 Christina König1,2Otto Frey3*Susanne Himmelein4Lisa Mulack1Alexander Brinkmann5
Christina König1,2Otto Frey3*Susanne Himmelein4Lisa Mulack1Alexander Brinkmann5 Aritz Perez Ruiz de Garibay4Tobias Bingold4
Aritz Perez Ruiz de Garibay4Tobias Bingold4- 1Department of Intensive Care Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 2Center for Anti-Infective Research and Development, Hartford Hospital, Hartford, CT, United States
- 3Department of Pharmacy, General Hospital of Heidenheim, Heidenheim, Germany
- 4ADVITOS GmbH, Munich, Germany
- 5Department of Anesthesiology, Special Pain Management and Intensive Care Medicine, Heidenheim General Hospital, Heidenheim, Germany
Background: Acute kidney injury (AKI) requiring continuous renal replacement therapy is common in critically ill patients. The ADVanced Organ Support (ADVOS) system is a novel hemodialysis machine that uses albumin enriched dialysate which allows the removal of protein-bound toxins and drugs. To date, data on antimicrobial removal under ADVOS has not yet been reported.
Methods: An in vitro study was conducted using whole porcine blood and continuous infusions of different antimicrobial agents to investigate the effect of ADVOS on drug exposure. Drugs with varying protein binding, molecular weights and renal clearances, anidulafungin, cefotaxime, daptomycin, fluconazole, ganciclovir, linezolid, meropenem and piperacillin were studied.
Results: All studied drugs were removed during the in vitro ADVOS experiment. Clearance under ADVOS (CLADVOS) for low protein-bound drugs, such as cefotaxime, fluconazole, ganciclovir, linezolid, meropenem and piperacillin ranged from 2.74 to 3.4 L/h at a blood flow of 100 mL/min. With a doubling of flow rate CL for these drugs increased. Although efficiently removed, this effect was not seen for CLADVOS in high protein-bound substances such as daptomycin (1.36 L/h) and anidulafungin (0.84 L/h).
Conclusion: The ADVOS system effectively removed protein-bound and unbound antimicrobials to a significant extent indicating that dose adjustments are required. Further, clinical studies are necessary to comprehensively assess the impact of ADVOS on antimicrobial drug removal. Until clinical data are available, therapeutic drug monitoring should guide antimicrobial dosing under ADVOS.
1 Introduction
Patients in the intensive care unit (ICU) who suffer from acute organ failure often require extracorporeal therapies to support failing organ systems (Huber and Ruiz de Garibay, 2020).
Moreover, infections are common in these patients and may trigger and/or worsen the progressive failure of one or more organ systems (Bajaj et al., 2014). Renal replacement therapy (RRT) for acute kidney injury (AKI), albumin dialysis, or plasma exchange for acute-on-chronic liver failure (ACLF) or acute liver failure (ALF) can be used to temporarily support failing organs. In RRT molecular size, protein binding, renal excreted fraction and volume of distribution are key determinants of drug removal, impacting under- or overdosing with risking adverse patient outcomes (Kollef et al., 2021). Additonally, studies have demonstrated that achieving appropriate antimicrobial exposure is crucial for reducing mortality rates in critically ill patients (Pai Mangalore et al., 2022; Roberts et al., 2014; Gatti et al., 2024). To guide antimicrobial dosing, in vitro studies (Roehr et al., 2015) as well as clinical trials investigating antimicrobial dosing under RRTs in critically ill patients (Roberts et al., 2020) have been published.
Among the profusion of extracorporeal organ replacement devices, the ADVanced Organ Support (ADVOS) albumin hemodialysis system (ADVITOS GmbH, Munich, Germany) has recently reported promising results in observational trials and is gaining attention for critically ill patients (Acharya et al., 2022; Sommerfeld et al., 2023). ADVOS is intended to remove water-soluble toxic substances, protein-bound toxic substances, to normalize or improve the composition of blood in case of e.g., electrolyte or acid-base disturbances (e.g., metabolic acidosis or respiratory acidosis). Additionally, it removes fluids in case of fluid overload in patients with acute, chronic and acute-on-chronic liver failure and/or renal failure and/or acidosis. However, studies investigating drug elimination under ADVOS have not been carried out systematically yet. Thus, understanding mechanistic and clinical factors that influence drug elimination is of major importance to attain appropriate drug exposure. Therefore, the present study employed a standardized in vitro blood model to assess the ability of ADVOS to remove a range of antimicrobial substances widely used in the ICU. Moreover, we aimed to quantify the amount of drug elimination to translate this information in clinical dosing regimens.
2 Materials and methods
2.1 In vitro model and blood preparation
Fresh porcine blood (Münchner Schlachthof Betriebs GmbH, Munich, Germany) was diluted with modified Ringer’s solution to achieve a hematocrit of 36%, standard electrolyte concentrations, and normal blood gas values. Porcine blood was mixed with human albumin (Albunorm 20%, Octapharma GmbH, Langenfeld, Germany) to obtain a human albumin level of 35 g/L. To prevent coagulation, 30,000 IU/L of heparin (Ratiopharm, Ulm, Germany) was added. The blood was maintained at a constant temperature of 37°C while continuously being stirred at 130 rpm. Drugs listed in Table 1 were individually added to attain initial concentrations as reported in Table 2.
