
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pharmacol., 07 March 2025
Sec. Inflammation Pharmacology
Volume 16 - 2025 | https://doi.org/10.3389/fphar.2025.1539756
 Antonio Vitale1,2
Antonio Vitale1,2 Flavia Leone3
Flavia Leone3 Valeria Caggiano1,2
Valeria Caggiano1,2 Andrea Hinojosa-Azaola4
Andrea Hinojosa-Azaola4 Eduardo Martín-Nares4
Eduardo Martín-Nares4 Guillermo Arturo Guaracha-Basañez4
Guillermo Arturo Guaracha-Basañez4 Jiram Torres-Ruiz4Perla Ayumi Kawakami-Campos5
Jiram Torres-Ruiz4Perla Ayumi Kawakami-Campos5 Pravin Hissaria6,7
Pravin Hissaria6,7 Alicia Callisto6,7Mark Beecher6,7
Alicia Callisto6,7Mark Beecher6,7 Lorenzo Dagna8,9
Lorenzo Dagna8,9 Alessandro Tomelleri8,9
Alessandro Tomelleri8,9 Corrado Campochiaro8,9
Corrado Campochiaro8,9 Micol Frassi10
Micol Frassi10 Francesca Crisafulli10
Francesca Crisafulli10 Franco Franceschini10
Franco Franceschini10 José Hernández-Rodríguez11
José Hernández-Rodríguez11 Verónica Gómez-Caverzaschi11
Verónica Gómez-Caverzaschi11 Olga Araújo11
Olga Araújo11 Paolo Sfriso12
Paolo Sfriso12 Sara Bindoli12
Sara Bindoli12 Chiara Baggio12
Chiara Baggio12 Jessica Sbalchiero1,2Jurgen Sota1,2
Jessica Sbalchiero1,2Jurgen Sota1,2 Abdurrahman Tufan13
Abdurrahman Tufan13 Ibrahim Vasi13
Ibrahim Vasi13 Matteo Piga14,15Alberto Cauli14,15Maria Antonietta D’Agostino3
Matteo Piga14,15Alberto Cauli14,15Maria Antonietta D’Agostino3 Amato De Paulis16,17
Amato De Paulis16,17 Ilaria Mormile16
Ilaria Mormile16 Henrique A. Mayrink Giardini18
Henrique A. Mayrink Giardini18 Rafael Alves Cordeiro18
Rafael Alves Cordeiro18 Francesco Gavioli1,2
Francesco Gavioli1,2 Giuseppe Lopalco18
Giuseppe Lopalco18 Florenzo Iannone19Carlomaurizio Montecucco20
Florenzo Iannone19Carlomaurizio Montecucco20 Sara Monti20
Sara Monti20 Guillermo Ruiz-Irastorza21,22
Guillermo Ruiz-Irastorza21,22 Adriana Soto-Peleteiro21,22Paola Triggianese23,24
Adriana Soto-Peleteiro21,22Paola Triggianese23,24 Carmelo Gurnari24,25
Carmelo Gurnari24,25 Ombretta Viapiana26Riccardo Bixio26Rosetta Vitetta27
Ombretta Viapiana26Riccardo Bixio26Rosetta Vitetta27 Edoardo Conticini1,2
Edoardo Conticini1,2 Francesco La Torre28
Francesco La Torre28 Gaafar Ragab29,30
Gaafar Ragab29,30 Ezgi Deniz Batu31Andrés González-García32Mercedes Peña-Rodríguez32Monica Bocchia2,33
Ezgi Deniz Batu31Andrés González-García32Mercedes Peña-Rodríguez32Monica Bocchia2,33 Ewa Wiesik-Szewczyk34
Ewa Wiesik-Szewczyk34 Karina Jahnz-Rózyk34
Karina Jahnz-Rózyk34 Alejandra de-la-Torre35Alberto Balistreri2,36Bruno Frediani1,2
Alejandra de-la-Torre35Alberto Balistreri2,36Bruno Frediani1,2 Claudia Fabiani2,37
Claudia Fabiani2,37 Luca Cantarini1,2*for the International AIDA (AutoInflammatory Diseases Alliance) Network and the Autoinflammatory Diseases Working Group of the Italian Society of Rheumatology (SIR)
Luca Cantarini1,2*for the International AIDA (AutoInflammatory Diseases Alliance) Network and the Autoinflammatory Diseases Working Group of the Italian Society of Rheumatology (SIR)Background: VEXAS (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) syndrome is an adult-onset autoinflammatory condition resulting in severe, often treatment-refractory inflammation. Currently, there are no established treatment guidelines for VEXAS syndrome.
Objectives: To assess the efficacy and safety of conventional disease-modifying antirheumatic drugs (cDMARDs) in a cohort of VEXAS patients.
Methods: Data from VEXAS patients were obtained from the International AIDA Network VEXAS registry.
Results: Data from 36 VEXAS patients were evaluated, with 28 (77.8%) treated with cDMARDs as monotherapy - and concomitant glucocorticoids (GC) - and 8 (22.2%) receiving a combination of different cDMARDs plus GC. Complete response (CR), partial response (PR), and failure to cDMARDs monotherapy were reported in 4/22 (18.2%), 11/22 (50%), and 7/22 (31.8%) courses, respectively. All patients were treated with GCs at the start of cDMARD monotherapy, and no GC discontinuation was observed later. No significant differences were observed in the GC dosage from the start of cDMARDs to the 3-month (p = 0.43), 6-month (p = 0.31), and 12-month (p = 0.21) visits. Conversely, the GC sparing resulted to be statistically significant when using methotrexate (p = 0.02). As for cDMARDs combinations, no cases achieved CR, while PR was observed in 5/9 (55.6%). Seventeen adverse events were reported, seven of which led to discontinuation.
