
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 26 April 2024
Sec. Renal Pharmacology
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1379338
 Hui-Fen Chen1Yu-Jie Lin1Yan Han1Xian-Long Zhang1,2
Hui-Fen Chen1Yu-Jie Lin1Yan Han1Xian-Long Zhang1,2 Ruo-Bing Wang1
Ruo-Bing Wang1 Jun-Hui Chen1
Jun-Hui Chen1 Ying Pi3Li-Zhe Fu1,4Fang Tang1,4
Ying Pi3Li-Zhe Fu1,4Fang Tang1,4 Xi-Na Jie1,2Xiao-Na Tang3*
Xi-Na Jie1,2Xiao-Na Tang3* Xu-Sheng Liu1,2*
Xu-Sheng Liu1,2* Yi-Fan Wu1,2*
Yi-Fan Wu1,2*Background: Chinese patent medicine is commonly used in China as an important treatment mechanism to thwart the progression of chronic kidney disease (CKD) stages 3–5, among which Niaoduqing granules are a representative Chinese patent medicine; however, its long-term efficacy on CKD prognosis remains unclear.
Methods: Patients were grouped according to Niaoduqing granule prescription duration (non-Niaoduqing granule (non-NDQ) group vs Niaoduqing granule (NDQ) group). Serum creatinine (SCr) variation was compared using a generalized linear mixed model (GLMM). Multivariate Cox regression models were constructed, adjusting for confounding factors, to explore the risk of composite outcomes (receiving renal replacement therapy (RRT) or having an estimated glomerular filtration rate (eGFR)<5 mL/min/1.73 m2, ≥50% decline in the eGFR from the baseline, and doubling of SCr) in individuals consuming Niaoduqing granules.
Results: A total of 1,271 patients were included, with a median follow-up duration of 29.71 (12.10, 56.07) months. The mean SCr Z-scores for the non-NDQ group and NDQ group were −0.175 and 0.153, respectively, at baseline (p = 0.015). The coefficients of the NDQ group from visit 1 to visit 5 were −0.207 (95% CI: −0.346, −0.068, p = 0.004), −0.214 (95% CI: 0.389, −0.039, p = 0.017), −0.324 (95% CI: 0.538, −0.109, p = 0.003), −0.502 (95% CI: 0.761, −0.243, p = 0.000), and −0.252 (95% CI: 0.569, 0.065, p = 0.119), respectively. The survival probability was significantly higher in the NDQ group (p = 0.0039). Taking Niaoduqing granules was a significant protective factor for thwarting disease progression (model 1: HR 0.654 (95% CI 0.489–0.875, p = 0.004); model 2: HR 0.646 (95% CI 0.476, 0.877, p = 0.005); and model 3: HR 0.602 (95% CI 0.442, 0.820, p = 0.001)).
Conclusion: The long-term use of Niaoduqing granules improved SCr variation and lowered the risk of CKD progression by 39.8%.
Chronic kidney disease (CKD) is defined as having a glomerular filtration rate (GFR) less than 60 mL/min/1.73 m2 with abnormalities in kidney structure biomarkers and/or function persisting for at least 3 months (National Kidney Foundation, 2002). It is a global health problem affecting 7.0%–34.3% of adults (Liyanage et al., 2022). Patients with stages 3–5 CKD experience more acute kidney impairment and worse outcomes. Renal replacement therapy (RRT) is required once a patient has progressed to end-stage kidney disease (ESRD), exerting a heavy burden on individuals, their families, and even society at large.
Therapies for CKD stages 3–5 consist of lifestyle adjustment, etiology treatment, and complication prevention. Medications such as angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACEIs/ARBs) and sodium-glucose cotransporter-2 inhibitors (SGLT2i) (KDIGO, 2021b) are routinely used to thwart disease progression. Traditional Chinese medicine (TCM) holds that CKD often arises from chronic nephropathy, diabetic nephropathy, and other syndromes. The primary etiologies underlying CKD are multifaceted and can be attributed to congenital deficiencies, unhealthy dietary habits, excessive exertion, external pathogenic influences, and emotional imbalances. Prolonged illness will be attributed to the deficiency of spleen–kidney qi, deficiency of both qi and yin, and accumulation of pathological factors such as dampness and blood stagnation, leading to a more complex and challenging illness to treat. In China, various Chinese patent medicines have become important treatments to thwart the progression of CKD stages 3–5 (Standardization project group, 2021; Wang et al., 2023). Niaoduqing granules are a representative Chinese patent medicine and have been used for years. They contain the following ingredients: Radix Astragali (黄芪 huánɡ qí), Codonopsis pilosula (党参 dǎnɡ shēn), Radix Polygoni Multiflori Preparata (制何首乌 zhì hé shǒu wū), Radix et Rhizoma Rhei (生大黄 shēnɡ dà huánɡ), Rhizoma Atractylodis macrocephalae (白术 bái zhú), Wolfiporia extensa (茯苓 fú línɡ), Plantago asiatica (车前草 chē qián cǎo), Rhizoma Pinelliae Praeparatum (姜半夏 jiānɡ bàn xià), mulberry root bark (桑白皮 sānɡ bái pí), Sophora flavescens (苦参 kǔ shēn), Radix Paeoniae Alba (白芍 bái sháo), Salvia miltiorrhiza (丹参 dān shēn), and Ligusticum striatum (川芎 chuān xiōnɡ) (Yan et al., 2020). Several clinical studies have demonstrated that Niaoduqing granules can reduce serum creatinine (SCr) in CKD patients and maintain a stable estimated glomerular filtration rate (eGFR) without serious adverse drug reactions (Zheng et al., 2017; Zheng et al., 2019).
