
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 22 January 2024
Sec. Drugs Outcomes Research and Policies
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1327155
This article is part of the Research Topic Recent Advances in Attempts to Improve Medication Adherence – from basic research to clinical practice, volume II View all 19 articles
 Tasmania Del Pino-Sedeño1,2,3,4,5†
Tasmania Del Pino-Sedeño1,2,3,4,5† Diego Infante-Ventura1,2,5*†
Diego Infante-Ventura1,2,5*† Diego Hernández-González4Yadira González-Hernández1,2
Diego Hernández-González4Yadira González-Hernández1,2 Beatriz González de León6
Beatriz González de León6 Amado Rivero-Santana1,2,3
Amado Rivero-Santana1,2,3 Isabel Hurtado3,7Francisco Javier Acosta Artiles8,9
Isabel Hurtado3,7Francisco Javier Acosta Artiles8,9Introduction: Current evidence reveals concerning rates of non-adherence to antidepressant treatment, possibly influenced by various relevant determinants such as sociodemographic factors or those related to the health system and their professionals. The aim of this paper is to review the scientific evidence on sociodemographic and clinical predictors of adherence to pharmacological treatment in patients diagnosed with a depressive disorder.
Methods: a systematic review (SR) was conducted. The search for a previous SR was updated and de novo searches were performed in Medline, EMBASE, Web of Science (WoS) and PsycInfo (last 10 years). The risk of bias was assessed using the Cochrane tool for non-randomized studies—of Exposure (ROBINS-E). Meta-analyses were conducted.
Results: Thirty-nine studies (n = 2,778,313) were included, 24 of them in the meta-analyses. In the initiation phase, no association of adherence was found with any of the predictors studied. In the implementation and discontinuation phases, middle-aged and older patients had better adherence rates and lower discontinuation rates than younger ones. White patients adhered to treatment better than African-American patients.
Discussion: Age and ethnicity are presented as the predictive factors of pharmacological adherence. However, more research is needed in this field to obtain more conclusive results on other possible factors.
Systematic Review Registration: [https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023414059], identifier [CRD42023414059]
Mood disorders have become a central axis of public health policies due to both their high prevalence and the consequences that this group of disorders have in patients (GBD, 2019 Mental Disorders Collaborator, 2022).
Depressive disorders are a common mental health condition that can have a significant impact on an individual’s overall well-being and daily functioning (World Health Organization, 2017; GBD, 2019 Mental Disorders Collaborator, 2022). This condition results in a reduction in the average life expectancy of 15 years with respect to the population that does not suffer from it (Rivera et al., 2019). In 2019, around 3.9% of the global population suffered from some type of depressive disorder, which translates into a figure of more than 279 million people (Santomauro et al., 2021). On the other hand, persistent depressive disorder, due to the long-lasting manifestation of symptoms, is related to higher rates of comorbidity and a considerable reduction in wellbeing and health-related quality of life (HRQoL) (Nübel et al., 2020).
There is a wide variability of therapeutic options available for the management of depressive disorders. Psychotherapy is indicated for mild to moderate depression, due to its proven effectiveness (NICE, 2022), its long-term superiority, as well as lower dropout rates and lower relapse rates than pharmacological treatments with tricyclic and second generation antidepressants (ADs) (selective serotonin reuptake inhibitors -SSRIs) (Cano-Vindel et al., 2012). However, for the approach and treatment of moderate to severe depressive disorders (Kok and Reynolds, 2017), pharmacological treatment with AD medications, accompanied by a relevant high-intensity psychological intervention is the recommended therapeutic choice (NICE, 2022). Therefore, pharmacological treatment is also among the treatments with proven effectiveness for the management of depression (NICE, 2022). The most recommended current pharmacological regimen, due to its benefit-risk balance, is monotherapy with second-generation ADs, such as SSRIs, among others. Therefore, it should be mentioned that the most recent generations of therapeutic agents have been shown to have higher adherence rates (Sheehan et al., 2008). Nevertheless, most patients do not achieve remission of their symptoms, which is why clinical practice guidelines recommend different second-order options, such as changing monotherapy or combined treatment with two types of ADs (Wolff et al., 2021). However, the effectiveness of a treatment depends on both the efficacy of a medication and patient adherence to the therapeutic regimen (Jimmy and Jose, 2011).
As stated by the World Health Organization (WHO) (World Health Organization, 2004), adherence is defined as the degree to which the person’s behavior-taking medication, following a diet and executing lifestyle changes-corresponds to the agreed recommendations from a healthcare provider. The pharmacological adherence process consists of three phases (Vrijens et al., 2012): initiation, when the patient takes the first dose of a prescribed drug; implementation, defined as the extent to which a patient’s actual dose corresponds to the dose of the prescribed regimen, and discontinuation, when the patient stops the medication on their own initiative, taking no doses thereafter.
Adherence to treatment with ADs significantly impacts the clinical outcomes of the recovery process, with non-adherent patients showing higher rates of relapse, hospitalizations, and visits to the emergency room for events related to depression. This increased need for ongoing medical care imposes a significant burden and economic impact on any healthcare system (Ho et al., 2016), especially considering that, 3 months after starting treatment, the percentage of non-adherent patients ranges from 30% to 70% (Párraga Martínez et al., 2014).
In this context, numerous studies have been carried out to determine the degree of adherence to psychopharmacological treatment with ADs and to analyze its correlates and predictors (Rivero-Santana et al., 2013; Párraga Martínez et al., 2014). The WHO identifies five groups of factors that influence, to a certain extent, the lack of adherence to drug treatment: social and economic factors, therapy-related factors, disease-related factors, patient-related factors, and healthcare system-related factors (Pagès-Puigdemont and Valverde-Merino, 2018). However, current evidence is not consistent regarding the factors relevant to predicting good adherence.
Lack of adherence has serious consequences for patients. Therefore, it is essential to identify the factors that influence the decision-making process regarding the initiation, continuation, or discontinuation of treatment. This information will help enhance current theoretical models and develop more precise and effective interventions tailored to diverse subgroups within the population (Saldaña et al., 2019) at a higher risk of non-adherence (Akincigil et al., 2007). However, the last systematic review (SR) published in this field was conducted 10 years ago (Rivero-Santana et al., 2013), and, thus, updating the available evidence is necessary.
The objective of this systematic review (SR) is to identify, critically evaluate and synthesize the new evidence available in the scientific literature on the sociodemographic and clinical predictive factors influencing adherence to drug treatment in adult patients diagnosed with a depressive disorder.
A systematic review (SR) was conducted by updating the search of a previous SR (Rivero-Santana et al., 2013), following the methodology of the Cochrane Collaboration, according to the MECIR (Methodological Expectations of Cochrane Intervention Reviews) standards (Higgins et al., 2016). The information related to this SR is presented following the guidelines of the PRISMA statement (Page et al., 2021). The SR protocol was registered in PROSPERO (registration number: CRD42023414059).
Studies that evaluated sociodemographic and clinical factors predictive of adherence to AD treatment in patients diagnosed with depressive disorders and which met the selection criteria described below were selected.
Observational studies of prospective and retrospective cohorts were included for the study design. Randomized clinical trials, non-randomized clinical trials, experimental studies with a before-after design, case-control studies, cross-sectional studies, case series and isolated cases, animal studies, and in vitro studies were excluded.
The patients included were those over the age of 18 diagnosed with a depressive disorder (ICD-10: F32, depressive episodes; F33, recurrent depressive disorder; F34.1, dysthymia; DSM-V: 296.33, major depressive disorder; 300.4, persistent depressive disorder) by a healthcare provider or by the study investigator. Studies with patients with a manic episode and bipolar affective disorder (ICD-10: F-30-31), schizophrenia, schizotypal, and delusional disorders (ICD-10: F20-29), as well as patients receiving AD treatment without reported diagnosis, were excluded.
The following sociodemographic and clinical variables were considered as predictive factors: age, sex, ethnicity, education, marital status, income, employment status, diagnostic subtype, severity of depression, previous episodes, psychiatric and medical comorbidities, cognitive impairment, and self-perceived health or HRQoL.
Adherence (initiation, implementation and discontinuation) of the pharmacological prescriptions were included as result measures.
Regarding language, only studies published in English and/or Spanish were considered.
As for the type of publication, complete original papers and those published in scientific journals were considered. Conference papers, editorials, conference abstracts, letters to the editor, and opinions were excluded.
The search for relevant studies was performed following a search strategy around the terms depressive disorders, antidepressants and adherence in Medline (Ovid platform), EMBASE (Elsevier interface), Web of Science (WoS) (Clarivate Analytics) and PsycInfo (11/09/2022) (see Supplementary Table S1). The search was restricted to studies published in English or Spanish in the last 10 years, the date of the search for the previous SR (Rivero-Santana et al., 2013). The search for published studies was completed with the review of the bibliography lists of the relevant publications retrieved from the electronic databases and with verification in Google Scholar of the studies citing the selected studies.
The bibliographic references recovered from the different databases were imported into the RAYYAN platform (Ouzzani et al., 2016) where duplicates were eliminated to subsequently select the pertinent studies.
Five reviewers performed the pairwise selection process independently and in parallel. The studies were selected in two phases, a first phase when the studies were selected based on the information provided in the title and abstract; and a second phase when the full texts of the studies selected as relevant in the first phase were analyzed and classified as included or excluded according to the specified selection criteria.
Data extraction from the studies was performed using data extraction sheets in Excel format designed ad hoc. A pilot test was conducted with two of the studies, independently by the all reviewers, with the aim of unifying extraction criteria. The rest of the extraction from each study was carried out in duplicate.
Data related to the identification of the article (authors, date of publication, country where the study was conducted, funding, etc.), the design and methodology (objective, design and duration of the study, characteristics and sociodemographic and clinical variables of participants and measure of adherence), as well as predictive factors and adherence, were extracted.
The methodological quality of the included studies was assessed independently and in parallel by all reviewers using the Cochrane tool for non-randomized studies - of Exposure, ROBINS-E (ROBINS-E Development Group et al., 2023). Following the guidelines of the ROBINS-E tool, some specific characteristics of the study led directly to the result having a very high risk of bias since the control of confounders did not match the study’s objective. In this SR, this minimal set of confounders include age, sex, and the level of depression.
The graphs for the summary of the risk of bias assessments were drawn with the Rovbis web app (McGuinness and Higgins, 2020).
Disagreements in the selection, extraction and risk of bias assessment phases were resolved after discussion and, if consensus was not reached, a third reviewer was consulted. The discussions and agreements were documented.
The information collected was synthesized narratively with tabulation of the results from each included study. A quantitative synthesis using meta-analyses (MA) was performed when the reported data were combinable and the studies were homogeneous in their methodology (population, predictive factors, etc.). To estimate adherence rates (implementation and discontinuation), MA was conducted using the metaprop command (Nyaga et al., 2014) in the STATA software version 17 for Windows (Stata Corp LLC, College Station, TX, United States). To synthesize the predictors of adherence, taking into account the weeks of follow-up, odds ratio (OR) or hazard ratio (HR) and their 95% confidence intervals were synthesized using the generic inverse variance method with the Review Manager software for Windows (RevMan, version 5.4.1., 2020; The Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark). MA were performed using univariate estimates only, multivariate estimates only, and preferably univariate or multivariate estimates for each predictor. MA were performed for each predictive factor using both univariate and/or multivariate estimates. An MA was performed exclusively using the respective data type in scenarios where only univariate or multivariate data were available. Conversely, when both univariate and multivariate data were present, preference was given to conducting multivariate estimates. If multivariate data were not available, univariate estimates were preferably used as an alternative. The I2 was used to assess statistical heterogeneity. Even so, a random effects model was used to address the inherent variability between studies. In the case of psychiatric comorbidities, the analysis was performed both globally (having a psychiatric comorbidity or not), and separately for different psychiatric comorbidities (sleep disorders vs. alcohol-related disorders vs. substance-related disorders). It was not possible to perform meta-regression or publication bias analyses due to the small number of studies included in each MA.
