 Lingbo Hu
Lingbo Hu Chao Yang3
Chao Yang3 Yingli Qiao
Yingli Qiao Aidong Wang
Aidong Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol., 29 July 2024
Sec. Gastrointestinal and Hepatic Pharmacology
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1443551
This article is part of the Research TopicHepatocellular Carcinoma: From Diagnostic Approaches to Surgical and Systemic TherapiesView all 17 articles
Background: Tenofovir (TDF) and entecavir (ETV) are highly effective and well-tolerated nucleos(t)ide analogs commonly prescribed for hepatitis B virus (HBV) treatment. Yet, it is unclear whether survival outcomes differ for HBV-related hepatocellular carcinoma (HCC) patients treated with ETV and TDF. Thus, this meta-analysis aimed to compare the prognostic effectiveness of ETV and TDF in HBV-related HCC patients.
Methods: We comprehensively searched four databases, PubMed, Web of Science, Embase, and the Cochrane Library, to identify pertinent studies utilizing keywords “entecavir,” “tenofovir,” “hepatocellular carcinoma,” and “liver resection.” Our primary outcomes of interest encompassed overall survival (OS), recurrence-free survival (RFS), early recurrence, and late recurrence. The statistical effect size for these measures was expressed in terms of hazard ratios (HRs).
Results: Our search yielded 10 studies encompassing 11 datasets involving 7,400 patients. Our meta-analysis revealed that patients treated with TDF achieved better OS (HR = 0.53; 95% confidence interval [CI] = 0.40–0.70, p < 0.0001), RFS (HR = 0.68; 95% CI = 0.57–0.80; p < 0.0001), early recurrence (HR = 0.80; 95% CI = 0.67–0.94; p < 0.0077), and late recurrence (HR = 0.64; 95% CI = 0.43–0.97; p = 0.0368). We detected publication bias potentially affecting OS but not RFS.
Conclusion: Our findings demonstrated that TDF outperformed ETV regarding RFS for HBV-related HCC patients. However, to bolster the evidence and establish more conclusive conclusions, further validation via extensive and high-quality randomized controlled trials is essential.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/#recordDetails, identifier CRD 42024542579.
Liver cancer is the sixth most common cancer globally and third leading cause of mortality (Sung et al., 2021), with hepatocellular carcinoma (HCC) constituting roughly 90% of the cases (Llovet et al., 2021). The considerable recurrence rate following liver resection contributes to an unfavorable prognosis in HCC patients (Llovet et al., 2021). Persistent hepatitis B virus (HBV) replication significantly elevates the risk of HCC recurrence. Nucleos(t)ide analog therapy, reducing the virus load, has the potential to substantially prolong overall survival (OS) and minimize tumor recurrence in HCC patients (Huang et al., 2015; Wang et al., 2020).
Tenofovir (TDF) and entecavir (ETV) are highly effective and well-tolerated nucleos(t)ide analogs used for HBV treatment. However, observations suggest that TDF may confer a significantly lower risk of HCC than ETV in patients with chronic hepatitis B (Choi et al., 2023). This finding prompts questions regarding whether the roles of TDF and ETV in the prognosis of HBV-associated HCC after liver resection differ. While some studies suggest a more favorable efficacy of TDF than ETV in the prognosis of HBV-related HCC patients (Choi et al., 2021; Qi et al., 2021), others have indicated similar efficacy of both drugs on the prognosis (Kao et al., 2023; Liang et al., 2024). Thus, we executed a meta-analysis to compare their prognostic efficacy following liver resection in HBV-related HCC patients.
This review has been registered in the PROSPERO database (registration No. CRD 42024542579).
On 19 March 2024, we systematically searched the Web of Science, PubMed, Embase, and Cochrane Library utilizing a combination of MeSH terms and keywords, focusing on HCC, liver resection, entecavir, and tenofovir. Supplementary Table S1 lists the comprehensive details of the search strategy.
We used the PICOS criteria for inclusion, where P indicates that patients with HBV-related HCC received liver resection; I indicates that TDF was adopted after liver resection; C indicates that ETV was adopted after liver resection; O indicates that outcomes included overall survival (OS), recurrence-free survival (RFS), early recurrence, or late recurrence; and S indicates that retrospective studies and randomized controlled trials (RCTs) were legal.
Non-comparative studies, case reports, abstracts, comments, and reviews were excluded. In the cases of overlapping patient cohorts, only the foremost study, determined by factors such as superior quality, larger sample size, or the most recent publication, was included.
OS and RFS were characterized as the duration from surgery to death and tumor recurrence, respectively. Early recurrence and late recurrence were specified as a recurrence within 2 years and 2 or more years post-liver resection, respectively.
