 Yueyang Huang
Yueyang Huang Hongmei Yuan*
Hongmei Yuan* Zhe Huang
Zhe Huang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 11 March 2025
Sec. Drugs Outcomes Research and Policies
Volume 16 - 2025 | https://doi.org/10.3389/fphar.2025.1546018
Background: Fabry disease (FD) is an X-chromosome-linked genetic disorder. Currently, the main treatments for FD include disease-nonspecific and disease-specific treatments. Nonspecific treatment involves symptomatic management of organ involvement. On the other hand, disease-specific treatment is to regulate the activity of the corresponding enzymes, which is targeted. Among them, enzyme replacement therapy (ERT) is a classical therapy. Several studies have demonstrated the significant ameliorative effect of agalactosidase-α (ALTA-a) on cardiac and renal function in patients with FD. Despite the excellent clinical performance, there are limited pharmacoeconomic studies on ERT for FD worldwide.
Objective: The aim of this study was to analyze the cost-effectiveness of ERT for FD in China from the perspective of the healthcare system.
Methods: We constructed a five-state Markov model based on the disease characteristics of FD. The modeling period was 1 month. The time horizon was 3 years. The willingness-to-pay threshold was chosen as 1-3 times the gross national product (GDP) per capita. The incremental cost-effectiveness ratio (ICER) was calculated from the base case analysis, and one-way sensitivity analysis and probabilistic sensitivity analysis were performed.
Results: The ICER value is ¥148071.95/QALY, which is between 1-3 times GDP per capita. The sensitivity analysis showed that the cost of ALTA-a had a significant effect on ICER and proved the stability of the results.
Conclusion: ERT therapy is a cost-effective program compared to “No ERT” therapy.
Fabry disease (FD), also known as Anderson-Fabry disease, is an X-chromosome-linked genetic disorder. It is a multisystem, progressive lysosomal storage disorder caused primarily by mutations in the galactosidase alpha (GLA) gene (Spada et al., 2006). As the second most prevalent lysosomal storage disease to date after Gaucher disease (Mallett et al., 2020), the population prevalence of FD ranges from 1/117,000 to 1/40,000 (Vardarli et al., 2020), and in newborns this value ranges from 1/8882 to 1/1250 (Linhart et al., 2020). The pathogenesis of FD is a partial or total loss of α-galactosidase A (α-Gal A) activity due to mutations in the GLA gene, resulting in the accumulation of large amounts of its metabolic substrate in various organs and tissues of the body, causing a series of organ pathologies to occur (Vardarli et al., 2020). Without timely and effective treatment, patients often die due to serious complications such as renal failure, heart failure, cardiac arrhythmia and stroke (Turkmen and Baloglu, 2020). As a rare disease typically inherited from the X chromosome, male patients with FD are more likely to develop symptoms of the disease and the above complications more readily and earlier compared to females (Turkmen and Baloglu, 2020). Life expectancy has been reported to be reduced by 15–20 years for male patients with FD and 6–10 years for female patients (Hagège et al., 2019). The therapeutic goals of FD are to slow disease progression, improve quality of life, reduce the incidence of associated complications, and prolong patient survival. Currently, the main treatments for FD include disease non-specific and disease-specific treatments. Non-specific treatment refers to the treatment of specific symptoms, such as renal lesions, cardiac lesions and neurological symptoms, etc. This type of treatment can effectively relieve the symptoms, but does not address the underlying problem of enzyme deficiency and substrate accumulation. These treatments are effective in relieving symptoms, but do not address the underlying problems of enzyme deficiency and substrate accumulation. Specific therapies achieve relief of FD symptoms mainly by targeting and regulating the activity of the corresponding enzymes (Bernardes et al., 2020; Lenders and Brand, 2021; Simonetta et al., 2020). Among them, Enzyme replacement therapy (ERT) is the first-line treatment option for FD recognized by guidelines and consensus in most regions of the world (Germain et al., 2019; Hopkin et al., 2016; Biegstraaten et al., 2015; Ortiz et al., 2018), which effectively relieves patients' pain and gastrointestinal symptoms, improves cardiac hypertrophy, and stabilizes renal function by supplementing the lack of α-Gal A in the patients' body, and reduces substrate accumulation, thus improving the patients' quality of life (Germain et al., 2019; Anderson et al., 2014). And ERT drugs mainly include agalactosidase-α(ALTA-a) (Garman and Garboczi, 2004) and agalactosidase-β(ALTA-b) (McCafferty and Scott, 2019), which have demonstrated excellent efficacy and safety in many FD-related studies (Ramaswami et al., 2006; Beck et al., 2015; Beck et al., 2004; Tahir et al., 2007; Germain et al., 2007). Among them, ALTA-a entered the national health insurance drug catalogue through health insurance negotiations in 2021. Comparison of the economics of treatment regimens is important given the significant reduction in ERT drug costs and increased drug accessibility. However, there are limited pharmacoeconomic evaluation studies (Rombach et al., 2013) of FD treatments globally, and direct comparisons of the economics of specific and non-specific therapies are urgently needed. Therefore, this study conducted a cost-effectiveness analysis of ALTA-a treatment for Chinese FD patients from the perspective of the healthcare system to inform the decision-making of relevant healthcare organizations.
