
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 02 October 2023
Sec. Pharmacoepidemiology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1260915
This article is part of the Research Topic Pharmacovigilance and Pharmacoepidemiology: Public Health and Safety View all 17 articles
 Basile Chrétien1*
Basile Chrétien1* Perrine Brazo2,3
Perrine Brazo2,3 Angélique Da Silva1Marion Sassier1
Angélique Da Silva1Marion Sassier1 Charles Dolladille1,4Véronique Lelong-Boulouard1,5Joachim Alexandre1,3
Charles Dolladille1,4Véronique Lelong-Boulouard1,5Joachim Alexandre1,3 Sophie Fedrizzi1
Sophie Fedrizzi1Introduction: Clozapine is primarily reserved for treatment-resistant schizophrenia due to safety concerns associated with its use. Infections have been reported with clozapine, which may lead to elevated serum levels of the drug. However, the existing literature on this topic is limited. Therefore, we conducted a study using VigiBase® to investigate the potential over-reporting of infections associated with clozapine, to explore the presence of dose-dependency, and to investigate the underlying mechanism.
Methods: Disproportionality analyses were performed using VigiBase to assess the association between clozapine and all types of infections, the association between clozapine-associated infections and neutropenia, the association between clozapine-associated infections and agranulocytosis, the dose–effect relationship between clozapine and infections, and the interaction between clozapine and the main strong CYP450 inhibitors using reports carried out until 11 April 2023.
Results: A statistically significant signal of infections was observed with clozapine, as indicated by an information component of 0.43 [95% CI: (0.41–0.45)]. The most commonly reported infections were respiratory and gastrointestinal in nature. Neutropenia showed weaker association with clozapine-associated reports of infections compared to other clozapine-associated reports [X2 (1, N = 204,073) = 454; p < 0.005], while agranulocytosis demonstrated a stronger association with clozapine-associated reports of infections [X2 (1, N = 204,073) = 56; p < 0.005]. No evidence of dose-dependency was observed. Among the 17 tested CYP inhibitors, significant drug–drug interactions were found with clarithromycin, metronidazole, valproic acid, lansoprazole, omeprazole, amiodarone, and esomeprazole.
Discussion: Our study revealed a significant safety signal between clozapine use and infections, predominantly respiratory and gastrointestinal infections. The co-administration of clozapine with valproic acid or proton pump inhibitors may potentially contribute to an increased risk of infection. Further vigilance is warranted in clinical practice, and consideration of therapeutic drug monitoring of clozapine in cases involving concomitant use of these drugs or in the presence of infections may be beneficial.
Clozapine is an atypical antipsychotic drug mostly used in patients with treatment-resistant schizophrenia. Over the years, its use has increased in many countries, with the prevalence of clozapine consumption in 2014 ranging from 0.9 to 173.2 per 100,000 persons, depending on the country (Bachmann et al., 2017; Remington et al., 2017). Safety issues associated with clozapine are common and include agranulocytosis (occurring in approximately 1.0% of patients) and neutropenia (occurring in approximately 3.0% of patients) (Rajagopal, 2005). Due to these safety concerns, clozapine is usually reserved for treatment-resistant schizophrenia despite its demonstrated efficacy in managing positive, negative, and overall symptoms and relapse rates in schizophrenia, compared to first-generation antipsychotics and pooled first-/second-generation antipsychotics (Wagner et al., 2021).
Infections have also been reported with clozapine, potentially leading to the elevation of serum levels of the drug. A systematic review identified 40 cases of infections with demonstrated elevated clozapine levels (Clark et al., 2018). In a Chinese cohort of patients undergoing therapeutic drug monitoring during infection and non-infection periods, the median levels of clozapine were significantly higher in the infection period compared to those in the non-infection period (n = 42; p < 0.001) (Zhang et al., 2021). Elevation of clozapine levels with infection may be due to downregulation of metabolizing enzymes such as cytochrome P450 (Clark et al., 2018). Additionally, a retrospective study from the UK found an increased risk of COVID-19 infection in clozapine-treated patients compared to those on other antipsychotic drugs (adjusted hazard ratio = 1.76; 95% CI 1.14–2.72) (Govind et al., 2021).
Clozapine might be more strongly associated with pneumonia than with other infections. A study on a Taiwanese registry with 33,024 inpatients with schizophrenia found that the current use of clozapine was associated with a dose-dependent increase in the risk of pneumonia (adjusted risk ratio = 3.18; 95% CI: 2.62–3.86) (Kuo et al., 2013). A study using VigiBase®, the WHO global safety report database, supports the prominent role of pneumonia in mortality associated with clozapine adverse drug reactions (De Leon et al., 2020).
Patients with schizophrenia often receive polypharmacotherapy, exposing them to potential drug–drug interactions (DDIs). A cross-sectional observational study in a psychiatric hospital found a high prevalence (88.7%) of potential DDI in this population (Bačar Bole et al., 2023). Clozapine is metabolized by various CYP450 enzymes, including CYP1A2, CYP3A4, CYP2D6, CYP2C9, and CYP2C19 (Chetty and Murray, 2007; Pardiñas et al., 2019). Therefore, the association of clozapine with CYP450 inhibitors could lead to clozapine overdose and increase the risk of infection.
Sex-related differences in clozapine tolerability have also been described in 147 treatment-resistant patients treated with clozapine (Martini et al., 2021). Age onset incidence of schizophrenia also differs by sex (Jauhar et al., 2022). As sex-specific differences in the susceptibility to infections and immune response to infection have been reported (McClelland and Smith, 2011), it is also possible that sex differences in clozapine-associated infections exist.
However, until now, studies about clozapine-associated infections remain scarce and are poorly described. Except for clozapine-induced pneumonia, which has been widely described (De Leon et al., 2020), it is unclear what kind of other infection clozapine exposure might lead to. The mechanism behind these infections also needs to be understood as it could be hypothesized that clozapine-induced infections are caused by clozapine-associated neutropenia. Dose-dependency, patient-associated risk factors, and potential DDIs leading to infections also need to be explored to improve preventive measures. Thus, for a better understanding of clozapine-associated infections, a study was conducted using VigiBase®. The objectives were to assess if clozapine was associated with an over-reporting of infections, to characterize these infections, to evaluate dose-dependency and sex differences, and to investigate potential DDIs associated with infections. The study also explored if clozapine-associated infections were more associated with neutropenia.
