? J. Strength Cond. Res. 30, 615–620. doi: 10.1519/JSC.0000000000001138
Hoffman, M. D., and Weiss, R. H. (2016). Does acute kidney injury from an ultramarathon increase the risk for greater subsequent injury? Clin. J. Sport Med. 26, 417–422. doi: 10.1097/JSM.0000000000000277
Hoffman, M. D., Badowski, N., Chin, J., and Stuempfle, K. J. (2016). A randomized controlled trial of massage and pneumatic compression for ultramarathon recovery. J. Orthop. Sports Phys. Ther. 46, 320–326. doi: 10.2519/jospt.2016.6455
Hoffman, M. D., Badowski, N., Chin, J., Stuempfle, K. J., and Parise, C. A. (2017a). Determinants of recovery from a 161-km ultramarathon. J. Sports Sci. 35, 669–677. doi: 10.1080/02640414.2016.1183808
Hoffman, M. D., Chen, L., and Krishnan, E. (2014). Body mass index and its correlates in 1,212 ultramarathon runners: baseline findings from the ultra study. J. Phys. Activity Health 11, 1549–1555. doi: 10.1123/jpah.2013-0056
Hoffman, M. D., Fogard, K., Winger, J., Hew-Butler, T., and Stuempfle, K. J. (2013a). Characteristics of 161-km ultramarathon finishers developing exercise-associated hyponatremia. Res. Sports Med. 21, 164–175. doi: 10.1080/15438627.2012.757230
Hoffman, M. D., Goulet, E. D. B., and Maughan, R. J. (2017b). Considerations in the use of body mass change to estimate change in hydration status during a 161-kilometer ultramarathon running competition. Sports Med. 48, 1–8. doi: 10.1007/s40279-017-0782-3
Hoffman, M. D., Ingwerson, J. L., Rogers, I. R., Hew-Butler, T., and Stuempfle, K. J. (2012a). Increasing creatine kinase concentrations at the 161-km western states endurance run. Wilderness Environ. Med. 23, 56–60. doi: 10.1016/j.wem.2011.11.001
Hoffman, M. D., Lebus, D. K., Ganong, A. C., Casazza, G. A., and Loan, M. V. (2010a). Body composition of 161-km ultramarathoners. Int. J. Sports Med. 31, 106–109. doi: 10.1055/s-0029-1241863
Hoffman, M. D., Lee, J., Zhao, H., and Tsodikov, A. (2007). Pain perception after running a 100-mile ultramarathon. Arch. Phys. Med. Rehabil. 88, 1042–1048. doi: 10.1016/j.apmr.2007.05.004
Hoffman, M. D., Ong, J. C., and Wang, G. (2010b). Historical analysis of participation in 161km ultramarathons in North America. Int. J. Hist. Sport 27, 1877–1891. doi: 10.1080/09523367.2010.494385
Hoffman, M. D., Stuempfle, K. J., Fogard, K., Hew-Butler, T., Winger, J., and Weiss, R. H. (2013b). Urine dipstick analysis for identification of runners susceptible to acute kidney injury following an ultramarathon. J. Sports Sci. 31, 20–31. doi: 10.1080/02640414.2012.720705
Hoffman, M. D., Stuempfle, K. J., Rogers, I. R., Weschler, L. B., and Hew-Butler, T. (2012b). Hyponatremia in the 2009 161-km Western States endurance run. Int. J. Sports Physiol. Perform. 7, 6–10.
Holt, N. L., Lee, H., Kim, Y., and Klein, K. (2014). Exploring experiences of running an ultramarathon. Sport Psychol. 28, 22–35. doi: 10.1123/tsp.2013-0008
Holtzhausen, L. M., and Noakes, T. D. (1995). The prevalence and significance of post-exercise (Postural) hypotension in ultramarathon runners. Med. Sci. Sports Exerc. 27, 1595–1601.
Holtzhausen, L. M., Noakes, T. D., Kroning, B., Klerk, M. D., Roberts, M., and Emsley, R. (1994). Clinical and biochemical characteristics of collapsed ultramarathon runners. Med. Sci. Sports Exerc. 26, 1095–1101.
Hou, S. K., Chiu, Y. H., Tsai, Y. F., Tai, L. C., Hou, P. C., How, C. K., et al. (2015). Clinical impact of speed variability to identify ultramarathon runners at risk for acute kidney injury. PLoS ONE 10:e0133146. doi: 10.1371/journal.pone.0133146
Huang, Y. H., Hsieh, T. Y., Chen, I. C., Lai, C. S., Lin, S. D., Lee, S. S., et al. (2014). Amputation of lower limb for necrotizing soft-tissue infection in an ultramarathon runner. Formos. J. Surg. 47, 62–65. doi: 10.1016/j.fjs.2013.10.003
Hunter, S. K., Stevens, A. A., Magennis, K., Skelton, K. W., and Fauth, M. (2011). Is there a sex difference in the age of elite marathon runners? Med. Sci. Sports Exerc. 43, 656–664. doi: 10.1249/MSS.0b013e3181fb4e00
Hurdiel, R., Pezé, T., Daugherty, J., Girard, J., Poussel, M., Poletti, L., et al. (2015). Combined effects of sleep deprivation and strenuous exercise on cognitive performances during The North Face® Ultra Trail du Mont Blanc® (UTMB®). J. Sports Sci. 33, 670–674. doi: 10.1080/02640414.2014.960883
Hutson, M. A. (1984). Medical implications of ultra marathon running: observations on a six day track race. Br. J. Sports Med. 18, 44–45.
Irving, R. A., Noakes, T. D., Raine, R. I., and Van Zyl Smit, R. (1990). Transient oliguria with renal tubular dysfunction after a 90 km running race. Med. Sci. Sports Exerc. 22, 756–760.
Jampen, S. C., Knechtle, B., Rüst, C. A., Lepers, R., and Rosemann, T. (2013). Increase in finishers and improvement of performance of masters runners in the Marathon des Sables. Int. J. Gen. Med. 6, 427–438. doi: 10.2147/ijgm.s45265
Jastrzębski, Z., Zychowska, M., Jastrzębska, M., Prusik, K., Prusik, K., Kortas, J., et al. (2015a). Changes in blood morphology and chosen biochemical parameters in ultra-marathon runners during a 100-km run in relation to the age and speed of runners. Int. J. Occup. Med. Environ. Health 29, 801–814.
Jastrzębski, Z., Zychowska, M., Radziminski, Ł., Konieczna, A., and Kortas, J. (2015b). Damage to liver and skeletal muscles in marathon runners during a 100 km run with regard to age and running speed. J. Hum. Kinet. 45, 93–102. doi: 10.1515/hukin-2015-0010
Jastrzebski, Z., Zychowska, M., Jastrzebska, M., Prusik, K., Kortas, J., Ratkowski, W., et al. (2016). Changes in blood morphology and chosen biochemical parameters in ultra-marathon runners during a 100-km run in relation to the age and speed of runners. Int. J. Occup. Med. Environ. Health 29, 801–814. doi: 10.13075/ijomeh.1896.00610
Jastrzebski, Z., Zychowska, M., Konieczna, A., Ratkowski, W., and Radziminski, Ł. (2015). Changes in the acid-base balance and lactate concentration in the blood in amateur ultramarathon runners during a 100-km run. Biol. Sport 32, 261–265. doi: 10.5604/20831862.1163372
Jee, H., and Jin, Y. (2012). Effects of prolonged endurance exercise on vascular endothelial and inflammation markers. J. Sports Sci. Med. 11, 719–726.
Jee, H., Park, J., Oh, J. G., Lee, Y. H., Shin, K. A., and Kim, Y. J. (2013). Effect of a prolonged endurance marathon on vascular endothelial and inflammation markers in runners with exercise-induced hypertension. Am. J. Phys. Med. Rehabil. 92, 513–522. doi: 10.1097/PHM.0b013e31829232db
Jeukendrup, A. E. (2017). Training the gut for athletes. Sports Med. 47, 101–110. doi: 10.1007/s40279-017-0690-6
Joslin, J., Mularella, J., Bail, A., Wojcik, S., and Cooney, D. R. (2015). Mandatory rest stops improve athlete safety during event medical coverage for ultramarathons. Prehosp. Disaster Med. 31, 43–45. doi: 10.1017/S1049023X15005555
Kallmeyer, J. C., and Miller, N. M. (1993). Urinary changes in ultra long-distance marathon runners. Nephron 64, 119–121.
