
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol., 23 January 2017
Sec. Exercise Physiology
Volume 8 - 2017 | https://doi.org/10.3389/fphys.2017.00004
This article is part of the Research TopicHypoxia and exercise - novel treatment strategy for obesity and related comorbiditiesView all 8 articles
 Germana P. L. Almeida1,2
Germana P. L. Almeida1,2 Ivani C. Trombetta3
Ivani C. Trombetta3 Felipe X. Cepeda1
Felipe X. Cepeda1 Elaine Hatanaka4
Elaine Hatanaka4 Rui Curi5
Rui Curi5 Cristiano Mostarda6Maria C. Irigoyen1José A. S. Barreto-Filho7Eduardo M. Krieger1Fernanda M. Consolim-Colombo1,3*
Cristiano Mostarda6Maria C. Irigoyen1José A. S. Barreto-Filho7Eduardo M. Krieger1Fernanda M. Consolim-Colombo1,3*Introduction: Recurrent hypoxia (HPX), a hallmark of the obstructive sleep apnea (OSA), impairs autonomic balance, and increases arterial blood pressure (BP). Oxidative stress is one of the mechanisms involved in these alterations. The cumulative effect of acute intermittent HPX and the chronicity may determine whether the response crosses the threshold from having protective value to pathology. However, the impact of acute intermittent HPX–reoxygenation on markers of oxidative stress in healthy individuals remains to be fully understood.
Objective: To analyze the effects of the acute intermittent HPX on the generation of neutrophil-derived superoxide, sympathovagal balance, and vascular function in healthy subjects.
Methods: We applied six cycles of intermittent HPX (10% O2 and 90% N2) for 5 min followed by 2 min of room-air in 15 healthy volunteers (34 ± 2 years; 22.3 ± 0.46 kg/m2), without OSA (polysomnography), during wakefulness. During the experimental protocol, we recorded O2 saturation, end-tidal CO2, heart rate (HR), systolic, and diastolic BP, cardiac output (CO) and peripheral resistance (PR). Cardiac sympathovagal balance was determined by HR variability analysis (low frequency and high frequency bands, LF/HF). Superoxide generation in polymorphonuclear neutrophil cells were established using relative luminescence units (PMNs RLU) at baseline (pre-HPX) and immediately after hypoxia induction (post-HPX6).
Results: The studied subjects had normal levels of BP, plasma glucose, lipid profile, and inflammatory marker (C-reactive protein). Acute intermittent HPX increased HR, systolic BP, CO, and decreased PR. Additionally, acute intermittent HPX increased PMNs RLU, measured post-HPX6 (470 ± 50 vs. 741 ± 135, P < 0.05). We found a similar increase in LF/HF post-HPX6 (0.91 ± 0.11 vs. 2.85 ± 0.40, P < 0.05). PR was diminished from pre-HPX to post-HPX6 (1.0 ± 0.03 vs. 0.85 ± 0.06, P < 0.05). Further analysis showed significant association between O2 saturation and PMNs RLU (R = −0.62, P = 0.02), and with LF/HF (R = −0.79, P = 0.02) post-HPX6. In addition, an association was found between PMNs RLU and PR post-HPX6 (R = 0.58, P = 0.04).
Conclusion: Acute exposure to intermittent HPX not only increased superoxide generation in neutrophils, but also impaired cardiac sympathovagal balance in healthy subjects. These data reinforce the role of intermittent HPX in superoxide generation on neutrophils, which may lead to an impairment in peripheral vascular resistance.
Intermittent hypoxia (HPX), defined as repeated episodes of hypoxia interspersed with episodes of normoxia, has been observed in different types of sleep-disordered breathing, including obstructive sleep apnea syndrome (OSA) (Lévy et al., 2008).
Repeated episodes of hypoxia elicit changes in a range of physiological responses (Lévy et al., 2008; Foster et al., 2010; Gilmartin et al., 2010; Tamisier et al., 2011). The cumulative effect of intermittent HPX and the chronicity of intermittent HPX may determine whether the response crosses the threshold from having protective value to pathology. Furthermore, the presence of clinical diseases and environmental conditions may interfere with the response to this challenge.
It is not known if acute intermittent HPX–reoxygenation are able to increase polymorphonuclear and peripheral blood mononuclear cell mobilization, enhance superoxide generation in neutrophils, and impair sympato-vagal control and vascular function in healthy volunteers. Indeed, the threshold from physiological to pathophysiological condition may be triggered by inflammation and oxidative stress. It has already been found that the continuum release of a number of pro-inflammatory cytokines by macrophages sensitizes neutrophils and macrophages, thus producing superoxide (Laskin et al., 2011). On the other hand, while the generation of active oxygen species by neutrophils is one of the defense mechanisms against foreign pathogens, in chronic condition it may lead to inflammation and diseases.
In a chronic state, autonomic and hemodynamic changes stimulate the intravascular production of superoxide (Schultz, 2009), promoting inflammation, and damage to the vascular integrity and endothelial cell function (Laskin et al., 2011). Moreover, among subjects with untreated OSA, the release of superoxide from circulating neutrophils, was markedly enhanced when compared to control subjects (Schulz et al., 2000). However, the effect of acute intermittent HPX on immune cells mobilization and activation in healthy humans has not been fully investigated.