In this study, we chose male FD patients and female patients with more severe symptoms because of the different severity of the disease in male and female patients, the greater susceptibility of male patients to the disease, and the greater impact on life expectancy (Turkmen and Baloglu, 2020; Hagège et al., 2019).
According to the purpose of this paper, we choose the healthcare system as the research perspective.
In this study, the control protocol was the corresponding symptomatic treatment. We chose three typical symptoms of FD as treatment targets, including: pain, cardiac impairment and renal lesions. The therapeutic drugs chosen for these symptoms were: (1) pain: carbamazepine; (2) cardiac impairment: angiotensin-converting enzyme inhibitor analogue - captopril; and (3) renal lesions: angiotensin receptor antagonist analogue - chlorosartan. Carbamazepine was administered orally twice daily at 100 mg. Captopril was administered orally three times daily at 12.5 mg. Chlorosartan was administered orally once daily at 100 mg. ERT treatment was chosen as the intervention option, specifically the use of ALTA-a. It was administered intravenously at a dosage of 0.2 mg/kg every 2 weeks. According to data published by the Chinese National Nutrition Survey, the average weight of Chinese adult males is 66.2 kg, and the average weight of adult women in China is 58.3 kg.
In this study, a Markov model was developed using previous research as a reference (Rombach et al., 2013). Five health states were established according to the characteristics of the symptoms of the disease, namely, “No symptoms”, “Acroparesthesia”, “Single complication”, “Multiple complications” and “Death”. The “Single complication” state means that the patient has one of the three typical symptoms (mentioned in 2.3). The “Multiple complications” state is when the patient has two or three of the three typical symptoms. Patients in any other state are able to move to the “Death” state. The detailed Markov model is presented in Figure 1. At the same time, we made the following assumptions for the model: (1) Since the initial probability distribution of FD patients was not queried, we assumed that all patients entered the model in the state of “No symptoms”; (2) It was assumed that when a patient made a transfer to a state, he is only able to maintain this state or transfer to a state with a lower utility value, and could not return to a state with a higher utility value.
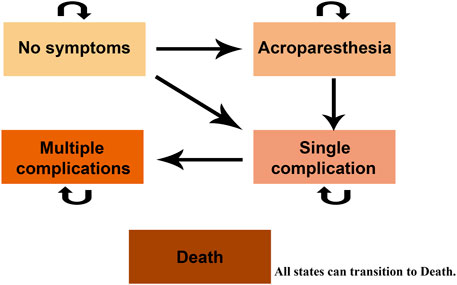
Figure 1. Markov model diagram.
Based on the disease characteristics of FD and the administration of the relevant therapeutic regimen, we set the model cycle to 1 month, and the total timeframe of the model run was 3 years. Because changes in the state of a patient may occur at any time during a cycle, we corrected the model for half-cycling in order to more accurately simulate the process of state transfer in FD patients.
The cost data, utility values, and data sources used in this study are presented in Tables 1, 2, respectively. Since the healthcare system was chosen as the research perspective for this study, the costs included were direct medical costs. Direct healthcare cost is the cost of healthcare resources consumed by a treatment regimen, which in this study includes outpatient, pharmaceutical, and hospitalization costs. It was assumed that patients with “Multiple complications” required hospitalization. Data on transfer probabilities are based on previously published studies, and detailed data are available in the supplementary material. In terms of the transfer probability of “No symptoms” and “Acroparesthesia” to “Death”, we used the officially announced Chinese natural mortality rate of 7.9‰ in 2023. With regard to adverse events, we did not find specific data on utility reductions due to adverse events for either treatment regimen, and therefore did not consider additional costs and utility reductions due to them in this study.

Table 1. Cost inputs.

Table 2. Utility inputs.
The health outcome measure used in this study is quality-adjusted life years (QALYs). This measure is a standardized, universal health outcome measure that represents the number of years a patient would live in a fully healthy state. To reflect the cost difference between the two treatment options at the unit of effectiveness, we use the incremental cost-effectiveness ratio (ICER), which is the increase in cost for the “ERT” group relative to the “No ERT” group divided by the increase in QALYs. We used 1-3 times the World Health Organization’s recommended gross domestic product (GDP) per capita as the willingness-to-pay threshold. In 2023, the per capita GDP of China was ¥89,358. According to the Chinese Guidelines for Economic Evaluation of Pharmaceuticals (2020 Edition), the discount rate for both costs and benefits in this study was set at 5%.