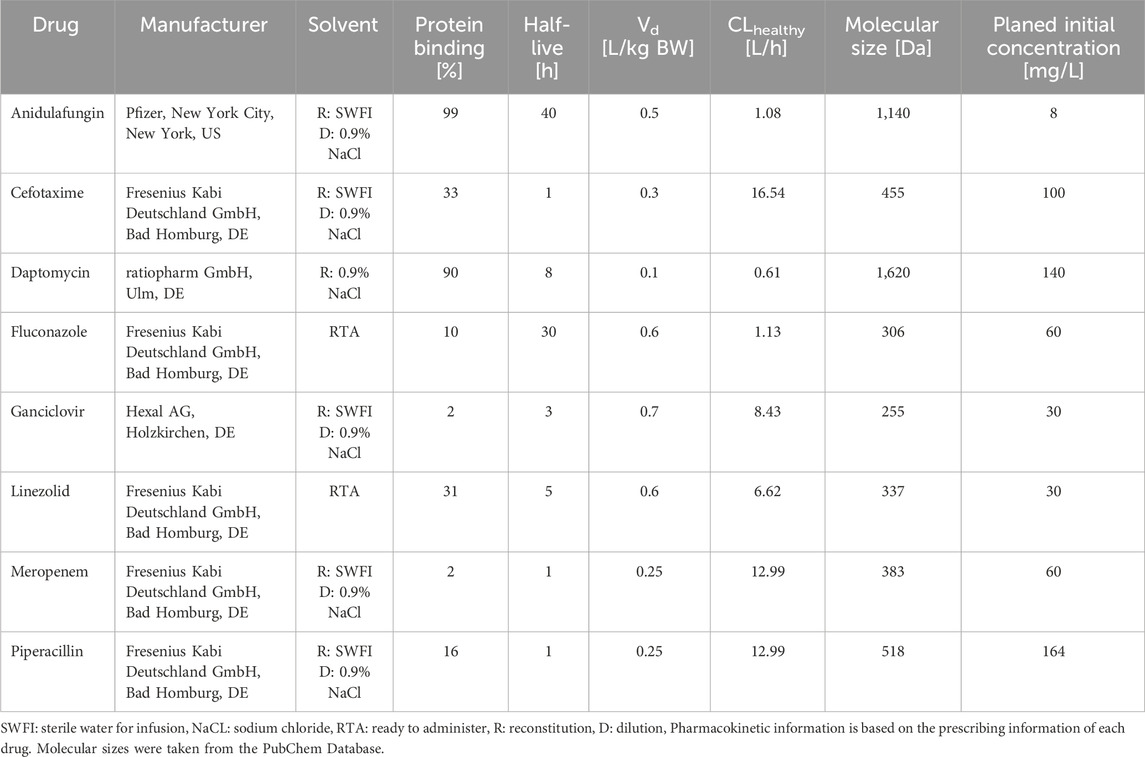
Table 1. Study drugs including pharmacokinetic properties.
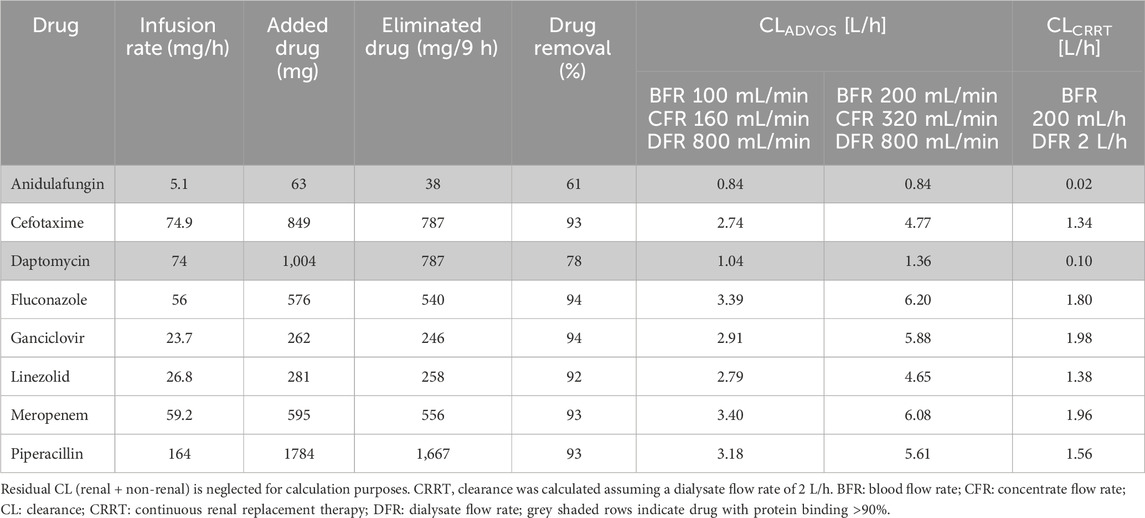
Table 2. Drug concentrations and clearance results.
2.2 ADVOS hemodialysis system
The ADVOS multi hemodialysis system (ADVITOS GmbH, Munich, Germany) utilizes three circuits (Figure 1) with two ELISIO 19H dialyzers (Nipro D. Med Germany GmbH, Hamburg, Germany) in a concurrent extracorporeal circuit. Blood flow rates (BFR) ranging from 100 to 500 mL/min are used with recirculating, albumin enriched (200 mL, 20% human albumin) dialysate at a flow rate of 800 mL/min (dialysate circuit) which employs acidic (Acid) and alkaline concentrates (Base) along with water for pH adjustments.
