
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 16 November 2023
Sec. Pharmacoepidemiology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1252251
This article is part of the Research Topic Women in Pharmacoepidemiology: 2023 View all 4 articles
 Noémie Tanguay1,2
Noémie Tanguay1,2 Nadia Abdelouahab3
Nadia Abdelouahab3 Marie-Noelle Simard4,5
Marie-Noelle Simard4,5 Jean R. Séguin4,6Isabelle Marc2,7Catherine M. Herba4,8
Jean R. Séguin4,6Isabelle Marc2,7Catherine M. Herba4,8 Andrea A. N. MacLeod9Yohann Courtemanche2
Andrea A. N. MacLeod9Yohann Courtemanche2 William D. Fraser4
William D. Fraser4 Gina Muckle1,2*
Gina Muckle1,2*Introduction: Approximately 5.5% of pregnant women take antidepressants. Studies on prenatal exposure to antidepressants reported no association with child cognition, and inconsistent results with motor function and language development. A limitation has been the failure to adjust for prenatal maternal distress.
Objectives: Assess the associations between prenatal exposure to antidepressants and child development at age two, while adjusting for maternal depressive symptoms and stress during pregnancy. Explore indirect effects through birth complications and consider sex-specific associations.
Methods: This is an ancillary study of the 3D (Design Develop, Discover) Study initiated during pregnancy. Data on antidepressants were collected through medication logs spanning the entire pregnancy. Depressive symptoms and stress were assessed during pregnancy by self-reported questionnaires, motor and cognitive development with the Bayley Scales of Infant and Toddler Development (BSID-III), and language development with the MacArthur Communicative Development Inventories at age 2. Multiple linear regressions were used to assess the associations between exposure and developmental outcomes. Mediation models were used to assess indirect effects. Interaction terms were introduced to assess sex-specific associations.
Results: 1,489 mother-child dyads were included, of whom 61 (4.1%) reported prenatal antidepressant use. Prenatal exposure was negatively associated with motor development (B = −0.91, 95% CI -1.73, −0.09 for fine motor, B = −0.89, 95% CI -1.81, 0.02 for gross motor), but not with cognitive (B = −0.53, 95% CI -1.82, 0.72) and language (B = 4.13, 95% CI -3.72, 11.89) development. Adjusting for maternal prenatal distress only slightly modified these associations. No indirect effect or differential effect according to child sex were found.
Conclusion: This study supports evidence of a negative association between prenatal exposure to antidepressants and motor development at age two, after adjusting for maternal distress, but the effect size remains very small, with about only one BSID-III point lower in average.
Depression is characterized by depressed mood, loss of interest or pleasure, feelings of worthlessness, and/or weight, sleep, cognitive and/or behavioural changes (American Psychiatric Association, 2015). In pregnant women, a systematic review based on information available in 2019 estimates the worldwide prevalence of depression at 12.6%, as established by a structured clinical interview, but elevated depressive symptoms are reported by 22.5% when based on self-reported questionnaires (Yin et al., 2021).
When treating depression in pregnant women, it is necessary to consider the potential risks to the pregnancy and the foetus. The American Psychiatric Association and the Canadian Network for Mood and Anxiety Treatments clinical guidelines recommend that psychotherapy must be considered as first-line treatment, independently of the depression severity, and pharmacotherapy should be considered a second-line recommendation (American Psychiatric Association, 2010; MacQueen et al., 2016). The prevalence of antidepressant use during pregnancy is estimated at 5.5% in North America (Molenaar et al., 2020). In Quebec, for pregnancies occurring between 1998 and 2002, 3.7% of pregnant women took antidepressants during the first trimester, 1.6% during the second trimester, and 1.1% during the last trimester (Ramos et al., 2007).
Antidepressants traverse the placental barrier and may affect the foetus. SSRIs (selective serotonin reuptake inhibitors), the most commonly prescribed antidepressant, have been associated with increased extracellular serotonin concentrations (Rampono et al., 2009), potentially altering the development of the serotonergic circuitries of the foetus, leading to reduced endogenous production (Oberlander et al., 2009). Serotonin plays a major role in the developing brain and lower concentrations of endogenous serotonin could affect cognition, learning abilities and stress response (Gaspar et al., 2003). The serotonergic system is also involved in muscle tone and motor performances (Galbally et al., 2012).
Studies examining associations between prenatal exposure to antidepressant medications and birth outcomes provide empirical evidence of a greater risk for preterm births (Fitton et al., 2020; Vlenterie et al., 2021), inconsistent results with birthweight (Tak et al., 2017; Fitton et al., 2020), and a possible increased risk of cardiac malformations for paroxetine and fluoxetine (Fitton et al., 2020).
Evidence supporting negative associations with child development before 4 years of age are less abundant. Regarding motor development, two systematic reviews found no evidence of association between prenatal exposure to antidepressants and child development, or inconsistent results since negative, weak positive and absence of associations are all reported (Araujo et al., 2020; Al-Fadel and Alrwisan, 2021). One review however found a significant negative association (Prady et al., 2018). A meta-analysis was conducted and included studies published up to 07/2017 reporting primary data (excluding individual case studies) and including a control group. The results support significant negative associations with an overall occurrence of poorer motor outcomes [effect size (standardized mean difference) = 0.22, 95% CI 0.07, 0.37] (Grove et al., 2018). Regarding cognitive development, all three systematic reviews concluded no evidence of association with prenatal antidepressants (Prady et al., 2018; Araujo et al., 2020; Al-Fadel and Alrwisan, 2021). For language development, only one systematic review included more than one study with a language outcome and found no evidence of an association (Araujo et al., 2020).
