
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 22 June 2023
Sec. Pharmacogenetics and Pharmacogenomics
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1209286
 Abdelrahman Alaa1*
Abdelrahman Alaa1* Neven Sarhan1
Neven Sarhan1 Mohamed Gamal Lotfy El-Ansary2
Mohamed Gamal Lotfy El-Ansary2 Naglaa Samir Bazan2
Naglaa Samir Bazan2 Khaled Farouk2
Khaled Farouk2 Raed Shahat Ismail3
Raed Shahat Ismail3 Mona Farag Schalaan4Adel R. A. Abd-Allah3*
Mona Farag Schalaan4Adel R. A. Abd-Allah3*Background: The world has been suffering from the Coronavirus Disease-2019 (COVID-19) pandemic since the end of 2019. The COVID-19-infected patients differ in the severity of the infection and the treatment response. Several studies have been conducted to explore the factors that affect the severity of COVID-19 infection. One of these factors is the polymorphism of the angiotensin converting enzyme 2 (ACE-2) and the type 2 transmembrane serine protease (TMPRSS2) genes since these two proteins have a role in the entry of the virus into the cell. Also, the ACE-1 regulates the ACE-2 expression, so it is speculated to influence the COVID-19 severity.
Objective: This study investigates the relationship between the ACE-1, ACE-2, and TMPRSS2 genes single nucleotide polymorphism (SNPs) and the COVID-19 disease severity, treatment response, need for hospitalization, and ICU admission in Egyptian patients.
Patients and Methods: The current study is an observational prospective, cohort study, in which 109 total COVID-19 patients and 20 healthy volunteers were enrolled. Of those 109 patients, 51 patients were infected with the non-severe disease and were treated in an outpatient setting, and 58 suffered from severe disease and required hospitalization and were admitted to the ICU. All 109 COVID-19 patients received the treatment according to the Egyptian treatment protocol.
Results: Genotypes and allele frequencies among severe and non-severe patients were determined for ACE-1 rs4343, TMPRSS2 rs12329760, and ACE-2 rs908004. The GG genotype and the wild allele of the ACE-2 rs908004 and the mutant allele of the ACE-1 rs4343 were significantly more predominant in severe patients. In contrast, no significant association existed between the TMPRSS2 rs12329760 genotypes or alleles and the disease severity.
Conclusion: The results of this study show that the ACE-1 and ACE-2 SNPs can be used as severity predictors for COVID-19 infection since also they have an effect on length of hospitalization.
Since the end of 2019, Egypt and the entire world have been suffering from the Coronavirus Disease 2019 (COVID-19) pandemic, which is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). According to the World Health Organization (WHO), since the emergence of this new pandemic, there have been more than 767 million confirmed cases of COVID-19 patients; around 516 thousand of these cases are in Egypt (https://covid19.who.int/, accessed on 31 May 2023). The COVID-19 is a highly contagious infection that is transmitted mainly through respiratory droplets or direct contact, with the possibility of fecal–oral transmission (Jin et al., 2020). The incubation period of the infection ranges from 2 to 14 days with the symptoms appearing within an average of 4–7 days (Öztürk et al., 2020). The symptoms can vary from mild symptoms (low-grade fever, dry cough, fatigue, and myalgia) to severe and critical symptoms (respiratory distress and pneumonia) (Wang et al., 2020), which require hospitalization and sometimes admission to the Intensive Care Unit (ICU) and can lead to death. Several factors affect the severity of the symptoms experienced by COVID-19 patients. Studies concluded that gender (males), advanced age (over 65), ethnicity (African American race) and presence of co-morbid conditions like hypertension, dyslipidemia, cancer and others are associated with more severe symptoms (Adhikari et al., 2020; Wang et al., 2021).
One of the mechanisms of cell entry of the SARS-CoV-2 is that its spike protein (S) binds to the angiotensin-converting enzyme (ACE) 2 receptor, which is a transmembrane present in many epithelial cells in the body including the airway and the alveoli (Kamel et al., 2021; Gusev et al., 2022; Jackson et al., 2022; Rouaud and Méan, 2022). When the virus binds to the ACE-2 receptor, the type 2 transmembrane serine protease (TMPRSS2) enzyme activates the viral spike by cleaving it when it is attached to the ACE-2 receptor, making the fusion with the cell possible and promoting the virus to release its Ribonucleic acid (RNA) into the cell cytoplasm (Kamel et al., 2021; Gusev et al., 2022; Jackson et al., 2022). As the ACE-2 plays a vital role in the COVID-19 infection, the whole tissue-based renin-angiotensin system (RAS) is affected. The ACE-1 controls the formation of ACE-2, and the ACE-2 converts angiotensin 2 to angiotensin 1. During SARS-CoV-2 infection, the plasma ACE-1 activity is increased while ACE2 expression is decreased, which in turn causes the levels of angiotensin 2 to become unopposed (Zheng and Cao, 2020; Aladag et al., 2021; Yamamoto et al., 2021). This imbalance disrupts the hemostasis of the of body and may contribute to exacerbating the COVID-19 infection indirectly through inflammation and thrombosis (Aladag et al., 2021; Yamamoto et al., 2021), or causing a direct acute lung injury through different mechanisms like inducing the apoptosis of endothelial cells and of alveolar epithelial cells (Rarani et al., 2022) while boosting pro-inflammatory mediators like IL-6 and IL-8 (Suzuki et al., 2003). Along with its role in the viral cell entry, the TMPRSS2 activity also influences the Interferon-induced transmembrane protein 3 (IFITM3), which has an important role in the control of SARS-CoV-2 infection given its role in other viral diseases along with its interaction with the S protein (Shi et al., 2021; Dobrijevic et al., 2022). Given the involvement of the ACE-1, ACE-2 and TMPRSS2 in the COVID-19 infection, several studies have shown that there might be a strong correlation between the variability and genetic polymorphism of the ACE-1, ACE-2 and the TMPRSS2 genes and the risk and severity of the COVID-19 infection (Asselta et al., 2020; Hou et al., 2020; Jahanafrooz et al., 2022; Li et al., 2022).
The aim of the current study is to investigate if the variation in three different Single Nucleotide Polymorphisms (SNPs), one for the ACE-1 gene, one for the ACE-2 gene and another for the TMPRSS2 gene have any effect in the COVID-19 disease severity, treatment response and need for hospitalization and admission to the ICU in Egyptian patients.