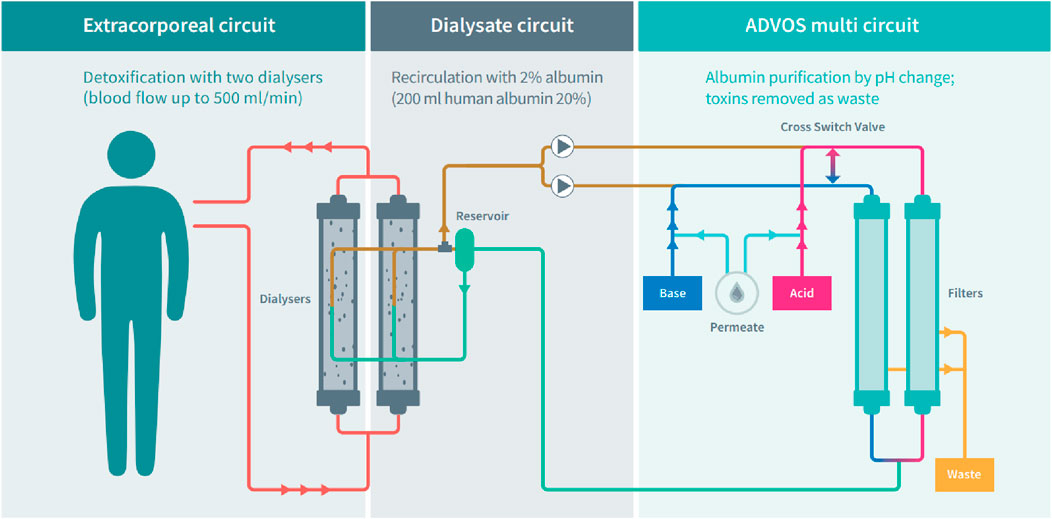
Figure 1. Schematic presentation of the ADVOS multi hemodialysis system. Adapted from https://advitos.com/wp-content/uploads/2023/07/20220630_ADVOS_kreislauf_poster_EN.pdf.
The dialysate is subsequently divided into an acidic and an alkaline path (ADVOS multi circuit). Herein, protein-bound and water-soluble toxins separate from the albumin dialysate through pH adjustment and convection. This arrangement effectively removes protein-bound molecules by inducing conformational changes in albumin, releasing bound molecules which are then removed through convection via two filters (ELISIO 11 H, Nipro D. Med Germany GmbH, Hamburg, Germany). Thereafter, the unloaded albumin dialysate is reintroduced into the dialysate circuit at a customized pH (Acharya et al., 2022). This conformation allows a continuous and efficient removal of protein-bound molecules as reported previously (Acharya et al., 2022; Sommerfeld et al., 2023; Huber et al., 2017; Falkensteiner et al., 2021). The concentrate flow rate (CFR) can range between 160 and 320 mL/min, determining both the quantity of dialysate cleaned via convective transport and the amount of fresh concentrate pumped into the system in the ADVOS multi circuit.
2.3 Experimental setup
The experiment comprised various consecutive phases designed to facilitate pharmacokinetic profiling of each drug during ADVOS treatments (Figure 2). A 4-L blood beaker containing 35 g/L albumin (Albunorm 20%, Octapharma GmbH, Langenfeld, Germany) was spiked with each individual drug (Table 2). The initial drug concentrations were set to mimic physiological peak concentrations (Roehr et al., 2015).
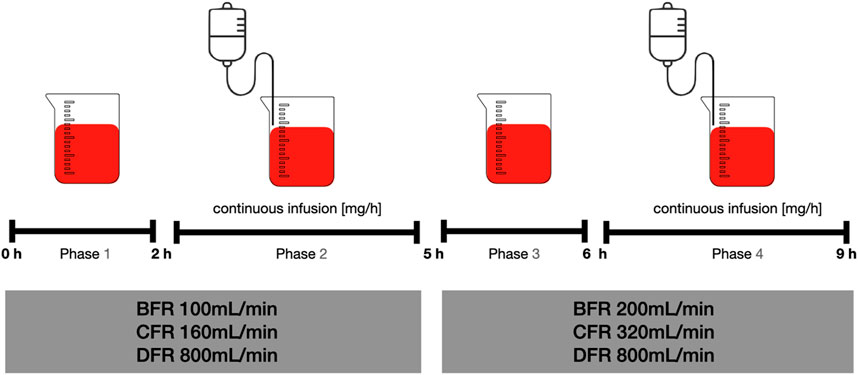
Figure 2. Consecutive phases of the experiment. BFR: Blood flow rate, CFR: Concentrate flow rate, DFR: Dialysate flow rate.
In phase one, ADVOS multi was started with a BFR, CFR and dialysate flow rate (DFR) of 100, 160, and 800 mL/min, respectively. Sampling from the beaker stated at the beginning (T0) to assess starting concentrations with an additional sample at 2 h (T2).
Phase two was initiated by the start of continuous infusions for 3 h as outlined in Table 2 with subsequent sampling at 5 h (T5).
For phase three, BFR and CFR were doubled to 200 mL/min and 320 mL/min, respectively while DFR remained fixed (800 mL/min). Sampling was performed after 1 h (T6) followed by phase four, where continuous infusion was resumed and ceased with a final sample at T9.
Additional blood samples were collected from the tubing system of the machine (pre and post the two parallel dialyzers) at T0, T2, T5, T6 and T9 h.
2.3.1 Drug quantification
The blood samples were centrifuged (4,000 rpm, 10 min), and the resulting serum supernatant separated into aliquots, which were stored at −80°C until further analysis. To obtain protein-free ultrafiltrate 800 µL serum was added to a Centrifree® tube (Ultrafiltration device with Ultracel® regenerated cellulose membrane, Merck KGaA, Germany) and spun at 1,000 × g, 30 min, 37°C. Subsequent quantification for both serum and ultrafiltrate was conducted using validated high performance liquid chromatography (HPLC) methods with UV detection. The methods already demonstrated linearity, with a relative standard deviation (SD) for intra- and inter-day precision and accuracy <10% at high, medium and low concentrations (Zimmer et al., 2021).