However, most of these studies have only involved short-term observations (for approximately 1 year) and have focused on surrogate indicators, such as urine protein, hemoglobin (Hb), calcium (Ca2+), and phosphorous (P). Few of the studies on Niaoduqing granules have observed their efficacy on long-term prognoses, such as all-cause mortality and RRT occurrence. In addition, although CKD patients usually use Niaoduqing granules for a long time, given the long course of the disease, there remains a lack of evidence on Niaoduqing granules’ long-term efficacy. Hence, we collected clinical information via a retrospective cohort study to explore this.
We searched the hospital information system (HIS) at Guangdong Provincial Hospital of Chinese Medicine (GPHCM) with the following keywords (in Chinese): “kidney disease” or “renal failure” or “renal disease” or “nephritis” or “proteinuria” or “hematuria.” Patients with kidney disease who visited from March 2012 to March 2023 were enrolled in a single-center, retrospective cohort study (ethics approval no. ZE 2023–330). Patients aged 18–80 years with CKD stages 3–5 (National Kidney Foundation, 2002) and who visited the nephrology department regularly (at least once every 6 months during the follow-up period) were eligible. Patients who had been diagnosed with acute and critical illnesses (e.g., acute cerebral infarction, acute heart failure, shock, malignant tumors, and hematological diseases) within 3 months of the baseline, had incomplete follow-up data, had received RRT (transplantation or dialysis) within 3 months from the baseline, had an eGFR less than 5 mL/min/1.73 m2, or had a follow-up period of less than 3 months were excluded.
Patients were grouped according to Niaoduqing granule prescription duration, defined as the time span from the first prescription date to the last prescription date during the follow-up duration. The prescription duration proportion was defined as prescription duration/follow-up duration. Participants with proportions over 80% were classified into the Niaoduqing granule (NDQ) group, and those with proportions of 0% were classified into the non-Niaoduqing granule (non-NDQ) group. Patients with proportions between 0% and 80% were excluded.
The composite outcome was defined as all-cause mortality, ESRD (received RRT or eGFR<5 mL/min/1.73 m2), and a ≥50% decline in the eGFR from baseline, along with at least a doubling of SCr. Patients were followed until the end of the follow-up time period (March 2023) or until they were lost to follow-up (defined as being unobservable during the time-at-risk period).
All covariates (except for sex) were time-updated and were collected at the baseline and once every 12 months over a 5-year follow-up duration. Demographic characteristics included age (continuous) and sex (fixed variables, male vs female). The clinical diagnosis included etiology, CKD stage, and comorbidities. The etiology included primary glomerulopathy, hypertensive nephropathy, diabetic nephropathy, other secondary kidney diseases (including infectious or autoimmune kidney diseases, obstructive nephropathy, uric acid nephropathy, and pyelonephritis), and unknown. Comorbidities included hypertension, diabetes, hyperuricemia, hyperlipidemia, anemia, cardiovascular diseases (CVDs), and cerebrovascular diseases.
Medication in use included ACEI/ARB, other antihypertensive drugs, hypoglycemic agents, urate-lowering drugs, lipid-lowering drugs, iron supplements, calcium supplements, sodium bicarbonate, ketoacid tablets, diuretics, and Chinese patent medicines. Chinese patent medicines were classified according to their clinical function in patients with CKD, such as removing turbidity, improving qi and yin deficiency (tonifying), and other functions.
Laboratory covariates included SCr, Hb, serum albumin (ALB), blood urea nitrogen (urea), total carbon dioxide (TCO2), uric acid (UA), P, Ca2+, potassium (K+), sodium (Na+), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), fasting blood glucose (Glu), and the protein/creatinine ratio (PCR). The eGFR was calculated using the CKD Epidemiology Collaboration (CKD-EPI) creatinine equation (KDIGO, 2021a).
Continuous variables were summarized using the mean ± standard deviation (SD) for normal distributions and median (interquartile ranges) for non-normal distributions. Categorical variables were summarized using frequencies and percentages. The Mann–Whitney U-test and chi-square test were applied to compare between-group characteristics.
For time-updated covariates, line graphs were plotted to visualize annual variations and estimated marginal SCr means. After standardizing all the time-updated continuous variables and transforming the follow-up duration to five consecutive visits, a generalized linear mixed model (GLMM) was constructed with individual random effects and group fixed effects.
For survival analysis, covariates with a missing rate greater than 40% were excluded, and outliers of continuous variables were winsorized with 0.1 cut-offs at each tail. Missing data were imputed using a random forest. A 1:2 nearest neighbor propensity score matching (PSM) with replacement within a caliper of 0 was applied to achieve covariate balance. The survival probability was compared using the Kaplan–Meier curve and a log-rank test. Variables with p < 0.10 in univariate Cox regression were included in multivariate Cox regression with a “backward” stepwise method. The Schoenfeld residual test was performed to check the proportional hazards assumption. The hazard ratio (HR) and 95% confidence interval (95% CI) values were used to describe the results. A subgroup analysis with interaction effects was conducted by stratification of age, sex, PCR, CKD stage, with or without hypertension, diabetes, and etiology. A forest plot was used to show the results.