However, an important limitation reported by authors is the absence of adjustment for prenatal maternal distress. Maternal depression, anxiety, and stress during pregnancy have all been shown to be negatively associated with offspring cognitive, motor, and language development (Rogers et al., 2020; Martucci et al., 2021) and it is expected that women taking antidepressants suffered from psychological distress. However, only a few studies of prenatal exposure to antidepressants have adjusted for prenatal maternal distress. For motor development, half of these studies reported negative associations [OR = 1.42, 95% CI 1.07-1.87 for being in a lower development category on the Age and Stages Questionnaire (Handal et al., 2016), and a mean difference of 1.1–1.2 points on the BSID gross motor scale (van der Veere et al., 2020)], while other studies did not (Nulman et al., 2002; Gustafsson et al., 2018). For cognitive development, most studies reported nonsignificant results (Nulman et al., 2002; Nulman et al., 2012; Johnson et al., 2016; Gustafsson et al., 2018) and only one reported a negative association (van der Veere et al., 2020). For language development, when adjusting for maternal distress, all studies obtained significant, but conflicting results (Nulman et al., 2002; Skurtveit et al., 2014; Johnson et al., 2016).
Our examination of the primary studies included in those systematic reviews and meta-analysis, and of more recent studies (Gustafsson et al., 2018; Galbally et al., 2021), lead to the observations that negative associations with child development outcomes are 1) mostly found in large sample size studies―most studies have limited statistical power to detect small to moderate associations due to small samples―, 2) when outcomes are reported by the mother, and 3) very few studies adjust for maternal distress during pregnancy, which can be associated with both the use of antidepressant and child developmental outcomes. Some of these limitations have already been highlighted (Araujo et al., 2020; Al-Fadel and Alrwisan, 2021).
The objective of this study is to assess the direct associations between prenatal exposure to antidepressants and child motor, cognitive and language development at 2 years of age, while adjusting for maternal distress during pregnancy through self-report of depressive symptoms and perceived stress. Secondary exploratory objectives include the examination of 1) an indirect effect through duration of gestation and birthweight, and 2) if the hypothesized associations differ by child sex since there is accumulating empirical evidence for sex difference vulnerabilities in studies focusing on developmental effects of utero exposure to environmental pollutants (Oulhote et al., 2020) and prenatal maternal distress (Sutherland and Brunwasser, 2018; Kumpulainen et al., 2023; Wu et al., 2023), and strong biological plausibility given the sexually dimorphic nature of prenatal development.
This project is an ancillary study of the 3D Cohort Study, a prospective study of Quebec’s pregnant women recruited during the first trimester (Fraser et al., 2016). It comprises data collected in case report form by research nurses, abstracted from obstetrical and neonatal hospital records, reported by mothers each trimester of pregnancy and postnatally through self-administered questionnaires, and direct child assessments carried out at one of the study centres. Women had to be between 18 and 47 years of age at the time of recruitment, and able to communicate in French or English. Exclusion criteria included current intravenous drug use, severe illness or life-threatening conditions, and multiple gestation pregnancies. Between May 2010 and August 2012, 2,366 women were recruited and followed in one of the nine collaborating hospital (see Fraser et al. (2016) for details). The 2-year follow-up comprises 1,580 families with an in-person child development evaluation (last follow-up March 2015). For our ancillary study, additional inclusion criteria included that the child be tested between 18 and 30 months of age, and a language development score obtained from French, English or Spanish test version from children being exposed to the test language at least 70% of the time. Children with medical conditions known to interfere with child development were excluded from our analyses. Our final sample includes 1,489 mother-child dyads (Figure 1), with a sample size for analyses ranging from 1,055 to 1,456 according to the developmental outcome (Supplementary Figure S1).
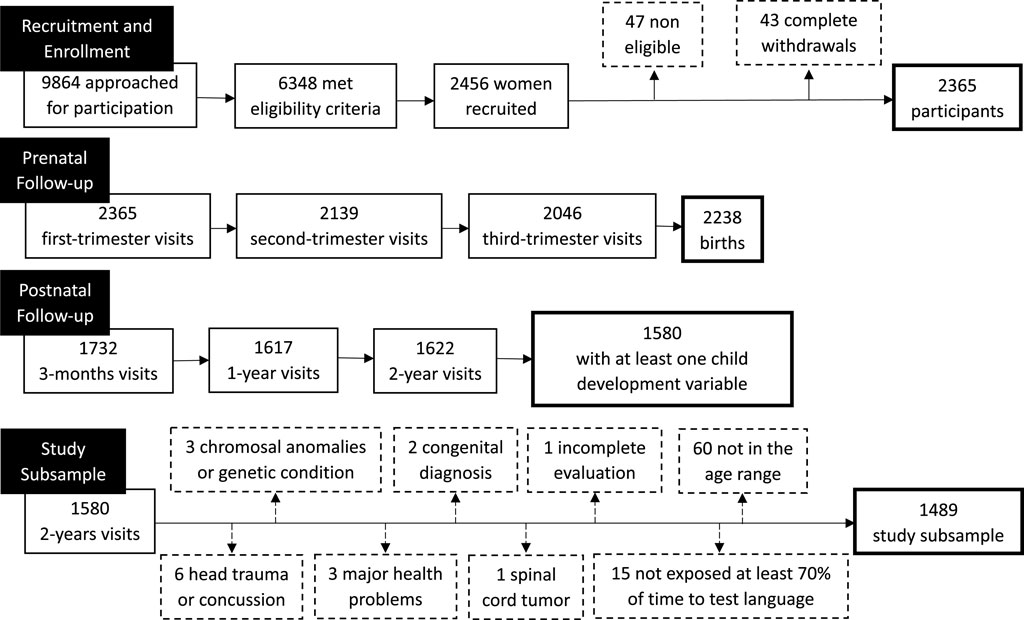
FIGURE 1. Flowchart for 3D Cohort Study participants included in the present study.
Use of antidepressants was collected at each trimester of pregnancy through a maternal medication log, and recorded via interviewer-administered questionnaires for the 3 months prior to pregnancy. Exposure was treated as a yes/no use of at least one antidepressant at any moment during pregnancy. Prenatal questionnaire at first trimester provided socio-demographic information including marital status (married or living with someone vs. not), annual family income in Canadian dollars (below 40,000$, 40,000$–79,999$, higher than 80,000$), maternal age (years), education (number of years) and parity before this pregnancy. Cigarette smoking and alcohol consumption (yes/no) were documented at each trimester of pregnancy. Gestation duration (weeks), birthweight (gr.), child sex were collected from hospital medical records. Child age (years) at time of testing was derived from dates of birth and of testing. Maternal distress during pregnancy was documented with two well-validated self-reported questionnaires: 1) the Center for Epidemiologic Studies—Depression Scale (Radloff, 1977) [CES-D - 10 items; Cronbach’s α = .89 (Björgvinsson et al., 2013)] completed at the first trimester of pregnancy, 2) the Perceived Stress Scale (PSS-4, Cronbach’s α = 0.79 (Karam et al., 2012; Cohen et al., 1983) completed during the second trimester.
