 Dengjianyi Xu
Dengjianyi Xu Yucong Zhang
Yucong Zhang Jian Bai
Jian Bai Huixing Yuan1
Huixing Yuan1 Tao Wang
Tao Wang Jihong Liu
Jihong Liu Wen Song
Wen Song Delin Ma
Delin Ma
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pharmacol. , 16 August 2023
Sec. Ethnopharmacology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1232774
This article is part of the Research Topic Applications of Herbal Medicine in Metabolic and Degenerative Diseases of Aging View all 7 articles
Phosphodiesterase-5 inhibitors (PDE5-i) have been widely used in clinical practice for the treatment of erectile dysfunction (ED). However, due to its suboptimal therapeutic effects and side effects, it is necessary to develop new medicines for ED treatment. Botanical drugs have been widely investigated as potential ED treatment drugs and have shown promising therapeutic effects. This review summarized 34 studies, including five botanical drugs with PDE5 inhibitory activity, seven botanical drugs without PDE5 inhibitory activity, and six mixed botanical drugs. The results of clinical studies regarding the aforementioned botanical drugs and relevant mechanisms are summarized in this study. It is necessary to conduct high-quality clinical trials to verify the dosage, targeted patients and therapeutic effects, and further pharmacology experiments are also needed to identify the active compounds.
Erectile dysfunction (ED) is the persistent or recurrent inability to achieve or maintain an sufficient erection for satisfying sexual intercourse requirements (Sin et al., 2021). Approximately 52% of non-institutionalized men aged 40–70 years were reported to suffer from some degree of ED, and the prevalence of ED is predicted to reach 322 million cases by 2025 (Sin et al., 2021).
The physiological basis of penile erection is the dilation of the penile artery and the relaxation of the trabecular corpus cavernosum. When the penile artery and the smooth muscle in the trabecular region contract, the penis is in a relaxed state. In contrast, when the penile artery and the smooth muscle in the trabecular bone relax, the penis is in an erection state. The nitric oxide/cyclic guanosine monophosphate (NO/cGMP) signalling pathway plays an important role in the physiological basis of penile erection. After receiving sexual stimulation, NO is released from neurons and vascular endothelial cells in the penis sponge. Then, NO activates guanylate cyclase (GC) in the smooth muscle cells of the cavernous body. GC can catalyse the transformation of guanosine triphosphate (GTP) into cGMP. cGMP can activate protein kinase G (PKG), which will reduce the flow of Ca2+ into smooth muscle cells. When Ca2+ in the smooth muscle cells decreases, the smooth muscle cells of the cavernous body relax, and blood flows into the cavernous sinus increase. This process will finally cause the erection of the penis. In this process, PDE5 can breakdown cGMP into inactive guanosine-5′-monophosphate (5′-GMP), resulting in an increase in the flow of Ca2+ into smooth muscle cells, thus inhibiting penile erection (Anand Ganapathy et al., 2021).
Currently, the mainstream pharmacological treatment for ED is phosphodiesterase-5 inhibitors (PDE5-i). By inhibiting PDE5, the breakdown of cGMP is suppressed, which promotes penile erection. At present, the commonly used PDE5-i in clinical practice are avanafil, sildenafil, tadalafil, and vardenafil. However, the therapeutic effects of PDE5-i are not satisfactory. It has been reported that PDE5-i showed efficacy in only approximately 70% of patients, which is significantly lower in harder-to-treat subpopulations (Anand Ganapathy et al., 2021). Meanwhile, the adverse events of PDE5-i should also be noted. As the NO/cGMP signalling pathway exists in many different tissues and cells, such as the urinary system, respiratory system, digestive system, visual system, central nervous system and immune system (Anand Ganapathy et al., 2021), PDE5-i can also cause side effects in these systems. Common adverse events of PDE5-i include flushing and headaches (Sudyka and Wick, 2021), while more serious side effects may include non-arteritic anterior ischemic optic neuropathy (NAION), hearing loss, nasopharyngitis and priapism (Anand Ganapathy et al., 2021).
Overall, it is necessary to develop new drugs for the treatment of ED, and botanical drugs can provide important sources. Many botanical drugs have been used as medicines to treat diseases for centuries. Among them, botanical drugs are used as “aphrodisiacs” when treating ED. Even today, many plants are still used as “aphrodisiacs” to enhance libido, treat ED, and other purposes. This article summarizes the clinical research results and mechanisms of 12 single botanical drugs and 6 mixed botanical drugs.
In this review, botanical drugs were categorized based on whether they were found to have PDE5 inhibitory activity (Tables 1, 2). The possible mechanisms of the non-PDE5 inhibitor botanical drugs were also discussed.

TABLE 1. Botanical drugs with phosphodiesterase-5 inhibitory activity.
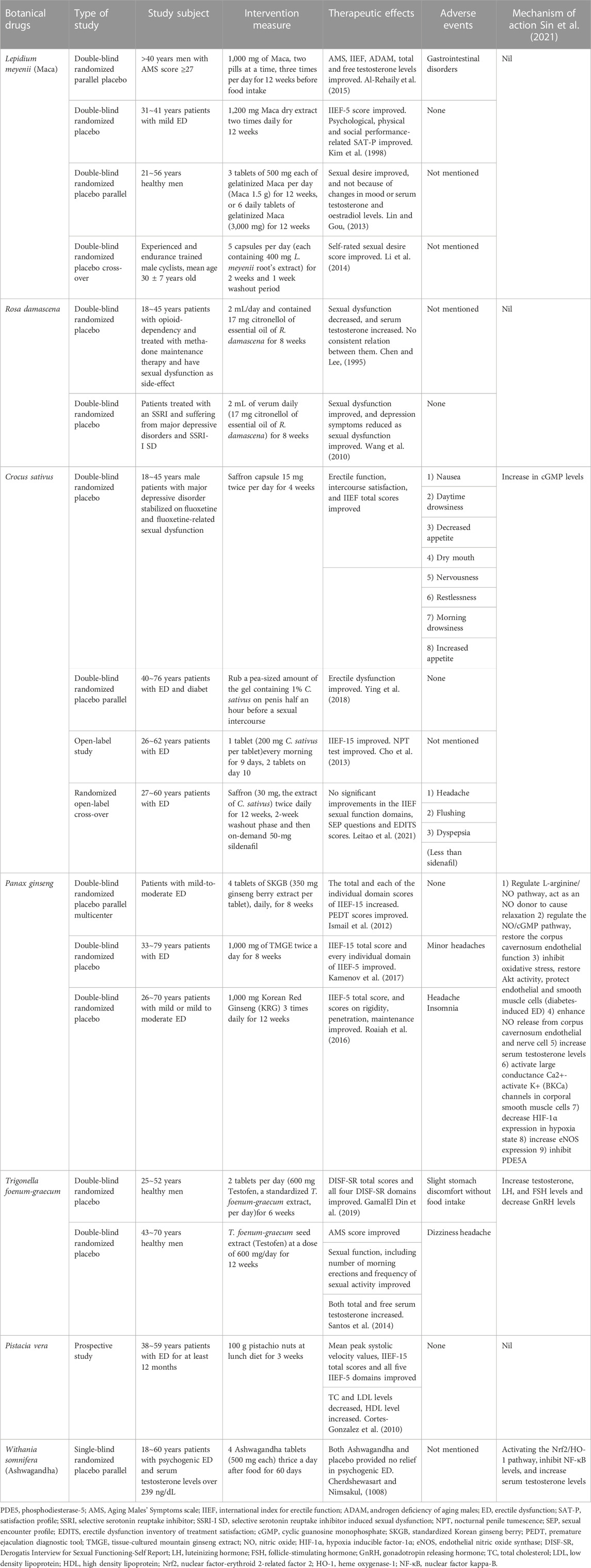
TABLE 2. Botanical drugs without phosphodiesterase-5 inhibitory activity.
Among 12 single botanical drugs, 5 plants show PDE5 inhibitor activity, while 7 do not (Anand Ganapathy et al., 2021; Sin et al., 2021). Apart from PDE5 inhibitory activity, the potential anti-ED mechanisms of the botanical drugs are as follows: 1) regulating NO-related pathways, 2) activating the nuclear factor-erythroid 2-related factor 2/heme oxygenase-1 (Nrf2/HO-1) signaling pathway and inhibiting nuclear factor kappa-B (NF-κB), and 3) increasing testosterone levels. As mentioned above, through the NO/cGMP pathway, increasing NO can enhance cavernosal smooth muscle relaxation and penile erection. NO is synthesized from L-arginine. NO synthase isoforms, neuronal nitric oxide synthase, endothelial nitric oxide synthase (eNOS), and inducible NOS are the main enzymes responsible for the synthesis of NO. The Nrf2/HO-1 signalling pathway plays a key role in the oxidative stress response, and Nrf2 is a significant transcription factor that promotes the expression of many antioxidant genes. HO-1 is an inducible isoform protein and can be induced by oxidative stress and many other conditions. NF-κB is an enhancer-binding transcription factor and participates in the immune response, cell proliferation and apoptosis. By activating the Nrf2/HO-1 pathway and inhibiting NF-κB, oxidative stress, an important factor in the development of ED, can be inhibited. Testosterone also plays a significant role in penile erection function in central and peripheral ways. Thus, increasing testosterone has positive effects on erectile function.