Kaminsky, L. A., and Paul, G. L. (1991). Fluid intake during an ultramarathon running race: relationship to plasma volume and serum sodium and potassium. J. Sports Med. Phys. Fit. 31, 417–419.
Kaminsky, L. A., Kanter, M. M., Nequin, N. D., Lesmes, G. R., and Laham-Saeger, J. (1988). Lipids and lipoproteins after an ultramarathon road race. Ann. Sports Med. 4, 41–44.
Kaminsky, L. A., Nequin, N. D., Lesmes, G. R., La Ham-Saeger, J., Schaffer, W., and Runke, J. A. (1989). Cholesterol, lipoproteins, and triglyceride before, during, and after an ultramarathon road race. J. Cardiopulm. Rehabil. 9, 263–267.
Kanter, M. M., Kaminsky, L. A., and Laham-Saeger, J. (1986). Serum enzyme levels and lipid peroxidation in ultramarathon runners. Ann. Sports Med. 3, 39–41.
Kao, W. F., Hou, S. K., Chiu, Y. H., Chou, S. L., Kuo, F. C., Wang, S. H., et al. (2015). Effects of 100-km ultramarathon on acute kidney injury. Clin. J. Sport Med. 25, 49–54. doi: 10.1097/JSM.0000000000000116
Kao, W. F., Shyu, C. L., Yang, X. W., Hsu, T. F., Chen, J. J., Kao, W. C., et al. (2008). Athletic performance and serial weight changes during 12- and 24-hour ultra-marathons. Clin. J. Sport Med. 18, 155–158. doi: 10.1097/JSM.0b013e31815cdd37
Kasprowicz, K., Ziemann, E., Ratkowski, W., Laskowski, R., Kaczor, J. J., Dadci, R., et al. (2013). Running a 100-km ultra-marathon induces an inflammatory response but does not raise the level of the plasma iron-regulatory protein hepcidin. J. Sports Med. Phys. Fit. 53, 533–537.
Kerhervé, H. A., Millet, G. Y., and Solomon, C. (2015). The dynamics of speed selection and psycho-physiological load during a mountain ultramarathon. PLoS ONE 10:e0145482. doi: 10.1371/journal.pone.0145482
Kerschan-Schindl, K., Thalmann, M., Sodeck, G. H., Skenderi, K., Matalas, A. L., Grampp, S., et al. (2009). A 246-km continuous running race causes significant changes in bone metabolism. Bone 45, 1079–1083. doi: 10.1016/j.bone.2009.07.088
Khodaee, M., Spittler, J., Vanbaak, K., Changstrom, B. G., and Hill, J. C. (2015). Effects of running an ultramarathon on cardiac, hematologic, and metabolic biomarkers. Int. J. Sports Med. 36, 867–871. doi: 10.1055/s-0035-1550045
Kim, H. J., Lee, Y. H., and Kim, C. K. (2007). Biomarkers of muscle and cartilage damage and inflammation during a 200 km run. Eur. J. Appl. Physiol. 99, 443–447. doi: 10.1007/s00421-006-0362-y
Kim, H. J., Lee, Y. H., and Kim, C. K. (2009). Changes in serum cartilage oligomeric matrix protein (COMP), plasma CPK and plasma hs-CRP in relation to running distance in a marathon (42.195 km) and an ultra-marathon (200 km) race. Eur. J. Appl. Physiol. 105, 765–770. doi: 10.1007/s00421-008-0961-x
Kim, Y. J., Shin, Y. O., Lee, J. B., Lee, Y. H., Shin, K. A., Kim, A. C., et al. (2014). The effects of running a 308 km ultra-marathon on cardiac markers. Eur. J. Sport Sci. 14(Suppl.1), S92–S97. doi: 10.1080/17461391.2011.654267
Kłapcinska, B., Waåkiewicz, Z., Chrapusta, S. J., Sadowska-Krępa, E., Czuba, M., and Langfort, J. (2013). Metabolic responses to a 48-h ultra-marathon run in middle-aged male amateur runners. Eur. J. Appl. Physiol. 113, 2781–2793. doi: 10.1007/s00421-013-2714-8
Kluitenberg, B., van Middelkoop, M., Diercks, R., and van der Worp, H. (2015). What are the differences in injury proportions between different populations of runners? A systematic review and meta-analysis. Sports Med. 45, 1143–1161. doi: 10.1007/s40279-015-0331-x
Knechtle, B. (2012). Ultramarathon runners: nature or nurture? Int. J. Sports Physiol. Perform. 7, 310–312. doi: 10.1123/ijspp.7.4.310
Knechtle, B., and Nikolaidis, P. T. (2017). The age of the best ultramarathon performance–the case of the “Comrades Marathon”. Res. Sports Med. 25, 132–143. doi: 10.1080/15438627.2017.1282357
Knechtle, B., Aschmann, A., Onywera, V., Nikolaidis, P. T., Rosemann, T., and Rust, C. A. (2016a). Performance and age of African and non-African runners in World Marathon Majors races 2000-2014. J. Sports Sci. 35, 1012–1024. doi: 10.1080/02640414.2016.1209302
Knechtle, B., Assadi, H., Lepers, R., Rosemann, T., and Rust, C. A. (2014a). Relationship between age and elite marathon race time in world single age records from 5 to 93 years. BMC Sports Sci. Med. Rehabil. 6:31. doi: 10.1186/2052-1847-6-31
Knechtle, B., Duff, B., Schulze, I., and Kohler, G. (2008a). The effects of running 1,200 km within 17 days on body composition in a female ultrarunner-Deutschlandlauf 2007. Res. Sports Med. 16, 167–188. doi: 10.1080/15438620802104120
Knechtle, B., Knechtle, P., and Rosemann, T. (2010a). Race performance in male mountain ultra-marathoners: anthropometry or training? Percept. Mot. Skills 110, 721–735. doi: 10.2466/pms.110.3.721-735
Knechtle, B., Knechtle, P., Mrazek, C., Senn, O., Rosemann, T., Imoberdorf, R., et al. (2011a). No effect of short-term amino acid supplementation on variables related to skeletal muscle damage in 100 km ultra-runners - a randomized controlled trial. J. Int. Soc. Sports Nutr. 8:6. doi: 10.1186/1550-2783-8-6
Knechtle, B., Knechtle, P., and Rosemann, T. (2011b). Do male 100-km ultra-marathoners overdrink? Int. J. Sports Physiol. Perform. 6, 195–207.
Knechtle, B., Knechtle, P., Rosemann, T., and Lepers, R. (2010b). Predictor variables for a 100-km race time in male ultra-marathoners. Percept. Mot. Skills 111, 681–693. doi: 10.2466/05.25.pms.111.6.681-693
Knechtle, B., Knechtle, P., Rosemann, T., and Lepers, R. (2011c). Personal best marathon time and longest training run, not anthropometry, predict performance in recreational 24-hour ultrarunners. J. Strength Cond. Res. 25, 2212–2218. doi: 10.1519/JSC.0b013e3181f6b0c7
Knechtle, B., Knechtle, P., Rosemann, T., and Senn, O. (2011d). What is associated with race performance in male 100-km ultra-marathoners anthropometry, training or marathon best time? J. Sports Sci. 29, 571–577. doi: 10.1080/02640414.2010.541272
Knechtle, B., Knechtle, P., Rust, C. A., and Rosemann, T. (2011e). Leg skinfold thicknesses and race performance in male 24-hour ultra-marathoners. Proc. (Bayl. Univ. Med. Cent). 24, 110–114.
Knechtle, B., Mrazek, C., Wirth, A., Knechtle, P., Rüst, C. A., Senn, O., et al. (2012a). Branched-chain amino acid supplementation during a 100-km ultra-marathon-A randomized controlled trial. J. Nutr. Sci. Vitaminol. 58, 36–44. doi: 10.3177/jnsv.58.36
Knechtle, B., Knechtle, P., Rust, C. A., Gnadinger, M., Imoberdorf, R., Kohler, G., et al. (2012b). Regulation of electrolyte and fluid metabolism in multi-stage ultra-marathoners. Horm. Metab. Res. 44, 919–926. doi: 10.1055/s-0032-1312647
Knechtle, B., Rüst, C. A., Knechtle, P., and Rosemann, T. (2012c). Does muscle mass affect running times in male long-distance master runners? Asian J. Sports Med. 3, 247–256.