Cognitive, fine and gross motor development were assessed at 2-years with the Bayley Scales of Infant and Toddler Development—Third Edition (BSID-III), administered in each research site by research nurses and research assistants dedicated to this project and trained by one licensed psychologist who was also responsible for post-training quality control. BSID-III items are rated 0 (skill not acquired) or 1 (skill acquired), and the subscales comprise 91, 66 and 72 items, respectively (Albers et al., 2006). A short version of the expressive vocabulary scale of the MacArthur Communicative Development Inventories (MCDI) (level II—form A) was handed over to the parent, mostly the mother, who returned the questionnaire by post or Internet; the respondents were asked to indicate the words said by the child on a list of 100 words (Fenson, 1993; Brodeur et al., 2016). The validity of the BSID-III is well established on general populations as the 3D cohort, and correlations of BSID-III scores with socioeconomic indicators, maternal distress, child sex, birthweight, gestation duration and MCDI score presented in Table 2 are providing information on its convergent validity in our sample. Higher BSID-III and MCDI scores reflected a more favourable development.
Comparative analyses (Welch’s t-test, chi-Square test of independence and Wilcoxon’s rank sum test) were carried out to compare the 3D participants included and not included in the present study. A DAG (directed acyclic graph) was developed to identify the confounders to be included in multivariate analyses (Shrier and Platt, 2008), from the list of the following potential variables selected for their hypothesized causal links based on previous studies and systematic reviews: child’s sex and age at testing, maternal age and parity at delivery, socioeconomic status (maternal education and annual family income), psychological distress (maternal depression and perceived stress), and substance use. We retained child’s sex and age at testing, maternal age, stress and depressive symptoms as mandatory covariates, as well as maternal education and annual family income as they were outlined by the DAG (see Supplementary Figure S2). Multiple linear regressions were used to assess the associations between prenatal exposure and child development, and four models were tested for each outcome: 1) minimally adjusted (child’s sex and age at testing, maternal age and education, annual family income); 2) adjusting for first trimester maternal depressive symptoms only; 3) adjusting for second trimester maternal stress only; and 4) fully adjusted for both depressive and stress symptoms. Fully adjusted mediation models were used to explore indirect effects explained by duration of gestation and birthweight, and interaction terms were introduced to assess differential effects according to child sex (moderation analysis). The E-value was estimated using VanderWeele and Ding (VanderWeele and Ding, 2017) method to address unmeasured confounding. Analyses were conducted using IBM SPSS Statistics 26 and R 4.1.0 (Rosseel, 2012; Kowarik and Templ, 2016; Team, 2022), and regressions were conducted using full information maximum likelihood estimation and bootstrapping (Lee and Shi, 2021).
The 3D Cohort protocol and procedures were approved by the Research Ethics Committees at the coordinating centre (Montreal CHU Sainte-Justine, approbation MP-21-2010-233) and in all study sites.
Sample characteristics are presented in Table 1. The study sample was largely composed of women in their late twenties/early thirties, living with a partner, highly educated and with a high annual family income. Few participants reported using tobacco during pregnancy, while more than half reported using alcohol. Few children were born preterm (5.4%

TABLE 1. Characteristics of study participants.
Missing data follows a MNAR pattern (missing not at random), and the three multivariate missing data patterns with the highest proportion of missing values are depressive symptoms missing (12.0%), both depressive symptoms and stress missing (5.1%), stress missing (3.9%) (see Supplementary Figure S3).
Correlations between study variables are presented in Table 2. Strongest intercorrelations were found among developmental indicators (r's: 0.31–0.58), gestation duration and birthweight (r = 0.56), depressive symptoms and perceived stress (r = 0.44). Antidepressant exposure was marginally associated with fine motor (r = −0.05), gross motor (r = −0.04) and cognitive development (r = −0.03), but not with language. Antidepressant exposure was related to maternal depressive symptoms (r = 0.11) and perceived stress (r = 0.16). Maternal perceived stress was related to cognitive (r = −0.11), fine motor (r = −0.07) and language (r = −0.09) development, but not with gross motor, while depressive symptoms were not associated with any of the child outcomes (r's: −0.04 to 0.04). Gestational age was associated with cognitive, fine motor and language development (r's: 0.06–0.12), but not with gross motor, while birthweight was related to cognition, fine motor and gross motor (r's: 0.06–0.08), but not with language. Gestational age and birthweight were not associated with antidepressant use.
