 David Montero
David Montero Candela Diaz-Cañestro2
Candela Diaz-Cañestro2- 1Department of Cardiology, University Heart Center, University Hospital Zurich, Zurich, Switzerland
- 2Center for Molecular Cardiology, University of Zurich, Zurich, Switzerland
- 3Zurich Center for Integrative Human Physiology, Institute of Physiology, University of Zurich, Zurich, Switzerland
Introduction
Anemia, as defined by hemoglobin concentration < 12.0 and < 13.0 g/dl in women and men, respectively, affects more than 150 million elderly people worldwide and even when mild is associated with increased disability, morbidity, and mortality (Ezekowitz et al., 2003; Penninx et al., 2004; De Benoist et al., 2008). The causes of anemia remain unresolved in approximately one-third of anemic older individuals, commonly referred as unexplained anemia in the elderly (UAE; Guralnik et al., 2004). As most types of anemia, UAE is normocytic and its prevalence increases with advancing age (Guralnik et al., 2004). UAE is uniquely characterized by low plasma erythropoietin (EPO) concentration compared to the other forms of anemia (Ferrucci et al., 2007; Artz and Thirman, 2011). Thus, provided that EPO is mainly synthesized in the kidneys and its clearance/degradation is not enhanced, UAE may be primarily determined by factors affecting renal EPO production and/or hemodilution (Lundby et al., 2014; de Seigneux et al., 2016). These factors are yet to be elucidated. Of note, while hemoglobin concentration is typically employed to diagnose anemia, true (non-hemodilutional) anemia is defined as a decrease in the total volume of red blood cells (RBCV) and/or hemoglobin mass. Herein, we present arguments to support the contention that a fundamental hallmark of vascular aging, arterial stiffness (AS), might be a primary etiological determinant of low EPO concentration and RBCV in UAE via the impairment of mechanisms regulating kidney perfusion, EPO production as well as blood volume. This viewpoint postulates that AS is augmented in UAE patients compared with healthy non-anemic elderly individuals. While direct proof is not available at present, independent lines of evidence demonstrate that UAE is characterized by alterations in biochemical, hematological, and physiological parameters consistently associated with AS (Ferrucci et al., 2007; Robinson et al., 2007; Artz et al., 2014; Malahfji et al., 2014), whereof some are described in detail below.
Association between Arterial Stiffness (AS) and the Total Volume of Red Blood Cells (RBCV)
AS characterizes the reduced capacity of an artery to expand and recoil in response to changes in blood pressure. When assessed in central elastic arteries (e.g., carotid), AS independently predicts incident cardiovascular events, kidney disease, and all-cause mortality (Hashimoto and Ito, 2011; van Sloten et al., 2014). Sedentary aging is inexorably associated with a linear or exponential increase in AS (Avolio et al., 1983; Mitchell et al., 2004; McEniery et al., 2005), possibly reflecting the gradual fragmentation of elastin fibers due to repetitive cyclic stress as well as the simultaneous accumulation of collagen fibers in the media layer of elastic arteries (O'Rourke and Hashimoto, 2007; Camici et al., 2015). Nonetheless, there is substantial variability in the degree of arterial stiffening with advancing age (Avolio et al., 1983). For instance, older individuals regularly involved in endurance training may present similar low levels of AS than healthy young controls (Vaitkevicius et al., 1993; Tanaka et al., 1998). These elderly endurance-trained individuals also exhibit a preserved blood volume and RBCV, both declining with age in sedentary adults (Jones et al., 1997). The increase in RBCV commonly observed with endurance training in healthy individuals has been proposed to be partially related to frequent reductions in central (intrathoracic) venous pressure (CVP) stimulating EPO synthesis after each exercise bout (Kirsch et al., 2005; Montero et al., 2015), in line with the basal (non-hypoxic) regulation of EPO production as outlined in the next section. Parenthetically, RBCV is the main determinant of cardiorespiratory capacity (Montero et al., 2015), which in turn is inversely associated with AS irrespective of age status (Vaitkevicius et al., 1993; Ferreira et al., 2003; Kitzman et al., 2013). Thus, it is reasonable to expect a negative relationship between AS and RBCV, and this has been recently confirmed experimentally (Montero et al., 2016a). Specifically, carotid AS and carotid-ankle pulse wave velocity are strongly and negatively associated (r ≥ −0.62) with total hemoglobin mass, RBCV, and blood volume independently of body weight and gender in healthy adults (Montero et al., 2016a). In addition, augmentation index, an indirect measure of AS, has been negatively related to blood hemoglobin concentration in a cohort of individuals presenting with diabetes alone or along with anemia (Demir et al., 2015). It should be noted, however, that statistical associations do not necessarily infer strict causal relationships. Both AS and impaired erythropoiesis could be caused by a common underlying process, e.g., an age-related increase in circulating pro-inflammatory cytokines (Makipour et al., 2008; Artz et al., 2014), which may hinder proliferation and differentiation of erythroid progenitor cells independently of circulating EPO levels (Means, 1995; Selleri et al., 1996). Acknowledging this uncertainty, multiple linear correlative evidence impelled us to ponder whether AS-related mechanisms may adversely influence the regulation of erythropoiesis and explain, at least in part, the uncertain pathophysiology of UAE.