Knechtle, B., Knechtle, P., Schulze, I., and Kohler, G. (2008b). Upper arm circumference is associated with race performance in ultra-endurance runners. Br. J. Sports Med. 42, 295–299; discussion 299. doi: 10.1136/bjsm.2007.038570
Knechtle, B., Rüst, C. A., Rosemann, T., and Lepers, R. (2012d). Age-related changes in 100-km ultra-marathon running performance. Age 34, 1033–1045. doi: 10.1007/s11357-011-9290-9
Knechtle, B., Knechtle, P., Wirth, A., Alexander Rüst, C., and Rosemann, T. (2012e). A faster running speed is associated with a greater body weight loss in 100-km ultra-marathoners. J. Sports Sci. 30, 1131–1140. doi: 10.1080/02640414.2012.692479
Knechtle, B., Senn, O., Imoberdorf, R., Joleska, I., Wirth, A., Knechtle, P., et al. (2011f). No fluid overload in male ultra-runners during a 100 km ultra-run. Res. Sports Med. 19, 14–27. doi: 10.1080/15438627.2010.510039
Knechtle, B., Valeri, F., Nikolaidis, P. T., Zingg, M. A., Rosemann, T., and Rüst, C. A. (2016b). Do women reduce the gap to men in ultra-marathon running? Springerplus 5:672. doi: 10.1186/s40064-016-2326-y
Knechtle, B., Valeri, F., Zingg, M. A., Rosemann, T., and Rüst, C. A. (2014b). What is the age for the fastest ultra-marathon performance in time-limited races from 6 h to 10 days? Age (Dordr) 36, 9715. doi: 10.1007/s11357-014-9715-3
Knechtle, B., Wirth, A., Knechtle, P., Rosemann, T., and Senn, O. (2011g). Do ultra-runners in a 24-h run really dehydrate? Ir. J. Med. Sci. 180, 129–134. doi: 10.1007/s11845-010-0500-8
Knechtle, B., Wirth, A., Knechtle, P., Zimmermann, K., and Kohler, G. (2009). Personal best marathon performance is associated with performance in a 24-h run and not anthropometry or training volume. Br. J. Sports Med. 43, 836–839. doi: 10.1136/bjsm.2007.045716
Knoth, C., Knechtle, B., Rüst, C. A., Rosemann, T., and Lepers, R. (2012). Participation and performance trends in multistage ultramarathons-the ‘Marathon des Sables’ 2003-2012. Extr. Physiol. Med. 1:13. doi: 10.1186/2046-7648-1-13
Koller, A., Mair, J., Schobersberger, W., Wohlfarter, T., Haid, C., Mayr, M., et al. (1998). Effects of prolonged strenuous endurance exercise on plasma myosin heavy chain fragments and other muscular proteins. Cycling vs running. J. Sports Med. Phys. Fit. 38, 10–17.
Krabak, B. J., Lipman, G. S., Waite, B. L., and Rundell, S. D. (2017). Exercise-associated hyponatremia, hypernatremia, and hydration status in multistage ultramarathons. Wilderness Environ. Med. 28, 291–298. doi: 10.1016/j.wem.2017.05.008
Krabak, B. J., Waite, B., and Schiff, M. A. (2011). Study of injury and illness rates in multiday ultramarathon runners. Med. Sci. Sports Exerc. 43, 2314–2320. doi: 10.1249/MSS.0b013e318221bfe3
Krouse, R. Z., Ransdell, L. B., Lucas, S. M., and Pritchard, M. E. (2011). Motivation, goal orientation, coaching, and training habits of women ultrarunners. J. Strength Cond. Res. 25, 2835–2842. doi: 10.1519/JSC.0b013e318207e964
Kruger, M., and Saayman, M. (2013). Who are the comrades of the comrades marathon? South Afr. J. Res. Sport Phys. Educ. Recreation 35, 71–92.
Krzeminski, K., Buraczewska, M., Miśkiewicz, Z., Dabrowski, J., Steczkowska, M., Kozacz, A., et al. (2016). Effect of ultra-endurance exercise on left ventricular performance and plasma cytokines in healthy trained men. Biol. Sport 33, 63–69. doi: 10.5604/20831862.1189767
Kupchak, B. R., Kraemer, W. J., Hoffman, M. D., Phinney, S. D., and Volek, J. S. (2014). The impact of an ultramarathon on hormonal and biochemical parameters in men. Wilderness Environ. Med. 25, 278–288. doi: 10.1016/j.wem.2014.03.013
Kupchak, B. R., Volk, B. M., Kunces, L. J., Kraemer, W. J., Hoffman, M. D., Phinney, S. D., et al. (2013). Alterations in coagulatory and fibrinolytic systems following an ultra-marathon. Eur. J. Appl. Physiol. 113, 2705–2712. doi: 10.1007/s00421-013-2709-5
Lambert, M. I., Dugas, J. P., Kirkman, M. C., Mokone, G. G., and Waldeck, M. R. (2004). Changes in running speeds in a 100 km ultramarathon race. J. Sports Sci. Med. 3, 167–173.
Landman, Z. C., Landman, G. O., and Fatehi, P. (2012). Physiologic alterations and predictors of performance in a 160-km ultramarathon. Clin. J. Sport Med. 22, 146–151. doi: 10.1097/JSM.0b013e318243ffdc
Landt, M., Lawson, G. M., Helgeson, J. M., Davila-Roman, V. G., Ladenson, J. H., Jaffe, A. S., et al. (1997). Prolonged exercise decreases serum leptin concentrations. Metab. Clin. Exp. 46, 1109–1112. doi: 10.1016/S0026-0495(97)90200-6
Lara, B., Salinero, J. J., and Del Coso, J. (2014). The relationship between age and running time in elite marathoners is U-shaped. Age (Dordr) 36, 1003–1008. doi: 10.1007/s11357-013-9614-z
Lathan, S. R., and Cantwell, J. D. (1981). A run for the record: studies on a Trans-American ultramarathoner. JAMA 245, 367–368. doi: 10.1001/jama.1981.03310290035019
Lebus, D. K., Casazza, G. A., Hoffman, M. D., and Van Loan, M. D. (2010). Can changes in body mass and total body water accurately predict hyponatremia after a 161-km running race? Clin. J. Sport Med. 20, 193–199. doi: 10.1097/JSM.0b013e3181da53ea
Lee, J. K. W., Nio, A. Q. X., Ang, W. H., Johnson, C., Aziz, A. R., Lim, C. L., et al. (2011). First reported cases of exercise-associated hyponatremia in Asia. Int. J. Sports Med. 32, 297–302. doi: 10.1055/s-0030-1269929
Lipman, G. S., Krabak, B. J., Rundell, S. D., Shea, K. M., Badowski, N., and Little, C. (2016). Incidence and prevalence of acute kidney injury during multistage ultramarathons. Clin. J. Sport Med. 26, 314–319. doi: 10.1097/JSM.0000000000000253
Lipman, G. S., Krabak, B. J., Waite, B. L., Logan, S. B., Menon, A., and Chan, G. K. (2014). A prospective cohort study of acute kidney injury in multi-stage ultramarathon runners: the biochemistry in endurance runner study (BIERS). Res. Sports Med. 22, 185–192. doi: 10.1080/15438627.2014.881824
