
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 06 March 2024
Sec. Pharmacoepidemiology
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1107185
 Alison Evans1,2*†
Alison Evans1,2*† Debabrata Roy1,2†
Debabrata Roy1,2† Sandeep Dhanda1,2
Sandeep Dhanda1,2 Samantha Lane1,2
Samantha Lane1,2 Graça Coutinho3Anuradha Kulasekaran3
Graça Coutinho3Anuradha Kulasekaran3 David Miller-Shakesby4
David Miller-Shakesby4 Nagalakshmi Ramamoorthi4Saad Shakir1,2
Nagalakshmi Ramamoorthi4Saad Shakir1,2Background: Flurbiprofen 8.75 mg lozenges and oromucosal sprays are used for symptomatic relief of sore throat in patients aged 12 years and over. The documented adverse events of flurbiprofen use include those related to its pharmacological actions, namely, increased risk of haemorrhagic events, however other adverse events (such as nephrotoxicity and cardiac failure) have been known to occur. The likelihood of occurrence of adverse events increases when flurbiprofen is used concomitantly with some other medications. Therefore, the objective of this systematic review was to collate the current evidence on adverse events which occur with flurbiprofen 8.75 mg dose (any formulation), in particular as a result of interaction with other medicinal products, with a focus on non-haemorrhagic events.
Methods: Systematic searches of the literature were conducted to identify literature on any formulation of flurbiprofen 8.75 mg up to the date of the electronic database search (data lock: 28 April 2020). Publications were screened to identify studies reporting non-haemorrhagic adverse events with flurbiprofen 8.75 mg and/or non-haemorrhagic adverse events in the comparator arm. Data extraction was performed for eligible studies according to pre-defined criteria and summarised in narratives, tables and figures. Risk of bias and certainty of evidence assessments were planned for each included study where results relating to the primary objective of the systematic review were available.
Results: Of 1,528 publications identified by systematic literature searches, 26 met the inclusion criteria and were included in this review. None of these 26 studies contained information on non-haemorrhagic adverse events occurring as a result of a drug-drug interaction (interaction with concomitant medication used with flurbiprofen 8.75 mg), as per the primary objective and secondary objectives of the systematic review.
Conclusion: Results from this systematic review on the risk of non-haemorrhagic events did not provide evidence for these events occurring as a result of interaction with other medicinal products. Additional appropriately designed studies would be required to confirm whether these findings suggest a true absence of risk or limitations in reporting.
Flurbiprofen is a non-steroidal anti-inflammatory drug (NSAID) which is used widely for its analgesic effect. Flurbiprofen is available as a tablet for treatment of musculoskeletal pain (including arthritis and osteoarthritis) and for the relief of mild to moderate pain including dental and post-operative pain (Reckitt Benckiser Healthcare UK Ltd, 2016). When applied to the pharynx, the local and systemic effects of flurbiprofen provide symptomatic relief of sore throat; this led to flurbiprofen 8.75 mg being manufactured in different formats, such as lozenge and spray (Reckitt Benckiser Healthcare UK Ltd, 2016). A single dose of flurbiprofen 8.75 mg (lozenge or oromucosal spray) has been demonstrated to provide relief for sore throat, through a significant reduction in pain intensity, difficulty swallowing, and sensations associated with swelling of the throat (Reckitt Benckiser Healthcare UK Ltd, 2016; Reckitt Benckiser Healthcare UK Ltd, 2018).
Flurbiprofen lozenge was first licensed in the European Union (EU) in 2006 for the short-term symptomatic relief of sore throat in adults and children over the age of 12 years. The oromucosal spray is licensed for use in adults aged 18 years and over (Reckitt Benckiser Healthcare UK Ltd, 2016; Reckitt Benckiser Healthcare UK Ltd, 2018).
A well-documented adverse event related to NSAID use is haemorrhage. NSAIDs, including flurbiprofen, inhibit the cyclooxygenase (COX) enzyme, specifically the COX-1 enzyme which is involved in gastroprotection and platelet aggregation for blood clot formation (Rao and Knaus, 2008; Moore et al., 2015). Consequently, the inhibition of COX-1 can result in an increase in the risk of bleeding, primarily gastrointestinal (GI) bleeding.
In addition to rare haemorrhagic events, a range of other adverse events (excluding haemorrhagic) are listed in the summary of product characteristics (SmPC); in many instances, these adverse events are a result of drug-drug interactions (DDIs) between flurbiprofen and other medicinal products. DDIs are known to occur between flurbiprofen and other NSAIDs, antihypertensive drugs, and cardiac glycosides which can result in adverse events such as nephrotoxicity, GI ulceration, and cardiac events (Reckitt Benckiser Healthcare UK Ltd, 2016). Furthermore, flurbiprofen may alter serum levels of concomitant medications resulting in the potential risk of increased toxicity or altered effectiveness of the medication (Reckitt Benckiser Healthcare UK Ltd, 2016). Examples of such medications are listed in the SmPC and include lithium and phenytoin (Reckitt Benckiser Healthcare UK Ltd, 2016). Thus, it is important to consider usage of concomitant medication in the evaluation of any potential risk of adverse events occurring with flurbiprofen (Reckitt Benckiser Healthcare UK Ltd, 2016).