OSA has been consistently associated with increased cardiovascular morbidity/mortality (Fu et al., 2016). There is growing evidence that OSA may be directly involved in multiple pathways associated with cardiovascular risk. In this context, autonomic dysfunction seems to play a major role (Trombetta et al., 2013). Recent studies have suggested that chronic and acute intermittent HPX increases sympathetic activation via peripheral chemoreceptors stimulation (Trombetta et al., 2013), acutely increasing arterial blood pressure (BP) (Foster et al., 2010; Gilmartin et al., 2010; Tamisier et al., 2011). Indeed, in OSA patients, regardless of other cardiovascular risk factors, the cumulative effect of the repetitive hypoxia/hypercapnia episodes has been found to lead to an autonomic imbalance shift toward sympathetic tone (Trombetta et al., 2010, 2013; Cepeda et al., 2015), proinflammatory response, (Yokoe et al., 2003; Ryan et al., 2005) endothelial dysfunction (Kato et al., 2000), and chronic oxidative stress (Schulz et al., 2000).
To avoid the effect of pathological chronicity interference and isolate the acute effect of intermittent HPX–reoxygenation in neutrophil-generated superoxide and sympathovagal balance, we chose to investigate the acute intermittent HPX–reoxygenation in in healthy subjects, which was to identify the implication of intermittent HPX as mediator in the genesis of oxidative stress, even in the absence of other pathophysiological changes.
In the present study, we tested the hypothesis that brief cycles of intermittent HPX–reoxygenation are able to increase polymorphonuclear and peripheral blood mononuclear cell mobilization, enhance superoxide generation in neutrophils, and impair sympato-vagal control and vascular function in healthy volunteers.
Fifteen healthy subjects from the community, with no clinical and laboratory evidence of disease, participated in the study. Women were studied during the proliferative phase of the reproductive cycle. Smokers and subjects presenting OSA (defined by an apnea-hypopnea index >5 events/hour of sleep by the polysomnography, Drager et al., 2005) were excluded. All subjects provided informed written consent, and the study was approved by the Ethics Committee of the Heart Institute of the University of São Paulo.
In order to exclude OSA, all subjects underwent an overnight polysomnography, performed as previously described (Trombetta et al., 2013). Briefly, the polysomnography was undertaken using the EMBLA digital system (17 channels, EMBLA, Flaga hf. Medical Devices, Reykjavik, Iceland). The apnea-hypopnea index (AHI) was calculated as the total number of respiratory events (apneas plus hypopneas) per hour of sleep, while the presence of OSA was defined by an AHI ≥5 events/h.
For all volunteers, blood samples were collected from venous blood after 12 h of overnight fasting, according to standard laboratory techniques in the clinical laboratory of the Heart Institute, to determine total cholesterol, low-density lipoprotein cholesterol (LDL-c), high-density lipoprotein cholesterol (HDL-c), triglycerides, glucose, and C-reactive protein.
All experiments were realized approximately at 8:00 a.m. Acute intermittent HPX protocol was performed while the subjects were awake after at least a 20 min of rest period in supine position in a quiet and temperature-controlled room. For the experimental protocol, the subjects completed a single day session of six cycles of breathing a gas mixture (10% O2, 90% N2) via a mouthpiece, for 5-min periods with intervening 2-min periods of room-air inspiration (Figure 1). A nose clip was used to ensure exclusive mouth breathing. The end-tidal carbon dioxide (CO2) and oxygen saturation were continuously monitored by a capnograph and pulse oximeter (Novametrix, model 7100 CO2 SMO ETCO2/SpO2 Monitor, Novametrix Medical Systems Inc.). The CO2 was titrated to maintain isocapnia. Non-invasive beat-to-beat arterial BP curves were continuously recorded by a finger photoplethysmography device (Finometer, Finometer Medical Systems BV, Arnhem, the Netherlands). Heart rate (HR) was evaluated by electrocardiography and arterial BP, cardiac output (CO) and peripheral vascular resistance (PR) were calculated using a BeatScope software and were analyzed as previously described (Barreto-Filho et al., 2003). Blood samples were collected before intermittent HPX (pre-HPX) and immediately after the completion of the protocol (post HPX 6) to perform white cell counting and analyze superoxide production at interval-period (approximately 45 min-period interval).
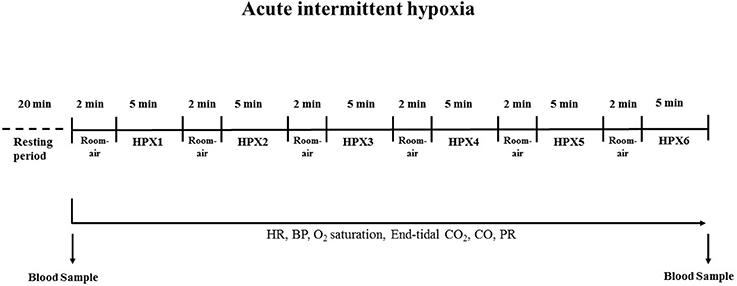
Figure 1. Experimental protocol for evaluation of the effects of acute intermittent hypoxia (HPX, 10% O2 and 90% N2). HR, heart rate; BP, blood pressure; CO, cardiac output; PR, peripheral resistance.