Two researchers independently performed quality assessment and data extraction using the Newcastle–Ottawa scale (NOS) for non-RCTs with scores of up to 9 points (Wells et al., 2014), and the Cochrane risk assessment tool was used for RCTs (Sterne et al., 2019). Study details, such as tumor characteristics, patient information, the first author, and the publication year, were extracted using pre-designed, standardized forms. Outcomes, including OS, RFS, early recurrence, and late recurrence, were extracted from original reports or via data conversion using ReviewManager software (version 5.3). Any disagreements between researchers were resolved by a third party.
Hazard ratio (HR) and 95% confidence interval (CI) values were determined using the inverse variance method. Heterogeneity was evaluated through the Q statistic and I2, with I2 of 25% and 50% denoting low and moderate heterogeneity, respectively. Heterogeneity sources were explored using either meta-regression with the random-effects model for studies with I2 > 50% or subgroup analysis. A leave-one-out sensitivity analysis was applied to assess the robustness of the conclusion. Funnel plots were used to examine publication bias, and its influence on the results was further analyzed using the trim-and-fill method. All analyses were conducted using the R program (version 4.4.0). Statistically significant difference was deemed at p < 0.05.
A thorough search produced 147 articles, which were reduced to 102 after eliminating duplicates. After reviewing titles and abstracts, 22 records were retained. Twelve studies were excluded due to duplicated data, incorrect comparisons, and inappropriate article types (Figure 1). Consequently, this meta-analysis incorporated 10 studies (Zhang et al., 2018; Choi et al., 2021; Qi et al., 2021; Shen et al., 2022; Tsai et al., 2022; Wang et al., 2022; Kao et al., 2023; Li et al., 2023; Linye et al., 2023; Liang et al., 2024).
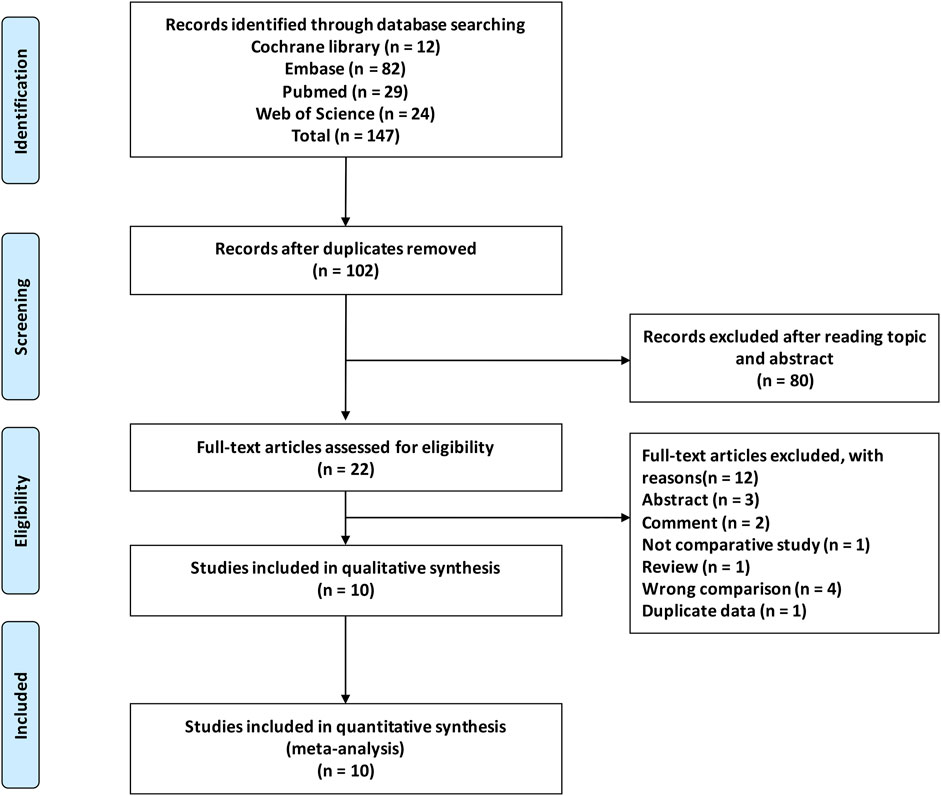
Figure 1. Flowchart depicting the selection process of studies.
Ten studies, comprising 11 datasets and involving 7,400 patients, compared TDF and ETF efficacy in HBV-related HCC prognosis. Among them, nine were from China, and one was from Korea. Two were retrospective studies, one was an RCT, and the rest were retrospective studies using propensity analysis (including propensity-score matching, propensity-score overlap weighting, and inverse probability of treatment weighting). Three studies exclusively included patients at the Barcelona Clinical Liver Cancer Staging (BCLC) 0 or A stage. Table 1 lists the detailed patient and tumor characteristics.