Lipman, G. S., Shea, K., Christensen, M., Phillips, C., Burns, P., Higbee, R., et al. (2017). Ibuprofen versus placebo effect on acute kidney injury in ultramarathons: a randomised controlled trial. Emerg. Med. J. 34, 637–642. doi: 10.1136/emermed-2016-206353
Lippi, G., Sanchis-Gomar, F., Salvagno, G. L., Aloe, R., Schena, F., and Guidi, G. C. (2012a). Variation of serum and urinary neutrophil gelatinase associated lipocalin (NGAL) after Strenuous physical exercise. Clin. Chem. Lab. Med. 50, 1585–1589. doi: 10.1515/cclm-2011-0954
Lippi, G., Schena, F., Salvagno, G. L., Aloe, R., Banfi, G., and Guidi, G. C. (2012b). Foot-strike haemolysis after a 60-km ultramarathon. Blood Transfusion 10, 377–383. doi: 10.2450/2012.0167-11
Lippi, G., Schena, F., Salvagno, G. L., Sanchis-Gomar, F., and Guidi, G. C. (2015). Serum copeptin and midregion proadrenomedullin (MR-proADM) after an ultramarathon. J. Clin. Lab. Anal. 29, 15–20. doi: 10.1002/jcla.21720
Liu, C. H., Tseng, Y. F., Lai, J. I., Chen, Y. Q., Wang, S. H., Kao, W. F., et al. (2018). The changes of red blood cell viscoelasticity and sports anemia in male 24-hr ultra-marathoners. J. Chin. Med. Assoc. 81, 475–481. doi: 10.1016/j.jcma.2017.09.011
Longman, D. P., Prall, S. P., Shattuck, E. C., Stephen, I. D., Stock, J. T., Wells, J. C. K., et al. (2018). Short-term resource allocation during extensive athletic competition. Am. J. Hum. Biol. 30:e23052. doi: 10.1002/ajhb.23052
Lopes, A. D., Hespanhol, L. C., Yeung, S. S., and Costa, L. O. P. (2012). What are the main running-related musculoskeletal injuries? A systematic review. Sports Med. 42, 891–905. doi: 10.2165/11631170-000000000-00000
Lord, R., George, K., Somauroo, J., Jain, N., Reese, K., Hoffman, M. D., et al. (2016a). Exploratory insights from the right-sided electrocardiogram following prolonged endurance exercise. Eur. J. Sport Sci. 16, 1014–1022. doi: 10.1080/17461391.2016.1165292
Lord, R., George, K., Somauroo, J., Stembridge, M., Jain, N., Hoffman, M. D., et al. (2016b). Alterations in cardiac mechanics following ultra-endurance exercise: insights from left and right ventricular area-deformation loops. J. Am. Soc. Echocardiogr. 29, 879.e871–887.e871. doi: 10.1016/j.echo.2016.05.004
Lord, R., Somauroo, J., Stembridge, M., Jain, N., Hoffman, M. D., George, K., et al. (2015). The right ventricle following ultra-endurance exercise: insights from novel echocardiography and 12-lead electrocardiography. Eur. J. Appl. Physiol. 115, 71–80. doi: 10.1007/s00421-014-2995-6
Machefer, G., Groussard, C., Zouhal, H., Vincent, S., Youssef, H., Faure, H., et al. (2007). Nutritional and plasmatic antioxidant vitamins status of ultra endurance athletes. J. Am. Coll. Nutr. 26, 311–316. doi: 10.1080/07315724.2007.10719616
Magrini, D., Khodaee, M., San-Millan, I., Hew-Butler, T., and Provance, A. J. (2017). Serum creatine kinase elevations in ultramarathon runners at high altitude. Phys. Sportsmed. 45, 129–133. doi: 10.1080/00913847.2017.1280371
Martinez, S., Aguilo, A., Rodas, L., Lozano, L., Moreno, C., and Tauler, P. (2017). Energy, macronutrient and water intake during a mountain ultramarathon event: the influence of distance. J. Sports Sci. 36, 333–339. doi: 10.1080/02640414.2017.1306092
Mastaloudis, A., Morrow, J. D., Hopkins, D. W., Devaraj, S., and Traber, M. G. (2004a). Antioxidant supplementation prevents exercise-induced lipid peroxidation, but not inflammation, in ultramarathon runners. Free Radic. Biol. Med. 36, 1329–1341. doi: 10.1016/j.freeradbiomed.2004.02.069
Mastaloudis, A., Traber, M. G., Carstensen, K., and Widrick, J. J. (2006). Antioxidants did not prevent muscle damage in response to an ultramarathon run. Med. Sci. Sports Exerc. 38, 72–80. doi: 10.1249/01.mss.0000188579.36272.f6
Mastaloudis, A., Yu, T. W., O'Donnell, R. P., Frei, B., Dashwood, R. H., and Traber, M. G. (2004b). Endurance exercise results in DNA damage as detected by the comet assay. Free Radic. Biol. Med. 36, 966–975. doi: 10.1016/j.freeradbiomed.2004.01.012
Matin, P., Lang, G., Carretta, R., and Simon, G. (1983). Scintigraphic evaluation of muscle damage following extreme exercise: concise communication. J. Nucl. Med. 24, 308–311.
Maufrais, C., Millet, G. P., Schuster, I., Rupp, T., and Nottin, S. (2016). Progressive and biphasic cardiac responses during extreme mountain ultramarathon. Am. J. Physiol. - Heart Circ. Physiol. 310, H1340–H1348. doi: 10.1152/ajpheart.00037.2016
McCormick, A., Meijen, C., and Marcora, S. (2015). Psychological determinants of whole-body endurance performance. Sports Med. 45, 997–1015. doi: 10.1007/s40279-015-0319-6
McCubbin, A. J., Cox, G. R., and Broad, E. M. (2016). Case study: nutrition planning and intake for marathon des sables-a series of five runners. Int. J. Sport Nutr. Exerc. Metab. 26, 581–587. doi: 10.1123/ijsnem.2016-0016
McGreal, K., Budhiraja, P., Jain, N., and Yu, A. S. (2016). Current challenges in the evaluation and management of hyponatremia. Kidney Dis (Basel) 2, 56–63. doi: 10.1159/000446267
McKechnie, J. K., Leary, W. P., and Noakes, T. D. (1982). Metabolic responses to a 90 km running race. South Afr. Med. J. 61, 482–484.
McKune, A. J., Smith, L. L., Semple, S. J., and Wadee, A. A. (2005). Influence of ultra-endurance exercise on immunoglobulin isotypes and subclasses. Br. J. Sports Med. 39, 665–670. doi: 10.1136/bjsm.2004.017194
Micklesfield, L. K., Lambert, E. V., Fataar, A. B., Noakes, T. D., and Myburgh, K. H. (1995). Bone mineral density in mature, premenopausal ultramarathon runners. Med. Sci. Sports Exerc. 27, 688–696.