The number of references identified during the bibliographic search, once the duplicates were eliminated, came to 1,066. After the title and abstract screening, 58 publications were retrieved for full-text evaluation. After applying the pre-established selection criteria, 45 were excluded. On the other hand, the review of the studies included in the previous SR according to the current selection criteria resulted in 16 additionally included studies. Finally, by hand-examining the bibliography listings of the selected studies, as well as by checking Google Scholar for studies citing the selected studies, an additional 10 studies were located.
Thus, 39 studies were included in the final selection (Lin et al., 1995; Lin et al., 2011; Keeley et al., 2000; Keeley et al., 2007; Demyttenaere et al., 2001; Sirey et al., 2001; Cohen et al., 2004; Donohue et al., 2004; Olfson et al., 2006; Akincigil et al., 2007; Goethe et al., 2007; McLaughlin et al., 2007; Stang et al., 2007; ten Doesschate et al., 2009; Yen et al., 2009; Chen et al., 2010; Ereshefsky et al., 2010; Holma et al., 2010; Liu et al., 2010; Liu et al., 2011; Milea et al., 2010; Woolley et al., 2010; Hung et al., 2011; Vlahiotis et al., 2011; Merrick et al., 2012; Wu et al., 2012; Wu et al., 2013; Kales et al., 2013; Kales et al., 2016; Wu and Davis-Ajami (2014); Yau et al., 2014; Kogut et al., 2016; Gerlach et al., 2017; Gerlach et al., 2019; Holvast et al., 2019; Bhattacharjee et al., 2020; Nam-Ju and Yeon-Pyo, 2020; Noh et al., 2020; Noh et al., 2022; Shin et al., 2022) (See Figure 1).
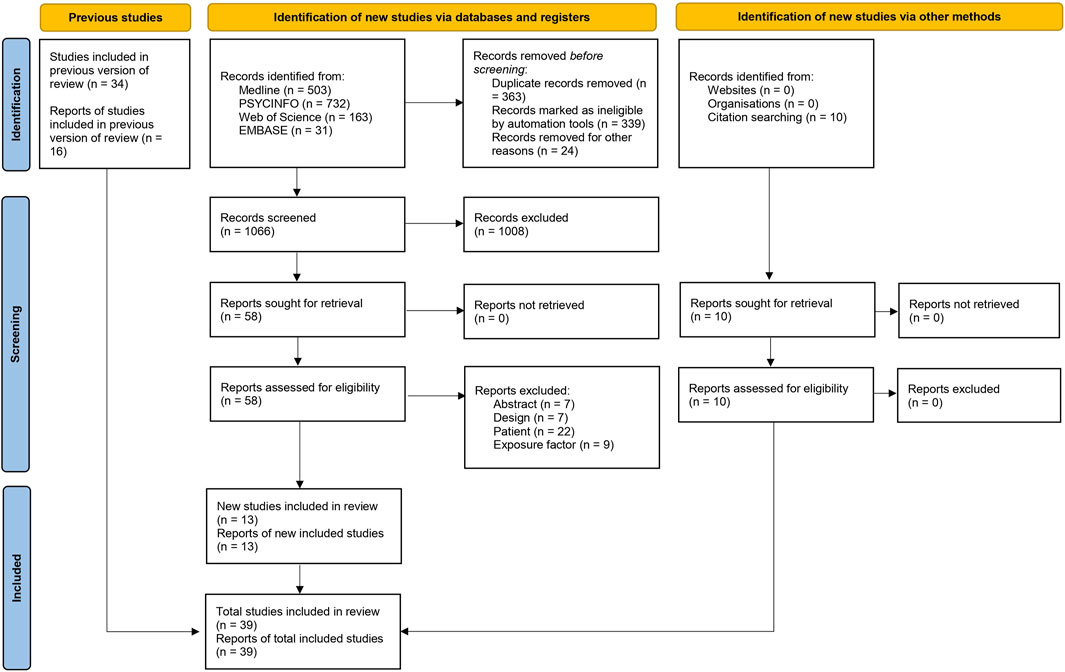
FIGURE 1. Flow diagram of the selection process of studies.
Although many of these articles were excluded because they did not meet more than one selection criteria, Supplementary Table S2 shows the main reason for their exclusion.
The characteristics of the studies, participants, predictive factors and adherence can be seen in more detail in Tables 1, 2, 3; however, a description of the main characteristics is provided below.
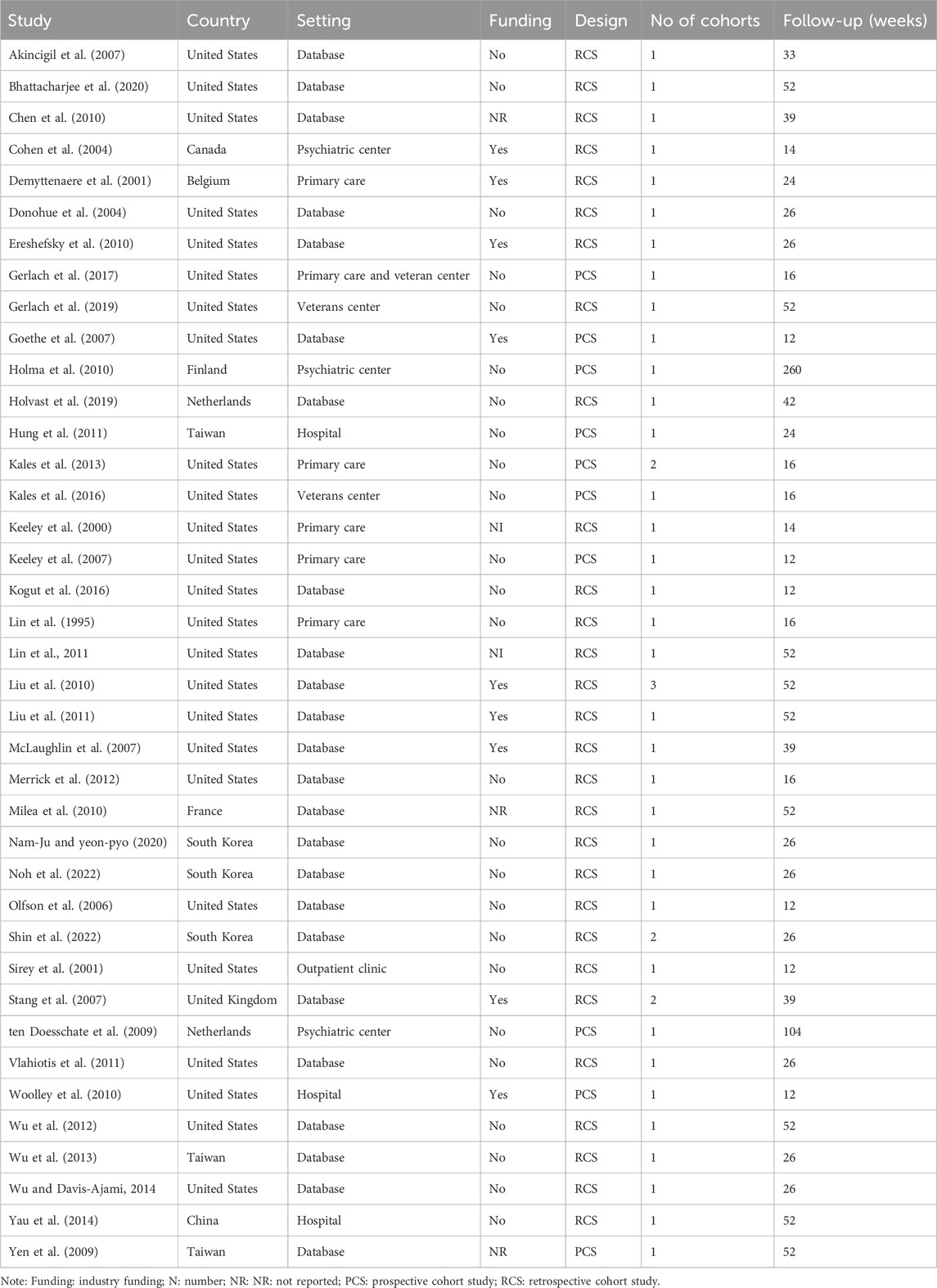
TABLE 1. General characteristics of the included studies.

TABLE 2. Main demographic and baseline clinical characteristics of the participants in the included studies.
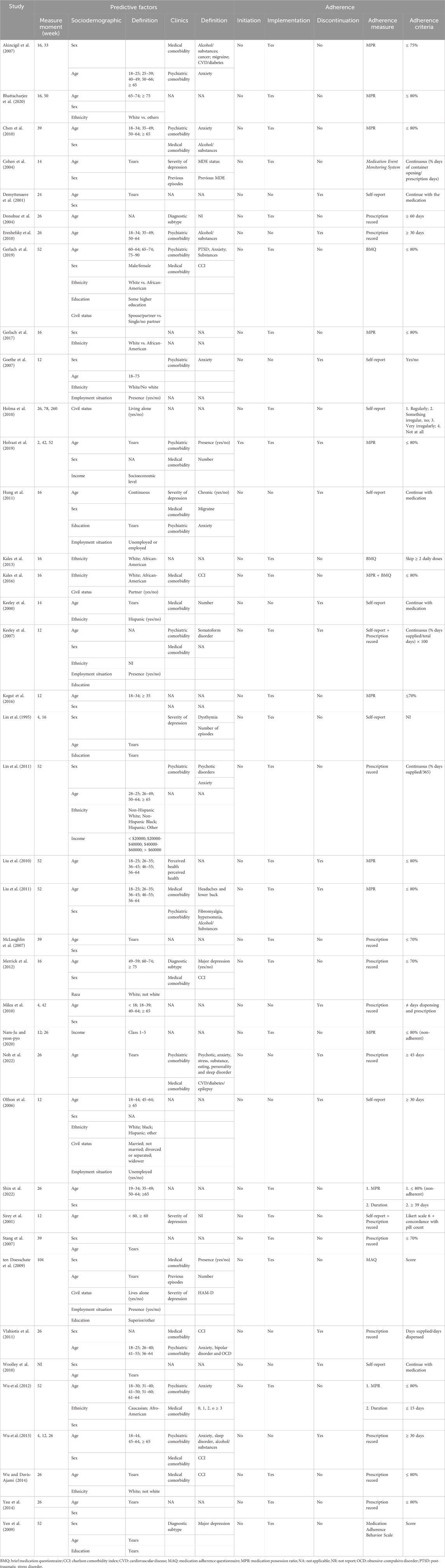
TABLE 3. Main characteristics of the predictive factors and the measure of adherence.
All included studies were published in English between the years 1995 and 2022. The countries where such studies were published were: United States (25 studies), South Korea (3 studies); Taiwan (3 studies), the Netherlands (2 studies), Belgium (1 study), Canada (1 study), China (1 study), Finland (1 study), France (1 study) and the United Kingdom (1 study).