The objective of the systematic review was to collate the current evidence on adverse events which occur with flurbiprofen 8.75 mg dose (any formulation), in particular as a result of interaction with other medicinal products. The systematic review was conducted in two parts according to event type: haemorrhagic and non-haemorrhagic adverse events. The results focusing on haemorrhagic events have been previously published (Dhanda et al., 2021). This paper focuses on non-haemorrhagic adverse events that occur in patients taking flurbiprofen 8.75 mg dose (any formulation).
The primary objective of this part of the systematic review was to identify the frequency of all non-haemorrhagic adverse events occurring as a result of concomitant use of flurbiprofen 8.75 mg dose (any formulation) with other medicinal products (i.e., DDIs). Secondary objectives included describing the nature of the drug interactions (i.e., class of drug interacting with flurbiprofen 8.75 mg), the severity of all non-haemorrhagic adverse events, and comparing the occurrence of non-haemorrhagic adverse events with flurbiprofen 8.75 mg dose (any formulation) in combination with other medicinal products to comparator arms (e.g., other NSAIDs) of studies where a comparator group is available.
The following relevant study designs were included: clinical trials (randomised and non-randomised, blinded and non-blinded), cohort studies (prospective and retrospective), case-control studies, cross sectional studies, case series and case reports.
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and the inclusion criteria were in line with the PICOS (Participants, Interventions, Comparators, Outcomes, and Study design) categories (Supplementary Material: Inclusion criteria) (Liberati et al., 2009; Page et al., 2021).
Studies in languages other than English, studies only specifying haemorrhagic events, pre-clinical studies, reviews (although references from any appropriate reviews were checked for any other papers that were eligible for inclusion), conference abstracts.
Systematic searches of the literature were conducted using methods previously described (Dhanda et al., 2021). Briefly, PubMed/MEDLINE, Embase, The Cochrane Library, Web of Science, ClinicalTrials.gov (http://clinicaltrials.gov), and EU Clinical Trials Register (https://www.clinicaltrialsregister.eu/ctr) were searched up to 28 April 2020 to identify literature on flurbiprofen 8.75 mg (any formulation). No restriction on dates or coverage were applied.
The following search strategy was used where possible:
Search concept 1:
‘Flurbiprofen (including all synonyms for this concept)’
AND.
Search concept 2:
‘Lozenge OR oromucosal spray (including all synonyms for these concepts, e.g., spray, buccal, oromucosal) OR 8.75’.
A manual search of reference lists from included literature was conducted to identify additional research not picked up in the initial search. Further searches were conducted for case reports in the publicly available EudraVigilance database and the European Medicines Agency (EMA) website.
Full details of the search strategy is included in the Supplementary Material: Search Strategy.
In addition, in order to include the most recent data for this publication, a literature review was conducted using the same search criteria to cover the period between 29 April 2020 to 14 February 2023.
Following de-duplication of studies identified during the electronic search, the resulting studies were reviewed independently by two reviewers. Any discrepancies were adjudicated by a third reviewer where necessary. Reasons for exclusion were recorded. References were managed in EndNote (X7.8) (apart from studies identified via ClinicalTrials.gov and EU Clinical Trials, for which export to EndNote was not possible).
For eligible studies, data was extracted independently by the two reviewers into a data extraction form (Table 1). Where data was not available, this was recorded as ‘not specified’.
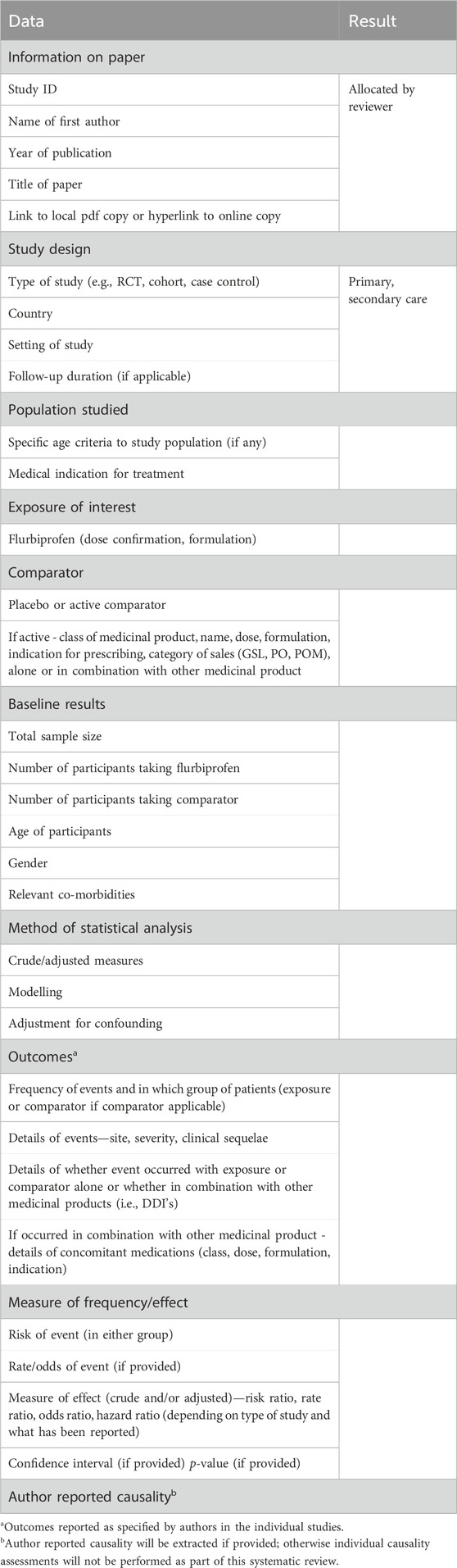
TABLE 1. Data items for extraction.