Micklewright, D., Parry, D., Robinson, T., Deacon, G., Renfree, A., Gibson, A. S. C., et al. (2015). Risk perception influences athletic pacing strategy. Med. Sci. Sports Exerc. 47, 1026–1037. doi: 10.1249/MSS.0000000000000500
Millet, G. Y. (2011). Can neuromuscular fatigue explain running strategies and performance in ultra-marathons?: the flush model. Sports Med. 41, 489–506. doi: 10.2165/11588760-000000000-00000
Moran, S. T., Dziedzic, C. E., and Cox, G. R. (2011). Feeding strategies of a female athlete during an ultraendurance running event. Int. J. Sport Nutr. Exerc. Metab. 21, 347–351. doi: 10.1123/ijsnem.21.4.347
Mrakic-Sposta, S., Gussoni, M., Moretti, S., Pratali, L., Giardini, G., Tacchini, P., et al. (2015). Effects of mountain ultra-marathon running on ROS production and oxidative damage by micro-invasive analytic techniques. PLoS ONE 10:e0141780. doi: 10.1371/journal.pone.0141780
Mündermann, A., Klenk, C., Billich, C., Nüesch, C., Pagenstert, G., Schmidt-Trucksäss, A., et al. (2017). Changes in cartilage biomarker levels during a transcontinental multistage footrace over 4486 km. Am. J. Sports Med. 45, 2630–2636. doi: 10.1177/0363546517712945
Musha, H., Nagashima, J., Awaya, T., Oomiya, K., Takada, H., and Murayama, M. (1997). Myocardial injury in a 100-KM ultramarathon. Curr. Ther. Res. Clin. Exp. 58, 587–593. doi: 10.1016/S0011-393X(97)80085-9
Nagashima, J., Musha, H., Takada, H., and Murayama, M. (2003). New upper limit of physiologic cardiac hypertrophy in japanese participants in the 100-km ultramarathon. J. Am. Coll. Cardiol. 42, 1617–1623. doi: 10.1016/j.jacc.2003.06.005
Nagashima, J., Musha, H., Takada, H., and Murayama, M. (2006). Left ventricular chamber size predicts the race time of Japanese participants in a 100 km ultramarathon. Br. J. Sports Med. 40, 331–333. doi: 10.1136/bjsm.2005.022673
Nagel, D., Seiler, D., Franz, H., and Jung, K. (1990). Ultra-long-distance running and the liver. Int. J. Sports Med. 11, 441–445. doi: 10.1055/s-2007-1024834
Newmark, S. R., Toppo, F. R., and Adams, G. (1991). Fluid and electrolyte replacement in the ultramarathon runner. Am. J. Sports Med. 19, 389–391. doi: 10.1177/036354659101900412
Nieman, D. C., and Nehlsen-Cannarella, S. L. (1991). The effects of acute and chronic exercise on immunoglobulins. Sports Med. 11, 183–201. doi: 10.2165/00007256-199111030-00003
Nieman, D. C., Dumke, C. I., Henson, D. A., McAnulty, S. R., McAnulty, L. S., Lind, R. H., et al. (2003). Immune and oxidative changes during and following the Western States Endurance Run. Int. J. Sports Med. 24, 541–547. doi: 10.1055/s-2003-42018
Nieman, D. C., Henson, D. A., Dumke, C. L., Oley, K., McAnulty, S. R., Davis, J. M., et al. (2006). Ibuprofen use, endotoxemia, inflammation, and plasma cytokines during ultramarathon competition. Brain Behav. Immun. 20, 578–584. doi: 10.1016/j.bbi.2006.02.001
Nieman, D. C., Henson, D. A., McAnulty, S. R., McAnulty, L., Swick, N. S., Utter, A. C., et al. (2002). Influence of vitamin C supplementation on oxidative and immune changes after an ultramarathon. J. Appl. Physiol. 92, 1970–1977. doi: 10.1152/japplphysiol.00961.2001
Nieman, D. C., Peters, E. M., Henson, D. A., Nevines, E. I., and Thompson, M. M. (2000). Influence of vitamin C supplementation on cytokine changes following an ultramarathon. J. Interferon Cytokine Res. 20, 1029–1035. doi: 10.1089/10799900050198480
Niemela, K. O., Palatsi, I. J., and Ikaheimo, M. J. (1984). Evidence of impaired left ventricular performance after an uninterrupted competitive 24 hour run. Circulation 70, 350–356.
Nikolaidis, P. T., and Knechtle, B. (2018a). Age of peak performance in 50-km ultramarathoners - is it older than in marathoners? Open Access. J. Sports Med. 9, 37–45. doi: 10.2147/oajsm.s154816
Nikolaidis, P. T., and Knechtle, B. (2018b). Performance in 100-km ultra-marathoners-At which age it reaches its peak? J. Strength Cond. Res. doi: 10.1519/jsc.0000000000002539. [Epub ahead of print].
Nikolaidis, P. T., Onywera, V. O., and Knechtle, B. (2016). Running performance, nationality, sex and age in 10km, half-marathon, marathon and 100km ultra-marathon IAAF 1999-2015. J. Strength Cond. Res. 31, 2189–2207. doi: 10.1519/jsc.0000000000001687
Noakes, T. D. (2008). Water intoxication - Considerations for patients, athletes and physicians. Pract. Gastroenterol. 32, 46–53.
Noakes, T. D., and Carter, J. W. (1982). The responses of plasma biochemical parameters to a 56-km race in novice and experienced ultra-marathon runners. Eur. J. Appl. Physiol. Occup. Physiol. 49, 179–186. doi: 10.1007/bf02334066
Noakes, T. D., Kotzenberg, G., McArthur, P. S., and Dykman, J. (1983). Elevated serum creatine kinase MB and creatine kinase BB-isoenzyme fractions after ultra-marathon running. Eur. J. Appl. Physiol. Occup. Physiol. 52, 75–79. doi: 10.1007/BF00429029
Noakes, T. D., Lambert, E. V., Lambert, M. I., McArthur, P. S., Myburgh, K. H., and Benade, A. J. S. (1988). Carbohydrate ingestion and muscle glycogen depletion during marathon and ultramarathon racing. Eur. J. Appl. Physiol. Occup. Physiol. 57, 482–489. doi: 10.1007/BF00417997
Noakes, T. D., Norman, R. J., Buck, R. H., Godlonton, J., Stevenson, K., and Pittaway, D. (1990). The incidence of hyponatremia during prolonged ultraendurance exercise. Med. Sci. Sports Exerc. 22, 165–170.
O'Hara, W. J., Allen, C., Shephard, R. J., and Gill, J. W. (1977). LaTulippe–a case study of a one hundred and sixty kilometre runner. Br. J. Sports Med. 11, 83–87.
Ohba, H., Takada, H., Musha, H., Nagashima, J., Mori, N., Awaya, T., et al. (2001). Effects of prolonged strenuous exercise on plasma levels of atrial natriuretic peptide and brain natriuretic peptide in healthy men. Am. Heart J. 141, 751–758. doi: 10.1067/mhj.2001.114371
Oxborough, D., Shave, R., Warburton, D., Williams, K., Oxborough, A., Charlesworth, S., et al. (2011). Dilatation and dysfunction of the right ventricle immediately after ultraendurance exercise: exploratory insights from conventional two-dimensional and speckle tracking echocardiography. Circulation 4, 253–263. doi: 10.1161/CIRCIMAGING.110.961938
Parise, C. A., and Hoffman, M. D. (2011). Influence of temperature and performance level on pacing a 161 km trail ultramarathon. Int. J. Sports Physiol. Perform. 6, 243–251. doi: 10.1123/ijspp.6.2.243
Passaglia, D. G., Emed, L. G. M., Barberato, S. H., Guerios, S. T., Moser, A. I., Silva, M. M. F., et al. (2013). Acute effects of prolonged physical exercise: evaluation after a twenty-four-hour ultramarathon. Arq. Bras. Cardiol. 100, 21–28. doi: 10.1590/s0066-782x2012005000118
Pearce, E. A., Myers, T. M., and Hoffman, M. D. (2015). Three cases of severe hyponatremia during a river run in Grand Canyon National Park. Wilderness Environ. Med. 26, 189–195. doi: 10.1016/j.wem.2014.08.007
Pestell, R. G., Hurley, D. M., and Vandongen, R. (1989). BIOCHEMICAL AND HORMONAL CHANGES DURING A 1000 km ULTRAMARATHON. Clin. Exp. Pharmacol. Physiol. 16, 353–361. doi: 10.1111/j.1440-1681.1989.tb01571.x
Pestell, R. G., Ward, G. M., Galvin, P., Best, J. D., and Alford, F. P. (1993). Impaired glucose tolerance after endurance exercise is associated with reduced insulin secretion rather than altered insulin sensitivity. Metab. Clin. Exp. 42, 277–282. doi: 10.1016/0026-0495(93)90074-X
Peter, L., Rüst, C. A., Knechtle, B., Rosemann, T., and Lepers, R. (2014). Sex differences in 24-hour ultra-marathon performance - A retrospective data analysis from 1977 to 2012. Clinics 69, 38–46. doi: 10.6061/clinics/2014(01)06
Peters, E. M. (1997). Exercise, immunology and upper respiratory tract infections. Int. J. Sports Med. Suppl. 18, S69–S77.
Peters, E. M., and Bateman, E. D. (1983). Ultramarathon running and upper respiratory tract infections. An epidemiological survey. South Afr. Med. J. 64, 582–584.
Peters, E. M., Anderson, R., and Theron, A. J. (2001a). Attenuation of increase in circulating cortisol and enhancement of the acute phase protein response in vitamin C-supplemented ultramarathoners. Int. J. Sports Med. 22, 120–126. doi: 10.1055/s-2001-11364
Peters, E. M., Anderson, R., Nieman, D. C., Fickl, H., and Jogessar, V. (2001b). Vitamin C supplementation attenuates the increases in circulating cortisol, adrenaline and anti-inflammatory polypeptides following ultramarathon running. Int. J. Sports Med. 22, 537–543. doi: 10.1055/s-2001-17610
Peters, E. M., Goetzsche, J. M., Grobbelaar, B., and Noakes, T. D. (1993). Vitamin C supplementation reduces the incidence of postrace symptoms of upper-respiratory-tract infection in ultramarathon runners. Am. J. Clin. Nutr. 57, 170–174.