Polymorphonuclear (PMNs) and peripheral mononuclear cells (PBMCs) were isolated from the blood, as previously described (Jun et al., 2008), using a commercial gradient of Ficoll–Hypaque (Sigma-Aldrich Histopaque) and counted on a Neubauer chamber.
Neutrophils were isolated from the blood (Böyum, 1968), using a commercial gradient of Ficoll–Hypaque (Histopaque). Lucigenin (1 mM) was added to neutrophil (2.5 × 106 cells/ml) incubation medium when required. This method has been widely used to measure kinetics productions of superoxide by neutrophils (Hatanaka et al., 2006). Lucigenin releases energy in the form of light after being excited with superoxide anion. The assays were performed in a PBS buffer supplemented with CaCl2 (1 mM), MgCl2 (1.5 mM), and glucose (10 mM), at 37°C, in a final volume of 0.3 ml. Chemiluminescence response was monitored for 20 min, at 37°C, in a microplate luminometer (EG&G Berthold LB96V), before and after the addition of 16 ng of phorbol 12-myristate 13-acetate (PMA). Superoxide generation in polymorphonuclear neutrophil cells in relative luminescence units (PMNs RLU) was expressed as nanomoles of O2 per 2.5 × 106 PMNs.
HR variability was analyzed in the frequency domains during the protocol, as previously described (Mello et al., 2012). The spectral bands for humans (very low frequency—VLF, 0.0–0.04 Hz; low frequency—LF, 0.04–0.15 Hz; and high frequency—HF, 0.15–0.4 Hz) were defined according to the literature (Pagani et al., 1986). The spectral power for the low- and high-frequency bands was calculated by power spectrum density integration within each frequency band width. Power density of each spectral component was calculated in normalized units. The powers in LF and HF for pulse interval were normalized by calculating the variance minus the power in VLF and were expressed in normalized units (nu). Sympathovagal balance was defined by the LF/HF ratio, expressed in nu. LF components of the R-R pulse interval variability was found to be markers of efferent sympathetic cardiac, whereas the HF component of the R-R pulse interval variability would reflect vagal modulation of the sinoatrial node (Pagani et al., 1986).
The data are presented as the means ± standard error. The normal distribution of each variable was evaluated using the Kolmogorov-Smirnov test. The comparison of the cell counts in both groups was done by Wilcoxon's nonparametric test. We used one-way ANOVA for repeated measures followed by Tukey-Kramer. Test for multiple comparisons were used in hemodynamic, autonomic and blood samples data. Values of P < 0.05 were considered statistically significant.
Baseline characteristics are shown in Table 1. Fifteen healthy subjects (predominantly women) participated in the present study. The volunteers had normal BMI, BP, glucose, lipid profiles and CRP. In addition, all participants were within the normal range of the AHI, based on the polysomnography records (Table 1).
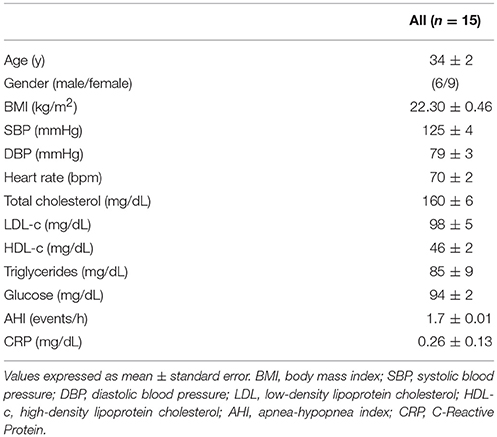
Table 1. Characteristics of the studied population.
The acute intermittent HPX effects on ventilatory, hemodynamic, vascular, and autonomic measures are shown in Table 2. Acute intermittent HPX reduced O2 saturation and increased HR, systolic BP, CO, PR, and HF band post HPX when compared to pre-HPX. However, there were no changes in end-tidal CO2 and diastolic BP from pre-HPX to post HPX 6. The LF band only increased in post HPX 5 and post HPX 6 when compared to pre-HPX (Table 2).
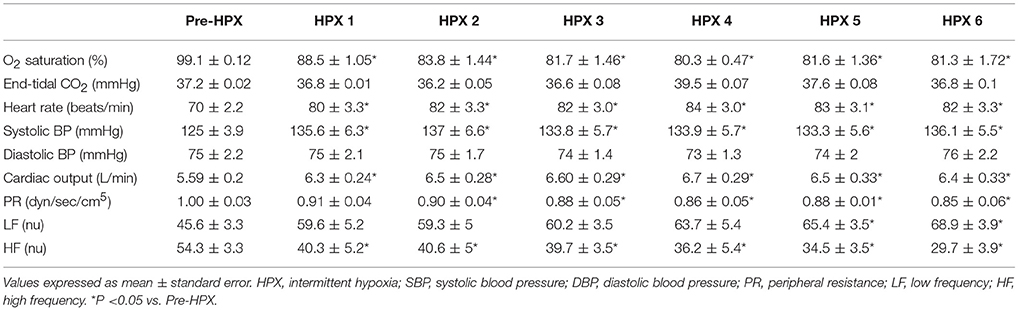
Table 2. Acute intermittent hypoxia (HPX) on ventilator, hemodynamic and autonomic measurements.