It was planned that each included study would be assessed for risk of bias and certainty of evidence where results relating to the primary objective of the systematic review were available. The aim was to use the Cochrane Risk-of-Bias (RoB2) tool and the Risk Of Bias In Non-randomised Studies–of Interventions (ROBINS-I) tool to assess risk of bias in the results of randomised trials and non-randomised studies, respectively (Sterne et al., 2016; Sterne et al., 2019), according to the guidelines outlined in the Cochrane Handbook (Higgins and Thomas, 2019), and Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework to conduct certainty of evidence assessments (Balshem et al., 2011).
Results are summarised in narratives, tables and figures. Treatments and outcomes reported in individual studies are presented as specified by the authors. An attempt was made to calculate measures of frequency (e.g., risk) in studies where only counts were specified (where the appropriate numerator and denominator information was provided).
In total, 1,528 publications were identified by the search strategy across the individual electronic databases utilised (Figure 1). After de-duplication, 1,093 publications were screened for possible eligibility; 1,038 publications were deemed ineligible and were excluded at this stage (Figure 1). Further screening of the remaining 55 publications determined an additional 29 publications did not meet the eligibility criteria, and thus were excluded. Reason for exclusion have been listed in Figure 1.
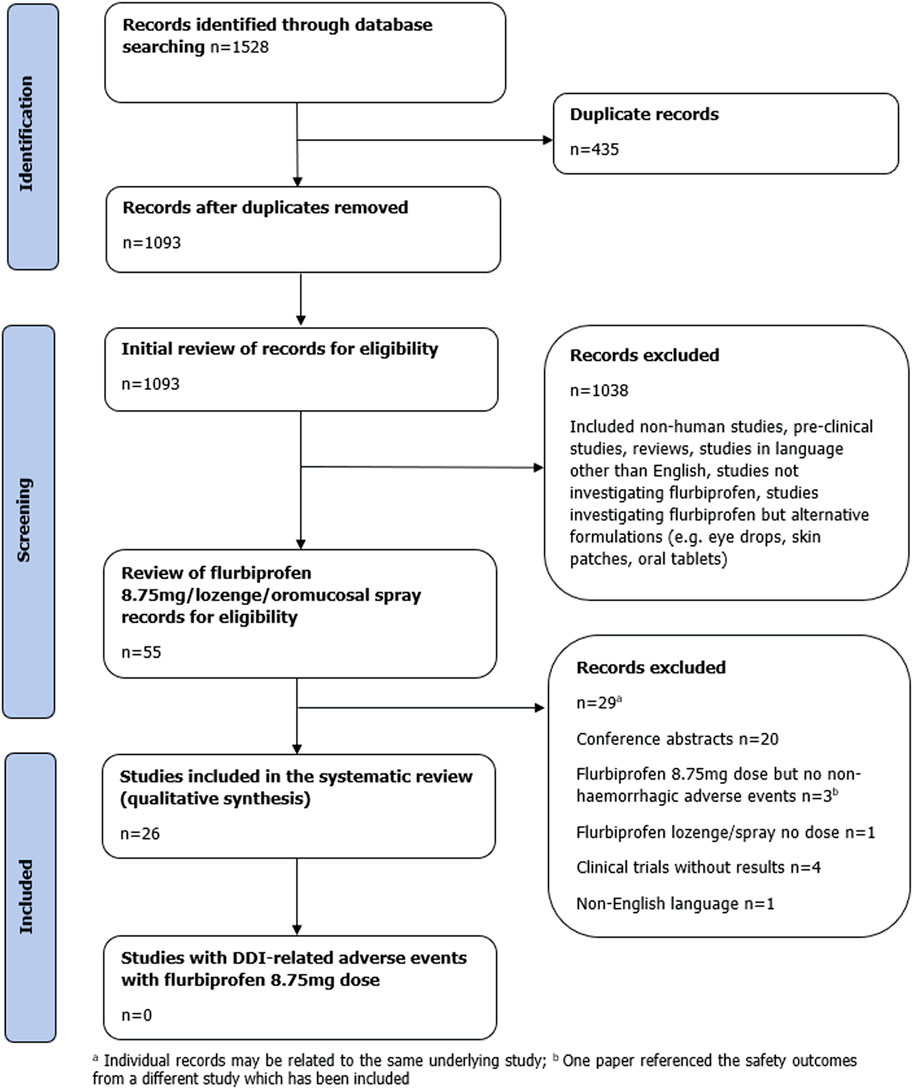
FIGURE 1. Flow diagram of study selection.