2.4 Pharmacokinetic calculations
Pharmacokinetic parameters of each drug were calculated through a non-compartmental analysis, assuming first-order kinetics and a volume of distribution of 4 L (beaker volume), utilizing Microsoft Excel 365 (Microsoft Corp., Redmond, WA, United States). A dialysate flow rate of 2 L/h was assumed for the calculation of CLCRRT (Equation 2). This is based on a dialysis dose of 25 mL/kg/h for an 80 kg patient, as suggested by the KDIGO 2012 clinical practice guideline for patients with AKI requiring CRRT (Khwaja, 2012). ADVOS clearance (CLADVOS) (Equation 1) and protein binding (PB) (Equation 3) were calculated as follows:
Dose (D) adjustments (Equation 5) were calculated using the Dettli equation (Equation 4) which determines the individual clearance (CLindividual) based on the underlying renal function and the non-renal elimination fraction (Q0) (Dettli, 1974).
Remaining renal function was set to either a creatinine clearance (CrCL) of 25 mL/min or anuria (CrCL = 0 mL/min). CLindividual resembles the endogenous CL as it combines non-renal and residual renal elimination based on CrCL.
The individually required dose (D) without ADVOS was calculated by proportionally adjusting CLindividual to CLhealthy, as reported in the literature (see Table 1), and multiplying it by the standard licensed dose.
The required dose using ADVOS (DADVOS) was calculated by adding the CLADVOS from our experiments to CLindividual (Equation 6).
Visualization and statistical evaluation were performed using linear or non-linear regression methods included in Prism 9 (GraphPad Software, San Diego, CA, United States).
3 Results
3.1 Protein binding in vitro
Protein binding were comparable to those found in the literature (Figure 3). As the free fraction of ganciclovir was below the limit of quantification (LLOQ) protein binding was calculated using ½ of the LLOQ.
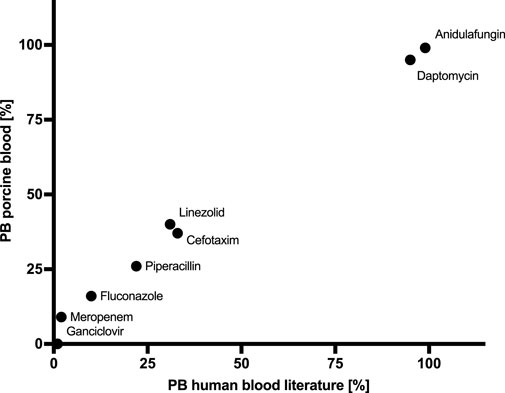
Figure 3. Protein binding (PB) in vitro vs. literature.
3.2 Observed drug concentrations and clearance during ADVOS treatments
All drugs showed a decline in concentrations (Figure 4). At a BFR of 100 mL/min, low protein-bound drugs with a low molecular weight, such as cefotaxime, fluconazole, ganciclovir, linezolid, meropenem and piperacillin showed a CLADVOS ranging from 2.74 to 3.4 L/h. An increase in the BFR to 200 mL/min resulted in a doubling of CLADVOS for all the aforementioned drugs.
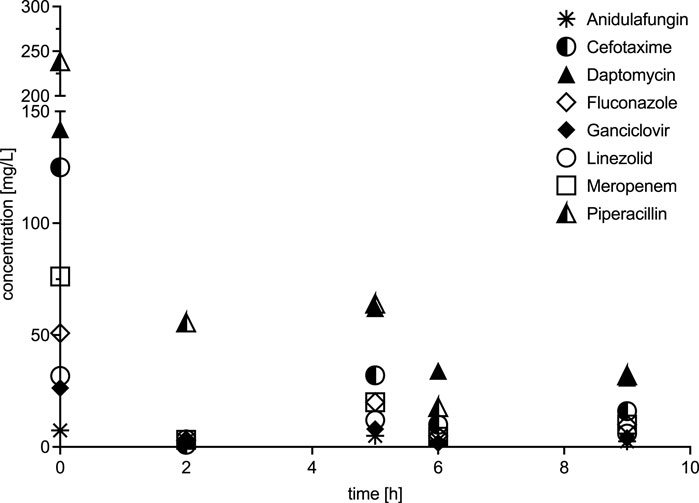
Figure 4. Concentration profiles over time.
For the two drugs with the largest molecular weight and highest protein binding daptomycin and anidulafungin CLADVOS at a BFR of 100 mL/min were 0.84 and 1.06 L/h, respectively. Doubling the BFR resulted in a moderate increase in CLADVOS only for daptomycin (1.36 L/h).
3.3 Calculated dose adjustment for ADVOS treatments in patients with impaired renal function
Dose calculations based on the CLCRRT and on the CLADVOS under the two different settings of ADVOS therapy are shown in Table 3. Drugs with a high protein binding ≥90% such as anidulafungin and daptomycin as well as linezolid with a moderate protein binding revealed an extended CLADVOS in the in vitro experiment (Table 2) resulting in increased daily dosages when compared to the licensed maintenance dosages for patients with CrCL >60 mL/min. In contrast, the low protein-bound (<35%) beta-lactam antibiotics such as cefotaxime, meropenem and piperacillin as well as the antiviral agent ganciclovir showed a significantly lower CLADVOS (Table 2), compared to patients with normal renal function (CLhealthy, Table 1). Thus, lower recommended doses were calculated since the cumulated CLindividual at CrCL ≤25 mL/min and CLADVOS was not as high as CLhealthy for those drugs. In the case of fluconazole, at a blood flow of 100 mL/min CLADVOS triplicates (Table 2) the CLhealthy (Table 1), which results in higher required doses during ADVOS treatments (Table 3). Finally, the calculated dosages under CRRT were lower than under ADVOS for each of the drugs (Table 3).