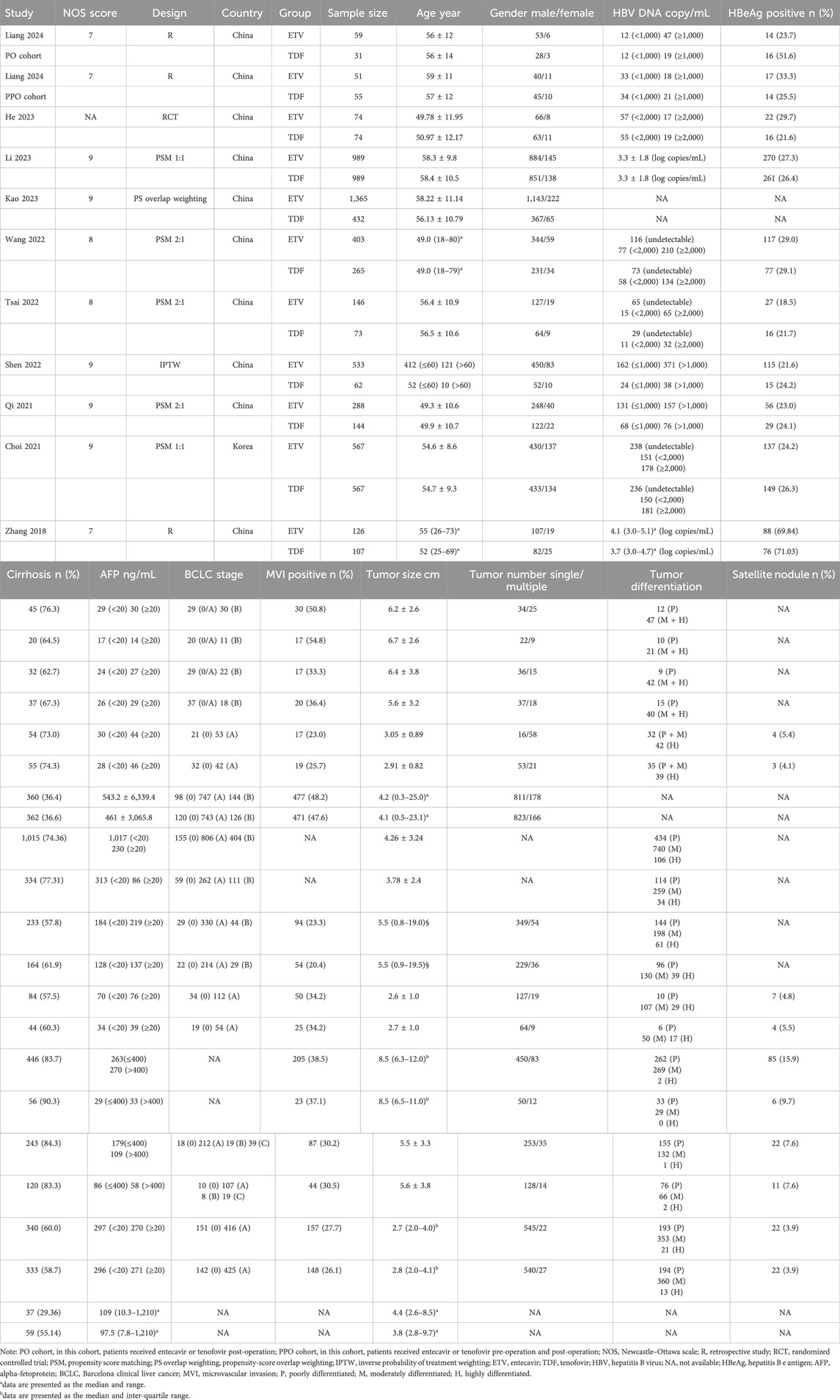
Table 1. Features of the incorporated studies.
Supplementary Tables S2, S3 list the quality assessment details of the included studies. Of the nine non-RCT studies, two scored 7 points, two scored 8 points, and five scored 9 points. Thus, the two studies with 7 points were deemed as moderate-quality, and the remaining seven were classified as high-quality. For the RCT, the blind method implementation was not elucidated in the article, with all other domains showing low risk.
HR values for OS were reported in eight studies comprising nine datasets and analyzed based on the random-effects model. The aggregated data indicated that patients treated with TDF achieved superior OS (HR, 0.53; 95% CI, 0.40–0.70; p < 0.0001) (Figure 2). Ten studies with 11 datasets documented the HR values for RFS, which was analyzed with the random-effects model. The combined data suggested that patients treated with TDF achieved better RFS (HR, 0.68; 95% CI, 0.57–0.80; p < 0.0001) (Figure 2).