This is an observational, prospective cohort study which was conducted between December 2020 and June 2022. The total enrolled study subjects were 129 Egyptians, among which 58 were severe cases from Cairo University Hospitals, Cairo, Egypt, 51 non-severe cases who were treated in an outpatient setting and 20 healthy controls. Eligible patients for each group were those with established COVID-19 infection according to the WHO COVID-19 guidelines (Coronavirus Disease, 2019 COVID-19 Treatment Guidelines, 2021). Patients with severe disease were defined as Individuals who have SpO2 <94% on room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mmHg, a respiratory rate >30 breaths/min, or lung infiltrates >50%. The study also included patients who had positive nasal swap for COVID-19 infection and their ages were between 18 and 80 years old. Patients with any prior respiratory problems such Asthma and chronic obstructive pulmonary disease (COPD) were excluded. The study was registered in ClinicalTrials.gov; Identifier: NCT05157217. The study protocol was approved by the Research Ethics Committee at the Faculty of medicine, Cairo University, Cairo, Egypt, and all participating patients provided written informed consent (REC number N-134-2020).
Patients who met the eligibility criteria were then divided into two groups; group 1 (Patients with Severe COVID-19 Disease): COVID-19 patients who suffered from serious respiratory complications that needed ICU admission and group 2 (Patients with non-severe COVID-19 Disease): COVID-19 carriers who were infected with SARS-CoV-2 and healed without suffering from any respiratory complications or the need for hospitalization. Patients were subjected to full laboratory including complete blood count (CBC), liver function and kidney function tests as well as inflammatory markers. Clinical and medical information were abstracted from the patient’s files and included age, sex, body weight, cigarette smoking status, medical history, and medications. All the patients received treatment according to the Egyptian COVID-19 treatment protocol (Table 1) established by the Egyptian Ministry of Health (Masoud et al., 2020). Whole blood samples (3 mL) were collected for DNA extraction and genotyping. The blood samples were stored at −80°C.
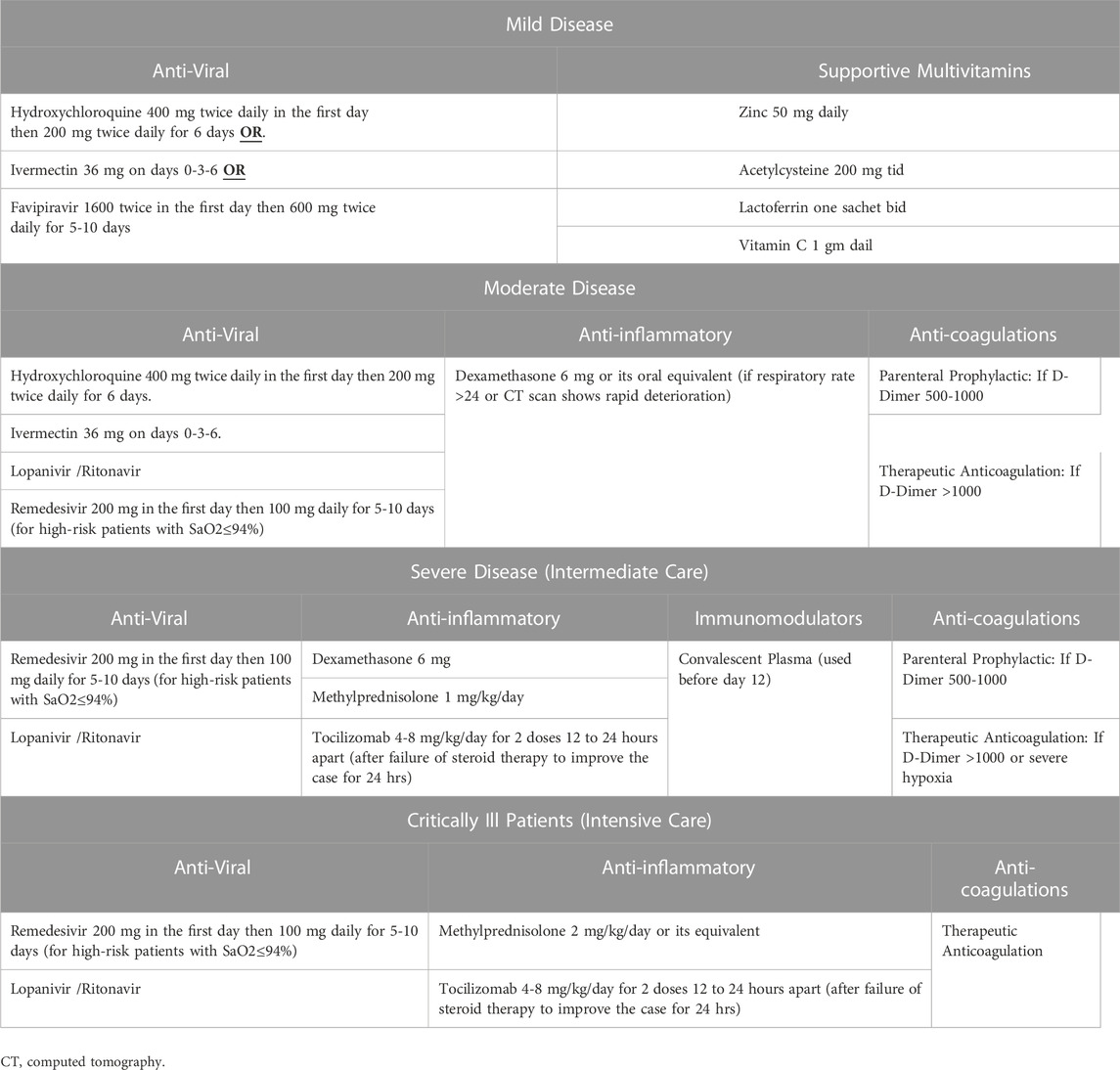
TABLE 1. Egyptian COVID-19 treatment guidelines.