Peters, E. M., Robson, P. J., Kleinveldt, N. C., Naicker, V. L., and Jogessar, V. D. (2004). Hematological recovery in male ultramarathon runners: The effect of variations in training load and running time. J. Sports Med. Phys. Fit. 44, 315–321.
Peters, E. M., Shaik, J., and Kleinveldt, N. (2010). Upper respiratory tract infection symptoms in ultramarathon runners not related to immunoglobulin status. Clin. J. Sport Med. 20, 39–46. doi: 10.1097/JSM.0b013e3181cb4086
Poussel, M., Laroppe, J., Hurdiel, R., Girard, J., Poletti, L., Thil, C., et al. (2015). Sleep management strategy and performance in an extreme mountain ultra-marathon. Res. Sports Med. 23, 330–336. doi: 10.1080/15438627.2015.1040916
Rae, D. E., Bosch, A. N., Collins, M., and Lambert, M. I. (2005). The interaction of aging and 10 years of racing on ultraendurance running performance. J. Aging Phys. Act. 13, 210–222. doi: 10.1123/japa.13.2.210
Rae, D. E., Knobel, G. J., Mann, T., Swart, J., Tucker, R., and Noakes, T. D. (2008). Heatstroke during endurance exercise: is there evidence for excessive endothermy? Med. Sci. Sports Exerc. 40, 1193–1204. doi: 10.1249/MSS.0b013e31816a7155
Rehrer, N. J., Brouns, F., Beckers, E. J., Frey, W. O., Villiger, B., Riddoch, C. J., et al. (1992). Physiological changes and gastro-intestinal symptoms as a result of ultra-endurance running. Eur. J. Appl. Physiol. Occup. Physiol. 64, 1–8.
Reid, S. A., and King, M. J. (2007). Serum biochemistry and morbidity among runners presenting for medical care after an australian mountain ultramarathon. Clin. J. Sport Med. 17, 307–310. doi: 10.1097/JSM.0b013e31804c77da
Renfree, A., Crivoi do Carmo, E., and Martin, L. (2016). The influence of performance level, age and gender on pacing strategy during a 100-km ultramarathon. Eur. J. Sport Sci. 16, 409–415. doi: 10.1080/17461391.2015.1041061
Robach, P., Boisson, R. C., Vincent, L., Lundby, C., Moutereau, S., Gergelé, L., et al. (2014). Hemolysis induced by an extreme mountain ultra-marathon is not associated with a decrease in total red blood cell volume. Scand. J. Med. Sci. Sports 24, 18–27. doi: 10.1111/j.1600-0838.2012.01481.x
Rogers, I. R., Hook, G., Stuempfle, K. J., Hoffman, M. D., and Hew-Butler, T. (2011). An intervention study of oral versus intravenous hypertonic saline administration in ultramarathon runners with exercise-associated hyponatremia: a preliminary randomized trial. Clin. J. Sport Med. 21, 200–203. doi: 10.1097/JSM.0b013e31821a6450
Romer, T., Rüst, C. A., Zingg, M. A., Rosemann, T., and Knechtle, B. (2014). Age and ultra-marathon performance - 50 to 1,000 km distances from 1969–2012. Springerplus 3:693. doi: 10.1186/2193-1801-3-693
Roth, H. J., Leithauser, R. M., Doppelmayr, H., Doppelmayr, M., Finkernagel, H., von Duvillard, S. P., et al. (2007). Cardiospecificity of the 3rd generation cardiac troponin T assay during and after a 216 km ultra-endurance marathon run in Death Valley. Clin. Res. Cardiol. 96, 359–364. doi: 10.1007/s00392-007-0509-9
Rothwell, O., George, K., Somauroo, J., Lord, R., Stembridge, M., Shave, R., et al. (2018). Right ventricular structure and function in the veteran ultramarathon runner: is there evidence for chronic maladaptation? J. Am. Soc. Echocardiogr. 31, 598.e1–605.e1. doi: 10.1016/j.echo.2017.11.021
Rüst, C. A., Knechtle, B., Eichenberger, E., Rosemann, T., and Lepers, R. (2013a). Finisher and performance trends in female and male mountain ultramarathoners by age group. Int. J. Gen. Med. 6, 707–718. doi: 10.2147/ijgm.s46984
Rüst, C. A., Knechtle, B., Knechtle, P., and Rosemann, T. (2012a). Comparison of anthropometric and training characteristics between recreational male marathoners and 24-hour ultramarathoners. Open Access J. Sports Med. 3, 121–129. doi: 10.2147/oajsm.s37389
Rüst, C. A., Knechtle, B., Knechtle, P., and Rosemann, T. (2012b). Similarities and differences in anthropometry and training between recreational male 100-km ultra-marathoners and marathoners. J. Sports Sci. 30, 1249–1257. doi: 10.1080/02640414.2012.697182
Rüst, C. A., Knechtle, B., Knechtle, P., Wirth, A., and Rosemann, T. (2012c). Body mass change and ultra endurance performance: a decrease in body mass is associated with an increased running speed in male 100-km ultra marathoners. J. Strength Cond. Res. 26, 1505–1516. doi: 10.1519/JSC.0b013e318231a7b5
Rüst, C. A., Knechtle, B., Rosemann, T., and Lepers, R. (2013b). Analysis of performance and age of the fastest 100- mile ultra-marathoners worldwide. Clinics 68, 605–611. doi: 10.6061/clinics/2013(05)05
Rüst, C. A., Rosemann, T., Zingg, M. A., and Knechtle, B. (2015). Do non-elite older runners slow down more than younger runners in a 100 km ultra-marathon? BMC Sports Sci. Med. Rehabil. 7:1. doi: 10.1186/2052-1847-7-1
Rüst, C. A., Zingg, M. A., Rosemann, T., and Knechtle, B. (2014). Will the age of peak ultra-marathon performance increase with increasing race duration? BMC Sports Sci. Med. Rehabil. 6:36. doi: 10.1186/2052-1847-6-36
Salvagno, G. L., Schena, F., Gelati, M., Danese, E., Cervellin, G., Guidi, G. C., et al. (2014). The concentration of high-sensitivity troponin I, galectin-3 and NT-proBNP substantially increase after a 60-km ultramarathon. Clin. Chem. Lab. Med. 52, 267–272. doi: 10.1515/cclm-2013-0601
Sandström, M. E., Siegler, J. C., Lovell, R. J., Madden, L. A., and McNaughton, L. (2008). The effect of 15 consecutive days of heat-exercise acclimation on heat shock protein 70. Cell Stress Chaperones 13, 169–175. doi: 10.1007/s12192-008-0022-8
Sansoni, V., Vernillo, G., Perego, S., Barbuti, A., Merati, G., Schena, F., et al. (2017). Bone turnover response is linked to both acute and established metabolic changes in ultra-marathon runners. Endocrine 56, 196–204. doi: 10.1007/s12020-016-1012-8
Sapounakis, K., Kotsiou, A., and Tesseromatis, C. (2010). Modifications of the lipidemic profile of ultramarathon runners in Greece. Rev. Clin. Pharmacol. Pharmacokinet. Int. Ed. 24, 255–258.
Saugy, J., Place, N., Millet, G. Y., Degache, F., Schena, F., and Millet, G. P. (2013). Alterations of neuromuscular function after the world's most challenging mountain ultra-marathon. PLoS ONE 8:e0065596. doi: 10.1371/journal.pone.0065596
Scheer, B. V., and Murray, A. (2011). Al andalus ultra trail: an observation of medical interventions during a 219-km, 5-day ultramarathon stage race. Clin. J. Sport Med. 21, 444–446. doi: 10.1097/JSM.0b013e318225b0df
Scheer, B. V., and Murray, A. (2015). “Ultramarathon running injuriesm” in Sports Injuries: Prevention, Diagnosis, Treatment and Rehabilitation, 2nd Edn., eds M. Doral and J. Karlsson (Berlin: Springer-Verlag), 2889–2898.
Scheer, B. V., Reljic, D., Murray, A., and Murray, A. (2014). The enemy of the feet blisters in ultraendurance runners. J. Am. Podiatr. Med. Assoc. 104, 473–478. doi: 10.7547/0003-0538-104.5.473
Schiff, H. B., MacSearraigh, E. T., and Kallmeyer, J. C. (1978). Myoglobinuria, rhabdomyolysis and marathon running. Q. J. Med. 47, 463–472.