Regulation of Erythropoietin (EPO) Synthesis Through Blood Volume Feedback Mechanisms
It is beyond dispute that tissue hypoxia in peritubular fibroblast-like cells of the renal cortex stimulates the synthesis of EPO upon stabilization of hypoxia-inducible factor-2α (Jelkmann, 2011). However, additional non-hypoxic feedback mechanisms must also regulate EPO production since arterial O2 partial pressure and renal blood flow/O2 consumption seldom fluctuate to values required to substantially increase the synthesis of EPO in healthy individuals (Halperin et al., 2006; Perez-Padilla et al., 2006). Among potential non-hypoxic factors related to erythropoiesis, EPO concentrations run inversely to CVP, a variable reflecting the filling state of the cardiovascular system (Ehmke et al., 1995; Gunga et al., 1996; Breymann et al., 2000). In this respect, early animal studies observed a 1.5-fold acute increase in plasma EPO levels following a reduction of blood volume (20%) and CVP while hematocrit was unaltered (Ehmke et al., 1995). In humans, hypervolemic hemodilution increasing CVP paralleled a decrease in circulating EPO seemingly beyond the dilution effect (Breymann et al., 2000). Recently, plasma EPO concentration was found increased independent of hemoconcentration, with moderate head-up tilt redistributing blood toward the lower limbs and thereby reducing CVP (Montero et al., 2016b). Overall, these studies suggest that CVP per-se could be a regulator of EPO production.
The specific mechanism(s) explaining the link between CVP and EPO synthesis has yet to be established. Nonetheless, changes in EPO concentration in response to variations in CVP resembles the pattern of hormones governing blood volume such as those pertaining to the renin-angiotensin-aldosterone system (RAAS) as well as natriuretic peptides and vasopressin (VPN; Gauer and Henry, 1963). These hormones regulate blood volume through feedback loops including veno-atrial and arterial baroreceptors (Gauer and Henry, 1963). Interestingly, angiotensin II (ANGII) and VPN stimulate EPO synthesis in vivo independently of kidney tissue hypoxia (Engel and Pagel, 1995; Kim et al., 2014), and are augmented when CVP is decreased (Segar and Moore, 1968; Egan et al., 1984; Bie et al., 1986; Sander-Jensen et al., 1986). Accordingly, the production of EPO has been proposed to be regulated under basal (non-kidney hypoxic) conditions by blood volume-regulating hormones (Kirsch et al., 2005). Hence, EPO synthesis and therefore erythropoiesis could be affected by alterations in hemodynamic and endocrine feedback pathways that control blood volume.