We conducted a retrospective pharmacovigilance cohort study using VigiBase®, the WHO global individual case safety report (ICSR) database. Access to the data was granted by the WHO Uppsala Monitoring Centre. The database contains suspected drugs, suspected adverse drug reactions (ADRs), patient demographics, and other variables, with over 32 million ICSRs received from 130 countries, since 1967 and previously described elsewhere (Chrétien et al., 2021). The study protocol was registered on ClinicalTrials.gov with the identifier NCT05919550.
We utilized all the reports from the de-duplicated VigiBase® dataset from the 11th of April 2023 version. The suspected duplicates were identified using vigiMatch, an algorithm developed by the Uppsala Monitoring Centre, and excluded. The scope of the dataset was limited to drugs; vaccines were excluded due to their distinct usage profile, potential for higher infection reporting, and reporting bias associated with the COVID-19 pandemic.
Infections were identified using the Medical Dictionary for Regulatory Activities (MedDRA v25.1) System Organ Class infections and infestations (Supplementary Table S1). The analysis included preferred terms of infection, as shown in Supplementary Table S1. Some terms were overly general, making it challenging to comprehensively understand the nature of the ongoing infection (e.g., the term “Infection”). Neutropenia and agranulocytosis were defined using their associated preferred terms. Clozapine was identified using the Anatomical and Therapeutic Chemical classification and/or its international non-proprietary name. The daily dose of clozapine was extracted from clozapine reports and divided into quartiles to perform the dose-dependency analysis (reports with the available daily dose were attributed to their corresponding quartile).
The primary outcome was the association between clozapine and all types of infections. Secondary outcomes included the following:
- The association between clozapine and all types of infections over time (cumulative).
- The association between clozapine and all types of infections:
o In women population
o In men population
o In people aged 44 or lower
o In people aged 45 or higher
- The association of clozapine with more detailed terms of infection (all MedDRA preferred terms included in the infection and infestation System Organ Class groups), for which at least five cases were reported with clozapine.
- The association between clozapine-associated infection and neutropenia, and the association between clozapine-associated infection and agranulocytosis.
- The dose–effect relationship between clozapine and infections.
- The interaction between clozapine and various strong CYP450 inhibitors [amiodarone, atazanavir, cannabidiol, ciclosporin, clarithromycin, clobazam, esomeprazole, felbamate, fluconazole, fluvoxamine, itraconazole, lansoprazole, metronidazole, omeprazole, ritonavir, voriconazole, and valproic acid (VPA)] and the reporting of infection. CYP450 inhibitors were defined using WHODrug Insight (Uppsala Center, 2023) and the interaction table from Geneva University Hospitals (Geneva University Hospital, 2020) (Supplementary Table S3).
To assess the association of clozapine with the reporting of infections, a disproportionality analysis was used to evaluate the associations between drugs and reactions using VigiBase® (Faillie, 2019). This type of study was previously described (Chrétien et al., 2021). In the present study, the information component (IC) and its 95% credibility interval (CI) were used to evaluate disproportionality. The IC is a Bayesian measure of the disproportionality between the observed and the expected reporting of a drug–ADR pair, developed by members of the WHO Uppsala Monitoring Centre (Bate et al., 1998). We chose to compute the analysis only for drugs that reported at least five cases of infections as IC was found to be more reliable when at least three to five cases of an ADR were reported for a drug (Evans et al., 2001). A lower end of the 95% CI of the IC > 0 was deemed significant.
- A disproportionality analysis was used to evaluate the association between clozapine and all MedDRA preferred terms included in the infection and infestation System Organ Class groups using the same method as described previously.
- A disproportionality analysis was used to evaluate the association between each quartile of the dose of clozapine and the reporting of infections using the same method as described previously.
- A disproportionality analysis was used to evaluate the association between clozapine and various CYP450 inhibitors (amiodarone, atazanavir, cannabidiol, ciclosporin, clarithromycin, clobazam, esomeprazole, felbamate, fluconazole, fluvoxamine, itraconazole, lansoprazole, metronidazole, omeprazole, ritonavir, voriconazole, and VPA) and the reporting of infection. IC was also used for this analysis.
- A chi-squared test was used to assess the association between clozapine-associated infection and neutropenias by comparing the reporting of neutropenia in clozapine-associated infection reports to the reporting of neutropenia in other clozapine-associated reports. The same test was used with agranulocytosis.
We described the clinical features of clozapine-related infections, reporting the reports’ completeness score, demographic parameters (age and sex), dose, seriousness, and percentage of death. The percentage of seriousness and death with other drugs associated with infections was also evaluated for comparison.
Out of the 204,073 reports of clozapine-associated suspected ADRs, 19,404 were related to infections. A statistically significant signal of infections was found with clozapine, with an IC of 0.43 [95% CI: (0.41–0.45)] (Table 1). This signal was of similar magnitude among genders and tested age classes (Table 1). It was also consistent over time (Figure 1).
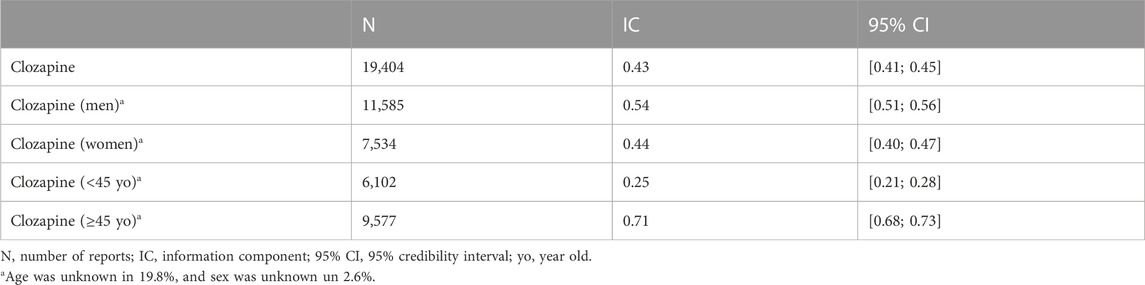
TABLE 1. Disproportionality analysis in VigiBase: reports of association of clozapine with infections.
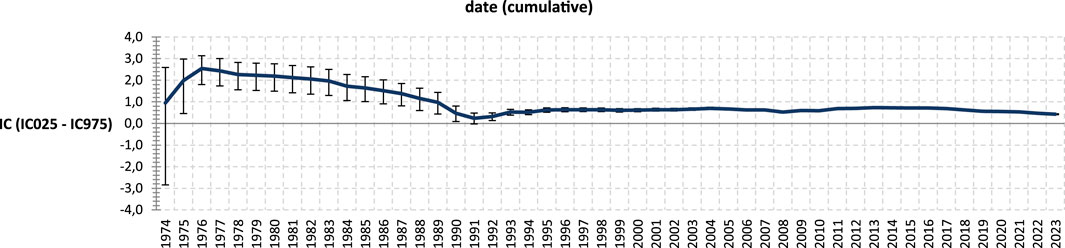
FIGURE 1. Disproportionality analysis of clozapine-associated infection over time (cumulative*). *Cumulative: previous data are used at the current date. For example, for the year 1977, data from 1974–1977 are used to compute the disproportionality analysis. Thus, at each point of the figure, cases and non-cases reported until this point are used to compute the information component.