We used one-way sensitivity analysis and probabilistic sensitivity analysis (PSA), respectively. The former is designed to detect the effect of a single parameter on ICER. The latter, on the other hand, simultaneously assesses the impact of uncertainty in all parameters on the results by performing 1000 random samples of each parameter in the model under different probability distributions, and then presenting the simulation results on the cost-effectiveness plane and plotting the cost-effectiveness acceptable curve. Both sensitivity analyses were able to test the stability of the test results.
All the above analytical procedures were carried out using TreeagePro2022 software (2022; TreeAge Software; Williamstown, Massachusetts).
The data related to this study were obtained from clinical trials and previously published papers. This study did not contain any human or animal related experiments and therefore did not require approval from the Ethics Committee.
The results of the base-case analysis results are shown in Table 3. In terms of health outputs, when QALY was used as a measure, the value for patients in the ERT group was 1.36, which was significantly higher than the QALY value for patients in the “No ERT” group (0.99). However, the ERT group also had to bear more costs. The ICER value derived from the deterministic analysis was ¥148,071.95/QALY, which is between one time the GDP per capita (¥89,358/QALY) and three times the GDP per capita (¥268,074/QALY). This indicates that ERT treatment is an economical program.

Table 3. Base-case results.
In order to test the stability of the results, this study conducted a one-way sensitivity analysis of the key parameters in the model. Specifically, it is presented by adjusting the key parameters upward as well as downward by 10% (the range of variation of the discount rate is 0%–8%), and finally the impact of the changes in the key parameters on the ICER is presented in the form of a tornado diagram (Figure 2). The different directional changes of the parameters in the figure are distinguished in red and blue color respectively. From the figure, it can be observed that the price of ALTA-a is the factor that has the greatest impact on the ICER, which reveals its important influence on the economics of the corresponding treatment program.
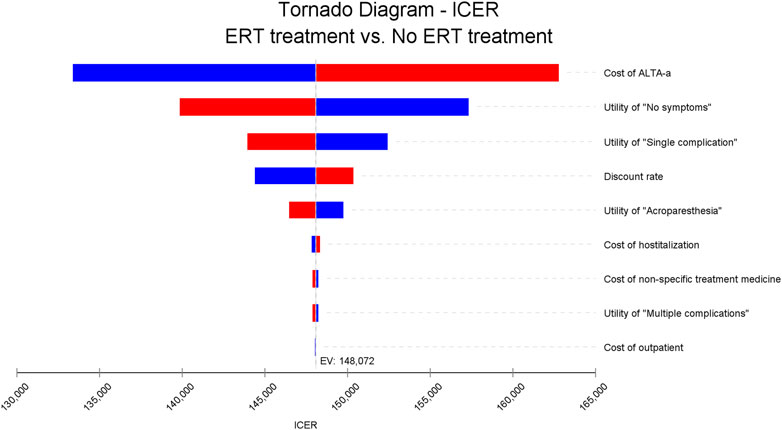
Figure 2. One-way sensitivity analysis results.
In order to assess the impact of parameter uncertainty on the results, we performed a PSA. we used 1% and 10% of the mean as the estimated range of variation in standard deviation for the cost and utility values, respectively. The simulation results are presented on cost-effect quadrant plots as shown in Figures 3–5. The X-axis represents the incremental QALY obtained and the Y-axis represents the incremental cost. The green ellipse contains the 95% ICER estimate. We chose 1 and 3 times GDP per capita as thresholds for the analysis, respectively (to be able to visualize the trend of changes more closely, we also chose 2 times GDP per capita as a threshold). The results show that ERT treatment brings more costs as well as additional effects in all simulations. The average ICER value (¥148630.53/QALY) was similar to the results of the deterministic analysis (¥148071.95/QALY). In addition, we plotted the cost-effectiveness acceptable curve, and the results are shown in Figure 6. It shows the probability that two treatment programs have cost-effects at a given threshold. We can find that as the willingness-to-pay threshold is adjusted upward, the probability of having a cost-effect in the ERT group increases. The probability that the ERT group is cost-effective is 0% at a threshold of 1x GDP per capita (¥89,358/QALY), and this value rises to 98.1% and 100% when the threshold rises to 2x GDP per capita (¥178,716/QALY) and 3x GDP per capita (¥268,074/QALY), respectively.
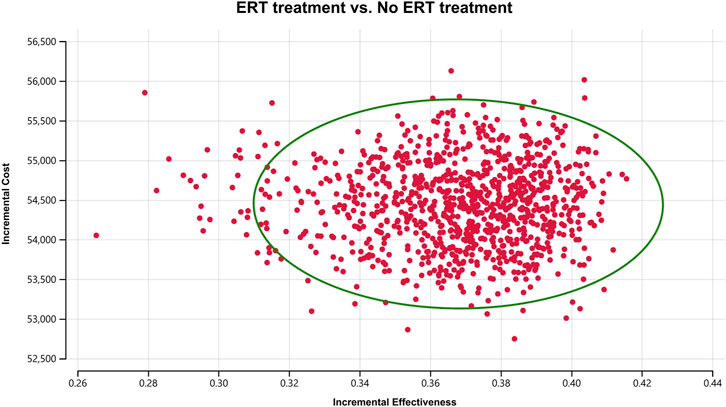
Figure 3. Cost-effectiveness plane for the ERT versus the “No ERT” group (WTP = ¥89358/QALY).