Potential Mechanisms Linking Arterial Stiffness (AS) and Low Erythropoietin (EPO) Concentration in Unexplained Anemia in the Elderly (UAE) (Figure 1)
Altered Baroreflex Sensitivity (BRS) and Stimulated Release of Blood Volume-Regulating Hormones
Baroreflex sensitivity (BRS) declines progressively with age and is primarily associated with the compliance of central elastic arteries in which high-pressure baroreceptors are located (aortic arch and carotid arteries; Monahan et al., 2001a). This is only natural given that baroreceptor firing rate is proportional to changes in arterial circumference (Kingwell et al., 1995). Monahan et al. demonstrated that carotid compliance independently explains the majority of the variance of BRS across the lifespan (Monahan et al., 2001a). Moreover, age-related reduction in BRS is largely attenuated by endurance training (Monahan et al., 2000, 2001a,b), which concurs with the aforementioned observations regarding AS and hematological variables. Taking into account that arterial baroreceptors control the secretion of blood volume-regulating hormones such as VPN (Thrasher, 1994; Thrasher and Keil, 1998), this could be affected by AS. In this regard, increased arterial pulse pressure, a common correlate of AS and impaired BRS (Virtanen et al., 2004), decreases the release of VPN even in the absence of changes in mean arterial pressure (Gabrielsen et al., 2000). In this line, aging has been associated with a blunted VPN release in response to conditions associated with reduced CVP such as acute post-exercise hypotension (Kirsch et al., 1986; Halliwill et al., 2000; Keck et al., 2000). Importantly, the increase in EPO concentration induced by decreasing CVP is abolished when adjusted for the concomitant increase in copeptin (Montero et al., 2016b), a marker of VPN (Morgenthaler et al., 2008). Indeed, changes in copeptin with experimental manipulation of CVP independently explained simultaneously occurring changes in EPO concentration in healthy adults (Montero et al., 2016b). Furthermore, VPN administration is associated with increased plasma EPO levels and red cell mass in hypopituitaric patients (Jepson et al., 1968). As for the underlying mechanisms, animal studies demonstrated that VPN directly induces EPO secretion through the activation of V1a receptors (Engel and Pagel, 1995), which are expressed in the renal cortex and medulla and mediate the vasopressor effect of VPN (Gózdz et al., 2002; Koshimizu et al., 2006). Therefore, whilst speculative, the characteristic low EPO concentration in UAE could be attributed, at least in part, to reduced VPN release secondary to AS and impaired BRS. The rate of VPN delivery to kidney target cells depends, in addition to plasma VPN concentration and plasma volume, on renal blood flow, which leads us to the next potential mechanisms linking AS and UAE.
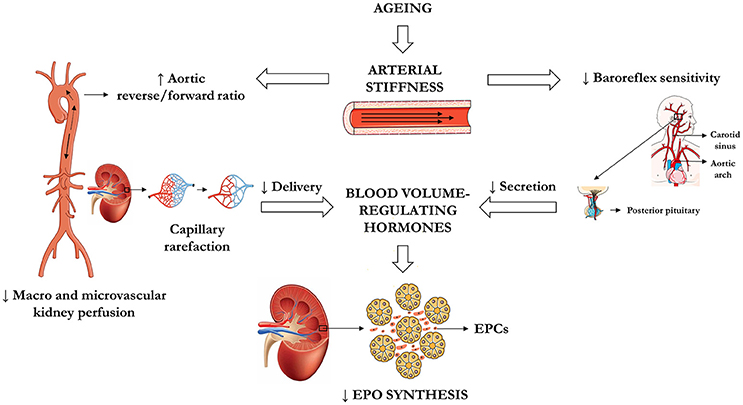
Figure 1. Central hypothesis linking arterial stiffness in central elastic arteries and low EPO concentration in UAE. EPCs, epo-producing cells; EPO, erythropoietin; UAE, unexplained anemia in the elderly.
Altered Renal Blood Flow
The relationship between AS and kidney function is amply acknowledged in the literature (Safar et al., 2004; O'Rourke and Safar, 2005; Ford et al., 2010). Central to this relationship is the inherent loss of the elastic recoil (Windkessel function) in the descending aorta, which supplies blood to the kidneys. The higher the degree of aortic stiffening, the greater is the aortic upstream (reverse) flow in early diastole (Hashimoto and Ito, 2013). Kidney perfusion and thereby glomerular filtration rate (GFR) are reduced according to the increase in aortic flow reversal, independent of cardiac output (Hashimoto and Ito, 2015). In fact, the aortic reverse/forward flow ratio is the strongest determinant of estimated GFR as well as renal blood flow, and mediates the association of AS with GFR in hypertensive patients (Hashimoto and Ito, 2015). In individuals with UAE, a low estimated GFR (≤ 60 mL·min·1.73 m2) seems prevalent (Robinson et al., 2007; Artz et al., 2014), possibly reflecting a concomitant reduction in renal blood flow considering its expected association with GFR (Lebkowska et al., 2007; Hashimoto and Ito, 2015). Consequently, AS may lead to a specific reduction of blood flow to the kidneys, thus diminish the delivery of blood-volume regulating hormones and as a direct consequence hereof affect EPO synthesis.