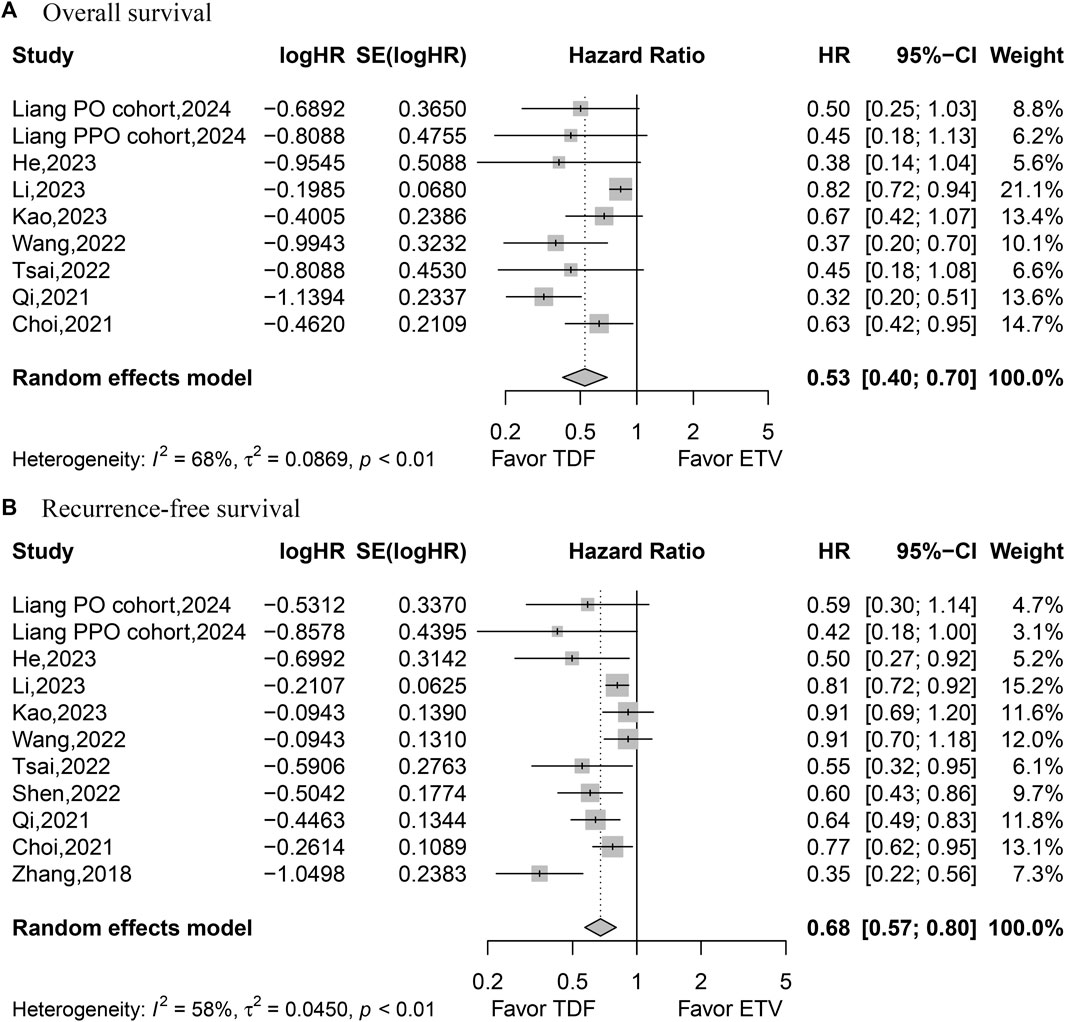
Figure 2. Forest plot for overall survival (A) and recurrence-free survival (B).
The 1-, 3-, and 5-year OS rates were reported in five, five, and four studies, respectively, and analyzed using the random-effects model due to the observed heterogeneity. The pooled results revealed a higher 5-year OS rate with TDF (5-year RR, 1.19; 95% CI, 1.04–1.35; p = 0.0113) but similar 1- and 3-year OS rates (Figure 3). Similarly, 1-, 3-, and 5-year RFS rates were documented in five, five, and four studies, respectively, and analyzed using the random-effects model, with the exception of the 3-year RFS rate, which presented low heterogeneity. The synthesized data revealed higher 3- and 5-year RFS rates with TDF (3-year RR, 1.14; 95% CI, 1.08–1.20; p < 0.0001; 5-year RR, 1.31; 95% CI, 1.13–1.53; p = 0.0005), with similar 1-year RFS rates (Figure 3).