Effects of acute intermittent HPX on PMNs and in PBMCs are shown in Figures 2A,B respectively. PMNs increased (34 ± 6.7–49 ± 6 cells × 105; P = 0.008) from pre-HPX to post HPX 6 (Figure 2A). Similar results were found for PBMCs, which increased (21.5 ± 4.2–26.7 ± 4.4 cells × 105; P = 0.03) from pre-HPX to post HPX6 (Figure 2B).
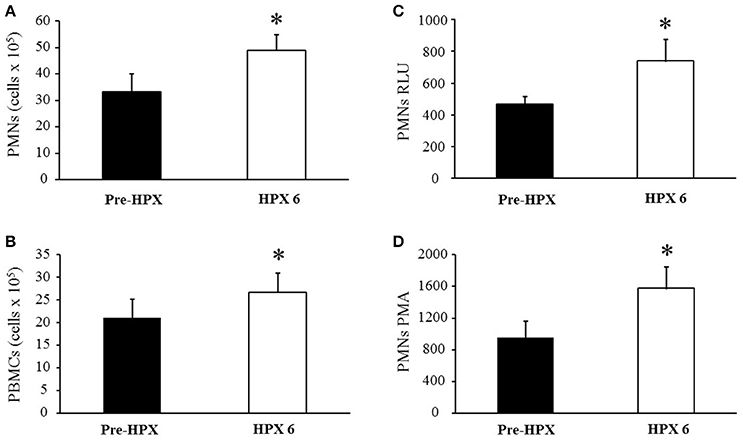
Figure 2. (A) Polymorphonuclear neutrophils (PMNs); (B) peripheral blood mononuclear cells (PBMCs); (C) polymorphonuclear in relative luminescence units (PMNs RLU); and (D) polymorphonuclear in relative phorbol myristate acetate (PMNs PMA). *P < 0.05 vs. Pre-HPX.
The effects of acute intermittent HPX on superoxide generation on PMNs-RLU and after the addition of 16 ng of phorbol 12-myristate 13-acetate (PMA) are shown in Figures 2C,D, respectively. Superoxide levels in PMNs RLU increased (470 ± 50–741 ± 135; P < 0.05) from pre-HPX to post HPX 6 (Figure 2C). The addition of PMA led to an increase in superoxide levels in PMNs harvested (1228 ± 247 vs. 1162 ± 265, P < 0.05) from pre-HPX to post HPX 6 (Figure 2D).
Further analysis showed significant association between O2 saturation in HPX 6 and PMNs RLU post HPX 6 (R = −0.62, P = 0.02; Figure 3A). We also found an association between peripheral resistance (PR) in HPX 6 and PMNs–RLU post HPX 6 (R = −0.58, P = 0.04; Figure 3B).
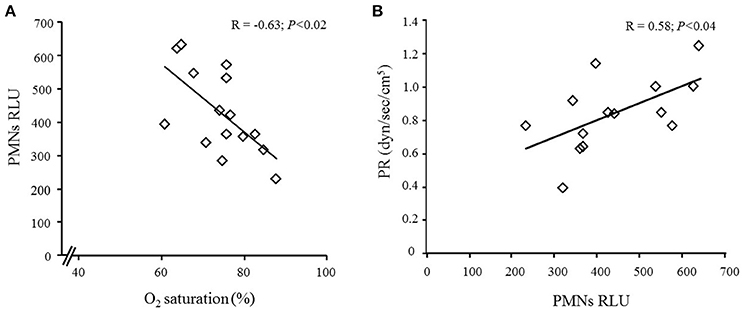
Figure 3. (A) Pearson correlation between O2 saturation and polymorphonuclear in relative luminescence units (PMNs RLU) in post HPX 6; and (B) Pearson correlation between PMNs RLU and peripheral resistance (PR) in post HPX 6.
Acute intermittent HPX caused a significant increase in the sympathovagal ratio (LF/HF index) when compared to pre-HPX (Figure 4). The LF/HF index increased from 0.91 ± 0.11 in pre-HPX to 2.85 ± 0.4 in post HPX 6 (Figure 4). Interestingly, we found a strong association between O2 saturation in post HPX 6 and LF/HF in post HPX 6 (R = −0.79, P = 0.02).
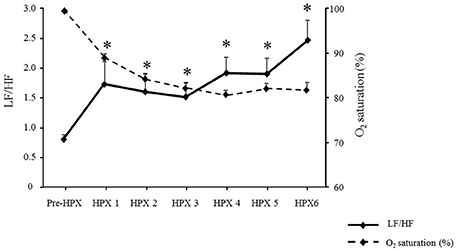
Figure 4. Effects of the protocol of acute intermittent hypoxia (Pre-HPX and post HPX 1–6) in O2 saturation and on sympathovagal balance (LF/HF). *P < 0.05 vs. Pre-HPX.