In terms of design, 12 were prospective observational cohort studies (Demyttenaere et al., 2001; Cohen et al., 2004; Goethe et al., 2007; Keeley et al., 2007; ten Doesschate et al., 2009; Yen et al., 2009; Holma et al., 2010; Woolley et al., 2010; Hung et al., 2011; Kales et al., 2013; Kales et al., 2016; Gerlach et al., 2017) and the remaining 27 were retrospective observational cohort studies.
Of all the selected studies, the majority, 35 (89.7%), included one cohort, three studies (7.69%) included two cohorts (Stang et al., 2007; Kales et al., 2013; Shin et al., 2022) and one study included three cohorts (Liu et al., 2010). Multiple cohort studies were compared based on characteristics such as the dose or type of medication, ethnicity, and the healthcare insurance coverage (e.g., uninsured, partially or fully insured).
The studies were carried out in psychiatric settings (Cohen et al., 2004; ten Doesschate et al., 2009; Holma et al., 2010), primary care centers (Lin et al., 1995; Keeley et al., 2000; Keeley et al., 2007; Demyttenaere et al., 2001; Kales et al., 2013; Gerlach et al., 2017), hospitals (Woolley et al., 2010; Hung et al., 2011; Yau et al., 2014), veterans clinics (Kales et al., 2016; Gerlach et al., 2017; Gerlach et al., 2019), outpatient clinics (Sirey et al., 2001), while the rest were conducted with database records.
Of the studies selected for this review, 23.08% received industry funding (Demyttenaere et al., 2001; Cohen et al., 2004; Goethe et al., 2007; McLaughlin et al., 2007; Stang et al., 2007; Ereshefsky et al., 2010; Liu et al., 2010; Liu et al., 2011; Woolley et al., 2010), 64.10% did not receive funding from industry and the source of their funding is unknown in 12.82% of the studies.
Follow-up periods were variable, with the closest follow-up being 12 weeks after starting treatment (Sirey et al., 2001; Olfson et al., 2006; Goethe et al., 2007; Keeley et al., 2007; Woolley et al., 2010; Kogut et al., 2016) and the longest period was 260 weeks (Holma et al., 2010). The information regarding the characteristics of the studies can be seen below in Table 1.
Regarding the predictive factors, more specifically the sociodemographic ones, of the 39 studies selected for this SR, 34 analyzed the effect of age on adherence to treatment, 28 the effect of sex, 13 studies analyzed ethnicity, six studies explored the influence of educational level, five of marital status, and five studies of employment status.
Regarding clinical factors, of the 39 studies, 13 analyzed the relationship of psychiatric comorbidities on adherence to treatment, 16 medical comorbidities, five the severity of depression, two the relationship of previous episodes, three the subtype of diagnosis and one perceived health on adherence.
In relation to the phases of adherence, of all the selected studies, only one studied the adherence initiation phase (Holvast et al., 2019), 29 studied the implementation phase and 16 the discontinuation phase.
The selected studies used different tools to measure adherence in the implementation phase. By using the Medication Possession Ratio (MPR), nine studies established a threshold of 80%, one study a threshold of 75% and another one a threshold of 70%; two studies used the Brief Medication Questionnaire; one study used the Medication Adherence Behavior Scale; one the Medication Event Monitoring System - Pill Count; one the Medication Adherence Questionnaire (MAQ); three used self-reports developed ad hoc and eight used prescription records.
The information described above is shown in more detail in Table 3 below.
In general, the risk of bias was considered very high in 20 of the studies in this SR due to the lack of control over significant confounding variables such as age, sex, and the severity of depression. In the rest of the fully evaluated articles, the risk of bias was high in four studies, low in 13 studies, while only one study presented unclear risk of bias.
Detailed judgments for each of the risk of bias domain criteria are shown in Figures 2, 3.
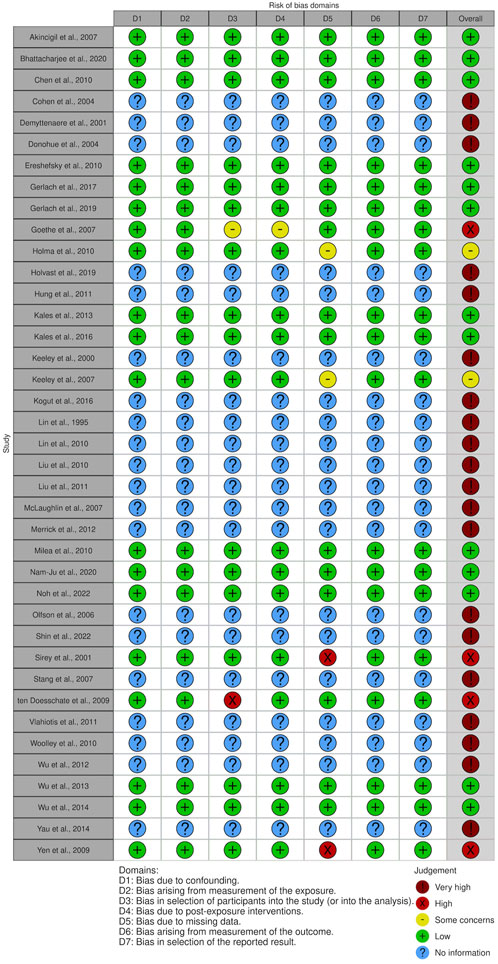
FIGURE 2. Risk of bias assessment of included studies.
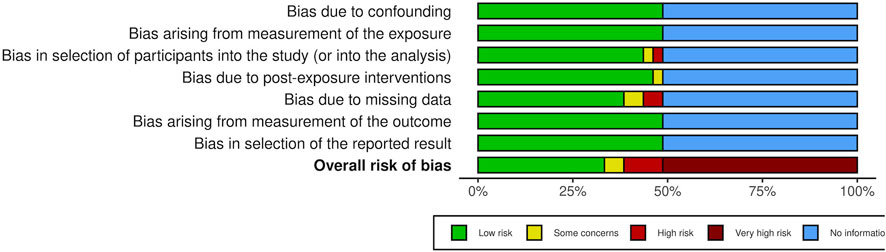
FIGURE 3. Risk of bias assessment across included studies.
The evidence tables included in Supplementary Tables S3–S6 show the main findings obtained in the included studies.
Of the total number of included studies, 24 could be included in the MA (Donohue et al., 2004; Olfson et al., 2006; Akincigil et al., 2007; Goethe et al., 2007; Stang et al., 2007; ten Doesschate et al., 2009; Yen et al., 2009; Chen et al., 2010; Ereshefsky et al., 2010; Liu et al., 2010; Liu et al., 2011; Milea et al., 2010; Woolley et al., 2010; Vlahiotis et al., 2011; Merrick et al., 2012; Wu et al., 2012; Wu et al., 2013; Kales et al., 2013; Kales et al., 2016; Yau et al., 2014; Kogut et al., 2016; Gerlach et al., 2019; Holvast et al., 2019; Noh et al., 2022). Tables 4, 5 show the results of the estimation of the global effect size for the outcome measures that could be meta-analyzed (see forest plots in Supplementary Figures S1–S13).
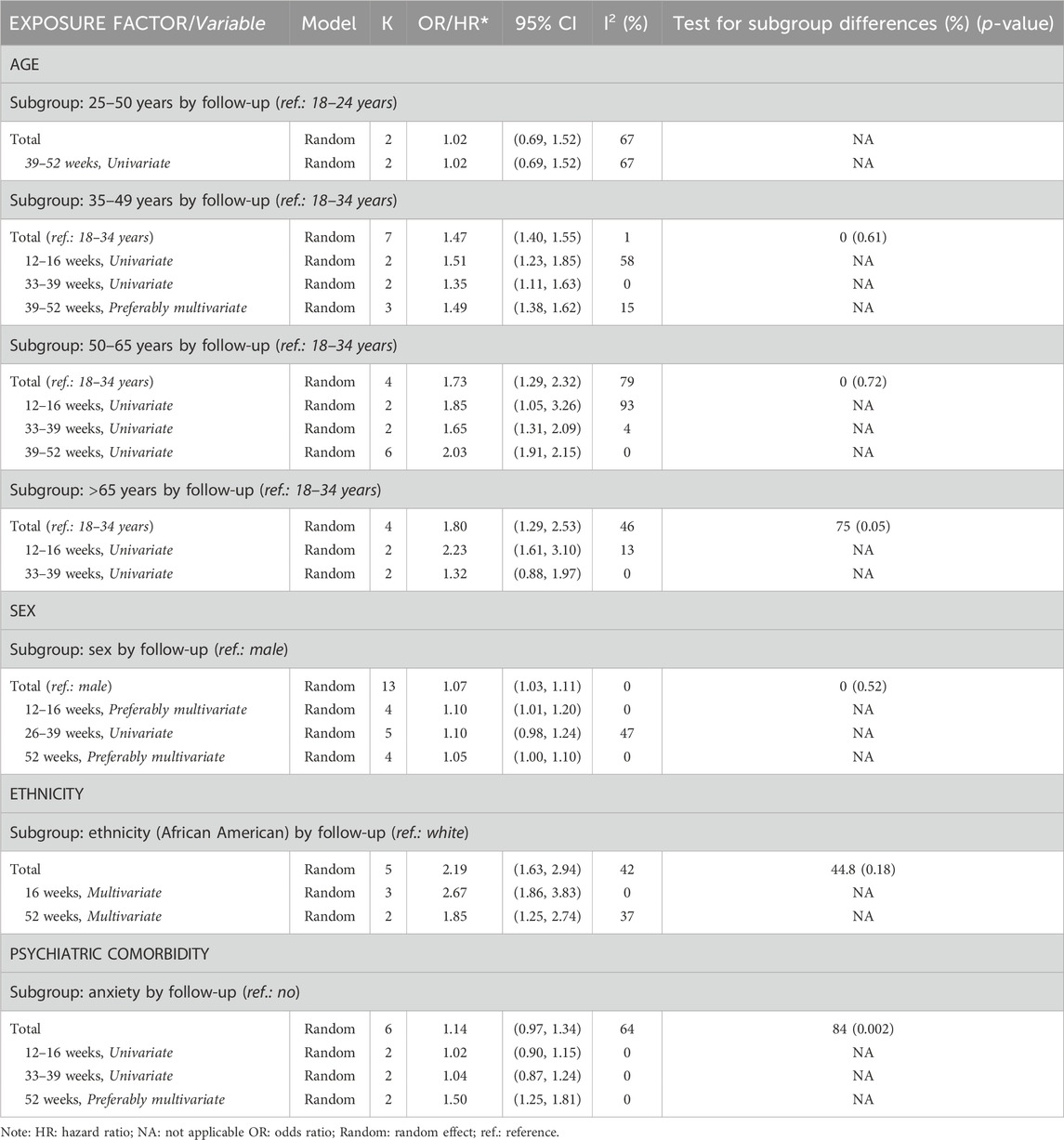
TABLE 4. Results of the meta-analyses. Implementation.