All statistical tests were two-sided, and p-values <0.05 were considered statistically significant. All statistical analyses were conducted via R Studio 4.3.0 and SPSS 25.0.
Of the 27,121 patients with kidney disease, 2,731 who were not non-dialysis adults with CKD stages 3–5 with complete information for composite outcome and 4,086 who were not regularly visiting a nephrologist or had an expected survival duration of less than 3 months were excluded. Moreover, 784 patients did not meet the 0%–80% prescription duration requirement. Ultimately, 1,271 participants were included in the final analysis, with 232 in the NDQ group and 1,039 in the non-NDQ group (Figure 1).
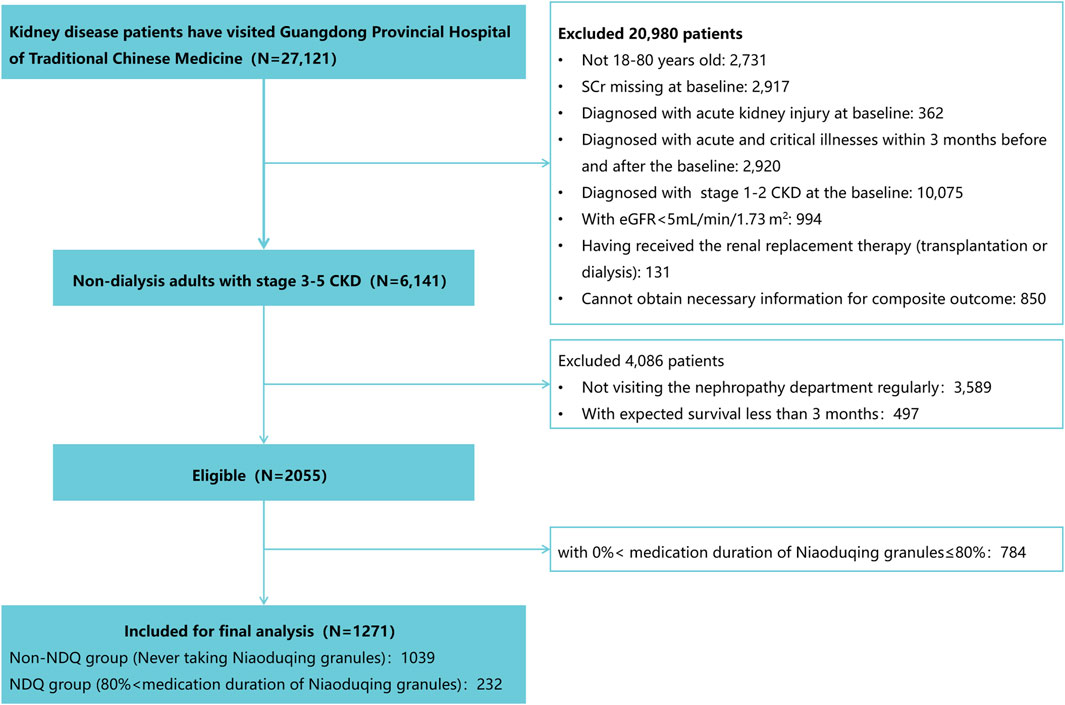
Figure 1. Recruitment flow chart.
The 1,271 participants had a median age of 58.30 (46.31, 66.97) years, and 585 (46.03%) were females. A total of 777 (61.13%) of the individuals had CKD stage 3, 273 (21.48%) had CKD stage 4, and 221 (17.39%) had CKD stage 5. The endpoint occurrence was 356 (28.01%), with a median follow-up duration of 29.71 (12.10, 56.07) months. The NDQ group had an endpoint occurrence of 84 (36.21%), with a median follow-up duration of 44.38 (23.27, 68.93) months. The non-NDQ group had an endpoint occurrence of 272 (26.18%), with a median follow-up duration of 26.85 (11.21, 52.46) months. Some covariates could not reach inter-group balance. These were CKD stage, Hb, urea, TCO2, HDL-C, etiology, CVDs, ACEI/ARB, other antihypertensive drugs, iron supplements, sodium bicarbonate, ketoacid tablets, and Chinese patent medicines (p < 0.05) (important laboratory data are highlighted in Table 1, and details can be found in Supplementary Table S1).