The present investigation explores the role of intermittent HPX, a major component of OSA, in hemodynamic and autonomic responses and in the mobilization and activation of immune cells even in acute response in healthy subjects. The novel finding of our study is that acute exposure to intermittent HPX promoted not only hemodynamic and autonomic impairment in healthy volunteers but also increased superoxide generation in neutrophils.
The major implication of these findings is that intermittent HPX, in the absence of other pathophysiological changes, may be an important mediator in the genesis of oxidative stress in healthy individuals. In fact, in the present study, we found association between O2 saturation and polymorphonuclear in relative luminescence units (PMNs RLU) and the association between PMNs RLU and peripheral resistance (PR) in response to acute intermittent HPX. However, our results have to be interpreted with caution, because other potential mechanisms could be involved. In addition, a simple correlation between oxygen reactive species and a biological outcome does not always could be interpreted to causality.
The effects of intermittent HPX on several pathways have mainly been explored in animal models of OSA. Several studies have indicated that HPX is related to increased sympathetic activation and BP (Fletcher et al., 1992; Trombetta et al., 2013), as well as to inducing inflammation (Tam et al., 2007), oxidative stress (Jun et al., 2008), insulin resistance (Iiyori et al., 2007), dyslipidemia (Li et al., 2005; Drager et al., 2011a), and atherosclerosis (Savransky et al., 2007). The harmful effects of intermittent HPX have been demonstrated in autonomic and hemodynamic impairment (Foster et al., 2010; Gilmartin et al., 2010; Tamisier et al., 2011) and in insulin resistance (Iiyori et al., 2007). Our findings extend the previous evidence in humans, suggesting that intermittent HPX could trigger superoxide production even in the absence of diseases.
It is well-established that oxidative stress is implicated in vascular dysfunction and atherosclerosis. Several cardiovascular risk factors, such as hypertension, hypercholesterolemia, and diabetes mellitus, stimulate the production of superoxide in the vascular wall (Tousoulis et al., 2011). Accumulated evidence suggests that OSA is associated with increased oxidative stress and endothelial dysfunction. Lavie (2003) and Monneret et al. (2010). Indeed, OSA seems to directly affect the vascular endothelium by promoting inflammation and oxidative stress, while decreasing NO availability and repair capacity (Jelic et al., 2008), which may ultimately contribute to atherosclerosis (Drager et al., 2011b). Our results seems to corroborate these previous investigations. Although responses between health and the chronic “disease” state may be very different, the present study brings to the light the role of intermittent HPX, a hallmark of OSA, in healthy individuals. We found that acute intermittent HPX not only significantly increases the number of polymorphonuclear and peripheral blood mononuclear cells but also augments superoxide generation in polymorphonuclear cells. The precise mechanisms by which intermittent HPX induces oxidative stress through polymorphonuclear cells are yet to be determined. It has been postulated that the episodic hypoxia in OSA leads to the increased production of O2 and other reactive oxygen species molecules via several enzymatic pathways. For instance, upon stimulation, activation of NADPH oxidase complex in the endothelium and in neutrophils produces a burst of superoxide anions, contributing to oxidative stress and the onset of inflammatory processes (Lavie, 2003). We also cannot rule out the effect of the adrenergic activation triggered by intermittent HPX, as observed in our study on polymorphonuclear cells and oxidative stress. Indeed, several models of stress induction have demonstrated the onset of leukocytosis in response to catecholamines. Iversen et al. (1994) have found an increase in lymphocytes (220%) and neutrophils (160%) in response to epinephrine injection in rats. This effect was quite rapid (5 min or less) and brief, returning to normal 25 min after injection (Iversen et al., 1994). An early rise in leukocyte count is also a feature of ischemia reperfusion injury, as previously demonstrated in experimental studies (Hallenbeck et al., 1986; Grøgaard et al., 1989). Regarding oxidative stress, the role of epinephrine and adrenergic agonists in triggering oxidative stress in cell culture models (Costa Rosa et al., 1992) and animal models has been reported (Zhang et al., 2005). Therefore, the experimental model of acute hypoxia/reoxygenation presently described is capable of inducing a change in autonomic balance resulting in a predominance of sympathetic activity and an increase in white blood cell counts and oxidative stress, resembling several phenomena related to ischemia-reperfusion injury.
Despite these observations, we cannot exclude the possibility that oxidative stress induced by intermittent HPX may, indeed, be a potential trigger for sympathetic activation and increased BP. Evidence in animal models has suggested that increased oxidative stress in the brain, possibly via the activation of NADPH oxidase, may contribute to the progression of hypertension through central sympathoexcitation (Chan et al., 2009; Nagae et al., 2009). These important issues should be further explored in future experiments.
Our results have to be interpreted with caution. We cannot assume that in OSA patients we would find similar results because possible disparity regarding the chronic and acute effect could interfere in the responses. In addition, we have to address others important limitations.