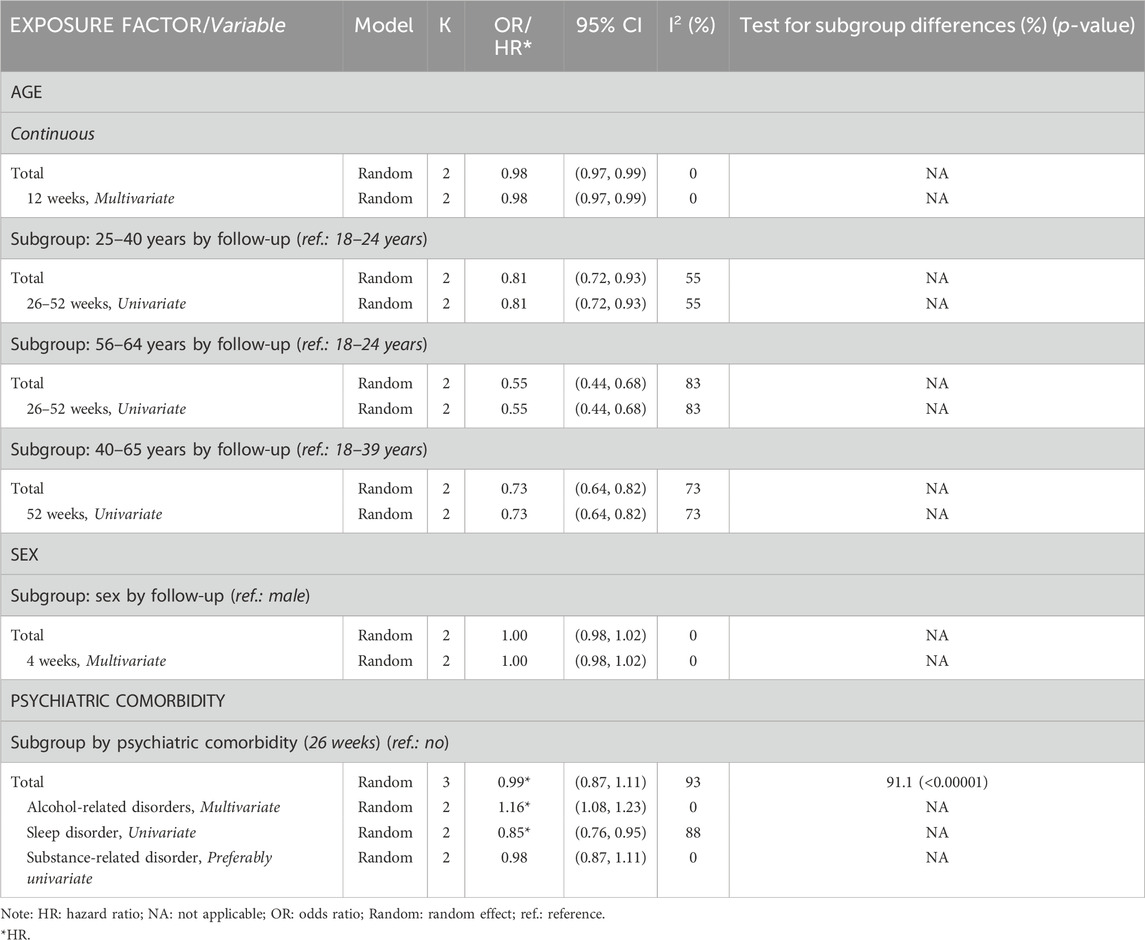
TABLE 5. Results of the meta-analyses. Discontinuation.
In relation to the initiation rates, 36.04% of the patients who were prescribed an AD treatment did not start it (Holvast et al., 2019).
Regarding the implementation phase, only 14% of the patients complied with the pharmacological treatment for up to 3 months, a similar percentage of the patients complied between months three and six (13%). In addition, a slight increase to 29% was observed between months six and nine and this increased to 57% between months nine and twelve, with this being the moment of greatest compliance. Once 1 year of treatment had been completed, the percentage of patients began to decrease to 31%, returning to a similar rate to the initial rates after 1 year (16%).
Regarding the discontinuation phase, 31% of the patients who were prescribed an AD treatment completed their treatment between the first three and 6 months of treatment and this rose to 52% of the patients at 40–52 weeks.
The results relating to the predictive factors of adherence during the initiation phase (Holvast et al., 2019), are described below.
When considering the different AD treatments together, no predictive factor (physical comorbidities, chronic drug use, age, sex, and socioeconomic status) was associated with non-initiation. However, specifically for the SSRIs, it was observed that not starting pharmacological therapy was associated with a higher socioeconomic level (OR = 1.13; 95% CI: 1.01, 1.27). Regarding other types of ADs (N06AF -monoamine oxidase inhibitors- and N06AX—other ADs), being a woman was associated with the risk of non-initiation (OR = 7.89; 95% CI: 1.50, 41.68), however, the increase in the number of medications for chronic use decreased this risk (OR = 0.65; 95% CI: 0.46–0.90).
The results obtained relating to the predictive factors of adherence during the implementation phase are described below.
Five studies (Akincigil et al., 2007; Chen et al., 2010; Liu et al., 2010; 2011; Wu et al., 2012) provided synthesizable data on the predictor variable age through an MA.
Between the first 12–16 weeks, patients older than 65 years of age (OR = 2.23; 95% CI: 1.61, 3.10; I2 = 13%; k = 2), patients between the ages of 35–49 (OR35-49 = 1.51; 95% CI: 1.23, 1.85; I2 = 58%; k = 2) and between 50 and 65 (OR50-65 = 1.85; 95% CI: 1.05, 3.26; I2 = 93%; k = 2) had better adherence rates when compared to younger ones (18–34 years).
Between 33 and 39 weeks, patients older than 65 years did not present better adherence rates (vs. 18–34 years) (OR = 1.32; 95% CI: 0.88, 1.97; I2 = 0%; k = 2). However, patients aged 35–49 and 50–65 did maintain better adherence rates than younger patients (OR35-49 = 1.35; 95% CI: 1.11, 1.63; I2 = 0%; k = 2; OR50- 65 = 1.65; 95% CI: 1.31, 2.09; I2 = 4%; k = 2).
Between 39 and 52 weeks, middle-aged patients (50–65 years of age) when compared to younger ones (18–35 years), continued to present better adherence rates (OR = 2.03; 95% CI: 1.91, 2.15; I2 = 0%; k = 6). However, this effect disappeared in patients aged between 25 and 50 years (OR = 1.02; 95% CI: 0.69, 1.52; I2 = 67%; k = 2).
From week 39 to 52, patients between 35 and 49 years, compared to those between 18 and 34, showed a better treatment adherence rate (OR = 1.49; 95% CI: 1.38, 1.62; I2 = 15%; k = 3).
Additionally, data were available in 17 studies assessing the implementation phase, but could not be synthesized through an MA. Four studies (McLaughlin et al., 2007; Stang et al., 2007; Yen et al., 2009; Yau et al., 2014) that evaluated age (continuous) as a predictor found that the treatment adherence rate was higher among older individuals. Among the studies comparing different age groups, one study indicated a higher likelihood of treatment adherence among individuals between the ages of 35–65 compared to younger individuals (Shin et al., 2022). Three other studies also provided similar data, indicating that elderly patients have better adherence rates than patients under 60 years (Sirey et al., 2001), 45 years (Merrick et al., 2012) or 35 years (Kogut et al., 2016) of age. In the remaining nine studies (Lin et al., 1995; Lin et al., 2011; Cohen et al., 2004; Keeley et al., 2007; ten Doesschate et al., 2009; Wu and Davis-Ajami (2014); Gerlach et al., 2017; Holvast et al., 2019; Bhattacharjee et al., 2020), no significant differences of adherence during the implementation phase were found among different age groups.
The MA incorporated the findings from 11 studies (Donohue et al., 2004; Akincigil et al., 2007; Stang et al., 2007; Yen et al., 2009; Chen et al., 2010; Liu et al., 2011; Merrick et al., 2012; Yau et al., 2014; Kogut et al., 2016; Gerlach et al., 2019; Holvast et al., 2019).
Women adhered better to treatment than men between weeks 12 and 16 (OR = 1.10; IC95%: 1.01, 1.20; I2 = 0%; k = 4), although as the weeks progressed (26–39 and 52 weeks), this effect subsided (OR26-39 = 1.10; 95% CI: 0.98, 1.24; I2 = 47%; k = 5; OR52 = 1.05; 95% CI: 1.00, 1.10; I2 = 0%; k = 4).
Eleven additional studies could not be included in the MA. One of them (Shin et al., 2022) reported that female individuals presented a better treatment adherence rate than male individuals. The rest of the studies (Lin et al., 1995; Lin et al., 2011; Cohen et al., 2004; Keeley et al., 2007; McLaughlin et al., 2007; ten Doesschate et al., 2009; Wu et al., 2012; Kales et al., 2013; Gerlach et al., 2017; Bhattacharjee et al., 2020) did not find significant differences in adherence rates by sex.
The MA incorporated the findings from five studies (Merrick et al., 2012; Wu et al., 2012; Kales et al., 2013; Kales et al., 2016; Gerlach et al., 2019).
White patients had higher treatment adherence rates than African-Americans at both 16 and 52 weeks (OR16 = 2.67; 95% CI: 1.86, 3.83; I2 = 0%; k = 3; OR52 = 1.85; 95% CI:1.25, 2.74; I2 = 37%; k = 2).
Additionally, data from five studies (Keeley et al., 2007; Lin et al., 2011; Wu and Davis-Ajami (2014); Gerlach et al., 2017; Bhattacharjee et al., 2020) could not be synthesized through an MA. Only one study (Keeley et al., 2007) did not find differences in adherence rates between Caucasian, African-Americans and Hispanic patients. Among the remaining studies, two of them reported a higher likelihood of treatment adherence in the implementation phase among white/Caucasian individuals compared to African-American or non-white/non-Caucasian patients (Wu et al., 2012; Wu and Davis-Ajami, 2014). In one study (Bhattacharjee et al., 2020), white patients showed better adherence compared to non-white race and Hispanic patients. The remaining study (Lin et al., 2011) provided similar results, finding that Hispanic patients have lower levels of adherence compared to Caucasian or other ethnic patients. However, this study found no differences between Hispanics and African-Americans.
Five studies evaluated the impact of education in the implementation phase of adherence (Lin et al., 1995; Keeley et al., 2007; ten Doesschate et al., 2009; Yen et al., 2009; Gerlach et al., 2019).
Two of the studies reported sufficient data on the influence of education on the implementation phase of adherence between week 54 and 104 to be included in an MA (ten Doesschate et al., 2009; Gerlach et al., 2019). However, the analysis showed very high heterogeneity rates (I2 = 76%), and as such the pooled data are not presented.
All studies (Lin et al., 1995; Keeley et al., 2007; ten Doesschate et al., 2009; Yen et al., 2009; Gerlach et al., 2019) reported a non-significant effect of years of education on the implementation phase of adherence.
Four studies (ten Doesschate et al., 2009; Holma et al., 2010; Kales et al., 2016; Gerlach et al., 2019) analyzed the effect of civil status on adherence. Three of them (Holma et al., 2010; Kales et al., 2016; Gerlach et al., 2019) found a significant result. Individuals with spouse, partner or not living alone presented higher rates of adherence than individuals without spouse, partner or living alone. Due to disparities in follow-up, the results presented could not be effectively synthesized using MA.
Please refer to Supplementary Table S3 in the Supplementary Material to access the data from individual studies.
Four studies (Akincigil et al., 2007; Holvast et al., 2019; Nam-Ju and Yeon-Pyo, 2020) examined the influence of income on adherence during the implementation phase. However, an MA could not be conducted due to the wide variability in categorizing income levels. Despite this limitation, three of them (Akincigil et al., 2007; Holvast et al., 2019; Nam-Ju and Yeon-Pyo, 2020) consistently found that adherence was lower among individuals with lower incomes compared to those with higher incomes. The remaining study (Lin et al., 2011) reported a non-significant result.