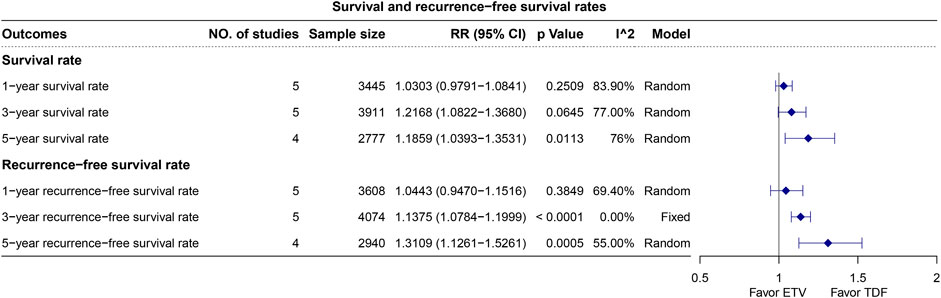
Figure 3. Plot for the overall survival and recurrence-free survival rates.
The studies with four datasets that reported HR values for early recurrence were analyzed using the fixed-effects model. The pooled data indicated that patients treated with TDF achieved better early recurrence outcomes (HR, 0.80; 95% CI, 0.67–0.94; p < 0.0077) (Figure 4). Furthermore, four studies with four datasets reporting HR values for late recurrence were analyzed with the random-effects model. The combined data suggested that patients treated with TDF achieved better late recurrence (HR, 0.64; 95% CI, 0.43–0.97; p = 0.0368) (Figure 4).
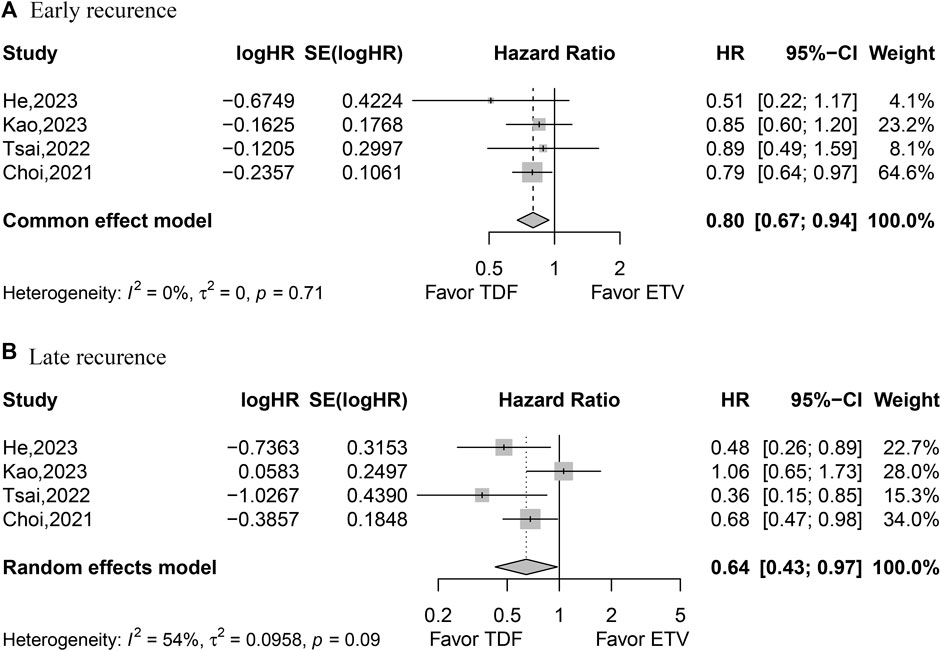
Figure 4. Forest plot for early recurrence (A) and late recurrence (B).
Meta-regression was performed only for RFS due to the smaller number of OS datasets (<10). The results revealed the sample size and retrospective study design as the heterogeneity sources (Supplementary Figure S1). Subgroup analyses were conducted for retrospective studies, propensity analysis studies combined with RCT, studies that only included BCLC early-stage HCC, studies conducted in China, and available patient characteristics. Figure 5 shows that patients receiving TDF achieved better OS and RFS in subgroup analyses. In the sensitivity analysis of OS, the overall heterogeneity decreased after the removal of the study conducted by Li, indicating that this study is one of the sources of heterogeneity but does not affect the results of the meta-analysis. This study was a propensity score matching (PSM) study with high quality and the largest sample size (Supplementary Figure S2). The sensitivity analysis for RFS indicated that the result was stable (Supplementary Figure S2B). Additionally, the sensitivity analyses indicated that the early recurrence and late recurrence results were less stable (Supplementary Figures S2C, D). The studies by Kao et al. and Choi et al. would affect the results of early recurrence and late recurrence.