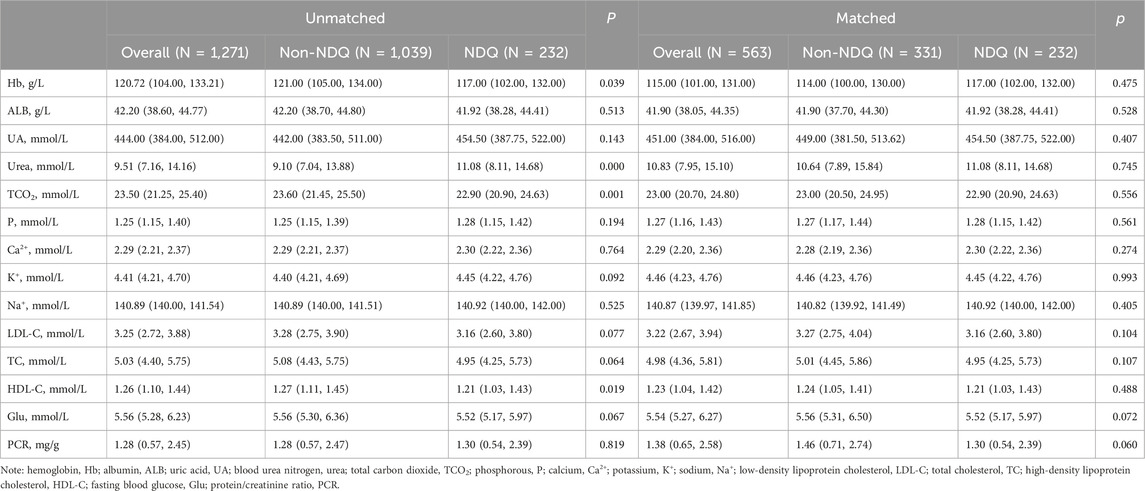
Table 1. Important laboratory characteristics before and after propensity score matching.
Line graphs indicated that SCr steadily increased over time in both NDQ and non-NDQ groups (Figure 2 and Figure 3). The NDQ group showed a higher SCr level than the non-NDQ group at the baseline, and it had a lower estimated marginal SCr mean than the non-NDQ group during the follow-up period. Additionally, the NDQ group had a smaller SCr slope than the non-NDQ group.
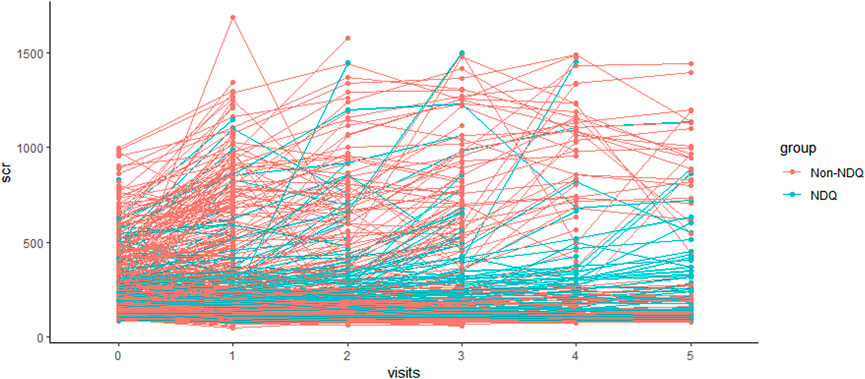
Figure 2. SCr variation of each individual.
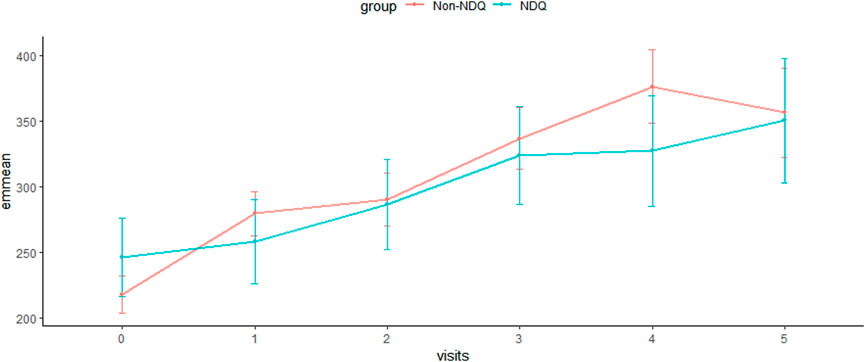
Figure 3. Estimated marginal means of SCr.
A generalized linear mixed model was constructed after adjusting the fixed and time-updated covariates. It had an F-statistic of 41.333, an Akaike information criterion (AIC) of 1,980.974, and a Bayesian information criterion (BIC) of 2,001.298 (p < 0.001). Among the 1,271 participants, the coefficients from visit 1 to visit 5 were 0.134 (95% CI 0.060, 0.208), 0.266 (95% CI 0.165, 0.368), 0.420 (95% CI 0.292, 0.547), 0.507 (95% CI 0.343, 0.671), and 0.347 (95% CI 0.140, 0.554) in overall participants compared to the baseline (p < 0.05), respectively. This indicated that SCr levels trended upward from visit 1 to visit 5, which was consistent (Figure 2 and Figure 3).
The mean SCr Z-scores for the non-NDQ and NDQ groups were −0.175 and 0.153, respectively, at baseline, with p = 0.015. This indicated significantly higher SCr levels in the NDQ group than in the non-NDQ group. Compared to the non-NDQ group, the NDQ group’s coefficients (95% CI) from visit 1 to visit 5 were 0.207 (95% CI: 0.346, −0.068), −0.214 (95% CI: 0.389, −0.039), −0.324 (95% CI: 0.538, −0.109), −0.502 (95% CI: 0.761, −0.243), and −0.252 (95% CI: 0.569, 0.065), with a significant p-value from visit 1 to visit 4. This indicated that the NDQ group’s mean SCr was significantly lower than that of the non-NDQ group from visit 1 to visit 4. This was also the case for visit 5; however, the results were not statistically significant (Table 2).

Table 2. Fixed coefficients from the generalized linear mixed model.