Among the plants with PDE5 inhibitory activity listed in Table 1, Kaempferia parviflora Wall. ex Baker (Zingiberaceae), Tribulus terrestris L. (Zygophyllaceae), and Eurycoma longifolia Jack (Simaroubaceae) show activities other than PDE5 inhibitors (Anand Ganapathy et al., 2021; Sin et al., 2021).
K. parviflora has been used in Thai traditional medicine to treat various diseases. It is believed by the locals that it could improve male erectile function. However, the subjective experience by users is not sufficient, and some studies have been conducted. There are indeed some active ingredients in K. parviflora that may improve erectile function. 3,5,7,3’,4’-Pentamethoxyflavone, an active ingredient of K. parviflora, can act as an L-type Ca2+ channel inhibitor to reduce intracellular Ca2+ to induce relaxation of the isolated human cavernosum (Jansakul et al., 2012). In Sprague‒Dawley rats (S-D rats), a 95% v/v ethanol extract of K. parviflora containing phenols as its major component, and flavonoids as its minor component increased blood flow in the testis (Chaturapanich et al., 2008).
T. terrestris has been recognized as a botanical drug with anti-inflammatory, antidiabetic and anticancer functions. T. terrestris has multiple effects that contribute to erectile function. A study used human platelets as a rich source of PDE enzymes, in which an 80% v/v methanol extract of T. terrestris showed cGMP PDE inhibitory activity (Khanavi et al., 2012). In addition, protodioscin in T. terrestris increased serum testosterone, dehydroepiandrosterone sulfate (DHEAS) and dihydrotestosterone (DHT) levels in baboons, rhesus monkeys, New Zealand white rabbits, and S-D rats. These androgens are crucial not only for the development of male external genitalia and male secondary sexual characteristics, but also for sexual desire and nocturnal penile erections (Gauthaman and Ganesan, 2008). Moreover, a study found that 70% v/v methanol extract of T. terrestris activated the Nrf2/HO-1 pathway, inhibited NF-κB in reproductive tissues, and increased serum testosterone levels in S-D rats. In this study, researchers showed that T. terrestris can inhibit the development of ED in an antioxidant way (Sahin et al., 2016). Similarly, in the corpus cavernosum of New Zealand white male rabbits, a 90% v/v methanol extract of T. terrestris regulated the NO/NOS pathway and relaxed the corpus cavernosum endothelium. By activating the NO/NOS pathway in the corpus cavernosum endothelium, NO was increased, and the NO/cGMP pathway was activated (Do et al., 2013).
E. longifolia, also named Tongkat Ali by locals in Malaysia, is a well-known botanical drug used as an aphrodisiac. Animal studies found that E. longifolia was able to improve libido and erectile function (Chiou and Wu, 2012). A β-carboline alkaloid, isolated from E. longifolia, 9-hydroxycanthin-6-one, was found to interfere with Ca2+ mobilization to relax the smooth muscle tension of the corpus cavernosum and seminal vesicle in the corpus cavernosum of S-D rats (Chiou and Wu, 2012). In addition, a dichloromethane (DCM) subfraction of 95% v/v ethanol tincture extract of E. longifolia antagonized angiotensin II (Ang II) induced contraction via inhibition of Ang II type l receptor and enhanced bradykinin (BK)-induced relaxation through inhibition of acetylcholinesterase (ACE) in rat corpus cavernosum. BK can induce corpus cavernosum relaxation, and Ang II can induce corpus cavernosum contraction. The renin-angiotensin system in the corpus cavernosum is important for maintaining corpus cavernosal tone (Tee et al., 2017). Moreover, some phenolic-rich extracts from E. longifolia, containing ellagic acid, rutin and quercetin, were reported to inhibit PDE5, arginase and ACE in penile tissues of Wistar albino rats (Oboh et al., 2018).
Four plants that may promote erectile function, including Withania somnifera (L.) Dunal (Solanaceae), Trigonella foenum-graecum L. (Fabaceae), Crocus sativus L. (Iridaceae) and Panax ginseng C.A.Mey. (Araliaceae) (Sin et al., 2021) (Table 2).
W. somnifera is an important botanical drug in traditional Indian medicine. It is reported to have anticancer, antioxidant, antistress, and immunomodulatory functions. In one study, 70% v/v methanol extract of W. somnifera was found to activate the Nrf2/HO-1 pathway, inhibit the NF-κB level in reproductive tissues of S-D rats, and increase serum testosterone levels in S-D rats (Sahin et al., 2016).
Seeds of T. foenum-graecum contain high level polyphenolic flavonoids, which possess reproductive protective effects and antioxidant, antidiabetic and anti-inflammatory functions. Vitexin, an active flavonoid of T. foenum-graecum, may modulate the hypothalamus-pituitary-gonadal axis to decrease serum gonadotropin releasing hormone (GnRH) levels, increase serum luteinizing hormone (LH) and follicle-stimulating hormone (FSH) levels, and increase serum testosterone levels in streptozotocin-induced diabetic mice. Therefore, vitexin may regulate androgen generation, enhance sex performance, and improve diabetic-induced fertility impairments (Li et al., 2019).
C. sativus is widely used in Iran, India, Greece, Spain, and Italy. It is believed by locals that it has an aphrodisiac effect (Modabbernia et al., 2012). In one study, the hexane fraction from the alcoholic extract of C. sativus increased cGMP levels in Wistar rats. This indicates that C. sativus might have active ingredients that can improve erectile function by increasing cGMP levels in corporal smooth muscle cells (Al-Rehaily et al., 2015).
P. ginseng is one of the most famous and most important botanical drugs in traditional Chinese medicine. It is believed to have multiple benefits for keeping healthy and has been used for thousands of years in China. Saponins have been found to be the major active ingredients in P. ginseng, which is responsible for the therapeutic effects. Multiple kinds of ginsenosides are considered to be the major active ingredients of saponins. A large number of studies have been performed to determine the mechanisms of P. ginseng, and some of them focused on reproductive effects. Saponins can regulate the L-arginine/NO pathway and act as NO donors to cause relaxation in the corpus cavernosum isolated from New Zealand White rabbits, regulate the NO/cGMP pathway and restore corpus cavernosum endothelial function in S-D rats, inhibit oxidative stress, restore Akt activity, and protect endothelial and smooth muscle cells in streptozotocin-induced diabetic rats (Kim et al., 1998; Lin and Gou, 2013; Li et al., 2014). Ginsenosides, the active ingredient complex of P. ginseng, enhanced NO release from corpus cavernosum endothelial and nerve cells in the corpus cavernosum of New Zealand white male rabbits in vitro (Chen and Lee, 1995). Ginsenoside Rg1 increased serum testosterone levels and regulated the NO/cGMP pathway in the corpus cavernosum of Kunming mice and New Zealand rabbits (Wang et al., 2010). Ginsenoside Rg3 activated large conductance Ca2+-activated K+ (BKCa) channels in rat brain BKCa channels (Choi et al., 2011). Ginsenosides Rk1, Rk3, Rg5, and Rh4, the active ingredient complex of P. ginseng, inhibited PDE5A in ICR mice and primary corpus cavernosum smooth muscle cells. Rg5 also decreased hypoxia inducible factor-1α (HIF-1α) expression in hypoxic state and increased eNOS expression (Ying et al., 2018). P. ginseng berry extract GB0710, containing ginsenoside Re as a major component and ginsenosides Rb1, Rb2, Rc, Rd, Rg1, and Rg2 as minor components, regulated the NO/cGMP pathway to enhance relaxation in rabbit corpus cavernosum in vitro and S-D rats in vivo (Cho et al., 2013). In summary, by increasing NO and cGMP levels in the corpus cavernosum, P. ginseng relaxed corpus cavernosum smooth muscles and thus improved erectile function. P. ginseng also showed therapeutic effects on ED by its antioxidant and antistress functions.