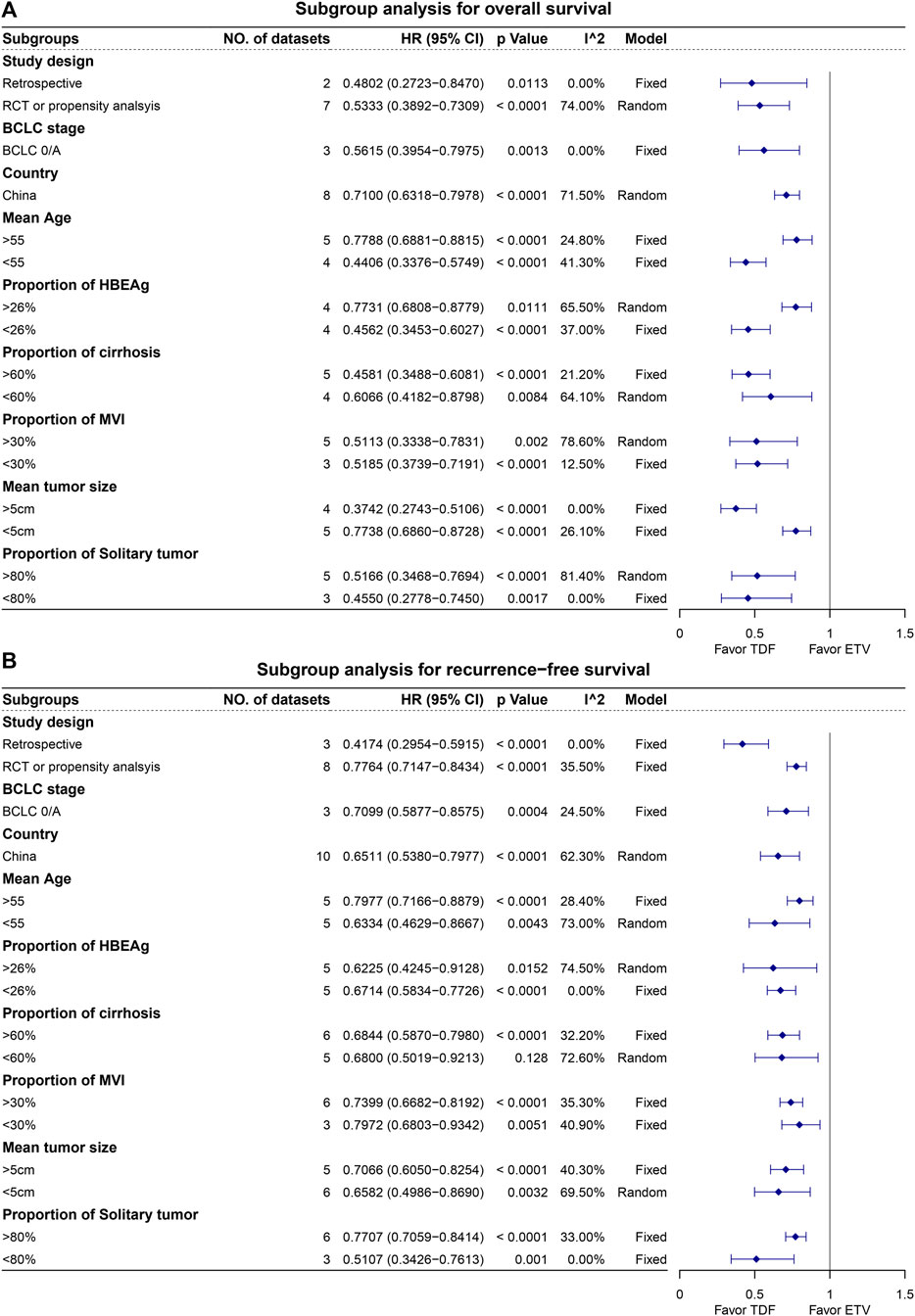
Figure 5. Subgroup analysis for overall survival (A) and recurrence-free survival (B).
Funnel plots with the Egger test revealed publication bias in OS and RFS but not in early recurrence and late recurrence (Supplementary Figure S3). Contour-enhanced funnel plots for OS and RFS indicated filled studies in the white area (p < 0.05), suggesting that publication bias affected the meta-analysis results (Supplementary Figures S4A, B). After filling potential unpublished studies, the meta-analysis showed superior RFS for patients receiving TDF compared to ETV, while OS remained similar between TDF and ETV recipients (Supplementary Figure S5).