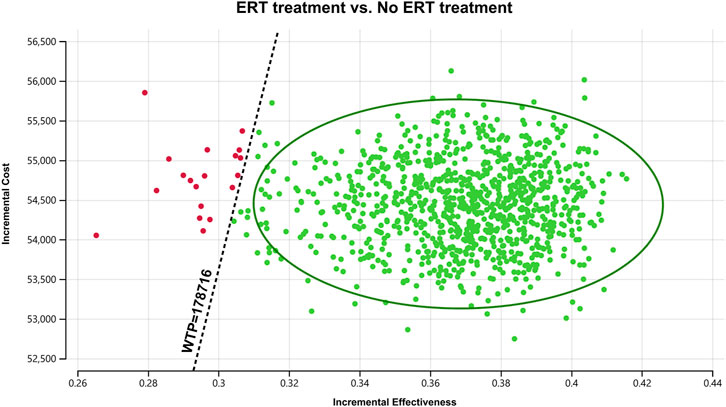
Figure 4. Cost-effectiveness plane for the ERT versus the “No ERT” group (WTP = ¥178716/QALY).
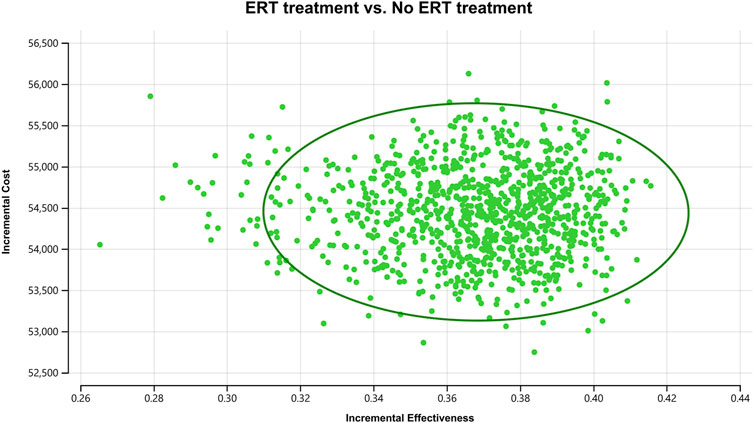
Figure 5. Cost-effectiveness plane for the ERT versus the “No ERT” group (WTP = ¥268074/QALY).
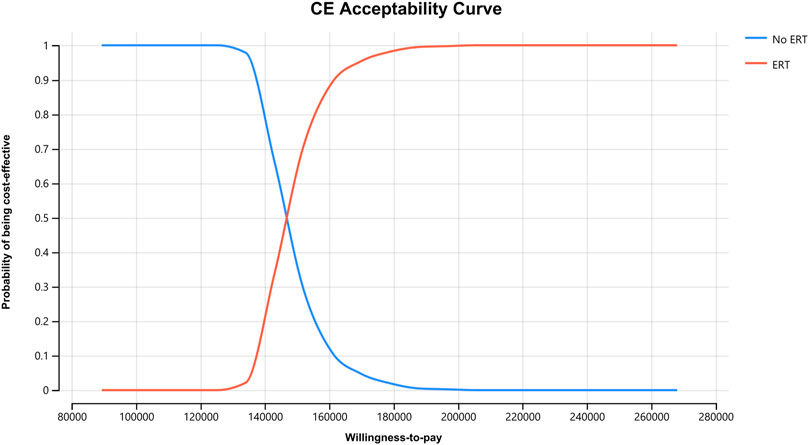
Figure 6. Cost-effectiveness acceptable curve.
As a rare X chromosome-associated lysosomal storage disease, FD can lead to multiple organ diseases such as cardiac and renal diseases and even life-threatening complications, and its clinical manifestations are diversified and non-specific. FD is ranked 27th in China’s First Rare Disease Catalog, and even though the number of patients with FD is relatively small, the complexity of its clinical symptoms still needs to be taken seriously. The treatment of FD includes non-specific and specific treatment. Nonspecific treatment is the symptomatic management of each organ involvement. Specific therapy, on the other hand, regulates the activity of the corresponding enzymes and is targeted. Among them, ERT is a classical therapy. Several studies have confirmed the significant improvement of cardiac and renal functions of ALTA-a in FD patients (Anderson et al., 2014; Tang et al., 2021; Choi et al., 2008; Sasa et al., 2019; Lin et al., 2014; Ramaswami et al., 2019). Despite the excellent clinical performance, there are limited pharmacoeconomic studies on ERT for FD worldwide. Therefore, this study evaluated the economics of ERT for the treatment of FD patients in China from the perspective of the healthcare system.