Conclusion: Many VEXAS patients report a partial benefit from cDMARDs, while a smaller yet not negligible number of patients exhibit a CR; cDMARDs remain a viable option for this disorder, especially when the initial GC dosage is low and the need for a steroid-sparing effect is not immediately urgent.
• Given the absence of standardized treatment guidelines for VEXAS syndrome, this study provides preliminary evidence on the therapy for this rare autoinflammatory condition
• This study evaluated the overall efficacy and safety profile of cDMARDs, administered either as monotherapy or in combination, in a substantial cohort of patients diagnosed with VEXAS syndrome
• This study highlights that cDMARDs achieved complete efficacy in only a minority of patients and demonstrated limited glucocorticoid-sparing effects; however, partial responses with effective control of specific clinical manifestations were common
VEXAS (Vacuoles, E1 enzyme, X-linked, Autoinflammatory, Somatic) syndrome is an acquired monogenic autoinflammatory disease caused by somatic mutations in the UBA1 gene. Discovered in 2020 by Beck et al. (Beck et al., 2020), VEXAS syndrome is characterized by severe systemic inflammation that can virtually affect all organs and tissues.
Regarding its etiopathogenesis, UBA1 mutations lead to a decrease in ubiquitination and, consequently, to aberrant activation of the innate immune response (Beck et al., 2020). As the UBA1 gene is located on the X chromosome, VEXAS syndrome primarily affects men. Due to the post-zygotic somatic onset of mutations, it generally manifests in adulthood, mainly after the age of 50. The most frequently reported UBA1 gene mutations are missense mutations involving methionine at amino acid position 41, and they are found in hematopoietic progenitor cells.
The clinical presentation may be extremely heterogeneous, mimicking various other systemic rheumatologic entities coexisting with hematological disorders. Generally, VEXAS patients exhibit clinical features of autoinflammation, such as recurrent fever episodes, ear and nose chondritis, cutaneous vasculitis, neutrophilic dermatosis, pulmonary infiltrates, alveolitis, and venous thromboembolism, along with hematologic abnormalities including macrocytic anemia, thrombocytopenia, and signs of myelodysplastic syndrome (MDS) (Georgin-Lavialle et al., 2022; Gurnari et al., 2024a).
Prognostically, patients with VEXAS syndrome have an increased risk of morbidity and mortality, with a 5-year survival of approximately 80% and a median survival from onset of 10 years (Georgin-Lavialle et al., 2022; Ferrada et al., 2021; Gutierrez-Rodrigues et al., 2023).
To date, there are no standardized guidelines for managing this syndrome, and the available recommendations are based on a limited number of retrospective studies. The coexistence of inflammatory and hematologic symptoms in this condition often necessitates a multidisciplinary approach, and treatments must be tailored to each patient based on the predominant manifestation. In general, there are two main therapeutic strategies: inhibiting inflammatory pathways or cytokines through immunosuppressive drugs, cytokine inhibitors, and DNA methylation inhibitors, or eradicating progenitor stem cell clones carrying the UBA1 mutation through hematopoietic cell transplantation (Nakajima and Kunimoto, 2024; Gurnari et al., 2024b). Certainly, glucocorticoids (GCs) have been the cornerstone of initial management for VEXAS syndrome, effectively alleviating inflammatory symptoms and cytopenia. However, medium to high doses are needed to achieve adequate control, necessitating alternative medications to reduce GC dosage and prevent long-term side effects.
Therefore, the purpose of this study is to evaluate the role of conventional disease-modifying antirheumatic drugs (cDMARDs) in patients with VEXAS syndrome based on real-world data gathered in the international AIDA Network VEXAS syndrome registry (Vitale et al., 2022).
The main objective of this study was to assess the global efficacy of cDMARDs, used as monotherapy or in combination with other cDMARDs, in a relatively large cohort of patients diagnosed with VEXAS syndrome. An additional objective was to assess the safety profile of cDMARDs in these patients.
The endpoints for evaluating cDMARDs effectiveness were: i) the frequency of complete response, partial response, and treatment failure while on treatment; ii) the variations in daily prednisone (or equivalent) dosage from the start of cDMARDs’ treatment and the 3-, 6-, 12-month visit as well as the last assessment while on cDMARDs’ treatment.
All adverse events observed during the cDMARDs’ treatment regimen were reported to assess the safety profile.
Therefore, patients with VEXAS syndrome were consecutively enrolled from November 2021 to May 2024 in the international AIDA Network VEXAS syndrome registry. Data collection regarding treatment, clinical, and laboratory features was conducted both retrospectively (from disease onset to the time of enrollment into the AIDA registry) and prospectively (from the time of enrollment into the AIDA registry to the last follow-up assessment).
Laboratory assessments at onset and during follow-up included screening for hematologic abnormalities (anemia, leukopenia, thrombocytosis, and thrombocytopenia) and the inflammatory markers erythrocyte sedimentation rate (ESR) and C reactive protein (CRP). Reference ranges depended on the laboratories of the recruiting centers.