Impaired Tissue Perfusion
One of the most clinically relevant outcomes derived from AS is the increase in blood pressure pulse amplitude (Struijker-Boudier, 2009). The augmented pulsatility primarily impacts on the smallest arteries and arterioles, i.e., the resistance vasculature. When the increase in pulse pressure is maintained, adverse phenotypic changes are commonly observed, particularly in vascular beds characterized by low resistance such as the renal microcirculation (Mitchell, 2008; Woodard et al., 2015). These microvascular alterations include increased media-to-lumen ratio, decreased arteriolar diameter, and capillary rarefaction, among others (Levy et al., 2001). In this respect, an increased vascular resistance and reduced arterial volume in the renal cortex explain the negative association between renal artery pulsatility index (PI) and GFR in older adults (Woodard et al., 2015). Furthermore, the association between AS, pulse pressure and microvascular abnormalities is not a one-way relationship, in that the latter may contribute to AS and pulse pressure, leading to a vicious circle (Struijker-Boudier, 2009). Not surprisingly, impaired tissue perfusion is common to diseases characterized by AS such as hypertension, obesity, diabetes mellitus, and aging per-se (Delp et al., 1998; Levy et al., 2008). Hence, AS could cause a specific reduction in the microvascular perfusion of peritubular fibroblast-like cells of the renal cortex (i.e., kidney EPO-producing cells; Jelkmann, 2011), thus being another contributing factor to low EPO concentration in UAE.
Conclusion
Among all types of anemia, the most prevalent, UAE, remain currently unexplained (Artz and Thirman, 2011). In this viewpoint, we have highlighted the plausibly overlooked role of AS, a well-known feature of the vascular aging process, as a primary contributing factor to the typical low EPO concentration observed in UAE. Underlying mechanisms are proposed to include the impairment of endocrine feedback pathways governing the basal regulation of kidney EPO synthesis as well as renal perfusion. In particular, AS in central elastic arteries leading to baroreceptor dysfunction may hinder the release of blood volume-regulating hormones directly stimulating EPO synthesis. Moreover, AS is closely linked with the reduction of renal blood flow and microvascular perfusion contributing to impaired hormone delivery to EPO-producing cells. While the rationale underlying the potential impact of AS on the etiology of UAE is based on fundamental hemodynamic and endocrine (dys) regulation, its specific relevance to UAE will have to be established in future studies. These may yield relevant insights for novel and effective therapeutic targets in the treatment of UAE.
Author Contributions
DM drafted the manuscript. DM, CD, AF, and CL critically revised the manuscript for important intellectual content, and approved the final the version to be published.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Artz, A. S., and Thirman, M. J. (2011). Unexplained anemia predominates despite an intensive evaluation in a racially diverse cohort of older adults from a referral anemia clinic. J. Gerontol. A Biol. Sci. Med. Sci. 66, 925–932. doi: 10.1093/gerona/glr090
Artz, A. S., Xue, Q. L., Wickrema, A., Hesdorffer, C., Ferrucci, L., Langdon, J. M., et al. (2014). Unexplained anaemia in the elderly is characterised by features of low grade inflammation. Br. J. Haematol. 167, 286–289. doi: 10.1111/bjh.12984
Avolio, A. P., Chen, S. G., Wang, R. P., Zhang, C. L., Li, M. F., and O'Rourke, M. F. (1983). Effects of aging on changing arterial compliance and left ventricular load in a northern Chinese urban community. Circulation 68, 50–58. doi: 10.1161/01.CIR.68.1.50
Bie, P., Secher, N. H., Astrup, A., and Warberg, J. (1986). Cardiovascular and endocrine responses to head-up tilt and vasopressin infusion in humans. Am. J. Physiol. 251, R735–R741.
Breymann, C., Rohling, R., Huch, A., and Huch, R. (2000). Intraoperative endogenous erythropoietin levels and changes in intravascular blood volume in healthy humans. Ann. Hematol. 79, 183–186. doi: 10.1007/s002770050577
Camici, G. G., Savarese, G., Akhmedov, A., and Lüscher, T. F. (2015). Molecular mechanism of endothelial and vascular aging: implications for cardiovascular disease. Eur. Heart J. 36, 3392–3403. doi: 10.1093/eurheartj/ehv587
De Benoist, B., McLean, E., Egli, I., and Cogswell, M. (eds.). (2008). “Worldwide prevalence of anaemia 1993–2005,” in WHO Global Database on Anaemia (Geneva: W.H. Organization), 7–12.
Delp, M. D., Evans, M. V., and Duan, C. (1998). Effects of aging on cardiac output, regional blood flow, and body composition in Fischer-344 rats. J. Appl. Physiol. 85, 1813–1822.