MA could not be performed. Eight studies explored the impact of medical comorbidities on adherence (Akincigil et al., 2007; Keeley et al., 2007; Liu et al., 2011; Merrick et al., 2012; Wu et al., 2012; Kales et al., 2016; Gerlach et al., 2019; Bhattacharjee et al., 2020).
Three studies (Merrick et al., 2012; Kales et al., 2016; Gerlach et al., 2019) analyzed the impact of medical comorbidities using the Charlson Comorbidity Index (CCI) on adherence. The CCI is a medical tool for assessing both the number and severity of comorbid diseases, which helps to predict mortality (Charlson et al., 1987). Of the three studies, two (Kales et al., 2016; Gerlach et al., 2019) found that individuals with a CCI score greater than zero had a higher rate of adherence during the implementation phase in contrast to individuals with other CCI scores. However, the remaining study (Merrick et al., 2012) did not find significant differences in adherence between individuals with a CCI score of two and those with a CCI score between 0 and 1. Additionally, one study used the Elixhauser Comorbidity Index (Wu et al., 2012). The said study found higher levels of adherence in patients who scored 2 or more on the Elixhauser Comorbidity Index compared to those who scored lower. However, patients who scored 1 did not differ from those who scored 0.
Two studies analyzed the impact of comorbid chronic pain conditions (such as low back pain, migraines, fibromyalgia, or headaches) on treatment adherence and found significant differences. One study (Liu et al., 2011) indicated that individuals with headaches, low back pain, or fibromyalgia had a lower likelihood of treatment adherence compared to those without these conditions. In the other study (Akincigil et al., 2007), patients with headaches or migraines were less likely to be adherent at 16 weeks, although this difference was not observed at the 33-week follow-up.
One study (Bhattacharjee et al., 2020) reported that people with Parkinson’s disease had a slightly higher probability of treatment adherence compared to people without Parkinson’s, Additionally, individuals with cardiovascular disease and diabetes showed a lower probability of adherence compared to those without these health conditions at 16 weeks, but this effect was not observed at the 33-week follow-up (Akincigil et al., 2007).
The MA incorporated the findings from four studies with regard to anxiety comorbidity. Presenting this type of disorder simultaneously with depression, between weeks 12–16 and 33–39, did not influence the rates of adherence to pharmacological treatment for depression (OR12-16 = 1.02; 95% CI: 0.90, 1.15; I2 = 0%; k = 2; OR33-39 = 1.04; 95% CI: 0.87, 1.24; I2 = 0%; k = 2). However, after week 52, suffering from anxiety at the same time as depression increased adherence rates (OR = 1.50; 95% CI: 1.25, 1.81; I2 = 0%; k = 2).
Additional data related to psychiatric comorbidities from five studies could not be included in the MA. Three studies (Keeley et al., 2007; Lin et al., 2011; Gerlach et al., 2019) revealed that the presence of several psychiatric comorbidities (i.e., anxiety disorder, somatoform complaints, substance use or post-traumatic stress disorders) did not significantly impact the implementation process. Furthermore, one study (Chen et al., 2010) reported that patients with a comorbid substance use disorder had a lower probability of adherence at 12 weeks, but not at 39 weeks of follow-up. The last study (Liu et al., 2011) found results consistent with the ones mentioned earlier. The finding was that patients with alcohol related-disorders and the use or abuse of substances had worse adherence rates compared to those who do not suffer from them. Conversely, patients with hypersomnia had a higher likelihood of continuing to adhere to treatment. On the contrary, patients with anxiety or comorbid fibromyalgia had worse implementation rates.
Threes studies (Cohen et al., 2004; Donohue et al., 2004; Yen et al., 2009) investigated the impact of diagnostic subtype on treatment adherence and did not observe any significant differences.
A single study (Cohen et al., 2004) investigated the impact of previous episodes on adherence and did not observe any significant differences.
MA could not be performed. Four studies (Lin et al., 1995; Sirey et al., 2001; Cohen et al., 2004; Merrick et al., 2012) investigated the impact of severity on treatment implementation and did not observe any significant differences.
The results obtained relating to the predictors of adherence during the discontinuation phase (non-persistence) are described below.
The MA incorporated the findings from six studies (Goethe et al., 2007; Liu et al., 2010; 2011; Milea et al., 2010; Woolley et al., 2010; Vlahiotis et al., 2011).
The increase in age generated a slight decrease in discontinuation rates at 12 weeks (OR = 0.98; 95% CI: 0.97, 0.99; I2 = 0%; k = 2).
Between weeks 26–52, patients aged 25–40 (OR = 0.81; 95% CI: 0.72, 0.93; I2 = 55%; k = 2) and 56–64 (OR = 0.55; 95% CI: 0.44, 0.68; I2 = 83%; k = 2) presented lower rates of discontinuation of AD treatment compared to those aged 18–24.
At week 52, only patients aged 40–64 (vs. 18–39) maintained lower discontinuation rates (OR = 0.73; 95% CI: 0.64, 0.82; I2 = 73%; k = 2) compared to those aged 18–39.
Data from another eight studies could not be synthesized using MA. In five studies, no significant differences were found among different age groups (Keeley et al., 2000; 2007; Demyttenaere et al., 2001; Olfson et al., 2006; Noh et al., 2020). However, two studies (Ereshefsky et al., 2010; Wu et al., 2013) reported that there was a lower likelihood of treatment discontinuation among individuals older than 35 and 45 years compared to younger individuals. A similar result was found in another study that evaluated age as a continuous variable (Hung et al., 2011), where a greater age independently predicted a lower risk of early discontinuation. In contrast, one study (Hung et al., 2011) found the opposite effect, where older people were at a higher risk of discontinuation.
Please refer to Supplementary Table S5 in the Supplementary Material to access the data from individual studies.
The MA investigating the influence of sex on adherence during the discontinuation phase included findings from two studies (Olfson et al., 2006; Milea et al., 2010). Sex did not affect the discontinuation rates at 4 weeks (OR = 1.00; 95% CI: 0.98, 1.02; I2 = 0%; k = 2).
Another seven studies (Demyttenaere et al., 2001; Goethe et al., 2007; Keeley et al., 2007; Hung et al., 2011; Vlahiotis et al., 2011; Wu et al., 2013; Holvast et al., 2019) were not included in the MA. Among them, two studies (Goethe et al., 2007; Vlahiotis et al., 2011) consistently reported that men had a significantly higher risk of discontinuation than women. Milea et al. (2010) reported a similar result, although this was observed as only a trend. In contrast, one study (Wu et al., 2013) reported that men presented a significantly lower risk than women. The remaining studies found no significant impact of gender on discontinuation.
MA could not be performed. Three studies examined the impact of ethnicity on discontinuation (Keeley et al., 2000; Keeley et al., 2007; Olfson et al., 2006). Two of them did not observe any significant differences (Keeley et al., 2000;Keeley et al., 2007), while another study found that Hispanic patients had a higher rate of treatment discontinuation than non-Hispanic patients (Olfson et al., 2006).
Two of the three studies (Olfson et al., 2006; Woolley et al., 2010) provided sufficient data regarding the impact of educational level on discontinuation within 12 weeks to conduct an MA. However, the analysis revealed a high level of heterogeneity (I2 = 83), and as such pooled data are not presented.
One study reported a higher rate of treatment discontinuation among patients with less than 12 years of formal education. However, the remaining two studies (Keeley et al., 2007; Woolley et al., 2010) did not observe significant differences.
MA could not be performed. The civil status of the patients did not influence the discontinuation rates at 4 weeks (Olfson et al., 2006).
MA could not be performed. Two studies (Olfson et al., 2006; Holvast et al., 2019) investigated the impact of income level on discontinuation. Only Olfson et al. (2006) observed that individuals with a low income had a significantly higher rate of treatment discontinuation compared to those with a high income.
MA could not be performed. Six studies (Keeley et al., 2000; Keeley et al., 2007; ten Doesschate et al., 2009; Vlahiotis et al., 2011; Wu et al., 2013; Wu and Davis-Ajami (2014)) explored the impact of medical comorbidities on discontinuation and did not observe significant differences.
Three studies suggested that the presence of various medical comorbidities could actually lead to a decreased risk of discontinuation of AD treatment. For instance, one study (Noh et al., 2022) reported that a reduced likelihood of AD discontinuation was found in women with a higher obstetric comorbidity index or the presence of cardiovascular disease. Similarly, another investigation highlighted the impact of somatic comorbidities, including hypertension, lipid metabolic disorder, and diabetes, which were associated with a lower occurrence of treatment discontinuation (Milea et al., 2010). Furthermore, in one study (Hung et al., 2011), patients with migraines were less inclined to discontinue treatment when compared to those without migraine conditions.
The MA included data from three studies (Ereshefsky et al., 2010; Wu et al., 2013; Noh et al., 2022) concerning psychiatric comorbidities. Overall, the presence of a psychiatric comorbidity did not significantly affect adherence rates (HR = 0.99; 95% CI 0.87, 1.13; I2 = 93%; k = 3).
However, when examining specific comorbidities, it was found that patients with alcohol-related disorders presented worse adherence rates to AD treatment at 26 weeks (HR = 1.16; 95% CI: 1.08, 1.23; I2 = 0%; k = 2) (Ereshefsky et al., 2010; Wu et al., 2013). Conversely, the presence of sleep disorders did not influence adherence rates at 26 weeks (HR = 0.85; 95% CI: 0.76, 0.95; I2 = 88%; k = 2) (Wu et al., 2013; Noh et al., 2022), nor did substance abuse-related disorders (HR = 0.98; 95% CI: 0.87, 1.11; I2 = 0%; k = 2) (Wu et al., 2013; Noh et al., 2022).
Additional data relating to psychiatric comorbidities from nine studies could not be synthesized using MA. One study (Liu et al., 2011) reported similar findings to the previous ones, suggesting that patients with alcohol related-disorders and the use or abuse of substances had worse adherence rates compared to those without these conditions at 52 weeks. However, patients with hypersomnia were more likely to continue complying with treatment. Another study (Holvast et al., 2019) found that the presence of psychological comorbidity was not associated with discontinuation. However, sensitivity analysis for different types of ADs revealed an association between the psychological comorbidity and discontinuation of SSRIs.
Concerning anxiety comorbidity, there is some variation in the findings. In one study (Wu et al., 2013), patients with anxiety comorbidity were less likely to discontinue AD treatment at 26 weeks. Conversely, another study (Vlahiotis et al., 2011) suggested that anxiety disorders often led to increased discontinuation. However, two other studies (Goethe et al., 2007; Wu et al., 2012) did not find this association at 12 and 52 weeks.
Different studies reported that comorbidities such as panic/agoraphobia or post-traumatic stress disorder (Hung et al., 2011), or sleep disorder and anxiety/stress related disorder (Noh et al., 2022), were associated with reduced treatment discontinuation rates. However, the presence of a psychosomatic comorbidity was associated with an increased discontinuation rate (Milea et al., 2010).
Finally, two studies (Keeley et al., 2007; Noh et al., 2020) found that the presence of somatoform complaints, mood disorders, eating disorders or personality disorders did not significantly affect the AD discontinuation process.
Two studies (ten Doesschate et al., 2009; Wu and Davis-Ajami, 2014) investigated the impact of previous episodes on discontinuation and did not observe any significant differences.
MA could not be performed. Two studies (ten Doesschate et al., 2009; Hung et al., 2011) explored the relation between depression severity and discontinuation. A single study (Hung et al., 2011) found that patients with chronic depression were less likely to discontinue treatment. Conversely, another study (ten Doesschate et al., 2009) did not identify any significant differences.