Inclusion criteria required the presence of a pathogenic or likely pathogenic mutation in the UBA1 gene, along with the onset of a not otherwise explained systemic inflammatory condition. Signed informed consent for using clinical, laboratory, and genetic data was obtained in all patients enrolled.
The study was approved by the Ethics Committee of the Azienda Ospedaliero-Universitaria Senese, Siena, Italy, in June 2019 (Ref. N. 14951) as part of the AIDA Program. The study protocol conformed to the tenets of the Declaration of Helsinki.
Mutations in the UBA1 gene, along with mutations associated with myelodysplastic syndrome or other oncohematological disorders, were detected through Next-Generation Sequencing or Sanger testing on peripheral blood or bone marrow samples.
Disease duration was defined as the period ranging from clinical onset to the start of each specific cDMARD. The follow-up period ranged from the initiation of cDMARDs to the last recorded assessment in the AIDA registry, with the index date corresponding to the start of cDMARD.
In the absence of standardized guidelines, physicians employed diverse treatment strategies based on their clinical expertise and the patient’s individual characteristics.
Regarding treatment outcomes, complete response (CR) was defined as the resolution of VEXAS-related clinical manifestations, accompanied by normalization or only a slight increase (no more than 10% above the upper limit of the cut-off) of inflammatory parameters (ESR and CRP) and no increase in the daily prednisone dosage. Partial response (PR) was defined as the persistence of clinical and laboratory manifestations with significantly reduced severity and/or frequency of acute exacerbations, as reported by patients and observed by physicians. Failure (F) was defined as the persistence of clinical manifestations and/or insufficient reduction in inflammatory markers to meet the previous definitions.
Both the terms “cDMARDs monotherapy” and “combination of cDMARDs” imply the concomitant use of glucocorticoids in all patients included in the analysis.
The term “adverse event” refers to any detrimental medical occurrence observed following exposure to any cDMARD treatment related to VEXAS syndrome, not necessarily caused by the treatment itself.
Regarding statistical analysis, descriptive statistics included percentages, mean, standard deviation (SD), median, interquartile range (IQR), and frequency counts as required. Qualitative data were analyzed using Fisher’s Exact test or Chi-squared test based on frequency counts and expected frequencies. Quantitative data were analyzed using Student's t-test or Mann-Whitney U test, depending on data distribution assessed through the Shapiro-Wilk test. Simple linear regression analysis was performed to search for any association between the cDMARDs discontinuation and the cDMARDs treatment duration (dependent variable) and the occurrence of withdrawal or the causes of withdrawal (independent variables). The significance level was set at 95% (p-value <0.05). The p-value was two-tailed in all cases. Statistical analysis was performed using RStudio software, version 4.3.0.
At the start of the data analysis (27 May 2024), 71 patients were enrolled in the international AIDA registry dedicated to VEXAS syndrome. In detail, cDMARDs were used as monotherapy in 32 (45%) patients, as a combination of two cDMARDs in 7 (9.9%) cases, and as a combination of three cDMARDs in 1 (1.4%) case. Since the remaining patients used a combination of cDMARDs and biotechnological DMARDs, they were excluded from this study.
Regarding cDMARDs used as monotherapy, statistical analysis was performed on 41 treatment courses observed in 28 patients. Data from the remaining patients were only partial and erased (data missing at random). In total, 36 patients were included in the present study to assess the role of cDMARDs in VEXAS syndrome, either as monotherapy (28 patients) or in combination with other cDMARDs (8 patients). Table 1 provides demographic, clinical, and therapeutic information on the patients included in the study. The UBA1 gene mutations identified in this cohort were: p.Met41Val in 10 (27.7%) cases, p.Met41Thr in 9 (25%) cases, p.Met41Leu in 4 (11.1%) cases; c.118-2A>G and c.118-1G>C mutations were identified in one patient each. Other 11 (30.6%) patients were reported to carry a UBA1 mutation, which was not specifically specified in the registry.
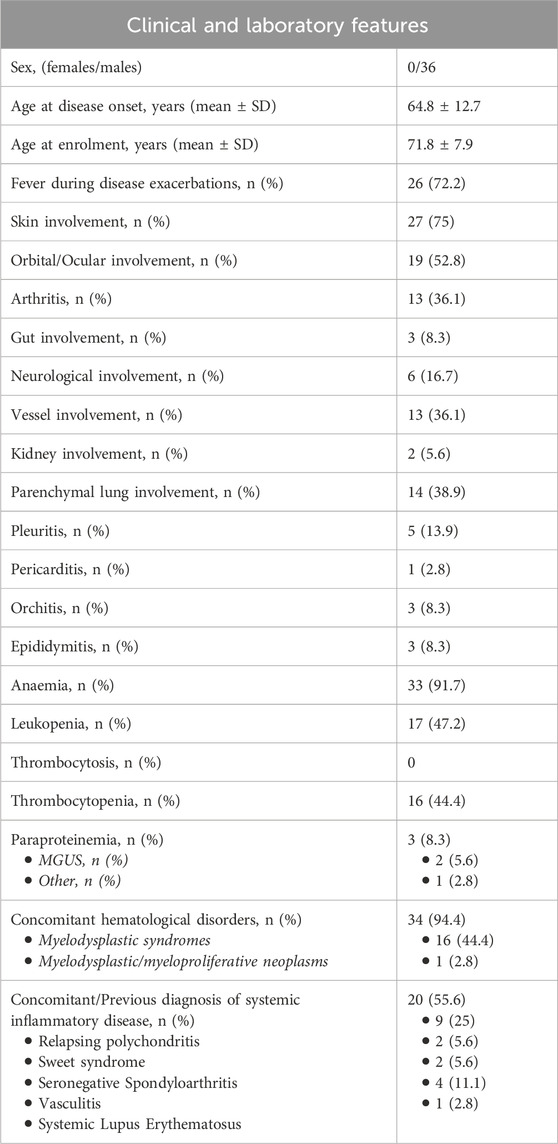
Table 1. Demographic, clinical and laboratory features describing the patients treated with conventional disease modifying anti-rheumatic drugs (cDMARDs) in the present study, either as monotherapy or as cDMARDs combinations.