Schobersberger, W., Hobisch-Hagen, P., Fries, D., Wiedermann, F., Rieder-Scharinger, J., Villiger, B., et al. (2000). Increase in immune activation, vascular endothelial growth factor and erythropoietin after an ultramarathon run at moderate altitude. Immunobiology 201, 611–620.
Schütz, U. H. W., Billich, C., König, K., Würslin, C., Wiedelbach, H., Brambs, H. J., et al. (2013). Characteristics, changes and influence of body composition during a 4486 km transcontinental ultramarathon: results from the Transeurope Footrace mobile whole body MRI-project. BMC Med. 11:122. doi: 10.1186/1741-7015-11-122
Schütz, U. H. W., Ellermann, J., Schoss, D., Wiedelbach, H., Beer, M., and Billich, C. (2014). Biochemical cartilage alteration and unexpected signal recovery in T2* mapping observed in ankle joints with mobile MRI during a transcontinental multistage footrace over 4486km. Osteoarthritis Cartilage 22, 1840–1850. doi: 10.1016/j.joca.2014.08.001
Schwabe, K., Schwellnus, M. P., Derman, W., Swanevelder, S., and Jordaan, E. (2014). Less experience and running pace are potential risk factors for medical complications during a 56 km road running race: a prospective study in 26 354 race starters-SAFER study II. Br. J. Sports Med. 48, 905–911. doi: 10.1136/bjsports-2014-093471
Scott, J. M., Esch, B. T., Shave, R., Warburton, D. E., Gaze, D., and George, K. (2009). Cardiovascular consequences of completing a 160-km ultramarathon. Med. Sci. Sports Exerc. 41, 26–34. doi: 10.1249/MSS.0b013e31818313ff
Seedat, Y. K., Aboo, N., Naicker, S., and Parsoo, I. (1989). Acute renal failure in the “Comrades Marathon” runners. Ren. Fail. 11, 209–212.
Senefeld, J., Smith, C., and Hunter, S. K. (2016). Sex differences in participation, performance, and age of ultramarathon runners. Int. J. Sports Physiol. Perform. 11, 635–642. doi: 10.1123/ijspp.2015-0418
Sengoku, Y., Nakamura, K., Ogata, H., Nabekura, Y., Nagasaka, S., and Tokuyama, K. (2015). Continuous glucose monitoring during a 100-km race: a case study in an elite ultramarathon runner. Int. J. Sports Physiol. Perform. 10, 124–127. doi: 10.1123/ijspp.2013-0493
Shave, R. E., Dawson, E., Whyte, G., George, K., Ball, D., Gaze, D. C., et al. (2002). Evidence of exercise-induced cardiac dysfunction and elevated cTnT in separate cohorts competing in an ultra-endurance mountain marathon race. Int. J. Sports Med. 23, 489–494. doi: 10.1055/s-2002-35069
Shephard, R. J., and Johnson, N. (2015). Effects of physical activity upon the liver. Eur. J. Appl. Physiol. 115, 1–46. doi: 10.1007/s00421-014-3031-6
Shin, K. A., Kim, A. C., Kim, Y. J., Lee, Y. H., Shin, Y. O., Kim, S. H., et al. (2012). Effect of ultra-marathon (308 km) race on bone metabolism and cartilage damage biomarkers. Ann. Rehabil. Med. 36, 80–87. doi: 10.5535/arm.2012.36.1.80
Shin, K. A., Park, K. D., Ahn, J., Park, Y., and Kim, Y. J. (2016). Comparison of changes in biochemical markers for skeletal muscles, hepatic metabolism, and renal function after three types of long-distance running. Medicine 95:e3657. doi: 10.1097/MD.0000000000003657
Shin, K., Jee, H., Lee, Y., Kim, T. K., Kim, H. S., Park, Y., et al. (2014). Effects of an extreme endurance ultra-marathon on musculoskeletal and hematologic functions. Gazz. Med. Ital. Arch. Sci. Med. 173, 283–289.
Shin, Y. O., and Lee, J. B. (2013). Leukocyte chemotactic cytokine and leukocyte subset responses during ultra-marathon running. Cytokine 61, 364–369. doi: 10.1016/j.cyto.2012.11.019
Simons, S. M., and Kennedy, R. G. (2004). Gastrointestinal problems in runners. Curr. Sports Med. Rep. 3, 112–116.
Simpson, D., Post, P. G., Young, G., and Jensen, P. R. (2014). “It's not about taking the easy road”: The experiences of ultramarathon runners. Sport Psychol. 28, 176–185. doi: 10.1123/tsp.2013-0064
Spiropoulos, A., Goussetis, E., Margeli, A., Premetis, E., Skenderi, K., Graphakos, S., et al. (2010). Effect of inflammation induced by prolonged exercise on circulating erythroid progenitors and markers of erythropoiesis. Clin. Chem. Lab. Med. 48, 199–203. doi: 10.1515/CCLM.2010.034
Spormann, R., Harding, U., Stuhr, M., Rother, J., Puschel, K., and Reifferscheid, F. (2012). [Serious complications following a marathon run: interactive case report of a dramatic course]. Anasthesiol. Intensivmed. Notfallmed. Schmerzther. 47, 696–702. doi: 10.1055/s-0032-1331366
Stellingwerff, T. (2013). Contemporary nutrition approaches to optimize elite marathon performance. Int. J. Sports Physiol. Perform. 8, 573–578.
Strachan, A. F., Noakes, T. D., Kotzenberg, G., Nel, A. E., and de Beer, F. C. (1984). C reactive protein concentrations during long distance running. Br. Med. J. 289, 1249–1251.
Stuempfle, K. J., and Hoffman, M. D. (2015). Gastrointestinal distress is common during a 161-km ultramarathon. J. Sports Sci. 33, 1814–1821. doi: 10.1080/02640414.2015.1012104
Stuempfle, K. J., Hoffman, M. D., and Hew-Butler, T. (2013). Association of gastrointestinal distress in ultramarathoners with race diet. Int. J. Sport Nutr. Exerc. Metab. 23, 103–109. doi: 10.1123/ijsnem.23.2.103
Stuempfle, K. J., Hoffman, M. D., Weschler, L. B., Rogers, I. R., and Hew-Butler, T. (2011). Race diet of finishers and non-finishers in a 100 mile (161 km) mountain footrace. J. Am. Coll. Nutr. 30, 529–535. doi: 10.1080/07315724.2011.10719999
Stuempfle, K. J., Lehmann, D. R., Case, H. S., Bailey, S., Hughes, S. L., McKenzie, J., et al. (2002). Hyponatremia in a cold weather ultraendurance race. Alaska Med. 44, 51–55.
Stuempfle, K. J., Valentino, T., Hew-Butler, T., Hecht, F. M., and Hoffman, M. D. (2016). Nausea is associated with endotoxemia during a 161-km ultramarathon. J. Sports Sci. 34, 1662–1668. doi: 10.1080/02640414.2015.1130238
Surgenor, S., and Uphold, R. E. (1994). Acute hyponatremia in ultra-endurance athletes. Am. J. Emerg. Med. 12, 441–444. doi: 10.1016/0735-6757(94)90057-4
Szauder, I., Kovács, A., and Pavlik, G. (2015). Comparison of left ventricular mechanics in runners versus bodybuilders using speckle tracking echocardiography. Cardiovasc. Ultrasound, 13:7. doi: 10.1186/s12947-015-0002-y
Tan, P. L. S., Tan, F. H. Y., and Bosch, A. N. (2016). Similarities and differences in pacing patterns in a 161-km and 101-km ultra-distance road race. J. Strength Cond. Res. 30, 2145–2155. doi: 10.1519/JSC.0000000000001326
Tauler, P., Martinez, S., Moreno, C., Martínez, P., and Aguilo, A. (2014). Changes in salivary hormones, immunoglobulin A, and C-reactive protein in response to ultra-endurance exercises. Appl. Physio. Nutr. Metab. 39, 560–565. doi: 10.1139/apnm-2013-0466
Tchou, I., Margeli, A., Tsironi, M., Skenderi, K., Barnet, M., Kanaka-Gantenbein, C., et al. (2009). Growth-differentiation factor-15, endoglin and N-terminal pro-brain natriuretic peptide induction in athletes participating in an ultramarathon foot race. Biomarkers 14, 418–422. doi: 10.1080/13547500903062976
Thalmann, M., Sodeck, G. H., Kavouras, S., Matalas, A., Skenderi, K., Yannikouris, N., et al. (2006). Proton pump inhibition prevents gastrointestinal bleeding in ultramarathon runners: a randomised, double blinded, placebo controlled study. Br. J. Sports Med. 40, 359–362. doi: 10.1136/bjsm.2005.024463
Theysohn, J. M., Kraff, O., Maderwald, S., Kokulinsky, P. C., Ladd, M. E., Barkhausen, J., et al. (2013). MRI of the ankle joint in healthy non-athletes and in marathon runners: image quality issues at 7.0 T compared to 1.5 T. Skeletal Radiol. 42, 261–267. doi: 10.1007/s00256-012-1454-x
Thompson, W. R., Nequin, N. D., Lesmes, G. R., and Garfield, D. S. (1982). Physiological and training profiles of ultramarathoners. Physician Sportsmed. 10, 61–65.