A total of 563 patients were included for survival analysis, with 188 (33.39%) reaching the endpoint and a median survival duration of 77.9 (67.6, 95.2) months. Of the included patients, 232 were from the NDQ group, with a composite outcome of 84 (36.21%) and a median survival duration of 92.4 (71.7, 110.2) months, and 331 were from the non-NDQ group, with a composite outcome of 104 (31.42%) and a median survival duration of 72.7 (54.7, 94.6) months. The Kaplan–Meier curves showed that the NDQ group had a higher survival probability than the non-NDQ group (p = 0.0039) (Figure 4).

Figure 4. Kaplan-Meier curve.
A total of 24 variables were significant in univariate Cox regression with p < 0.10: NDQ group, age, CKD stage, Hb, ALB, urea, TCO2, P, Ca2+, K+, PCR, hypertension, diabetes, hyperuricemia, anemia, other antihypertensive drugs, hypoglycemic drugs, lipid-lowering drugs, calcium supplements, iron supplements, sodium bicarbonate, ketoacid tablets, diuretics, and turbidity-removing Chinese patent medicines (Supplementary Table S2).
As presented in Table 3, three models were constructed: model 1 was a univariate Cox model of exposure; model 2 further adjusted the significant comorbidities based on model 1; and model 3 further adjusted other significant covariates in univariate Cox regression based on model 2. The HR of the NDQ group in models 1 and 2 was 0.654 (95% CI: 0.489, 0.875, p = 0.004) and 0.646 (95% CI: 0.476, 0.877, p = 0.005), respectively. After adjusting for all covariates, the NDQ group still had a significant HR (95% CI) in model 3 (HR: 0.602, 95% CI: 0.441, 0.820, p = 0.001). These results indicated that taking Niaoduqing granules is an independent protective factor for thwarting long-term decline among CKD patients at stages 3–5.
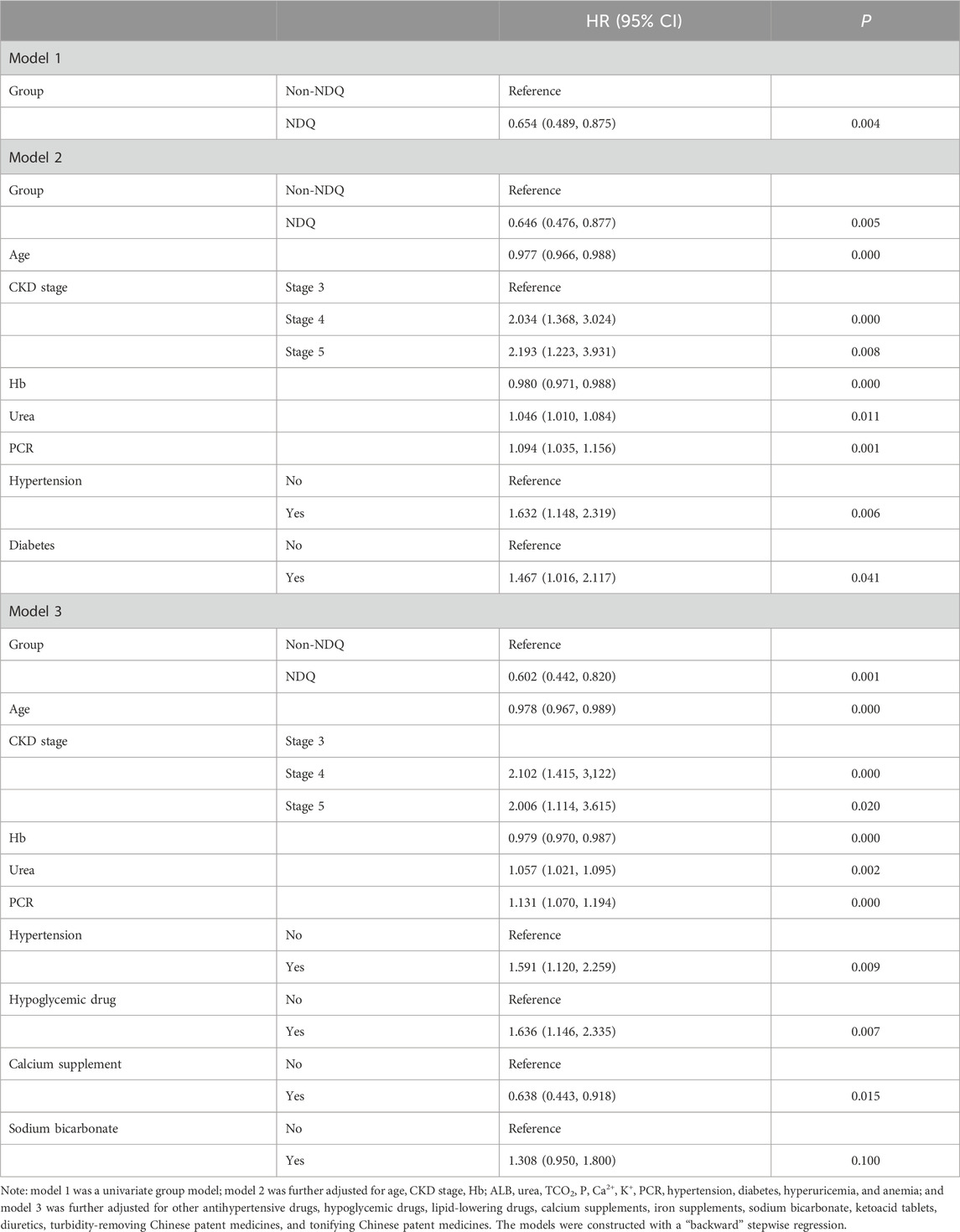
Table 3. Cox regression results.