Details about the cDMARDs employed in the 28 patients undergoing monotherapy are reported in Table 2. Data on treatment outcomes (CR, PR, and F according to the definitions provided in the Methods section) were available for 22 treatment courses and are also depicted in Table 2. A CR to cDMARDs monotherapy was reported in 4/22 (18.2%) courses. These were treated with azathioprine 75 mg/day in one case and with methotrexate in 3 cases, two of which initially administered 15 mg/week and later increased to 20 mg/week; the third case was treated with 15 mg/week, later increased to 25 mg/week.
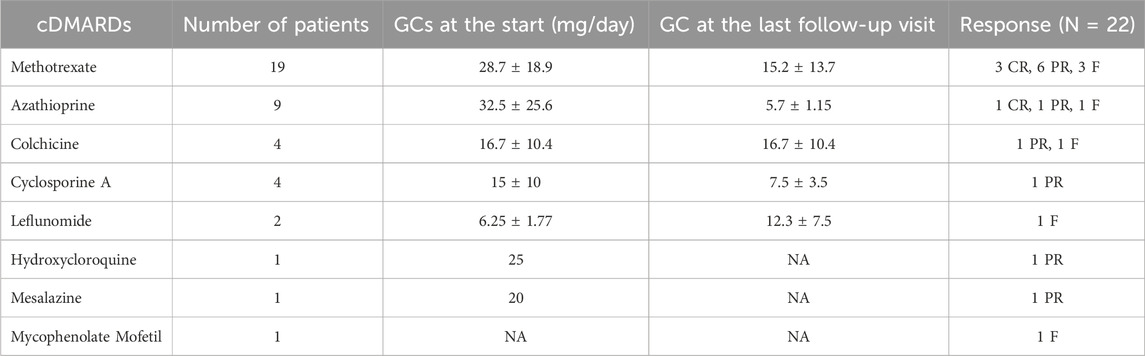
Table 2. cDMARDs used as monotherapy included in the present study. This table depicts data on patients that underwent cDMARDs as monotherapy: the mean prednisone or equivalent dose at the start of cDMARD, the mean prednisone or equivalent dose at the last follow-up visit while on cDMARD and the overall response to the treatment are reported. Note that the treatment response, provided according to definitions reported in the Methods section, is available for 22 treatment courses; mean and standard deviations for glucocorticoid dosages at the start of cDMARDs and at the last assessment have been calculated based on data from 33 treatment courses. The decrease in the glucocorticoid dosage was statistically significant for methotrexate (p = 0.02), while the difference did not achieve significance for azathioprine (p = 0.17); this computation was not performed for other cDMARDs because of the small sample size. Abbreviations: cDMARDs, conventional disease modifying anti-rheumatic drugs; CR, complete response; F, failure; GCs, glucocorticoids (prednisone or equivalent); NA, not available; PR, partial response.
A PR was reported in 11/22 (50%) courses: six treated with methotrexate (3 with 10 mg/week, one with 15 mg/week, one with 20 mg/week, one with no data regarding dose); one treated with hydroxychloroquine (400 mg/day); one treated with mesalazine (800 mg x3/day, later decreased to 400 × 3/day); one treated with cyclosporine (150 mg x2/day); one treated with azathioprine (100 mg/day); and one with colchicine (1 mg/day).
Failure was reported for 7/22 (31.8%) courses, as follows: three treated with methotrexate (10 mg/week later increased to 15 mg/week in one case, 10 mg/week in the second patient, 15 mg/week in the third patient), one treated with mycophenolate mofetil (dosage not provided), one case treated with leflunomide (dosage not provided), one treated with azathioprine (50 mg/day), and one treated with colchicine (1 mg/day).
The median duration of cDMARD treatment was 5 (IQR:11.25) months. At the time of data analysis, the current use of cDMARD was as follows: 16/28 (58.1%) patients discontinued after a median of 9 (9) months; 5/28 (17.9%) patients continued cDMARDs with biotechnological DMARDs; 6/28 (21.4%) patients continued cDMARDs alone; data for one patient was missing.
Data regarding the reasons leading to cDMARD withdrawal were available for 12 cases and were the following: no efficacy in 2 cases, poor efficacy in 2 cases, loss of efficacy in 2 cases, adverse events in 6 cases; there was no association between the duration of cDMARDs treatment and the withdrawal (linear regression model: β1 estimate = −10.36, p = 0.32) or the cause of withdrawal (β1 estimate from lack/loss of efficacy to adverse events = 14.00; p = 0.18).