Twenty-six publications met the inclusion criteria and were included in the final analysis. Of these, 23 studies were randomised controlled trials (RCTs), and three were case reports.
No additional studies were identified in the EMA database of case reports. Furthermore, it was not possible to identify relevant cases in EudraVigilance, due to lack of detail on formulation and/or dose of flurbiprofen. No additional relevant publications were identified through the manual search of reference lists. Four publications were identified using the initial search strategy which examined low doses of flurbiprofen (other than 8.75 mg); however these did not meet inclusion criteria and so were excluded (Heasman et al., 1989; Schachtel et al., 2002; Dionne et al., 2004; Cebi, 2020).
No adverse events resulting from DDIs were identified in the 26 studies included in this study, therefore the objectives could not be investigated further. The results of the 26 studies have been summarised to describe the reported non-haemorrhagic adverse events. Of the 26 studies, 14 studies detailed at least one non-haemorrhagic AE which the authors considered was possibly or probably treatment related (Table 2). It was not specified whether adverse events in the other 12 studies were related to flurbiprofen treatment (Supplementary Material: Table 1).
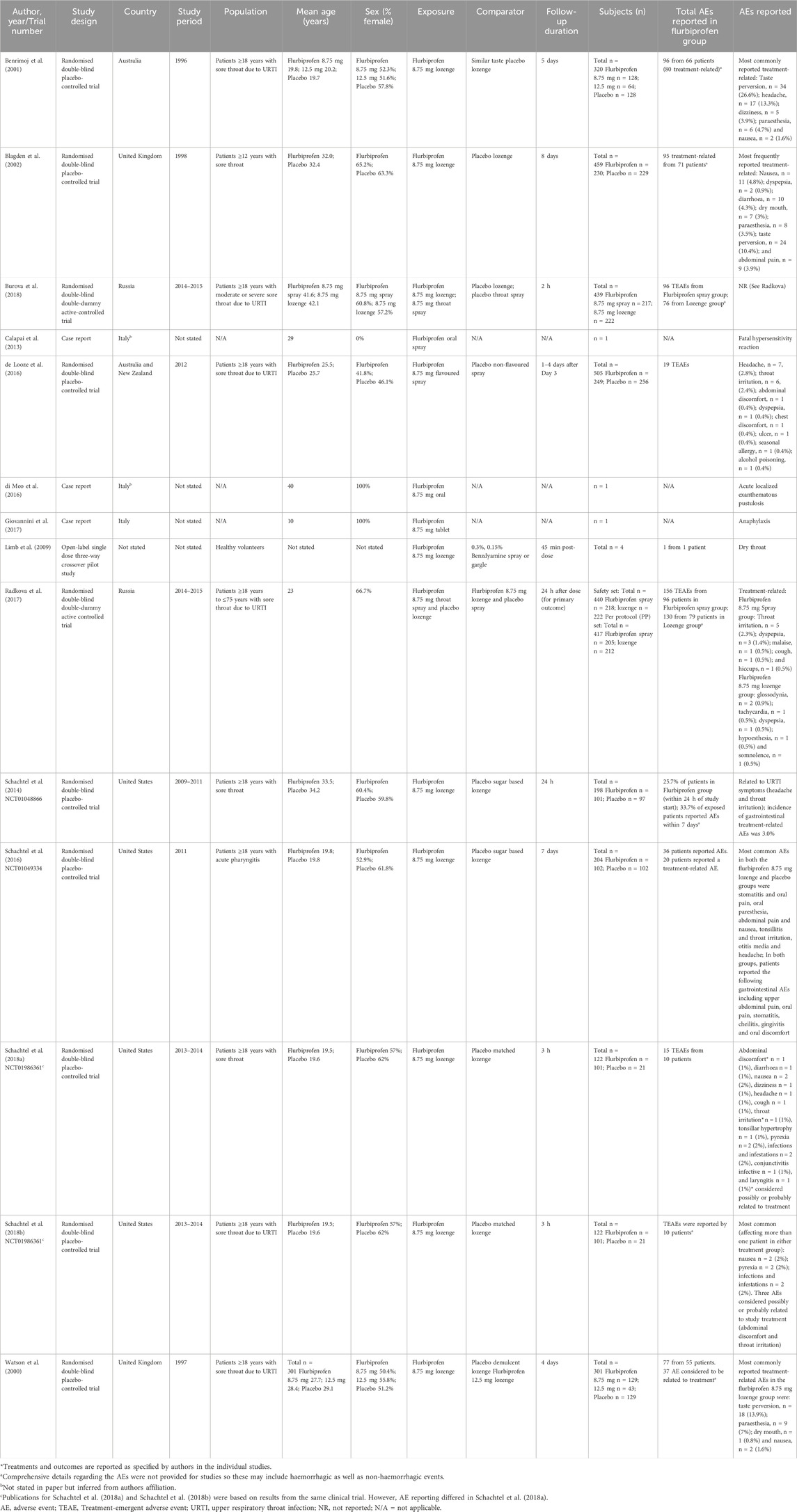
TABLE 2. Summary of studies reporting treatment-related non-haemorrhagic events with flurbiprofen 8.75 mg*.