Notably, the majority of studies did not solely study one single identified bioactive substance of plants. They studied crude plant extracts or semipurified fractions, both of which are mixtures of active substances. Some active substances may produce a synergistic action. Furthermore, some environmental factors, such as temperature, humidity and soil composition undergo alterations, may influence the presence and concentration of active substances within botanical drugs. These facts could in some way explain the following phenomenon: the pharmacological mechanisms for the same botanical drug varied from studies with different extraction methods. For example, three studies of T. terrestris used 70%, 80%, and 90% v/v methanol extracts. Researchers found that 70% methanol v/v extract activated the Nrf2/HO-1 pathway, inhibited NF-κB levels and increased serum testosterone levels, 80% v/v methanol extract inhibited PDE, and 90% v/v methanol extract regulated the NO/NOS pathway and corpus cavernosum endothelium. Two studies of P. ginseng used total ginsenosides and ginsenosides Rk1, Rk3, Rg5, and Rh4. Researchers found that total ginsenosides activated large conductance Ca2+-activated K+ (BKCa) channels in corporal smooth muscle cells, while ginsenosides Rk1, Rk3, Rg5, and Rh4 inhibited PDE5A. Some studies analysed the pharmacological mechanisms of specific active substances, such as crocin in C. sativus and ginsenoside Rg1 in P. ginseng.
The results of two clinical trials (randomized, double-blind, placebo-controlled) on E. longifolia significantly increased International Index of Erectile Function (IIEF) scores (Ismail et al., 2012; Leitao et al., 2021). Additionally, one of the studies found that E. longifolia increased serum testosterone levels, which was not reported in preclinical experiments. In this study, 45- to 49-year-old patients with androgen deficiency of aging males (ADAM) (total testosterone ≤ 346 ng/dL) were enrolled (Leitao et al., 2021). Moreover, another study also found that interventional subjects (30–55-year-old healthy men) with Body Mass Index (BMI) ≥ 25 kg/m2 showed significant improvement in fat mass loss after E. longifolia treatment (p = 0.008) (Ismail et al., 2012). The E. longifolia capsule in one clinical trial was produced by a local compounding pharmacy, containing 200 mg of standardized dry extract [2-dihydro-18-dedihydrolongilactone: 0.32% (w/w); 9-hydroxycanthin-6-one 0.49% (w/w); Eurycomanone: 1.21% (w/w); total protein: 26.3%; total polysaccharide: 28.8% ⋅ glycosaponin: 44.2%]. The duration of this study spanned a period of 6 months. Forty-five patients were recruited, and 8 dropped out (Leitao et al., 2021). The E. longifolia capsule in the other clinical trial contained 300 mg of a special freeze-dried water extract of E. longifolia root containing 75 mg of active ingredients. The duration of this study spanned a period of 3 months. A total of 109 patients were recruited (Ismail et al., 2012).
There are four clinical trials on T. terrestris. Three of them found that T. terrestris significant improved ED (Roaiah et al., 2016; Kamenov et al., 2017; GamalEl Din et al., 2019), while one prospective, randomized, double-blind, placebo-controlled study did not, which may be because of the limited intervention period (Santos et al., 2014).
For 40–70-year-old patients with partial ADAM (PADAM) who mainly complained of ED and low libido, one before-after study found that T. terrestris (250 mg per dose, three times per day) increased both total and free serum testosterone levels (p = 0.026, p = 0.034, respectively), and there was a significant correlation between the increase in serum testosterone levels and the improvement in IIEF-5 scores (total testosterone: p = 0.001 and 0.054, before, p = 0.003 and 0.013, after; free testosterone: p = 0.001 and 0.025, before, p = 0.013 and 0.024, after). However, there were only 30 study subjects enrolled without control group. In this study, T. terrestris was collected from natural habitats during flowering. After air drying, rinsing with water, drying after evaporation of the solvent, powdering, extraction with 500 ml of 70% ethanol (or methanol or acetonitrile or hexane), and evaporation to dryness, the final dry extract was obtained. The duration of this study spanned a period of 3 months (Roaiah et al., 2016).
One randomized, double-blind, placebo-controlled study found that T. terrestris improved libido in patients with low sexual desire (intercourse satisfaction: p = 0.0005; orgasmic function, p = 0.0325; sexual desire: p = 0.0038; overall satisfaction: p = 0.0028). In this study, patients were required to orally intake Tribestan (Sopharma AD), an botanical medicinal product of Bulgarian origin, standardized with respect to furostanol saponins, calculated against protodioscin. Each Tribestan tablet contained 250 mg of the active substance T. terrestris herbal extractum siccum, and the content of furostanol saponins was no less than 112.5 mg. Moreover, it was reported that T. terrestris growing in different geographic regions of the world showed differences in the saponin content and the saponin composition, and T. terrestris used in this study was reported to have a high content of furostanol saponins of the diosgenin type. Patients aged 18–65 years with mild or moderate ED with or without hypoactive sexual desire disorder were enrolled. The duration of this study spanned a period of 3 months. A total of 180 patients were recruited, and 8 dropped out (Kamenov et al., 2017).
It is also worth noting that one randomized, single-blind, placebo-controlled study found that T. terrestris might slightly increase total Prostate Specific Antigen (PSA-t) levels (p = 0.007). In this study, 70 patients aged 40–70 years who suffered from ED and partial androgen deficiency (total testosterone < 3.5 ng/mL) were enrolled. They were required to take T. terrestris capsules (each containing 250 mg T. terrestris extracts) three times daily for 3 months. The T. terrestris extracts were standardized to contain no more than 45% steroidal saponins, but the detail process for the extraction was not mentioned in the study (GamalEl Din et al., 2019).
In two studies on B. superba, the result of one open-label study showed that B. superba did not improve ED over the sildenafil group (Cortes-Gonzalez et al., 2010). It is worth noting that in this study, 100 mg of B. superba extract was given 1–2 h before each sexual encounter (Cortes-Gonzalez et al., 2010). However, in another study, B. superba was given with a larger dose regularly per day (Cherdshewasart and Nimsakul, 1008). In fact, in most studies, the experimental drug or placebo was given 1–3 times daily, rather than just before sexual intercourse. In addition, B. superba capsules in this study were obtained from BioC Ltd., Stockholm Sweden, a natural health product supplier. Researchers believed that PDE5-i was blended in the B. superba capsule. Furthermore, this study was not randomized, double-blind or placebo-controlled. Only 33 patients aged 42–78 years took B. superba capsules for only 1 week, and 1 patient dropped out. The period intervention and the sample size were limited (Cortes-Gonzalez et al., 2010).
Moreover, in the randomized, double-blind, placebo-controlled study, although B. superba did not increase serum testosterone levels, it did significantly improve ED symptoms and increase IIEF-5 scores, especially in domains 4 (almost never or never able to maintain erection after penetration) and 5 (difficult to maintain erection to completion of intercourse) (p < 0.05 and p < 0.01, respectively). In this study, B. superba was collected from Lampang Province. Their fresh tubers were cleaned, sliced into pieces, dried in a hot air oven, ground into fine powder, and passed through 100 mesh sieves. The powder was finally filled into capsules at 250 mg/capsule. 30–70 years old patients with ED were enrolled and required to orally take 2 capsules per day for the first 4 days and 4 capsules per day for the rest of the time. The duration of this study spanned a period of 3 months. 39 patients were recruited, and 8 dropped out (Cherdshewasart and Nimsakul, 1008).
It should be noted that the study subjects in both clinical trials were limited. In one study, 33 study subjects were included (Cortes-Gonzalez et al., 2010), while 39 study subjects were included and 8 dropped out in another study (Cherdshewasart and Nimsakul, 1008).
Two clinical trials on G. biloba found that it did not improve ED symptoms (Kang et al., 2002; Wheatley, 2004). However, it is worth noting that both studies enrolled patients with sexual dysfunction caused by antidepressant drugs, especially selective serotonin reuptake inhibitors (SSRIs). Whether G. biloba has effect on other types of ED needs to be confirmed by more clinical trials.
In a randomized, triple-blind, placebo-controlled study, 24 patients aged 23–66 years were included, and 3 dropped out (Wheatley, 2004). In the randomized, double-blind, placebo-controlled study, thirty-seven patients aged 36–60 years were included, and 12 dropped out. Researchers believed that selection bias occurred in this study because some patients who subjectively experienced no sexual improvement did not participate in the second-month trial (Kang et al., 2002).
An open-label study on K. parviflora found that KaempMax™ (a K. parviflora rhizome extract standardized to 5% DMF) significantly improved the total score of IIEF (p = 0.0067), the score of erectile dysfunction domain (p = 0.0269), and the score of intercourse satisfaction domain (p = 0.0296) (Stein et al., 2018). Only 14 generally healthy males aged 50–68 years with self-reported mild ED were enrolled without control group (Stein et al., 2018).