A subgroup analysis was stratified by median age, sex, CKD stage, median PCR, hypertension, diabetes, and etiology based on model 3. The findings showed no interaction effect in the subgroup analysis (p > 0.05) (Figure 5).

Figure 5. Forest plot of subgroup analysis.
Our retrospective cohort study showed the long-term efficacy of Niaoduqing granules on non-dialysis CKD patients at stages 3–5. The results of the GLMM and survival analysis indicated that the participants taking Niaoduqing granules over the long term had a more steady growth in their SCr levels and a higher survival probability. Taking Niaoduqing granules was an independent protective factor for thwarting CKD progression (HR: 0.602, 95% CI: 0.441, 0.820, p = 0.001). Without any stratification, there was an interaction effect on the correlation between the NDQ group and the composite outcome.
CKD at stages 3–5 is known as “consumptive disease” or “edema” in traditional Chinese medicine. The pathogenesis involves spleen and kidney deficiency and retention of dampness, turbidity, and stasis, which lead to toxins congesting the body and can cause a series of diseases. In Niaoduqing granules, Radix Astragali (黄芪 huánɡ qí) and Codonopsis pilosula (党参 dǎnɡ shēn) can invigorate the spleen and supplement qi; Radix Polygoni Multiflori Preparata (制何首乌 zhì hé shǒu wū) nourishes the kidneys and strengthens essence; Radix et Rhizoma Rhei (生大黄 shēnɡ dà huánɡ) and Radix Paeoniae Alba (白芍 bái sháo) clear Fu organs and expel turbidity; Rhizoma A. macrocephalae (白术 bái zhú) strengthens the spleen and removes dampness; Wolfiporia extensa (茯苓 fú línɡ) and Plantago asiatica (车前草 chē qián cǎo) remove dampness; Rhizoma Pinelliae Praeparatum (姜半夏 jiānɡ bàn xià), mulberry root bark (桑白皮 sānɡ bái pí), and S. flavescens (苦参 kǔ shēn) eliminate dampness and harmonize the center; and L. striatum (川芎 chuān xiōnɡ) and S. miltiorrhiza (丹参 dān shēn) activate blood circulation and remove stasis. These ingredients work synergistically to strengthen the spleen and the kidneys, clear Fu organs, expel turbidity, activate blood circulation, and dissolve stasis. Theoretically, the effects of Niaoduqing granules should be consistent with the pathogenesis of CKD stages 3–5, promoting the expulsion of turbid toxins and thwarting disease progression.
Research has shown that the bioactive components of Niaoduqing granules might regulate M2 microglia and mediate the signal transducer and activator of transcription 6 (STAT6) and phosphoinositide-3 kinase γ (PI3Kγ) signaling pathways by affecting the phosphatase and tensin homolog (PTEN) and Jumonji domain-containing protein-3 (JMJD3) (Liu et al., 2020; Jiao et al., 2021a; Jiao et al., 2021b; An et al., 2022; Li et al., 2022; An et al., 2023; Liu et al., 2023). This can suppress tubular epithelial–mesenchymal cell transformation, improve microinflammatory states, reduce oxidative stress, and alleviate insulin resistance to mitigate renal fibrosis (Wei, 2013; Wang et al., 2017; Ai et al., 2021; Xu et al., 2023). Furthermore, Niaoduqing granules affect several amino acid metabolism pathways by regulating the intestinal flora to improve kidney function (Wu et al., 2016). Thus, its pharmacological and metabolomic mechanisms might relate to various bioactive ingredients, such as astragaloside, emodin, isoflavonoids, salvianolic acid A, and paeoniflorin (Kong et al., 2021; Zhao and Li, 2022). These ingredients may serve as an explanation for the clinical efficacy of Niaoduqing granules in modern pharmacology.
Our results were consistent with several clinical studies (Zheng et al., 2019; Song et al., 2022; Zhong et al., 2022) and offered several additional advantages. First, to the best of our knowledge, our study utilized the largest sample size of any study on Niaoduqing granules to date. We collected as many clinical characteristics as possible to imitate a real-world setting. It provided valuable data for supporting the long-term efficacy and safety of Niaoduqing granules. Second, the study used GLMM, which combined fixed and random effects to maximize the interpretation of data variability. PSM was used to reduce selection bias, and COX regression models were used to analyze the effect of independent variables on survival time and composite outcomes to minimize the effects of any confounding factors. Through these analyses, it was possible to demonstrate the clinical efficacy of Niaoduqing granules in the composite outcomes of CKD progression.