Table 2 presents the features of clozapine-associated reports of infections. Among these reports, 94.3% were considered serious and 9.8% of cases resulted in death. This is compared with reports of infection associated with other drugs, where 62.6% were considered serious and 6.8% resulted in death.
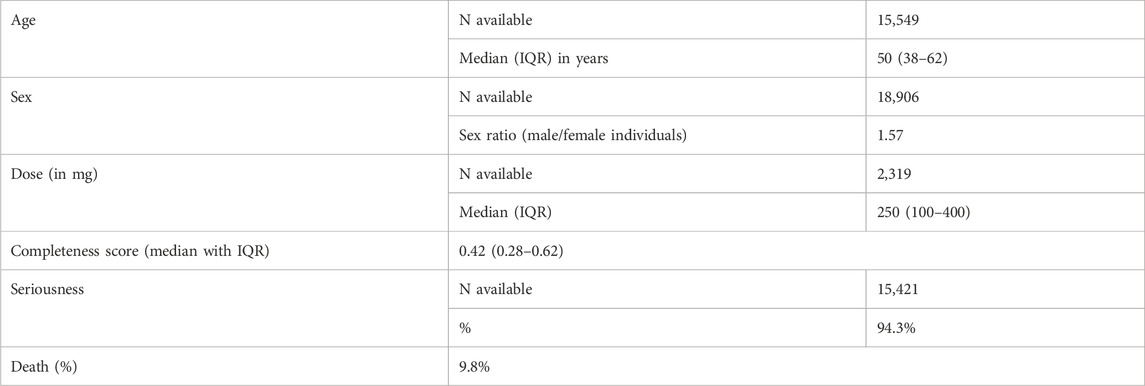
TABLE 2. Description of clozapine-associated reports of infection.
A total of 60 terms of infection were significantly associated with clozapine. The four most reported terms were pneumonia (5,751 reports), lower respiratory tract infection (2,268 reports), urinary tract infection (1,628 reports), and infections (1,564 reports). The 10 most significant signals were pneumonia aspiration [N = 850; IC: 3.28 (3.17–3.37)], viral myocarditis [N = 25; IC: 3.64 (2.97–4.11)], empyema [N = 75; IC = 3.22 (2.83–3.49)], lower respiratory tract infection [N = 2,268; IC: 2.79 (2.72–2.84)], infective exacerbation of chronic obstructive airways disease [N = 30; IC: 3.24 (2.63–3.67)], appendicitis perforated [N = 93; IC: 2.81 (2.46–3.05)], appendicitis [N = 261; IC: 2.61 (2.41–2.76)], abdominal sepsis [N = 24; IC: 3.01 (2.32–3.49)], lung abscess [N = 58; IC: 2.69 (2.25–3.00)], and complicated appendicitis [N = 9; IC: 3.18 (2.04–3.94)] (Table 3; Supplementary Table S5).
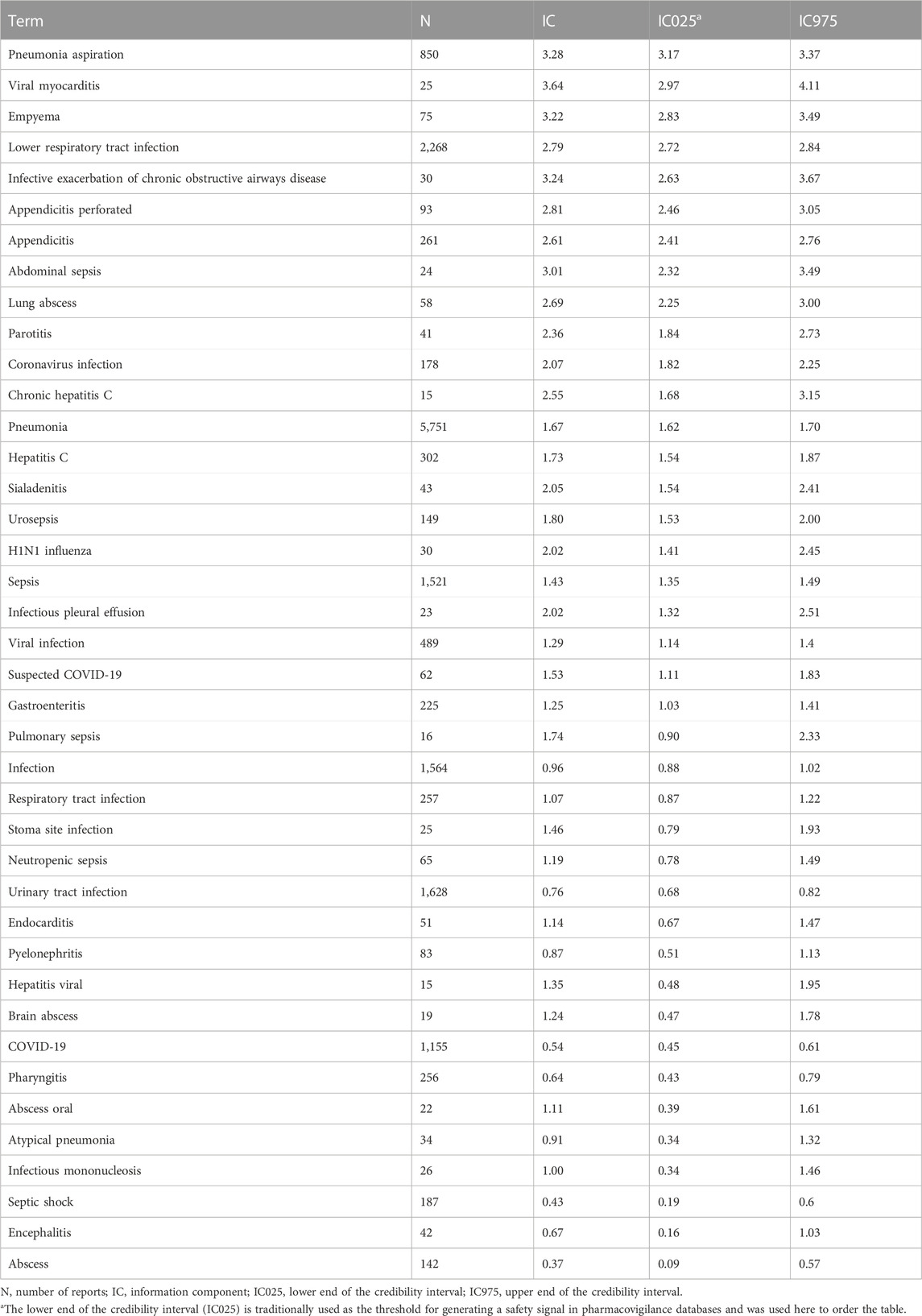
TABLE 3. Terms of infection associated with a significant over-reporting with clozapine (more than 15 reports per term).