In this study, we first performed a base-case analysis. The results showed that the ERT therapy group incurred higher costs and also obtained more QALYs. The ICER obtained by calculation was ¥148071.95/QALY, a value that is between 1 and 3 times the per capita GDP of China. This indicates that ERT therapy is an economical program. In a later unidirectional sensitivity analysis, we found that the cost of ALTA-a was the most important parameter leading to the change in ICER, which indicates that in the case of ERT therapy, the price of the drug is still the determining factor leading to the economics of the treatment program. Using PSA analysis, we found that the probability of the ERT treatment group being economical increases with the willingness-to-pay threshold, rising from 0% corresponding to 1x GDP per capita to 100% corresponding to 3x GDP per capita. We also assess the effect of parameter uncertainty on the results, demonstrating the stability of the results.
This study has several advantages. First, this study selected ERT, a classic and representative therapy, as a research subject, which will provide a reference for subsequent studies. Second, this study is the first pharmacoeconomic evaluation of ERT for the treatment of FD in China, which is useful for the selection of therapies for FD patients in China. Finally, this paper used a relatively novel Markov model, and the individual states can comprehensively reflect the disease progression of FD patients.
However, there are limitations to this study. First, due to the lack of data from the Chinese region and from FD-related clinical trials, some of the data used in the model of this study were derived from studies in other countries, which are likely not applicable to FD patients in China. In addition, due to the lack of reference standards, the effects of adverse reactions were not included in the model. However, the fact is that in clinical practice, prolonged injection of ALTA-a can lead to the formation of anti-drug antibodies (mostly IgG-type antibodies) that produce adverse reactions (van der Veen et al., 2019). These are likely to lead to an increase in the cost of treatment as well as a decrease in the associated utility values and have some impact on the final outcome. Secondly, due to the lack of relevant data, the distribution of costs as well as utilities in the PSA used mean values ± 1% and ±10%, respectively. The uncertainty of the real situation may be different from that reflected in the PSA of this study. Moreover, considering the ubiquity of ALTA-a at this stage, only ALTA-a therapy in ERT was considered in this study, however, ERT also includes other therapies such as ALTA-β. As a classical therapy for these diseases, a comprehensive pharmacoeconomic evaluation of ERT is necessary. Future studies can be conducted from other ERT therapies, which will strengthen the persuasive conclusions. Finally, this study still used the more traditional 1-3 times GDP per capita as the willingness-to-pay threshold, which is likely no longer applicable to diseases such as FD. We believe that the setting of willingness-to-pay thresholds for drugs related to rare diseases is an important aspect of future pharmacoeconomic evaluations. We recognize that the above limitations may lead to very different conclusions. However, based on the limited data available, we believe that all data in this study were obtained from the best available sources, minimizing the impact of data bias on obtaining realistic conclusions.
Our study applied Markov modeling, which has distinct advantages and disadvantages. It has been pointed out that in the field of pharmacoeconomic analysis, Markov modeling is particularly suitable for diseases involving duration risk, including the risk of death (Carta and Conversano, 2020), which fits well with the disease characteristics of FD. In terms of application, it can predict future state shifts, which helps relevant decision making. However, its disadvantages cannot be ignored. The first is that additions to the modeled states will become complex. If the FD disease states are further refined and more disease states are obtained in the future, the transfer matrix will be large and difficult to manage. At the same time, the model is highly dependent on assumptions and ignores the interference of other external factors, which can affect the accuracy of the study. As FD studies continue to be conducted, we believe that dynamic modeling on pharmacoeconomic evaluation is likely to be applied in future FD-related studies. As new clinical evidence continues to emerge, such dynamic modeling will provide a clearer and more specific perspective on the innovation of FD therapies.
In addition, based on real-world data, ERT is effective in slowing down disease progression (Beck et al., 2022; Parini et al., 2020). At the same time, it is associated with high costs and burden of healthcare resource utilization (Katsigianni and Petrou, 2022; Jovanovic et al., 2024). This corresponds to the results of our study. Analyzing the real-world data in conjunction with the expected results of our model can provide a more objective perspective.
It is worth noting that despite the fact that ALTA-a has been included in the health insurance catalog and the cost of medication has dropped significantly, there will still be some patients who will not be able to afford this portion of the expenditure. This will have a greater impact when patients consider ERT treatment. We agree with the recommendation made by previous scholars, that is, we suggest the relevant drug manufacturers to implement “patient assistance programs” to improve the accessibility of the drug (Xiang et al., 2023), so that more patients can obtain more effective treatment.