Overall, across the 26 studies, the adverse events stated to be treatment-related with flurbiprofen 8.75 mg were taste perversion, paraesthesia, headache, dizziness, nausea, dyspepsia, diarrhoea, dry mouth, dry throat, abdominal pain, abdominal discomfort, dry nipping throat, throat irritation, cough, hiccups, glossodynia, hypoesthesia, somnolence, malaise, tachycardia and gastrointestinal adverse events (reported in RCTs) and anaphylaxis, fatal hypersensitivity and acute localised exanthematous pustulosis (reported in case reports) (Table 2).
Adverse events related to DDIs were not reported in any of the studies identified. Consequently, results relating to the primary objective of the systematic review were not available and thus these assessments for each individual study were not conducted.
The primary objective of this systematic review was to identify the frequency of all non-haemorrhagic events occurring as a result of concomitant use of flurbiprofen 8.75 mg dose with other medicinal products (i.e., DDIs). Secondary objectives included describing the nature of the drug interactions, the severity of the non-haemorrhagic event(s) and comparing frequencies of non-haemorrhagic events following exposure to flurbiprofen 8.75 mg in combination with other medicinal products, with the frequency of such events in a comparator group, where available. No adverse events resulting from DDIs were identified in the 26 studies included in this study, therefore the objectives could not be investigated further.
Amongst the 26 studies included in this systematic review, there were 21 distinct treatment-related adverse events reported (Table 2). With the exception of malaise and tachycardia, these treatment-related adverse events are in keeping with known adverse events listed in the SmPC for both flurbiprofen 8.75 mg lozenge and spray formulations (Reckitt Benckiser Healthcare UK Ltd, 2016; Reckitt Benckiser Healthcare UK Ltd, 2018). Tachycardia was the only cardiovascular treatment-related adverse event reported. Three case reports were included for consideration in the review, describing a fatal hypersensitivity reaction to oral flurbiprofen spray (Calapai et al., 2013), anaphylaxis to an oral 8.75 mg flurbiprofen tablet (Giovannini et al., 2017), and acute localised exanthematous pustulosis to oral 8.75 mg flurbiprofen (di Meo et al., 2016).
To identify additional adverse events resulting from possible DDIs when flurbiprofen was used concomitantly with another medication, a review of EudraVigilance data was conducted. However, it was not possible to determine dose and/or formulation of flurbiprofen in each reported event, therefore it was not possible to conduct further analyses using spontaneously reported data from this source. Further searches of EMA case reports were carried out, however no additional cases were identified.
Importantly, 23 of the 26 included studies were RCTs. RCTs are considered to be the gold standard for investigating efficacy of medicines, however there are recognised limitations for reporting adverse events in RCTs (Junqueira et al., 2021). In addition, external validity of the results of RCTs is often a limitation of this study design (Hariton and Locascio, 2018; He et al., 2020). One reason for this is the highly selected study population included in trials; strict exclusion criteria are usually applied, meaning non-healthy subjects are excluded. Most commonly applied exclusion criteria in clinical research relates to age, comorbidities, and concomitant medications (He et al., 2020). As most studies included in this systematic review were randomised controlled trials, this could be a reason that we did not identify any DDI-related adverse events in this analysis. Examination of the protocols for the randomised controlled trials included in this systematic review revealed that the exclusion criteria were broadly as per section 4.5 of the SmPC for flurbiprofen (Interaction with other medicinal products and other forms of interaction) i.e., NSAIDs, Anticoagulants, e.g., warfarin, lithium, mifepristone, quinolone antibiotics and alcohol (Reckitt Benckiser Healthcare UK Ltd, 2016; Reckitt Benckiser Healthcare UK Ltd, 2018; Reckitt Benckiser Healthcare (UK) Ltd, 2022). Real-world observational studies of flurbiprofen 8.75 mg in normal clinical use are required to determine the types, frequency, and severity of adverse events when flurbiprofen is used in combination with other medicinal products.