Neutropenia was reported in 6.13% of the reports of clozapine-associated infections. It was less associated with clozapine-associated reports of infections compared to other clozapine-associated reports: X2 (1, N = 204,073) = 454; p < 0.0005). However, agranulocytosis was more associated with clozapine-associated reports of infections compared to other clozapine-associated reports: X2 (1, N = 204,073) = 56; p < 0.0005. However, agranulocytosis was reported in only 3.33% of the reports of clozapine-associated infection.
The dose was rarely reported as only 2,319 (1.14%) reports included this information. When using the dose to perform the disproportionality analysis, no signal of dose-dependency could be found (Supplementary Table S4). The quartiles of doses found in our study were as follows: 100 mg/day, 250 mg/day, and 400 mg/day.
Among the 17 tested CYP inhibitors, a significant drug–drug interaction was found with clarithromycin, metronidazole, VPA, lansoprazole, omeprazole, amiodarone, and esomeprazole (Table 4).
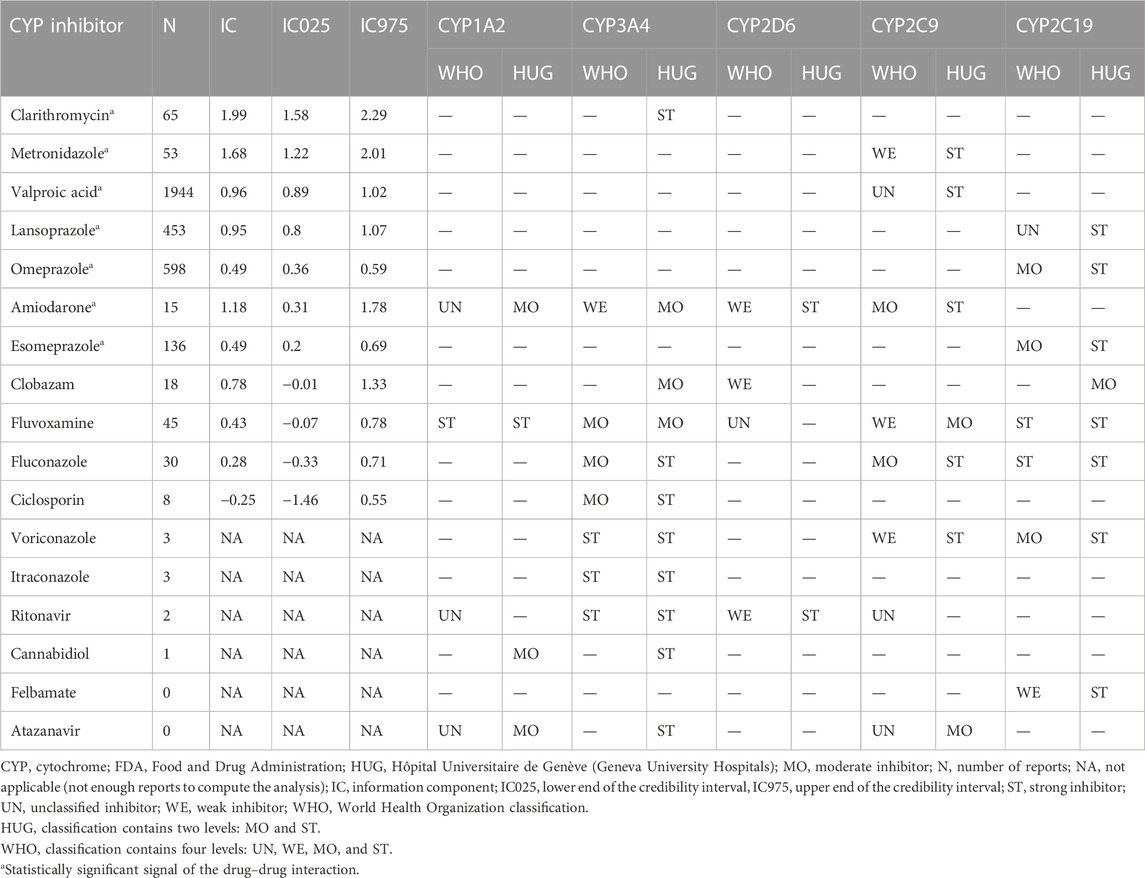
TABLE 4. Disproportionality analysis for the drug–drug interaction between clozapine and a list of CYP450 inhibitors on the reporting of infections.
In our study, conducted under real-life conditions using the largest pharmacovigilance database worldwide, we identified a significant association between clozapine and reported infections. This signal was consistent over time (Figure 1). Various types of infections were linked to clozapine use in our study, with 94.3% of them considered serious and 9.8% resulting in death at the time of reporting. Although serious adverse effects tend to be more reported than non-serious effects, our findings imply that people treated with clozapine should be carefully followed in the case of symptoms of infection.
The most frequently reported infections were respiratory and gastrointestinal in nature. Patients and families should be educated about the risk of infections, particularly respiratory and gastrointestinal infections.
Clozapine may be particularly associated with pneumonia compared to other infections. A Taiwanese registry study involving a nationwide cohort of 33,024 inpatients with schizophrenia found that the current use of clozapine (adjusted RR = 3.18; 95% CI: 2.62–3.86, p < 0.001) was linked to a dose-dependent increase in the risk of pneumonia. On the other hand, quetiapine, olanzapine, zotepine, and risperidone showed a lesser extent of association with an increased risk of pneumonia. Unlike clozapine, no clear dose-dependent relationship was observed for these antipsychotics. The risk of pneumonia with clozapine was found to be strongest within the first 30 days of treatment (Kuo et al., 2013).