Demir, B. K., Sezer, S. D., Topaloğlu, O., Taşkıran, E., Işık, B., Soyaltın, U. E., et al. (2015). The relationship between nephropathy, retinopathy, obesity and arterial stiffness in type 2 diabetes mellitus. FNG Bilim Tip Dergisi 1, 59–67. doi: 10.5606/fng.btd.2015.012
de Seigneux, S., Lundby, A. M., Berchtold, L., Berg, A. H., Saudan, P., and Lundby, C. (2016). Increased synthesis of liver erythropoietin with CKD. J. Am. Soc. Nephrol. 27, 2265–2269. doi: 10.1681/asn.2015050508
Egan, B., Grekin, R., Ibsen, H., Osterziel, K., and Julius, S. (1984). Role of cardiopulmonary mechanoreceptors in ADH release in normal humans. Hypertension 6, 832–836. doi: 10.1161/01.HYP.6.6.832
Ehmke, H., Just, A., Eckardt, K. U., Persson, P. B., Bauer, C., and Kirchheim, H. R. (1995). Modulation of erythropoietin formation by changes in blood volume in conscious dogs. J. Physiol. 488(Pt 1), 181–191. doi: 10.1113/jphysiol.1995.sp020956
Engel, A., and Pagel, H. (1995). Increased production of erythropoietin after application of antidiuretic hormone. A consequence of renal vasoconstriction? Exp. Clin. Endocrinol. Diabetes 103, 303–307. doi: 10.1055/s-0029-1211370
Ezekowitz, J. A., McAlister, F. A., and Armstrong, P. W. (2003). Anemia is common in heart failure and is associated with poor outcomes: insights from a cohort of 12 065 patients with new-onset heart failure. Circulation 107, 223–225. doi: 10.1161/01.CIR.0000052622.51963.FC
Ferreira, I., Twisk, J. W., Stehouwer, C. D., van Mechelen, W., and Kemper, H. C. (2003). Longitudinal changes in.VO2max: associations with carotid IMT and arterial stiffness. Med. Sci. Sports Exerc. 35, 1670–1678. doi: 10.1249/01.MSS.0000089247.37563.4B
Ferrucci, L., Guralnik, J. M., Bandinelli, S., Semba, R. D., Lauretani, F., Corsi, A., et al. (2007). Unexplained anaemia in older persons is characterised by low erythropoietin and low levels of pro-inflammatory markers. Br. J. Haematol. 136, 849–855. doi: 10.1111/j.1365-2141.2007.06502.x
Ford, M. L., Tomlinson, L. A., Chapman, T. P., Rajkumar, C., and Holt, S. G. (2010). Aortic stiffness is independently associated with rate of renal function decline in chronic kidney disease stages 3 and 4. Hypertension 55, 1110–1115. doi: 10.1161/HYPERTENSIONAHA.109.143024
Gabrielsen, A., Warberg, J., Christensen, N. J., Bie, P., Stadeager, C., Pump, B., et al. (2000). Arterial pulse pressure and vasopressin release during graded water immersion in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 278, R1583–R1588.
Gauer, O. H., and Henry, J. P. (1963). Circulatory basis of fluid volume control. Physiol. Rev. 43, 423–481.
Gózdz, A., Szczepanska-Sadowska, E., Szczepanska, K., Maslinski, W., and Luszczyk, B. (2002). Vasopressin V1a, V1b and V2 receptors mRNA in the kidney and heart of the renin transgenic TGR(mRen2)27 and Sprague Dawley rats. J. Physiol. Pharmacol. 53, 349–357.
Gunga, H. C., Kirsch, K., Baartz, F., Maillet, A., Gharib, C., Nalishiti, W., et al. (1996). Erythropoietin under real and simulated microgravity conditions in humans. J. Appl. Physiol. 81, 761–773.
Guralnik, J. M., Eisenstaedt, R. S., Ferrucci, L., Klein, H. G., and Woodman, R. C. (2004). Prevalence of anemia in persons 65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood 104, 2263–2268. doi: 10.1182/blood-2004-05-1812
Halliwill, J. R., Minson, C. T., and Joyner, M. J. (2000). Effect of systemic nitric oxide synthase inhibition on postexercise hypotension in humans. J. Appl. Physiol. 89, 1830–1836.