Among the four randomized, double-blind placebo-controlled clinical trials regarding L. meyenii (Maca), two clinical trials found that L. meyenii significantly improved of IIEF (p < 0.001), International Prostatic Symptom Score (IPSS) (p = 0.001), Aging Males’ Symptoms scale (AMS) (p < 0.001), Androgen Deficiency in the Aging Males (ADAM) (p < 0.001), and Satisfaction Profile (SAT-P) (p < 0.05) (Zenico et al., 2009; Shin et al., 2023). In the other two studies, L. meyenii significantly increased the subjects’ sexual desire (p < 0.001, p = 0.03, respectively) (Gonzales et al., 2002; Stone et al., 2009). One study also found that the positive effect of L. meyenii on sexual desire was not because of changes in either Hamilton scores for depression or anxiety or serum testosterone and oestradiol levels. In addition, 1.5 g maca significantly improved sexual desire, similar to 3.0 g maca (Gonzales et al., 2002).
The detailed study designs of the 4 studies were summarized as follows: 1) men over 40 years of age with AMS total scores ≥27 were enrolled. The duration of this study spanned a period of 3 months. Eighty-eight patients were recruited, and 8 dropped out. 2 Maca extract capsules at a time, 3 times per day for 3 months (1,000 mg/capsule, containing 833 mg Maca gelatinized powder, n-benzyl-hexadecanamide between 115 and 175 μg/g, cadmium and total mercury less than 0.3 mg/kg, total arsenic and plumbum less than 0.5 mg/kg, absence of coliform bacteria) (Shin et al., 2023).
2) Patients aged 31–41 years with mild ED were enrolled. The duration of this study spanned a period of 3 months. Fifty patients were recruited. 1,200 mg Maca tablets 2 times daily for 3 months. The pulverized dehydrated Maca root tablets were directly imported from Peruvian Andes and kindly provided by Ibersan Srl, Forli, Italy (Zenico et al., 2009).
3) Twenty-one- to 56-year-old healthy men were enrolled. The duration of this study spanned a period of 3 months. Fifty-seven patients were recruited. Gelatinized maca tablet (500 mg maca per tablet, Laboratorios Hersil, Lima, Peru, provided), 3 tablets (1.5 g Maca) or 6 tablets (3.0 g Maca) per day for 3 months (Gonzales et al., 2002).
4) Experienced and endurance-trained male cyclists with a mean age of 30 ± 7 years were enrolled. As a crossover study, study subjects were required to take Maca or placebo for 2 weeks, with a 1-week washout period. Eight patients were recruited, and none dropped out. Maca root extract capsule (400 mg Maca per capsule, collected from the Cerro de Pasco region in the central Peruvian Andes Mountains, milled, soaked in 40°C water 3 times, filtered, solution concentrated under vacuum at 65°C, concentrated again to solid, mixed with modified starch and silica, spry dried to obtain a fine powder), 5 capsules (2.0 g Maca) per day for 2 weeks (Stone et al., 2009)
The number of sample sizes in the 4 studies was limited, and a pilot study only enrolled 8 healthy male cyclists, and Maca capsules were only taken for 2 weeks (Stone et al., 2009).
There are two randomized, double-blind, placebo-controlled clinical trials on R. damascena. One study focused on 18–45-year-old patients with sexual dysfunction caused by methadone (Farnia et al., 2017), while the other focused on patients with sexual dysfunction caused by SSRIs (Farnia et al., 2015). Both studies used R. damascena oil 2 mL/day, containing 17 mg citronellol of essential oil of R. damascena (drops). The duration of both studies spanned a period of 2 months. One study recruited 50 patients with no drop-out (Farnia et al., 2017), and the other study recruited 68 patients with 8 drop-outs (Farnia et al., 2015). R. damascena was found to significantly improve sexual dysfunction caused by methadone and significantly increase serum testosterone levels, but there was no association between the two effects (Farnia et al., 2017). R. damascena also significantly improved both SSRI-induced sexual dysfunction and major depressive disorder (MDD) symptoms, and improve MDD symptoms occurred with the improvement in sexual dysfunction (Farnia et al., 2015). R. damascena might be used to treat sexual dysfunction caused by SSRIs.
There were also limitations in the two studies. The sample sizes were limited. Second, the inclusion criteria and single-center design could cause systematic selection bias. Third, the potential and unassessed physiological and psychological variables might also bring bias.
In four clinical trials regarding C. sativus, three studies found that C. sativus significantly improved the IIEF scores (p < 0.0001, p < 0.001, p < 0.001, respectively) (Shamsa et al., 2009; Modabbernia et al., 2012; Mohammadzadeh-Moghadam et al., 2015).
In addition, one study found that C. sativus significantly improved tip rigidity, tip tumescence, base rigidity, and base tumescence (p < 0.0001). This is an open-label study without placebo group. The intervention duration was only 10 days. In addition, only 20 patients aged 26–62 years were recruited. The optimum dose of C. sativus was not investigated (Shamsa et al., 2009).
One study found that C. sativus significantly improved the IIEF scores of ED patients with diabetes, and the intervention measure was to rub the C. sativus gel on patients’ penis half an hour before sexual intercourse, which is completely different from the daily timed and quantified oral administration used in most clinical trials. In this randomized, double-blind, placebo-controlled, parallel-group study, 40–76-year-old patients with ED and diabetes were enrolled and required to rub a pea-sized amount of the gel containing 1% C. sativus on their penis half an hour before sexual intercourse. Fifty patients were recruited, and none dropped out. The duration of the study spanned a period of 1 month (Mohammadzadeh-Moghadam et al., 2015).
One study found that C. sativus significantly improved the IIEF scores of patients with sexual dysfunction caused by fluoxetine, an SSRI. In this randomized, double-blind, placebo-controlled study, 18- to 45-year-old married male patients with MDD stabilized on fluoxetine and with fluoxetine-related sexual dysfunction were enrolled and required to take 15 mg C. sativus capsule twice per day. C. sativus was donated by Green Plants of Life Co., (IMPIRAN; Tehran, Iran). Each capsule contained 15 mg of dried C. sativus stigma extract and 1.65–1.75 mg of crocin, an important component of C. sativus. Thirty-six patients were recruited, and 6 dropped out. The duration of the study spanned a period of 1 month. In addition, because of the limited sample size, researchers failed to obtain significant differences in the orgasmic function domain (Modabbernia et al., 2012).
Moreover, one randomized, crossover, open-label clinical trial found that C. sativus did not improve the IIEF scores compared with sildenafil (Safarinejad et al., 2010). The duration of this study spanned 26 weeks. Patients were required to take 2 C. sativus capsules (each 15 mg, dried C. sativus stigma was produced by Novin Saffron Co., Mashhad, Iran) twice daily for 12 weeks followed by on-demand 50-mg sildenafil for another 12 weeks or vice versa, separated by a 2-week washout phase. A total of 346 patients were recruited, and 39 dropped out.
The results of three randomized, double-blind, placebo-controlled clinical trials regarding P. ginseng showed that P. ginseng significantly improved the IIEF scores (de Andrade et al., 2007; Kim et al., 2009; Choi et al., 2013).
One study found that P. ginseng significantly improved the domains of erectile function (p = 0.046), intercourse satisfaction (p = 0.005), orgasmic function (p = 0.002), sexual desire (p = 0.001), overall satisfaction (p = 0.001), and IIEF-15 total score (p = 0.002). In this study, researchers used 4-year-old P. ginseng berries to obtain standardized Korean ginseng berry (SKGB) extract. Patients were required to take 4 SKGB tablets (350 mg SKGB extract per tablet) per day. The duration of this study spanned a period of 2 months. A total of 119 patients were recruited, and 1 dropped out (Choi et al., 2013).
The other two studies showed similar results, with statistically significant improvements in all domains and IIEF-5 total score in the P. ginseng group but not in the placebo group (de Andrade et al., 2007; Kim et al., 2009). In addition, one study found that erectile function, intercourse satisfaction and overall satisfaction scores in the five domains of the IIEF were significantly higher in the P. ginseng group than in the placebo group (p < 0.05). The other study showed that scores on rigidity, penetration, and maintenance were significantly higher in the P. ginseng group than in the placebo group after treatment (p < 0.01) (de Andrade et al., 2007).
In one study, researchers used tissue-cultured mountain ginseng extract (TMGE). Patients were required to take 1,000 mg TMGE twice a day. Patients aged 33–79 years were enrolled. The duration of this study spanned a period of 2 months. A total of 143 patients were recruited, and 57 dropped out. Despite the staggering number of dropouts, 47 of them were in the placebo group because of no improvement in their ED. Considering the 68 patients contained in the placebo group at the beginning, only 21 patients in the placebo group finally finished the trial (Kim et al., 2009).