A retrospective study based on clinical records from the UK also reported an increased risk of COVID-19 infection in clozapine-treated patients compared to those on other antipsychotic medications (adjusted HR = 1.76; 95% CI 1.14–2.72) (Govind et al., 2021). However, a register-based cohort study from the Stockholm region did not find an association between clozapine treatment and severe COVID-19 infection. The adjusted HR for the exposed group compared to the unexposed group was 0.96 (95% CI: 0.54 and 1.70) for inpatient care, 1.69 (0.48 and 5.93) for care in an intensive care unit (ICU), and 0.86 (0.26 and 2.80) for death (Ohlis et al., 2022). This study might have lacked statistical power due to the low number of clozapine-treated patients suffering from COVID-19 during the study period. In another English retrospective 1-year cohort study, the incidence of infection was compared between 64 patients starting clozapine and 120 patients starting paliperidone palmitate long-acting injection (PPLAI). The incidence of infection was greater in clozapine starters than in PPLAI starters (28% vs. 6%; p = 0.001; adjusted odds ratio 5.82 (95% CI = 2.15–15.76). Similar to our findings, infectious episodes in clozapine patients were not statistically related to changes in neutrophil counts. According to the authors’ classification, the most commonly reported infection in the clozapine group was respiratory infection; however, the majority of infections were non-respiratory-related (Mace et al., 2022).
Regarding the risk of gastrointestinal infection, particularly appendicitis, a retrospective study including 465 patients, of whom 65 were on clozapine, showed that the clozapine exposure group exhibited a higher incidence of appendicitis during the observation period than the non-exposure group (863 cases vs. 124 cases per 100,000 person-years) (Kawakita et al., 2022). Additionally, a case series of six patients with perforated appendicitis during clozapine treatment reported a 20-fold increase in appendicitis incidence compared to the general population in male subjects of the same age group (Steinert and Jans, 2021). The authors also suspected a dose-dependency as they observed high clozapine serum levels in three of those patients during the course of appendicitis.
Possible indirect mechanisms of clozapine predisposition to infection, particularly aspiration pneumonia, include sialorrhea and impairment of swallowing function with esophageal dilatation and hypomotility (Abdelmawla and Ahmed, 2009). A systematic review during the first month of clozapine treatment indicated that up to 50% of patients develop fever and flu-like symptoms, seemingly driven by increased cytokines (Røge et al., 2012). A recent study comparing the levels of secondary antibodies of clozapine users with those of the users of antipsychotics other than clozapine (control group) noted lower secondary antibodies among clozapine users. Total serum immunoglobulins [immunoglobulin (Ig)G, IgA, and IgM] and specific immunoglobulin antibodies to Haemophilus influenzae and pneumococcus were decreased (Ponsford et al., 2019). Lower immunoglobulin levels might contribute to the onset of infections.
In our study, neutropenia was less associated with clozapine-associated reports of infections compared to other clozapine-associated reports (p-value < 0.005), indicating that most of these infections were probably not linked to clozapine-associated neutropenia. However, agranulocytosis was more associated with clozapine-associated reports of infections compared to other clozapine-associated reports (p-value < 0.005), which is expected as infection is very common in agranulocytosis patients. Indeed, a retrospective Finn study on 163 patients with clozapine-induced agranulocytosis found that 78.6% of the patients presented with an infection (Lahdelma and Appelberg, 2012). The median age of the patients in this study was 49 years, which is very close to the median age in our study (50 years), but the sex ratio was lower in their study (1.09 vs. 1.57 in our study). However, since agranulocytosis was reported in only 3.33% of the reports of clozapine-associated infections, it is not the main cause of the signal of infections observed in our study.
Although men and women have a similar prevalence of schizophrenia (Li et al., 2016), research indicates that men often experience the onset of severe schizophrenia symptoms at an earlier age compared to women. Specifically, men tend to encounter the peak period of initial pronounced psychotic symptoms between 20 and 24 years of age, whereas women tend to experience these symptoms 5 or more years later (Kahn et al., 2015). This might be the reason why there are important gender differences in clozapine prescription. Indeed, several studies, including ours, have reported that men represented between 63.1% and 78.6% of patients treated with clozapine (Taylor, 2004; Silveira et al., 2015). Consequently, sex is probably not a risk factor for clozapine-induced infections.
The median dose in our study was 250 mg (IQR = 100–400). This aligns with the typical dose found in the clozapine-treated population as Caucasians are usually prescribed 300–600 mg/day to reach the therapeutic range, while in Asian countries, average clozapine doses are lower than 300 mg/day (de Leon et al., 2020). However, it is essential to consider that dose reporting was unavailable in more than 98% of the reports in the database. The results of the tests performed in this study to explore a dose-dependency effect do not allow us to draw a conclusion.
The results of the disproportionality analysis for drug–drug interactions (DDI) between clozapine and CYP450 inhibitors on the reporting of infections are more challenging to interpret. Except for ciclosporin (an inhibitor of CYP3A4), a trend toward a DDI was found with all CYP inhibitors, for which a disproportionality analysis could be computed. However, it is unclear which specific CYP450 enzymes may be involved. The associations observed with certain CYP inhibitors, such as clarithromycin and metronidazole, may be influenced by an indication bias since these drugs are commonly prescribed in the context of infections. VPA, one of the most co-reported drugs in the DDI analysis, has been associated with an increase in oxidative stress. Given the potential for clozapine to induce oxidative stress as well, the combination of VPA and clozapine may potentially favor the onset of certain types of infections (Gai et al., 2020; Salimi et al., 2022).
Some authors suspect that the association of clozapine with proton pump inhibitors (PPI) might increase the formation of reactive metabolites and contribute to the increase in hematological adverse drug reactions (ADRs) (Wiciński et al., 2017). However, the oxidative stress hypothesis is inconclusive with PPIs as these drugs usually alleviate oxidative stress (Gao et al., 2019; Gandhi et al., 2021). PPIs have been associated with respiratory infections in different retrospective studies, suggesting a potential pharmacodynamic interaction (Ho et al., 2017; Wang et al., 2019). In a retrospective chart review, aiming to explore the potential effect of polypharmacy on the hematologic profiles of clozapine patients, 24 out of 26 (96%) of the subset of patients who were prescribed a PPI or ranitidine concomitantly with clozapine experienced hematological ADRs (Shuman et al., 2014). A case of infection during PPI treatment with elevated plasma clozapine levels was reported in a 51-year-old woman and could potentially be linked to the switch from omeprazole to esomeprazole (Wagner et al., 2011). The authors speculated that this might be due to the removal of induction of clozapine metabolism by omeprazole. However, the delay was not in favor of this hypothesis. Omeprazole and lansoprazole, in addition to being CYP2C19 inhibitors, are also CYP1A2 inducers. In a case series involving two patients, the prescription of omeprazole was associated with a reduction in clozapine plasma concentrations of 41.9% and 44.7% (Frick et al., 2003). Another retrospective study in 13 psychiatric patients found that the switch from omeprazole to pantoprazole led to an increase in clozapine levels in non-smoking patients and to a decrease in clozapine levels in smoking patients. This was probably caused by the discontinuation of enzyme induction in the cytochrome P450 enzyme 1A2 by omeprazole in non-smokers, whereas CYP1A2 remained induced in smokers (Mookhoek and Loonen, 2004). As the prevalence of cigarette smoking is high in schizophrenia patients (around 70%–80%) and probably even higher in treatment-resistant schizophrenia patients (Ding and Hu, 2021), we believe that the DDI observed in our study between PPIs and clozapine is probably more linked to the CYP2C19 inhibition by PPIs.