Data on the use of GCs were available for 33 treatment courses and are depicted in Table 2; all patients were treated with GC at the start of cDMARD monotherapy, and no discontinuation was observed during the follow-up period. The median (IQR) prednisone equivalent dosage was 20 (17.5) mg/day at the start of cDMARDs, 15 (24.1) mg/day after 3 months, 21.25 (16.9) mg/day after 6 months, and 8.75 (4.38) mg/day at the 12-month assessment. No statistically significant differences were observed in the daily GC dosage from the start of cDMARDs to the 3-month (p = 0.43), 6-month (p = 0.31), and 12-month (p = 0.21) visits. Nine (27.3%) patients continued cDMARDs for more than 12 months; the decrease in GC dosage from the start of treatment to the last assessment was not statistically significant in these patients [from 30 (35) to 15 (35) mg/day, p = 0.18].
On the contrary, GCs sparing effect was statistically significant in the 19 cases treated with methotrexate, with a daily GC dosage of 28.7 ± 18.9 mg/day at the start of treatment and 15.2 ± 13.7 mg/day at the last assessment, after a median treatment duration of 6 (12.5) months (p = 0.02). The GCs sparing effect was not statistically significant for azathioprine (29.7 ± 21.4 versus 12.5 ± 10.9, p = 0.17); this aspect was not assessed for other cDMARDs because of the small sample sizes.
As depicted in Table 3, a combination of cDMARDs was used in 8 cases, mainly as a combination of colchicine with another cDMARD: two patients with colchicine (1 mg/day) and methotrexate (15 mg/week), one patient with colchicine (0.5 mg/day) and hydroxychloroquine (200 mg/day), one patient with colchicine (0.5 mg/day) and leflunomide (20 mg/day). Other combinations included methotrexate (20 mg/week) plus hydroxychloroquine (300 mg/day), methotrexate (20 mg/week) plus azathioprine (50 mg/day), and methotrexate (10 mg/week) plus cyclosporine (200 mg/day), each used in one patient. The eighth patient received methotrexate (15 mg/week) plus hydroxychloroquine (200 mg/day) plus colchicine (1 mg/day).
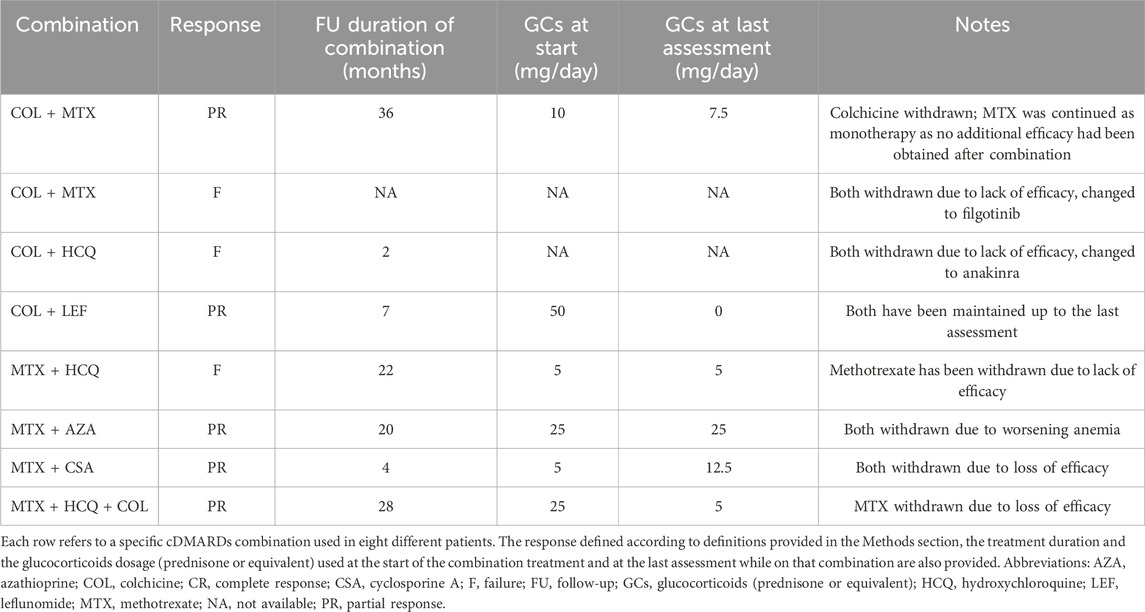
Table 3. Treatment courses with conventional disease-modifying anti-rheumatic drugs (cDMARDs) combinations included in the present study.
No cases achieved a complete response, while partial response was observed in 5/8 (62.5%) cases, as detailed in Table 3 along with other treatment specifics.
Among the 36 patients who received at least one course of cDMARDs (either as monotherapy or in combination), 17 AEs were observed in 12 (33.3%) patients throughout the follow-up period. In 7 out of 17 cases, AEs led to treatment discontinuation. Adverse events consisted of cytopenia (n = 9), gastrointestinal intolerance (n = 6), skin reaction (n = 1), and cutaneous abscess (n = 1). Adverse events are specifically illustrated in Table 4.