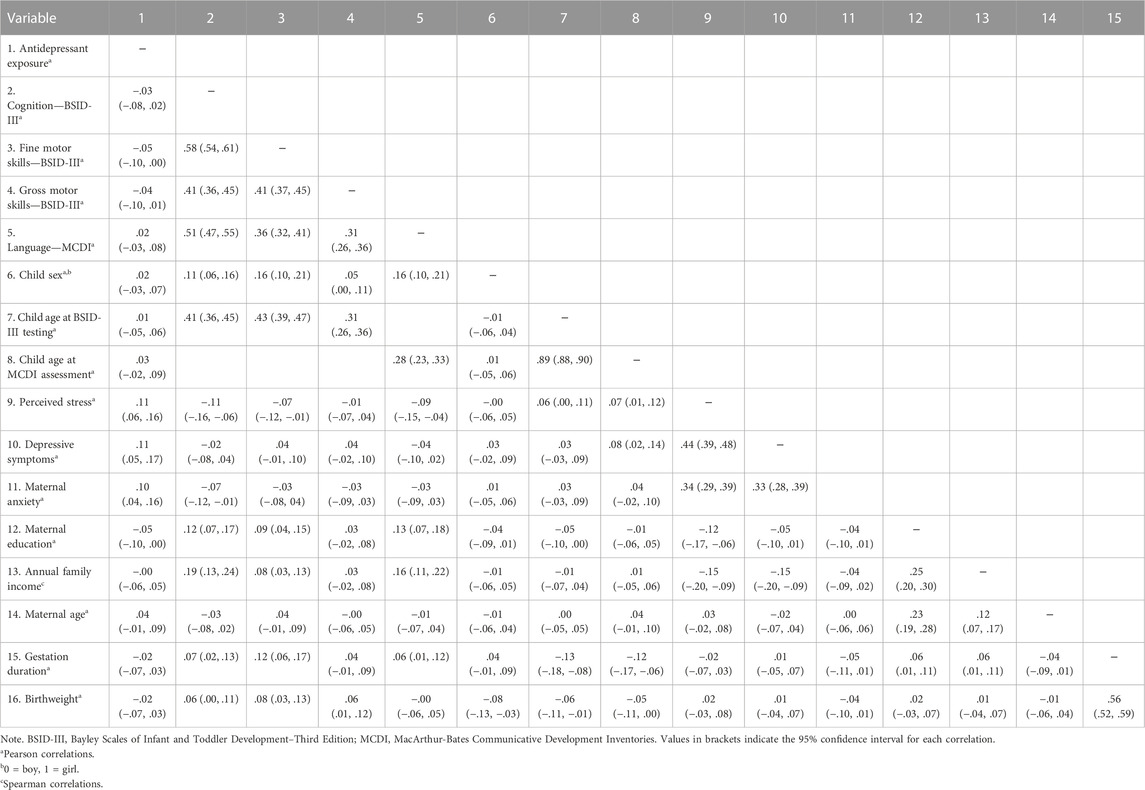
TABLE 2. Correlations of study variables.
Results of multiple linear regressions are presented in Table 3. There were no multivariable extreme data, and all assumptions were met. Antidepressant use was related to lower BSID-III fine motor score after adjusting for confounders (β = −0.26), and the strength of this association was slightly modified after inclusion of depressive symptoms (β = −0.29), maternal perceived stress (β = −0.23), but not when both were included (β = −0.26). Negative standardised linear regression coefficients with BSID-III gross motor score were in the same range although slightly lower. BSID-III cognitive and MCDI language development scores were unrelated to antidepressant use. The E-value has been estimated to address unmeasured confounding in the fully adjusted models. In the estimation of the association between exposure to antidepressants and fine motor development, the observed association could be explained away by an unmeasured confounder which would be associated with both the exposure and the developmental outcome by a risk ratio between 1.18 and 1.86-fold. As a comparison, all potential confounders included in our models have a combined E-value of 1.16.
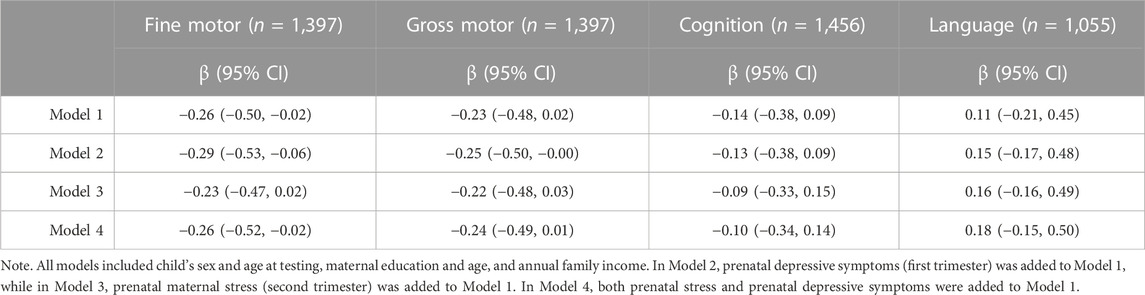
TABLE 3. Standardized linear regression coefficients of exposure to antidepressants (yes/no) on child’s development.
Results of mediation analyses shows that all indirect effects were non-significant (see Supplementary Figures S4–S11). No differences according to child sex were found in moderation analyses (data not shown).
We report negative associations between prenatal antidepressant exposure and fine and gross motor development, but no association with cognitive and language development. Inclusion of prenatal maternal distress only slightly attenuated the strength of these associations. These negative associations are of low magnitude since changes in BSID-III scores were only about one point in relation to exposure. No indirect association, mediated by gestation duration or birthweight, were found, nor differential effects according to child sex.
The sample size of this study is greater than most of the published studies to date, thus allowing for better statistical power. Among the 17 studies consulted, 13 included a sample of less than 800 participants (Nulman et al., 1997; Nulman et al., 2002; Simon et al., 2002; Casper et al., 2011; Gentile and Galbally, 2011; Nulman et al., 2012; Austin et al., 2013; Casper et al., 2003; Santucci et al., 2014; Johnson et al., 2016; Gustafsson et al., 2018; van der Veere et al., 2020; Galbally et al., 2021). We used prospective data providing antidepressant use and maternal distress at each trimester of pregnancy. The adjustment for prenatal distress addresses a major limitation of previous studies. Furthermore, our results appear to be robust against unmeasured confounding: the E-value analysis indicated that an unmeasured confounder would need to have a stronger association with exposure and developmental outcomes than all our covariates combined, which is unlikely since we controlled for well recognized and empirically supported confounding variables. Finally, the validated tool used to assess child cognitive, fine and gross motor development provided objective information independent from parental reports.
Antidepressant use during pregnancy was low (n = 61, 4.1%) in this study sample, which makes impossible to consider dose, duration, classes of antidepressants and timing of exposure in the analyses. Women who used antidepressants during pregnancy took them daily for most of their pregnancy. The medication log was not specific to antidepressants, and we assumed that if no antidepressant agents were reported, none were taken. Under-reporting due to social desirability could potentially lead to misclassifications in the non-exposed group, which may have reduced the strength of the negative associations reported. Finally, the assessment of language development only considered vocabulary knowledge, which do not represent the multidimensional aspect of language development, and, maternal report of child vocabulary may be prone to bias such maternal education, distress and use of antidepressant. Additionally, the testing of vocabulary in young children could strongly depend on the education/training given by parents and thus may not fully reflect the underlying deficits of the developing brain. One major limitation is the uncertainty regarding MCDI, given the mother’s application.