Our study also has several limitations. First, we did not collect or analyze the characteristics of TCM syndrome differentiation or the symptoms due to the limitations of a retrospective study. We also did not analyze the characteristics of Chinese herbal decoctions because most participants regularly took Chinese herbal decoctions at GPHCM. Second, the prescription duration did not cover any diagnosis or medication records from other medical institutions, and medication adherence was not assessed during the follow-up period. This may have introduced a selection bias. Third, although we adjusted for unbalanced covariates in model 2, there may still have been confounding effects. Fourth, although our study utilized the largest sample size, prospective studies with larger sample sizes will be necessary for further research.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Ethics Committee of Guangdong Provincial Hospital of Chinese Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because our study is a retrospective cohort study based on the HIS dataset.
H-FC: formal analysis, methodology, and writing–original draft. Y-JL: data curation, visualization, and writing–review and editing. YH: data curation, visualization, and writing–review and editing. X-LZ: methodology, visualization, and writing–review and editing. R-BW: visualization and writing–review and editing. JC: data curation and writing–review and editing. YP: methodology, visualization, and writing–review and editing. L-ZF: supervision and writing–review and editing. FT: supervision and writing–review and editing. X-NJ: supervision and writing–review and editing. X-NT: funding acquisition and writing–review and editing. X-SL: funding acquisition, project administration, and writing–review and editing. Y-FW: funding acquisition and writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the National Key Research and Development Program of China (project no. 2019YFE0196300), the Guangzhou Technology Program of Agriculture and Social Development of Key Research and Development Scheme (project no. 202206010102), and the Sanming Project of Medicine in Shenzhen (no. SZZYSM202206014).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2024.1379338/full#supplementary-material
AIC, Akaike information criterion; ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; ALB, serum albumin; BIC, Bayesian information criterion; CKD, chronic kidney disease; Ca2+, calcium; CVDs, cardiovascular diseases; eGFR, estimated glomerular filtration rate; ESRD, end-stage kidney disease; GPHCM, Guangdong Provincial Hospital of Chinese Medicine; GFR, glomerular filtration rate; Glu, fasting blood glucose; GLMM, generalized linear mixed model; HIS, hospital information system; Hb, hemoglobin; HR, hazard ratio; HDL-C, high-density lipoprotein cholesterol; K+, potassium; LDL-C, low-density lipoprotein cholesterol; NDQ, Niaoduqing group; Na+, sodium; 95% CI, 95% confident interval; P, phosphorous; PCR, protein/creatinine ratio; PSM, propensity score matching; RRT, renal replacement therapy; SCr, serum creatinine; SGLT2i, sodium–glucose cotransporter-2 inhibitors; SE, standard error; TCO2, total carbon dioxide; TC, total cholesterol; urea, blood urea nitrogen; UA, uric acid.
Ai, S., Zhu, Z., Zheng, H., et al. (2021). Analyzing the internal mechanism of Niaoduqing Granule for treating chronic kidney disease based on network pharmacology. Chin. J. Integr. Traditional West. Nephrol. 22, 409–413.
An, C., Jiao, B., Du, H., Tran, M., Song, B., Wang, P., et al. (2023). Jumonji domain-containing protein-3 (JMJD3) promotes myeloid fibroblast activation and macrophage polarization in kidney fibrosis. Br. J. Pharmacol. 180 (17), 2250–2265. doi:10.1111/bph.16096
An, C., Jiao, B., Du, H., Tran, M., Zhou, D., and Wang, Y. (2022). Myeloid PTEN deficiency aggravates renal inflammation and fibrosis in angiotensin II-induced hypertension. J. Cell Physiol. 237 (1), 983–991. doi:10.1002/jcp.30574
Jiao, B., An, C., Du, H., Tran, M., Wang, P., Zhou, D., et al. (2021b). STAT6 deficiency attenuates myeloid fibroblast activation and macrophage polarization in experimental folic acid nephropathy. Cells 10 (11), 3057. Published 2021 Nov 6. doi:10.3390/cells10113057
Jiao, B., An, C., Tran, M., Du, H., Wang, P., Zhou, D., et al. (2021a). Pharmacological inhibition of STAT6 ameliorates myeloid fibroblast activation and alternative macrophage polarization in renal fibrosis. Front. Immunol. 12, 735014. Published 2021 Aug 26. doi:10.3389/fimmu.2021.735014
KDIGO (2021a). Kidney disease: improving global outcomes (KDIGO) blood pressure work group, KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 99, S1–S87. doi:10.1016/j.kint.2020.11.003
KDIGO (2021b). Kidney disease: improving global outcomes (KDIGO) glomerular diseases work group, KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 100, S1–S276. doi:10.1016/j.kint.2021.05.021
Kong, F., Wang, H., and Zhou, J. (2021). HPLC method for determination contents of paeoniflorin, plantamoside and tanshinone ⅡA in Niaoduqing granules (sugar-free type). Anhui Med. Pharm. J. 25, 2178–2181.
Li, Z., Ma, D., Wang, Y., Wu, S., Wang, L., Jiang, Y., et al. (2022). Astragali radix-coptis rhizoma herb pair attenuates atherosclerosis in ApoE-/- mice by regulating the M1/M2 and Th1/Th2 immune balance and activating the STAT6 signaling pathway. Evid. Based Complement. Altern. Med. 2022, 7421265. Published 2022 Feb 7. doi:10.1155/2022/7421265
Liu, L., Zhang, R., Chen, C., Xia, C., Yao, G., He, X., et al. (2023). The effect of Banxia-houpo decoction on CUMS-induced depression by promoting M2 microglia polarization via TrkA/Akt signalling. J. Cell Mol. Med. 27 (21), 3339–3353. doi:10.1111/jcmm.17906
Liu, X., Lu, J., Liu, S., Huang, D., Chen, M., Xiong, G., et al. (2020). Huangqi-Danshen decoction alleviates diabetic nephropathy in db/db mice by inhibiting PINK1/Parkin-mediated mitophagy. Am. J. Transl. Res. 12 (3), 989–998. Published 2020 Mar 15.