In our meta-analysis, HBV-related HCC patients on TDF exhibited better OS, RFS, early recurrence, and late recurrence. Previous meta-analyses that mainly compared TDF and ETV for HBV-related HCC prognosis (Giri et al., 2023; Liu et al., 2023; Kong et al., 2024) included patients receiving various treatments, such as liver transplantation, radiofrequency ablation, and liver resection, inevitably introducing bias. We focused solely on HCC patients undergoing liver resection to minimize bias from different treatments. Additionally, we comprehensively analyzed the result reliability. The meta-regression analysis revealed the heterogeneity sources, urging for larger, higher-quality studies. The subgroup analyses by study design and tumor stage supported our findings. Moreover, publication bias was identified. Addressing publication bias by filling the potentially unpublished studies revealed the consistently better efficacy of TDF on RFS over ETV, questioning its superiority on OS. This increases our confidence in the hypothesis that TDF can lead to better outcomes for HCC patients than ETV. Additionally, we advocate for publishing articles with negative or conflicting conclusions. Based on the meta-analysis, we believe that TDF is superior to ETV in improving RFS. The current research suggested that the improvement in RFS with TDF is due to its superior HBV-DNA suppression and anti-inflammatory effects compared to ETV (12). Therefore, TDF is more suitable as an antiviral medication for postoperative patients with higher viral loads.
Our study is subject to some constrains. First, the majority of the incorporated studies were non-RCTs. Although they demonstrated high quality, the inherent bias cannot be fully addressed by propensity analysis. Second, all studies were performed in Asia, potentially restricting the generalizability of our findings to other populations. Third, heterogeneity was present. Although we conducted a meta-regression analysis to explore its source, the subgroup analysis supported the reliability of our results. Fourth, publication bias was identified. However, using the trim-and-fill method, we observed the consistent efficacy of TDF over ETV in terms of RFS. Lastly, some studies had relatively small sample sizes, potentially impacting the robustness of our findings.
Our meta-analysis demonstrated the superiority of TDF over ETV in RFS for HBV-related HCC patients. These findings carry significant implications for postoperative antiviral therapy selection. However, further extensive, high-quality RCTs are necessary to bolster evidence and draw more conclusive recommendations.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
LH: conceptualization, data curation, formal analysis, methodology, software, visualization, writing–original draft, and writing–review and editing. CY: data curation and writing–review and editing. YQ: funding acquisition, validation, and writing–review and editing. AW: funding acquisition, validation, and writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was sponsored by the Zhejiang Provincial Basic Public Welfare Research Project (No. LTGY23H030008), the Taizhou Science and Technology Planning Project (Nos 20ywb25 and 22ywa34), the Medical and Health Technology Plan of Zhejiang Province (Nos 2021RC140 and 2024KY1825), and the Taizhou High-level Talents Special Support Program (the third level).
The authors thank TopEdit (www.topeditsci.com) for the English language editing of this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2024.1443551/full#supplementary-material
Choi, J., Jo, C., and Lim, Y. S. (2021). Tenofovir versus entecavir on recurrence of hepatitis B virus–related hepatocellular carcinoma after surgical resection. Hepatology 73 (2), 661–673. doi:10.1002/hep.31289
Choi, W. M., Yip, T. C., Wong, G. L., Kim, W. R., Yee, L. J., Brooks-Rooney, C., et al. (2023). Hepatocellular carcinoma risk in patients with chronic hepatitis B receiving tenofovir-vs. entecavir-based regimens: individual patient data meta-analysis. J. Hepatol. 78 (3), 534–542. doi:10.1016/j.jhep.2022.12.007
Giri, S., Agrawal, D., Afzalpurkar, S., Gopan, A., Angadi, S., and Sundaram, S. (2023). Tenofovir versus entecavir for tertiary prevention of hepatocellular carcinoma in chronic hepatitis B infection after curative therapy: a systematic review and meta-analysis. J. Viral Hepat. 30 (2), 108–115. doi:10.1111/jvh.13766
G. A. Wells, G. Wells, B. Shea, B. Shea, D. O'Connell, J. Petersonet al. (2014). The newcastle-ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. (Ottawa: The Ottawa Hospital).