In the other study, patients were required to take 1,000 mg Korean red ginseng (KRG) 3 times daily. Patients aged 26–70 years with mild or mild to moderate ED were enrolled. The duration of this study spanned a period of 3 months. Sixty patients were recruited, and none dropped out (de Andrade et al., 2007).
The results of two randomized, double-blind, placebo-controlled clinical trials on T. foenum-graecum found that, compared with the baseline and the placebo group, Testofen, the active extract of T. foenum-graecum, significantly improved Derogatis Interview for Sexual Functioning-Self Report (DISF-SR) (p < 0.01) and AMS scores (p < 0.001, p < 0.013, respectively) in healthy males (Steels et al., 2011; Rao et al., 2016). These two studies also found that Testofen significantly improved the scores of the sexual arousal domain and orgasm domain, especially the ability to obtain full erections, and the ability, intensity and duration of orgasm (Steels et al., 2011; Rao et al., 2016). One study also found that the average erection time per week (p = 0.001) and sexual activity per month (p = 0.004) increased significantly after receiving Testofen (Rao et al., 2016).
In one study, the Testofen tablet was supplied by Gencor Pacific Ltd. One tablet contained 300 mg Testofen, as well as 17 mg magnesium, 15 mg elemental zinc and 5 mg pyridoxine. Study subjects were required to take 2 tablets per day. Sixty healthy males aged 25–52 years were recruited, and 6 dropped out. The duration of this study spanned 6 weeks (Steels et al., 2011).
In the other study, 43–70-year-old healthy males were required to take 600 mg Testofen (extracted from T. foenum-graecum seed) per day. The duration of this study spanned a period of 3 months. A total of 120 males were recruited, and 9 dropped out (Rao et al., 2016).
A prospective study on P. vera found that P. vera significantly improved the IIEF-15 and IIEF-5 scores, as well as the mean peak systolic velocity (p = 0.001, p < 0.05, p = 0.018, respectively). Additionally, the study also found that the levels of total cholesterol (TC) and low density lipoprotein (LDL) in the experimental group decreased, while the levels of high density lipoprotein (HDL) increased (p = 0.008, 0.007 and 0.001, respectively), suggesting potential hypolipidaemic effects (Aldemir et al., 2011). In this study, 38–59-year-old patients with ED for at least 12 months were enrolled, and they were required to eat 100 g pistachio (P. vera) nuts at lunch for 3 weeks.
The prospective study had only 17 study subjects, and no placebo group was set.
W. somnifera did not show therapeutic effect on psychogenic ED in a clinical study. In this study, patients with psychogenic ED who had a serum testosterone level of no less than 240 ng/dL were enrolled (Mamidi and Thakar, 2011).
In this randomized, single-blind, placebo-controlled study, patients were required to take 4 W. somnifera tablets (dried root powder of W. somnifera, 500 mg each) 3 times per day. The duration of this study spanned a period of 2 months. Ninety-five patients were recruited, and 9 dropped out. More than half of the patients had high severity of ED, and more than 80% of the patients had interpersonal conflicts with their partners (Mamidi and Thakar, 2011).
The mixed botanical medicine was either a mixture of herbal plant extracts (Iacono et al., 2012; Sansalone et al., 2014; Quarto et al., 2017; Park et al., 2019; Mirone et al., 2021) or a mixture of active herbal plant ingredients (Shirai et al., 2021). The results of the six mixed botanical drugs showed therapeutic effects on ED.
Among them, a randomized, multicenter, double-blind, placebo-controlled study found that “a new nutritional supplement” [500 mg of P. ginseng, 200 mg of Moringa oleifera Lam. (Moringaceae), and 50 mg of rutin] combined with tadalafil increased cGMP levels (p < 0.05). Patients were required to take the “new nutritional supplement” with/without 5 mg tadalafil once a day. The duration of this study spanned a period of 3 months. Patients aged 38–69 years with mild to moderate ED and with hypertension and/or type 2 diabetes were enrolled. Eighty-six patients were recruited, and 8 dropped out (Mirone et al., 2021).
A prospective, randomized, single-blind, placebo-controlled study found that Tradamix TX1000 (300 mg of alga Ecklonia bicyclis, 450 mg of T. terrestris, and 250 mg of glucosamine oligosaccharide) improved peak systolic velocity (PSV) and ED symptoms in patients with moderate arterial dysfunction. Patients were required to take Tradamix TX1000 tablets twice a day. The duration of this study spanned a period of 3 months. Two hundred patients were recruited, and 23 dropped out (Sansalone et al., 2014).
A randomized, double-blind study found that compared with tadalafil, Tradamixina (150 mg of alga E. bicyclis, 396 mg of T. terrestris, and 144 mg of D-glucosamine and N-acetyl-D-glucosamine), with the same main ingredients as Tradamix TX1000, showed a stronger effect of improving ED symptoms, especially in the ED and libido domains of the IIEF-5 scores. In addition, Tradamixina also showed the ability to increase serum testosterone levels. Patients were required to take Tradamixina twice a day. The duration of this study spanned a period of 2 months. Over 60 years of age, patients with reduced libido, with or without ED, were enrolled. Seventy patients were recruited (Iacono et al., 2012).
A randomized, double-blind, placebo-controlled study found that KBMSI-2 [260.53 μg/g Rb1, 543.91 μg/g Rb2, 424.92 μg/g Rc, 377.32 μg/g Re, 1,160.55 μg/g Rf, 703.97 μg/g Rg1, 60.73 μg/g curcumin, 98.66 μg/g allantoin, and 744.13 μg/g loganin, extracted from Ginseng Radix Rubra, Dioscorea tenuipes Franch. & Sav. (Dioscoreaceae), Cornus officinalis Siebold & Zucc. (Cornaceae), Lycium chinense Mill (Solanaceae), and Curcuma longa L. (Zingiberaceae)] showed statistically significant improvement in the IIEF-EF domain, intercourse satisfaction domain, and IIEF total scores. Forty-to eighty-year-old patients with ED were enrolled and required to take 6 g of KBMSI-2 twice per day. The duration of this study spanned a period of 2 months. Forty-four patients were recruited, and 18 dropped out (Park et al., 2019).
IDIProst® Gold [100 mg of C. sativus stigma dry extract 0.3% minimum safranal, 120 mg of Pinus massoniana Lamb. (Pinaceae) bark extract 95% minimum proanthocyanidins, and 320 mg of Serenoa repens (W. Bartram) Small (Arecaceae) fruit oil extract 88% minimum fatty acids] significantly improved IIEF-5, IPSS, and QoL (question of life) scores, especially in the 40–60 age group. In addition, IDIProst® Gold increased Qmax (maximum urinary flow rate) variation in subjects under 50 years old but had no effect on subjects over 50 years old. The detailed study design was not mentioned. Patients aged 20–75 years with concomitant lower urinary tract symptoms (LUTS) and ED were enrolled and required to take one IDIProst® Gold capsule per day. The duration of this study spanned a period of 3 months. A total of 164 patients were recruited, and 24 dropped out (Quarto et al., 2017).
A randomized, double-blind, placebo-controlled, crossover study found that “supplement drink” (testofen 600 mg/d extracted from T. foenum-graecum, L-citrulline 800 mg/d, resveratrol 300 mg/d, and caffeine 40 mg/d) showed significantly improved the IIEF total scores, especially in the domains of IIEF-1, IIEF-2, IIEF-7, IIEF-9, IIEF-10, IIEF-13, and IIEF-15. The duration of this study spanned a period of only 5 weeks (2 weeks for “supplement drink” and 2 weeks for placebo, with 1 week for wash-out). Thirty-to forty-year-old patients with ED were enrolled. Twenty patients were recruited, and none dropped out. In addition, the study lacked information on comorbidities that could affect sexual function, such as diabetes (Shirai et al., 2021).