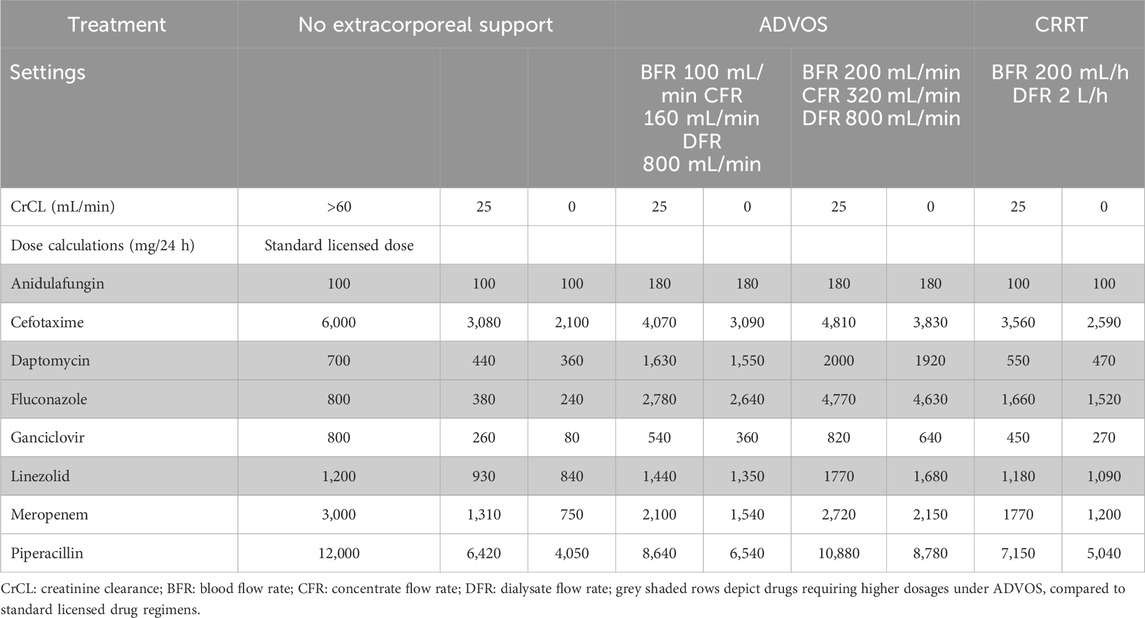
Table 3. Dose calculations based on in vitro CLADVOS and calculated CLCRRT.
4 Discussion
To date, several cohort studies as well as data from a patient registry (Fuhrmann et al., 2021; Fuhrmann et al., 2020) demonstrate effective removal of water-soluble and protein-bound substances with ADVOS (Huber et al., 2017; Falkensteiner et al., 2021; Kaps et al., 2021). Although each of these reports describes the therapy as feasible and safe, data regarding pharmacokinetics of anti-infective agents were not presented. Our study is the first to systematically investigate the effect of ADVOS on the elimination of antimicrobials. The results highlight that all tested drugs were efficiently removed by the ADVOS system. Moreover, blood and concentrate flows played a role in the removal of small water-soluble drugs as CLADVOS for these drugs doubled with doubling of flow rates. Small molecules with low protein binding (<35%) showed pronounced removal, with CLADVOS ranging from 2.74 L/h (cefotaxime) up to 3.4 L/h (meropenem) at a BFR of 100 mL/min, CFR of 160 mL/min and a fixed DFR of 800 mL/min. The doubling of the CLADVOS for low protein-bound drugs with a twofold increase in the BFR (200 mL/min) and CFR (320 mL/min) during the experiment strengthens this assumption. These data correlate well with CLADVOS (6.3 L/h at BFR 250 mL/min) published in a clinical case report (König et al., 2021).
Our data showed that, assuming a standard dialysate flow of 2 L/h for CRRT, CLADVOS surpassed calculated CLCRRT for all tested anti-infective agents (Table 2). Moreover, CLADVOS was higher than previously reported clinical total body clearances for patients receiving different types of CRRT. For instance, meropenem CLADVOS was up to 6.08 L/h, whereas studies report lower total body clearances under CRRT (4.1 L/h (Varghese et al., 2015); 3.5 L/h (Bilgrami et al., 2010); 1.9 L/h (Jamal et al., 2015)). The same trend was observed for linezolid (CLADVOS 4.65 vs. 2.3 L/h (Meyer et al., 2005)) and piperacillin (CLADVOS 5.61 vs. 2.1 L/h (Sharrock et al., 2023) or 3.9 L/h (Awissi et al., 2015)). Moreover, Muhl et al. reported total fluconazole clearance under CRRT of 2.57 L/h (Muhl, 2005), which was well exceeded when using ADVOS (CLADVOS up to 6.2 L/h). For ganciclovir, a similar pattern was seen with a reported total body clearance under CRRT of 2.71 L/h (Horvatits et al., 2014), in comparison to a CLADVOS of 5.88 L/h. Interestingly, this effect was not as pronounced for cefotaxime, which showed CRRT clearance of 5.8 L/h (Koedijk et al., 2016), whereas CLADVOS was up to 4.77 L/h. Overall, the high removal rates are in line with using two parallel dialyzers (total surface area 3.8 m2) in combination with high CFR (160–320 mL/min) which can explain the high CLADVOS observed for antimicrobials with low protein binding.