Halperin, M. L., Cheema-Dhadli, S., Lin, S. H., and Kamel, K. S. (2006). Properties permitting the renal cortex to be the oxygen sensor for the release of erythropoietin: clinical implications. Clin. J. Am. Soc. Nephrol. 1, 1049–1053. doi: 10.2215/CJN.00100106
Hashimoto, J., and Ito, S. (2011). Central pulse pressure and aortic stiffness determine renal hemodynamics: pathophysiological implication for microalbuminuria in hypertension. Hypertension 58, 839–846. doi: 10.1161/HYPERTENSIONAHA.111.177469
Hashimoto, J., and Ito, S. (2013). Aortic stiffness determines diastolic blood flow reversal in the descending thoracic aorta: potential implication for retrograde embolic stroke in hypertension. Hypertension 62, 542–549. doi: 10.1161/HYPERTENSIONAHA.113.01318
Hashimoto, J., and Ito, S. (2015). Aortic blood flow reversal determines renal function: potential explanation for renal dysfunction caused by aortic stiffening in hypertension. Hypertension 66, 61–67. doi: 10.1161/HYPERTENSIONAHA.115.05236
Jelkmann, W. (2011). Regulation of erythropoietin production. J. Physiol. (Lond) 589, 1251–1258. doi: 10.1113/jphysiol.2010.195057
Jepson, J. H., McGarry, E. E., and Lowenstein, L. (1968). Erythropoietin excretion in a hypopituitary patient. Effects of testosterone and vasopressin. Arch. Intern. Med. 122, 265–270. doi: 10.1001/archinte.1968.00300080073014
Jones, P. P., Davy, K. P., Desouza, C. A., van Pelt, R. E., and Seals, D. R. (1997). Absence of age-related decline in total blood volume in physically active females. Am. J. Physiol. 272, H2534–H2540.
Keck, M. E., Hatzinger, M., Wotjak, C. T., Landgraf, R., Holsboer, F., and Neumann, I. D. (2000). Ageing alters intrahypothalamic release patterns of vasopressin and oxytocin in rats. Eur. J. Neurosci. 12, 1487–1494. doi: 10.1046/j.1460-9568.2000.00030.x
Kim, Y. C., Mungunsukh, O., McCart, E. A., Roehrich, P. J., Yee, D. K., and Day, R. M. (2014). Mechanism of erythropoietin regulation by angiotensin II. Mol. Pharmacol. 85, 898–908. doi: 10.1124/mol.113.091157
Kingwell, B. A., Cameron, J. D., Gillies, K. J., Jennings, G. L., and Dart, A. M. (1995). Arterial compliance may influence baroreflex function in athletes and hypertensives. Am. J. Physiol. 268, H411–H418.
Kirsch, K. A., Röcker, L., von Ameln, H., and Hrynyschyn, K. (1986). The cardiac filling pressure following exercise and thermal stress. Yale J. Biol. Med. 59, 257–265.
Kirsch, K. A., Schlemmer, M., De Santo, N. G., Cirillo, M., Perna, A., and Gunga, H. C. (2005). Erythropoietin as a volume-regulating hormone: an integrated view. Semin. Nephrol. 25, 388–391. doi: 10.1016/j.semnephrol.2005.05.007
Kitzman, D. W., Herrington, D. M., Brubaker, P. H., Moore, J. B., Eggebeen, J., and Haykowsky, M. J. (2013). Carotid arterial stiffness and its relationship to exercise intolerance in older patients with heart failure and preserved ejection fraction. Hypertension 61, 112–119. doi: 10.1161/HYPERTENSIONAHA.111.00163
Koshimizu, T. A., Nasa, Y., Tanoue, A., Oikawa, R., Kawahara, Y., Kiyono, Y., et al. (2006). V1a vasopressin receptors maintain normal blood pressure by regulating circulating blood volume and baroreflex sensitivity. Proc. Natl. Acad. Sci. U.S.A. 103, 7807–7812. doi: 10.1073/pnas.0600875103
Lebkowska, U., Malyszko, J., Lebkowski, W., Brzósko, S., Kowalewski, R., Lebkowski, T., et al. (2007). The predictive value of arterial renal blood flow parameters in renal graft survival. Transplant. Proc. 39, 2727–2729. doi: 10.1016/j.transproceed.2007.08.043
Levy, B. I., Ambrosio, G., Pries, A. R., and Struijker-Boudier, H. A. (2001). Microcirculation in hypertension: a new target for treatment? Circulation 104, 735–740. doi: 10.1161/hc3101.091158
Levy, B. I., Schiffrin, E. L., Mourad, J. J., Agostini, D., Vicaut, E., Safar, M. E., et al. (2008). Impaired tissue perfusion: a pathology common to hypertension, obesity, and diabetes mellitus. Circulation 118, 968–976. doi: 10.1161/CIRCULATIONAHA.107.763730