Regarding superoxide generation in neutrophils determined by relative luminescence units, a large debate exists in the literature about the sensitivity of this assay and the use lucigenin. Indeed, although this assay presents a limitation due to the fact that lucigenin radical undergoes redox cycling with oxygen and generates superoxide, it has been widely used to measure kinetics productions of superoxide by neutrophils. We had previously reported that the assay conditions herein described are more appropriate than other techniques used to measure ROS production (Hatanaka et al., 2006). Luminol-amplified chemiluminescence, cytochrome c, hydroethidine, and phenol red assays also have limitations. The presence of antioxidant/oxidant molecules, enzymes such as neutrophil myeloperoxidase and even oxygen impairs the measurements of ROS production through the mentioned assays.
Other several limitations in our study that merit discussion. First, the duration of each cycle of intermittent HPX does not precisely mimic the duration of the sleep apnea events observed in OSA patients. In addition, the acute intermittent HPX protocol was brief and limited to only 30 min (6 cycles for 5 min). Additional exposure would involve substantial participant burden and could have untoward effects. Second, intermediate mechanisms were crudely assessed, using HR variability rather than microneurography for the assessment of sympathetic activity. Third, the acute intermittent HPX was induced during wakefulness and not during sleep. The decision to characterize hemodynamics, autonomic responses and oxidative stress during wakefulness was based on the awareness that hypoxic exposure during sleep would induce a range of pathophysiological abnormalities, including periodic breathing and sleep disruption. Thus, to characterize the isolated effects of intermittent HPX, the experiment was undertaken during wakefulness. Fourth, the experimental paradigm focused strictly on the effects of intermittent HPX and did not include other pathophysiological concomitants of OSA, such as hypercapnia or asphyxia. Finally, our study lack of a control group not exposed to intermittent HPX. The pre HPX measurements was used to identify the effects of acute intermittent HPX on superoxide generation.
In conclusion, acute exposure to intermittent HPX promoted autonomic impairments as well as increased oxidative stress. These data reinforce the role of intermittent HPX in superoxide generation on neutrophils, which may lead to an impairment in peripheral vascular resistance as observed in patients with obstructive sleep apnea.
The specific contributions for each authors are: GA, EK, FC-C. Conception design of the work, the acquisition, analysis, interpretation of data for the work, drafting the work and revising it critically for important intellectual content. IT, FC, EH, RC, CM, MI, JB. Interpretation of data for the work; drafting the work, revising it critically for important intellectual content. All above authors read and approved the final version to be published; and all authors agree with all aspects of the work in order to ensure the accuracy and the integrity of the work.
This was not an industry-supported study. The work was performed at the Heart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil and was supported by Fundação Zerbini. This study was supported by Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP # 04/0222). FXC (FAPESP#2015/17533-6 and #2016/16831-7), RC (FAPESP 2010/02963-2, CNPq 303853/2015-3 and Guggenheim Foundation), CM (CNPq 442374/2014-3 and FAPEMA UNIVERSAL-00358/15 - Edital 40/2014).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Barreto-Filho, J. A. S., Consolim-Colombo, F. M., Guerra-Riccio, G. M., Santos, R. D., Chacra, A. P., Lopes, H. F., et al. (2003). Hypercholesterolemia blunts forearm vasorelaxation and enhances the pressor response during acute systemic hypoxia. Aterioscler. Thromb. Vasc. Biol. 23, 1660–1666. doi: 10.1161/01.ATV.0000089471.61037.21
Böyum, A. (1968). Isolation of mononuclear cells and granulocytes from human blood. Isolation of mononuclear cells by one centrifugation, and of granulocytes by combining centrifugation and sedimentation at 1 g. Scand. J. Clin. Lab. Invest. 97, 77–89.
Cepeda, F. X., Toschi-Dias, E., Maki-Nunes, C., Rondon, M. U., Alves, M. J., Braga, A. M., et al. (2015). Obstructive sleep apnea impairs postexercise sympathovagal balance in patients with metabolic syndrome. Sleep 38, 1059–1066. doi: 10.5665/sleep.4812
Chan, S. H., Wu, K. L., Chang, A. Y., Tai, M. H., and Chan, J. Y. (2009). Oxidative impairment of mitochondrial electron transport chain complexes in rostral ventrolateral medulla contributes to neurogenic hypertension. Hypertension 53, 217–227. doi: 10.1161/HYPERTENSIONAHA.108.116905
Costa Rosa, L. F., Safi, D. A., Cury, Y., and Curi, R. (1992). Effect of epinephrine on glucose metabolism and hydrogen peroxide content in incubated rat macrophages. Biochem. Pharmacol. 44, 2235–2241.
Drager, L. F., Bortolotto, L. A., Lorenzi, M. C., Figueiredo, A. C., Krieger, E. M., and Lorenzi-Filho, G. (2005). Early signs of atherosclerosis in obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 172, 613–618. doi: 10.1164/rccm.200503-340OC
Drager, L. F., Li, J., Reinke, C., Bevans-Fonti, S., Jun, J. C., and Polotsky, V. Y. (2011a). Intermittent hypoxia exacerbates metabolic effects of diet-induced obesity. Obesity 19, 2167–2174. doi: 10.1038/oby.2011.240
Drager, L. F., Polotsky, V. Y., and Lorenzi-Filho, G. (2011b). Obstructive sleep apnea: an emerging risk factor for atherosclerosis. Chest 140, 534–542. doi: 10.1378/chest.10-2223
Fletcher, E. C., Lesske, J., Qian, W., Miller, C. C. III, and Unger, T. (1992). Repetitive, episodic hypoxia causes diurnal elevation of blood pressure in rats. Hypertension 19, 555–561.