For larger molecules with protein binding >90% such as daptomycin or anidulafungin, minor or no changes in CLADVOS were observed with increased flows. Daptomycin showed low clearance (0.56 L/h (Xu et al., 2017)) with negligible changes in pharmacokinetics and clearances in patients undergoing CRRT (CL 1.1 L/h) (Bellmann and Smuszkiewicz, 2017) whereas CLADVOS is more than twice as high (1.36 L/h). Anidulafungin presented with an in vitro CLADVOS of 0.84 L/h (Table 2), which is almost the non-renal excretion capacity of healthy volunteers (Wasmann et al., 2018). In this scenario, the total clearance under ADVOS is twice as high as in healthy volunteers (CLhealthy, Table 1). Therefore, highly protein-bound drugs would require higher maintenance dosages under ADVOS to achieve optimal targets (Table 3). In this experiment, the removal of high protein-bound antimicrobials is likely due to the utilization of an albumin primed dialysate, which is continuously regenerated (ADVOS multi circuit). However, the recirculation of the dialysate might hinder a complete removal of circulating substances.
There are certain limitations that need to be discussed. We report an in vitro experiment designed to investigate the elimination capacity of the ADVOS hemodialysis system, as reported previously (Roehr et al., 2015; Konig et al., 2019; Wenzler et al., 2022). Herein, similar to other studies characterizing drug removal by extracorporeal support we substituted human with porcine blood (Schneider et al., 2021). Yet, its results cannot be translated into direct clinical practice as pathophysiological changes affecting antimicrobial exposure in critical illness were absent in this approach. In critically ill patients, metabolic and biochemical changes, such as hypoalbuminemia, can alter drug ionization and protein binding (Wong et al., 2018). Furthermore, resuscitation strategies and vasoactive medications can induce a hyperdynamic state, increasing blood flow to major organs and affecting hepatic metabolism and renal excretion (Roberts et al., 2011). Due to the frequent use of multiple medications in critically ill patients, drug-drug interactions further influence metabolism and pharmacokinetic exposure [ (Koeck et al., 2021). These factors contribute to both inter- and intra-patient variability in drug pharmacokinetics, making drug response difficult to predict in this population (Roberts and Lipman, 2009). Moreover, our experiment did only simulate for a single dosing interval and conducted over a limited time course (9h). Therefore, reduced ADVOS effectiveness over the course of therapy (24h) cannot be ruled out. Thus, these data can be used to guide future clinical studies to identify appropriate dosing regimens whilst using ADVOS. Extrapolation to other substance classes often used in critical illness settings should be used cautiously but might help to inform clinicians to closely monitor therapies in terms of efficacy. Further studies are warranted to investigate and validate the findings of this in vitro experiment. In the meantime, therapeutic drug monitoring (TDM) of antimicrobials is highly recommended to guide and optimize treatment in critically ill patients undergoing ADVOS treatment.
5 Conclusion
Our study shows for the first time that the ADVOS hemodialysis system can efficiently remove antimicrobials. In comparison to CRRT, low protein-bound drugs follow a similar removal mechanism under ADVOS, which is dependent on BFR and dialysis dose (i.e., concentrate flow). However, the CLADVOS appeared higher than CL calculated and/or reported under CRRT. Moreover, in contrast to CRRT, ADVOS removed protein-bound antimicrobials (e.g. anidulafungin, daptomycin) with clearances comparable to those in healthy volunteers. Until clinical data are available, individualized dosing and TDM are recommended to guide effective and safe concentrations under ADVOS treatments.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
CK: Formal Analysis, Writing–original draft. OF: Conceptualization, Methodology, Writing–review and editing. SH: Data curation, Project administration, Writing–review and editing. LM: Formal Analysis, Writing–review and editing. AB: Writing–review and editing. AP: Writing–original draft. TB: Conceptualization, Writing–review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. ADVITOS GmbH covered the costs of the study.
Conflict of interest
Authors SH, AP, and TB were employed by ADVITOS GmbH.OF reports lecture fees from ADVITOS. CK reports lecture fees from AMEOS, Gilead, Pfizer and Shionogi.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Acharya, M., Berger, R., and Popov, A. F. (2022). The role of the ADVanced Organ Support (ADVOS) system in critically ill patients with multiple organ failure. Artif. Organs 46 (5), 735–746. doi:10.1111/aor.14188
Awissi, D. K., Beauchamp, A., Hébert, E., Lavigne, V., Munoz, D. L., Lebrun, G., et al. (2015). Pharmacokinetics of an extended 4-hour infusion of piperacillin-tazobactam in critically ill patients undergoing continuous renal replacement therapy. Pharmacotherapy 35 (6), 600–607. doi:10.1002/phar.1604