There were 24 studies that analysed the incidence of adverse events (Tables 1–3). Overall, no serious adverse events were reported in clinical studies. Among these 24 studies, 11 did not report any adverse events. The reported adverse events included gastrointestinal symptoms, headache, facial flushing, dizziness, and insomnia, and these symptoms were mostly mild to moderate. Among all the adverse events, headache and gastrointestinal symptoms were most common. One clinical trial analysed the incidence rate of adverse events between the combined use of “a new nutritional composition” (500 mg P. ginseng, 200 mg M. oleifera, and 50 mg rutin) and tadalafil and the use of tadalafil alone. No difference in the incidence rate of adverse events between the two groups was found (Mirone et al., 2021). This clinical trial also reported that one study subject experienced insomnia in the combined use of the two drugs group, while no study subject experienced insomnia in the use of tadalafil alone group (Mirone et al., 2021). A clinical trial of G. biloba reported that in addition to headache and gastrointestinal symptoms, the experimental subjects who took G. biloba also experienced sedation and increased oral intake (Kang et al., 2002). Another clinical trial of G. biloba reported that the experimental subjects experienced paraesthesia fingers, but the incidence rate was not statistically significant compared to the placebo group (Wheatley, 2004). Similarly, a clinical trial of C. sativus reported that the experimental subjects experienced nausea, daytime drowsiness, decreased appetite, dry mouth, nervousness, restlessness, morning drowsiness, and increased appetite. Although this clinical trial had more different adverse events compared to other studies, statistical analysis found that the incidence rate of these side effects was not significantly different from the placebo group and mostly at the mild to moderate degree and therefore tolerable (Modabbernia et al., 2012). In a clinical trial of E. longifolia, two severe adverse events, low back pain and liposome, were reported in the experimental group, but they were not considered to be associated with the intervention measure. In addition, this clinical trial also recorded some mild to moderate adverse events, such as upper respiratory tract infections, generalized body ache, conjunctivitis, infected chalazion, ankle pain, achilles tendinitis, herpes zoster, and R index finger pain, but these adverse events were not considered to be associated with the intervention measure (Ismail et al., 2012).
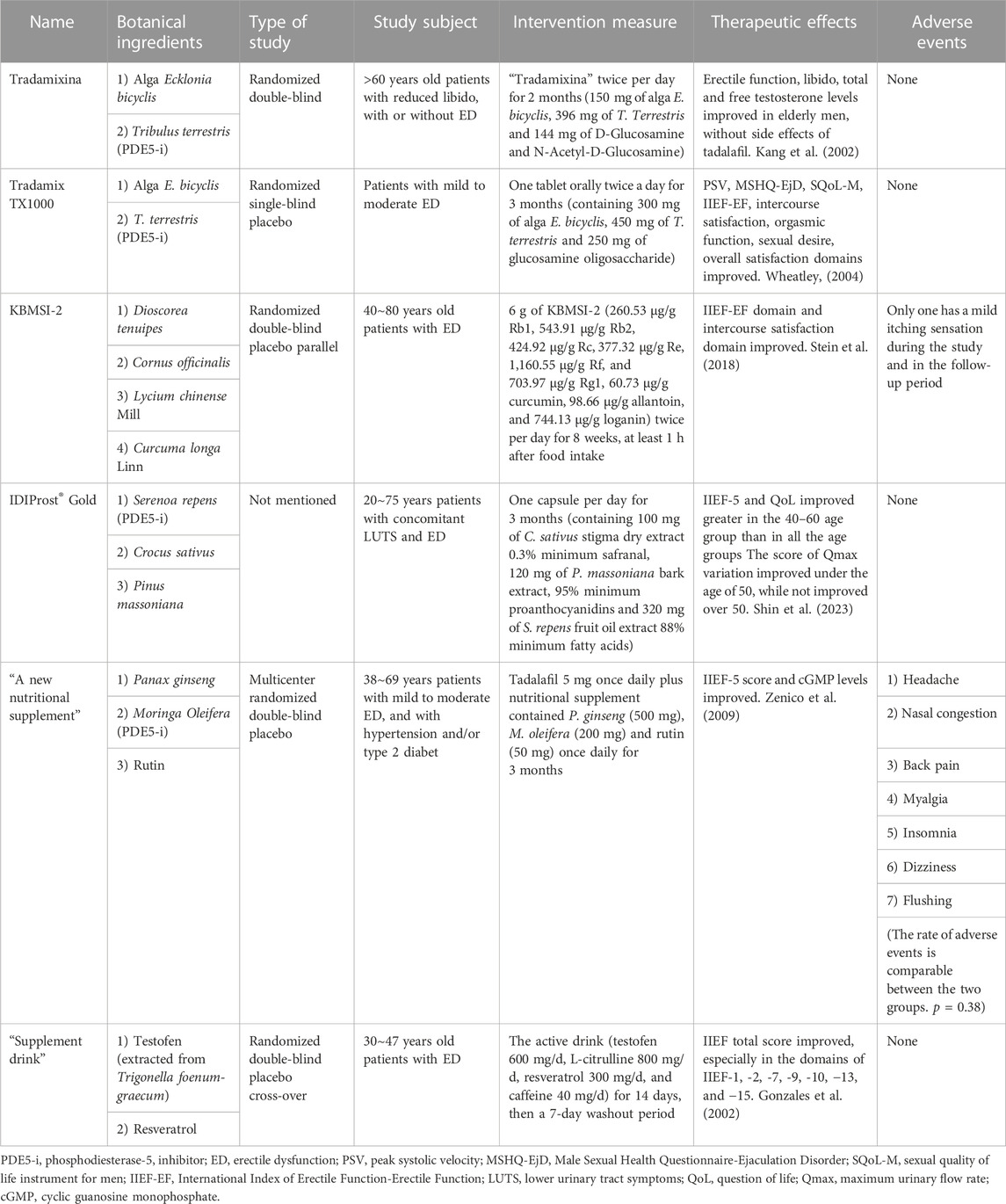
TABLE 3. Mixed botanical drugs.
Although most clinical studies for the included botanical drugs are randomized double-blind placebo-controlled trials, some limitations should be noted. The age and comorbidities of participants vary in different studies. For example, some studies enrolled patients over 40 years old, while one study enrolled patients approximately 18–45 years old. Some studies have enrolled androgen deficiency of aging males. Interestingly, the intervention method for one study was to rub the C. sativus gel. In addition, the sample size of most studies is limited. The above factors limit the extension of the conclusion. Clinical trials enrolling more representative populations with larger sample sizes are needed in the future to confirm the efficacy of botanical drugs in treating ED. Encouragingly, most clinical trials indeed demonstrate the efficacy of botanical drugs in treating ED without significant adverse effects. These botanical drugs may be used along with PDE5-i or alone to treat ED in clinical practice.
Overall, this review summarizes several botanical drugs with promising therapeutic effects for ED in clinical studies without significant adverse effects. Further placebo-controlled or head-to-head randomized controlled trials are needed to verify these therapeutic effects, and determine the appropriate usage and dosage and target patients. In addition, further pharmacology experiments need to be conducted for the screening of active compounds and further drug development.
Conceptualization: WS and DM. Methodology: DX and YZ. Investigation: JB and HY. Data curation: WS and TW. Formal analysis: DX and YZ. Writing, review and editing of the manuscript: DX, YZ, and JL. All authors contributed to the article and approved the submitted version.
The authors would like to thank the patients included in the studies we reviewed.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Al-Rehaily, A. J., Alhowiriny, T. A., El-Tahir, K. E., Al-Taweel, A. M., and Perveen, S. (2015). Molecular mechanisms that underlie the sexual stimulant actions of Avicennia marina (Forssk) Vierh. and Crocus sativus L. Pak J. Pharm. Sci. 28 (1), 49–58.