Antidepressant use during pregnancy was reported by 4.1% of the participants, which is lower than the North American prevalence (5.5%) (Molenaar et al., 2020), but similar to Quebec statistics reporting a prevalence of 3.7% during the first trimester, which later drops to less than 2% for the subsequent trimesters (Ramos et al., 2007).
Our findings indicate that antidepressants use during pregnancy is negatively related to fine and gross motor development, but not to cognitive and language development at 2 years of age, and that the associations with motor development are only slightly attenuated after consideration of prenatal maternal distress. The strength of these negative associations, in the range of −0.22 to −0.29, should be considered of low magnitude since changes in BSID-III motor scores are only about one point lower in relation to the exposure (data not shown). These results corroborate those of two other prospective cohort studies using the Ages and Stages Questionnaire (completed by the mother) and the BSID-III, and adjusting for maternal distress (Handal et al., 2016; van der Veere et al., 2020). They both adjusted for depressive symptoms and anxiety and found negative associations with child outcomes, and Van der Veere reported differences of 1.1-1.2 BSID-III gross motor score, which is comparable to the strength of associations found in our study. The strength of associations we observed (β from −0.22 to −0.29) are in same range of those from a meta-analysis: effect size of 0.22 (95% CI 0.07, 0.37) (Grove et al., 2018).
In our study, adjusting for depressive symptoms did not change the strength of the associations between antidepressant and motor development since depressive symptoms were unrelated to motor development scores, most likely due to the objective assessment of motor development instead of relying on maternal report. The strength of the antidepressant-fine motor association was only slightly reduced after adjusting for maternal perceived stress (from −0.26 to −0.23) and remained the same for gross motor development (−0.23 to −0.22). We expected a greater decrease in the antidepressant-outcome association considering known associations of prenatal perceived stress with foetal brain development (Wu et al., 2022) and child development (D'Souza et al., 2019; Polanska et al., 2017; Berthelon et al., 2021). This could be due to relatively low levels of maternal prenatal perceived stress (median PSS-4 score of 3 out of a potential maximum score of 16) in this economically advantaged sample, largely composed of mothers in couples (96%) who graduated from university.
The absence of an association between prenatal exposure to antidepressants and cognitive development at age 2 years is consistent with the current literature. Except for one prospective cohort study, which reported a mean difference of −0.8 points on BSID-III for exposed children (yes/no) after adjustment for depressive symptoms and anxiety (van der Veere et al., 2020), all other studies adjusting for prenatal maternal distress (depressive symptoms and/or anxiety) found no evidence of associations between prenatal exposure to antidepressants (yes/no, or duration of exposure for Johnson et al.) and cognition, as assessed with objective tools (e.g., BSID-II, Differential Ability Scales, McCarthy Scales of Children’s Abilities, Wechsler Preschool and Primary Scale of Intelligence) (Nulman et al., 2002; Nulman et al., 2012; Johnson et al., 2016; Gustafsson et al., 2018). In the present study, adjusting for depressive symptoms and maternal perceived stress did not modify the strength of the associations.
For language development, we found conflicting results in the literature with studies reporting negative (Skurtveit et al., 2014; Johnson et al., 2016) and positive associations (Nulman et al., 2002). Johnson et al. found negative associations in a sample of 178 participants (102 exposed), using the duration of exposure and language development assessed by an objective tool independent from maternal report, while adjusting for depressive symptoms (Johnson et al., 2016). Skurtveit et al. also found negative associations, using data on 51,748 participants (386 exposed), with language development as reported by the mother, while adjusting for depressive symptoms and anxiety (Skurtveit et al., 2014). On the other hand, Nulman et al. found positive associations with language assessed by an objective tool in a study group of 122 participants (86 exposed), while adjusting for depressive symptoms (Nulman et al., 2002). In the present study, we reported positive regression coefficients with large confidence intervals indicative of no associations. The instrument used was completed by the mother and the results are thus likely influenced by her subjectivity and moods. Negative associations between language scores and maternal perceived stress were indeed observed. Also, some children were exposed to more than one language, but evaluated only in one. Because we cannot be confident that the child’s language score truly represents linguistic abilities in these family situations, we limited our analyses to the sample of children exposed at least 70% of the time to the language of testing. This may have reduced the language score variability.
The absence of indirect effects in this study is most likely explained by the absence of associations between antidepressant exposure and the chosen mediators, gestation duration, and birthweight, although small associations are seen between these mediators and the developmental outcomes. Even if duration of gestation ≤37 weeks has been associated with antidepressant use during pregnancy, when studies adjust for depression, these associations are diminished, or even nullified (Tak et al., 2017). With regard to birthweight, the literature is inconsistent about its relationship with prenatal antidepressant exposure, but some systematic reviews report an absence of significant associations (Prady et al., 2018; Tak et al., 2017).
Finally, we found no differential effects depending on the child’s sex. Very few studies commented on sex dependant effects. Pedersen and its colleagues did report that boys were at greater risk for motor development delay, but the associations reported were non-significant (Pedersen et al., 2010).
This study provides evidence of negative associations between antidepressant use during pregnancy and subsequent motor development among 2 years old children. However, the effect sizes remain very small. No associations are reported with cognitive and language development. Even if adjustment for maternal depressive symptoms and prenatal perceived stress only slightly modified the antidepressant-motor development associations in our study, it remains important to consider these variables in other population studies providing larger samples and greater statistical power. Such larger size studies would also allow to consider dose, duration and classes of antidepressants, timing of exposure during the prenatal period, and to study whether obstetric complications may be considered as a mediator or a moderator of the relationship between prenatal exposure to antidepressant and later child development.