Lundby, A. K., Keiser, S., Siebenmann, C., Schäffer, L., and Lundby, C. (2014). Kidney-synthesized erythropoietin is the main source for the hypoxia-induced increase in plasma erythropoietin in adult humans. Eur. J. Appl. Physiol. 114, 1107–1111. doi: 10.1007/s00421-014-2844-7
Makipour, S., Kanapuru, B., and Ershler, W. B. (2008). Unexplained anemia in the elderly. Semin. Hematol. 45, 250–254. doi: 10.1053/j.seminhematol.2008.06.003
Malahfji, M., Al Mheid, I., Uphoff, I., Cunningham, L., Martin, G. S., and Quyyumi, A. (2014). Neutrophil to lymphocyte ratio and measures of systemic inflammation are associated with arterial stiffness in healthy humans. J. Am. Coll. Cardiol. 63. doi: 10.1016/S0735-1097(14)62103-3
McEniery, C. M., Yasmin Hall, I. R., Qasem, A., Wilkinson, I. B., Cockcroft, J. R., et al. (2005). Normal vascular aging: differential effects on wave reflection and aortic pulse wave velocity: the Anglo-Cardiff Collaborative Trial (ACCT). J. Am. Coll. Cardiol. 46, 1753–1760. doi: 10.1016/j.jacc.2005.07.037
Means, R. T. Jr. (1995). Pathogenesis of the anemia of chronic disease: a cytokine-mediated anemia. Stem Cells 13, 32–37. doi: 10.1002/stem.5530130105
Mitchell, G. F. (2008). Effects of central arterial aging on the structure and function of the peripheral vasculature: implications for end-organ damage. J. Appl. Physiol. 105, 1652–1660. doi: 10.1152/japplphysiol.90549.2008
Mitchell, G. F., Parise, H., Benjamin, E. J., Larson, M. G., Keyes, M. J., Vita, J. A., et al. (2004). Changes in arterial stiffness and wave reflection with advancing age in healthy men and women: the Framingham Heart Study. Hypertension 43, 1239–1245. doi: 10.1161/01.HYP.0000128420.01881.aa
Monahan, K. D., Dinenno, F. A., Seals, D. R., Clevenger, C. M., Desouza, C. A., and Tanaka, H. (2001a). Age-associated changes in cardiovagal baroreflex sensitivity are related to central arterial compliance. Am. J. Physiol. Heart Circ. Physiol. 281, H284–H289.
Monahan, K. D., Dinenno, F. A., Tanaka, H., Clevenger, C. M., DeSouza, C. A., and Seals, D. R. (2000). Regular aerobic exercise modulates age-associated declines in cardiovagal baroreflex sensitivity in healthy men. J. Physiol. 529(Pt 1), 263–271. doi: 10.1111/j.1469-7793.2000.00263.x
Monahan, K. D., Tanaka, H., Dinenno, F. A., and Seals, D. R. (2001b). Central arterial compliance is associated with age- and habitual exercise-related differences in cardiovagal baroreflex sensitivity. Circulation 104, 1627–1632. doi: 10.1161/hc3901.096670
Montero, D., Cathomen, A., Jacobs, R. A., Flück, D., de Leur, J., Keiser, S., et al. (2015). Haematological rather than skeletal muscle adaptations contribute to the increase in peak oxygen uptake induced by moderate endurance training. J. Physiol. (Lond) 593, 4677–4688. doi: 10.1113/JP270250
Montero, D., Diaz-Cañestro, C., Keiser, S., and Lundby, C. (2016a). Arterial stiffness is strongly and negatively associated with the total volume of red blood cells. Int. J. Cardiol. 221, 77–80. doi: 10.1016/j.ijcard.2016.06.265
Montero, D., Rauber, S., Goetze, J. P., and Lundby, C. (2016b). Reduction in central venous pressure enhances erythropoietin synthesis: role of volume-regulating hormones. Acta Physiol. (Oxf). 218, 89–97. doi: 10.1111/apha.12708
Morgenthaler, N. G., Struck, J., Jochberger, S., and Dünser, M. W. (2008). Copeptin: clinical use of a new biomarker. Trends Endocrinol. Metab. 19, 43–49. doi: 10.1016/j.tem.2007.11.001
O'Rourke, M. F., and Hashimoto, J. (2007). Mechanical factors in arterial aging: a clinical perspective. J. Am. Coll. Cardiol. 50, 1–13. doi: 10.1016/j.jacc.2006.12.050
O'Rourke, M. F., and Safar, M. E. (2005). Relationship between aortic stiffening and microvascular disease in brain and kidney: cause and logic of therapy. Hypertension 46, 200–204. doi: 10.1161/01.HYP.0000168052.00426.65