To date, although the increased risk of adverse events due to the interaction of flurbiprofen with other medicinal products are known, the authors are not aware of any published systematic review of the risk of non-haemorrhagic events occurring with flurbiprofen 8.75 mg lozenge/oromucosal spray as a result of DDIs. An extensive search was conducted across multiple databases using broad search terms for flurbiprofen including all synonyms for flurbiprofen and the formulation where this was possible. Both published and unpublished sources of data were reviewed with the aim of identifying all eligible studies, thereby reducing the likelihood of capturing a biased sample of studies. Eligibility was decided and data was extracted by two independent reviewers. A third reviewer adjudicated any discrepancies if these could not be resolved by discussion. Therefore, the potential for reporting bias was reduced.
A review of EudraVigilance and the EMA website was conducted in order capture any non-haemorrhagic adverse events which were not reported within the initial search of published studies. However, examination of EudraVigilance was restricted by the limited information available for dose and formulation of flurbiprofen.
This systematic review was part of a wider study with the aim to assess current evidence on adverse events (haemorrhagic and non-haemorrhagic) which occur with flurbiprofen 8.75 mg dose, in particular, as a result of interaction with other medicinal products. The search was conducted up to 28 April 2020 with the results focusing on haemorrhagic events published in 2021 (Dhanda et al., 2021). In order to include the most recent data for this publication, a literature review was conducted using the same search criteria to cover the period between 29 April 2020 to 14 February 2023. One newly published paper was identified (Schachtel et al., 2021). This publication only included data combined from two individual RCTs, both of which were already identified in the search conducted for this systematic review (Schachtel et al., 2014; Schachtel et al., 2016; Dhanda et al., 2021).
There are a number of limitations which have been described previously (Dhanda et al., 2021). Some limitations are inherent to the systematic review methodology, whereas others relate to limitations of the published studies which were eligible for inclusion.
Potential biases in the review process include only reviewing English language studies. The studies included were based in Australia, Europe, Russia, the United States, and New Zealand. It is possible that results may not be generalisable to other populations, however, it is not expected that flurbiprofen 8.75 mg would have a differing safety profile in other geographical regions. Conference abstracts were excluded from this review which may introduce publication bias. In addition, studies that are smaller and have few results, in terms of both efficacy and safety, may not be published. There are only a few published studies relating to the lower dose of flurbiprofen, i.e., 8.75 mg. Non-haemorrhagic events presented are those that were reported in publications, i.e., those that were available in the public domain. There is a potential for under-reporting and misclassification of DDI-related non-haemorrhagic adverse events in studies that were not specifically designed to investigate this outcome. The studies included in the systematic review were not specifically designed (and therefore not powered) to investigate non-haemorrhagic adverse events, in particular DDI-related non-haemorrhagic adverse events of flurbiprofen 8.75 mg dose with concomitant medication use. The findings from this systematic review may therefore not provide a true representation of the overall risk. It is possible that in open-label trials and observational studies, reporter and/or observer bias may have led to differential misclassification of the outcome whereby awareness that a low dose of flurbiprofen was being used may have led to a reporting bias, impacting patient and/or investigator data collection.
Finally, in terms of quality of evidence, risk of bias assessments were not performed as no DDI-related non-haemorrhagic events occurring as a result of concomitant use of flurbiprofen 8.75 mg dose (any formulation) with other medicinal products were identified.
In conclusion, results from this first systematic review on the risk of non-haemorrhagic events occurring as a result of concomitant use of flurbiprofen 8.75 mg lozenge/oromucosal spray with other medical products did not provide evidence for DDI related adverse events.
Additional, appropriately designed research would be required to confirm whether these findings suggest a true absence of risk or limitations in reporting. Such studies could include observational post-authorisation safety studies (PASS) specifically designed to collect data on DDI-related non-haemorrhagic safety outcomes with flurbiprofen 8.75 mg dose. These ‘real-world’ studies may aid further investigation of any potential risk.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
AE, DR, SD, and SS: study design and concept, approved protocol. AE and DR: Literature search, study selection, data extraction, report write up. SL: drafting of manuscript, interpretation of results. SD: third adjudicator, interpretation of results, review of final report. GC, AK, DM-S, and NR: study design and concept, approved protocol and final report. All authors contributed to the article and approved the submitted version.
The Drug Safety Research Unit (DSRU) is an independent academic institution which works in association with the University of Portsmouth. Funding was received from the marketing authorisation holder of flurbiprofen 8.75 mg lozenge (Strefen Honey and Lemon), Reckitt Benckiser Healthcare (UK) Ltd. The funder had the following involvement with the study; study design, decision to publish, and preparation of the manuscript.