Bajaj, J. S., O'Leary, J. G., Reddy, K. R., Wong, F., Biggins, S. W., Patton, H., et al. (2014). Survival in infection-related acute-on-chronic liver failure is defined by extrahepatic organ failures. Hepatology 60 (1), 250–256. doi:10.1002/hep.27077
Bellmann, R., and Smuszkiewicz, P. (2017). Pharmacokinetics of antifungal drugs: practical implications for optimized treatment of patients. Infection 45 (6), 737–779. doi:10.1007/s15010-017-1042-z
Bilgrami, I., Roberts, J. A., Wallis, S. C., Thomas, J., Davis, J., Fowler, S., et al. (2010). Meropenem dosing in critically ill patients with sepsis receiving high-volume continuous venovenous hemofiltration. Antimicrob. Agents Chemother. 54 (7), 2974–2978. doi:10.1128/AAC.01582-09
Dettli, L. (1974). Individualization of drug dosage in patients with renal disease. Med. Clin. North Am. 58 (5), 977–985. doi:10.1016/s0025-7125(16)32094-6
Falkensteiner, C., Kortgen, A., Leonhardt, J., Bauer, M., and Sponholz, C. (2021). Comparison of albumin dialysis devices molecular adsorbent recirculating system and ADVanced Organ Support system in critically ill patients with liver failure-A retrospective analysis. Ther. Apher. Dial. 25 (2), 225–236. doi:10.1111/1744-9987.13533
Fuhrmann, V., Perez Ruiz de Garibay, A., Faltlhauser, A., Tyczynski, B., Jarczak, D., Lutz, J., et al. (2021). Registry on extracorporeal multiple organ support with the advanced organ support (ADVOS) system: 2-year interim analysis. Med. Baltim. 100 (7), e24653. doi:10.1097/MD.0000000000024653
Fuhrmann, V., Weber, T., Roedl, K., Motaabbed, J., Tariparast, A., Jarczak, D., et al. (2020). Advanced organ support (ADVOS) in the critically ill: first clinical experience in patients with multiple organ failure. Ann. Intensive Care 10 (1), 96. doi:10.1186/s13613-020-00714-3
Gatti, M., Cojutti, P. G., and Pea, F. (2024). Impact of attaining aggressive vs. conservative PK/PD target on the clinical efficacy of beta-lactams for the treatment of Gram-negative infections in the critically ill patients: a systematic review and meta-analysis. Crit. Care 28 (1), 123. doi:10.1186/s13054-024-04911-5
Horvatits, T., Kitzberger, R., Drolz, A., Zauner, C., Jäger, W., Böhmdorfer, M., et al. (2014). Pharmacokinetics of ganciclovir during continuous venovenous hemodiafiltration in critically ill patients. Antimicrob. Agents Chemother. 58 (1), 94–101. doi:10.1128/AAC.00892-13
Huber, W., Henschel, B., Schmid, R., and Al-Chalabi, A. (2017). First clinical experience in 14 patients treated with ADVOS: a study on feasibility, safety and efficacy of a new type of albumin dialysis. BMC Gastroenterol. 17 (1), 32. doi:10.1186/s12876-017-0569-x
Huber, W., and Ruiz de Garibay, A. P. (2020). Options in extracorporeal support of multiple organ failure. Med. Klin. Intensivmed. Notfmed 115 (Suppl. 1), 28–36. doi:10.1007/s00063-020-00658-3
Jamal, J. A., Mat-Nor, M. B., Mohamad-Nor, F. S., Udy, A. A., Wallis, S. C., Lipman, J., et al. (2015). Pharmacokinetics of meropenem in critically ill patients receiving continuous venovenous haemofiltration: a randomised controlled trial of continuous infusion versus intermittent bolus administration. Int. J. Antimicrob. Agents 45 (1), 41–45. doi:10.1016/j.ijantimicag.2014.09.009
Kaps, L., Ahlbrand, C. J., Gadban, R., Nagel, M., Labenz, C., Klimpke, P., et al. (2021). Applicability and safety of discontinuous ADVanced Organ Support (ADVOS) in the treatment of patients with acute-on-chronic liver failure (ACLF) outside of intensive care. PLoS One 16 (4), e0249342. doi:10.1371/journal.pone.0249342
Khwaja, A. (2012). KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 120 (4), c179–c184. doi:10.1159/000339789
Koeck, J. A., Hilgarth, H., von Ameln-Mayerhofer, A., Meyn, D., Warlich, R., Münstedt, A., et al. (2021). Clinically relevant interactions with anti-infectives on intensive care units-A multicenter delphi study. Antibiot. (Basel) 10 (11), 1330. doi:10.3390/antibiotics10111330
Koedijk, J. B., Valk-Swinkels, C. G. H., Rijpstra, T. A., Touw, D. J., Mulder, P. G. H., van der Voort, P. H. J., et al. (2016). Pilot study of the pharmacokinetics of cefotaxime in critically ill patients with acute kidney injury treated with continuous renal replacement therapy. Antimicrob. Agents Chemother. 60 (6), 3587–3590. doi:10.1128/AAC.02888-15
Kollef, M. H., Shorr, A. F., Bassetti, M., Timsit, J. F., Micek, S. T., Michelson, A. P., et al. (2021). Timing of antibiotic therapy in the ICU. Crit. Care 25 (1), 360. doi:10.1186/s13054-021-03787-z
König, C., Kluge, S., Fuhrmann, V., and Jarczak, D. (2021). Pharmacokinetics of meropenem during advanced organ support (ADVOS®) and continuous renal replacement therapy. Int. J. Artif. Organs 44 (10), 783–786. doi:10.1177/03913988211021101
Konig, C., Röhr, A. C., Frey, O. R., Brinkmann, A., Roberts, J. A., Wichmann, D., et al. (2019). In vitro removal of anti-infective agents by a novel cytokine adsorbent system. Int. J. Artif. Organs 42 (2), 57–64. doi:10.1177/0391398818812601