Tokudome, S., Kuriki, K., Yamada, N., Ichikawa, H., Miyata, M., Shibata, K., et al. (2004). Anthropometric, lifestyle and biomarker assessment of Japanese non-professional ultra-marathon runners. J. Epidemiol. 14, 161–167. doi: 10.2188/jea.14.161
Tomaszewski, M., Charchar, F. J., Crawford, L., Zukowska-Sczechowska, E., Grzeszczak, W., Sattar, N., et al. (2004). Serum C-reactive protein and lipids in ultra-Marathon runners. Am. J. Cardiol. 94, 125–126. doi: 10.1016/j.amjcard.2004.03.043
Uberoi, H. S., Dugal, J. S., Kasthuri, A. S., Kolhe, V. S., Kumar, A. K., and Cruz, S. A. (1991). Acute renal failure in severe exertional rhabdomyolysis. J. Assoc. Physicians India 39, 677–679.
Valentino, T. R., Stuempfle, K. J., Kern, M., and Hoffman, M. D. (2016). The influence of hydration state on thermoregulation during a 161-km ultramarathon. Res. Sports Med. 24, 212–221. doi: 10.1080/15438627.2016.1191491
Van Helder, T., and Radoki, M. W. (1989). Sleep deprivation and the effect on exercise performance. Sports Med. 7, 235–247. doi: 10.2165/00007256-198907040-00002
Vernillo, G., Savoldelli, A., La Torre, A., Skafidas, S., Bortolan, L., and Schena, F. (2016). Injury and illness rates during ultratrail running. Int. J. Sports Med. 37, 565–569. doi: 10.1055/s-0035-1569347
Videbæk, S., Bueno, A. M., Nielsen, R. O., and Rasmussen, S. (2015). Incidence of running-related injuries per 1000 h of running in different types of runners: a systematic review and meta-analysis. Sports Med. 45, 1017–1026. doi: 10.1007/s40279-015-0333-8
Wardenaar, F. C., Dijkhuizen, R., Ceelen, I. J. M., Jonk, E., De Vries, J. H. M., Witkamp, R. F., et al. (2015). Nutrient intake by ultramarathon runners: can they meet recommendations? Int. J. Sport Nutr. Exerc. Metab. 25, 375–386. doi: 10.1123/ijsnem.2014-0199
Waśkiewicz, Z., Kápcinska, B., Sadowska-Krępa, E., Czuba, M., Kempa, K., Kimsa, E., et al. (2012). Acute metabolic responses to a 24-h ultra-marathon race in male amateur runners. Eur. J. Appl. Physiol. 112, 1679–1688. doi: 10.1007/s00421-011-2135-5
Wegelin, J. A., and Hoffman, M. D. (2011). Variables associated with odds of finishing and finish time in a 161-km ultramarathon. Eur. J. Appl. Physiol. 111, 145–153. doi: 10.1007/s00421-010-1633-1
Wellershoff, G. (2013). [Hyponatremic encephalopathy with non-cardiogenic pulmonary edema. Development following marathon run]. Med. Klin. Intensivmed. Notfmed. 108, 234–237. doi: 10.1007/s00063-012-0198-7
Willmott, A. G. B., Hayes, M., Waldock, K. A. M., Relf, R. L., Watkins, E. R., James, C. A., et al. (2017). Short-term heat acclimation prior to a multi-day desert ultra-marathon improves physiological and psychological responses without compromising immune status. J. Sports Sci. 35, 2249–2256. doi: 10.1080/02640414.2016.1265142
Winger, J. M., Hoffman, M. D., Hew-Butler, T. D., Stuempfle, K. J., Dugas, J. P., Fogard, K., et al. (2013). The effect of physiology and hydration beliefs on race behavior and postrace sodium in 161-km ultramarathon finishers. Int. J. Sports Physiol. Perform. 8, 536–541. doi: 10.1123/ijspp.8.5.536
Wittert, G. A., Livesey, J. H., Espiner, E. A., and Donald, R. A. (1996). Adaptation of the hypothalamopituitary adrenal axis to chronic exercise stress in humans. Med. Sci. Sports Exerc. 28, 1015–1019.
Wollseiffen, P., Schneider, S., Martin, L. A., Kerhervé, H. A., Klein, T., and Solomon, C. (2016). The effect of 6 h of running on brain activity, mood, and cognitive performance. Exp. Brain Res. 234, 1829–1836. doi: 10.1007/s00221-016-4587-7
Wu, H. J., Chen, K. T., Shee, B. W., Chang, H. C., Huang, Y. J., and Yang, R. S. (2004). Effects of 24 h ultra-marathon on biochemical and hematological parameters. World J. Gastroenterol. 10, 2711–2714. doi: 10.3748/wjg.v10.i18.2711
Yoon, J. H., Park, Y., Ahn, J., Shin, K. A., and Kim, Y. J. (2016). Changes in the markers of cardiac damage in men following long-distance and ultra-long-distance running races. J. Sports Med. Phys. Fit. 56, 295–301.
Zakovska, A., Knechtle, B., Chlibkova, D., Milickova, M., Rosemann, T., and Nikolaidis, P. T. (2017). The effect of a 100-km ultra-marathon under freezing conditions on selected immunological and hematological parameters. Front. Physiol. 8:638. doi: 10.3389/fphys.2017.00638
Zaryski, C., and Smith, D. J. (2005). Training principles and issues for ultra-endurance athletes. Curr. Sports Med. Rep. 4, 165–170. doi: 10.1097/01.CSMR.0000306201.49315.73
Zingg, M. A., Karner-Rezek, K., Rosemann, T., Knechtle, B., Lepers, R., and Rüst, C. A. (2014a). Will women outrun men in ultra-marathon road races from 50 km to 1,000 km? Springerplus 3:97. doi: 10.1186/2193-1801-3-97
Zingg, M. A., Knechtle, B., Rüst, C. A., Rosemann, T., and Lepers, R. (2013a). Analysis of participation and performance in athletes by age group in ultramarathons of more than 200 km in length. Int. J. Gen. Med. 6, 209–220. doi: 10.2147/IJGM.S43454
Zingg, M. A., Rüst, C. A., Rosemann, T., Lepers, R., and Knechtle, B. (2014b). Runners in their forties dominate ultra-marathons from 50 to 3,100 miles. Clinics 69, 203–211. doi: 10.6061/clinics/2014(03)11
Keywords: extreme endurance, pathophysiology, performance, injury, gender
Citation: Knechtle B and Nikolaidis PT (2018) Physiology and Pathophysiology in Ultra-Marathon Running. Front. Physiol. 9:634. doi: 10.3389/fphys.2018.00634
Received: 01 March 2018; Accepted: 11 May 2018;
Published: 01 June 2018.
Edited by:
Hassane Zouhal, University of Rennes 2–Upper Brittany, FranceReviewed by:
Samuel Verges, Joseph Fourier University, FranceCopyright © 2018 Knechtle and Nikolaidis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Beat Knechtle, YmVhdC5rbmVjaHRsZUBoaXNwZWVkLmNo
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.