Finally, with the data reported in the included studies, it was not possible to synthesize the relationship between cognitive impairment, and perceived health or health-related quality of life with adherence (for more information on the results obtained in the included studies see Supplementary Table S6).
The main objective of this SR was to evaluate the possible sociodemographic and clinical predictive factors that influence adherence to AD treatment in adult patients diagnosed with a depressive disorder.
The data obtained in this SR show worrying rates of adherence to pharmacological treatment in the three phases, initiation, implementation and discontinuation (Vrijens et al., 2012). Specifically, non-adherence rates in the first months of therapy exceed 80%, which places this problem in a more unfavorable scenario than those reported in previous studies, which reported values close to 50% (Sansone and Sansone, 2012). These high rates of non-adherence may be influenced by factors such as the side effects of medication, especially given that this occurs in the early weeks of AD treatment. This underscores the need for a professional approach concerning the experience of the disease and the treatment (feelings, ideas, function and expectations) to adequately manage the condition and improve therapeutic adherence. This is particularly important in scenarios where pharmacological therapy is the only viable option for the patient (Samalin et al., 2018; González de León et al., 2022).
In relation to the predictive factors, advanced age, was found to be a predictor of good adherence in both the implementation phase and in the discontinuation phase, which is consistent with the literature (Rivero-Santana et al., 2013; Holbrook et al., 2021). However, in the present SR, this effect was maintained over time in middle-aged people (35–65 years), while it was less evident in older people (>65 years). In the latter population group, the use of patient reminders or alerts could play an important role in reducing involuntary lack of adherence (Hamine et al., 2015; González de León et al., 2021). Additionally, it is important to consider the role of patient’s beliefs and preferences about medication at the start of treatment, as well as patient preferences about treatment, as they may be correlated with therapeutic efficacy and adherence, especially in younger patients (Horne et al., 2013; Kong et al., 2021).
In the present SR, it was observed that being female was associated with better adherence rates during the first weeks of treatment, but correlated with the risk of SSRIs non-initiation. However, as treatment time progresses, this association became less conclusive. Previous studies similarly reported a better adherence rate between female patients nevertheless, this finding could not be consistently confirmed due to many studies not yielding statistically significant results (Rivero-Santana et al., 2013).
On the other hand, white patients showed better levels of adherence compared to Afro-American or Hispanic patients, consistent with some previous literature (Rivero-Santana et al., 2013) that mainly pointed to the age and ethnicity of the patients as the most consistent factors influencing non-compliance with treatment. This finding contrasts with the results of the SR of Holbrook et al. (2021), where they did not consider ethnicity as a predictive factor. This controversial relationship may be mediated by confounders such as economic resources, educational level or healthcare access, as in other outcomes in depression (Finegan et al., 2018). Therefore, future studies designed to corroborate these results are needed.
Although having a low educational level has often been considered a potential risk factor for poor adherence, as people with less education may have more difficulty understanding treatment regimens, medical recommendations, or the nature of their disease; the educational level of the patients did not influence treatment adherence rates. This finding is consistent with previous studies (Burra et al., 2007; Rivero-Santana et al., 2013; Roca et al., 2013).
Another possible association, in line with previous research on chronic conditions, was found between marital or cohabitation status and medication adherence. Studies conducted on other chronic diseases have found a relationship between marital status and adherence, with a greater adherence in those people who were in a relationship (Trivedi et al., 2008; Wu et al., 2012).
Marital or cohabitation status may also be associated with medication adherence. Research on various chronic conditions has suggested that individuals in relationships tend to present better adherence (Trivedi et al., 2008; Wu et al., 2012).
Previous studies suggest that socioeconomically disadvantaged individuals, characterized by factors such as low income, unemployment, financial struggles, lack of homeownership, or limited formal education, have poorer prognoses regardless of the type of treatment they receive and the severity of depression (Buckman et al., 2022). In the present SR, low income appears to have a negative impact on both the initiation of SSRI treatment and adherence levels to AD therapy, and possibly on discontinuation rates, which could be influencing the poor progression of the disease.
Regarding psychiatric comorbidities, the findings in the present SR showed varied results. During the first weeks, the presence of anxiety disorders did not seem to influence adherence. However, over time, the absence of anxiety disorders was associated with better adherence rates. Consistent with previous research on chronic conditions (Grodensky et al., 2012), it appears that patients with comorbid depression and alcohol abuse disorder may present reduced adherence to treatment. Nevertheless, no significant results were found for sleep disorders and substance abuse-related disorders. These results highlight a potentially important gap in the evidence about the effect of psychiatric comorbidities on medication adherence.
On the other hand, patients with a higher medical comorbidity index score showed better adherence during the implementation phase. However, contrary to expectations, studies examining the role of comorbid chronic pain found lower adherence rates among patients with these conditions (Akincigil et al., 2007; Liu et al., 2011). Both of these studies reported a similar difference in the adherence ratio between patients with or without chronic pain of around 4%, although this was relatively small, it is significant. Non-adherence to prescribed analgesic medication in chronic pain is quite common, influenced by factors such as polymedication and concerns about pain medication, which are commonly associated with non-adherence in this condition (Timmerman et al., 2019). These aspects might also affect adherence to antidepressants. This finding emphasizes the need for further studies to draw more robust conclusions. Furthermore, it is necessary to understand how these findings translate into real clinical practice situations.
For individuals dealing with comorbid conditions, simplifying the medication regimen may prove beneficial. As seen in prior literature (Rivero-Santana et al., 2013), medical comorbidities have been shown to have significant associations with both positive and negative adherence outcomes in the studies examined here. Patients coping with multiple health conditions may develop a more profound understanding of medication management. However, when combined with other factors like limited education, or incomplete or unclear physician instructions, this can lead to a complex treatment regimen that complicates adherence. It is also important to address patients’ myths and beliefs with scientific information and explanations (Marasine and Sanki, 2021). This combined approach could help improve adherence in patients with comorbidities and contribute to better treatment outcomes.
The evidence in the present SR suggests that the severity of depression by itself does not significantly predict adherence, which is consistent with previous SR (Rivero-Santana et al., 2013). However, older patients experiencing severe and persistent depressive symptoms are more inclined to tend to perceive medication as a necessary treatment for their condition. Conversely, in younger patients with severe initial depression, the dropout rate from pharmacotherapy tends to be higher (Aikens et al., 2008). Data from databases usually lack essential information, such as disease severity and prior episode history, which is required to understand the disease. The loss of information derived from incomplete coding during the diagnosis process and its subsequent updating complicates the analysis of possible relationships between these factors and treatment adherence (Donohue et al., 2004). Hence, additional scientific evidence is needed to shed light on what is happening with the more purely clinical characteristics of these patients.
The findings here suggest that depression severity alone might not significantly predict adherence, which is consistent with previous systematic reviews (Rivero-Santana et al., 2013). Nevertheless, older individuals experiencing severe and persistent depressive symptoms are more inclined to view medication as a necessary treatment for their condition. Conversely, in younger individuals with severe initial depression, the dropout rate from pharmacotherapy tends to be higher (Aikens et al., 2008).
The study of all the potential predictive factors influencing the decision-making about starting (or not), maintaining (or not), and discontinuing (or not) the treatment is necessary to enhance the existing theoretical models and develop more precise and adjusted interventions for different subgroups of the population. The identification of these predictors of adherence holds significant value for primary care and mental health professionals in their everyday clinical practice. It enables them to identify patients who may be at a higher risk of non-adherence, allowing for the implementation of targeted interventions for these individuals. By doing so, it becomes possible to enhance clinical outcomes in the recovery process and optimize the utilization of public health resources efficiently. This proactive approach can ultimately lead to better patient outcomes and a more effective allocation of healthcare resources.
This SR has a series of strengths, namely, 1) it is the most extensive work to date in relation to the number of participants, which in addition to incorporating MA, 2) used a transparent and rigorous methodology according to the SR and MA standards, and 3) each of the steps is explained in detail, as well as providing all the necessary data to be able to replicate this SR.
With regard to the weaknesses of this study, the following should be mentioned: 1) despite conducting an exhaustive bibliographic search in the main databases of indexed journals, there may be studies not included in these databases that have therefore been left out of this SR, 2) only studies published in English and/or Spanish were taken into account, 3) a large number of the studies presented a high overall risk of bias, which limits the certainty of the evidence, 4) there was heterogeneity between the selected studies, especially in how and when adherence is assessed, and in the definition and categorization of the predictors, which, in some cases, has meant that it has not been possible to obtain an estimate of the effect of some of the predictive factors and, 5) despite ongoing consensus efforts, the considerable variability in defining adherence and its phases has posed a challenge to comparing studies.
Other limitations, mainly concern the low number of studies per predictor factor, are 6) the absence of a meta-regression analysis, 7) the lack of sensitivity analysis and the adherence measurement method in included studies. Adherence is a multifactorial phenomenon, and as such, it should ideally be evaluated from various perspectives. Relying solely on a single measurement method, whether objective or subjective, through the use of validated scales, might prove insufficient. In the future, studies should incorporate the gold standard—electronic monitoring—(Hess et al., 2006) and, when the reference standard is not used, two evaluation methods should be applied: one using objective measures and the other subjective measures of adherence (Sajatovic et al., 2010).
Finally, despite the efforts, the profile obtained, due to its restriction to unmodified predictors of adherence, is limited in its usefulness in clinical practice for effectively identifying a well-defined non-adherence patient profile.
According to the results obtained here, middle-aged, elderly and Caucasian participants have higher rates of adherence, although time determines whether these rates are maintained in older patients. Despite finding data that support age and ethnicity as predictors of pharmacological adherence, further studies of a higher methodological quality that can obtain more data, but, above all, that explore other possible factors that may influence adherence are recommended.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
TP-S: Conceptualization, Methodology, Writing–original draft, Writing–review and editing, Funding acquisition, Project administration. DI-V: Conceptualization, Methodology, Writing–original draft, Writing–review and editing. DH-G: Methodology, Writing–original draft, Writing–review and editing. YG-H: Methodology, Writing–original draft, Writing–review and editing. BG: Methodology, Writing–original draft, Writing–review and editing. AR-S: Conceptualization, Supervision, Writing–review and editing. IH–N: Conceptualization, Supervision, Writing–review and editing. FA: Conceptualization, Supervision, Writing–review and editing, Funding acquisition.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work has been carried out within the framework of a project financed by the Canary Islands Health Research Institute Foundation (FIISC) in the Call for Research, Development and Innovation Projects aimed at satisfying the health needs of the population of the Canary Islands and improving the sustainability and solvency of the Canary Health Service (SCS) (PIFIISC20_05).