Liyanage, T., Toyama, T., Hockham, C., Ninomiya, T., Perkovic, V., Woodward, M., et al. (2022). Prevalence of chronic kidney disease in Asia: a systematic review and analysis. BMJ Glob. Health 7 (1), e007525. doi:10.1136/bmjgh-2021-007525
National Kidney Foundation (2002). K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am. J. Kidney Dis. 39, S1–S266.
Song, J., Han, X., Zhang, J., et al. (2022). Efficacy analysis of Niaoduqing granules combined with iontophoresis with traditional Chinese medicine in the renal region to treat stage 3-4 chronic kidney disease. China Pract. Med. 17, 20–24.
Standardization project group (2021). Standardization project group for the Guidelines for the Clinical Use of Chinese Patent Medicine in Dominant Diseases, Guidelines for the clinical use of Chinese patent medicine for treating stage 3-5 chronic kidney diseases (non-dialysis) (2020). Chin. J. Integr. Med. 41 (3), 261–272.
Wang, X., Yu, S., Jia, Q., Chen, L., Zhong, J., Pan, Y., et al. (2017). NiaoDuQing granules relieve chronic kidney disease symptoms by decreasing renal fibrosis and anemia. Oncotarget 8, 55920–55937. doi:10.18632/oncotarget.18473
Wang, Y., Sun, L., Li, M., et al. (2023). Scoping review of clinical studies of oral Chinese patent medicine for treating chronic kidney disease. Chin. J. Exp. Traditional Med. Formulae 29, 99–108.
Wei, Q. (2013). Mechanism of Niaoduqing Granule in regulating MMPs in kidney tissues and their signaling pathways to promote ECM degradation in renal failure model. Nanjing, China: Nanjing University of Traditional Chinese Medicine, 48.
Wu, W., Huang, Y., Wan, Y., Yang, H. M., Mao, Z. M., Yang, J. J., et al. (2016). Effects and mechanisms of UCG ameliorating renal interstitial fibrosis by regulating TGF-β1/SnoN/Smads signaling pathway in renal failure rats. China J. Chin. Materia Medica 41, 2291–2297. doi:10.4268/cjcmm20161220
Xu, Y., Huang, Y., He, M., and Chu, F. J. (2023). Effect of Uremic Clearance Granules on improvement of chronic kidney disease in rats based on microbiome-metabolomics and its mechanism. China J. Chin. Materia Medica 48, 160–169. doi:10.19540/j.cnki.cjcmm.20220901.401
Yan, M., Lv, J., Xie, Y., et al. (2020). Expert questionnaire survey analysis for the clinical use of Chinese patent medicine for treating stage 3-5 chronic kidney diseases (non-dialysis). Chin. J. Integr. Traditional West. Nephrol. 21, 1047–1050.
Zhao, L., and Li, Q. (2022). Determination of three constituents in Niaoduqing Particles by high per-formance liquid chromatography. China Med. Her. 19, 112–115.
Zheng, Y., Cai, G., He, L., Lin, H. L., Cheng, X. H., Wang, N. S., et al. (2017). Efficacy and safety of niaoduqing particles for delaying moderate-to-severe renal dysfunction: a randomized, double-blind, placebo-controlled, multicenter clinical study. Chin. Med. J. Engl. 130, 2402–2409. doi:10.4103/0366-6999.216407
Zheng, Y., Wang, N. S., Liu, Y. N., He, L. Q., Jian, G. H., Liu, X. S., et al. (2019). Effects of niaoduqing particles on delaying progression of renal dysfunction: a post-trial, open-label, follow-up study. Chin. J. Integr. Med. 25, 168–174. doi:10.1007/s11655-018-2998-y
Keywords: chronic kidney disease, long-term efficacy, Chinese patent medicine, longitudinal analyze, Niaoduqing granules
Citation: Chen H-F, Lin Y-J, Han Y, Zhang X-L, Wang R-B, Chen J-H, Pi Y, Fu L-Z, Tang F, Jie X-N, Tang X-N, Liu X-S and Wu Y-F (2024) A Chinese patent medicine’s long-term efficacy on non-dialysis patients with CKD stages 3–5: a retrospective cohort study. Front. Pharmacol. 15:1379338. doi: 10.3389/fphar.2024.1379338
Received: 31 January 2024; Accepted: 02 April 2024;
Published: 26 April 2024.
Edited by:
Dong Zhou, University of Connecticut, United StatesCopyright © 2024 Chen, Lin, Han, Zhang, Wang, Chen, Pi, Fu, Tang, Jie, Tang, Liu and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiao-Na Tang, dGFuZ3hpYW9uYTgxQGd6Y3VtLmVkdS5jbg==; Xu-Sheng Liu, bGl1eHU4MDFAMTI2LmNvbQ==; Yi-Fan Wu, d3V5aWZhbjAwN0BnenVjbS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.