DNA was extracted from peripheral blood leukocytes using the QIAamp DNA blood kits, cat no: 51,104 (Qiagen, Hilden, Germany). The procedure of extraction was by silica-membrane-based technology. Three genes’ variants were determined using TaqMan probe-based polymerase chain reaction (PCR). The Angiotensin-converting enzyme gene (ACE) rs4343 (A2350G), Paired Ig-like receptors (PIR) gene G15494752T rs908004, and Transmembrane serine protease 2 Polymorphisms (TMPRSS2) gene rs12329760 C478G genotype variants were determined using Applied Biosystems™ TaqMan™ SNP Genotyping Assays “ACE rs4343 A/G, assay ID: C_11942562, PIR rs908004 G/T assay ID: C_8816953, and TMPRSS2 rs12329760 C/G, assay ID: C_25622353, purchased from (ThermoFisher Scientific, Germany). The PCR TaqMan Genotyping Master Mix kit, cat no: 4371353 (ThermoFisher, Germany). The appropriate volume from PCR reaction mix was prepared with a total volume of 10 µL/well. The reaction mix of each sample is composed of 5 µL of 2X TaqMan Genotyping Master Mix, 0.5 µL of TaqMan assay (20X), and 4.5 µL RNase free water. The thermal cycling protocol is optimized as follows” 950°C for 10 min for AmpliTaq Gold, UP Enzyme Activation, followed by denaturation step at 950°C for 15 s and annealing/extension at 600°C for 1 min for 40 cycles. The qPCR was performed on Applied BioSystems PCR instrument (ThermoFisher Scientific, Germany).
Continuous variables were represented as mean ± standard deviation. Categorical variables were presented as numbers and percentages. Hardy–Weinberg Equilibrium was tested using Chi-square test with one degree of freedom. Chi-square was used to compare the allele and genotype frequencies as appropriate. The association of genotypes with changes in endpoints was tested separately for each SNP. The three SNPs were tested in a dominant model. One-way ANOVA was used to analyze genotype group differences. We included covariates with a p-value <0.2 in a stepwise linear regression model. The binary logistic regression was used to investigate the association between the tested genotypes regarding outcomes of interest.
All reported p values were two-tailed, and a p-value of less than 0.05 was considered significant. Significant SNPs were determined according to the corrected Bonferroni p-value (p = 0.05/3 tested SNPs = 0.017, the Bonferroni-corrected significance threshold). All statistical analyses were carried out using Statistical Package for the Social Sciences (SPSS) software (version 22.0 for Windows; SPSS Inc., Chicago, Illinois, United States).
The current study was conducted on 129 Egyptians who were sub-classed into three main groups: the COVID-19 severe patients (n = 58), the COVID-19 non-severe patients (n = 51) and healthy control (n = 20). The baseline characteristics for each group are presented in Table 2. There was no significant difference between the baseline characteristics of the severe, non-severe and healthy control groups except for the room air SO2, respiratory rate, C-reactive protein (CRP), procalcitonin and interleukin-6 (IL-6) levels. Genotyping was carried out in 3 SNPs for each patient in each group. The distribution of ACE-1 (rs4343), TMPRSS2 (rs12329760) and ACE-2 (rs908004) SNP genotypes among severe, non-severe COVID-19 patients and healthy control was analyzed. When comparing the distribution of the three SNPs’ genotypes among severe and non-severe patients, the ACE-2 rs908004 G/G genotype was found to be significantly more prevalent in severe patients (n = 21) than non-severe patients (n = 7), unlike the G/T genotype which was significantly more prevalent in non-severe patients (n = 39) than severe patients (n = 29). The ACE-1 rs4343 and TMPRSS2 rs12329760 genotypes, however, have shown no significant difference between severe and non-severe COVID-19 patients. These results are shown in Table 3. There was no significant difference between COVID-19 infected patients and healthy control regarding the three SNPs’ genotypes distribution, as presented in Table 4. When comparing the three beforementioned SNPs’ allele distribution among the two groups; the mutant allele of the ACE-1 rs4343 SNP and the wild allele of the ACE-2 rs908004 SNP were found to significantly more predominant in the severe COVID-19 patients than the non-severe COVID-19 patients, as shown in Table 5. The risk factors of ACE-2 rs908004 for COVID-19 severity calculated by linear logistic regression is shown in Table 6. In the severe group, the total and intensive care unit (ICU) length of stay (LOS) was compared to find if there is any association between the LOS and different genotypes of each SNP. The ICU LOS has shown no significant difference between the different genotypes of each SNP. When comparing the ACE-1 rs4343 SNP genotypes with the total LOS of severe COVID-19 patients, patients with the A/A genotype have significantly higher total LOS than the other two genotypes. Also, when comparing the ACE-2 rs908004 SNP genotypes with the total LOS in severe COVID-19, patients with the T/T genotype have significantly higher total LOS than the other two genotypes. The TMPRSS2 rs12329760 SNP genotypes seem to have no impact on the total LOS, since there is no significant difference in the total LOS between the three different genotypes. These results are shown in Table 7. There was no significant association between any of the SNPs and the patient’s mortality. A Kaplan-Meier survival function curve was plotted to further support these results and is illustrated in Figure 1. The combined genotypic effect of the ACE-1 rs4343 and ACE-2 rs908004 was compared with the different comorbidities that patients of both groups suffered from, and a linear-by-linear association was established and shown in Table 8. The combined genotypic effect was found to have a significant association with patients suffering from hypothyroidism. The other comorbidities show no significant association with the combined effect of the two SNPs.