Huang, G., Lau, W. Y., Wang, Z. G., Pan, Z. Y., Yuan, S. X., Shen, F., et al. (2015). Antiviral therapy improves postoperative survival in patients with hepatocellular carcinoma: a randomized controlled trial. Ann. Surg. 261 (1), 56–66. doi:10.1097/SLA.0000000000000858
Kao, W. Y., Tan, E. C. H., Lee, H. L., Huang, Y. H., Huo, T. I., Chang, C. C., et al. (2023). Entecavir versus tenofovir on prognosis of hepatitis B virus-related hepatocellular carcinoma after curative hepatectomy. Alimentary Pharmacol. Ther. 57 (11), 1299–1312. doi:10.1111/apt.17438
Kong, Q., Yi, M., Teng, F., and Chen, Z. (2024). Enhanced prognosis of HCC patients undergoing radical treatments with tenofovir versus entecavir: a meta-analysis based on propensity score matching studies. Asian J. Surg. 47 (1), 55–62. doi:10.1016/j.asjsur.2023.09.057
Li, P. P., Wang, Y. Y., Yu, J., Yu, J. D., Tao, Q. F., Zhang, J. W., et al. (2023). Tenofovir vs entecavir among patients with HBV-related HCC after resection. Jama Netw. Open 6 (10), e2340353. doi:10.1001/jamanetworkopen.2023.40353
Liang, Y., Zhong, D., Zhang, Z., Su, Y., Yan, S., Lai, C., et al. (2024). Impact of preoperative antiviral therapy on the prognosis of hepatitis B virus-related hepatocellular carcinoma. BMC Cancer 24 (1), 291. doi:10.1186/s12885-024-12031-0
Linye, H., Zijing, X., Xiaoyun, Z., Zhihui, L., Tianfu, W., and Chuan, L. (2023). Tenofovir versus entecavir on the prognosis of hepatitis B-related hepatocellular carcinoma after surgical resection: a randomised controlled trial. Int. J. Surg. Lond. Engl. 109 (10), 3032–3041. doi:10.1097/JS9.0000000000000554
Liu, H., Han, C. L., Tian, B. W., Ding, Z. N., Yang, Y. F., Ma, Y. L., et al. (2023). Tenofovir versus entecavir on the prognosis of hepatitis B virus-related hepatocellular carcinoma: a systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 17 (6), 623–633. doi:10.1080/17474124.2023.2212161
Llovet, J. M., Kelley, R. K., Villanueva, A., Singal, A. G., Pikarsky, E., Roayaie, S., et al. (2021). Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 7 (1), 6. doi:10.1038/s41572-020-00240-3
Qi, W., Shen, J., Dai, J., Wu, Y., Zhang, Y., Leng, S., et al. (2021). Comparison of nucleoside and nucleotide analogs in the recurrence of hepatitis B virus-related hepatocellular carcinoma after surgical resection: a multicenter study. Cancer Med. 10 (23), 8421–8431. doi:10.1002/cam4.4348
Shen, J., Qi, W., Dai, J., Leng, S., Jiang, K., Zhang, Y., et al. (2022). Tenofovir vs. entecavir on recurrence of hepatitis B virus-related hepatocellular carcinoma beyond Milan criteria after hepatectomy. Chin. Med. J. 135 (3), 301–308. doi:10.1097/CM9.0000000000001864
Sterne, J. A. C., Savović, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., et al. (2019). RoB 2: a revised tool for assessing risk of bias in randomised trials. Bmj 366, l4898. doi:10.1136/bmj.l4898
Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., et al. (2021). Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71 (3), 209–249. doi:10.3322/caac.21660
Tsai, M. C., Wang, C. C., Lee, W. C., Lin, C. C., Chang, K. C., Chen, C. H., et al. (2022). Tenofovir is superior to entecavir on tertiary prevention for BCLC stage 0/A hepatocellular carcinoma after curative resection. Liver Cancer 11 (1), 22–37. doi:10.1159/000518940
Wang, X. H., Hu, Z. L., Fu, Y. Z., Hou, J. Y., Li, W. X., Zhang, Y. J., et al. (2022). Tenofovir vs. entecavir on prognosis of hepatitis B virus-related hepatocellular carcinoma after curative resection. J. Gastroenterology 57 (3), 185–198. doi:10.1007/s00535-022-01855-x
Wang, Z. Y., Tao, Q. F., Wang, Z. H., Lin, K. Y., Huang, G., Yang, Y., et al. (2020). Antiviral therapy improves post-operative survival outcomes in patients with HBV-related hepatocellular carcinoma of less than 3 cm - a retrospective cohort study. Am. J. Surg. 219 (4), 717–725. doi:10.1016/j.amjsurg.2019.05.016
Keywords: hepatocellular carcinoma, entecavir, tenofovir, liver resection, meta-analysis, prognosis
Citation: Hu L, Yang C, Qiao Y and Wang A (2024) A systematic review and meta-analysis comparing the impact of tenofovir and entecavir on the prognosis of hepatitis B virus-related hepatocellular carcinoma patients undergoing liver resection. Front. Pharmacol. 15:1443551. doi: 10.3389/fphar.2024.1443551
Received: 04 June 2024; Accepted: 08 July 2024;
Published: 29 July 2024.
Edited by:
Pradeep Kumar Shukla, University of Tennessee Health Science Center (UTHSC), United StatesReviewed by:
Ka Zhang, Sun Yat-sen University, ChinaCopyright © 2024 Hu, Yang, Qiao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aidong Wang, d2FuZ2FpZG9uZ0BlbnplbWVkLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.