Aldemir, M., Okulu, E., Neselioglu, S., Erel, O., and Kayigil, O. (2011). Pistachio diet improves erectile function parameters and serum lipid profiles in patients with erectile dysfunction. Int. J. Impot. Res. 23 (1), 32–38. doi:10.1038/ijir.2010.33
Anand Ganapathy, A., Hari Priya, V. M., and Kumaran, A. (2021). Medicinal plants as a potential source of phosphodiesterase-5 inhibitors: A review. J. Ethnopharmacol. 267, 113536. doi:10.1016/j.jep.2020.113536
Chaturapanich, G., Chaiyakul, S., Verawatnapakul, V., and Pholpramool, C. (2008). Effects of Kaempferia parviflora extracts on reproductive parameters and spermatic blood flow in male rats. Reproduction 136 (4), 515–522. doi:10.1530/REP-08-0069
Chen, X., and Lee, T. J. F. (1995). Ginsenosides-induced nitric oxide-mediated relaxation of the rabbit corpus cavernosum. Br. J. Pharmacol. 115 (1), 15–18. doi:10.1111/j.1476-5381.1995.tb16313.x
Cherdshewasart, W., and Nimsakul, N. Clinical trial of Butea superba, an alternative herbal treatment for erectile dysfunction. Asian J. Androl., 243–6. doi:10.1152/ajprenal.00114.2003
Chiou, W. F., and Wu, T. S. (2012). 9-hydroxycanthin-6-one induces penile erection and delays ejaculation. J. Sex. Med. 9 (4), 1027–1036. doi:10.1111/j.1743-6109.2011.02296.x
Cho, K. S., Park, C. W., Kim, C. K., Jeon, H. Y., Kim, W. G., Lee, S. J., et al. (2013). Effects of Korean ginseng berry extract (GB0710) on penile erection: evidence from in vitro and in vivo studies. Asian J. Androl. 15 (4), 503–507. doi:10.1038/aja.2013.49
Choi, S. H., Shin, T. J., Lee, B. H., Hwang, S. H., Lee, S. M., Lee, B. C., et al. (2011). Ginsenoside Rg3 enhances large conductance Ca2+-activated potassium channel currents: A role of Tyr360 residue. Mol. Cells 31 (2), 133–140. doi:10.1007/s10059-011-0017-7
Choi, Y. D., Park, C. W., Jang, J., Kim, S. H., Jeon, H. Y., Kim, W. G., et al. (2013). Effects of Korean ginseng berry extract on sexual function in men with erectile dysfunction: A multicenter, placebo-controlled, double-blind clinical study. Int. J. Impot. Res. 25 (2), 45–50. doi:10.1038/ijir.2012.45
Cortes-Gonzalez, J. R., Arratia-Maqueo, J. A., Gomez-Guerra, L. S., and Holmberg, A. R. (2010). The use of Butea superba (Roxb) compared to sildenafil for treating erectile dysfunction. BJU Int. 105 (2), 225–228. doi:10.1111/j.1464-410X.2009.08748.x
de Andrade, E., de Mesquita, A. A., Claro Jde, A., de Andrade, P. M., Ortiz, V., Paranhos, M., et al. (2007). Study of the efficacy of Korean Red Ginseng in the treatment of erectile dysfunction. Asian J. Androl. 9 (2), 241–244. doi:10.1111/j.1745-7262.2007.00210.x
Do, J., Choi, S., Choi, J., and Hyun, J. S. (2013). Effects and mechanism of action of a Tribulus terrestris extract on penile erection. Korean J. Urol. 54 (3), 183–188. doi:10.4111/kju.2013.54.3.183
Farnia, V., Shirzadifar, M., Shakeri, J., Rezaei, M., Bajoghli, H., Holsboer-Trachsler, E., et al. (2015). Rosa damascena oil improves SSRI-induced sexual dysfunction in male patients suffering from major depressive disorders: results from a double-blind, randomized, and placebo-controlled clinical trial. Neuropsychiatr. Dis. Treat. 11, 625–635. doi:10.2147/NDT.S78696
Farnia, V., Tatari, F., Alikhani, M., Shakeri, J., Taghizadeh, M., Karbasizadeh, H., et al. (2017). Rosa Damascena oil improved sexual function and testosterone in male patients with opium use disorder under methadone maintenance therapy-results from a double-blind, randomized, placebo-controlled clinical trial. Drug Alcohol Depend. 176, 117–125. doi:10.1016/j.drugalcdep.2017.02.008
GamalEl Din, S. F., Abdel Salam, M. A., Mohamed, M. S., Ahmed, A. R., Motawaa, A. T., Saadeldin, O. A., et al. (2019). Tribulus terrestris versus placebo in the treatment of erectile dysfunction and lower urinary tract symptoms in patients with late-onset hypogonadism: A placebo-controlled study. Urologia 86 (2), 74–78. doi:10.1177/0391560318802160
Gauthaman, K., and Ganesan, A. P. (2008). The hormonal effects of Tribulus terrestris and its role in the management of male erectile dysfunction--an evaluation using primates, rabbit and rat. Phytomedicine 15 (1-2), 44–54. doi:10.1016/j.phymed.2007.11.011
Gonzales, G. F., Cordova, A., Vega, K., Chung, A., Villena, A., Gonez, C., et al. (2002). Effect of Lepidium meyenii (MACA) on sexual desire and its absent relationship with serum testosterone levels in adult healthy men. Andrologia 34 (6), 367–372. doi:10.1046/j.1439-0272.2002.00519.x
Iacono, F., Prezioso, D., Illiano, E., Romeo, G., Ruffo, A., and Amato, B. Sexual asthenia: tradamixina versus tadalafil 5 mg daily. BMC Surg. 2012;12 Suppl. 1(Suppl. 1):S23, doi:10.1186/1471-2482-12-S1-S23
Ismail, S. B., Wan Mohammad, W. M., George, A., Nik Hussain, N. H., Musthapa Kamal, Z. M., and Liske, E. (2012). Randomized clinical trial on the use of PHYSTA freeze-dried water extract of eurycoma longifolia for the improvement of quality of life and sexual well-being in men. Evid. Based Complement. Altern. Med. 2012, 429268. doi:10.1155/2012/429268
Jansakul, C., Tachanaparuksa, K., Mulvany, M. J., and Sukpondma, Y. (2012). Relaxant mechanisms of 3, 5, 7, 3', 4'-pentamethoxyflavone on isolated human cavernosum. Eur. J. Pharmacol. 691 (1-3), 235–244. doi:10.1016/j.ejphar.2012.07.019
Kamenov, Z., Fileva, S., Kalinov, K., and Jannini, E. A. (2017). Evaluation of the efficacy and safety of Tribulus terrestris in male sexual dysfunction-A prospective, randomized, double-blind, placebo-controlled clinical trial. Maturitas 99, 20–26. doi:10.1016/j.maturitas.2017.01.011
Kang, B. J., Lee, S. J., Kim, M. D., and Cho, M. J. (2002). A placebo-controlled, double-blind trial of Ginkgo biloba for antidepressant-induced sexual dysfunction. Hum. Psychopharmacol. 17 (6), 279–284. doi:10.1002/hup.409
Khanavi, M., Azimi, H., Ghiasi, S., Hassani, S., Rahimi, R., Nikfar, S., et al. (2012). Specifying human platelet cAMP and cGMP phosphodiesterase inhibitory activity of the plants used in traditional Iranian medicine for the purpose of erectile dysfunction. Int. J. Pharmacol. 8 (3), 161–168. doi:10.3923/ijp.2012.161.168
Kim, H. J., Woo, D. S., Lee, G., and Kim, J. J. (1998). The relaxation effects of ginseng saponin in rabbit corporal smooth muscle: is it a nitric oxide donor? Br. J. Urol. 82 (5), 744–748. doi:10.1046/j.1464-410x.1998.00811.x
Kim, T. H., Jeon, S. H., Hahn, E. J., Paek, K. Y., Park, J. K., Youn, N. Y., et al. (2009). Effects of tissue-cultured mountain ginseng (Panax ginseng CA Meyer) extract on male patients with erectile dysfunction. Asian J. Androl. 11 (3), 356–361. doi:10.1038/aja.2008.32
Leitao, A. E., Vieira, M. C. S., Pelegrini, A., da Silva, E. L., and Guimaraes, A. C. A. (2021). A 6-month, double-blind, placebo-controlled, randomized trial to evaluate the effect of Eurycoma longifolia (Tongkat Ali) and concurrent training on erectile function and testosterone levels in androgen deficiency of aging males (ADAM). Maturitas 145, 78–85. doi:10.1016/j.maturitas.2020.12.002
Li, H., He, W. Y., Lin, F., and Gou, X. (2014). Panax notoginseng saponins improve erectile function through attenuation of oxidative stress, restoration of Akt activity and protection of endothelial and smooth muscle cells in diabetic rats with erectile dysfunction. Urol. Int. 93 (1), 92–99. doi:10.1159/000354878
Li, Z. M., Liu, N., Jiang, Y. P., Yang, J. M., Zheng, J., Sun, M., et al. (2019). Vitexin alleviates streptozotocin-induced sexual dysfunction and fertility impairments in male mice via modulating the hypothalamus-pituitary-gonadal axis. Chem. Biol. Interact. 297, 119–129. doi:10.1016/j.cbi.2018.10.013
Lin, F., and Gou, X. (2013). Panax notoginseng saponins improve the erectile dysfunction in diabetic rats by protecting the endothelial function of the penile corpus cavernosum. Int. J. Impot. Res. 25 (6), 206–211. doi:10.1038/ijir.2013.19