Authors GC, AK, DM-S, and NR are employed by Reckitt Benckiser Healthcare (UK) Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2024.1107185/full#supplementary-material
Balshem, H., Helfand, M., Schünemann, H. J., Oxman, A. D., Kunz, R., Brozek, J., et al. (2011). GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 64, 401–406. doi:10.1016/j.jclinepi.2010.07.015
Benrimoj, S. I., Langford, J. H., Christian, J., Charlesworth, A., and Steans, A. (2001). Efficacy and tolerability of the anti-inflammatory throat lozenge flurbiprofen 8.75mg in the treatment of sore throat a randomised, double-blind, placebo-controlled study. Clin. Drug Investig. 21, 183–193. doi:10.2165/00044011-200121030-00004
Blagden, M., Christian, J., Miller, K., and Charlesworth, A. (2002). Multidose flurbiprofen 8.75 mg lozenges in the treatment of sore throat: a randomised, double-blind, placebo-controlled study in UK general practice centres. Int. J. Clin. Pract. 56, 95–100. doi:10.1111/j.1742-1241.2002.tb11204.x
Burova, N., Bychkova, V., and Shephard, A. (2018). Improvements in throat function and qualities of sore throat from locally applied Flurbiprofen 8.75 mg in spray or lozenge format: findings from a randomized trial of patients with upper respiratory tract infection in the Russian federation. J. Pain Res. 11, 1045–1055. doi:10.2147/JPR.S149331
Calapai, G., Imbesi, S., Cafeo, V., Spagnolo, E. V., Minciullo, P. L., Caputi, A. P., et al. (2013). Fatal hypersensitivity reaction to an oral spray of flurbiprofen: a case report. J. Clin. Pharm. Ther. 38, 337–338. doi:10.1111/jcpt.12073
Cebi, A. T. (2020). Efficiency of topical and systemic flurbiprofen on pain and edema after impacted third molar surgery and comparison of gastrointestinal adverse effects. Cukurova Med. J. 45 (1), 141–147. doi:10.17826/cumj.631371
De Looze, F., Russo, M., Bloch, M., Montgomery, B., Shephard, A., Smith, G., et al. (2016). Efficacy of flurbiprofen 8.75 mg spray in patients with sore throat due to an upper respiratory tract infection: a randomised controlled trial. Eur. J. Gen. Pract. 22, 111–118. doi:10.3109/13814788.2016.1145650
Dhanda, S., Evans, A., Roy, D., Osborne, V., Townsley, A., Coutinho, G., et al. (2021). A systematic review of flurbiprofen 8.75 mg dose and risk of haemorrhagic events. Front. Pharmacol. 12, 726141. doi:10.3389/fphar.2021.726141
Di Meo, N., Stinco, G., Patrone, P., Trevisini, S., and Trevisan, G. (2016). Acute localized exanthematous pustulosis caused by flurbiprofen. Cutis 98, E9–E11.
Dionne, R. A., Haynes, D., Brahim, J. S., Rowan, J. S., and Guivarc', H. P. H. (2004). Analgesic effect of sustained-release flurbiprofen administered at the site of tissue injury in the oral surgery model. J. Clin. Pharmacol. 44 (12), 1418–1424. doi:10.1177/0091270004265703
Giovannini, M., Sarti, L., Barni, S., Pucci, N., Novembre, E., and Mori, F. (2017). Anaphylaxis to over-the-counter flurbiprofen in a child. Pharmacology 99, 121–123. doi:10.1159/000452671
Hariton, E., and Locascio, J. J. (2018). Randomised controlled trials - the gold standard for effectiveness research: study design: randomised controlled trials. Bjog 125, 1716. doi:10.1111/1471-0528.15199
Heasman, P. A., Seymour, R. A., and Boston, P. F. (1989). The effect of a topical non-steroidal antiinflammatory drug on the development of experimental gingivitis in man. J. Clin. periodontology 16 (6), 353–358. doi:10.1111/j.1600-051x.1989.tb00004.x
He, J., Morales, D. R., and Guthrie, B. (2020). Exclusion rates in randomized controlled trials of treatments for physical conditions: a systematic review. Trials 21, 228. doi:10.1186/s13063-020-4139-0
Higgins, J., and Thomas, J. (2019). Cochrane Handbook for systematic review of Interventions. Chicester: The Cochrane Collaboration. Version 6.