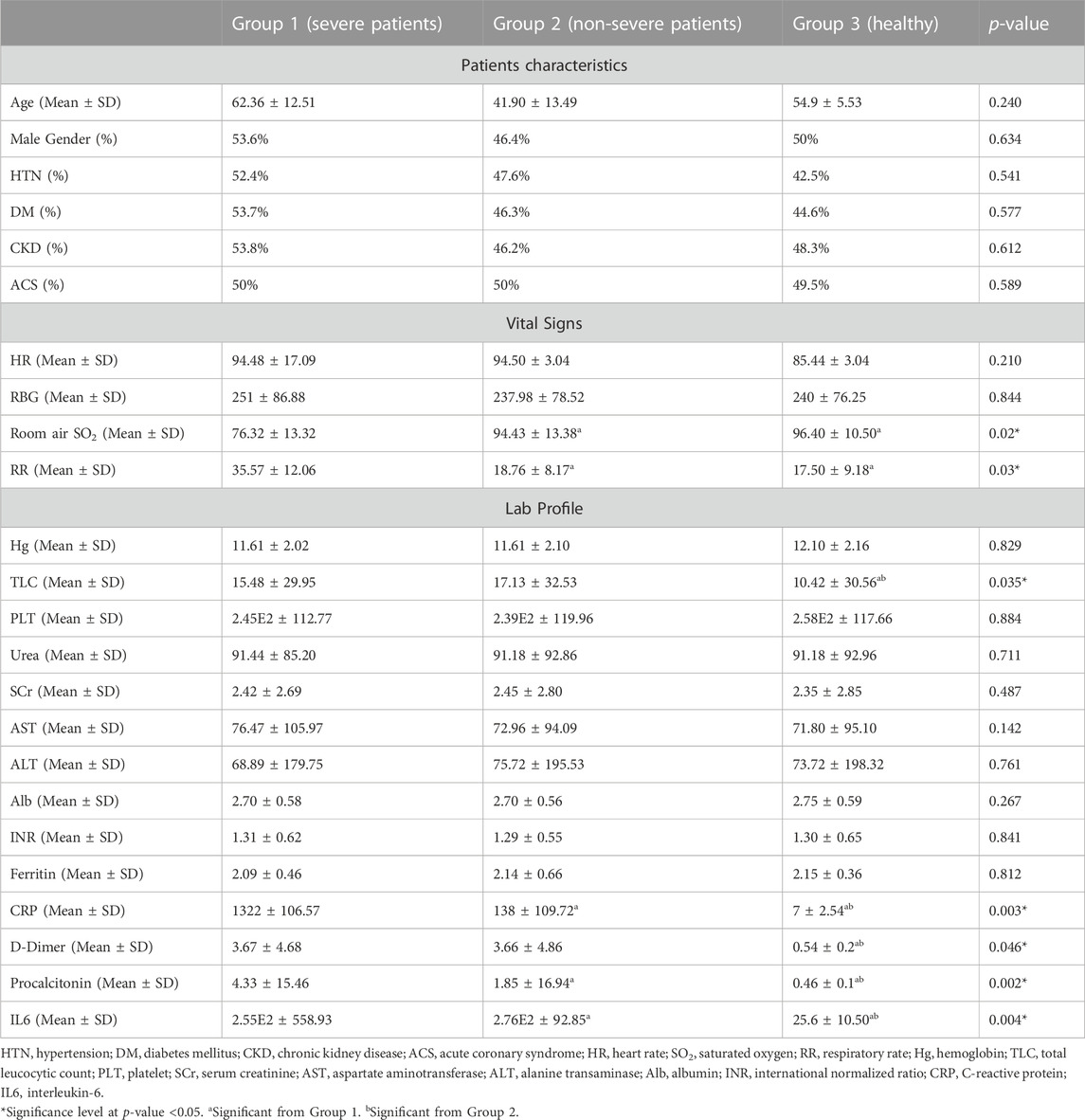
TABLE 2. Baseline characteristics comparison between severe COVID-19 patients, non-severe COVID-19 patients, and healthy volunteers.
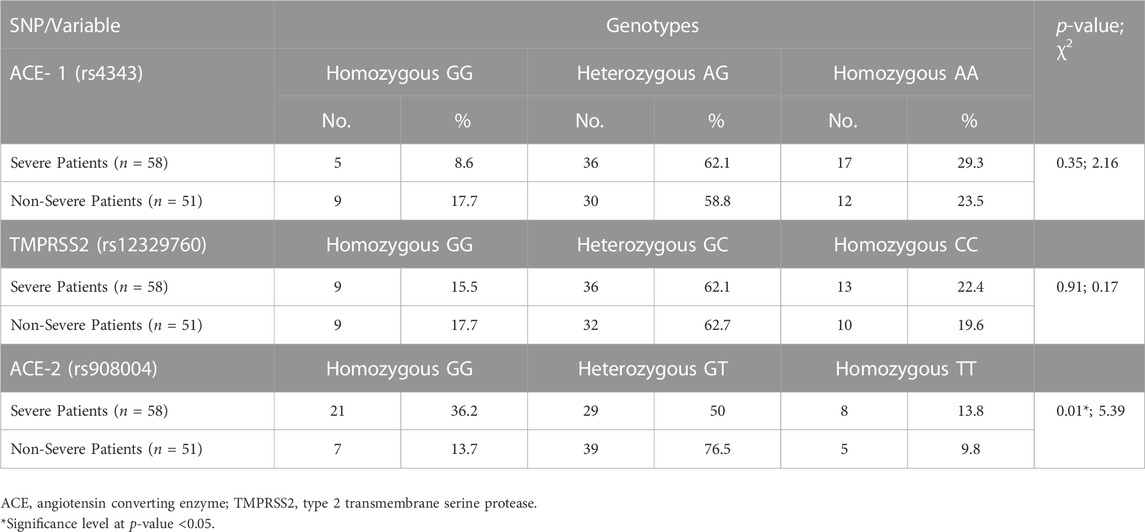
TABLE 3. Distribution of ACE-1 (rs4343), TMPRSS2 (rs12329760) and ACE-2 (rs908004) SNPs Genotypes among severe and non-severe COVID-19 patients. Statistical analysis done was chi-square test.
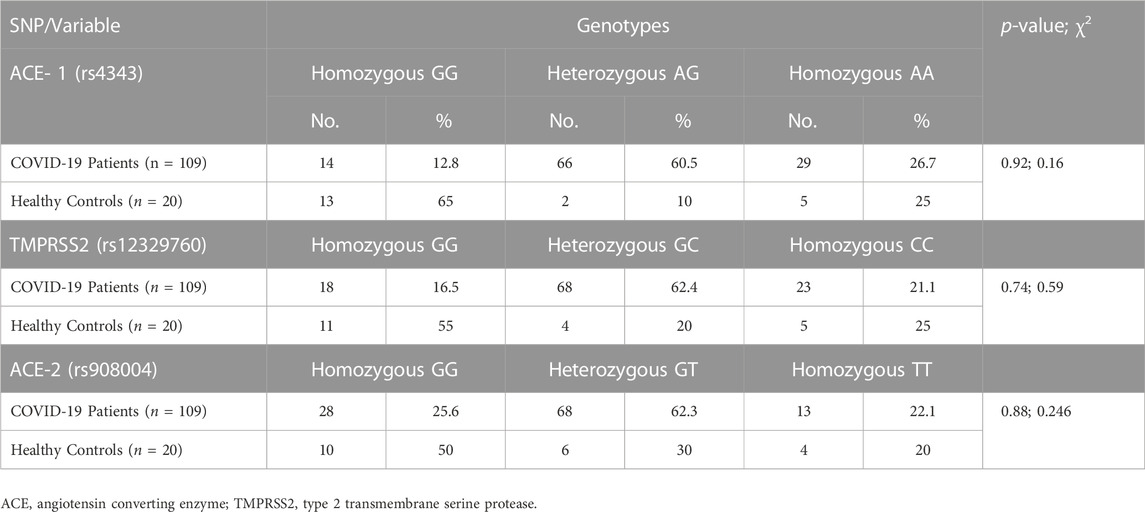
TABLE 4. Distribution of ACE-1 (rs4343), TMPRSS2 (rs12329760) and ACE-2 (rs908004) SNPs Genotypes among COVID-19 positive patients and healthy controls. The statistical analysis done was chi-square test.