The datasets presented in this article are not readily available because any researcher interested in accessing the IRNPQEO Biobank and Database can contact the Biobank Manager. Requests to access the datasets should be directed to https://www.irnpqeo.ca/en/―email address of Biobank Manager: aXNhYmVsbGUua3JhdXNzLmhzakBzc3NzLmdvdXYucWMuY2E=.
The studies involving humans were approved by the 3D Cohort protocol and procedures were approved by the Research Ethics Committees at the coordinating centre (Montreal CHU Sainte-Justine, approbation MP-21-2010-233) and in all study sites. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
NT carried out this work as part of her doctorate in psychology. The design of the project was carried out in collaboration by NT and her research director, GM, who also contributed to the design, funding, and data collection of the 3D study, with WF and JRS. IM also contributed to data collection at one of the study sites. The manuscript was approved by the Scientific Publications Committee of IRNPQEO (Integrated Perinatal Research Network of Quebec and Eastern Ontario). All authors contributed to the article and approved the submitted version.
The data used for this research originate from the Integrated Research Network in Perinatology of Quebec and Eastern Ontario (IRNPQEO) Databank and/or Biobank. This work was supported by the Canadian Institutes of Health Research [funding reference number: CRI 88413]. NT work was supported by the Frederick-Banting and Charles-Best Graduate Scholarship from the Canadian Institutes of Health Research.
The authors thank Isabelle Krauss and Catherine Allard for their assistance.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1252251/full#supplementary-material
Albers, C. A., and Grieve, A. J.Test Review: Bayley, N (2006). Test review: Bayley, N. (2006). Bayley scales of infant and toddler development– third edition. San antonio, TX: harcourt assessment. J. Psychoeduc. Assess. 25 (2), 180–190. doi:10.1177/0734282906297199
Al-Fadel, N., and Alrwisan, A. (2021). Antidepressant use during pregnancy and the potential risks of motor outcomes and intellectual disabilities in offspring: a systematic review. Drugs Real World Outcomes 8 (2), 105–123. doi:10.1007/s40801-021-00232-z
American Psychiatric Association (2010). Practice guideline for the treatment of patients with major depressive disorder.
American Psychiatric Association (2015). “DSM-5: manuel diagnostique et statistique des troubles mentaux. 5e édition,” in Issy-les-Moulineaux (France: Elsevier Masson. lvii), 1114.
Araujo, J. S. A., Delgado, I. F., and Paumgartten, F. J. R. (2020). Antenatal exposure to antidepressant drugs and the risk of neurodevelopmental and psychiatric disorders: a systematic review. Cad. Saúde Pública 36 (2), e00026619. doi:10.1590/0102-311X00026619
Austin, M.-P., Karatas, J. C., Mishra, P., Christl, B., Kennedy, D., and Oei, J. (2013). Infant neurodevelopment following in utero exposure to antidepressant medication. Acta Paediatr. 102 (11), 1054–1059. doi:10.1111/apa.12379
Berthelon, M., Kruger, D., and Sanchez, R. (2021). Maternal stress during pregnancy and early childhood development. Econ. Hum. Biol. 43, 101047. doi:10.1016/j.ehb.2021.101047
Björgvinsson, T., Kertz, S. J., Bigda-Peyton, J. S., McCoy, K. L., and Aderka, I. M. (2013). Psychometric properties of the CES-D-10 in a psychiatric sample. Assessment 20 (4), 429–436. doi:10.1177/1073191113481998
Brodeur, M.-E., Sakulinskaya, E., and Trudeau, N. (2016). Les formes courtes québécoises des Inventaires MacArthur-Bates du développement de la communication (IMBDC-fc): en route vers une validation.
Casper, R. C., Fleisher, B. E., Lee-Ancajas, J. C., Gilles, A., Gaylor, E., DeBattista, A., et al. (2003). Follow-up of children of depressed mothers exposed or not exposed to antidepressant drugs during pregnancy. J. Pediatr. 142 (4), 402–408. doi:10.1067/mpd.2003.139
Casper, R. C., Gilles, A. A., Fleisher, B. E., Baran, J., Enns, G., and Lazzeroni, L. C. (2011). Length of prenatal exposure to selective serotonin reuptake inhibitor (SSRI) antidepressants: effects on neonatal adaptation and psychomotor development. Psychopharmacology 217 (2), 211–219. doi:10.1007/s00213-011-2270-z
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 24 (4), 385–396. doi:10.2307/2136404
D'Souza, S., Crawford, C. N., Buckley, J., Underwood, L., Peterson, E. R., Bird, A., et al. (2019). Antenatal determinants of early childhood talking delay and behavioural difficulties. Infant Behav. Dev. 57, 101388. doi:10.1016/j.infbeh.2019.101388
Fenson, L. (1993). MacArthur communicative development Inventories: user's guide and technical manual. Cengage Learning.
Fitton, C. A., Steiner, M. F. C., Aucott, L., Pell, J. P., Mackay, D. F., Fleming, M., et al. (2020). In utero exposure to antidepressant medication and neonatal and child outcomes: a systematic review. Acta Psychiatr. Scand. 141 (1), 21–33. doi:10.1111/acps.13120
Fraser, W. D., Shapiro, G. D., Audibert, F., Dubois, L., Pasquier, J. C., Julien, P., et al. (2016). 3D cohort study: the integrated research Network in Perinatology of Quebec and eastern Ontario. Paediatr. Perinat. Epidemiol. 30 (6), 623–632. doi:10.1111/ppe.12320
Galbally, M., Lewis, A., Gentile, S., Walker, S., and Buist, A. (2012). The biology of fetal exposure to serotonin reuptake inhibitors: Implications for neurodevelopment. Antidepressants: Pharmacology, Health Effects and Controversy, 1–26.