Meyer, B., Kornek, G. V., Nikfardjam, M., Karth, G. D., Heinz, G., Locker, G. J., et al. (2005). Multiple-dose pharmacokinetics of linezolid during continuous venovenous haemofiltration. J. Antimicrob. Chemother. 56 (1), 172–179. doi:10.1093/jac/dki133
Muhl, E. (2005). Antimykotika unter kontinuierlicher Nierenersatztherapie. Mycoses 48 (s1), 56–60. doi:10.1111/j.1439-0507.2005.01113.x
Pai Mangalore, R., Ashok, A., Lee, S. J., Romero, L., Peel, T. N., Udy, A. A., et al. (2022). Beta-lactam antibiotic therapeutic drug monitoring in critically ill patients: a systematic review and meta-analysis. Clin. Infect. Dis. 75 (10), 1848–1860. doi:10.1093/cid/ciac506
Roberts, J. A., Joynt, G. M., Lee, A., Choi, G., Bellomo, R., Kanji, S., et al. (2020). The effect of renal replacement therapy and antibiotic dose on antibiotic concentrations in critically ill patients: data from the multinational sampling antibiotics in renal replacement therapy study. Clin. Infect. Dis. 72, 1369–1378. doi:10.1093/cid/ciaa224
Roberts, J. A., and Lipman, J. (2009). Pharmacokinetic issues for antibiotics in the critically ill patient. Crit. Care Med. 37 (3), 840–859. doi:10.1097/CCM.0b013e3181961bff
Roberts, J. A., Paul, S. K., Akova, M., Bassetti, M., De Waele, J. J., Dimopoulos, G., et al. (2014). DALI: defining antibiotic levels in intensive care unit patients: are current beta-lactam antibiotic doses sufficient for critically ill patients? Clin. Infect. Dis. 58 (8), 1072–1083. doi:10.1093/cid/ciu027
Roberts, J. A., Roberts, M. S., Semark, A., Udy, A. A., Kirkpatrick, C. M., Paterson, D. L., et al. (2011). Antibiotic dosing in the “at risk” critically ill patient: linking pathophysiology with pharmacokinetics/pharmacodynamics in sepsis and trauma patients. BMC Anesthesiol. 11, 3. doi:10.1186/1471-2253-11-3
Roehr, A. C., Frey, O. R., Koeberer, A., Fuchs, T., Roberts, J. A., and Brinkmann, A. (2015). Anti-infective drugs during continuous hemodialysis–using the bench to learn what to do at the bedside. Int. J. Artif. organs 38 (1), 17–22. doi:10.5301/ijao.5000377
Schneider, A. G., André, P., Scheier, J., Schmidt, M., Ziervogel, H., Buclin, T., et al. (2021). Pharmacokinetics of anti-infective agents during CytoSorb hemoadsorption. Sci. Rep. 11 (1), 10493. doi:10.1038/s41598-021-89965-z
Sharrock, L., Ankravs, M. J., Deane, A. M., Rechnitzer, T., Wallis, S. C., Roberts, J. A., et al. (2023). Clearance of piperacillin-tazobactam and vancomycin during continuous renal replacement with regional citrate anticoagulation. Ther. Drug Monit. 45 (2), 265–268. doi:10.1097/FTD.0000000000001028
Sommerfeld, O., Neumann, C., Becker, J., von Loeffelholz, C., Roth, J., Kortgen, A., et al. (2023). Extracorporeal albumin dialysis in critically ill patients with liver failure: comparison of four different devices-A retrospective analysis. Int. J. Artif. Organs 46 (8-9), 481–491. doi:10.1177/03913988231191952
Varghese, J. M., Jarrett, P., Wallis, S. C., Boots, R. J., Kirkpatrick, C. M. J., Lipman, J., et al. (2015). Are interstitial fluid concentrations of meropenem equivalent to plasma concentrations in critically ill patients receiving continuous renal replacement therapy? J. Antimicrob. Chemother. 70 (2), 528–533. doi:10.1093/jac/dku413
Wasmann, R. E., Ter Heine, R., van Dongen, E. P., Burger, D. M., Lempers, V. J., Knibbe, C. A., et al. (2018). Pharmacokinetics of anidulafungin in obese and normal-weight adults. Antimicrob. Agents Chemother. 62 (7), 00063-18. doi:10.1128/AAC.00063-18
Wenzler, E., Butler, D., Tan, X., Katsube, T., and Wajima, T. (2022). Pharmacokinetics, pharmacodynamics, and dose optimization of cefiderocol during continuous renal replacement therapy. Clin. Pharmacokinet. 61 (4), 539–552. doi:10.1007/s40262-021-01086-y
Wong, G., Briscoe, S., McWhinney, B., Ally, M., Ungerer, J., Lipman, J., et al. (2018). Therapeutic drug monitoring of β-lactam antibiotics in the critically ill: direct measurement of unbound drug concentrations to achieve appropriate drug exposures. J. Antimicrob. Chemother. 73 (11), 3087–3094. doi:10.1093/jac/dky314
Xu, X., Khadzhynov, D., Peters, H., Chaves, R. L., Hamed, K., Levi, M., et al. (2017). Population pharmacokinetics of daptomycin in adult patients undergoing continuous renal replacement therapy. Br. J. Clin. Pharmacol. 83 (3), 498–509. doi:10.1111/bcp.13131
Keywords: extracorporeal organ support, pharmacokinetics, antibiotic, renal replacement therapy, drug monitoring
Citation: König C, Frey O, Himmelein S, Mulack L, Brinkmann A, Perez Ruiz de Garibay A and Bingold T (2024) In vitro elimination of antimicrobials during ADVanced Organ Support hemodialysis. Front. Pharmacol. 15:1447511. doi: 10.3389/fphar.2024.1447511
Received: 11 June 2024; Accepted: 22 November 2024;
Published: 16 December 2024.
Edited by:
Alastair George Stewart, The University of Melbourne, AustraliaReviewed by:
Aspasia Pefanis, University of Melbourne, AustraliaJana Zielinski, The University of Melbourne, Australia
Copyright © 2024 König, Frey, Himmelein, Mulack, Brinkmann, Perez Ruiz de Garibay and Bingold. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Otto Frey, b3R0by5mcmV5QGtsaW5pa2VuLWhlaWRlbmhlaW0uZGU=