Penninx, B. W., Pahor, M., Cesari, M., Corsi, A. M., Woodman, R. C., Bandinelli, S., et al. (2004). Anemia is associated with disability and decreased physical performance and muscle strength in the elderly. J. Am. Geriatr. Soc. 52, 719–724. doi: 10.1111/j.1532-5415.2004.52208.x
Perez-Padilla, R., Torre-Bouscoulet, L., Muiño, A., Marquez, M. N., Lopez, M. V., De Oca, M. M., et al. (2006). Prevalence of oxygen desaturation and use of oxygen at home in adults at sea level and at moderate altitude. Eur. Respir. J. 27, 594–599. doi: 10.1183/09031936.06.00075005
Robinson, B., Artz, A. S., Culleton, B., Critchlow, C., Sciarra, A., and Audhya, P. (2007). Prevalence of anemia in the nursing home: contribution of chronic kidney disease. J. Am. Geriatr. Soc. 55, 1566–1570. doi: 10.1111/j.1532-5415.2007.01389.x
Safar, M. E., London, G. M., and Plante, G. E. (2004). Arterial stiffness and kidney function. Hypertension 43, 163–168. doi: 10.1161/01.HYP.0000114571.75762.b0
Sander-Jensen, K., Secher, N. H., Astrup, A., Christensen, N. J., Giese, J., Schwartz, T. W., et al. (1986). Hypotension induced by passive head-up tilt: endocrine and circulatory mechanisms. Am. J. Physiol. 251, R742–R748.
Segar, W. E., and Moore, W. W. (1968). The regulation of antidiuretic hormone release in man: I. Effects of change in position and ambient temperature on blood ADH levels. J. Clin. Invest. 47, 2143–2151. doi: 10.1172/JCI105900
Selleri, C., Maciejewski, J. P., Sato, T., and Young, N. S. (1996). Interferon-gamma constitutively expressed in the stromal microenvironment of human marrow cultures mediates potent hematopoietic inhibition. Blood 87, 4149–4157.
Struijker-Boudier, H. A. J. (2009). The burden of vascular disease in diabetes and hypertension: from micro- to macrovascular disease–the “bad loop”. Medicographia 31, 251–256.
Tanaka, H., DeSouza, C. A., and Seals, D. R. (1998). Absence of age-related increase in central arterial stiffness in physically active women. Arterioscler. Thromb. Vasc. Biol. 18, 127–132. doi: 10.1161/01.ATV.18.1.127
Thrasher, T. N. (1994). Baroreceptor regulation of vasopressin and renin secretion: low-pressure versus high-pressure receptors. Front. Neuroendocrinol. 15, 157–196. doi: 10.1006/frne.1994.1007
Thrasher, T. N., and Keil, L. C. (1998). Arterial baroreceptors control blood pressure and vasopressin responses to hemorrhage in conscious dogs. Am. J. Physiol. 275, R1843–R1857.
Vaitkevicius, P. V., Fleg, J. L., Engel, J. H., O'Connor, F. C., Wright, J. G., Lakatta, L. E., et al. (1993). Effects of age and aerobic capacity on arterial stiffness in healthy adults. Circulation 88, 1456–1462. doi: 10.1161/01.CIR.88.4.1456
van Sloten, T. T., Schram, M. T., Van Den Hurk, K., Dekker, J. M., Nijpels, G., Henry, R. M., et al. (2014). Local stiffness of the carotid and femoral artery is associated with incident cardiovascular events and all-cause mortality: the Hoorn study. J. Am. Coll. Cardiol. 63, 1739–1747. doi: 10.1016/j.jacc.2013.12.041
Virtanen, R., Jula, A., Huikuri, H., Kuusela, T., Helenius, H., Ylitalo, A., et al. (2004). Increased pulse pressure is associated with reduced baroreflex sensitivity. J. Hum. Hypertens. 18, 247–252. doi: 10.1038/sj.jhh.1001661
Keywords: arterial stiffness, erythropoietin, blood volume, anemia
Citation: Montero D, Diaz-Cañestro C, Flammer A and Lundby C (2016) Unexplained Anemia in the Elderly: Potential Role of Arterial Stiffness. Front. Physiol. 7:485. doi: 10.3389/fphys.2016.00485
Received: 06 September 2016; Accepted: 10 October 2016;
Published: 25 October 2016.
Edited by:
Kari Kalliokoski, University of Turku, FinlandReviewed by:
Dietmar Fuchs, Innsbruck Medical University, AustriaCopyright © 2016 Montero, Diaz-Cañestro, Flammer and Lundby. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Montero, ZGF2aWQubW9udGVyby5iYXJyaWxAZ21haWwuY29t