Foster, G. E., Hanly, P. J., Ahmed, S. B., Beaudin, A. E., Pialoux, V., and Poulin, M. J. (2010). Intermittent hypoxia increases arterial blood pressure in humans through a Renin-Angiotensin system-dependent mechanism. Hypertension 56, 369–377. doi: 10.1161/HYPERTENSIONAHA.110.152108
Fu, Y., Xia, Y., Yi, H., Xu, H., Guan, J., and Yin, S. (2016). Is obstructive sleep apnea associated with cardiovascular and all-cause mortality? Sleep Breath. 8, e69432. doi: 10.1007/s11325-016-1393-1
Gilmartin, G. S., Lynch, M., Tamisier, R., and Weiss, J. W. (2010). Chronic intermittent hypoxia in humans during 28 nights results in blood pressure elevation and increased muscle sympathetic nerve activity. Am. J. Physiol. Heart Circ. Physiol. 299, H925–H931. doi: 10.1152/ajpheart.00253.2009
Grøgaard, B., Schurer, L., Gerdin, B., and Arfors, K. E. (1989). Delayed hypoperfusion after incomplete forebrain ischemia in the rat. The role of polymorphonuclear leukocytes. J. Cereb. Blood Flow Metab. 9, 500–505.
Hallenbeck, J. M., Dutka, A. J., Tanishima, T., Kochanek, P. M., Kumaroo, K. K., Thompson, C. B., et al. (1986). Polymorphonuclear leukocyte accumulation in brain regions with low blood flow during the early postischemic period. Stroke 17, 246–253.
Hatanaka, E., Levada-Pires, A. C., Pithon-Curi, T. C., and Curi, R. (2006). Systematic study on ROS production induced by oleic, linoleic, and γ-linolenic acids in human and rat neutrophils. Free Radic. Biol. Med. 41, 1124–1132. doi: 10.1016/j.freeradbiomed.2006.06.014
Iiyori, N., Alonso, L. C., Li, J., Sanders, M. H., Garcia-Ocana, A., O'Doherty, R. M., et al. (2007). Intermittent hypoxia causes insulin resistance in lean mice independent of autonomic activity. Am. J. Respir. Crit. Care Med. 175, 851–857. doi: 10.1164/rccm.200610-1527OC
Iversen, P. O., Stokland, A., Rolstad, B., and Benestad, H. B. (1994). Adrenaline-induced leucocytosis: recruitment of blood cells from rat spleen, bone marrow and lymphatics. Eur. J. Appl. Physiol. Occup. Physiol. 68, 219–227. doi: 10.1007/BF00376770
Jelic, S., Padeletti, M., Kawut, S. M., Higgins, C., Canfield, S. M., Onat, D., et al. (2008). Inflammation, oxidative stress, and repair capacity of the vascular endothelium in obstructive sleep apnea. Circulation 117, 2270–2278. doi: 10.1161/CIRCULATIONAHA.107.741512
Jun, J., Savransky, V., Nanayakkara, A., Bevans, S., Li, J., Smith, P. L., et al. (2008). Intermittent hypoxia has organ-specific effects on oxidative stress. Am. J. Physiol. Regul. Integr. Comp. Physiol. 295, R1274–R1281. doi: 10.1152/ajpregu.90346.2008
Kato, M., Roberts-Thomson, P., Phillips, B. G., Haynes, W. G., Winnicki, M., Accurso, V., et al. (2000). Impairment of endothelium-dependent vasodilation of resistance vessels in patients with obstructive sleep apnea. Circulation 102, 2607–2610. doi: 10.1161/01.CIR.102.21.2607
Laskin, D. L., Sunil, V. R., Gardner, C. R., and Laskin, J. D. (2011). Macrophages and tissue injury: agents of defense or destruction? Annu. Rev. Pharmacol. Toxicol. 51, 267–288. doi: 10.1146/annurev.pharmtox.010909.105812
Lavie, L. (2003). Obstructive sleep apnoea syndrome - an oxidative stress disorder. Sleep Med. Rev. 7, 35–51. doi: 10.1053/smrv.2002.0261
Lévy, P., Pépin, J. L., Arnaud, C., Tamisier, R., Borel, J. C., Dematteis, M., et al. (2008). Intermittent hypoxia and sleep-disordered breathing: current concepts and perspectives. Eur. Respir. J. 32, 1082–1095. doi: 10.1183/09031936.00013308
Li, J., Thorne, L. N., Punjabi, N. M., Sun, C.-K., Schwartz, A. R., Smith, P. L., et al. (2005). Intermittent hypoxia induces hyperlipidemia in lean mice. Circ Res. 30, 698–706. doi: 10.1161/01.RES.0000183879.60089.a9
Mello, P. R., Guerra, G. M., Borile, S., Rondon, M. U., Alves, M. J., Negrão, C. E., et al. (2012). Inspiratory muscle training reduces sympathetic nervous activity and improves inspiratory muscle weakness and quality of life in patients with chronic heart failure: a clinical trial. J. Cardiopulm. Rehabil. Prev. 32, 255–261. doi: 10.1097/HCR.0b013e31825828da
Monneret, D., Pepin, J. L, Godin-Ribuot, D., Ducros, V., Baguet, J. P., Levy, P., et al. (2010). Association of urinary 15-F2t-isoprostane level with oxygen desaturation and carotid intima-media thickness in nonobese sleep apnea patients. Free Radic. Biol. Med. 48, 619–625. doi: 10.1016/j.freeradbiomed.2009.12.008
Nagae, A., Fujita, M., Kawarazaki, H., Matsui, H., Ando, K., and Fujita, T. (2009). Sympathoexcitation by oxidative stress in the brain mediates arterial pressure elevation in obesity-induced hypertension. Circulation 119, 978–986. doi: 10.1161/CIRCULATIONAHA.108.824730
Pagani, M., Lombardi, F., Guzzetti, S., Rimoldi, O., Furlan, R., Pizzinelli, P., et al. (1986). Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ. Res. 59, 178–193.