Galbally, M., Watson, S. J., Spigset, O., Boyce, P., Oberlander, T. F., and Lewis, A. J. (2021). Antidepressant exposure in pregnancy and child sensorimotor and visuospatial development. J. Psychiatric Res. 143, 485–491. doi:10.1016/j.jpsychires.2020.11.035
Gaspar, P., Cases, O., and Maroteaux, L. (2003). The developmental role of serotonin: news from mouse molecular genetics. Nat. Rev. Neurosci. 4 (12), 1002–1012. doi:10.1038/nrn1256
Gentile, S., and Galbally, M. (2011). Prenatal exposure to antidepressant medications and neurodevelopmental outcomes: a systematic review. J. Affect. Disord. 128 (1-2), 1–9. doi:10.1016/j.jad.2010.02.125
Grove, K., Lewis, A. J., and Galbally, M. (2018). Prenatal antidepressant exposure and child motor development: a meta-analysis. Pediatrics 142 (1), e20180356. doi:10.1542/peds.2018-0356
Gustafsson, H. C., Goodman, S. H., Feng, T., Choi, J., Lee, S., Newport, D. J., et al. (2018). Major depressive disorder during pregnancy: psychiatric medications have minimal effects on the fetus and infant yet development is compromised. Dev. Psychopathol. 30 (3), 773–785. doi:10.1017/S0954579418000639
Handal, M., Skurtveit, S., Furu, K., Hernandez-Diaz, S., Skovlund, E., Nystad, W., et al. (2016). Motor development in children prenatally exposed to selective serotonin reuptake inhibitors: a large population-based pregnancy cohort study. Bjog 123 (12), 1908–1917. doi:10.1111/1471-0528.13582
Johnson, K. C., Smith, A. K., Stowe, Z. N., Newport, D. J., and Brennan, P. A. (2016). Preschool outcomes following prenatal serotonin reuptake inhibitor exposure: differences in language and behavior, but not cognitive function. J. Clin. Psychiatry 77 (2), e176–e182. doi:10.4088/JCP.14m09348
Karam, F., Bérard, A., Sheehy, O., Huneau, M. C., Briggs, G., Chambers, C., et al. (2012). Reliability and validity of the 4-item perceived stress scale among pregnant women: results from the OTIS antidepressants study. Res. Nurs. Health 35 (4), 363–375. doi:10.1002/nur.21482
Kowarik, A., and Templ, M. (2016). Imputation with the R package VIM. J. Stat. Softw. 74 (7), 1–16. doi:10.18637/jss.v074.i07
Kumpulainen, V., Copeland, A., Pulli, E. P., Silver, E., Kataja, E. L., Saukko, E., et al. (2023). Prenatal and postnatal maternal depressive symptoms are associated with white matter integrity in 5-year-olds in a sex-specific manner. Biol. Psychiatry. In press. doi:10.1016/j.biopsych.2023.05.014
Lee, T., and Shi, D. (2021). A comparison of full information maximum likelihood and multiple imputation in structural equation modeling with missing data. Psychol. Methods 26 (4), 466–485. doi:10.1037/met0000381
MacQueen, G. M., Frey, B. N., Ismail, Z., Jaworska, N., Steiner, M., Lieshout, R. J. V., et al. (2016). Canadian Network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 6. Special populations: youth, women, and the elderly. Can. J. Psychiatry 61 (9), 588–603. doi:10.1177/0706743716659276
Martucci, M., Aceti, F., Giacchetti, N., and Sogos, C. (2021). The mother-baby bond: a systematic review about perinatal depression and child developmental disorders. Riv. Psichiatr. 56 (5), 223–236. doi:10.1708/3681.36670
Molenaar, N. M., Bais, B., Lambregtse-van den Berg, M. P., Mulder, C. L., Howell, E. A., Fox, N. S., et al. (2020). The international prevalence of antidepressant use before, during, and after pregnancy: a systematic review and meta-analysis of timing, type of prescriptions and geographical variability. J. Affect. Disord. 264, 82–89. doi:10.1016/j.jad.2019.12.014
Nulman, I., Koren, G., Rovet, J., Barrera, M., Pulver, A., Streiner, D., et al. (2012). Neurodevelopment of children following prenatal exposure to venlafaxine, selective serotonin reuptake inhibitors,or untreated maternal depression. Am. J. Psychiatry 169 (11), 1165–1174. doi:10.1176/appi.ajp.2012.11111721
Nulman, I., Rovet, J., Stewart, D. E., Wolpin, J., Gardner, H. A., Theis, J. G., et al. (1997). Neurodevelopment of children exposed in utero to antidepressant drugs. N. Engl. J. Med. 336 (4), 258–262. doi:10.1056/NEJM199701233360404
Nulman, I., Rovet, J., Stewart, D. E., Wolpin, J., Pace-Asciak, P., Shuhaiber, S., et al. (2002). Child development following exposure to tricyclic antidepressants or fluoxetine throughout fetal life: a prospective, controlled study. Am. J. Psychiatry 159 (11), 1889–1895. doi:10.1176/appi.ajp.159.11.1889
Oberlander, T. F., Gingrich, J. A., and Ansorge, M. S. (2009). Sustained neurobehavioral effects of exposure to SSRI antidepressants during development: molecular to clinical evidence. Clin. Pharmacol. Ther. 86 (6), 672–677. doi:10.1038/clpt.2009.201
Oulhote, Y., Lanphear, B., Braun, J. M., Webster, G. M., Arbuckle, T. E., Etzel, T., et al. (2020). Gestational exposures to phthalates and folic acid, and autistic traits in Canadian children. Environ. Health Perspect. 128 (2), 27004. doi:10.1289/EHP5621
Pedersen, L. H., Henriksen, T. B., and Olsen, J. (2010). Fetal exposure to antidepressants and normal milestone development at 6 and 19 months of age. Pediatrics 125 (3), e600–e608. doi:10.1542/peds.2008-3655
Polanska, K., Krol, A., Merecz-Kot, D., Jurewicz, J., Makowiec-Dabrowska, T., Chiarotti, F., et al. (2017). Maternal stress during pregnancy and neurodevelopmental outcomes of children during the first 2 years of life. J. Paediatr. Child Health 53 (3), 263–270. doi:10.1111/jpc.13422