The authors would like to thank Leticia Rodríguez for her guidance in developing the search strategy and Wenceslao Peñate for his revision of the final manuscript. We are also grateful to Patrick Dennis for English language editing support with the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2024.1327155/full#supplementary-material
Aikens, J. E., Nease, D. E., and Klinkman, M. S. (2008). Explaining patients’ beliefs about the necessity and harmfulness of antidepressants. Ann. Fam. Med. 6, 23–29. doi:10.1370/afm.759
Akincigil, A., Bowblis, J. R., Levin, C., Walkup, J. T., Jan, S., and Crystal, S. (2007). Adherence to antidepressant treatment among privately insured patients diagnosed with depression. Med. Care 45, 363–369. doi:10.1097/01.mlr.0000254574.23418.f6
Bhattacharjee, S., Lee, J. K., Vadiei, N., Patanwala, A. E., Malone, D. C., Knapp, S. M., et al. (2020). Extent and factors associated with adherence to antidepressant treatment during acute and continuation phase depression treatment among older adults with dementia and major depressive disorder. Neuropsychiatr. Treat. 16, 1433–1450. doi:10.2147/NDT.S241749
Buckman, J. E. J., Saunders, R., Stott, J., Cohen, Z. D., Arundell, L.-L., Eley, T. C., et al. (2022). Socioeconomic indicators of treatment prognosis for adults with depression: a systematic review and individual patient data meta-analysis. JAMA Psychiatry 79, 406–416. doi:10.1001/jamapsychiatry.2022.0100
Burra, T. A., Chen, E., McIntyre, R. S., Grace, S. L., Blackmore, E. R., and Stewart, D. E. (2007). Predictors of self-reported antidepressant adherence. Behav. Med. 32, 127–134. doi:10.3200/BMED.32.4.127-134
Cano-Vindel, A., José, M. S., Wood, C., Dongil-Collado, E., and Latorre, J. (2012). La depresión en Atención Primaria: prevalencia, diagnóstico y tratamiento [Depression in Primary Care: prevalence, Diagnosis and Treatment]. Papeles Psicólogo 33, 2–11.
Charlson, M. E., Pompei, P., Ales, K. L., and MacKenzie, C. R. (1987). A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40, 373–383. doi:10.1016/0021-9681(87)90171-8
Chen, S.-Y., Hansen, R. A., Gaynes, B. N., Farley, J. F., Morrissey, J. P., and Maciejewski, M. L. (2010). Guideline-concordant antidepressant use among patients with major depressive disorder. Gen. Hosp. Psychiatry 32, 360–367. doi:10.1016/j.genhosppsych.2010.03.007
Cohen, N. L., Ross, E. C., Bagby, R. M., Farvolden, P., and Kennedy, S. H. (2004). The 5-factor model of personality and antidepressant medication compliance. Can. J. Psychiatry Rev. Can. Psychiatr. 49, 106–113. doi:10.1177/070674370404900205
Demyttenaere, K., Enzlin, P., Dewe, W., Boulanger, B., De Bie, J., De Troyer, W., et al. (2001). Compliance with antidepressants in a primary care setting, 2: the influence of gender and type of impairment. J. Clin. Psychiatry 62, 34–37.
Donohue, J. M., Berndt, E. R., Rosenthal, M., Epstein, A. M., and Frank, R. G. (2004). Effects of pharmaceutical promotion on adherence to the treatment guidelines for depression. Med. Care 42, 1176–1185. doi:10.1097/00005650-200412000-00004
Ereshefsky, L., Saragoussi, D., Despiégel, N., Hansen, K., François, C., and Maman, K. (2010). The 6-month persistence on SSRIs and associated economic burden. J. Med. Econ. 13, 527–536. doi:10.3111/13696998.2010.511050
GBD 2019 Mental Disorders Collaborator (2022). Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 9, 137–150. doi:10.1016/S2215-0366(21)00395-3
Finegan, M., Firth, N., Wojnarowski, C., and Delgadillo, J. (2018). Associations between socioeconomic status and psychological therapy outcomes: A systematic review and meta-analysis. Depress Anxiety. 35, 560–573. doi:10.1002/da.22765
Gerlach, L. B., Chiang, C., and Kales, H. C. (2019). The start predicts the finish: factors associated with antidepressant nonadherence among older veterans during the acute and maintenance treatment phases. J. Clin. Psychiatry 80, 18m12476. doi:10.4088/JCP.18m12476
Gerlach, L. B., Kavanagh, J., Watkins, D., Chiang, C., Kim, H. M., and Kales, H. C. (2017). With a little help from my friends? racial and gender differences in the role of social support in later-life depression medication adherence. Int. Psychogeriatr. 29, 1485–1493. doi:10.1017/S104161021700076X
Goethe, J. W., Woolley, S. B., Cardoni, A. A., Woznicki, B. A., and Piez, D. A. (2007). Selective serotonin reuptake inhibitor discontinuation: side effects and other factors that influence medication adherence. J. Clin. Psychopharmacol. 27, 451–458. doi:10.1097/jcp.0b013e31815152a5
González de León, B., Abt-Sacks, A., Acosta Artiles, F. J., del Pino-Sedeño, T., Ramos-García, V., Rodríguez Álvarez, C., et al. (2022). Barriers and facilitating factors of adherence to antidepressant treatments: an exploratory qualitative study with patients and psychiatrists. Int. J. Environ. Res. Public. Health 19, 16788. doi:10.3390/ijerph192416788
González de León, B., León Salas, B., del Pino-Sedeño, T., Rodríguez-Álvarez, C., Bejarano-Quisoboni, D., and Trujillo-Martín, M. M. (2021). Aplicaciones móviles para mejorar la adherencia a la medicación: revisión y análisis de calidad. Aten. Primaria 53, 102095. doi:10.1016/j.aprim.2021.102095
Grodensky, C. A., Golin, C. E., Ochtera, R. D., and Turner, B. J. (2012). Systematic review: effect of alcohol intake on adherence to outpatient medication regimens for chronic diseases. J. Stud. Alcohol Drugs 73, 899–910. doi:10.15288/jsad.2012.73.899
Hamine, S., Gerth-Guyette, E., Faulx, D., Green, B. B., and Ginsburg, A. S. (2015). Impact of mHealth chronic disease management on treatment adherence and patient outcomes: a systematic review. J. Med. Internet Res. 17, e52. doi:10.2196/jmir.3951
Hess, L. M., Raebel, M. A., Conner, D. A., and Malone, D. C. (2006). Measurement of adherence in pharmacy administrative databases: a proposal for standard definitions and preferred measures. Ann. Pharmacother. 40, 1280–1288. doi:10.1345/aph.1H018
Higgins, J., Lasserson, T., Chandler, J., Tovey, D., and Churchill, R. (2016). Standards for the conduct and reporting of new Cochrane intervention reviews. London: Cochrane.
Ho, S. C., Chong, H. Y., Chaiyakunapruk, N., Tangiisuran, B., and Jacob, S. A. (2016). Clinical and economic impact of non-adherence to antidepressants in major depressive disorder: a systematic review. J. Affect. Disord. 193, 1–10. doi:10.1016/j.jad.2015.12.029
Holbrook, A. M., Wang, M., Lee, M., Chen, Z., Garcia, M., Nguyen, L., et al. (2021). Cost-related medication nonadherence in Canada: a systematic review of prevalence, predictors, and clinical impact. Syst. Rev. 10, 11. doi:10.1186/s13643-020-01558-5
Holma, I. A. K., Holma, K. M., Melartin, T. K., and Isometsä, E. T. (2010). Treatment attitudes and adherence of psychiatric patients with major depressive disorder: a five-year prospective study. J. Affect. Disord. 127, 102–112. doi:10.1016/j.jad.2010.04.022
Holvast, F., Voshaar, R. C. O., Wouters, H., Hek, K., Schellevis, F., Burger, H., et al. (2019). Non-adherence to antidepressants among older patients with depression: a longitudinal cohort study in primary care. Fam. Pract. 36, 12–20. doi:10.1093/fampra/cmy106
Horne, R., Chapman, S. C. E., Parham, R., Freemantle, N., Forbes, A., and Cooper, V. (2013). Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS ONE 8, e80633. doi:10.1371/journal.pone.0080633
Hung, C.-I., Wang, S.-J., Liu, C.-Y., Hsu, S.-C., and Yang, C.-H. (2011). Comorbidities and factors related to discontinuation of pharmacotherapy among outpatients with major depressive disorder. Compr. Psychiatry 52, 370–377. doi:10.1016/j.comppsych.2010.08.005
Jimmy, B., and Jose, J. (2011). Patient medication adherence: measures in daily practice. Oman Med. J. 26, 155–159. doi:10.5001/omj.2011.38
Kales, H. C., Kavanagh, J., Chiang, C., Kim, H. M., Bishop, T., Valenstein, M., et al. (2016). Predictors of antidepressant nonadherence among older veterans with depression. Psychiatr. Serv. 67, 728–734. doi:10.1176/appi.ps.201500120
Kales, H. C., Nease, D. E., Sirey, J. A., Zivin, K., Kim, H. M., Kavanagh, J., et al. (2013). Racial differences in adherence to antidepressant treatment in later life. Am. J. Geriatr. Psychiatry 21, 999–1009. doi:10.1016/j.jagp.2013.01.046
Keeley, R., Smith, M., and Miller, J. (2000). Somatoform symptoms and treatment nonadherence in depressed family medicine outpatients. Arch. Fam. Med. 9, 46–54. doi:10.1001/archfami.9.1.46
Keeley, R. D., Davidson, A. J., Crane, L. A., Matthews, B., and Pace, W. (2007). An association between negatively biased response to neutral stimuli and antidepressant nonadherence. J. Psychosom. Res. 62, 535–544. doi:10.1016/j.jpsychores.2006.12.006
Kogut, S., Quilliam, B. J., Marcoux, R., McQuade, W., Wojciechowski, C., Wentworth, C., et al. (2016). Persistence with newly initiated antidepressant medication in Rhode Island medicaid: analysis and insights for promoting patient adherence. R. Med. J. 99, 28–32.
Kok, R. M., and Reynolds, C. F. (2017). Management of depression in older adults: A review. J. Am. Med. Assoc. 317, 2114–2122. doi:10.1001/jama.2017.5706
Kong, F.-Z., Ji, C.-F., Du, X.-D., Logan, R., Zhao, H.-Y., Wu, G.-H., et al. (2021). Baseline beliefs about medication are associated with outcomes of antidepressants in inpatients with first-diagnosed depression under supervised therapeutic compliance. Aging 13, 21400–21407. doi:10.18632/aging.203477
Lin, E. H., Von Korff, M., Katon, W., Bush, T., Simon, G. E., Walker, E., et al. (1995). The role of the primary care physician in patients’ adherence to antidepressant therapy. Med. Care 33, 67–74. doi:10.1097/00005650-199501000-00006
Lin, H.-C., Erickson, S. R., and Balkrishnan, R. (2011). Antidepressant utilization, adherence, and health care spending in the United States: the case of MDD patients 2000-2007. Health Outcomes Res. Med. 2, e79–e89. doi:10.1016/j.ehrm.2011.06.003
Liu, X., Chen, Y., and Faries, D. E. (2011). Adherence and persistence with branded antidepressants and generic SSRIs among managed care patients with major depressive disorder. Clin. Outcomes Res. 3, 63–72. doi:10.2147/CEOR.S17846
Liu, X., Gelwicks, S., Faries, D. E., and Able, S. L. (2010). Initial duloxetine prescription dose and treatment adherence and persistence in patients with major depressive disorder. Int. Clin. Psychopharmacol. 25, 315–322. doi:10.1097/YIC.0b013e32833db42e
Marasine, N. R., and Sanki, S. (2021). Factors associated with antidepressant medication non-adherence. Turk. J. Pharm. Sci. 18, 242–249. doi:10.4274/tjps.galenos.2020.49799
McGuinness, L. A., and Higgins, J. P. T. (2020). Risk-of-bias VISualization (robvis): an R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 12, 55–61. doi:10.1002/jrsm.1411
McLaughlin, T., Hogue, S. L., and Stang, P. E. (2007). Once-daily bupropion associated with improved patient adherence compared with twice-daily bupropion in treatment of depression. Am. J. Ther. 14, 221–225. doi:10.1097/01.mjt.0000208273.80496.3f
Merrick, E. L., Hodgkin, D., Panas, L., Soumerai, S. B., and Ritter, G. (2012). Is customization in antidepressant prescribing associated with acute-phase treatment adherence? antidepressant treatment customization. J. Pharm. Health Serv. Res. 3, 11–16. doi:10.1111/j.1759-8893.2011.00068.x
Milea, D., Guelfucci, F., Bent-Ennakhil, N., Toumi, M., and Auray, J.-P. (2010). Antidepressant monotherapy: a claims database analysis of treatment changes and treatment duration. Clin. Ther. 32, 2057–2072. doi:10.1016/j.clinthera.2010.11.011
Nam-Ju, J., and Yeon-Pyo, H. (2020). Effect of income level on adherence to antidepressant treatment in first onset depression outpatients. PLoS ONE 15, e0238623. doi:10.1371/journal.pone.0238623
NICE (2022). Depression in adults: treatment and management. NICE guideline [NG222]. London: National Institute for Health and Care Excellence. Available at: http://www.ncbi.nlm.nih.gov/books/NBK583074/.