Mamidi, P., and Thakar, A. B. (2011). Efficacy of Ashwagandha (Withania somnifera Dunal. Linn) in the management of psychogenic erectile dysfunction. Ayu 32 (3), 322–328. doi:10.4103/0974-8520.93907
Mirone, V., Napolitano, L., D'Emmanuele di Villa Bianca, R., Mitidieri, E., Sorrentino, R., Vanelli, A., et al. (2021). A new original nutraceutical formulation ameliorates the effect of Tadalafil on clinical score and cGMP accumulation. Arch. Ital. Urol. Androl. 93 (2), 221–226. doi:10.4081/aiua.2021.2.221
Modabbernia, A., Sohrabi, H., Nasehi, A. A., Raisi, F., Saroukhani, S., Jamshidi, A., et al. (2012). Effect of saffron on fluoxetine-induced sexual impairment in men: randomized double-blind placebo-controlled trial. Psychopharmacol. Berl. 223 (4), 381–388. doi:10.1007/s00213-012-2729-6
Mohammadzadeh-Moghadam, H., Nazari, S. M., Shamsa, A., Kamalinejad, M., Esmaeeli, H., Asadpour, A. A., et al. (2015). Effects of a topical saffron (Crocus sativus L) gel on erectile dysfunction in diabetics: A randomized, parallel-group, double-blind, placebo-controlled trial. J. Evid. Based Complement. Altern. Med. 20 (4), 283–286. doi:10.1177/2156587215583756
Oboh, G., Adebayo, A. A., and Ademosun, A. O. (2018). Phenolic-rich extracts of Eurycoma longifolia and Cylicodiscus gabunensis inhibit enzymes responsible for the development of erectile dysfunction and are antioxidants. J. Basic Clin. Physiol. Pharmacol. 29 (6), 689–696. doi:10.1515/jbcpp-2017-0160
Park, N. C., Kim, S. W., Hwang, S. Y., and Park, H. J. (2019). Efficacy and safety of an herbal formula (KBMSI-2) in the treatment of erectile dysfunction: A preliminary clinical study. Investig. Clin. Urol. 60 (4), 275–284. doi:10.4111/icu.2019.60.4.275
Quarto, G., Cola, A., and Perdona, S. (2017). Efficacy of a formulation containing Serenoa repens, Crocus sativus and Pinus massoniana extracts in men with concomitant LUTS and erectile dysfunction. Minerva Urol. Nefrol. 69 (3), 300–306. doi:10.23736/S0393-2249.16.02661-8
Rao, A., Steels, E., Inder, W. J., Abraham, S., and Vitetta, L. (2016). Testofen, a specialised Trigonella foenum-graecum seed extract reduces age-related symptoms of androgen decrease, increases testosterone levels and improves sexual function in healthy aging males in a double-blind randomised clinical study. Aging Male 19 (2), 134–142. doi:10.3109/13685538.2015.1135323
Roaiah, M. F., El Khayat, Y. I., GamalEl Din, S. F., and Abd El Salam, M. A. (2016). Pilot study on the effect of botanical medicine (Tribulus terrestris) on serum testosterone level and erectile function in aging males with partial androgen deficiency (PADAM). J. Sex. Marital Ther. 42 (4), 297–301. doi:10.1080/0092623X.2015.1033579
Safarinejad, M. R., Shafiei, N., and Safarinejad, S. (2010). An open label, randomized, fixed-dose, crossover study comparing efficacy and safety of sildenafil citrate and saffron (Crocus sativus Linn) for treating erectile dysfunction in men naive to treatment. Int. J. Impot. Res. 22 (4), 240–250. doi:10.1038/ijir.2010.10
Sahin, K., Orhan, C., Akdemir, F., Tuzcu, M., Gencoglu, H., Sahin, N., et al. (2016). Comparative evaluation of the sexual functions and NF-κB and Nrf2 pathways of some aphrodisiac herbal extracts in male rats. BMC Complement. Altern. Med. 16 (1), 318. doi:10.1186/s12906-016-1303-x
Sansalone, S., Leonardi, R., Antonini, G., Vitarelli, A., Vespasiani, G., et al. (2014). Alga Ecklonia bicyclis, Tribulus terrestris, and glucosamine oligosaccharide improve erectile function, sexual quality of life, and ejaculation function in patients with moderate mild-moderate erectile dysfunction: A prospective, randomized, placebo-controlled, single-blinded study. Biomed. Res. Int. 2014, 121396. doi:10.1155/2014/121396
Santos, C. A., Reis, L. O., Destro-Saade, R., Luiza-Reis, A., and Fregonesi, A. (2014). Tribulus terrestris versus placebo in the treatment of erectile dysfunction: A prospective, randomized, double blind study. Actas Urol. Esp. 38 (4), 244–248. doi:10.1016/j.acuro.2013.09.014
Shamsa, A., Hosseinzadeh, H., Molaei, M., Shakeri, M. T., and Rajabi, O. (2009). Evaluation of Crocus sativus L. (saffron) on male erectile dysfunction: A pilot study. Phytomedicine 16 (8), 690–693. doi:10.1016/j.phymed.2009.03.008
Shin, D., Jeon, S. H., Piao, J., Park, H. J., Tian, W. J., Moon, D. G., et al. (2023). Efficacy and safety of maca (Lepidium meyenii) in patients with symptoms of late-onset hypogonadism: A randomized, double-blind, placebo-controlled clinical trial. Korea: World J Mens Health.
Shirai, M., Miyoshi, Y., Ogasa, T., Miyoshi, M., Ishikawa, K., Hiramatsu, I., et al. (2021). Oral testofen, L-citrulline, resveratrol, and caffeine supplement drink improves sexual function in men with phosphodiesterase 5 inhibitors: randomized, double-blind, placebo-controlled crossover pilot study. World J. Mens. Health 39 (4), 733–739. doi:10.5534/wjmh.200129
Sin, V. J., Anand, G. S., and Koh, H. L. (2021). Botanical medicine and natural products used for erectile dysfunction. Sex. Med. Rev. 9 (4), 568–592. doi:10.1016/j.sxmr.2020.10.005
Steels, E., Rao, A., and Vitetta, L. (2011). Physiological aspects of male libido enhanced by standardized Trigonella foenum-graecum extract and mineral formulation. Phytother. Res. 25 (9), 1294–1300. doi:10.1002/ptr.3360
Stein, R. A., Schmid, K., Bolivar, J., Swick, A. G., Joyal, S. V., and Hirsh, S. P. (2018). Kaempferia parviflora ethanol extract improves self-assessed sexual health in men: A pilot study. J. Integr. Med. 16 (4), 249–254. doi:10.1016/j.joim.2018.05.005
Stone, M., Ibarra, A., Roller, M., Zangara, A., and Stevenson, E. (2009). A pilot investigation into the effect of maca supplementation on physical activity and sexual desire in sportsmen. J. Ethnopharmacol. 126 (3), 574–576. doi:10.1016/j.jep.2009.09.012
Sudyka, J., and Wick, J. Y. (2021). Treating erectile dysfunction with prescription medications & natural products: A pharmacist's guide. Sr. Care Pharm. 36 (12), 632–644. doi:10.4140/TCP.n.2021.632
Tee, B. H., Hoe, S. Z., Cheah, S. H., and Lam, S. K. (2017). Effects of root extracts of eurycoma longifolia Jack on corpus cavernosum of rat. Med. Princ. Pract. 26 (3), 258–265. doi:10.1159/000464363
Wang, X., Chu, S., Qian, T., Chen, J., and Zhang, J. (2010). Ginsenoside Rg1 improves male copulatory behavior via nitric oxide/cyclic guanosine monophosphate pathway. J. Sex. Med. 7 (2 Pt 1), 743–750. doi:10.1111/j.1743-6109.2009.01482.x
Wheatley, D. (2004). Triple-blind, placebo-controlled trial of Ginkgo biloba in sexual dysfunction due to antidepressant drugs. Hum. Psychopharmacol. 19 (8), 545–548. doi:10.1002/hup.627
Ying, A., Yu, Q. T., Guo, L., Zhang, W. S., Liu, J. F., Li, Y., et al. (2018). Structural-activity relationship of ginsenosides from steamed ginseng in the treatment of erectile dysfunction. Am. J. Chin. Med. 46 (1), 137–155. doi:10.1142/S0192415X18500088
Zenico, T., Cicero, A. F., Valmorri, L., Mercuriali, M., and Bercovich, E. (2009). Subjective effects of Lepidium meyenii (maca) extract on well-being and sexual performances in patients with mild erectile dysfunction: A randomised, double-blind clinical trial. Andrologia 41 (2), 95–99. doi:10.1111/j.1439-0272.2008.00892.x
Keywords: botanical drugs, natural products, erectile dysfunction, clinical study, phosphodiesterase-5
Citation: Xu D, Zhang Y, Bai J, Yuan H, Wang T, Liu J, Song W and Ma D (2023) Botanical drugs for treating erectile dysfunction: clinical evidence. Front. Pharmacol. 14:1232774. doi: 10.3389/fphar.2023.1232774
Received: 01 June 2023; Accepted: 03 August 2023;
Published: 16 August 2023.
Edited by:
Lu Zhao, Zhejiang University, ChinaReviewed by:
Xianghu Meng, Nanjing Medical University, ChinaCopyright © 2023 Xu, Zhang, Bai, Yuan, Wang, Liu, Song and Ma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wen Song, c29uZ3dlbjkyMkAxNjMuY29t; Delin Ma, bWFkZXJpbmU0QDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.