In addition, due to the diversity of clinical symptoms of FD, patients with FD are often delayed in diagnosis, resulting in failure to receive timely and effective treatment (Mehta et al., 2010). Therefore, starting ERT as early as possible or at the right time may have a positive impact on the economics of the relevant ERT treatment regimen. This also requires a concerted effort between patients and clinicians in terms of disease awareness. In addition, because China’s economic development is highly unbalanced, there are large differences in the level of economic development between regions. Therefore, the results of this study should be considered in the context of local economic development in different regions. In economically developed regions, such as Beijing and Shanghai (with GDP per capita of $27,729 and $26,252, respectively, which are both more than twice the national GDP per capita (Xiang et al., 2023)), the probability of ERT having a cost-effectiveness will be higher. Conversely, this probability decreases in regions with relatively poor economic development. Finally, we call for the emergence of more clinical data based on FD patients in Chinese regions, which will provide more reliable evidence for the economic evaluation of FD treatment and facilitate more accurate study results. Although the cost-effectiveness of ERT treatment was demonstrated in our study, the patients’ quality of life and the economic burden still need to be emphasized (Jovanovic et al., 2024). For example, as suggested by some scholars, home infusion and self-administration may help to reduce the burden associated with ERT (Milligan et al., 2006; Beck et al., 2013).
It has already been mentioned that the life expectancy of FD patients, especially men, is significantly lower. In context (timeliness of treatment and misdiagnosis, etc.), the actual life expectancy of these patients may be even lower. In the future, the clinical diagnosis of FD patients will be crucial, as the clinical phenotype of FD is extensive and heterogeneous, as the same genotype is not identical in the same family, and the detection of mutation sites of unknown significance is unsupported by, or does not correspond to clinical data, which creates multiple complexities in clinical diagnosis and treatment. Therefore, the development of individualized diagnosis and treatment plans for FD is very important in the future, and requires the relevant healthcare professionals to have a full understanding of the disease characteristics, progression patterns, and socio-economic conditions of patients with FD. In addition, besides ERT, molecular chaperone therapy is also a popular therapy for FD. Among them, the molecular chaperone with more clinical use is migalastat, which is suitable for patients with GLA missense mutations that retain some α-Gal A activity. Currently, it is not yet available in China. Relevant studies incorporating real-world data from the Chinese healthcare system are one aspect that could be pursued in future FD-related studies, especially if there is sufficient local Chinese data for these popular therapies. The availability of more evidence of economic evaluation based on the Chinese context will strengthen the conclusions we have drawn and will help to customize future pharmacoeconomic models.
In summary, ERT treatment is the economically viable option from the perspective of the healthcare system. This study will help relevant organizations in their decision-making process, and the excellent efficacy, safety, and affordability of ERT are likely to make it a dominant treatment for FD in the future.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
YH: Conceptualization, Methodology, Software, Writing–original draft. HY: Supervision, Resources, Writing–review and editing. ZH: Supervision, Writing–review and editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2025.1546018/full#supplementary-material
Anderson, L. J., Wyatt, K. M., Henley, W., Nikolaou, V., Waldek, S., Hughes, D. A., et al. (2014). Long-term effectiveness of enzyme replacement therapy in Fabry disease: results from the NCS-LSD cohort study. J. Inherit. Metabolic Dis. 37, 969–978. doi:10.1007/s10545-014-9717-4
Beck, M., Gaedeke, J., Martus, P., Karabul, N., and Rolfs, A. (2013). Infusionsbehandlung in häuslicher Umgebung–ein praktikabler Ansatz für chronisch Kranke? Neue Wege der Versorgung am Beispiel des Morbus Fabry [Home-based infusion therapy–a feasible approach for chronically ill patients? A new path to provide superior patient care exemplified for Fabry's disease]. Dtsch Med Wochenschr. 138, 2345–2350. doi:10.1055/s-0033-1349624