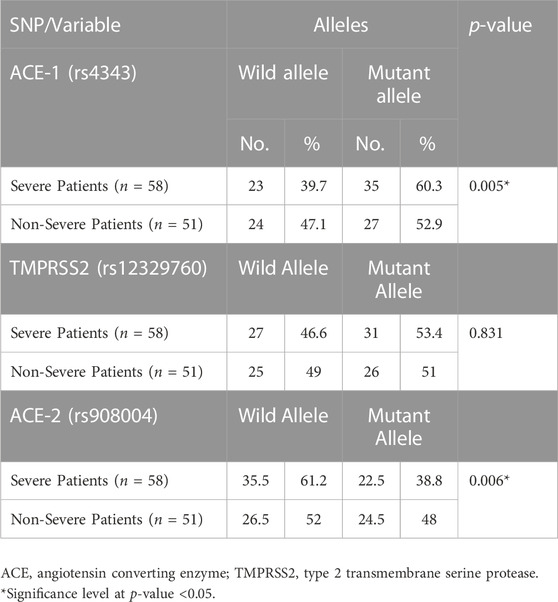
TABLE 5. Distribution of ACE-1 (rs4343), TMPRSS2 (rs12329760) and ACE-2 (rs908004) Alleles among severe and non-severe COVID-19 patients.

TABLE 6. Risk factors for COVID-19 severity by binary logistic regression.
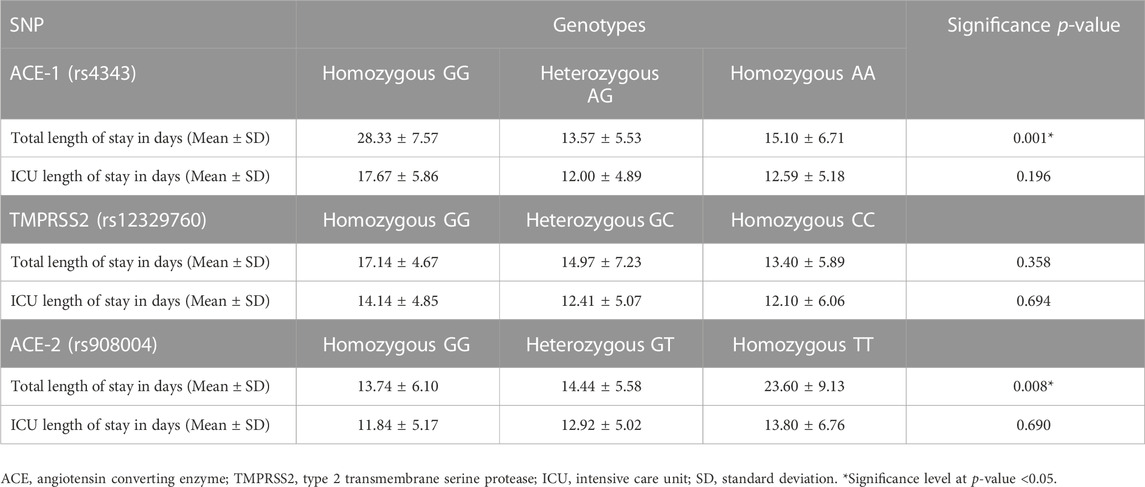
TABLE 7. Comparison between total and ICU length of stay among the different genotypes in severe COVID-19 patients.
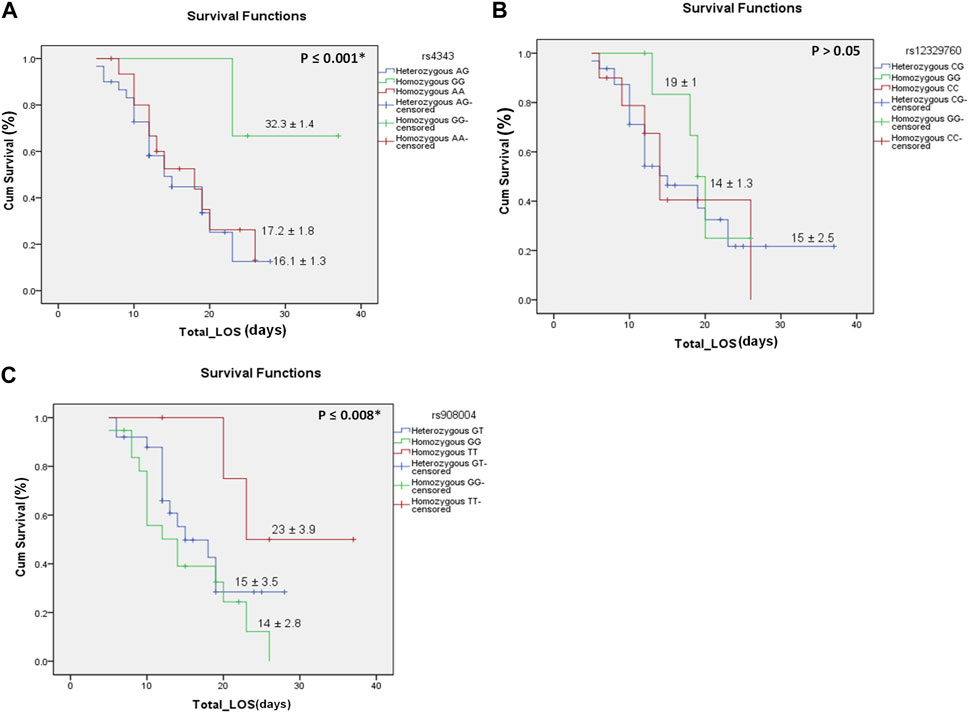
FIGURE 1. Kaplan-Meier survival versus the total length of stay in each of the three SNPs and their genotypes. (A) is for the ACE-1 rs4343genotypes, (B) is for the TMPRSS2 rs12329760 genotypes, (C) is for the ACE-2 rs908004 genotypes. Data is presented on the curve as median ± standard error. Significance levels at p < 0.05. The ACE-1 rs4343GG genotype was more significantly associated with longer hospitalization than the other genotypes. The ACE-2 rs908004TT genotype was more significantly associated with longer hospitalization than the other genotypes. Total_LOS, total length of stay presented as days; Cum Survival, cumulative survival presented as %.*Significance level at p-value <0.05.