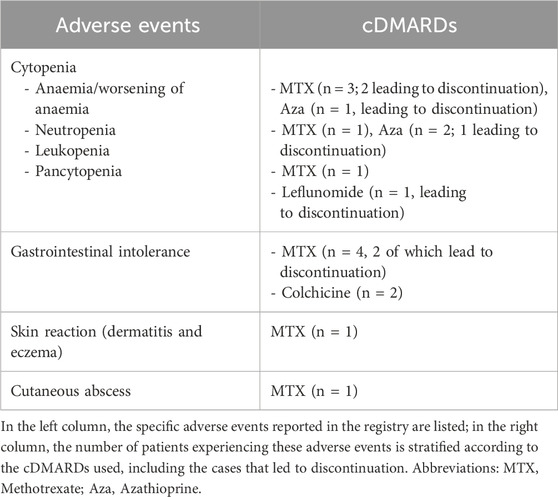
Table 4. Adverse events recorded during conventional disease modifying anti-rheumatic drugs (cDMARDs) treatment follow-up, considering cDMARDs monotherapy and combination therapy.
AEs occurred in 4/16 patients with myelodisplastic syndrome and 8/20 patients without myelodisplastic syndrome (p = 0.48); peripheral blood count alterations occurred during cDMARDs treatment in 2/16 patients with myelodisplastic syndrome and 5/20 patients without myelodisplastic syndrome (p = 0.43).
Currently, there are no established treatment guidelines for this newly recognized clinical entity, as no randomized controlled trials have been conducted. Consequently, managing VEXAS syndrome relies on clinical experience from other autoinflammatory conditions and insights from recently published case series and case reports.
Since immunologic studies of patient samples and zebrafish models in VEXAS syndrome demonstrated upregulation of multiple cytokine signatures including TNF, IL-6 and IFN-γ (Beck et al., 2020), a broad therapeutic approach could be beneficial rather than the specific blockade of single cytokines.
According to the limited data based on case series, cDMARDs are mostly effective temporarily and do not exhibit significant steroid-sparing effect in VEXAS syndrome (Bourbon et al., 2021; Koster et al., 2021; van der Made et al., 2022; Patel and Young, 2022; Boyadzhieva et al., 2023). In our study a complete response could be achieved in less than one-fifth of the patients treated with cDMARDs as monotherapy and none requiring a combination of cDMARDs, likely due to more severe disease activity in this group. About half of the patients reported some improvement in either the severity of symptoms or the frequency of inflammatory exacerbations, both in the monotherapy group and in those receiving cDMARDs’ combination therapy. Conversely, at least 30% of VEXAS patients did not experience any therapeutic benefit from cDMARDs. Overall, these results suggest that cDMARDs may have only a minor effect in patients with VEXAS syndrome. Furthermore, our findings confirm the poor GC-sparing effect. In this regard, discontinuing systemic steroids was nearly impossible while using cDMARDs, and the daily dosage of GCs did not decrease throughout the follow-up period in a significant fashion. An exception was observed in the subgroup of patients treated with methotrexate, who showed a statistically significant halving of the daily GCs dosages. This may suggest a more substantial role of methotrexate, but not enough sample sizes were available to assess this aspect for other cDMARDs.
Most patients treated with cDMARDs had to discontinue the treatment partially due to safety issues and partially due to lack or loss of efficacy or poor clinical benefit. However, there was no association between the duration of cDMARDs treatment and the likelihood of discontinuation. This finding indicates that both inefficacy/loss of efficacy and safety concerns equally impacted treatment persistence, i.e., treatment discontinuation was not preferentially related to efficacy or safety issues. Similarly, no statistically significant association was observed between treatment duration and cDMARDs withdrawal, indicating that treatment discontinuation equally occurred during the entire follow-up period. Therefore, the occurrence of discontinuation was not polarised either in the initial months or in later stages, suggesting that efficacy or safety issues could arise with equal probability both in the first weeks of treatment and in subsequent phases.
Overall, according to our results and in line with the literature, the therapeutic role of cDMARDs appears quite poor in patients with this condition. However, since no treatment has proven definitively effective in VEXAS syndrome, cDMARDs may be considered a potential option and could be used as a therapeutic trial when other treatments are not feasible or effective.
The study’s limitations include the relatively small number of enrolled patients and the nature of data collection, as a registry can lead to various interpretations of results across different centers worldwide. Although these results need confirmation from future studies with larger cohorts to better assess the role of cDMARDs at varying dosages and to distinguish among different cDMARDs, the present study provides valuable evidence from real-life data collected from a consistent number of patients. Moreover, it would be helpful to assess the GCs sparing effect of cDMARDs other than methotrexate, but this will require larger sample sizes. Actually, response criteria were intentionally chosen with a relatively low stringent approach, including the absence of a mandatory reduction in glucocorticoids dosage. This decision was driven by the limited available knowledge on the real effectiveness of cDMARDs in patients with VEXAS syndrome and the recognized challenge of achieving a complete response when requiring a combination of symptoms resolution, normalization of laboratory parameters, and steroid dose reduction. Notably, attaining clinical and laboratory control without increasing a previously inadequate steroid dosage represents per se a meaningful achievement.
In conclusion, many VEXAS patients report a partial benefit from cDMARDs, while a smaller yet not negligible number of patients may exhibit a complete response. Therefore, given the limited treatment strategies currently available, cDMARDs may represent a therapeutic option to consider for VEXAS syndrome, particularly when the initial glucocorticoid dosage is low and the need for a steroid-sparing effect is not immediately urgent.