Regardless of the cause of infection, several reports showed that infection leads to an increase in the toxicity levels of clozapine and its metabolites in the serum (Darling and Huthwaite, 2011; Espnes et al., 2012; Zhang et al., 2021; Chengappa et al., 2022). This is likely to be mediated by cytokine suppression of cytochrome P450 1A2 (CYP1A2), the main hepatic microsomal system involved in clozapine metabolism, which is also involved in the metabolism of several antibiotics commonly used to treat infections. This further enhances the potential for clozapine toxicity (Røge et al., 2012). However, despite sex being a factor of cytochrome P450 expression (Zanger and Schwab, 2013), we did not find any sex-related significant differences in clozapine-associated infections.
Our study was subject to various inherent limitations stemming from the utilization of a pharmacovigilance database. Of paramount importance among these limitations is the issue of under-reporting. Nevertheless, it is reassuring that despite this limitation, the results and significance of the disproportionality analysis remained unaffected (Montastruc et al., 2011).
However, it is crucial to recognize that the likelihood of a suspected ADR being drug-related may not be uniform across all cases. Although disproportionality analysis of spontaneous reports is a valuable tool for detecting safety signals, it possesses certain intrinsic limitations as well. One such limitation is the potential presence of low-quality data due to missing information. Additionally, the causal relationship between the reported drug and the ADR remains unproven (Egberts et al., 2002; Garbe and Suissa, 2014).
Moreover, it is worth noting that the reporting pattern of ADRs may vary between new and old drugs, with more rigorous monitoring typically occurring during the period of drug marketing and shortly thereafter.
It is vital to emphasize that, due to under-reporting of ADRs, pharmacovigilance data cannot be utilized to determine the incidence rates of ADRs (Sharrar and Dieck, 2013). Furthermore, our study lacked information on the smoking history of participants despite its significant impact on the pharmacokinetics of clozapine and the risk of respiratory infection.
This study has revealed a significant safety signal concerning the association between clozapine and reported infections. Respiratory infections, as well as gastrointestinal infections, including appendicitis, were the most commonly reported infections. The co-administration of clozapine with valproic acid (VPA) or proton pump inhibitors (PPIs) may potentially increase the risk of infection. However, as this study was based on pharmacovigilance data, a definitive causal relationship between clozapine exposure and the occurrence of infections cannot be established with certainty. Nevertheless, in clinical practice, psychiatrists should remain vigilant for signs of infections when prescribing clozapine and ensure that mandatory vaccines, including pneumococcal vaccination, have been administered. Conducting a study to evaluate the relevance of therapeutic drug monitoring of clozapine when the patient’s treatment regimen is altered (especially with VPA or PPIs) or when an infection occurs would be of considerable interest.
The datasets presented in this article are not readily available because data are owned by the WHO Uppsala Monitoring Center. Requests to access the datasets should be directed to https://who-umc.org/vigibase/.
The studies involving humans were approved by the Comité d’éthique du CHU de Caen. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
BC: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Validation, Writing–original draft. PB: Writing–review and editing. AS: Writing–review and editing. MS: Writing–review and editing. CD: Writing–review and editing. VL-B: Writing–review and editing. JA: Supervision, Writing–review and editing. SF: Writing–review and editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The information presented in this study does not represent the opinion of WHO. The authors would like to thank the custom search team at the Uppsala Monitoring Centre (Uppsala, Sweden) research section, without whom this study would not have been possible.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1260915/full#supplementary-material
Abdelmawla, N., and Ahmed, M. I. (2009). Clozapine and risk of pneumonia. Br. J. Psychiatry 194, 468–469. doi:10.1192/bjp.194.5.468a
Bačar Bole, C., Nagode, K., Pišlar, M., Mrhar, A., Grabnar, I., and Vovk, T. (2023). Potential drug-drug interactions among patients with schizophrenia spectrum disorders: Prevalence, association with risk factors, and replicate analysis in 2021. Med. Kaunas. 59, 284. doi:10.3390/medicina59020284
Bachmann, C. J., Aagaard, L., Bernardo, M., Brandt, L., Cartabia, M., Clavenna, A., et al. (2017). International trends in clozapine use: A study in 17 countries. Acta Psychiatr. Scand. 136, 37–51. doi:10.1111/acps.12742
Bate, A., Lindquist, M., Edwards, I. R., Olsson, S., Orre, R., Lansner, A., et al. (1998). A Bayesian neural network method for adverse drug reaction signal generation. Eur. J. Clin. Pharmacol. 54, 315–321. doi:10.1007/s002280050466
Chengappa, K. N. R., Thomas, J., Kahn, C. E., Clinebell, K., Mullen, K. K., Arbutiski, L., et al. (2022). COVID-19 infection, fluctuations in the clozapine/norclozapine levels and metabolic ratio and clozapine toxicity: An illustrative case-report. Schizophr. Res. 244, 66–68. doi:10.1016/j.schres.2022.05.009