Ryan, S., Taylor, C. T., and McNicholas, W. T. (2005). Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation 112, 2660–2667. doi: 10.1161/CIRCULATIONAHA.105.556746
Savransky, V., Nanayakkara, A., Li, J., Bevans, S., Smith, P. L, Rodriguez, A., et al. (2007). Chronic intermittent hypoxia induces atherosclerosis. Am. J. Respir. Crit. Care Med. 175, 1290–1297. doi: 10.1164/rccm.200612-1771OC
Schultz, H. D. (2009). Nitric oxide regulation of autonomic function in heart failure. Curr. Heart Fail. Rep. 6, 71–80. doi: 10.1007/s11897-009-0012-x
Schulz, R., Mahmoudi, S., Hattar, K., Sibelius, U., Olschewski, H., Mayer, K., et al. (2000). Enhanced release of superoxide from polymorphonuclear neutrophils in obstructive sleep apnea. Impact of continuous positive airway pressure therapy. Am. J. Respir. Crit. Care Med. 162, 566–570. doi: 10.1164/ajrccm.162.2.9908091
Tam, C. S., Wong, M., Tam, K., Aouad, L., and Waters, K. A. (2007). The effect of acute intermittent hypercapnic hypoxia treatment on IL-6, TNF-α, and CRP levels in piglets. Sleep 30, 723–727.
Tamisier, R., Pépin, J. L., Rémy, J., Baguet, J. P., Taylor, J. A., Weiss, J. W., et al. (2011). 14 nights of intermittent hypoxia elevate daytime blood pressure and sympathetic activity in healthy humans. Eur. Respir. J. 37, 119–128. doi: 10.1183/09031936.00204209
Tousoulis, D., Briasoulis, A., Papageorgiou, N., Tsioufis, C., Tsiamis, E., Toutouzas, K., et al. (2011). Oxidative stress and endothelial function: therapeutic interventions. Recent Pat. Cardiovasc. Drug Discov. 6, 103–114. doi: 10.2174/157489011795933819
Trombetta, I. C., Maki-Nunes, C., Toschi-Dias, E., Alves, M. J., Rondon, M. U., Cepeda, F. X., et al. (2013). Obstructive sleep apnea is associated with increased chemoreflex sensitivity in patients with metabolic syndrome. Sleep 36, 41–49. doi: 10.5665/sleep.2298
Trombetta, I. C., Somers, V. K., Maki-Nunes, C., Drager, L. F., Toschi-Dias, E., Alves, M. J., et al. (2010). Consequences of comorbid sleep apnea in the metabolic syndrome–implications for cardiovascular risk. Sleep 33, 1193–1199.
Yokoe, T., Minoguchi, K., Matsuo, H., Oda, N., Minoguchi, H., Yoshino, G., et al. (2003). Elevated levels of C-reactive protein and interleukin-6 in patients with obstructive sleep apnea syndrome are decreased by nasal continuous positive airway pressure. Circulation 107, 1129–1134. doi: 10.1161/01.CIR.0000052627.99976.18
Keywords: oxidative stress, sympathovagal balance, chemoreflex, O2 saturation, peripheral vascular resistance, blood pressure
Citation: Almeida GPL, Trombetta IC, Cepeda FX, Hatanaka E, Curi R, Mostarda C, Irigoyen MC, Barreto-Filho JAS, Krieger EM and Consolim-Colombo FM (2017) The Role of Acute Intermittent Hypoxia in Neutrophil-Generated Superoxide, Sympathovagal Balance, and Vascular Function in Healthy Subjects. Front. Physiol. 8:4. doi: 10.3389/fphys.2017.00004
Received: 11 November 2016; Accepted: 04 January 2017;
Published: 23 January 2017.
Edited by:
Tadej Debevec, Jožef Stefan Institute, SloveniaReviewed by:
Mark Christopher Fogarty, University of Hull, UKCopyright © 2017 Almeida, Trombetta, Cepeda, Hatanaka, Curi, Mostarda, Irigoyen, Barreto-Filho, Krieger and Consolim-Colombo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fernanda M. Consolim-Colombo, aGlwZmVybmFuZGFAaW5jb3IudXNwLmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.