The authors of this publication [Antonio Vitale, Valeria Caggiano, Jessica Sbalchiero, Edoardo Conticini, Lorenzo Dagna, Alessandro Tomelleri, Corrado Campochiaro, Micol Frassi, Francesca Crisafulli, Franco Franceschini, Jurgen Sota, Francesco Gavioli, José Hernández-Rodríguez, Verónica Gómez-Caverzaschi, Olga Araújo, Paolo Sfriso, Sara Bindoli, Chiara Baggio, Carlomaurizio Montecucco, Sara Monti, Monica Bocchia, Alberto Balistreri, Bruno Frediani, Claudia Fabiani and Luca Cantarini] belong to institutes that are members of the ERN RITA [Azienda Ospedaliero-Universitaria Senese of Siena; Università Vita-Salute San Raffaele; University of Brescia; University of Padua; University of Pavia; Hospital Clínic of Barcelona].
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. Requests to access these datasets should be directed to the corresponding author.
The studies involving humans were approved by Azienda Ospedaliero Universitaria Senese. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
AV: Conceptualization, Investigation, Methodology, Writing–original draft. FL: Investigation, Writing–original draft. VC: Investigation, Writing–original draft. AH-A: Investigation, Writing–review and editing. EM-N: Investigation, Writing–review and editing. GG-B: Investigation, Writing–review and editing. JT-R: Investigation, Writing–review and editing. PK-C: Investigation, Writing–review and editing. PH: Investigation, Writing–review and editing. AC: Investigation, Writing–review and editing. MB: Investigation, Writing–original draft. LD: Investigation, Writing–review and editing. AT: Investigation, Writing–review and editing. CC: Investigation, Writing–review and editing. MF: Investigation, Writing–review and editing. FC: Investigation, Writing–review and editing. FF: Investigation, Writing–review and editing. JH-R: Investigation, Writing–review and editing. VG-C: Investigation, Writing–review and editing. OA: Investigation, Writing–review and editing. PS: Investigation, Writing–review and editing. SB: Investigation, Writing–review and editing. CB: Investigation, Writing–review and editing. JeS: Investigation, Writing–review and editing. JuS: Investigation, Writing–review and editing. AT: Investigation, Writing–review and editing. IV: Investigation, Writing–review and editing. MP: Investigation, Writing–review and editing. AC: Investigation, Writing–review and editing. MD’A: Investigation, Writing–review and editing. AP: Investigation, Writing–review and editing. IM: Investigation, Writing–review and editing. HM: Investigation, Writing–review and editing. RC: Investigation, Writing–review and editing. FG: Investigation, Writing–review and editing. GL: Investigation, Writing–review and editing. FI: Investigation, Writing–review and editing. CM: Investigation, Writing–review and editing. SM: Investigation, Writing–review and editing. GR-I: Investigation, Writing–review and editing. AS-P: Investigation, Writing–review and editing. PT: Investigation, Writing–review and editing. CG: Investigation, Writing–review and editing. OV: Investigation, Writing–review and editing. RB: Investigation, Writing–review and editing. RV: Investigation, Writing–review and editing. EC: Investigation, Writing–review and editing. FL: Investigation, Writing–review and editing. GR: Investigation, Writing–review and editing. EB: Investigation, Writing–review and editing. AG-G: Investigation, Writing–review and editing. MP-R: Investigation, Writing–review and editing. MB: Investigation, Writing–review and editing. EW-S: Investigation, Writing–review and editing. KJ-R: Investigation, Writing–review and editing. Ade-T: Investigation, Writing–review and editing. AB: Investigation, Writing–review and editing. BF: Investigation, Writing–review and editing. CF: Investigation, Writing–review and editing. LC: Investigation, Writing–review and editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
This research is supported (not financially) by the European Reference Network (ERN) for Rare Immunodeficiency, Autoinflammatory and Autoimmune Diseases (RITA). We thank the University of Siena for the financial support in supporting the open access fees.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Beck, D. B., Ferrada, M. A., Sikora, K. A., Ombrello, A. K., Collins, J. C., Pei, W., et al. (2020). Somatic mutations in UBA1 and severe adult-onset autoinflammatory disease. N. Engl. J. Med. 383 (27), 2628–2638. doi:10.1056/NEJMoa2026834
Bourbon, E., Heiblig, M., Gerfaud, V. M., Barba, T., Durel, C. A., Lega, J. C., et al. (2021). Therapeutic options in VEXAS syndrome: insights from a retrospective series. Blood 137 (26), 3682–3684. doi:10.1182/blood.2020010177