Noh, Y., Choe, S.-A., Kim, W. J., and Shin, J.-Y. (2022). Discontinuation and re-initiation of antidepressants during pregnancy: a nationwide cohort study. J. Affect. Disord. 298, 500–507. doi:10.1016/j.jad.2021.10.069
Noh, Y., Choe, S.-A., and Shin, J.-Y. (2020). Discontinuation and reinitiation of antidepressants during pregnancy in South Korea, 2013-2017. Pharmacoepidemiol Drug Saf. 29, 540–541. doi:10.1002/pds.5114
Nübel, J., Guhn, A., Müllender, S., Le, H. D., Cohrdes, C., and Köhler, S. (2020). Persistent depressive disorder across the adult lifespan: results from clinical and population-based surveys in Germany. BMC Psychiatry 20, 58. doi:10.1186/s12888-020-2460-5
Nyaga, V. N., Arbyn, M., and Aerts, M. (2014). Metaprop: a Stata command to perform meta-analysis of binomial data. Arch. Public Health Arch. Belg. Sante Publique 72, 39. doi:10.1186/2049-3258-72-39
Olfson, M., Marcus, S. C., Tedeschi, M., and Wan, G. J. (2006). Continuity of antidepressant treatment for adults with depression in the United States. Am. J. Psychiatry 163, 101–108. doi:10.1176/appi.ajp.163.1.101
Ouzzani, M., Hammady, H., Fedorowicz, Z., and Elmagarmid, A. (2016). Rayyan—a web and mobile app for systematic reviews. Syst. Rev. 5, 210. doi:10.1186/s13643-016-0384-4
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71. doi:10.1136/bmj.n71
Pagès-Puigdemont, N., and Valverde-Merino, M. I. (2018). Adherencia terapéutica: factores modificadores y estrategias de mejora. Ars Pharm. Internet 59, 251–258. doi:10.30827/ars.v59i4.7357
Párraga Martínez, I., López-Torres Hidalgo, J., Del Campo Del Campo, J. M., Villena Ferrer, A., Morena Rayo, S., Escobar Rabadán, F., et al. (2014). Adherence to patients antidepressant treatment and the factors associated of non-compiance. Seguim. Adherencia Al Trat. Antidepresivo En. Pacientes Que Inician Su Consumo 46, 357–366. doi:10.1016/j.aprim.2013.11.003
Rivera, M., Porras-Segovia, A., Rovira, P., Molina, E., Gutiérrez, B., and Cervilla, J. (2019). Associations of major depressive disorder with chronic physical conditions, obesity and medication use: results from the PISMA-ep study. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 60, 20–27. doi:10.1016/j.eurpsy.2019.04.008
Rivero-Santana, A., Perestelo-Perez, L., Pérez-Ramos, J., Serrano-Aguilar, P., and De Las Cuevas, C. (2013). Sociodemographic and clinical predictors of compliance with antidepressants for depressive disorders: systematic review of observational studies. Patient prefer. Adherence 7, 151–169. doi:10.2147/PPA.S39382
ROBINS-E Development Group, Higgins, J., Morgan, R., Roney, A., Taylor, K., Thayer, K., et al. (2023). Risk of bias in non-randomized studies - of exposure (ROBINS-E). Launch version, 20 june 2023. Available at: https://www.riskofbias.info/welcome/robins-e-tool.
Roca, A., Imaz, M. L., Torres, A., Plaza, A., Subira, S., Valdes, M., et al. (2013). Unplanned pregnancy and discontinuation of SSRIs in pregnant women with previously treated affective disorder. J. Affect. Disord. 150, 807–813. doi:10.1016/j.jad.2013.02.040
Sajatovic, M., Velligan, D. I., Weiden, P. J., Valenstein, M. A., and Ogedegbe, G. (2010). Measurement of psychiatric treatment adherence. J. Psychosom. Res. 69, 591–599. doi:10.1016/j.jpsychores.2009.05.007
Saldaña, A. T., Sánchez, Y. O., Suárez, H. M., Corrales, Y. N. F., and Ballester, D. P. (2019). Factors associated with adherence to treatment in patients with depression. Mul. Med. 23, 1–10.
Samalin, L., Genty, J.-B., Boyer, L., Lopez-Castroman, J., Abbar, M., and Llorca, P.-M. (2018). Shared decision-making: a systematic review focusing on mood disorders. Curr. Psychiatry Rep. 20, 23. doi:10.1007/s11920-018-0892-0
Sansone, R. A., and Sansone, L. A. (2012). Antidepressant adherence: are patients taking their medications? Innov. Clin. Neurosci. 9, 41–46.
Santomauro, D. F., Mantilla Herrera, A. M., Shadid, J., Zheng, P., Ashbaugh, C., Pigott, D. M., et al. (2021). Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 398, 1700–1712. doi:10.1016/S0140-6736(21)02143-7
Sheehan, D. V., Keene, M. S., Eaddy, M., Krulewicz, S., Kraus, J. E., and Carpenter, D. J. (2008). Differences in medication adherence and healthcare resource utilization patterns: older versus newer antidepressant agents in patients with depression and/or anxiety disorders. CNS Drugs 22, 963–973. doi:10.2165/00023210-200822110-00005
Shin, G., Jang, B., Bae, G., Jeon, H.-L., and Bae, S. (2022). The impact of payment scheme changes on medication adherence and persistence of patients diagnosed with depression in Korea. Int. J. Environ. Res. Public. Health 19, 11100. doi:10.3390/ijerph191711100
Sirey, J. A., Bruce, M. L., Alexopoulos, G. S., Perlick, D. A., Friedman, S. J., and Meyers, B. S. (2001). Stigma as a barrier to recovery: perceived stigma and patient-rated severity of illness as predictors of antidepressant drug adherence. Psychiatr. Serv. Wash. D.C. 52, 1615–1620. doi:10.1176/appi.ps.52.12.1615
Stang, P., Suppapanaya, N., Hogue, S. L., Park, D., and Rigney, U. (2007). Persistence with once-daily versus twice-daily bupropion for the treatment of depression in a large managed-care population. Am. J. Ther. 14, 241–246. doi:10.1097/MJT.0b013e31802b59e4
ten Doesschate, M. C., Bockting, C. L. H., Koeter, M. W. J., and Schene, A. H. (2009). Predictors of nonadherence to continuation and maintenance antidepressant medication in patients with remitted recurrent depression. J. Clin. Psychiatry 70, 63–69. doi:10.4088/jcp.08m04119
Timmerman, L., Stronks, D. L., and Huygen, F. J. (2019). The relation between patients’ beliefs about pain medication, medication adherence, and treatment outcome in chronic pain patients: a prospective study. Clin. J. Pain 35, 941–947. doi:10.1097/AJP.0000000000000760
Trivedi, R. B., Ayotte, B., Edelman, D., and Bosworth, H. B. (2008). The association of emotional well-being and marital status with treatment adherence among patients with hypertension. J. Behav. Med. 31, 489–497. doi:10.1007/s10865-008-9173-4
Vlahiotis, A., Devine, S. T., Eichholz, J., and Kautzner, A. (2011). Discontinuation rates and health care costs in adult patients starting generic versus brand SSRI or SNRI antidepressants in commercial health plans. J. Manag. Care Pharm. 17, 123–132. doi:10.18553/jmcp.2011.17.2.123
Vrijens, B., De Geest, S., Hughes, D. A., Przemyslaw, K., Demonceau, J., Ruppar, T., et al. (2012). A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 73, 691–705. doi:10.1111/j.1365-2125.2012.04167.x
Wolff, J., Reißner, P., Hefner, G., Normann, C., Kaier, K., Binder, H., et al. (2021). Pharmacotherapy, drug-drug interactions and potentially inappropriate medication in depressive disorders. PloS One 16, e0255192. doi:10.1371/journal.pone.0255192
Woolley, S. B., Fredman, L., Goethe, J. W., Lincoln, A. K., and Heeren, T. (2010). Hospital patients’ perceptions during treatment and early discontinuation of serotonin selective reuptake inhibitor antidepressants. J. Clin. Psychopharmacol. 30, 716–719. doi:10.1097/jcp.0b013e3181fc343b
World Health Organization (2004). Adherence to long-term therapies evidence for ActionWorld health organization (WHO). 2003, 216 pages [English]. ISBN 92 4 154599 2. Ann. Saudi Med. 24, 221–222. doi:10.5144/0256-4947.2004.221
World Health Organization (2017). Depresión y otros trastornos mentales comunes. Estimaciones sanitarias mundiales. Organ. Mund. Salud 2017, 2–22.
Wu, C.-S., Shau, W.-Y., Chan, H.-Y., and Lai, M.-S. (2013). Persistence of antidepressant treatment for depressive disorder in Taiwan. Gen. Hosp. Psychiatry 35, 279–285. doi:10.1016/j.genhosppsych.2012.12.003
Wu, J., and Davis-Ajami, M. L. (2014). Antidepressant treatment persistence in low-income, insured pregnant women. J. Manag. Care Spec. Pharm. 20, 631–637. doi:10.18553/jmcp.2014.20.6.631
Wu, J., Sykes, L., Keiser, S., and Davis-Ajami, M. L. (2012). PMH34 persistence in use of antidepressants in pregnant women enrolled in medicaid in the United States. Value Health 15, A340. doi:10.1016/j.jval.2012.08.824
Yau, W.-Y., Chan, M.-C., Wing, Y.-K., Lam, H.-B., Lin, W., Lam, S.-P., et al. (2014). Noncontinuous use of antidepressant in adults with major depressive disorders - a retrospective cohort study. Brain Behav. 4, 390–397. doi:10.1002/brb3.224
Keywords: adherence, antidepressants, depression, depressive disorder, sociodemographic predictors, clinical predictors, systematic review, meta-analysis
Citation: Del Pino-Sedeño T, Infante-Ventura D, Hernández-González D, González-Hernández Y, González de León B, Rivero-Santana A, Hurtado I and Acosta Artiles FJ (2024) Sociodemographic and clinical predictors of adherence to antidepressants in depressive disorders: a systematic review with a meta-analysis. Front. Pharmacol. 15:1327155. doi: 10.3389/fphar.2024.1327155
Received: 24 October 2023; Accepted: 03 January 2024;
Published: 22 January 2024.
Edited by:
Maria Teresa Herdeiro, University of Aveiro, PortugalCopyright © 2024 Del Pino-Sedeño, Infante-Ventura, Hernández-González, González-Hernández, González de León, Rivero-Santana, Hurtado and Acosta Artiles. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diego Infante-Ventura, ZGllZ28uaW5mYW50ZXZlbnR1cmFAc2VzY3MuZXM=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.