Chetty, M., and Murray, M. (2007). CYP-Mediated clozapine interactions: How predictable are they? Curr. Drug Metab. 8, 307–313. doi:10.2174/138920007780655469
Chrétien, B., Lelong-Boulouard, V., Chantepie, S., Sassier, M., Bertho, M., Brazo, P., et al. (2021). Haematologic malignancies associated with clozapine v. all other antipsychotic agents: A pharmacovigilance study in VigiBase®. Psychol. Med. 51, 1459–1466. doi:10.1017/S0033291720000161
Clark, S. R., Warren, N. S., Kim, G., Jankowiak, D., Schubert, K. O., Kisely, S., et al. (2018). Elevated clozapine levels associated with infection: A systematic review. Schizophrenia Res. 192, 50–56. doi:10.1016/j.schres.2017.03.045
Darling, P., and Huthwaite, M. A. (2011). Infection-associated clozapine toxicity. Clin. Schizophr. Relat. Psychoses 5, 159–160. doi:10.3371/CSRP.5.3.7
de Leon, J., Rajkumar, A. P., Kaithi, A. R., Schoretsanitis, G., Kane, J. M., Wang, C.-Y., et al. (2020). Do asian patients require only half of the clozapine dose prescribed for Caucasians? A critical overview. Indian J. Psychol. Med. 42, 4–10. doi:10.4103/IJPSYM.IJPSYM_379_19
De Leon, J., Sanz, E. J., and De las Cuevas, C. (2020). Data from the World health organization’s pharmacovigilance database supports the prominent role of pneumonia in mortality associated with clozapine adverse drug reactions. Schizophr. Bull. 46, 1–3. doi:10.1093/schbul/sbz093
Ding, J. B., and Hu, K. (2021). Cigarette smoking and schizophrenia: Etiology, clinical, pharmacological, and treatment implications. Schizophr. Res. Treat. 2021, 7698030. doi:10.1155/2021/7698030
Egberts, A. C. G., Meyboom, R. H. B., and van Puijenbroek, E. P. (2002). Use of measures of disproportionality in pharmacovigilance: Three Dutch examples. Drug-Safety 25, 453–458. doi:10.2165/00002018-200225060-00010
Espnes, K. A., Heimdal, K. O., and Spigset, O. (2012). A puzzling case of increased serum clozapine levels in a patient with inflammation and infection. Ther. Drug Monit. 34, 489–492. doi:10.1097/FTD.0b013e3182666c62
Evans, S. J., Waller, P. C., and Davis, S. (2001). Use of proportional reporting ratios (PRRs) for signal generation from spontaneous adverse drug reaction reports. Pharmacoepidemiol Drug Saf. 10 (6), 483–486. doi:10.1002/pds.677
Faillie, J.-L. (2019). Case-non-case studies: Principle, methods, bias and interpretation. Therapie 74, 225–232. doi:10.1016/j.therap.2019.01.006
Frick, A., Kopitz, J., and Bergemann, N. (2003). Omeprazole reduces clozapine plasma concentrations. A case report. Pharmacopsychiatry 36, 121–123. doi:10.1055/s-2003-39980
Gandhi, T., Sharma, A., Vyas, N., Gupta, P., Parikh, M., and Shah, H. (2021). Lansoprazole a proton pump inhibitor prevents IBD by reduction of oxidative stress and NO levels in the rat. Drug Res. (Stuttg) 71, 379–387. doi:10.1055/a-1389-5499
Gai, Z., Krajnc, E., Samodelov, S. L., Visentin, M., and Kullak-Ublick, G. A. (2020). Obeticholic acid ameliorates valproic acid-induced hepatic steatosis and oxidative stress. Mol. Pharmacol. 97, 314–323. doi:10.1124/mol.119.118646
Gao, H., Zhang, S., Hu, T., Qu, X., Zhai, J., Zhang, Y., et al. (2019). Omeprazole protects against cisplatin-induced nephrotoxicity by alleviating oxidative stress, inflammation, and transporter-mediated cisplatin accumulation in rats and HK-2 cells. Chem. Biol. Interact. 297, 130–140. doi:10.1016/j.cbi.2018.11.008
Garbe, E., and Suissa, S. (2014). “Pharmacoepidemiology,” in Handbook of epidemiology. Editors W. Ahrens,, and I. Pigeot (New York, NY: Springer New York), 1875–1925. doi:10.1007/978-0-387-09834-0_31
Geneva University Hospital (2020). carte_des_cytochromes_2020.pdf. Available at: https://www.hug.ch/sites/interhug/files/structures/pharmacologie_et_toxicologie_cliniques/images/carte_des_cytochromes_2020.pdf (Accessed May 26, 2023).
Govind, R., Fonseca de Freitas, D., Pritchard, M., Hayes, R. D., and MacCabe, J. H. (2021). Clozapine treatment and risk of COVID-19 infection: Retrospective cohort study. Br. J. Psychiatry 219, 368–374. doi:10.1192/bjp.2020.151
Ho, S.-W., Teng, Y.-H., Yang, S.-F., Yeh, H.-W., Wang, Y.-H., Chou, M.-C., et al. (2017). Association of proton pump inhibitors usage with risk of pneumonia in dementia patients. J. Am. Geriatr. Soc. 65, 1441–1447. doi:10.1111/jgs.14813
Jauhar, S., Johnstone, M., and McKenna, P. J. (2022). Schizophrenia. Lancet 399, 473–486. doi:10.1016/S0140-6736(21)01730-X
Kahn, R. S., Sommer, I. E., Murray, R. M., Meyer-Lindenberg, A., Weinberger, D. R., Cannon, T. D., et al. (2015). Schizophrenia. Nat. Rev. Dis. Prim. 1, 15067. doi:10.1038/nrdp.2015.67
Kawakita, Y., Takeshima, M., Komatsu, T., Imanishi, A., Fujiwara, D., Itoh, Y., et al. (2022). Relationship between clozapine exposure and the onset of appendicitis in schizophrenia patients: A retrospective cohort study. BMC Psychiatry 22, 653. doi:10.1186/s12888-022-04312-4
Kuo, C.-J., Yang, S.-Y., Liao, Y.-T., Chen, W. J., Lee, W.-C., Shau, W.-Y., et al. (2013). Second-generation antipsychotic medications and risk of pneumonia in schizophrenia. Schizophr. Bull. 39, 648–657. doi:10.1093/schbul/sbr202
Lahdelma, L., and Appelberg, B. (2012). Clozapine-induced agranulocytosis in Finland, 1982-2007: Long-term monitoring of patients is still warranted. J. Clin. Psychiatry 73, 837–842. doi:10.4088/JCP.11m07244
Li, R., Ma, X., Wang, G., Yang, J., and Wang, C. (2016). Why sex differences in schizophrenia? J. Transl. Neurosci. (Beijing) 1, 37–42.