Beck, M., Hughes, D., Kampmann, C., Larroque, S., Mehta, A., Pintos-Morell, G., et al. (2015). Long-term effectiveness of agalsidase alfa enzyme replacement in Fabry disease: a Fabry Outcome Survey analysis. Mol. Genet. Metabolism Rep. 3, 21–27. doi:10.1016/j.ymgmr.2015.02.002
Beck, M., Ramaswami, U., Hernberg-Ståhl, E., Hughes, D. A., Kampmann, C., Mehta, A. B., et al. (2022). Twenty years of the Fabry Outcome Survey (FOS): insights, achievements, and lessons learned from a global patient registry. Orphanet J. Rare Dis. 17, 238. doi:10.1186/s13023-022-02392-9
Beck, M., Ricci, R., Widmer, U., Dehout, F., De Lorenzo, A. G., Kampmann, C., et al. (2004). Fabry disease: overall effects of agalsidase alfa treatment. Eur. J. Clin. Investigation 34, 838–844. doi:10.1111/j.1365-2362.2004.01424.x
Bernardes, T. P., Foresto, R. D., and Kirsztajn, G. M. (2020). Fabry disease: genetics, pathology, and treatment. Rev. Assoc. Médica Bras. 66, s10–s16. doi:10.1590/1806-9282.66.S1.10
Biegstraaten, M., Arngrímsson, R., Barbey, F., Boks, L., Cecchi, F., Deegan, P. B., et al. (2015). Recommendations for initiation and cessation of enzyme replacement therapy in patients with Fabry disease: the European Fabry Working Group consensus document. Orphanet J. Rare Dis. 10, 36. doi:10.1186/s13023-015-0253-6
Carta, A., and Conversano, C. (2020). On the use of markov models in pharmacoeconomics: pros and cons and implications for policy makers. Front. Public Health. 8, 569500. doi:10.3389/fpubh.2020.569500
Choi, J.-H., Cho, Y. M., Suh, K.-S., Yoon, H.-R., Kim, G.-H., Kim, S.-S., et al. (2008). Short-Term efficacy of enzyme replacement therapy in Korean patients with fabry disease. J. Korean Med. Sci. 23, 243–250. doi:10.3346/jkms.2008.23.2.243
Garman, S. C., and Garboczi, D. N. (2004). The molecular defect leading to Fabry disease: structure of human alpha-galactosidase. J. Mol. Biol. 337, 319–335. doi:10.1016/j.jmb.2004.01.035
Germain, D. P., Fouilhoux, A., Decramer, S., Tardieu, M., Pillet, P., Fila, M., et al. (2019). Consensus recommendations for diagnosis, management and treatment of Fabry disease in paediatric patients. Clin. Genet. 96, 107–117. doi:10.1111/cge.13546
Germain, D. P., Waldek, S., Banikazemi, M., Bushinsky, D. A., Charrow, J., Desnick, R. J., et al. (2007). Sustained, long-term renal stabilization after 54 months of agalsidase beta therapy in patients with Fabry disease. J. Am. Soc. Nephrol. 18, 1547–1557. doi:10.1681/ASN.2006080816
Hagège, A., Réant, P., Habib, G., Damy, T., Barone-Rochette, G., Soulat, G., et al. (2019). Fabry disease in cardiology practice: literature review and expert point of view. Archives Cardiovasc. Dis. 112, 278–287. doi:10.1016/j.acvd.2019.01.002
Hopkin, R. J., Jefferies, J. L., Laney, D. A., Lawson, V. H., Mauer, M., Taylor, M. R., et al. (2016). The management and treatment of children with Fabry disease: a United States-based perspective. Mol. Genet. Metabolism 117, 104–113. doi:10.1016/j.ymgme.2015.10.007
Jovanovic, A., Miller-Hodges, E., Castriota, F., Takyar, S., Howitt, H., Ayodele, O., et al. (2024). A systematic literature review on the health-related quality of life and economic burden of Fabry disease. Orphanet J. Rare Dis. 19, 181. doi:10.1186/s13023-024-03131-y
Katsigianni, E. I., and Petrou, P. (2022). A systematic review of the economic evaluations of Enzyme Replacement Therapy in Lysosomal Storage Diseases. Cost Eff. Resour. Alloc. 20, 51. doi:10.1186/s12962-022-00369-w
Lenders, M., and Brand, E. (2021). Fabry disease: the current treatment landscape. Drugs 81, 635–645. doi:10.1007/s40265-021-01486-1
Lin, H.-Y., Huang, Y.-H., Liao, H.-C., Liu, H.-C., Hsu, T.-R., Shen, C.-I., et al. (2014). Clinical observations on enzyme replacement therapy in patients with Fabry disease and the switch from agalsidase beta to agalsidase alfa. J. Chin. Med. Assoc. 77, 190–197. doi:10.1016/j.jcma.2013.11.006
Linhart, A., Germain, D. P., Olivotto, I., Akhtar, M. M., Anastasakis, A., Hughes, D., et al. (2020). An expert consensus document on the management of cardiovascular manifestations of Fabry disease. Eur. J. Heart Fail. 22, 1076–1096. doi:10.1002/ejhf.1960
Mallett, A., Kearey, P., Cameron, A., Healy, H., Denaro, C., Thomas, M., et al. (2020). The Ckd. Qld fabRy Epidemiology (aCQuiRE) study protocol: identifying the prevalence of Fabry disease amongst patients with kidney disease in Queensland, Australia. BMC Nephrol. 21, 58. doi:10.1186/s12882-020-01717-9