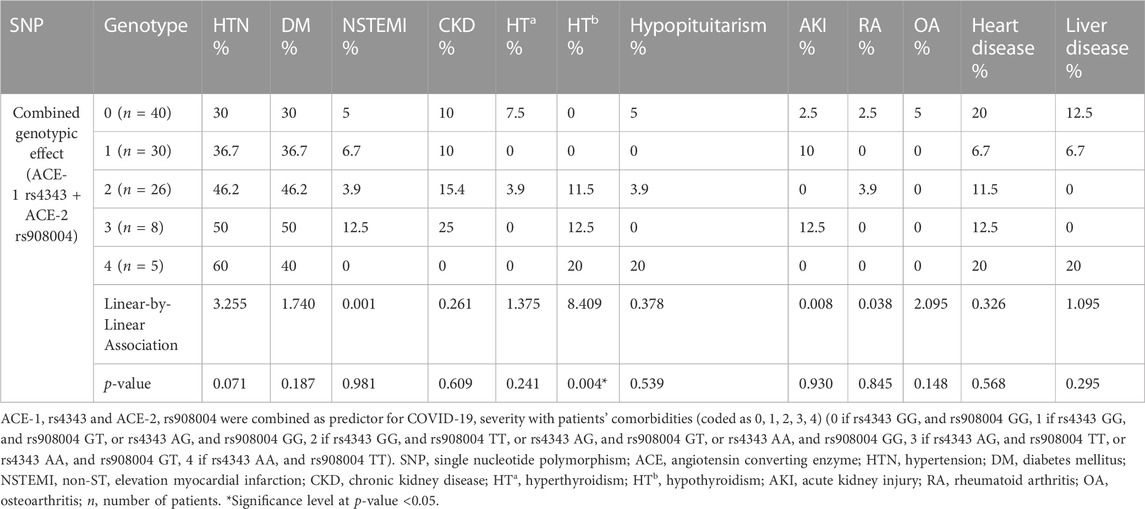
TABLE 8. Association between ACE-1 and ACE-2 SNP combination and comorbidities.
To this day, factors that affect COVID-19 clinical severity are still unraveled. Many studies attempted to investigate the relation between different gene polymorphisms and COVID-19 severity. The present prospective cohort study aims to assess the association between the ACE-1 rs4343, ACE-2 rs908004 and TMPRSS2 rs12329760 genes and the COVID-19 clinical severity in Egyptian patients. To our best knowledge, this is the first study to try to establish a relationship between these specific SNPs in these genes, the clinical severity of COVID-19 along with the total length of hospitalization and treatment response, especially in Egyptian patients. A total of109 patients were enrolled in the study, 58 patients suffered from severe COVID-19 disease and were admitted to the ICU, while 51 patients suffered from non-severe disease and were treated in an outpatient setting.
We found that there was a significant difference in the ACE-2 rs908004 genotypes and allele frequencies between the severe and the non-severe patients, where the GG genotype and the wild G-allele was more dominant in severe patients. We also found a significant association between the ACE-2 rs908004 polymorphism and the total length of hospitalization among clinically severe COVID-19 patients (Patients with GG genotype had significantly more total length of hospital stay than other genotypes). Several studies have reached a similar conclusion. In a study on German population, Möhlendick et al. (2021) found that the GG genotype or G-allele of ACE-2 rs2285666 was associated with patients that developed severe COVID-19 disease than the rest of the SARS-CoV-2 positive patient. In a recent Russian study, Shikov et al. (2020) found that several rare ACE-2 variants (for example, rs146598386, rs755766792 and others) influenced the clinical severity and outcome of COVID-19 disease. These results are also in agreement with Cafiero et al. (2021), which found that the ACE-2 rs2074192 SNP had a significant impact on disease severity. However, their results show that the T-allele was more dominant in symptomatic patients than asymptomatic patients, this difference from our results may be due to the difference in the measured SNP. In contrast to our findings, Karakaş Çelik et al. (2021) carried out a study on 155 COVID-19 patients in Turkey which showed that there is no correlation between the COVID-19 clinical severity and the ACE-2 rs2106809 and rs2285666 polymorphisms. Also, Gómez et al. (2020)’s results were not in agreement with our results, where they found that in 204 COVID-19 patients in Spain that there was no link between the ACE-2 rs2285666 SNP and the COVID-19 disease severity. These differences between our results and these two studies can be contributed to the difference in the studied SNP, ethnicity, or sample size.
The current findings revealed that there was no significant difference in neither the genotypes nor alleles of the TMPRSS2 rs12329760 between the severe and non-severe patients. This agreed with the findings German case-control study done by Schönfelder et al. (2021) on 239 COVID-19 positive patients. Their study results showed no correlation between neither TMPRSS2 rs2070788 nor rs12329760 polymorphism and the clinical severity of COVID-19. Also, Wulandari et al. (2021) found no association between the TMPRSS2 rs12329760 polymorphism and COVID-19 severity. In contrast to our findings, Monticelli et al. (2021) found a relation between TMPRSS2 rs12329760 polymorphism and COVID-19 severity and thus can help identifying individuals at risk of developing clinically severe COVID-19 disease in Italian patients. Also, in a study on Indian population, Ravikanth et al. (2021) found a significant link between TMPRSS2 rs12329760 variant and decreased COVID-19 disease severity.
Regarding the ACE-1 rs4343 assessed in the present study, there was no significant association between the SNP’s genotypes and COVID-19 disease severity. However, the mutant A-allele of rs4343 gene was significantly more dominant in non-severe COVID-19 patients than severe COVID-19 patients. We also found a significant association between the ACE-1 rs4343 polymorphism and the total length of hospitalization among clinically severe COVID-19 patients (Patients with TT genotype had significantly more total length of hospital stay than other genotypes). To our knowledge, all other studies conducted to test an association between ACE-1 gene and COVID-19 severity was on the ACE-1 insertion/deletion (I/D) polymorphism, however this is the first study attempting to investigate the association between an ACE-1 SNP and the COVID-19 severity. Two studies conducted by Möhlendick et al. (2021) and Karakaş Çelik et al. (2021) found no association between ACE I/D and COVID-19 disease severity. Another two studies by Cafiero et al. (2021) and Gunal et al. (2021) found that the ACE I/I allele was significantly more prevalent in asymptomatic COVID-19 patients, while the D/D allele was significantly more prevalent in symptomatic COVID-19 patients. Gómez et al. (2020) also found that depending on the hypertension status of COVID-19 patients, ACE I/D polymorphism can be associated with the risk of developing severe COVID-19 disease.