Prady, S. L., Hanlon, I., Fraser, L. K., and Mikocka-Walus, A. (2018). A systematic review of maternal antidepressant use in pregnancy and short- and long-term offspring’s outcomes. Archives of Women's Mental Health 21 (2), 127–140. doi:10.1007/s00737-017-0780-3
Radloff, L. S. (1977). The CES-D Scale: a self-report depression scale for research in the general population. Appl. Psychol. Meas. 1 (3), 385–401. doi:10.1177/014662167700100306
Ramos, E., Oraichi, D., Rey, E., Blais, L., and Bérard, A. (2007). Prevalence and predictors of antidepressant use in a cohort of pregnant women. Bjog 114 (9), 1055–1064. doi:10.1111/j.1471-0528.2007.01387.x
Rampono, J., Simmer, K., Ilett, K. F., Hackett, L. P., Doherty, D. A., Elliot, R., et al. (2009). Placental transfer of SSRI and SNRI antidepressants and effects on the neonate. Pharmacopsychiatry 42 (3), 95–100. doi:10.1055/s-0028-1103296
Rogers, A., Obst, S., Teague, S. J., Rossen, L., Spry, E. A., Macdonald, J. A., et al. (2020). Association between maternal perinatal depression and anxiety and child and adolescent development: a meta-analysis. JAMA Pediatr. 174, 1082–1092. doi:10.1001/jamapediatrics.2020.2910
Rosseel, Y. (2012). Lavaan: an R package for structural equation modeling. J. Stat. Softw. 48 (2), 1–36. doi:10.18637/jss.v048.i02
Santucci, A. K., Singer, L. T., Wisniewski, S. R., Luther, J. F., Eng, H. F., Dills, J. L., et al. (2014). Impact of prenatal exposure to serotonin reuptake inhibitors or maternal major depressive disorder on infant developmental outcomes. J. Clin. Psychiatry 75 (10), 1088–1095. doi:10.4088/JCP.13m08902
Shrier, I., and Platt, R. W. (2008). Reducing bias through directed acyclic graphs. BMC Med. Res. Methodol. 8 (1), 70. doi:10.1186/1471-2288-8-70
Simon, G. E., Cunningham, M. L., and Davis, R. L. (2002). Outcomes of prenatal antidepressant exposure. Am. J. Psychiatry 159 (12), 2055–2061. doi:10.1176/appi.ajp.159.12.2055
Skurtveit, S., Selmer, R., Roth, C., Hernandez-Diaz, S., and Handal, M. (2014). Prenatal exposure to antidepressants and language competence at age three: results from a large population-based pregnancy cohort in Norway. Bjog 121 (13), 1621–1631. doi:10.1111/1471-0528.12821
Sutherland, S., and Brunwasser, S. M. (2018). Sex differences in vulnerability to prenatal stress: a review of the recent literature. Curr. Psychiatry Rep. 20 (11), 102. doi:10.1007/s11920-018-0961-4
Tak, C. R., Job, K. M., Schoen-Gentry, K., Campbell, S. C., Carroll, P., Costantine, M., et al. (2017). The impact of exposure to antidepressant medications during pregnancy on neonatal outcomes: a review of retrospective database cohort studies. Eur. J. Clin. Pharmacol. 73 (9), 1055–1069. doi:10.1007/s00228-017-2269-4
Team, R. C. R. (2022). A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing.
van der Veere, C. N., de Vries, N. K. S., van Braeckel, K. N. J. A., and Bos, A. F. (2020). Intra-uterine exposure to selective serotonin reuptake inhibitors (SSRIs), maternal psychopathology, and neurodevelopment at age 2.5years — results from the prospective cohort SMOK study. Early Hum. Dev. 147, 105075. doi:10.1016/j.earlhumdev.2020.105075
VanderWeele, T. J. P., and Ding, P. P. (2017). Sensitivity analysis in observational research: introducing the E-value. Ann. Intern. Med. 167 (4), 268–274. doi:10.7326/M16-2607
Vlenterie, R., van Gelder, M. M. H. J., Anderson, H. R., Andersson, L., Broekman, B. F. P., Dubnov-Raz, G., et al. (2021). Associations between maternal depression, antidepressant use during pregnancy, and Adverse pregnancy outcomes: an individual participant data meta-analysis. Obstetrics Gynecol. 138 (4), 633–646. doi:10.1097/AOG.0000000000004538
Wu, Y., Espinosa, K. M., Barnett, S. D., Kapse, A., Quistorff, J. L., Lopez, C., et al. (2022). Association of elevated maternal psychological distress, altered fetal brain, and offspring cognitive and social-emotional outcomes at 18 months. JAMA Netw. Open 5 (4), e229244. doi:10.1001/jamanetworkopen.2022.9244
Wu, Y., Zeng, F., Li, J., Jiang, Y., Zhao, S., Knibbs, L. D., et al. (2023). Sex-specific relationships between prenatal exposure to metal mixtures and birth weight in a Chinese birth cohort. Ecotoxicol. Environ. Saf. 262, 115158. doi:10.1016/j.ecoenv.2023.115158
Keywords: antidepressants, pregnancy, child development, cognition, motor skills, language
Citation: Tanguay N, Abdelouahab N, Simard M-N, Séguin JR, Marc I, Herba CM, MacLeod AAN, Courtemanche Y, Fraser WD and Muckle G (2023) Antidepressants use during pregnancy and child psychomotor, cognitive and language development at 2 years of age—Results from the 3D Cohort Study. Front. Pharmacol. 14:1252251. doi: 10.3389/fphar.2023.1252251
Received: 03 July 2023; Accepted: 30 October 2023;
Published: 16 November 2023.
Edited by:
Tatiane Da Silva Dal Pizzol, Federal University of Rio Grande do Sul, BrazilReviewed by:
Anne-Laure Sutter-Dallay, Centre Hospitalier Charles Perrens, FranceCopyright © 2023 Tanguay, Abdelouahab, Simard, Séguin, Marc, Herba, MacLeod, Courtemanche, Fraser and Muckle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gina Muckle, Z2luYS5tdWNrbGVAY3JjaHVkZXF1ZWJlYy51bGF2YWwuY2E=, Z2luYS5tdWNrbGVAcHN5LnVsYXZhbC5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.