Mace, S., Dzahini, O., Cornelius, V., Langerman, H., Oloyede, E., and Taylor, D. (2022). Incident infection during the first year of treatment - a comparison of clozapine and paliperidone palmitate long-acting injection. J. Psychopharmacol. 36, 232–237. doi:10.1177/02698811211058973
Martini, F., Spangaro, M., Buonocore, M., Bechi, M., Cocchi, F., Guglielmino, C., et al. (2021). Clozapine tolerability in treatment resistant schizophrenia: exploring the role of sex. Psychiatry Res. 297, 113698. doi:10.1016/j.psychres.2020.113698
McClelland, E. E., and Smith, J. M. (2011). Gender specific differences in the immune response to infection. Arch. Immunol. Ther. Exp. Warsz. 59, 203–213. doi:10.1007/s00005-011-0124-3
Montastruc, J.-L., Sommet, A., Bagheri, H., and Lapeyre-Mestre, M. (2011). Benefits and strengths of the disproportionality analysis for identification of adverse drug reactions in a pharmacovigilance database. Br. J. Clin. Pharmacol. 72, 905–908. doi:10.1111/j.1365-2125.2011.04037.x
Mookhoek, E. J., and Loonen, A. J. M. (2004). Retrospective evaluation of the effect of omeprazole on clozapine metabolism. Pharm. World Sci. 26, 180–182. doi:10.1023/B:PHAR.0000026808.97403.05
Ohlis, A., Sörberg Wallin, A., Sarafis, A., Sjöqvist, H., MacCabe, J. H., Ahlen, J., et al. (2022). Clozapine treatment and risk of severe COVID-19 infection. Acta Psychiatr. Scand. 145, 79–85. doi:10.1111/acps.13379
Pardiñas, A. F., Nalmpanti, M., Pocklington, A. J., Legge, S. E., Medway, C., King, A., et al. (2019). Pharmacogenomic variants and drug interactions identified through the genetic analysis of clozapine metabolism. Am. J. Psychiatry 176, 477–486. doi:10.1176/appi.ajp.2019.18050589
Ponsford, M., Castle, D., Tahir, T., Robinson, R., Wade, W., Steven, R., et al. (2019). Clozapine is associated with secondary antibody deficiency. Br. J. Psychiatry 214, 1–7. doi:10.1192/bjp.2018.152
Rajagopal, S. (2005). Clozapine, agranulocytosis, and benign ethnic neutropenia. Postgrad. Med. J. 81, 545–546. doi:10.1136/pgmj.2004.031161
Remington, G., Addington, D., Honer, W., Ismail, Z., Raedler, T., and Teehan, M. (2017). Guidelines for the pharmacotherapy of schizophrenia in adults. Can. J. Psychiatry 62, 604–616. doi:10.1177/0706743717720448
Røge, R., Møller, B. K., Andersen, C. R., Correll, C. U., and Nielsen, J. (2012). Immunomodulatory effects of clozapine and their clinical implications: what have we learned so far? Schizophr. Res. 140, 204–213. doi:10.1016/j.schres.2012.06.020
Silveira, A. S. de A., Rocha, D. M. L. V., Attux, C. R. de F., Daltio, C. S., Silva, L. A. da, Elkis, H., et al. (2015). Patterns of clozapine and other antipsychotics prescriptions in patients with treatment-resistant schizophrenia in community mental health centers in São Paulo, Brazil. Archives Clin. Psychiatry (São Paulo) 42, 165–170. doi:10.1590/0101-60830000000069
Salimi, A., Alyan, N., Akbari, N., Jamali, Z., and Pourahmad, J. (2022). Selenium and L-carnitine protects from valproic acid-Induced oxidative stress and mitochondrial damages in rat cortical neurons. Drug Chem. Toxicol. 45, 1150–1157. doi:10.1080/01480545.2020.1810259
Sharrar, R. G., and Dieck, G. S. (2013). Monitoring product safety in the postmarketing environment. Ther. Adv. Drug Saf. 4, 211–219. doi:10.1177/2042098613490780
Shuman, M. D., Trigoboff, E., Demler, T. L., and Opler, L. A. (2014). Exploring the potential effect of polypharmacy on the hematologic profiles of clozapine patients. J. Psychiatr. Pract. 20, 50–58. doi:10.1097/01.pra.0000442937.61575.26
Steinert, T., and Jans, F. (2021). Six cases of perforated appendicitis during clozapine treatment. J. Clin. Psychiatry 82, 20cr13841. doi:10.4088/JCP.20cr13841
Taylor, D. M. (2004). Prescribing of clozapine and olanzapine: dosage, polypharmacy and patient ethnicity. Psychiatr. Bull. 28, 241–243. doi:10.1192/pb.28.7.241
Uppsala Center, (2023). WHO drug Insight. Available at: https://who-umc.org/whodrug/whodrug-global/applications/whodrug-insight/ (Accessed May 25, 2023).
Wagner, E., Siafis, S., Fernando, P., Falkai, P., Honer, W. G., Röh, A., et al. (2021). Efficacy and safety of clozapine in psychotic disorders-a systematic quantitative meta-review. Transl. Psychiatry 11, 487. doi:10.1038/s41398-021-01613-2
Wagner, S., Varet-Legros, M. G., Fabre, C., Montastruc, J. L., and Bagheri, H. (2011). Confounding factors for variation of clozapine plasma levels: drug interactions with proton pump inhibitor or infectious etiologies? Eur. J. Clin. Pharmacol. 67, 533–534. doi:10.1007/s00228-010-0925-z
Wang, K. N., Bell, J. S., Tan, E. C. K., Gilmartin-Thomas, J. F. M., Dooley, M. J., and Ilomäki, J. (2019). Proton pump inhibitors and infection-related hospitalizations among residents of long-term care facilities: A case-control study. Drugs Aging 36, 1027–1034. doi:10.1007/s40266-019-00704-6
Wiciński, M., Węclewicz, M. M., Miętkiewicz, M., Malinowski, B., Grześk, E., and Klonowska, J. (2017). Potential mechanisms of hematological adverse drug reactions in patients receiving clozapine in combination with proton pump inhibitors. J. Psychiatr. Pract. 23, 114–120. doi:10.1097/PRA.0000000000000223
Zanger, U. M., and Schwab, M. (2013). Cytochrome P450 enzymes in drug metabolism: Regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol. Ther. 138, 103–141. doi:10.1016/j.pharmthera.2012.12.007
Keywords: clozapine, infection, overdose, interaction, pharmacovigilance
Citation: Chrétien B, Brazo P, Da Silva A, Sassier M, Dolladille C, Lelong-Boulouard V, Alexandre J and Fedrizzi S (2023) Infections associated with clozapine: a pharmacovigilance study using VigiBase®. Front. Pharmacol. 14:1260915. doi: 10.3389/fphar.2023.1260915
Received: 18 July 2023; Accepted: 06 September 2023;
Published: 02 October 2023.
Edited by:
Thierry Trenque, Centre Hospitalier Universitaire de Reims, FranceReviewed by:
Brian J. Piper, Geisinger Commonwealth School of Medicine, United StatesCopyright © 2023 Chrétien, Brazo, Da Silva, Sassier, Dolladille, Lelong-Boulouard, Alexandre and Fedrizzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Basile Chrétien, Y2hyZXRpZW4tYkBjaHUtY2Flbi5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.