Other studies tried to find other predictive biomarkers for COVID-19 Severity. Ciaglia et al. (2021) found that long-lived individuals who are less susceptible to COVID-19 infection had higher levels of BPIFB4 protein circulating their blood than old healthy people and was even lower in COVID-19 infected patients. Sabbatino et al. (2021) suggests that the Programmed death-1 (PD-1) and its ligand programmed deathl-igand1 (PD-L1) has a potential prognostic role in COVID-19 and can be studied as target for future treatment.
In conclusion, our study demonstrated that the ACE-2 rs908004 genotype and allele as well as ACE-1 rs4343 allele can be a predictive factor for COVID-19 severity and treatment response in Egyptian patients. In contrast, ACE-1 rs4343 genotype and both TMPRSS2 rs12329760 genotypes and alleles were not associated to neither the COVID-19 severity nor treatment response in Egyptian patients. It could be concluded that the ACE-1 and ACE-2 variants were associated with an increased length of hospitalization in severe patients and thus require more aggressive approach and closer monitoring during treatment. We also found that there was no significant difference in the three SNPs’ genotypes between the COVID-19 infected patients and the healthy control.
Among the limitations of this study was the limited sample size and the study being single centered. Moreover, ACE-2 serum levels would have given us a better insight on predicting the severity and outcome of COVID-19. Unfortunately, no blood sample was left to perform this test. Further studies involving larger sample size and more diverse populations should be conducted to provide better understanding of the relationship between the ACE-1, ACE-2 and TMPRSS2 polymorphism and COVID-19 disease severity.
The original contributions presented in the study are included in the article/supplementary materials,further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the Research Ethics Committee at the Faculty of medicine, Cairo University, Cairo, Egypt. The patients/participants provided their written informed consent to participate in this study.
AA performed the research; AA, NS, and ARA-A. wrote and revised the research; AA, NS, NSB, and ARA-A. designed the research; NS and AA analyzed the data; NSB, ML, and KF provided access to patient’s samples and data; RI, MS, and ARA-A drafted the article. NSB, ML, KF, RI, MS, and ARA-A performed supervision, and revised the manuscript. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Adhikari, S. P., Meng, S., Wu, Y-J., Mao, Y-P., Ye, R-X., Wang, Q-Z., et al. (2020). Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 9 (1), 29. doi:10.1186/s40249-020-00646-x
Aladag, E., Tas, Z., Ozdemir, B. S., Akbaba, T. H., Akpinar, M. G., Goker, H., et al. (2021). Human ace D/I polymorphism could affect the clinicobiological course of COVID-19. J. Renin Angiotensin Aldosterone Syst. 2021, 5509280. doi:10.1155/2021/5509280
Asselta, R., Paraboschi, E. M., Mantovani, A., and Duga, S. (2020). ACE2 and TMPRSS2 variants and expression as candidates to sex and country differences in COVID-19 severity in Italy. Aging 12 (11), 10087–10098. doi:10.18632/aging.103415
Cafiero, C., Rosapepe, F., Palmirotta, R., Re, A., Ottaiano, M. P., Benincasa, G., et al. (2021). Angiotensin system polymorphisms' in SARS-CoV-2 positive patients: Assessment between symptomatic and asymptomatic patients: A pilot study. Pharmacogenomics personalized Med. 14, 621–629. doi:10.2147/PGPM.S303666
Ciaglia, E., Lopardo, V., Montella, F., Sellitto, C., Manzo, V., De Bellis, E., et al. (2021). BPIFB4 circulating levels and its prognostic relevance in COVID-19. J. Gerontol. A Biol. Sci. Med. Sci. 76 (10), 1775–1783. doi:10.1093/gerona/glab208
Coronavirus Disease 2019 (COVID-19) Treatment Guidelines (2021). Coronavirus disease 2019 (COVID-19) treatment guidelines. Bethesda (MD): National Institutes of Health (US.
Dobrijevic, Z., Robajac, D., Gligorijevic, N., Sunderic, M., Penezic, A., Miljus, G., et al. (2022). The association of ACE1, ACE2, TMPRSS2, IFITM3 and vdr polymorphisms with COVID-19 severity: A systematic review and meta-analysis. EXCLI J. 21, 818–839. doi:10.17179/excli2022-4976
Gómez, J., Albaiceta, G. M., García-Clemente, M., López-Larrea, C., Amado-Rodríguez, L., Lopez-Alonso, I., et al. (2020). Angiotensin-converting enzymes (ACE, ACE2) gene variants and COVID-19 outcome. Gene 762, 145102. doi:10.1016/j.gene.2020.145102
Gunal, O., Sezer, O., Ustun, G. U., Ozturk, C. E., Sen, A., Yigit, S., et al. (2021). Angiotensin-converting enzyme-1 gene insertion/deletion polymorphism may be associated with COVID-19 clinical severity: A prospective cohort study. Ann. Saudi Med. 41 (3), 141–146. doi:10.5144/0256-4947.2021.141
Gusev, E., Sarapultsev, A., Solomatina, L., and Chereshnev, V. (2022). Molecular mechanisms of pathogenesis, prevention, and therapy of COVID-19: Summarizing the results of 2021. Int. J. Mol. Sci. 23 (3), 14210. doi:10.3390/ijms232214210
Hou, Y., Zhao, J., Martin, W., Kallianpur, A., Chung, M. K., Jehi, L., et al. (2020). New insights into genetic susceptibility of COVID-19: An ACE2 and TMPRSS2 polymorphism analysis. BMC Med. 18 (1), 216. doi:10.1186/s12916-020-01673-z
Jackson, C. B., Farzan, M., Chen, B., and Choe, H. (2022). Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 23 (1), 3–20. doi:10.1038/s41580-021-00418-x
Jahanafrooz, Z., Chen, Z., Bao, J., Li, H., Lipworth, L., and Guo, X. (2022). An overview of human proteins and genes involved in SARS-CoV-2 infection. Gene 808, 145963. doi:10.1016/j.gene.2021.145963
Jin, Y., Yang, H., Ji, W., Wu, W., Chen, S., Zhang, W., et al. (2020). Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 12 (4), 372. doi:10.3390/v12040372
Kamel, N. A., El Wakeel, L. M., and Aboshanab, K. M. (2021). Exploring SARS-CoV-2 spikes glycoproteins for designing potential antiviral targets. Viral Immunol. 34 (8), 510–521. doi:10.1089/vim.2021.0023
Karakaş Çelik, S., Çakmak Genç, G., Pişkin, N., Açikgöz, B., Altinsoy, B., Kurucu İşsiz, B., et al. (2021). Polymorphisms of ACE (I/D) and ACE2 receptor gene (Rs2106809, Rs2285666) are not related to the clinical course of COVID-19: A case study. J. Med. virology 93 (10), 5947–5952. doi:10.1002/jmv.27160
Li, J., Wang, Y., Liu, Y., Zhang, Z., Zhai, Y., Dai, Y., et al. (2022). Polymorphisms and mutations of ACE2 and TMPRSS2 genes are associated with COVID-19: A systematic review. Eur. J. Med. Res. 27 (1), 26. doi:10.1186/s40001-022-00647-6
Möhlendick, B., Schönfelder, K., Breuckmann, K., Elsner, C., Babel, N., Balfanz, P., et al. (2021). ACE2 polymorphism and susceptibility for SARS-CoV-2 infection and severity of COVID-19. Pharmacogenetics genomics 31 (8), 165–171. doi:10.1097/FPC.0000000000000436
Masoud, H., Elassal, G., Hassany, M., Shawky, A., Hakim, M., Zaky, S., et al. (2020). Management Protocol for COVID-19 Patients MoHP Protocol for COVID19 November 2020.