McCafferty, E. H., and Scott, L. J. (2019). Migalastat: a review in fabry disease. Drugs 79, 543–554. doi:10.1007/s40265-019-01090-4
Mehta, A., Beck, M., Eyskens, F., Feliciani, C., Kantola, I., Ramaswami, U., et al. (2010). Fabry disease: a review of current management strategies. Qjm 103, 641–659. doi:10.1093/qjmed/hcq117
Milligan, A., Hughes, D., Goodwin, S., Richfield, L., and Mehta, A. (2006). Intravenous enzyme replacement therapy: better in home or hospital? Br J Nurs. 15, 330. doi:10.12968/bjon.2006.15.6.20681
Ortiz, A., Germain, D. P., Desnick, R. J., Politei, J., Mauer, M., Burlina, A., et al. (2018). Fabry disease revisited: management and treatment recommendations for adult patients. Mol. Genet. Metabolism 123, 416–427. doi:10.1016/j.ymgme.2018.02.014
Ramaswami, U., Beck, M., Hughes, D., Kampmann, C., Botha, J., Pintos-Morell, G., et al. (2019). Cardio- renal outcomes with long- term agalsidase alfa enzyme replacement therapy: a 10- year fabry outcome Survey (FOS) analysis. Drug Des. Dev. Ther. 13, 3705–3715. doi:10.2147/DDDT.S207856
Parini, R., Pintos-Morell, G., Hennermann, J. B., Hsu, T.-R., Karabul, N., Kalampoki, V., et al. (2020). Analysis of renal and cardiac outcomes in male participants in the fabry outcome survey starting agalsidase alfa enzyme replacement therapy before and after 18 years of age. Drug Des. Devel. Ther. 14, 2149–2158. doi:10.2147/DDDT.S249433
Ramaswami, U., Wendt, S., Pintos-Morell, G., Parini, R., Whybra, C., Leon Leal, J. A., et al. (2006). Enzyme replacement therapy with agalsidase alfa in children with Fabry disease. Acta Paediatr. 96, 122–127. doi:10.1111/j.1651-2227.2007.00029.x
Rombach, S. M., Hollak, C. E., Linthorst, G. E., and Dijkgraaf, M. G. (2013). Cost-effectiveness of enzyme replacement therapy for Fabry disease. Orphanet J. Rare Dis. 8, 29. doi:10.1186/1750-1172-8-29
Sasa, H., Nagao, M., and Kino, K. (2019). Safety and effectiveness of enzyme replacement therapy with agalsidase alfa in patients with Fabry disease: post-marketing surveillance in Japan. Mol. Genet. Metabolism 126, 448–459. doi:10.1016/j.ymgme.2019.02.005
Simonetta, I., Tuttolomondo, A., Daidone, M., Miceli, S., and Pinto, A. (2020). Treatment of anderson-fabry disease. Curr. Pharm. Des. 26, 5089–5099. doi:10.2174/1381612826666200317142412
Spada, M., Pagliardini, S., Yasuda, M., Tukel, T., Thiagarajan, G., Sakuraba, H., et al. (2006). High incidence of later-onset fabry disease revealed by newborn screening. Am. J. Hum. Genet. 79, 31–40. doi:10.1086/504601
Tahir, H., Jackson, L. L., and Warnock, D. G. (2007). Antiproteinuric therapy and fabry nephropathy: sustained reduction of proteinuria in patients receiving enzyme replacement therapy with agalsidase-beta. J. Am. Soc. Nephrol. 18, 2609–2617. doi:10.1681/ASN.2006121400
Tang, A. S. O., Wong, Q. Y., Pao Lin Ting, I., Selvesten, P., Yeo, S. T., Chew, L. P., et al. (2021). First 2 fabry cases with novel mutation and their associated clusters in Malaysia. Am. J. Case Rep. 22, e932923. doi:10.12659/AJCR.932923
Turkmen, K., and Baloglu, I. (2020). Fabry disease: where are we now? Int. Urology Nephrol. 52, 2113–2122. doi:10.1007/s11255-020-02546-3
van der Veen, S. J., van Kuilenburg, A. B. P., Hollak, C. E. M., Kaijen, P. H. P., Voorberg, J., and Langeveld, M. (2019). Antibodies against recombinant alpha-galactosidase A in Fabry disease: subclass analysis and impact on response to treatment. Mol. Genet. Metabolism 126, 162–168. doi:10.1016/j.ymgme.2018.11.008
Vardarli, I., Rischpler, C., Herrmann, K., and Weidemann, F. (2020). Diagnosis and screening of patients with fabry disease. Ther. Clin. Risk Manag. 16, 551–558. doi:10.2147/TCRM.S247814
Keywords: fabry disease, enzyme replacement therapy, agalactosidase-α, Markov model, incremental cost-effectiveness ratio, sensitivity analysis
Citation: Huang Y, Yuan H and Huang Z (2025) Cost-effectiveness analysis of enzyme replacement therapy for the treatment of Chinese patients with fabry disease: a Markov model. Front. Pharmacol. 16:1546018. doi: 10.3389/fphar.2025.1546018
Received: 16 December 2024; Accepted: 07 February 2025;
Published: 11 March 2025.
Edited by:
Sandro Feriozzi, Azienda Sanitaria Locale di Viterbo, ItalyReviewed by:
Segundo Mariz, European Medicines Agency, NetherlandsCopyright © 2025 Huang, Yuan and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hongmei Yuan, eXVhbmhtNjEyQDE2My5jb20= Zhe Huang, aHVhbmd6aGUyMDAwQHNpbmEuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.