Boyadzhieva, Z., Ruffer, N., Kotter, I., and Krusche, M. (2023). How to treat VEXAS syndrome: a systematic review on effectiveness and safety of current treatment strategies. Rheumatol. Oxf. 62 (11), 3518–3525. doi:10.1093/rheumatology/kead240
Ferrada, M. A., Sikora, K. A., Luo, Y., Wells, K. V., Patel, B., Groarke, E. M., et al. (2021). Somatic mutations in UBA1 define a distinct subset of relapsing polychondritis patients with VEXAS. Arthritis Rheumatol. 73 (10), 1886–1895. doi:10.1002/art.41743
Georgin-Lavialle, S., Terrier, B., Guedon, A. F., Heiblig, M., Comont, T., Lazaro, E., et al. (2022). Further characterization of clinical and laboratory features in VEXAS syndrome: large-scale analysis of a multicentre case series of 116 French patients. Br. J. Dermatol 186 (3), 564–574. doi:10.1111/bjd.20805
Gurnari, C., Koster, L., Baaij, L., Heiblig, M., Yakoub-Agha, I., Collin, M., et al. (2024b). Allogeneic hematopoietic cell transplantation for VEXAS syndrome: results of a multicenter study of the EBMT. Blood Adv. 8 (6), 1444–1448. doi:10.1182/bloodadvances.2023012478
Gurnari, C., Pascale, M. R., Vitale, A., Diral, E., Tomelleri, A., Galossi, E., et al. (2024a). Diagnostic capabilities, clinical features, and longitudinal UBA1clonal dynamics of a nationwide VEXAS cohort. Am. J. Hematol. 99 (2), 254–262. doi:10.1002/ajh.27169
Gutierrez-Rodrigues, F., Kusne, Y., Fernandez, J., Lasho, T., Shalhoub, R., Ma, X., et al. (2023). Spectrum of clonal hematopoiesis in VEXAS syndrome. Blood 142 (3), 244–259. doi:10.1182/blood.2022018774
Koster, M. J., Kourelis, T., Reichard, K. K., Kermani, T. A., Beck, D. B., Cardona, D. O., et al. (2021). Clinical heterogeneity of the VEXAS syndrome: a case series. Mayo Clin. Proc. 96 (10), 2653–2659. doi:10.1016/j.mayocp.2021.06.006
Nakajima, H., and Kunimoto, H. (2024). VEXAS syndrome. Int. J. Hematol. Epub ahead of print. PMID: 38819628. doi:10.1007/s12185-024-03799-9
Patel, B. A., and Young, N. S. (2022). Towards treatments for VEXAS. Br. J. Haematol. 196 (4), 804–805. doi:10.1111/bjh.17930
van der Made, C. I., Potjewijd, J., Hoogstins, A., Willems, H. P. J., Kwakernaak, A. J., de Sevaux, R. G. L., et al. (2022). Adult-onset autoinflammation caused by somatic mutations in UBA1: a Dutch case series of patients with VEXAS. J. Allergy Clin. Immunol. 149 (1), 432–439.e4. doi:10.1016/j.jaci.2021.05.014
Keywords: cDMARDs, clinical outcomes, autoinflammatory diseases, diagnosis, treatment
Citation: Vitale A, Leone F, Caggiano V, Hinojosa-Azaola A, Martín-Nares E, Guaracha-Basañez GA, Torres-Ruiz J, Ayumi Kawakami-Campos P, Hissaria P, Callisto A, Beecher M, Dagna L, Tomelleri A, Campochiaro C, Frassi M, Crisafulli F, Franceschini F, Hernández-Rodríguez J, Gómez-Caverzaschi V, Araújo O, Sfriso P, Bindoli S, Baggio C, Sbalchiero J, Sota J, Tufan A, Vasi I, Piga M, Cauli A, D’Agostino MA, De Paulis A, Mormile I, Mayrink Giardini HA, Cordeiro RA, Gavioli F, Lopalco G, Iannone F, Montecucco C, Monti S, Ruiz-Irastorza G, Soto-Peleteiro A, Triggianese P, Gurnari C, Viapiana O, Bixio R, Vitetta R, Conticini E, La Torre F, Ragab G, Batu ED, González-García A, Peña-Rodríguez M, Bocchia M, Wiesik-Szewczyk E, Jahnz-Rózyk K, de-la-Torre A, Balistreri A, Frediani B, Fabiani C and Cantarini L (2025) Efficacy and safety of conventional disease-modifying antirheumatic drugs in VEXAS syndrome: real-world data from the international AIDA network. Front. Pharmacol. 16:1539756. doi: 10.3389/fphar.2025.1539756
Received: 04 December 2024; Accepted: 11 February 2025;
Published: 07 March 2025.
Edited by:
Emanuela Ricciotti, University of Pennsylvania, United StatesReviewed by:
David Hagin, Tel Aviv Sourasky Medical Center, IsraelCopyright © 2025 Vitale, Leone, Caggiano, Hinojosa-Azaola, Martín-Nares, Guaracha-Basañez, Torres-Ruiz, Ayumi Kawakami-Campos, Hissaria, Callisto, Beecher, Dagna, Tomelleri, Campochiaro, Frassi, Crisafulli, Franceschini, Hernández-Rodríguez, Gómez-Caverzaschi, Araújo, Sfriso, Bindoli, Baggio, Sbalchiero, Sota, Tufan, Vasi, Piga, Cauli, D’Agostino, De Paulis, Mormile, Mayrink Giardini, Cordeiro, Gavioli, Lopalco, Iannone, Montecucco, Monti, Ruiz-Irastorza, Soto-Peleteiro, Triggianese, Gurnari, Viapiana, Bixio, Vitetta, Conticini, La Torre, Ragab, Batu, González-García, Peña-Rodríguez, Bocchia, Wiesik-Szewczyk, Jahnz-Rózyk, de-la-Torre, Balistreri, Frediani, Fabiani and Cantarini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luca Cantarini, Y2FudGFyaW5pbHVjYUBob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.