Monticelli, M., Hay Mele, B., Benetti, E., Fallerini, C., Baldassarri, M., Furini, S., et al. (2021). Protective role of a TMPRSS2 variant on severe COVID-19 outcome in young males and elderly women. Genes (Basel) 12 (4), 596. doi:10.3390/genes12040596
Öztürk, R., Taşova, Y., and Ayaz, A. (2020). COVID-19: Pathogenesis, genetic polymorphism, clinical features and laboratory findings. Turkish J. Med. Sci. 50 (1), 638–657. doi:10.3906/sag-2005-287
Rarani, F. Z., Rashidi, B., Najaf Abadi, J. M. H., Hamblin, M. R., Reza Hashemian, S. M., and Mirzaei, H. (2022). Cytokines and microRNAs in SARS-CoV-2: What do we know? Mol. Ther. Nucleic acids 29, 219–242. doi:10.1016/j.omtn.2022.06.017
Ravikanth, V., Sasikala, M., Naveen, V., Latha, S. S., Parsa, K. V. L., Vijayasarathy, K., et al. (2021). A variant in TMPRSS2 is associated with decreased disease severity in COVID-19. Meta gene 29, 100930. doi:10.1016/j.mgene.2021.100930
Rouaud, F., and Méan, I. (2022). The ACE2 receptor for coronavirus entry is localized at apical cell-cell junctions of epithelial cells. Cells 11 (4), 627. doi:10.3390/cells11040627
Sabbatino, F., Conti, V., Franci, G., Sellitto, C., Manzo, V., Pagliano, P., et al. (2021). PD-L1 dysregulation in COVID-19 patients. Front. Immunol. 12, 695242. doi:10.3389/fimmu.2021.695242
Schönfelder, K., Breuckmann, K., Elsner, C., Dittmer, U., Fistera, D., Herbstreit, F., et al. (2021). Transmembrane serine protease 2 polymorphisms and susceptibility to severe acute respiratory syndrome coronavirus type 2 infection: A German case-control study. Front. Genet. 12, 667231. doi:10.3389/fgene.2021.667231
Shi, G., Kenney, A. D., Kudryashova, E., Zani, A., Zhang, L., Lai, K. K., et al. (2021). Opposing activities of IFITM proteins in SARS-CoV-2 infection. EMBO J. 40 (3), e106501. doi:10.15252/embj.2020106501
Shikov, A. E., Barbitoff, Y. A., Glotov, A. S., Danilova, M. M., Tonyan, Z. N., Nasykhova, Y. A., et al. (2020). Analysis of the spectrum of ACE2 variation suggests a possible influence of rare and common variants on susceptibility to COVID-19 and severity of outcome. Front. Genet. 11, 551220. doi:10.3389/fgene.2020.551220
Suzuki, Y., Ruiz-Ortega, M., Lorenzo, O., Ruperez, M., Esteban, V., and Egido, J. (2003). Inflammation and angiotensin II. Int. J. Biochem. Cell Biol. 35 (6), 881–900. doi:10.1016/s1357-2725(02)00271-6
Wang, F., Cao, J., Yu, Y., Ding, J., Eshak, E. S., Liu, K., et al. (2021). Epidemiological characteristics of patients with severe COVID-19 infection in wuhan, China: Evidence from a retrospective observational study. Int. J. Epidemiol. 49 (6), 1940–1950. doi:10.1093/ije/dyaa180
Wang, Y., Wang, Y., Chen, Y., and Qin, Q. (2020). Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J. Med. virology 92 (6), 568–576. doi:10.1002/jmv.25748
Wulandari, L., Hamidah, B., Pakpahan, C., Damayanti, N. S., Kurniati, N. D., Adiatmaja, C. O., et al. (2021). Initial study on TMPRSS2 p.Val160Met genetic variant in COVID-19 patients. Hum. genomics 15 (1), 29. doi:10.1186/s40246-021-00330-7
Yamamoto, N., Nishida, N., Yamamoto, R., Gojobori, T., Shimotohno, K., Mizokami, M., et al. (2021). Angiotensin-converting enzyme (ACE) 1 gene polymorphism and phenotypic expression of COVID-19 symptoms. Genes (Basel) 12 (10), 1572. doi:10.3390/genes12101572
Keywords: COVID-19, ACE2, ACE1, TMPRSS2, severity, genetic polymorphism
Citation: Alaa A, Sarhan N, Lotfy El-Ansary MG, Bazan NS, Farouk K, Ismail RS, Schalaan MF and Abd-Allah ARA (2023) Association between genetic polymorphism, severity, and treatment response among COVID-19 infected Egyptian patients. Front. Pharmacol. 14:1209286. doi: 10.3389/fphar.2023.1209286
Received: 20 April 2023; Accepted: 09 June 2023;
Published: 22 June 2023.
Edited by:
Luis Abel Quiñones, University of Chile, ChileReviewed by:
Carmine Sellitto, University of Salerno, ItalyCopyright © 2023 Alaa, Sarhan, Lotfy El-Ansary, Bazan, Farouk, Ismail, Schalaan and Abd-Allah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abdelrahman Alaa, YWJkZWxyYWhtYW4xMTQ1NDlAbWl1ZWd5cHQuZWR1LmVn; Adel R. A. Abd-Allah, YXJhYmRhbGxhaEBob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.