Junqueira, D. R., Phillips, R., Zorzela, L., Golder, S., Loke, Y., Moher, D., et al. (2021). Time to improve the reporting of harms in randomized controlled trials. J. Clin. Epidemiol. 136, 216–220. doi:10.1016/j.jclinepi.2021.04.020
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339, b2700. doi:10.1136/bmj.b2700
Limb, M., Connor, A., Pickford, M., Church, A., Mamman, R., Reader, S., et al. (2009). Scintigraphy can be used to compare delivery of sore throat formulations. Int. J. Clin. Pract. 63, 606–612. doi:10.1111/j.1742-1241.2008.01984.x
Moore, N., Pollack, C., and Butkerait, P. (2015). Adverse drug reactions and drug-drug interactions with over-the-counter NSAIDs. Ther. Clin. Risk Manag. 11, 1061–1075. doi:10.2147/TCRM.S79135
Page, M. J., Mckenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj 372, n71. doi:10.1136/bmj.n71
Radkova, E., Burova, N., Bychkova, V., and Devito, R. (2017). Efficacy of flurbiprofen 8.75 mg delivered as a spray or lozenge in patients with sore throat due to upper respiratory tract infection: a randomized, non-inferiority trial in the Russian Federation. J. Pain Res. 10, 1591–1600. doi:10.2147/JPR.S135602
Rao, P., and Knaus, E. E. (2008). Evolution of nonsteroidal anti-inflammatory drugs (NSAIDs): cyclooxygenase (COX) inhibition and beyond. J. Pharm. Pharm. Sci. 11, 81s–110s. doi:10.18433/j3t886
Reckitt Benckiser Healthcare (UK) LTD (2016). Summary of product characteristics. Flurbiprofen 8.75mg strefen Honey and Lemon.
Reckitt Benckiser Healthcare (UK) LTD (2018). Summary of product characteristics. Strefen Direct. 8.75mg/dose Oromucosal Spray, Solution.
Schachtel, B. P., Homan, H. D., Gibb, I. A., and Christian, J. (2002). Demonstration of dose response of flurbiprofen lozenges with the sore throat pain model. Clin. Pharmacol. Ther. 71 (5), 375–380. doi:10.1067/mcp.2002.124079
Schachtel, B. P., Shephard, A., Shea, T., Sanner, K., Savino, L., Rezuke, J., et al. (2016). Flurbiprofen 8.75 mg lozenges for treating sore throat symptoms: a randomized, double-blind, placebo-controlled study. Pain Manag. 6, 519–529. doi:10.2217/pmt-2015-0001
Schachtel, B., Aspley, S., Shephard, A., Schachtel, E., Lorton, M. B., and Shea, T. (2018a). Onset of analgesia by a topically administered flurbiprofen lozenge: a randomised controlled trial using the double stopwatch method. Br. J. Pain 12, 208–216. doi:10.1177/2049463718756152
Schachtel, B., Aspley, S., Shephard, A., Shea, T., Smith, G., and Schachtel, E. (2014). Utility of the sore throat pain model in a multiple-dose assessment of the acute analgesic flurbiprofen: a randomized controlled study. Trials 15, 263. doi:10.1186/1745-6215-15-263
Schachtel, B., Shephard, A., Schachtel, E., Lorton, M. B., Shea, T., and Aspley, S. (2018b). Qualities of Sore Throat Index (QuaSTI): measuring descriptors of sore throat in a randomized, placebo-controlled trial. Pain Manag. 8, 85–94. doi:10.2217/pmt-2017-0041
Schachtel, B., Shephard, A., Schachtel, E., Shea, T., Smith, A., and Tselenti, E. (2021). Evidence of the efficacy of flurbiprofen 8.75 mg lozenges for patients receiving antibiotics for laboratory-confirmed streptococcal pharyngitis. Ear Nose Throat J. 102, NP609–NP617. doi:10.1177/01455613211025754
Sterne, J. A., Hernán, M. A., Reeves, B. C., Savović, J., Berkman, N. D., Viswanathan, M., et al. (2016). ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355, i4919. doi:10.1136/bmj.i4919
Sterne, J. A. C., Savović, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., et al. (2019). RoB 2: a revised tool for assessing risk of bias in randomised trials. Bmj 366, l4898. doi:10.1136/bmj.l4898
Watson, N., Nimmo, W. S., Christian, J., Charlesworth, A., Speight, J., and Miller, K. (2000). Relief of sore throat with the anti-inflammatory throat lozenge flurbiprofen 8.75 mg: a randomised, double-blind, placebo-controlled study of efficacy and safety. Int. J. Clin. Pract. 54, 490–496. doi:10.1111/j.1742-1241.2000.tb10910.x
Keywords: flurbiprofen, lozenge, oromucosal spray, drug-drug interactions, adverse events
Citation: Evans A, Roy D, Dhanda S, Lane S, Coutinho G, Kulasekaran A, Miller-Shakesby D, Ramamoorthi N and Shakir S (2024) A systematic review of flurbiprofen 8.75 mg dose and risk of adverse events (excluding haemorrhagic) resulting from drug-drug interactions. Front. Pharmacol. 15:1107185. doi: 10.3389/fphar.2024.1107185
Received: 24 November 2022; Accepted: 14 February 2024;
Published: 06 March 2024.
Edited by:
Anick Bérard, Montreal University, CanadaReviewed by:
Kuntheavy Ing Lorenzini, Hôpitaux universitaires de Genève (HUG), SwitzerlandCopyright © 2024 Evans, Roy, Dhanda, Lane, Coutinho, Kulasekaran, Miller-Shakesby, Ramamoorthi and Shakir. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alison Evans, QWxpc29uLkV2YW5zQGRzcnUub3Jn
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.